

Abstract
Background
Low vision rehabilitation aims to optimise the use of residual vision after severe vision loss, but also aims to teach skills in order to improve visual functioning in daily life. Other aims include helping people to adapt to permanent vision loss and improving psychosocial functioning. These skills promote independence and active participation in society. Low vision rehabilitation should ultimately improve quality of life (QOL) for people who have visual impairment.
Objectives
To assess the effectiveness of low vision rehabilitation interventions on health‐related QOL (HRQOL), vision‐related QOL (VRQOL) or visual functioning and other closely related patient‐reported outcomes in visually impaired adults.
Search methods
We searched relevant electronic databases and trials registers up to 18 September 2019.
Selection criteria
We included randomised controlled trials (RCTs) investigating HRQOL, VRQOL and related outcomes of adults, with an irreversible visual impairment (World Health Organization criteria). We included studies that compared rehabilitation interventions with active or inactive control.
Data collection and analysis
We used standard methods expected by Cochrane. We assessed the certainty of the evidence using the GRADE approach.
Main results
We included 44 studies (73 reports) conducted in North America, Australia, Europe and Asia. Considering the clinical diversity of low vision rehabilitation interventions, the studies were categorised into four groups of related intervention types (and by comparator): (1) psychological therapies and/or group programmes, (2) methods of enhancing vision, (3) multidisciplinary rehabilitation programmes, (4) other programmes. Comparators were no care or waiting list as an inactive control group, usual care or other active control group. Participants included in the reported studies were mainly older adults with visual impairment or blindness, often as a result of age‐related macular degeneration (AMD). Study settings were often hospitals or low vision rehabilitation services. Effects were measured at the short‐term (six months or less) in most studies. Not all studies reported on funding, but those who did were supported by public or non‐profit funders (N = 31), except for two studies.
Compared to inactive comparators, we found very low‐certainty evidence of no beneficial effects on HRQOL that was imprecisely estimated for psychological therapies and/or group programmes (SMD 0.26, 95% CI ‐0.28 to 0.80; participants = 183; studies = 1) and an imprecise estimate suggesting little or no effect of multidisciplinary rehabilitation programmes (SMD ‐0.08, 95% CI ‐0.37 to 0.21; participants = 183; studies = 2; I2 = 0%); no data were available for methods of enhancing vision or other programmes. Regarding VRQOL, we found low‐ or very low‐certainty evidence of imprecisely estimated benefit with psychological therapies and/or group programmes (SMD ‐0.23, 95% CI ‐0.53 to 0.08; studies = 2; I2 = 24%) and methods of enhancing vision (SMD ‐0.19, 95% CI ‐0.54 to 0.15; participants = 262; studies = 5; I2 = 34%). Two studies using multidisciplinary rehabilitation programmes showed beneficial but inconsistent results, of which one study, which was at low risk of bias and used intensive rehabilitation, recorded a very large and significant effect (SMD: ‐1.64, 95% CI ‐2.05 to ‐1.24), and the other a small and uncertain effect (SMD ‐0.42, 95%: ‐0.90 to 0.07).
Compared to active comparators, we found very low‐certainty evidence of small or no beneficial effects on HRQOL that were imprecisely estimated with psychological therapies and/or group programmes including no difference (SMD ‐0.09, 95% CI ‐0.39 to 0.20; participants = 600; studies = 4; I2 = 67%). We also found very low‐certainty evidence of small or no beneficial effects with methods of enhancing vision, that were imprecisely estimated (SMD ‐0.09, 95% CI ‐0.28 to 0.09; participants = 443; studies = 2; I2 = 0%) and multidisciplinary rehabilitation programmes (SMD ‐0.10, 95% CI ‐0.31 to 0.12; participants = 375; studies = 2; I2 = 0%). Concerning VRQOL, low‐certainty evidence of small or no beneficial effects that were imprecisely estimated, was found with psychological therapies and/or group programmes (SMD ‐0.11, 95% CI ‐0.24 to 0.01; participants = 1245; studies = 7; I2 = 19%) and moderate‐certainty evidence of small effects with methods of enhancing vision (SMD ‐0.24, 95% CI ‐0.40 to ‐0.08; participants = 660; studies = 7; I2 = 16%). No additional benefit was found with multidisciplinary rehabilitation programmes (SMD 0.01, 95% CI ‐0.18 to 0.20; participants = 464; studies = 3; I2 = 0%; low‐certainty evidence).
Among secondary outcomes, very low‐certainty evidence of a significant and large, but imprecisely estimated benefit on self‐efficacy or self‐esteem was found for psychological therapies and/or group programmes versus waiting list or no care (SMD ‐0.85, 95% CI ‐1.48 to ‐0.22; participants = 456; studies = 5; I2 = 91%). In addition, very low‐certainty evidence of a significant and large estimated benefit on depression was found for psychological therapies and/or group programmes versus waiting list or no care (SMD ‐1.23, 95% CI ‐2.18 to ‐0.28; participants = 456; studies = 5; I2 = 94%), and moderate‐certainty evidence of a small benefit versus usual care (SMD ‐0.14, 95% CI ‐0.25 to ‐0.04; participants = 1334; studies = 9; I2 = 0%). ln the few studies in which (serious) adverse events were reported, these seemed unrelated to low vision rehabilitation.
Authors' conclusions
In this Cochrane Review, no evidence of benefit was found of diverse types of low vision rehabilitation interventions on HRQOL. We found low‐ and moderate‐certainty evidence, respectively, of a small benefit on VRQOL in studies comparing psychological therapies or methods for enhancing vision with active comparators.
The type of rehabilitation varied among studies, even within intervention groups, but benefits were detected even if compared to active control groups. Studies were conducted on adults with visual impairment mainly of older age, living in high‐income countries and often having AMD. Most of the included studies on low vision rehabilitation had a short follow‐up,
Despite these limitations, the consistent direction of the effects in this review towards benefit justifies further research activities of better methodological quality including longer maintenance effects and costs of several types of low vision rehabilitation. Research on the working mechanisms of components of rehabilitation interventions in different settings, including low‐income countries, is also needed.
Plain language summary
Low vision rehabilitation for better quality of life in visually impaired adults
What was the aim of the review? The aim of this review was to find out if low vision rehabilitation can improve quality of life (QOL) for vision impaired people. Cochrane Review authors collected and analysed all relevant studies to answer this question and found 44 studies.
Key messages Low vision rehabilitation does not appear to have an important impact on health‐related QOL however the evidence is very low‐certainty. There is low‐certainty evidence that some low vision rehabilitation interventions, particularly psychological therapies and methods of enhancing vision, may improve vision‐related QOL in people with sight loss compared to usual care.
What was studied in the review? A person who is vision impaired has problems with their eyesight. If the vision loss cannot be corrected by glasses or contact lenses, or otherwise treated, then low vision rehabilitation may help to improve quality of life for people with vision impairment.
There are different types of low vision rehabilitation and these include:
• Psychological therapies and group programmes to help people adapt to permanent vision loss and improve well‐being. • Methods of enhancing vision such as teaching the use of magnifying devices, or other technologies, or teaching skills to improve the use of residual vision in daily life. • Multidisciplinary rehabilitation programmes, which may include the use of magnifying devices and psychological therapies, as well as other services, including at patients’ homes. • Other less common types of rehabilitation services such as balance training or home safety programs.
What were the main results of the review? Cochrane Review authors identified 44 studies of low vision rehabilitation and QOL.
Most of these studies took place in vision rehabilitation services in high‐income countries. Many of the participants in these studies were older and had a diagnosis of macular degeneration. The studies considered psychological therapies and group programmes, methods of enhancing vision as well as multidisciplinary rehabilitation programmes. In these studies, vision impaired people completed questionnaires about their general health, their vision, or other aspects of well‐being.
Compared to people with vision loss who received no low vision rehabilitation:
• People with vision loss receiving psychological therapies and/or group programmes may experience:
⇒ no improvement in health‐related QOL (very low‐certainty); ⇒ some improvement in vision‐related QOL (low‐certainty).
• People with vision loss receiving methods of enhancing vision may experience:
⇒ some improvement in vision‐related QOL (very low‐certainty); ⇒ (there were no data available on health‐related QOL).
• People with vision loss receiving a multidisciplinary rehabilitation programme may experience:
⇒ little or no improvement in health‐related QOL (very low‐certainty); ⇒ some improvement in vision‐related QOL, particularly if an intensive programme is used (very low‐certainty).
Compared to people with vision loss who received usual care:
• People with vision loss receiving psychological therapies and/or group programmes may experience:
⇒ little or no improvement in either health‐related QOL (very low‐certainty) or vision‐related QOL (low‐certainty).
• people with vision loss receiving methods of enhancing vision may experience:
⇒ little or no improvement in health‐related QOL (very low‐certainty); ⇒ some improvement in vision‐related QOL (moderate‐certainty).
• People with vision loss receiving a multidisciplinary rehabilitation programme may experience:
⇒ little or no improvement in either health‐related QOL (very low‐certainty) or vision‐related QOL (low‐certainty).
There was some evidence that psychological therapies had a positive impact on self‐esteem (very low‐certainty) and depression (moderate‐certainty evidence)
There was no evidence to suggest any harms (adverse effects) of rehabilitation but data were limited.
How up‐to‐date is the review? Cochrane Review authors searched for studies published up to 18 September 2019.
Summary of findings
Summary of findings for the main comparison. Psychological therapies and/or group programmes compared to waiting list or no care for better quality of life in visually impaired adults.
| Psychological therapies and/or group programmes compared to waiting list or no care for better quality of life in visually impaired adults | |||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low‐vision services Intervention: low vision rehabilitation such as problem‐solving treatment (PST), self‐management programme Comparison: passive control group such as a waiting list | |||
| Outcomes | № of participants (studies) Follow‐up | Standardised mean difference (SMD) with low vision rehabilitation | Certainty of the evidence (GRADE) |
|
Health‐related quality of life measured with EQ‐5D |
54
(1 study) Short‐term maintenance effect |
SMD 0.26 SD worse (‐0.28 to 80) | ⊕⊝⊝⊝ VERY LOW1 |
|
Vision‐related quality of life measured with NEI‐VFQ and NEI‐VFQ‐7 |
285
(2 studies) Short‐term direct or maintenance effect |
SMD‐0.23 SD better (‐0.53 to 0.08) | ⊕⊕⊝⊝ LOW2 |
| Adverse events | 285
(2 studies) Short‐term direct or maintenance effect |
Brody 2002: No data available Nollet 2016: 2 AEs and 10 SAEs not related to rehabilitation |
⊕⊕⊝⊝ LOW3 |
| EQ‐5D: EuroQol 5 Dimensions; NEI‐VFQ: National Eye Institute Visual Functioning Questionnaire; SAEs: serious adverse events; VFQ: Visual Functioning Questionnaire | |||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||
1Downgraded 1 level due to study limitations (unclear risk of performance bias) and two levels due to very serious imprecision (small sample size of n = 54, and wide confidence interval crossing the line of no effect) 2Downgraded 1 level due to study limitations (unclear risk of performance bias) and one level due to serious imprecision (sample size of n = 285, and wide confidence interval crossing the line of no effect) 3Downgraded 1 level due to study limitations (unclear risk of performance bias) and no reporting of adverse events in 1 study
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Summary of findings 2. Methods of enhancing vision compared to waiting list or no care for better quality of life in visually impaired adults.
| Methods of enhancing vision compared to waiting list or no care for better quality of life in visually impaired adults | |||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low‐vision services Intervention: low vision rehabilitation such as immediate low vision assessment, provision of magnifying aids and training, low vision outpatient service, customised prism glasses Comparison: passive control group such as a waiting list, delayed low vision assessment, low vision examination and no intervention, placebo prisms | |||
| Outcomes | № of participants (studies) Follow‐up | Standardised mean difference (SMD) with low vision rehabilitation | Certainty of the evidence (GRADE) |
| Health‐related quality of life | No data were available for this outcome | ||
|
Vision‐related quality of life measured with questionnaires: NEI‐VFQ‐ 25, VA‐LV‐VFQ48, Activity Inventory, IVI |
262
(5 studies) Short‐term direct or maintenance effect |
SMD ‐0.19 SDs (better) (‐0.54 better to 0.15 worse) | ⊕⊝⊝⊝ VERY LOW1 |
| Adverse events | 262
(5 studies) Short‐term direct or maintenance effect |
Kaltenegger 2019 reported no adverse events. No data available for the other studies | not applicable |
| NEI‐VFQ: National Eye Institute Visual Functioning Questionnaire; VA‐LV‐VFQ: Veterans Affairs Low Vision Visual Functioning Questionnaire | |||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||
1Downgraded one level due to study limitations (unclear risk of performance bias in 3 out of 4 studies) and two levels due to very serious imprecision (sample size of n = 237, and wide confidence interval crossing the line of no effect)
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Summary of findings 3. Multidisciplinary rehabilitation compared to waiting list or no care for better quality of life in visually impaired adults.
| Multidisciplinary rehabilitation compared to waiting list or no care for better quality of life in visually impaired adults | ||||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low‐vision services Intervention: low vision rehabilitation such as multidisciplinary low vision rehabilitation plus home visit, multidisciplinary low vision programme Comparison: passive control group such as a waiting list | ||||
| Outcomes | № of participants (studies) Follow‐up | Standardised mean difference (SMD) with low vision rehabilitation | Certainty of the evidence (GRADE) | Explanation |
|
Health‐related quality of life measured with EQ‐5D, SF‐36 |
183 (2 studies) | SMD ‐0.08 SD (better)
(‐0.37 to 0.21) Short‐term direct or maintenance effect |
⊕⊝⊝⊝ VERY LOW1 | |
|
Vision‐related quality of life measured with NEI‐VFQ, VFQ 48 questionnaire |
193 (2 studies) | See comment Short‐term direct or maintenance effect |
⊕⊝⊝⊝ VERY LOW2 | Both studies beneficial, but large effect in a large trial delivering intensive rehabilitation (Stelmack 2008: SMD: ‐1.64, 95%CI ‐2.05 to ‐1.24) and less benefit in the other (Acton 2016: SMD ‐0.42, 95%: ‐0.90 to 0.07), P = 0.0001 for inconsistency |
| Adverse events | 193 (2 studies) |
Acton 2016: 19 AEs probably unrelated to treatment Stelmack 2008: no (S)AEs related to the study. Short‐term direct or maintenance effect |
⊕⊕⊝⊝ LOW3 | |
| EQ‐5D: EuroQol 5 Dimensions; SAEs: serious adverse events; SF‐36: Short Form‐36 item Health Survey; VA‐LV‐VFQ: Veterans Affairs Low Vision Visual Functioning Questionnaire | ||||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||
1Downgraded one level due to study limitations (unclear risk of performance bias) and two levels due to very serious imprecision (sample size of N = 183, and wide confidence interval crossing the line of no effect)
2Downgraded one level due to study limitations (unclear risk of performance bias), two levels due to very serious imprecision (sample size of N = 193, and wide confidence interval crossing the line of no effect) and one level due to heterogeneity (both studies beneficial, but important and significant effect in a large trial delivering intensive rehabilitation and less benefit in the other)
3Downgraded one level due to study limitations (unclear risk of performance bias) and no reporting of adverse events in 1 study
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Summary of findings 4. Psychological therapies and/or group programmes compared to active control for better quality of life in visually impaired adults.
| Psychological therapies and/or group programmes compared to active control for better quality of life in visually impaired adults | |||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low‐vision services Intervention: low vision rehabilitation such as a health education programme, self‐management programme with usual rehabilitation care, stepped‐care (including cognitive behavioural therapy, problem‐solving treatment and/or referral to general practitioner), expressive writing course, problem‐solving treatment, behavioural activation Comparison: active control group such as an individual low vision programme, usual low vision rehabilitation, usual care by low vision service or other care providers, neutral writing exercise, supportive therapy | |||
| Outcomes | № of participants (studies) Follow‐up | Standardised mean difference (SMD) with low vision rehabilitation | Certainty of the evidence (GRADE) |
|
Health‐related quality of life measured with EQ‐5D, SF‐36 and a general health measure |
600
(4 studies) Long and short‐term maintenance effect |
SMD ‐0.09 SDs better (‐0.39 to 0.20) | ⊕⊝⊝⊝ VERY LOW1 |
|
Vision‐related quality of life measured with NEI‐VFQ‐17 and 25, IVI, LVQOL 18, vision=specific mental health questionnaire |
1245
(7 studies) Long and short‐term maintenance effect |
SMD ‐0.11 SDs better (‐0.24 to 0.01) | ⊕⊕⊝⊝ LOW2 |
| Adverse events | 1453
(9 studies) Long and short‐term maintenance effect |
No data available for Eklund 2008, Girdler 2010, Bryan 2014, Rees 2015, Rovner 2007, Rovner 2013, Rovner 2014, Tey 2019. Van der Aa 2015: no (S)AEs related to the study. |
⊕⊝⊝⊝ VERY LOW3 |
| EQ‐5D: EuroQol‐5 Dimensions; NEI‐VFQ: National Eye Institute Visual Functioning Questionnaire; IVI: Impact of Vision Impairment profile, LVQOL: low vision quality of life questionnaire | |||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||
1Downgraded one level due to study limitations (unclear risk of performance bias) and two levels due to very serious imprecision (sample size of N = 473, and wide confidence interval crossing the line of no effect)
2Downgraded one level due to study limitations (unclear risk of performance bias), one level due to imprecision (large sample size of N = 1118, but confidence interval including the line of no effect)
3Downgraded one level due to study limitations (unclear risk of performance bias) and no reporting of adverse events in 7 studies
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Summary of findings 5. Methods of enhancing vision and/or group programmes compared to active control for better quality of life in visually impaired adults.
| Methods of enhancing vision compared to active control for better quality of life in visually impaired adults | |||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low vision services Intervention: low vision rehabilitation such as CCTV training sessions from a low vision therapist, home‐based low vision rehabilitation, low vision devices with instruction, usual comprehensive vision rehab and access to desk top video magnifier, CCTV and training, low vision support service, nonportable and portable electronic devices Comparison: active control group such as CCTV instructions from supplier, clinic‐based low vision rehabilitation, low vision devices without instruction, usual comprehensive vision rehab without access to desk top video magnifier, eccentric viewing training, placebo support by a nurse, nonportable devices only | |||
| Outcomes | № of participants (studies) Follow‐up | Standardized Mean Difference (SMD) with Low vision rehabilitation | Certainty of the evidence (GRADE) |
|
Health‐related quality of life measured with EQ‐5D, SF‐36 |
443
(2 studies) Short‐term maintenance effect |
SMD ‐0.09 SD (better) (‐0.28 to 0.09) | ⊕⊝⊝⊝ VERY LOW1 |
|
Vision‐related quality of life measured with questionnaires: VISQOL, LVQOL subscales, VA‐LV‐VFQ‐48, VFQ‐25, Activity Inventory, IVI |
660
(7 studies) Short‐term direct or maintenance effect |
SMD ‐0.24 SD (better) (‐0.40 to ‐0.08) | ⊕⊕⊕⊝ MODERATE2 |
| Adverse events | 660
(7 studies) Short‐term direct or maintenance effect |
Burggraaff 2012: no AEs. Stelmack 2017: 10 AEs not treatment‐related. No data available for Draper 2016, Jackson 2017, Leat 2017, Pearce 2011, Taylor 2017. |
⊕⊝⊝⊝ VERY LOW3 |
| EQ‐5D: EuroQol 5 Dimensions, SF‐36: Short Form 36‐item Health Survey, VISQOL: vision‐related quality of life, VFQ: Visual Functioning Questionnaire; VA‐LV‐VFQ: Veterans Affairs Low Vision Visual Functioning Questionnaire; IVI: Impact of Vision Impairment profile, LVQOL: low vision quality of life questionnaire | |||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||
1Downgraded one level due to study limitations (unclear risk of performance bias) and two levels due to very serious imprecision (sample size of N = 443, but wide confidence interval crossing the line of no effect)
2Downgraded one level due to study limitations (unclear risk of performance bias and other domains at unclear or high risk of bias in some studies); no downgrade for imprecision (large sample size of N = 660, and confidence interval consistent with small effects)
3Downgraded one level due to study limitations (unclear risk of performance bias) and no reporting of adverse events in 7 studies
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Summary of findings 6. Multidisciplinary rehabilitation compared to active control for better quality of life in visually impaired adults.
| Multidisciplinary rehabilitation compared to active control for better quality of life in visually impaired adults | |||
|
Patient or population: adults (>= 18 years) with an irreversible visual impairment Setting: low vision services Intervention: low vision rehabilitation such as pooled community + centre‐ and community‐based low vision service delivery, family rehabilitation intervention where family is present at all stages, enhanced low vision rehabilitation including home visits Comparison: active control group such as community placebo home visits, individual rehabilitation intervention with no family present, conventional low vision rehabilitation and control home visits from a community worker with no rehabilitation, conventional clinic‐based low vision rehabilitation including placebo home visits | |||
| Outcomes | № of participants (studies) Follow‐up | Standardised mean difference (SMD) with low vision rehabilitation | Certainty of the evidence (GRADE) |
|
Health‐related quality of life measured with WHO‐QOL, SF‐36 |
375
(2 studies) Long‐term maintenance effect |
SMD ‐0.10 SD (better) (‐0.31 to 0.12) | ⊕⊝⊝⊝ VERY LOW1 |
|
Vision‐related quality of life measured with IVI, FAQ, VCM1 |
464
(3 studies) Short‐term direct or long‐term maintenance effect |
SMD 0.01 SD (same) (‐0.18 to 0.20) | ⊕⊕⊝⊝ LOW2 |
| Adverse events | 464
(3 studies) Short‐term direct or long‐term maintenance effect |
No data available | not applicable |
| SF‐36: Short Form‐36 item Health Survey; WHO‐QOL: World Health Organization Quality of Life; IVI: Impact of Vision Impairment profile; VCM1: Vision‐related quality of life Core Measure 1, FAQ: Functional Assessment Questionnaire, observer‐rated functional visual performance test | |||
|
GRADE Working Group grades of evidence High‐certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate‐certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low‐certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low‐certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||
1Downgraded one level due to study limitations (unclear risk of performance bias) and two levels due to very serious imprecision (sample size of N = 443, and wide confidence interval crossing the line of no effect)
2Downgraded one level due to study limitations (unclear risk of performance bias), one levels due to imprecision (large sample size of N = 660, but confidence interval including moderate or small effects)
Note: the following rule of thumb can be used to interpret the clinical magnitude of meta‐analysis results expressed as SMD: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect.
Background
From a systematic review and meta‐analysis on global prevalence data, it has been estimated that approximately 216.6 million people have moderate to severe visual impairment (< 6/18) and that 36 million people are blind (Bourne 2017). Visual impairment is especially problematic in developing countries where approximately 80% of all visually impaired persons live. Vision loss mainly affects older people; 82% of those who are blind and 65% of those with mild to severe vision loss are 50 years or older (Pascolini 2012). Worldwide, the leading causes of visual impairment are uncorrected refractive error and cataract (Bourne 2017; Pascolini 2012). There certainly is a large regional variation, e.g. the leading conditions for visual impairment in high‐income countries are uncorrected refractive error, cataract, macular degeneration, diabetic retinopathy and glaucoma (Bourne 2014). Vision loss is one of the leading causes of disability in older people (Brody 2001). Besides physical dysfunction (Bookwala 2011; Hayman 2007; Kempen 2012), limitations in daily life activities (Bookwala 2011; Hayman 2007), depression and anxiety (Bookwala 2011; Kempen 2012; Van der Aa 2015), vision loss is associated with a decreased life satisfaction (Bookwala 2011; Brody 2001) and quality of life (QOL) (Stelmack 2012; Van Nispen 2009). In addition, visual impairment affects many social and work‐related aspects of people's lives, including computer work (Bruijning 2013) and driving (Massof 2007). Part of the World Health Organization's (WHO) global action plan 2014 to 2019 is to assess and monitor the magnitude and causes of visual impairment and to invest in programmes to eliminate avoidable blindness, which is also strongly recommended by the European initiatives (e.g. EC Vision). This plan also urges countries to evaluate their programmes and services as part of their overall health care system. The need of governments and their partners to invest in supporting those with irreversible visual impairment to overcome the barriers that they face in daily life is stressed as well (WHO 2013). This is also reflected in the new standards for low vision rehabilitation that have been initiated by the WHO (WHO 2017). During the last few decades, the outcome of rehabilitation has been measured mainly by performance‐based measures, such as reading speed, walking distance, functional performance of daily activities and other performance‐based measures. General or disease‐specific QOL questionnaires and other patient‐reported outcome measures have become increasingly important in the assessment of quality of health care, including rehabilitation (Amtmann 2011).
Description of the condition
Vision impairment includes low vision as well as blindness. There are different definitions for visual impairment given in the literature. We adopted the WHO criteria, because these are the most widely used. The WHO defines low vision as best corrected visual acuity in the better eye < 3/18 but ≥ 3/60, and/or visual field < 30º around the central point of fixation. Blindness is defined as best corrected visual acuity in the better eye < 3/60, and/or visual field < 10º around the central point of fixation (WHO 2007). Furthermore, we defined irreversible vision impairment as vision impairment with a duration of at least six months and/or chronic diseases such as diabetic retinopathy, age‐related macular degeneration or glaucoma as causes of the irreversible vision impairment.
Description of the intervention
Low vision rehabilitation for adults usually is a professional service which aims to optimise residual vision, but also to teach visually impaired people skills in order to improve (visual) functioning in daily life. Other aims may be to help patients with adaptation to vision loss or to improve psychosocial functioning. This may lead to more independence and active participation in society. Low vision rehabilitation should ultimately improve quality of life (QOL) of visually impaired patients.
Low vision rehabilitation is not available everywhere and, when present, is organised differently in nearly every country. Some countries may have multidisciplinary in‐ or outpatient centres, where occupational therapists, optometrists, low vision specialists, clinical physicists, psychologists, social workers, mobility and orientation trainers and computer trainers work closely together. Other countries have a single service system, where prescription of optical aids is done by one organisation and, for example, social work is provided by another. Some countries have their outpatient services linked to ophthalmology departments, e.g. in academic hospitals, where others have not. Individual or group sessions with social workers or psychologists seem to be increasingly common, as are the home environment assessments and training sessions in the use of optical or other aids (e.g. canes) and low vision software. Training in leisure time or vocational activities are important aspects of rehabilitation as well. Depending on agreements between organisations or policies in different countries, low vision rehabilitation services are either commercial, non‐profit or charity organisations. In some countries, low vision aids and services are reimbursed by health insurance, exceptional medical expenses acts or veterans affairs (European Network for Vision Impairment Training Education & Research: ENVITER; Lim 2014; Owsley 2009).
Why it is important to do this review
There have been several studies in the field of low vision rehabilitation, focusing on objective tasks or specific measures of functional ability such as reading speed (Virgili 2018) or other performance‐based measures. Although these measures are important and necessary to assess functioning, they do not capture all facets of the individual state (Scott 1999). Comprehensive patient‐reported outcome measures such as HRQOL or disease‐specific QOL have been introduced because of the growing interest of governments and health insurance companies in these outcome measures as parameters for quality of care (Amtmann 2011; Massof 2001; Stelmack 2001). In the field of low vision, there has been an increased attention on the theoretical constructs of VRQOL and visual functioning as important outcomes of rehabilitation. These constructs are measured by self‐report questionnaires, which are increasingly analysed with modern psychometric techniques, i.e. item response theory models (Pesudovs 2007). A comprehensive literature review of Binns and colleagues has shown that the evidence of vision rehabilitation services is not very clear with respect to HRQOL or VRQOL (Binns 2012). The authors did not specifically assess methodological quality and included observational studies as well. Skelton and colleagues performed a Cochrane Review to assess effectiveness of environmental and behavioural interventions for visually impaired older adults (60+) and found no RCTs (Skelton 2013). Hence, to date there has not been a systematic review that assesses the effectiveness, including certainty of evidence, of the various existing rehabilitation interventions using HRQOL, VRQOL or closely related patient‐reported outcomes of visually impaired adults aged 18 years or over. There may be a potential overlap, however, with the secondary outcomes of a previous Cochrane Review on orientation interventions to improve mobility in people with visual impairment (Virgili 2010). Studies on low‐vision rehabilitation for children were summarised in a Cochrane Review by Barker 2015 and a review by Elsman 2019, which found limited evidence for developmental and rehabilitation interventions on the participation and QOL of children with a visual impairment.
In order to develop better understanding of the most effective healthcare interventions for visually impaired people, it is necessary to draw on all forms of relevant scientific evidence. An essential step in this process is to collect and analyse the evidence from quantitative and comparative studies. The global action plan for 2014 to 2019 of the WHO stresses the importance of assessing effectiveness of eye health and rehabilitation services (WHO 2013) as are the new standards for services (WHO 2017). This review will describe the state‐of‐the‐art regarding evidence for low vision rehabilitation interventions up to September 2019. We aim to quantitatively synthesise the entire available literature on HRQOL, VRQOL and other closely related patient‐reported outcomes as an effect of rehabilitation for visually impaired adults. The secondary patient‐reported outcomes include the physical and functional, psychological and social domains so as to capture all health and well‐being outcomes available.
Objectives
To assess the effectiveness of low vision rehabilitation interventions on health‐related QOL (HRQOL), vision‐related QOL (VRQOL) or visual functioning and other closely related patient‐reported outcomes in visually impaired adults.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs). Non‐RCTs, quasi‐RCTs or observational studies were excluded.
Types of participants
We included studies in which the effect of low vision rehabilitation among adults (>= 18 years) of either gender, with a vision impairment according to the WHO 2007 definition. Included studies had to be about vision impairment of irreversible nature, which was defined as a duration of at least six months. This means there was a focus on chronic eye diseases such as diabetic retinopathy, age‐related macular degeneration or glaucoma. Studies that included participants of all ages were only included if separate data on adult participants were reported.
Types of interventions
We included RCTs that compared one or more rehabilitation interventions with waiting lists or no care, or, usual or other care. We excluded studies focusing on the following interventions or devices:
neuro‐rehabilitation interventions (e.g. eye‐movement after stroke, such as the Cochrane Review by Pollock 2011);
interventions to improve visual field loss after brain damage;
medical interventions (e.g. cataract surgery, retinal or telescope implants such as the review by Maghami 2014);
preferences of low vision aid designs (e.g. different brands or designs of head mounted magnification devices or canes).
Types of outcome measures
We included studies that measured HRQOL, VRQOL as two primary outcomes or related patient‐reported outcomes as secondary outcomes at any follow‐up time point after the intervention ended, such as physical and functional measures, psychological measures and/or social measures. RCTs with measured outcomes not related in any way to the outcomes of interest were considered ineligible, however, some descriptive information and main outcomes of these RCTs were reported in an additional table (Table 7).
1. Descriptive characteristics of relevant RCTs: exclusion based on outcome measures.
| Author year (country) |
Study design, follow‐up, sample size, % dropout |
Sample: mean age, % female, vision impairment | Setting and study type | Outcome measures | Intervention and control groups | Outcome of study |
| Ballemans 2012 (Netherlands) | 2‐arm RCT, 8 weeks, N = 68, 10% |
76 years, 60%, AMD, glaucoma, other conditions | Low vision rehabilitation service IV other programmes |
Process evaluation: usefulness and acceptability of intervention from participants’ and trainers’ perspectives | I: standardised orientation and mobility training C: regular orientation and mobility training (without protocol) |
Both the standardised and regular training showed to be useful and acceptable from both participants’ and trainers’ perspectives |
|
Campbell 2005 (New Zealand) |
4‐arm RCT, 1 year, N = 391, 8% |
84 years, 68%, AMD, cataract, DRP, eye surgery | Home‐based IV other programmes |
Number of falls and injuries and costs of implementation of the intervention | I: home safety assessment and modification programme by OT I: exercise programme by PT + vitamin D I: intervention 1 + 2 C: social visits |
The home safety programme reduced falls and was more cost‐effective than the exercise programme. The exercise group was not effective in reducing falls. |
|
Chen 2012 (China) |
2‐arm RCT, 16 weeks, N = 40, 45% |
84 years, vision impairment |
Residential care homes IV other programmes |
Knee proprioception, concentric isokinetic knee strength, sensory organisation | I: Tai Chi (Yang style) C: music percussion activity |
After Tai Chi, significant improvement was seen in knee proprioception and visual and vestibular ratios. Tai Chi can improve balance control. |
|
Connors 2014 (United States) |
3‐arm RCT, Immediate, N = 38, 0% |
28 years, 47% ocular related blindness |
Laboratory IV other programmes |
Performance of virtual navigation in virtual target building, physical navigation and drop‐off tasks in actual target building | I: video game for full exploration of virtual environment I: directed navigation by sighted facilitator and specific paths in game C: video game but not corresponding with target virtual environment |
Highly interactive and immersive exploration of the virtual environment engages a blind user to develop skills akin to positive near transfer of learning. |
|
Dannenbaum 2010 (Canada) |
2‐arm RCT, 7 weeks, N = 32, unknown |
83 years, partially sighted, legally blind | Day centre for the visually impaired IV other programmes |
Balance tests with open and closed eyes, perceived balance | I: balance training C: sitting stretching exercises |
Perceived confidence in balance increased after training, however, objectively no improvement was found. |
|
Elliot 2014 (United States) |
2‐arm RCT, 5 weeks N = 228, 9% |
75 years, 58% N = 29 visually impaired, N = 199 normally sighted |
Laboratory, home‐based II methods to enhance vision |
Useful field of view performance | I: speed of processing training C: social and computer contact |
Speed of processing training effectively improved useful field of view performance. |
|
Szlyk 2000 (United States) |
3‐arm RCT, 3‐6 months, N = 25 |
47 years, 48% various (hereditary) retinal diseases |
Laboratory‐based training and on‐road driving II methods to enhance vision |
Clinical vision tests, functional orientation and mobility tasks, driving skills, psychophysical measures | I: bioptic telescopes and training I: lenses and training C: lenses without training |
Significant improvement in visual skills using a bioptic telescope, including driving‐related skills |
AMD: age‐related macular degeneration C: control group DRP: diabetic retinopathy I: intervention group OT: occupational therapy PT: physical therapy RCT: randomised controlled trial
Primary outcomes
We evaluated studies that assessed QOL using validated one‐dimensional or multidimensional questionnaires. Examples of generic HRQOL questionnaires are the Short Form‐36 (SF‐36) and the Euroqol‐5 dimensions (EQ‐5D). Examples of VRQOL and visual functioning questionnaires are the VF‐14, the National Eye Institute Visual Functioning Questionnaire (NEI‐VFQ) with different item lengths and the Low Vision Quality of Life questionnaire (LVQOL). HRQOL questionnaires are valuable for policy makers to compare effects of different healthcare interventions and to make informed decisions on how to spend resources. However, we are aware that HRQOL questionnaires are found to be less sensitive to change than disease‐specific outcome measures. Therefore, we believe interpretations should be made using both generic and disease‐specific outcome measures; we did not place a hierarchy in the sense that one outcome would be more important than the other.
Self‐reported questionnaires filled out by the individual, a relative or independent rater were considered eligible for inclusion. Additionally, the questionnaires that were used in different studies had to be validated in terms of reliability (the extent to which a test effectively measures the underlying concept correctly) and validity (the extent to which a test measures the underlying concept). Even though it adds to heterogeneity, different end points regarding timing were allowed and considered in the meta‐analysis:
short‐term: outcomes up to six months after baseline (direct effect within one month after intervention, or maintenance effects, one month to six months after intervention);
long‐term: outcomes more than six months after baseline (direct effect within one month after intervention, or maintenance effects, one month or longer after intervention).
Secondary outcomes
Secondary outcomes were patient‐reported outcomes closely related to QOL concerning health and well‐being, such as:
physical and functional measures (e.g. activities of daily living, mobility and orientation, reading);
psychological measures (e.g. depression, mood, anxiety, adaptation to vision loss, self‐esteem);
social measures (e.g. loneliness or independence).
The timing of the secondary outcome assessment was similar to that of the primary outcomes.
Adverse outcomes
If reported, all adverse outcomes in RCTs were mentioned in the review, which could be serious adverse events or adverse events, related or unrelated to the trial or intervention studied.
Search methods for identification of studies
Electronic searches
The Cochrane Eyes and Vision Information Specialist conducted systematic searches in the following electronic databases for RCTs and controlled clinical trials. There were no restrictions by language or year of publication. The date of the search was 18 September 2019.
Cochrane Central Register of Controlled Trials (CENTRAL; 2019, Issue 9) (which contains the Cochrane Eyes and Vision Trials Register) in the Cochrane Library (searched 18 September 2019) (Appendix 1).
MEDLINE Ovid (1946 to 18 September 2019) (Appendix 2).
Embase Ovid (1980 to 18 September 2019) (Appendix 3).
Cumulative Index to Nursing and Allied Health Literature (CINAHL) EBSCO (1937 to 18 September 2019) (Appendix 4).
PsycINFO Ovid (1806 to 18 September 2019) (Appendix 5).
International Standard Research Clinical Trial Number (ISRCTN) registry (www.isrctn.com/editAdvancedSearch; searched 18 September 2019) (Appendix 6).
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov; searched 18 September 2019) (Appendix 7).
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp; searched 18 September 2019) (Appendix 8).
Searching other resources
We searched reference lists of relevant articles to find additional trials. We manually searched the Visual Impairment Research journal from January 1999 to the last issue in December 2006 and several related proceedings. In addition, we contacted authors of relevant trials to identify further published and/or unpublished reports. We manually searched the proceedings of the International Society for Low Vision Research and Rehabilitation (ISLRR) of their International Conferences on Low Vision held between 1999 to 2017 for relevant trials. There were no language or data restrictions in the searches.
Data collection and analysis
Selection of studies
Three review authors, working independently, assessed the titles and abstracts resulting from the electronic searches. Full copies of all seemingly relevant papers were obtained and assessed according to the 'Criteria for considering studies for this review'. We only assessed trials that met these criteria. Disagreements about whether a trial should be included were resolved by discussion and consensus. In cases where additional information was needed before deciding whether to include a trial, we obtained the full report.
Data extraction and management
Three review authors working independently extracted data using a data extraction form developed by Cochrane. Any discrepancies were resolved by discussion. We contacted investigators to obtain missing data if necessary. For most studies, data were obtained directly from the trial reports. If the source of data was from a personal communication with an investigator, we reported this in Notes in the Characteristics of included studies table.
Furthermore, since QOL and depression data are often skewed with more persons having favourable outcomes, we considered log‐transforming data. However, since the raw data were not available and skewness was difficult to assess with certainty from means and standard deviations (SDs) only, it was decided not to create precision that might not hold in reality.
Assessment of risk of bias in included studies
Two review authors working independently assessed risk of bias according to the methods set out in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). Six parameters were considered: random sequence generation (selection bias), allocation concealment (selection bias), blinding (masking) of participants and personnel (performance bias), masking of outcome assessment (detection bias), incomplete outcome data addressed (attrition bias) and selective outcome reporting (reporting bias). See Table 8 for more information on these parameters.
2. Parameters for assessing risk of bias.
Any other sources of bias were reported under notes in the Characteristics of included studies table. |
Each parameter was graded as a low, high or unclear risk. Every study was assessed separately by two review authors. We resolved discrepancies between assessments by discussion or by consulting another review author. Finally, we planned to address reporting bias by using funnel plots if more than 10 studies could be pooled. Since fewer than 10 studies could be pooled per comparison, it was decided not to report publication bias.
Measures of treatment effect
Data analysis was conducted according to Section 4.8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017). Questionnaire outcomes usually are continuous outcomes with different scaling for different questionnaires (e.g. summary scores for Likert‐type scales). This means that standardised mean differences (SMD) are indicated to synthesise data. The SMD is the difference in mean effects in the experimental and control groups divided by the pooled standard deviation of participants’ outcomes (see Chapter 9, Section 9.2.3.2 of the Cochrane Handbook). The value of the SMD thus depends on both the size of the effect (the difference between means) and the standard deviation of the outcomes (the inherent variability among participants). The SMD expresses the intervention effect in standard units rather than the original units of measurement. However, this is inevitable when comparing outcomes using different questionnaires. We extracted means, mean differences, standard deviations, standard errors and/or P‐values from the studies in order to calculate SMDs, which were summarised in forest plots and in the 'Summary of Findings' tables. SMDs were interpreted as (Cohen's) effect sizes, where 0.2 represents a small effect, 0.5 represents a moderate effect and 0.8 represents a large effect. If only one study was available in a comparison, forest plots showed SMDs whereas in the text, mean differences were also reported for the main outcomes.
Unit of analysis issues
Participants (rather than eyes) were the unit of analysis in this systematic review. Unit of analysis issues were studied using multiple outcomes or subscales to measure a single construct (e.g. HRQOL measured by a physical and a mental health summary score of the SF‐36, or depression measured by two depression questionnaires), or studies having multiple intervention or control groups. This was solved (post hoc decision) by choosing only one questionnaire when similar constructs were measured in one study, or by combining the means and SDs of subscales (e.g. SF‐36 mental and physical summary score) into one effect estimate. Although it can be considered unconventional to report one score of a multidimensional questionnaire where it is common to report summary scores of subscales, this overcomes the issue of presenting correlated data in the meta‐analysis.
Dealing with missing data
If data were missing or difficult to interpret from a paper, if feasible, our intention was to contact the authors for more information on whether they thought missing data was (completely) at random. Missing data were expected to be an issue when many respondents were lost to follow‐up, or if there were an unequal loss to follow‐up in the trial arms (attrition bias). During the data extraction, missing data were described in tables for every study, also with respect to baseline imbalances between respondents and those lost to follow‐up on the main outcomes (missingness not at random).
Assessment of heterogeneity
Before data synthesis, heterogeneity was assessed by examining the characteristics of each study separately and for every planned comparison with respect to clinical diversity (variability in participants, interventions, controls and outcomes) and methodological diversity (variability in study design and risk of bias). We planned to use forest plots to present study results. These included a Chi2 test for statistical heterogeneity and the I2 test which estimated the amount of heterogeneity between trials by describing the percentage of variation between studies.
In order to deal with heterogeneity in the interventions and comparators, we decided (post hoc) to conduct two sets of analyses dividing studies with inactive control groups, such as no care or a waiting list, from studies with active comparators. An active comparator was defined as 'usual care' by some authors, but we acknowledge that no standard exists to define usual care and we briefly describe its components for each comparison. An active comparator could also be some other type of programme, such as a lower dose of the studied intervention. Finally, we did not conduct an overall meta‐analysis for 'low vision rehabilitation', but presented them for each subgroup of analyses. Nonetheless, we believed it to be important to present different intervention groups in the same forest plot since this would allow formal and graphical heterogeneity assessment.
Data synthesis
In most cases, relevant data for the separate treatment arms could be obtained from the questionnaire outcomes (continuous data) in order to calculate SMDs. If data were not available, these studies were then excluded from our efforts to synthesise data. If two or more treatment arms were compared to a control group, combined data of treatment arms were entered in the forest plots or treatment arms were ignored if these were adding to clinical diversity. Combining means and SDs of study arms outcomes, or other reasons such as combining means and SDs of subscales of questionnaires, was performed in IBM SPSS version 22 and according to Chapter 7 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
As was recommended in Chapter 11 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2017), results were summarised in the 'Summary of Findings' (SoF) table using GRADE, where a) imprecision due to few participants (< 400), b) imprecision due to wide confidence intervals including no effect, imprecision due to wide confidence intervals including no effect and appreciable harm and benefit, c) unclear and/or high risk of bias limitations, d) indirectness (e.g. indirect comparison), inconsistency of effect expressed by extensive heterogeneity of results (I2 > 60%) were considered to be potential reasons to downgrade the certainty of evidence. Footnotes were used to explain reasons to downgrade the certainty of evidence. In the SoF table, the intervention subgroups were listed by most important outcomes (HRQOL, VRQOL) and by comparator (inactive or active), as were the SMDs, 95% confidence intervals, number of studies and persons included in the analysis. The overall assumed risk of the control group could not be calculated, since the outcome measures used were often different which means that different units of measurement were used.
Since heterogeneity was expected to be found (I² > 50%), the meta‐analysis was based on the random‐effects model if there were enough studies within one comparison. We had planned to use the fixed‐effects model If there were fewer than three trials in a certain comparison. However, this is not possible when a single forest plot is produced for several subgroups. Thus, we always used random‐effects and we chose pragmatically to comment on individual studies when heterogeneity was apparent due to poor overlap of 95% CIs of two studies in a subgroup.
Dealing with multiple study arms
To facilitate interpretation of results, we chose to ignore certain study arms in the data analysis as a post hoc decision, taking into account intervention and comparison subgroup definitions. This was done for three studies. In Christy 2012, the arm in which only the centre‐based intervention was presented was ignored. Three other arms remained: the community intervention arm was combined with the centre plus community intervention arm and compared to the community intervention plus placebo home‐visits which served as the control group (other care). In Reeves 2004, the conventional low vision rehabilitation arm was also ignored, facilitating a comparison between the community‐based enhanced rehabilitation to a placebo community‐based control group (other care). Finally, in Smith 2005, the standard prism prescription arm was ignored, facilitating a comparison between the customised prism spectacles and sham prism spectacles ('no' care).
Subgroup analysis and investigation of heterogeneity
Some studies presented only short‐ or long‐term data, or, both short‐ and long‐term data as trial outcomes. Since long‐term outcomes were scarce and were considered a possible threat to homogeneity of the data, we originally planned to first analyse data using short‐term outcomes only and if long‐term data were available, to enter them in the analyses and report separately if differences with only short‐term outcomes were relevant. However, given the small number of studies in each subgroup and the limitation in data reporting, we analysed the data as available.
Sensitivity analysis
We originally planned sensitivity analyses by excluding studies from the analysis if they presented unclear and/or high risk of bias on at least four out of six domains on which risk of bias was assessed, or, in case of outliers. However, following this procedure, given the small number of studies in each subgroup, with unclear or high risk of bias in at least one domain, we decided not to conduct such analyses.
Results
Description of studies
Results of the search
The electronic searches identified a total of 15,891 records (Figure 1). The Cochrane Information Specialist removed 2699 duplicates and screened the remaining 13,192 reports, of which 4626 were not relevant to the scope of the review. We reviewed the remaining 8566 reports and discarded 8403 records as not relevant to the scope of the review. We obtained 163 full‐text reports for potential inclusion in the review. We included 73 reports of 44 studies, see Characteristics of included studies table for details. Seventy‐two reports of 65 studies were excluded, see Characteristics of excluded studies table for details.
1.
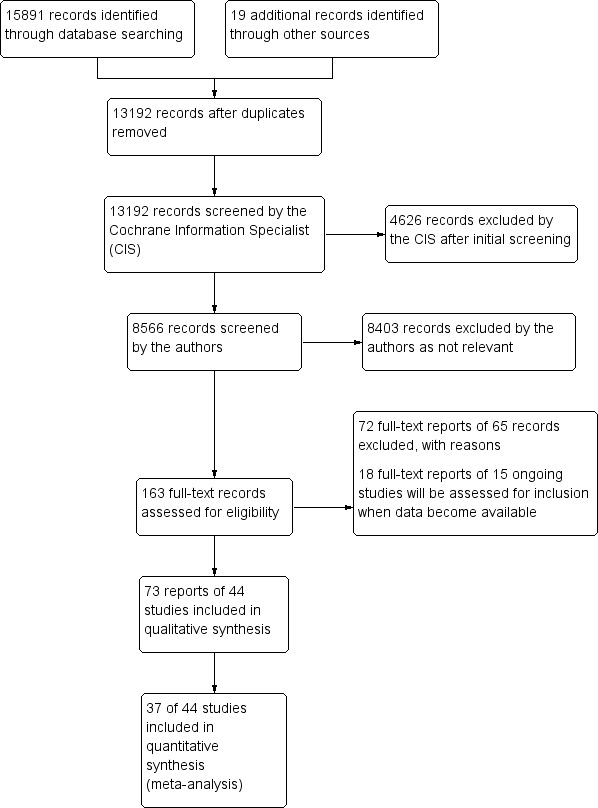
Study flow diagram.
Eighteen reports of 15 study protocols or design papers were found with potentially relevant outcomes for a future update of the current review (see Characteristics of ongoing studies) However, the studies by NCT00971464 and Zijlstra 2009 can be considered unpublished as reported by the study authors, and NCT00545220, Rees 2013, and Rubin 2011 might be considered unpublished since the end date of the study must have passed over more than two years ago (pending personal contact with the study authors).
Included studies
Forty‐four studies were reported in 73 documents and were included in the review (i.e. some studies had multiple publications; see Characteristics of included studies), of which 22 had a published study protocol in a journal and/or trials register (mainly the more recent studies). Twenty‐seven studies described the main HRQOL (N = 3) or VRQOL (N = 18) outcomes or both main outcomes (N = 8). Of these, 27 described both main and secondary outcomes (patient‐reported outcomes closely related to QOL) and in an additional 11 studies, only secondary outcomes were described.
Compared to the original protocol (Langelaan 2008), the focus on mono‐ versus multidisciplinary rehabilitation was not feasible due to clinical diversity. Low vision aids training or psychological treatment would both be considered monodisciplinary rehabilitation services, since one type of professional would be involved in treatment of the participant. However, based on content of the service and the professionals involved, to combine these completely different types of monodisciplinary rehabilitation did not seem to be the best option. Therefore, as a post hoc decision, they were categorised into four groups according to the types of interventions assessed:
psychological therapies and/or group programmes (20 studies);
methods of enhancing vision (14 studies);
multidisciplinary rehabilitation programmes (7 studies);
other programmes (3 studies)
In addition, the type of comparator was divided into inactive or active comparators:
inactive: no care (4 studies) or waiting list (14 studies);
active: usual care (13 studies) or other care (13 studies).
Types of interventions
1. Psychological therapies or group programmes, or both
Twenty studies assessed the effect of psychological therapies or group programmes, or both. In five studies, self‐management interventions were investigated (Brody 1999; Brody 2002; Girdler 2010; Rees 2015; Tey 2019). Two studies described educational interventions (Eklund 2008; Goldstein 2007). Individual problem‐solving treatment (PST) was investigated by Rovner 2007 and again in 2013 (Rovner 2013). PST falls under the umbrella of cognitive‐behavioural therapies where the focus is on the development of personal coping strategies that aim to solve daily issues and problems and target changing unhelpful patterns in cognitions, such as thoughts, beliefs, and attitudes, but also focus on changing behaviours and emotional regulation. In Van der Aa 2015, PST was part of a stepped‐care intervention, which also included watchful waiting, cognitive‐behavioural therapy based self‐help and a referral to the general practitioner. Nollet 2016 also studied PST and compared it to a referral to the general practitioner. There were other treatments which can be considered psychological therapies or group programmes, or both, i.e. group‐based peer support by Bradley 2005, expressive writing to deal with traumatic experiences by Bryan 2014, perceptual training versus group or individual psychological counselling by Conrod 1998, a stress‐reducing intervention for people with glaucoma by Kaluza 1996, group‐based rational emotive therapy by Mozaffar Jalali 2014, behavioural activation versus supportive treatment by Rovner 2014, social competence training for visually impaired employees by Rumrill 1999, and psychological therapy by Sun 2012.
Self‐management programmes
Brody 1999 compared a self‐management group programme of seven to 10 participants focusing on behavioural skills training in six sessions of 2 hours with a waiting list control group.
In a new study, Brody 2002 again compared a self‐management group programme, however this time, the intervention was compared to two control conditions. The self‐management group intervention of 8 to 10 participants consisted of six 2‐hour sessions and was led by an experienced professional in public health and behavioural medicine. The intervention was composed of both cognitive and behavioural components and focused on health education and enhancement of problem‐solving skills. The first control condition was an audiotape intervention consisting of a series of 12 hours of audiotapes of health lectures on age‐related macular degeneration (AMD) and healthy ageing, which they could listen to during a period of six weeks. The second control group was a waiting list control group.
Girdler 2010 also investigated a self‐management intervention plus usual care which they compared to the effects of usual care. The group intervention with six to 10 participants was led by an occupational therapist and a social worker and lasted eight weeks (total 24 hours). The programme was structured in several steps including understanding vision loss, optimising residual vision and other senses, practicing problem‐solving skills, daily life and safety skills, and focusing on the future. Usual care was an individual case management model and multidisciplinary work including, for example, a visual assessment and a prescription of low vision aids, occupational therapy, social work, and orientation and mobility training.
Rees 2015 investigated a low vision self‐management group programme held once a week over eight weeks, with 3‐hour sessions facilitated by two low vision rehabilitation counsellors. The programme also included a guest speaker from a national advocacy organisation, sessions with an orthoptist, a low vision technology expert and an orientation and mobility instructor. Two important components of the self‐management programme were problem‐solving skills training and goal planning. The control condition consisted of usual care, which was provided by the low vision rehabilitation service with an initial assessment by a member of the multidisciplinary team, an optometric assessment and prescription of optical aids. If needed, further training was provided by the multidisciplinary team.
Tey 2019 studied a low vision self‐management programme which was held four times during three 5‐hour weekly group sessions with six to eight participants. The intervention group also received usual care which consisted of standard ophthalmologic care, low vision aid training and referral to occupational or mobility training at the participant's request. In the self‐management group, participants could choose a goal they wished to achieve. Furthermore, there was a focus on the process of learning new techniques to enhance activities of daily living, information was provided, experiences with low vision were explored and problem‐solving skills were taught including positive self‐talk and the use of other senses (touch and hearing). The group work was aimed at sharing and practicing activities of daily living, as well.
Educational programmes
Eklund 2008 developed and investigated a health education programme called 'Discovering new ways', with groups of four to six participants. The programme was for eight weeks, two hours per week, and was led by an occupational therapist. The programme's main focus was on providing information and skills training. The intervention was compared with an individual standard intervention programme for the target group at the low vision clinic. Prescription of low vision aids and information about lighting was provided. If requested, additional information about the disease could be received. This programme mainly consisted of one to two 1‐hour sessions at the clinic followed by telephone contact.
Goldstein 2007 developed an educational video to help people achieve self‐efficacy with regard to obtaining and using assistive devices and other rehabilitation resources. The educational video addressed educational, emotional and motivational needs associated with low vision. Participants were given two weeks to watch the video. The control group was a waiting list control group.
Problem‐solving treatment (PST)
Rovner 2007 compared PST to usual care provided by an ophthalmologist or other health care providers. With the intervention, problem‐solving skills were taught to participants in addition to usual care (similar to control group). Six PST sessions were provided by trained therapists at the participant's home, with a duration of 45 to 60 minutes, for a period of eight weeks.
In a new study, PST was compared to supportive therapy as a placebo intervention (Rovner 2013). The intervention consisted of workshops, review and discussion of the PST at the participant's home. The supportive therapy control group was a standardised psychological nondirective treatment in which the therapist investigated the impact of vision loss on their lives. In contrast with PST, there was no discussion of vision function goals, problem‐solving or low vision rehabilitative strategies.
PST was also part of the stepped‐care intervention which consisted of four steps and was studied and compared to usual care by Van der Aa 2015. The first step comprised of three months of watchful waiting, involving an active decision not to treat the condition but, instead, to intermittently reassess its status. Telephone calls were made at baseline and after three months of watchful waiting. Participants could contact the executive researcher by telephone during this period, if necessary. In the second step, guided self‐help was based on a written, digital, audio, and Braille version of a self‐help course based on cognitive behavioural therapy (with specific vision‐related examples and exercises). Guidance was provided by trained and supervised occupational therapists from outpatient low vision rehabilitation organisations. Two face‐to‐face contacts took place at the beginning of the intervention for about 60 minutes and one to three telephone calls. Participants followed the intervention at home. In the third step, trained and supervised social workers and psychologists from the low vision rehabilitation centres offered problem‐solving treatment with a maximum of seven face‐to‐face contacts of about 60 minutes each. Finally, if symptoms of depression and anxiety persisted, a fourth step was available which was a referral to the general practitioner to discuss further treatment, such as the use of drug treatment. Stepped‐care plus usual care was compared to usual care and included outpatient low vision rehabilitation care and/or care that was provided by other healthcare providers.
Nollet 2016 also investigated PST and compared it to a referral to the general practitioner and to a waiting list condition. PST consisted of a brief manualised cognitive behavioural therapy based on the therapy used by Rovner 2007, however, this time the intervention included large‐print self‐help materials on depression and a list of vision‐related organisations. The optometrists providing the low vision assessment shared the participant’s treatment plan with the psychologists. Therapists who were rigorously trained, worked with the participants on an individual basis in their own home or at one of the research centres to teach them a seven‐step method for approaching and solving their problems. The referral condition consisted of a standardised letter sent to the participant’s physician within two weeks of randomisation. It informed the physician that his or her patient had screened positive for significant depressive symptoms and asked the physician to offer treatment according to National Institute for Health and Care Excellence (NICE) guidelines. Participants in the waiting list control arm received no intervention other than the 6‐week follow‐up low vision assessment.
Other psychological or group treatments, or both
Bradley 2005 studied group‐based peer support and information provision. Discussion groups were organised and six leaflets with information were distributed in six weekly sessions of 1.5 hours which were led by people who were experienced in living with macular degeneration. The control group was on a waiting list for six weeks.
Bryan 2014 investigated an expressive writing intervention and compared it to a non‐emotional topic writing task. The intervention group was asked to write about their most stressful experiences related to Stargardt’s eye disease and to reveal their deepest emotions. Participants wrote for 20 minutes on three separate days during a 1‐week period. The control group was instructed to write about their day completely factually and without emotions.
Conrod 1998 investigated the effect of perceptual training which consisted of five weekly one‐hour training sessions to enhance visual skills versus individual psychological counselling or group counselling with the same frequency.
Kaluza 1996 investigated the effect of a stress‐reducing intervention for people with glaucoma. The aim of the programme was to support patients' coping with glaucoma and to enable them to self‐regulate stress‐induced elevated intraocular pressure by teaching them relaxation techniques. Home assignments were part of the intervention as well. Eight weekly 90‐minute group sessions were conducted by an experienced clinical psychologist. The control group was a waiting list control group.
Kamga 2017 investigated the effect of a cognitive behavioural therapy‐based self‐care tool intervention (anti‐depressant skills workbook, mood monitoring tool, DVD on depression) plus up to three coaching 10‐minute phone calls by a trained former nurse. Controls were a waiting list group receiving the intervention after follow‐up with one phone call.
Mozaffar Jalali 2014 studied a group‐based rational emotive behavioural therapy which is a comprehensive, active‐directive psychotherapy which focuses on resolving emotional and behavioural problems and irrational beliefs. It was offered by therapists and compared to no treatment.
Rumrill 1999 studied the effects of a social competence training programme which aimed to increase accommodation request activity, self‐efficacy and knowledge of the Disabilities Act among employees with a visual impairment. Training duration was 16 weeks by a rehabilitation professional. The intervention was compared to a waiting list control group.
In contrast to earlier studies in which PST was investigated, Rovner 2014 now studied behavioural activation which is considered a functional analytic psychotherapy which focuses on targeting behaviours that might maintain or worsen depression. This therapy leaves the 'changing cognitions' part out, which can be quite difficult for older persons. Sessions were one hour in duration and were offered six times by occupational therapists, on top of low vision rehabilitation treatment. The control group received supportive therapy, offered in similar dose and intensity. Supportive therapy is a non‐directive, psychological treatment that provides emotional support and was used as a control for attention in this explanatory trial.
Sun 2012 investigated psychological therapy given to people with glaucoma while receiving clinical therapy from ophthalmologists versus clinical therapy only. Therapy was provided by psychodynamic psychiatrists for about six months. Ophthalmologists and nurses were also involved in psychological support. Ophthalmologists talked about prognosis, offered help to eliminate any fears, and to have a positive outlook on the disease. Specialist nurses provided psychological care during the period of surgery, but also offered telephone counselling and family follow‐up after discharge from the hospital. Participants were encouraged to listen to light music, and stroll in the woodlands or park to relax their minds. The control group received clinical treatment only, such as drug treatment and surgery, if needed.
2. Methods of enhancing vision
Fourteen studies assessed methods of enhancing vision. In six studies, low vision device training was assessed, i.e. CCTV‐training (Burggraaff 2012) and general low vision device training, including magnifiers or microscopes (Kaltenegger 2019; Mielke 2013; Pearce 2011; Scanlan 2004; Stelmack 2017). In five studies, prescription of low vision devices such as magnifiers and CCTVs was investigated sometimes with some form of training or self‐practice (Dunbar 2013; Jackson 2017; Leat 2017; Patodia 2017; Taylor 2017). The other studies focused on the effect of light adaptation (Brunnström 2004), vision strategies in reading training (Seiple 2011) and use of low vision devices, such as prism spectacles (Smith 2005). Control groups received delayed treatment (waiting list or cross‐over), placebo treatment or usual care.
Low vision device training
Burggraaff 2012 investigated the effect of a standardised CCTV training programme. The treatment group received usual instructions from the supplier when the CCTV was delivered at home combined with training sessions in the use of the device from a low vision therapist. Training sessions were once a week, with a duration of 60 minutes. Participants were trained until they had practiced with every assignment or until no further improvement in reading ability was to be expected. The control group received only usual instructions from the supplier who delivered the CCTV.
Kaltenegger 2019 investigated reading training with sequentially presented text (RSVP) on a laptop computer for home‐based training in addition to magnifying aids. The control group performed a placebo training (doing crossword puzzles) in addition to magnifying aids. Both groups performed the training exercises at home for 6 weeks, 5 days/week, 30 min/day.
Mielke 2013 investigated the effects in a pilot study of professional visual rehabilitation. The treatment group received magnifying visual aids and training. There was a waiting list control group.
Pearce 2011 investigated the effect of adding low vision device training on top of consultation with an optometrist for conventional low vision assessment. The intervention group received a one‐hour appointment with a low vision specialist to review handling of low vision devices and to discuss problems at home. The control group received a placebo treatment by a nurse, only measuring weight, height, vision and blood pressure in addition to the conventional low vision assessment.
Scanlan 2004 investigated a low vision service that made use of an extended period of education to assist clients with the use of low vision devices. The intervention group received an extended teaching programme in reading with microscopes (near vision telescopes), consisting of five one‐hour sessions at a low vision clinic. The control group received a traditional teaching session at the low vision clinic of one hour in reading with microscopes.
Stelmack 2017 studied low vision rehabilitation, where participants received basic low vision services plus one to three therapy sessions which included an instruction in eccentric viewing, the use of low vision devices, environmental modification, integration of low vision devices into the participant's lifestyle, and homework assignments to practice using low vision devices for everyday tasks. The control group received basic low vision services, where the optometrist dispensed low vision devices without therapy or homework assignments.
Prescription of low vision devices
Dunbar 2013 evaluated a low vision assessment, within two weeks of enrolment in a hospital‐based low vision centre versus a delayed assessment (waiting list). During the assessment, information was provided on aids and services and prescribed low vision aids were dispensed.
Jackson 2017 evaluated the immediate provision of a CCTV to usual comprehensive vision rehabilitation with optical aids of preference as compared to usual rehabilitation alone.
Leat 2017 compared the prescription of a CCTV associated with the request to practice everyday for 10 minutes twice for six weeks with a control group receiving eccentric viewing training and then home training with an observer giving feedback on accuracy.
Patodia 2017 evaluated a low vision outpatient treatment programme including examination, prescription of low vision devices for four‐week use to determine which would be most beneficial, and a single training session, i.e. binocular and monocular telescopes, telemicroscopes, magnifiers, portable CCTV and absorptive filters. Controls received a low vision examination, but no intervention.
Taylor 2017 evaluated the benefit of adding an electronic portable device on top of non‐electronic optical devices, compared to the use of non‐electronic optical devices in controls.
Other methods of vision enhancement
Brunnström 2004 evaluated the effect of additional light adaptation in the living room on top of basic light adjustments in other rooms such as the kitchen, bathroom and hall, which was the usual care received by the control group.
Seiple 2011 evaluated reading rehabilitation training exercises which were derived from the literature and from the laboratory’s curriculum. Three training groups were compared in a cross‐over design and also compared to a waiting list control group: 1) visual awareness and eccentric viewing; 2) control of reading eye movements; 3) reading practice with sequential presentation of lexical information.
Smith 2005 evaluated the effect of prism spectacles in people with AMD. Participants in the first treatment group received custom bilateral prisms which matched the participants' preferred power and base direction. Treatment group two received standard bilateral prisms (six prism diopters). The control group received placebo prisms, consisting of spectacles matched in weight and thickness to prism spectacles but without the prism.
3. Multidisciplinary rehabilitation programmes
Seven studies evaluated outpatient multidisciplinary programmes which sometimes included home visits by professionals.
Acton 2016 evaluated the effect of home visits from a visual rehabilitation officer who assessed areas such as emotional issues, low vision function, lighting, personal care, medication management, kitchen tasks, household chores, entitlements, orientation and mobility, and communication. The control group was on a waiting list receiving no care.
Christy 2012 evaluated different methods of multidisciplinary low vision service delivery. Group 1 received centre‐based service delivery, which took place in vision rehabilitation centres and included a clinical assessment and prescription of low vision devices. A qualified rehabilitation professional trained all individuals in independent living skills, based on their individual needs, for three consecutive days (four to six hours per day) and six to 12 follow‐up visits (two to five hours per visit) at the centre. Group 2 received community‐based service delivery by trained rehabilitation workers who provided rehabilitation at the participant’s home environment. Frequency was similar to group 1 and family members and neighbours were involved in training. Group 3 received centre‐ and community‐based service delivery. Individuals were trained in needs‐based independent living skills on a one‐to‐one basis for three consecutive days, four to six hours a day at the centre by a rehabilitation professional. Additional training was provided at the participant's home by a community‐based rehabilitation worker with a similar frequency and family members and neighbours were also involved in training. Finally, group 4 received centre‐based services with non‐interventional community visits. The low vision intervention was similar to the model of the centre‐based service delivery, however, no additional follow‐up training was provided at the rehabilitation centre. Home visits made by community workers were non‐interventional.
Draper 2016 compared two programmes delivering five visits over two to three months: a home‐based low vision rehabilitation with visit 1, 3, 5 in the clinic and visit 2 and 4 at home, including low vision aids prescription and training, and home adaptations. The second programme was clinic‐based low vision rehabilitation with all five visits in the clinic.
McCabe 2000 evaluated a model of outpatient vision rehabilitation in order to assess whether involving families in rehabilitation would result in better rehabilitation outcomes. All participants in the study received the “Infirmary's standard vision rehabilitation programme” which included training in the use of prescribed optical and non‐optical devices, instruction in adaptive techniques, and adjustment counselling. In contrast to controls, in the treatment arm where family was involved, time was spent educating family members about the ophthalmic condition and the rehabilitation process. Families also used simulators to understand the nature of the participant's vision loss. The social work interview included an exploration of the meaning of vision loss for the family unit and the ways the family members worked together to adapt to the loss. In the control group, individual rehabilitation interventions focused solely on the participant. Family members were excluded from all sessions.
Pankow 2004 tested the effectiveness of a vision rehabilitation programme which included orientation and mobility training, blind rehabilitation teaching, such as occupational therapy, and a low vision evaluation by optometrists and social workers, all depending upon the participants’ needs. The control group was on a waiting list and merely received education regarding ocular disease.
Reeves 2004 investigated the effectiveness of different strategies of low vision rehabilitation. Group 1 received conventional low vision rehabilitation (CLVR) by the hospital eye service, which included optometric services or other hospital‐based services, such as social work (usual care). Group 2 received enhanced low vision rehabilitation (ELVR), which was CLVR enhanced by home visits from a rehabilitation officer who provided low vision interventions. Participants received three visits which took place at approximately two weeks, four to eight weeks and at four to six months after the first hospital low vision assessment. The control groups received a placebo treatment, which was CLVR supplemented with home visits from a community care worker, who did not provide rehabilitation, but gave general advice and support unrelated to vision (CELVR).
Stelmack 2008 evaluated an outpatient low vision rehabilitation programme for veterans with moderate and severe vision loss due to macular disease (LOVIT). Treatment consisted of five weekly sessions (approximately two hours per session) at the low vision clinic to teach strategies for more effective use of remaining vision and use of low vision devices. In addition, one home visit was provided to teach environmental adaptations and to set up low vision devices so that participants could practice using them in their homes. Each participant was assigned five hours of homework per week after each therapy session to practice performing everyday tasks. The control group was a waiting list control group, which received additional bimonthly telephone calls from low vision therapists during the four months.
4. Other programmes
There were three other intervention studies that were considered eligible for inclusion in this review.
Gleeson 2014 studied the Alexander technique to improve balance in participants with vision loss. The Alexander Technique lesson was given by an accredited teacher 12 times for 30 minutes in 12 weeks in addition to usual care. The technique provides a cognitive construct for examining habitual responses to the familiar stimuli that precede voluntary movements. Everyday activities were practiced during the lessons such as movements between sitting and standing, getting to and from the floor, walking, climbing stairs and carrying things. The control group received usual care from Guide Dogs.
Pinninger 2013 investigated a tango dance programme for people with AMD with sessions of one and a half hours twice a week, for four weeks. The control group was a waiting list control group.
Waterman 2016 used three treatment arms; 1) home safety programme by occupational therapist visiting twice and making safety modifications plus one phone call; 2) home safety plus home exercise programme stressing strength and balance, at least three times every week for 30 minutes, walking twice per week by occupational therapists who visited two times, and visits three times and phone calls twice per week by peer mentors; 3) control: usual care from NHS which made three social visits, as well as two telephone calls by trained voluntary lay visitors.
Types of participants
Among the psychological therapies or group programmes, or both, the number of participants randomised in the trials ranged from 12 to 265. The most common cause of visual impairment was AMD in most studies. Between 50% and 100% of the participants were female. Eight studies were performed in the USA, three in Australia, two in Germany, two in the United Kingdom, two in Canada, one in the Netherlands and Belgium, one in Singapore, one in China, one in Iran, and one in Sweden. Except for Rumrill 1999, most studies focused on older adults recruited from hospitals or low vision services.
Bradley 2005 included 12 participants with AMD (United Kingdom, mean age 76 years);
Brody 1999 included 92 participants with AMD (USA, mean age 79 years); a separate study, Brody 2002, included 252 participants with AMD (mean age 81 years), however, for the Brody 2006 study citation, a subsample of 32 participants was chosen (Brody 2002);
Bryan 2014 randomised 81 adults with Stargardt's disease (juvenile AMD, USA, mean age 42 years);
Conrod 1998 randomised 49 adults with low vision (78% AMD, Canada, mean age 70 years) and included a group of 50 adults who were fully sighted as well (mean age 70 years);
Kamga 2017 randomised 80 participants of whom 55% had AMD and 45% diabetic retinopathy as a cause of low vision (Canada, mean age 76 years);
Eklund 2008 included 253 participants with AMD (Sweden, mean age 79 years); participants were allowed to have relatively good visual acuities;
Girdler 2010 included 77 participants with age‐related vision disorders (Australia, 79% AMD, mean age 79 years);
Goldstein 2007 included 156 low vision participants (eye disorders not reported, USA, median age 78 years);
Kaluza 1996 included 23 participants with primary angle glaucoma (visual acuity not reported, Germany, mean age 52 years);
Mozaffar Jalali 2014 randomised 60 participants with blindness (Iran, age 20 to 60 years);
Nollet 2016 randomised 85 participants with low vision (United Kingdom, mean age 70 years);
Rees 2015 randomised 153 participants, of which 70% had AMD (Australia, mean age 80 years);
Rovner 2007 included 206 AMD participants (USA, mean age 81 years); Rovner 2013 included 241 participants with AMD (neovascular 88%, mean age 82 years); and in their latest study, Rovner 2014 randomised 188 AMD participants (USA, mean age 84 years);
Rumrill 1999 included 48 participants with low vision (eye disorders not reported, USA, mean age 44 years);
Sun 2012 included 100 participants with glaucoma (China, mean age 62 years);
Tey 2019 randomised 165 participants with glaucoma, DRP, RP, pathological myopia and other eye conditions (Singapore, mean age 60 years);
Van der Aa 2015 randomised 265 participants with low vision of which 46% had AMD (Netherlands and Belgium, mean age 74 years).
Among the methods of enhancing vision studies, the number of participants randomised in the trials varied between 14 and 323. In most studies, the cause of low vision was AMD. Between 3% and 73% of the participants were female. Four studies were from the UK, three from the USA, three from Canada, one from Sweden, one from the Netherlands, and two from Germany. All studies focused on older adults.
Brunnström 2004 included 46 participants of whom 61% had dry and wet AMD; other specified diagnoses were glaucoma (11%) and retinitis pigmentosa (4%) (Sweden, mean age 76 years);
Burggraaff 2012 included 122 participants of whom 68% had AMD (the Netherlands, mean age 77 years);
Coleman 2006a included 131 participants, however, the majority had relatively good vision (VA (visual acuity) > 20/32). Participants with a VA < 20/40 had AMD or cataract, numbers not reported (USA, mean age 80 years);
Dunbar 2013 included 100 participants with diabetic retinopathy (UK, mean age 57 years);
Kaltenegger 2019 included 37 participants with AMD (Germany, median age 72 years);
Mielke 2013 included 20 participants with AMD (Germany, mean age 79 years);
Jackson 2017 included 37 participants of which 73% had AMD or juvenile MD (USA, mean age 72 years);
Leat 2017 included 14 participants with AMD (Canada, mean age 82 years);
Patodia 2017 included 16 participants with glaucoma (Canada, mean age not reported);
Taylor 2017 included 100 participants of which 61% had AMD and 39% other vision disorders (UK, mean age 71 years);
Pearce 2011 included 120 low vision participants (eye disorders not reported, UK, mean age 73 years);
Scanlan 2004 included 64 participants with AMD (Canada, mean age 81 years);
Seiple 2011 included 30 participants with AMD in the intervention groups (USA, median age 79 years) and 6 in the control group (mean 78.5 years);
Smith 2005 included 243 participants with AMD (UK, mean age 81 years);
Stelmack 2017 randomised 323 participants with various types of macular disease of which only 3% was female (USA, mean age 80 years).
Among the multidisciplinary rehabilitation programmes, the number of participants randomised in the trials ranged from 30 to over 300 adult participants. Also in the multidisciplinary intervention studies, AMD was often the most common cause of low vision. Studies reported between 2% and 66% females among their populations. There were four American studies, two from the UK and one from India. Except for the Indian study, all studies focused on (older) adults.
Acton 2016 included 71 participants of whom 58% had AMD (UK, mean age 75 years);
Christy 2012 included 436 participants of whom 347 were aged 16 years or older, AMD was the most common cause of low vision (32%, India);
Draper 2016 included 55 participants with low vision, eye disorders not reported (USA, mean age approximately 64 years);
McCabe 2000 included 97 participants of whom 64% had AMD (USA, mean age 69 years, median 76);
Pankow 2004 included 30 participants who most frequently had AMD (USA, mean age 78 years);
Reeves 2004 included 226 participants with AMD (UK, median age 81 years);
Stelmack 2008 included 126 participants (98% male) mostly with macular disease (USA, mean age 79 years).
There were three studies focusing on other programmes related to low vision rehabilitation:
Gleeson 2014 randomised 120 visually impaired participants of whom 64% were female (USA, mean age 77.5 years);
Pinninger 2013 included 17 female participants with AMD (Australia, mean age 79 years);
Waterman 2016 included 49 participants with various eye diseases of which 57% had AMD (UK, mean age 81 years).
Types of outcomes
Main outcome measures
There were several QOL outcome measures used. For thepsychological therapies or group programmes, or both, potential comparisons could be made on HRQOL between Bradley 2005 who used the 12‐item Well‐Being questionnaire, Brody 1999 with the Quality of Well‐Being scale which is a comprehensive measure of HRQOL that includes functional scales for mobility, physical activity and social activity, Eklund 2008 who used a general health measure, stating diseases and Girdler 2010 who used the well‐known Short Form‐36 (SF‐36). In addition, Nollet 2016, Tey 2019 and Van der Aa 2015 used the Euroqol‐5 dimensions (EQ‐5D). On VRQOL and visual functioning, potential comparisons could be made between Brody 2002, Bryan 2014, Nollet 2016, Rovner 2007, Rovner 2013 and Rovner 2014 who all used the National Eye Institute Visual Functioning Questionnaire of different lengths (NEI‐VFQ‐ 7, 17 and 25 items). In addition, Rovner 2013 and Rovner 2014 used the Activity Inventory, Bradley 2005 used the MacDQOL, Nollet 2016 used the LV‐VFQ‐48 for reading ability, Rees 2015 and Tey 2019 the Impact of Vision Impairment (IVI) and Van der Aa 2015 the Low Vision Quality of Life questionnaire (LVQOL).
For methods of enhancing vision, potential comparisons could be made on HRQOL between Brunnström 2004 who used the Psychological and General Well‐Being scale (PGWB) which included items on well‐being, vitality and depression, Burggraaff 2012, Stelmack 2017 and Taylor 2017 who used the EQ‐5D, Stelmack 2017 who also used the SF‐36, and Taylor 2017 the WHO‐5. On VRQOL and visual functioning, potential comparisons could be made between Burggraaff 2012 who used the LVQOL, Leat 2017, Mielke 2013, Scanlan 2004 and Smith 2005 who used the NEI‐VFQ or the NV‐VFQ‐15 or Taylor 2017 who also used the VISQOL to measure VRQOL. In addition, Pearce 2011 and Dunbar 2013 used the Activity Inventory, Burggraaff 2012 part of the Dutch ICF Activity Inventory, and Jackson 2017 the reading subscale of the Activity Inventory, however, they also used the IVI; Kaltenegger 2019; Patodia 2017, Seiple 2011 and Stelmack 2017 used the Veterans Affairs VFQ‐48.
For themultidisciplinary rehabilitation programmes, potential comparisons could be made on HRQOL between Acton 2016 who used the EQ‐5D, Christy 2012 who used the World Health Organisation Quality Of Life questionnaire (WHOQOL), and Reeves 2004 and Stelmack 2008 who both used the SF‐36. On VRQOL and visual functioning, potential comparisons could be made between Christy 2012 who used the Impact of Visual Impairment (IVI), Reeves 2004 who used the Vision‐Related Quality of Life Core Measure (VCM1), Acton 2016; Draper 2016 and Stelmack 2008 who used the Veterans Affairs Visual Functioning Questionnaire‐48 (VA‐VFQ‐48) and McCabe 2000 who used the Functional Assessment Questionnaire which measures visual function and overall well‐being.
For the other programmes, measurements of VRQOL were made by Pinninger 2013 who used the NEI‐VFQ, Gleeson 2014 who used the IVI emotional well‐being subscale and Waterman 2016 who used the VCM1 and also the SF‐12 for a measure of HRQOL.
Secondary outcome measures
Secondary outcomes were patient‐reported outcomes closely related to QOL, concerning concepts of health and well‐being. With respect to physical and functional measures, examples were the Functional Independence Measure for Blind Adults (FIMBA), included by Pankow 2004 as an assessment of the participant's ability to perform daily tasks, orientation and mobility skills independently; the Dependency in ADL levels by Eklund and colleagues (2008; seeEklund 2008); and the Melbourne Low Vision ADL (MLVA) which consisted of questions on the performance of specified typical activities of daily living (not) dependent on vision, used by Smith 2005. The Perceived Visual Ability Scale (PVAS) was used by Gleeson 2014 for measuring mobility difficulty for a range of situations. The Health and Impact Questionnaire, used by Brody 1999 and Brody 2002, is an instrument that obtains, for example, questions about medical history, current medical conditions, medications and the impact of AMD. Brunnström 2004 used an interview in which ADL‐type questions were posed. Finally, Taylor 2017 used the five timed instrumental activities of daily living questionnaire (5‐TIADL).
The questionnaire for measuring perceived security in performing daily activities was developed as a primary outcome for the purpose of evaluating the health education programme of Eklund 2008. It measures participants' perceived security in performing specified tasks. Girdler 2010 used the Activity Card Sort as a primary outcome to measure participation levels.
Psychological measures, for example, to measure depression, mood disorders and anxiety, were as follows: the centre for Epidemiological Studies – Depression scale (CES‐D, used by Bryan 2014, Burggraaff 2012; Mielke 2013; Stelmack 2008, Van der Aa 2015), the Geriatric Depression Scale (GDS; Girdler 2010; Gleeson 2014, Mielke 2013; Nollet 2016; Pinninger 2013; Leat 2017 which was used as a primary outcome measure in the study by Brody as well (seeBrody 2002), the Beck Depression Inventory‐II (also used by Nollet 2016), the Patient Health Questionnaire‐9 (PHQ‐9 used by Acton 2016; Kamga 2017; Rovner 2013 and Rovner 2014), the Montgomery–Åsberg Depression Rating Scale (MADRS used by Kaltenegger 2019), the Profile Of Mood States (POMS) for emotional distress, a psychological strain questionnaire (used by Brody 1999; Brody 2002 as a primary outcome measure), the Warwick Edinburgh Mental Well‐being Scale by Acton 2016, the Perceived Stress Scale (PSS) by Bryan 2014, the Life Orientation Test‐Revised (LOT‐R; used by Brody 2002) which assesses an optimistic versus a pessimistic life outlook and the Mood Episodes section and the Global Assessment of Function Scale of the SCID‐IV (Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM‐IV) used by Brody 2002. Rovner 2007 assessed depressive disorders with the Schedule for Affective Disorders and Schizofrenia and the Structured Interview Guide for the Hamilton Depression Rating Scale. Van der Aa 2015 also used a diagnostic interview, namely the Mini International Neuropsychiatric Interview which is based on the DSM‐IV. Jackson 2017; Mozaffar Jalali 2014, Rees 2015 and Tey 2019 measured depression, anxiety and stress symptoms with the DASS. The study of Van der Aa 2015 also focused on anxiety, which was measured with the Hospital Anxiety Depression Scale ‐ Anxiety subscale (HADS‐A); Kamga 2017 measured generalised anxiety disorder with the GAD‐7.
Adaptation to vision loss was measured with the Adaptation to age‐related Vision Loss questionnaire (AVL, used by Acton 2016; Burggraaff 2012; Christy 2012; Girdler 2010; Rees 2015; Van der Aa 2015) and the Nottingham Adjustment Scale (NAS, used by Pankow 2004 and Reeves 2004).
Self‐efficacy and self‐esteem were measured with the Macular Degeneration Self‐Efficacy Questionnaire (AMD‐SEQ) which evaluates the degree of self‐confidence in the individual’s ability to handle situations related to AMD (used by Brody 1999 and Brody 2002 and adapted and used by Girdler 2010 to reflect age‐related vision loss). Mozaffar Jalali 2014 used Eysenck's self‐esteem questionnaire. Girdler 2010, Rees 2015 and Tey 2019 used the Generalised Self‐Efficacy Scale (GSES) and Kamga 2017 and Pinninger 2013 a Self‐Esteem Scale (SES). Rumrill 1999 used the Accommodation Self‐efficacy measure and an Accomodation Activity scale to assess a participant’s self‐efficacy in the accommodation request process. Sheres Self‐Efficacy Scale was designed to measure general expectancies. Conrod 1998 used a ‘beliefs questionnaire’ and an ‘expectations questionnaire’ to assess functional effects and attitudes toward low vision and blindness and whether expectations about the future play a meaningful role in the adjustment process. Goldstein 2007 measured emotional responses (sadness, fear, confusion, peace) to low vision and self‐efficacy with regard to obtaining and using assistive devices. Kaluza 1996 measured psychological strain with the Kurzfragebogen zur Aktuellen Beanspruchung (KAB). Mozaffar Jalali 2014 used the Jones irrational beliefs questionnaire. Pinninger 2013 used the Satisfaction With Life scale (SWL) which measures global perceptions of well‐being and contentment with life.
Social functioning was measured with the Duke Social Support Index (DSSI) which measures satisfaction in terms of frequency, content and quality of support and social interaction with family and friends (Brody 2002). Acton 2016 used the University of California Los Angeles Loneliness Scale, Bryan 2014 used a the Medical Outcomes Study Social Support Scale and Brunnström 2004 used a one‐item measure of loneliness. Gleeson 2014 measured participation with Keele's assessment of participation (KAP) and socialisation which was defined as the number of contacts with others. Rumrill 1999 used the Work Experience Survey which measures career maintenance barriers in people with disabilities.
Length of follow‐up, direct and maintenance effects
Short‐term follow‐up included measurements directly or within one month after treatment, one month after baseline (Jackson 2017; Mozaffar Jalali 2014; Patodia 2017 and Pinninger 2013), six weeks after baseline (Bradley 2005 and Leat 2017, whereas for Kaltenegger 2019 this measurement was used in the study before cross‐over of the control group to treatment), eight weeks after baseline (Kaluza 1996 and Kamga 2017), eight to nine weeks after baseline (Conrod 1998), 10 weeks after baseline which was within four weeks after the intervention (Brody 1999), two to three months after baseline (Draper 2016), four months after baseline (Stelmack 2008 and Taylor 2017), 18 weeks after baseline (Seiple 2011), six months after baseline (Sun 2012 and Waterman 2016), and, for McCabe 2000, the follow‐up measurement seemed to occur directly after one to five intervention visits but the length of follow‐up was not reported.
There were also short‐term follow‐up measurements reported with maintenance effects of between one and six months: the maintenance period was approximately four weeks after intervention for the study by Girdler 2010 with follow‐up 12 weeks after baseline, four to six weeks (Pankow 2004, 12 to 14 weeks after baseline), six weeks (Bryan 2014, seven weeks after baseline), seven weeks (Scanlan 2004, 12 weeks after baseline), approximately two to two and a half months (Burggraaff 2012; Dunbar 2013; Mielke 2013 and Pearce 2011, three months after baseline; Rovner 2014 and Rumrill 1999, four months after baseline), three to three and a half months (Goldstein 2007, three months after baseline and Stelmack 2017, four months after baseline), approximately four months (Acton 2016; Nollet 2016; Rovner 2007 and Rovner 2013, six months after baseline), approximately four and a half months (Brody 2002, six months after baseline) and six months post‐intervention and baseline (Brunnström 2004 and Tey 2019).
Long‐term follow‐up consisted of maintenance effects of four to five months post‐intervention (Christy 2012, nine months after baseline), six months following treatment (Rees 2015, approximately eight months after baseline), six to nine months post‐intervention (Reeves 2004, 12 months after baseline), nine months post‐intervention (Gleeson 2014, 12 months after baseline) and 28 months after intervention (Eklund 2008, approximately 30 months after baseline). Finally, Van der Aa 2015 produced a maintenance effect of at least 12 months following intervention, which was 24 months after baseline and included an intervention period of between three and 12 months.
Excluded studies
Of the 163 potentially useful full papers that were screened, there were 72 reports of 65 studies that were subsequently excluded mainly because they were RCTs or studies with other designs on topics that were not the focus of this review (e.g. medical or vision restoration therapy), or because of study designs: nonrandomised controlled studies (NRCTs), observational studies without comparison groups, of which two studies were written in Japanese, literature reviews, and other reasons such as irrelevant population (children) or intervention or questionnaire development articles; for some of the excluded studies that might be of interest, see: Characteristics of excluded studies table.
Furthermore, some studies were excluded because they did not measure any of the prespecified review outcomes, but the interventions could be interpreted as relevant, therefore, an additional table is included, see Table 7. For example, the quasi‐RCT of Culham 2009 was excluded, because it was set up to compare reading speed and satisfaction with different head mounted devices. Although a Visual Functioning questionnaire was used as a secondary outcome, the questionnaire was modified and the design of the study was not set up to properly assess VRQOL. Moreover, the study has been evaluated in the Cochrane Review by Virgili 2018 in its main outcomes, including a 'Risk of bias' assessment. The study by La Grow 2004 was excluded because of the matching of the intervention and a contrast group; randomisation was not possible. Participants in the contrast group were recommended by ophthalmic and optometric practices, living in areas where low vision services were not available.
Ongoing studies
Ongoing studies
There were 14 study protocols found of ongoing randomised studies that could not be used in the current review, but should possibly be included in the future update.
Risk of bias in included studies
The results of the quality assessment are described for all parameters which are shown in the Characteristics of included studies and 'Risk of bias' tables and which are summarised in Figure 2 and Figure 3. Almost all studies lacked information to properly assess risk of bias for some of the criteria. However, from the 20 psychological therapies, or group programmes, or both (type I interventions), Rovner’s studies (Rovner 2007; Rovner 2013; Rovner 2014), but also Van der Aa 2015 performed well on most risk of bias criteria. Considering the 14 studies in which methods of enhancing vision (type II interventions) were described, the studies by Burggraaff 2012; Dunbar 2013; Smith 2005 and Stelmack 2017 performed well. With respect to the seven multidisciplinary rehabilitation programmes (type III interventions), Reeves 2004 and Stelmack 2008 performed best and also from the other programmes (type IV interventions) Gleeson 2014 performed very well.
2.
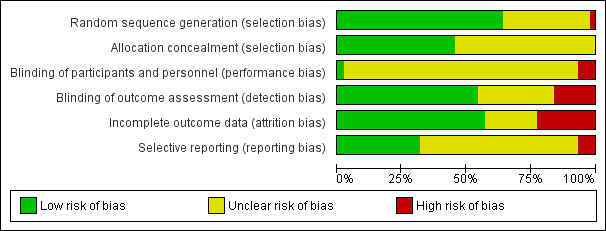
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
3.

Methodological quality summary: review authors' judgements about each methodological quality item for each included study. Studies were categorized into: (I) psychological therapies and/or group programs; (II) methods of enhancing vision; (III) multidisciplinary rehabilitation programs.
Not all studies reported on funding, but those that did were supported by public or non‐profit funders (N = 31), except for two studies which received low vision aids by commercial producers (Jackson 2017; Pankow 2004).
Allocation
In most studies (N = 27), the random sequence generation was considered to be good, because random number tables, or computer random number generators or other low tech methods were used to randomise participants (e.g. numbers drawn from a hat). In one study, risk for selection bias was assessed as high; Rumrill 1999 used a matching procedure in which first pairs of two participants were made, after which randomisation took place where one of a pair would be in the intervention group and the other in the control group. In other studies, methods were unclear.
In more than half of the studies (N = 24), allocation concealment was not reported, however, in the other 20 studies, it was reported and considered to be appropriately done e.g. by central allocation methods or use of sealed opaque envelopes.
Blinding
In the field of low vision, most trials had a pragmatic nature in which masking of participants and personnel was not possible. Therefore, these studies were assessed as having an unclear risk (N = 40). Still, for one study masking was possible and was done properly (Smith 2005). The study investigators randomised three types of prism glasses, of which one placebo was made similar in weight. Participants and the investigator doing the analyses were not aware which glasses were prescribed. In two studies, however, masking could not have been performed, and there could have been contamination between trial interventions. I.e. personnel were trained in the different treatment options in the study of Conrod 1998, which means personnel could have conveyed elements of treatment to the control group. Another example is the study by Pankow 2004, where researchers were also trainers of the intervention and outcome assessors at the same time.
In more than half of the studies (N = 24), the risk of detection bias was assessed as low risk, because masking of assessors was reported and performed accurately. In some studies, participants were notified that they should not reveal their allocation concealment. To gain insight into possible detection bias, outcome assessors were sometimes asked to guess in which treatment arm the participant would be (e.g. Rovner 2013; Van der Aa 2015). In 13 studies, the risk of detection bias was unclear and in another seven studies, it was considered to be high. Goldstein 2007 and Pankow 2004 reported that outcome assessors were not masked to group assignment; Pinninger 2013 reported that volunteers assisted in completion of the pre‐ and post‐test questionnaires; for the treatment arm, this meant an assessment at the treatment location, whereas the control group was assessed by telephone. Rumrill 1999 and Scanlan 2004 reported that trainers were also outcome assessors, which may stimulate socially desirable answering and may influence unbiased reporting of participants.
Incomplete outcome data
In 24 studies, the risk of attrition bias was considered to be low, because follow‐up rates and compliance were similar in the groups, analyses were often based on the intention‐to‐treat principle and attrition was limited. For 10 studies, attrition bias was unclear, but another 10 studies seemed to have a high risk. In these studies, a high risk assessment was often due for multiple reasons. Per‐protocol or as‐treated analyses were performed in Brody 1999, Mielke 2013 and Scanlan 2004 and possibly in Conrod 1998 and Kaluza 1996. In addition, Bryan 2014, Conrod 1998, Jackson 2017, Kaltenegger 2019, Leat 2017 and Mielke 2013 reported a relatively high attrition rate. Finally, Scanlan 2004 replaced participants with deteriorating vision, which can be considered a design flaw. Although it is difficult to indicate to what magnitude, missingness in the data analysis may have influenced the means and SDs of single studies and subsequently the SMD of the pooled outcomes.
Selective reporting
In 15 studies, protocols or trial registrations revealed that predefined outcomes of interest were assessed. In 26 studies, it was unclear if all relevant outcomes were assessed and in four studies, a high risk was expected because e.g. the outcome measure was not completely reported or other durations of follow‐up were planned. Contacting the authors did not provide us with an answer.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6
Low vision rehabilitation versus waiting list or no care
Fifteen studies provided data for this comparison. The effects on the primary outcomes are shown in Figure 4 and Figure 5.
4.
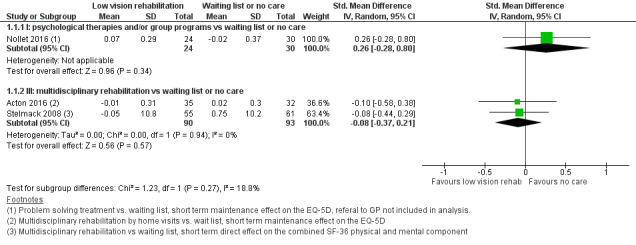
Forest plot of comparison: 1 Low vision rehabilitation versus waiting list or no care, outcome: 1.1 Health‐related quality of life.
5.
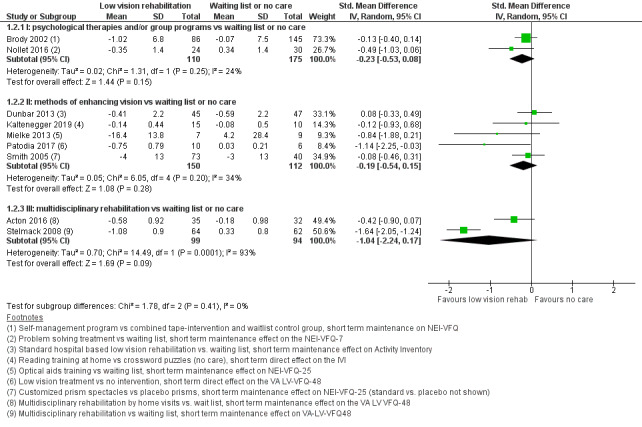
Forest plot of comparison: 1 Low vision rehabilitation versus waiting list or no care, outcome: 1.2 Vision‐related quality of life.
Primary outcomes
Health‐related quality of life
Three studies investigated the effect of a psychological or multidisciplinary interventions against an inactive comparator on the HRQOL outcome (Analysis 1.1).
1.1. Analysis.
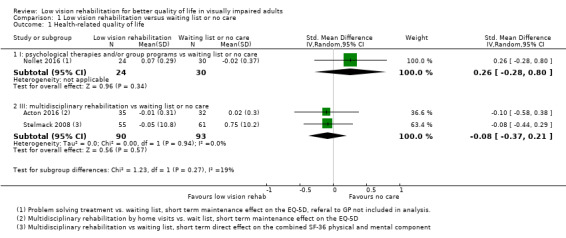
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 1 Health‐related quality of life.
Nollet 2016 (54 participants) investigated PST (group I) and compared it to a referral to the general practitioner; the short‐term maintenance effect was imprecise and did not suggest a benefit (standard mean difference (SMD) 0.26, 95% confidence interval (CI) ‐0.28 to 0.80; participants = 54; studies = 1). Two studies investigated multidisciplinary rehabilitation (group III). Stelmack 2008 (114 participants) evaluated an outpatient multidisciplinary low vision rehabilitation programme for veterans with moderate and severe vision loss due to macular disease (LOVIT) and Acton 2016 (67 participants) evaluated the effect of home visits from a visual rehabilitation officer. Both found effects (i.e. short‐term direct and maintenance, respectively) which favoured rehabilitation, but estimates were very imprecise and included no effect (SMD ‐0.08, 95% CI ‐0.37 to 0.21; participants = 183; studies = 2; I2 = 0%). This evidence was of very low‐certainty due to imprecision (‐2) and risk of bias (‐1) for both comparisons.
Vision‐related quality of life
Nine studies investigated the effect of psychological therapies, methods for enhancing vision and multidisciplinary interventions against an inactive comparator on the VRQOL outcome (Analysis 1.2).
1.2. Analysis.
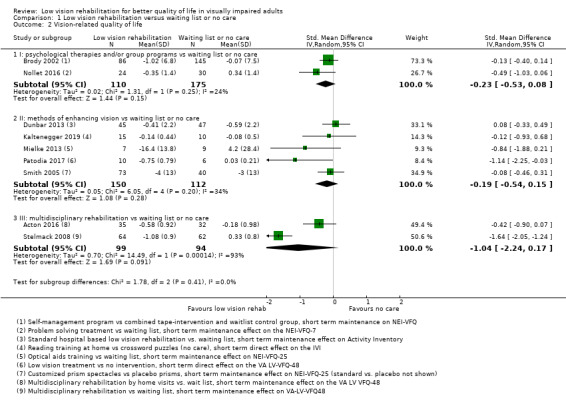
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 2 Vision‐related quality of life.
Two studies investigated group I interventions (psychological therapies and/or group programmes), i.e. Brody 2002: short‐term direct effects of a self‐management group programme; Nollet 2016: short‐term maintenance effects of PST. We found low‐certainty evidence of small and imprecisely estimated benefit (SMD ‐0.23, 95% CI ‐0.53 to 0.08; studies = 2; I2 = 24%).
Five studies investigated group II interventions (methods of enhancing vision), i.e. Dunbar 2013: rehabilitation in a hospital‐based low vision centre; Kaltenegger 2019: reading (self‐)training at home; Mielke 2013: professional rehabilitation with prescription of magnifying visual aids and training; Patodia 2017: prescription of low vision devices and training; Smith 2005: prism spectacles in AMD participants. All effects were short‐term maintenance effects, except for Patodia 2017 which investigated short‐term direct effects. The meta‐analysis suggested a small benefit but effects were moderately heterogenous and imprecisely estimated including no benefit (SMD ‐0.19, 95% CI ‐0.54 to 0.15; participants = 262; studies = 5; I2 = 34%). This evidence was of very low‐certainty due to imprecision (‐2), and risk of bias (‐1).
Two studies investigated group III interventions (multidisciplinary rehabilitation programmes) and yielded heterogeneous short‐term maintenance effects. Stelmack 2008 (126 participants) found a large and significant benefit in the LOVIT study (SMD: ‐1.64, 95% CI ‐2.05 to ‐1.24), which was at low risk of bias and used an intensive rehabilitation programme. Acton 2016 (67 participants) evaluated the effect of home visits from a visual rehabilitation officer and found a benefit but estimates were imprecise and included no effect (SMD ‐0.42, 95%: ‐0.90 to 0.07); the study was at unclear risk of bias regarding at least allocation concealment and estimates were imprecise. We did not consider the pooled estimate of these two studies because their confidence intervals did not overlap (P < 0.0001 for inconsistency). The two studies had domains at unclear, but not high risk of bias.
Secondary outcomes
Physical aspect of quality of life
Two studies investigated the effect on activities of daily living as a 'physical aspect' of QOL (Analysis 1.3) and against an inactive comparator.
1.3. Analysis.
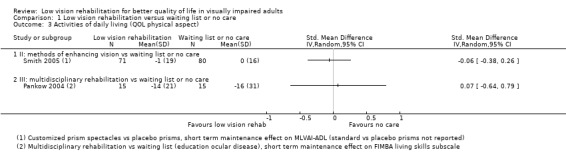
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 3 Activities of daily living (QOL physical aspect).
In group II, Smith 2005 (151 participants, short‐term maintenance effect) evaluated the effect of prism spectacles (methods of enhancing vision) in AMD participants and found no benefit (SMD ‐0.06; 95%CI ‐0.38 to 0.26). In group III, Pankow 2004 (30 participants, short‐term maintenance effect of multidisciplinary rehabilitation) delivered a vision rehabilitation programme which included orientation and mobility training, blind rehabilitation teaching, such as occupational therapy and a low vision evaluation by optometrists and social workers, all depending upon the participants’ needs and found no difference, but estimates were imprecise (SMD 0.07; 95%CI ‐0.64 to 0.79). The certainty of evidence was very low for both comparisons (‐2 for imprecision, ‐1 for risk of bias).
Psychological aspect of quality of life
Nine studies investigated the effect of the intervention groups on depressive symptoms (Analysis 1.4), five studies on self‐esteem (Analysis 1.5) and two studies on adaptation to vision loss Analysis 1.6 as a 'psychological aspect' of QOL and against an inactive comparator.
1.4. Analysis.
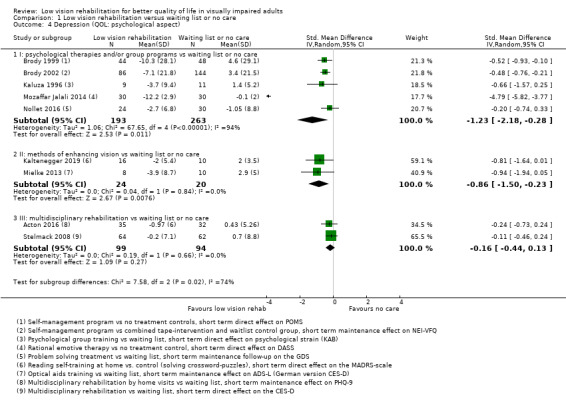
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 4 Depression (QOL: psychological aspect).
1.5. Analysis.
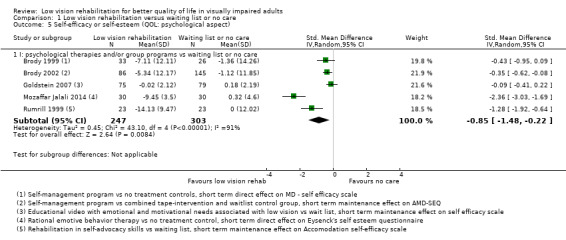
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 5 Self‐efficacy or self‐esteem (QOL: psychological aspect).
1.6. Analysis.
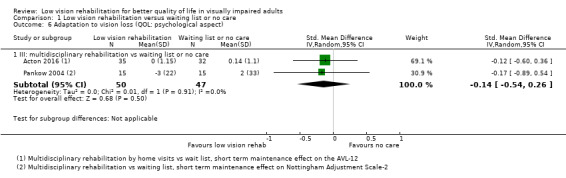
Comparison 1 Low vision rehabilitation versus waiting list or no care, Outcome 6 Adaptation to vision loss (QOL: psychological aspect).
Depression
Five studies assessing group I psychological therapies and/or group programmes on depression (Brody 1999 and Brody 2002: short‐term direct and maintenance effects, respectively, of self‐management programmes; short‐term direct effects by Kaluza 1996: stress‐reducing intervention, and Mozaffar Jalali 2014: group‐based rational emotive behavioural therapy; and short‐term maintenance effect of PST by Nollet 2016) found a large and significant, but imprecise benefit (SMD ‐1.23, 95% CI ‐2.18 to ‐0.28; participants = 456; studies = 5; I2 = 94%); effects were heterogenous and very large in one outlying study (Mozaffar Jalali 2014). The certainty of this evidence was very low (‐1 for risk of bias, ‐2 for imprecision, ‐1 for inconsistency). However, after removing the outlier which was a study with mainly unclear risk of bias, the effect was moderate and heterogeneity decreased substantively due to reasons that could not be explained (SMD ‐0.46, 95% CI ‐0.66 to ‐0.26; participants = 396; studies = 4; I2 = 0%), thereby also increasing the certainty of evidence to moderate (‐1 for risk of bias, ‐1 for imprecision).
Kaltenegger 2019 compared a reading (self‐)training at home with doing crossword puzzles as a placebo, and Mielke 2013 compared magnifying aids and training with a waiting list (both studies short‐term maintenance effect of group II methods for enhancing vision) and found a large but imprecisely estimated benefit (SMD ‐0.86, 95% CI ‐1.50 to ‐0.23; participants = 44; studies = 2; I2 = 0%); very low‐certainty of evidence for imprecision (‐1) and risk of bias (‐1).
Acton 2016 and Stelmack 2008 investigated the short‐term maintenance and direct effects, respectively, of group III multidisciplinary rehabilitation and found a small benefit which was imprecisely estimated and included no benefit (SMD ‐0.16, 95% CI ‐0.44 to 0.13; participants = 193; studies = 2; I2 = 0%). The certainty of this evidence was very low (‐1 for risk of bias, ‐2 for imprecision).
Self‐esteem
Five studies investigated the effect on self‐esteem (Analysis 1.5), all assessing group I psychological therapies and/or group programmes (Brody 1999; Brody 2002: short‐term direct and maintenance effects, respectively, of self‐management programmes; Goldstein 2007: short‐term maintenance effect of an educational video to help participants achieve self‐efficacy; Mozaffar Jalali 2014: short‐term direct effect of a group‐based rational emotive behavioural therapy; Rumrill 1999: short‐term maintenance effect of a social competence training). Overall effects were all in the direction of benefit but very heterogenous, thus the benefit was significant, but imprecisely estimated (SMD ‐0.85, 95% CI ‐1.48 to ‐0.22; participants = 550; studies = 5; I2 = 91%). The certainty of this evidence was very low (‐1 for risk of bias, ‐1 for imprecision, ‐1 for inconsistency). We were unable to find reasons for such high heterogeneity, but pooled the data as effects were in the direction of benefit for all studies.
Adaptation to vision loss
Acton 2016 and Pankow 2004 investigated the short‐term maintenance effect of group III multidisciplinary rehabilitation interventions on adaptation to vision loss (Analysis 1.6) and found an effect in the direction of benefit but very imprecisely estimated and included no benefit (SMD ‐0.14, 95% CI ‐0.54 to 0.26; participants = 97; studies = 2; I2 = 0%). The certainty of this evidence was very low (‐1 for risk of bias, ‐2 for imprecision).
Social aspect of quality of life
Although the studies by Acton 2016, Brody 2002, and Rumrill 1999 used some measure to investigate effects of an intervention versus an inactive comparator on a social aspect of QOL, these were not feasible for entering in a meta‐analysis.
Low vision rehabilitation versus active control group
Twenty‐three studies provided data for this comparison, in which interventions of interest were compared to usual care or other interventions. The effects on the primary outcomes are shown in Figure 6 and Figure 7.
6.
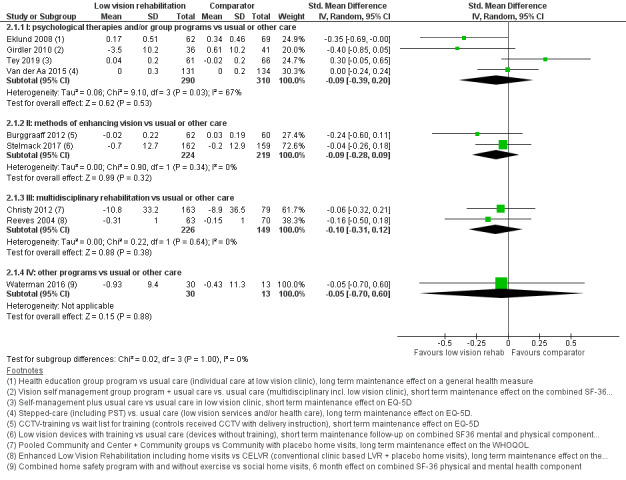
Forest plot of comparison: 2 Low vision rehabilitation versus active comparator, outcome: 2.1 Health‐related quality of life.
7.
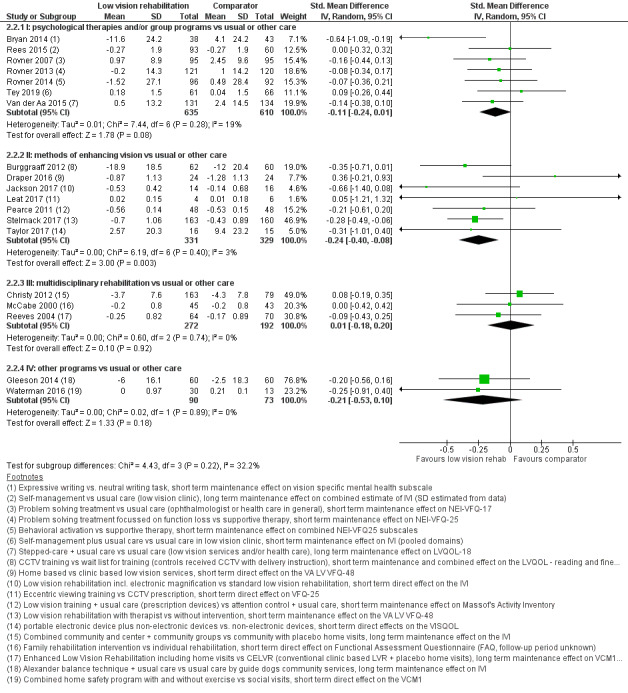
Forest plot of comparison: 2 Low vision rehabilitation versus active comparator, outcome: 2.2 Vision‐related quality of life.
Primary outcomes
Health‐related quality of life
Nine studies investigated the effect of psychological therapies, methods for enhancing vision, multidisciplinary interventions or other interventions against an active comparator on the HRQOL outcome (Analysis 2.1).
2.1. Analysis.
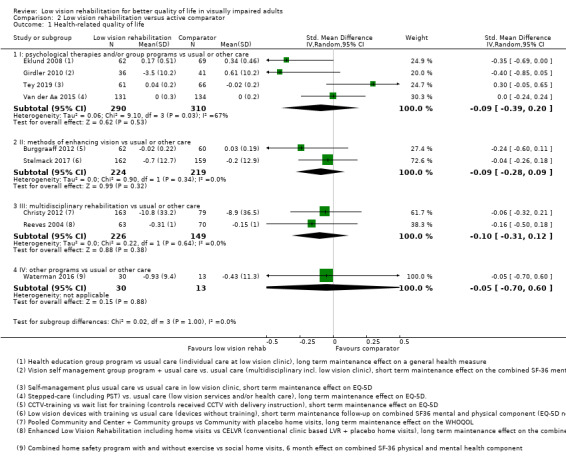
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 1 Health‐related quality of life.
There were four studies in group I psychological interventions: (Eklund 2008: long‐term maintenance effect of an educational programme by an occupational therapist versus standard low vision clinic; Girdler 2010 and Tey 2019: short‐term maintenance effects of a self‐management programme plus usual care versus usual care; Van der Aa 2015: long‐term maintenance effect of a stepped‐care intervention including cognitive‐behavioural therapy‐based self‐help and/or PST plus usual care versus usual care consisting of outpatient low vision rehabilitation care or any other (medical) care needed). Overall effects suggested small benefits, but were heterogenous and included no benefit (SMD ‐0.09, 95% CI ‐0.39 to 0.20; participants = 600; studies = 4; I2 = 67%) and larger in Eklund 2008 and Girdler 2010. The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
Two studies investigated short‐term maintenance effects of group II methods for enhancing vision (Burggraaff 2012: standardised CCTV training programme versus usual instruction by the supplier; Stelmack 2017: additional sessions on eccentric viewing, use of low vision devices, environmental modification plus low vision care versus low vision care only). Overall effects were modest and imprecisely estimated, including no benefit (SMD ‐0.09, 95% CI ‐0.28 to 0.09; participants = 443; studies = 2; I2 = 0%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
Two studies investigated long‐term maintenance effects of group III multidisciplinary rehabilitation (Christy 2012; different methods of multidisciplinary low vision service delivery versus centre‐based non‐interventional community visits; Reeves 2004: home visits from a rehabilitation officer in addition to conventional low vision rehabilitation versus conventional low vision rehabilitation only). The results suggested a small or no benefit (SMD ‐0.10, 95% CI ‐0.31 to 0.12; participants = 375; studies = 2; I2 = 0%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
Waterman 2016 (group IV other programmes, 43 participants) investigated short‐term direct effects of a home safety programme by occupational therapist with usual care and found an imprecise effect which did not suggest a benefit (SMD ‐0.05, 95% CI ‐0.70 to 0.60; very low‐certainty evidence).
Vision‐related quality of life
Nineteen studies investigated the effect of psychological therapies, methods for enhancing vision, multidisciplinary interventions or other interventions against an active comparator on the VRQOL outcome (Analysis 2.2).
2.2. Analysis.
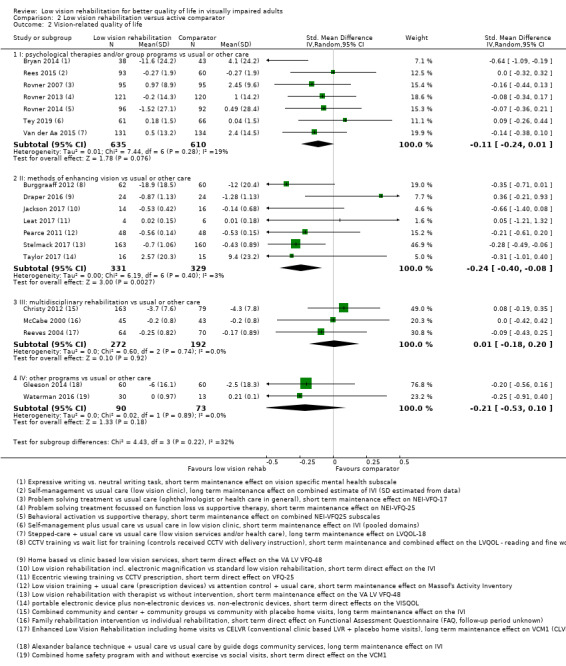
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 2 Vision‐related quality of life.
Seven studies investigated group I psychological therapies and/or group programmes where short‐term maintenance effects were studied by Bryan 2014: expressive writing intervention versus non‐emotional topic writing task; Rovner 2007: PST versus usual care by an ophthalmologist; Rovner 2013: PST versus standardised psychological nondirective treatment; Rovner 2014: behavioural activation versus standardised psychological nondirective treatment; and long‐term maintenance effects by Rees 2015: low vision self‐management group programme; Tey 2019: self‐management programme, and Van der Aa 2015: stepped‐care intervention including cognitive‐behavioural therapy‐based self‐help plus usual care versus usual care consisting of outpatient low vision rehabilitation care). Overall, a small benefit was found (SMD ‐0.11, 95% CI ‐0.24 to 0.01; participants = 1245; studies = 7; I2 = 19%). The certainty of this evidence was low due to risk of bias (‐1) and imprecision (‐1).
Seven studies investigated group II methods for enhancing vision (short‐term maintenance effects by Burggraaff 2012: of a standardised CCTV training programme versus usual instruction by the supplier; Stelmack 2017: additional sessions on eccentric viewing, use of low vision devices, environmental modification plus low vision care versus low vision care only, and Pearce 2011: low vision device training on top of consultation with an optometrist for conventional low vision assessment versus placebo treatment by a nurse; and short‐term direct effects by Draper 2016: home‐based versus clinical‐based rehabilitation; Jackson 2017: provision of CCTV in addition to optical aids versus optical aids only; Leat 2017: CCTV provision and training versus eccentric fixation training; and Taylor 2017: use of portable electronic devices on top of optical devices versus optical devices only). The meta‐analysis of these studies suggested small, but significant benefits (SMD ‐0.24, 95% CI ‐0.40 to ‐0.08; participants = 660; studies = 7; I2 = 3%). The certainty of this evidence was moderate due to risk of bias (‐1), whereas we did not downgrade for imprecision since the confidence interval was consistent with small effects..
Three studies investigated group III multidisciplinary rehabilitation (long‐term maintenance effects by Christy 2012: different methods of multidisciplinary rehabilitation versus centre‐based services with non‐interventional community visits; and Reeves 2004: home visits from a rehabilitation officer in addition to conventional low vision rehabilitation versus conventional low vision rehabilitation only; and short‐term direct effects by McCabe 2000: involvement of families in addition to individual outpatient vision rehabilitation versus individual rehabilitation only). Overall effects were not beneficial (SMD 0.01, 95% CI ‐0.18 to 0.20; participants = 464; studies = 3; I2 = 0%). The certainty of this evidence was low due to risk of bias (‐1) and imprecision (‐1).
Among group IV, other types of interventions, Gleeson 2014 (120 participants) as a long‐term maintenance effect compared the Alexander technique to improve balance in people with vision loss with usual Guide Dog care (charity foundation). Waterman 2016 investigated a short‐term direct effect of a home safety programme with and without exercise versus social visits. In both studies, the benefits found were very imprecisely estimated (very low‐certainty evidence).
Secondary outcomes
Physical aspect of quality of life
Three studies investigated the effect of psychological therapies and/or group programmes, or other interventions on activities of daily living as a 'physical aspect' of QOL (Analysis 2.3) against an active comparator.
2.3. Analysis.
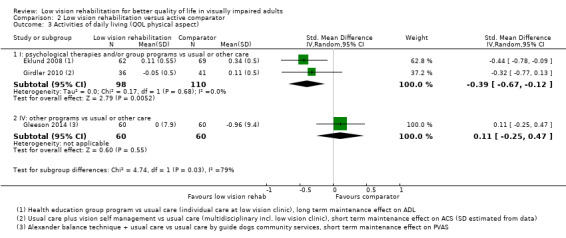
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 3 Activities of daily living (QOL physical aspect).
Two studies used group I psychological therapies and/or group programmes (Eklund 2008; long‐term maintenance effect of a health education programme versus standard low vision programme: Girdler 2010: short‐term maintenance effect of a self‐management intervention plus usual care versus usual care which was individual case management model and multidisciplinary work). An overall significant moderate effect was recorded (SMD ‐0.39, 95% CI ‐0.67 to ‐0.12; participants = 208; studies = 2; I2 = 0%). The certainty of this evidence was low due to risk of bias (‐1) and imprecision (‐1).
Among other types of interventions, Gleeson 2014 (120 participants) investigated a long‐term maintenance effect of the Alexander technique to improve balance in people with vision loss with usual low vision care delivered by Guide Dogs (charity foundation) and found no benefits compared to low vision care.
Psychological aspect of quality of life
Several studies investigated the effect of the intervention groups on depressive symptoms (Analysis 2.4), on self‐efficacy or self‐esteem (Analysis 2.5) and on adaptation to vision loss (Analysis 2.6) as a 'psychological aspect' of QOL and against an active comparator.
2.4. Analysis.
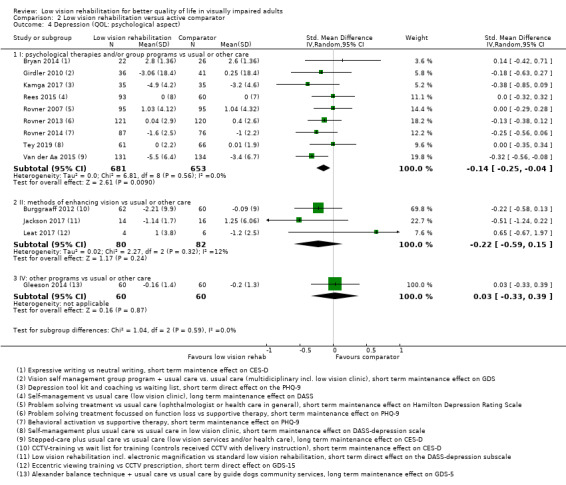
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 4 Depression (QOL: psychological aspect).
2.5. Analysis.
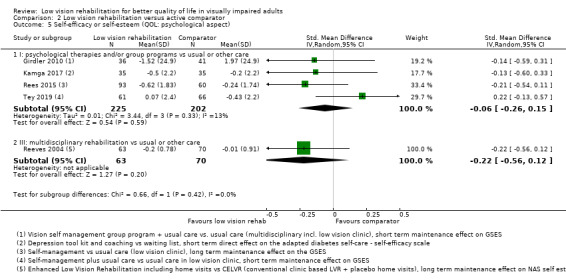
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 5 Self‐efficacy or self‐esteem (QOL: psychological aspect).
2.6. Analysis.
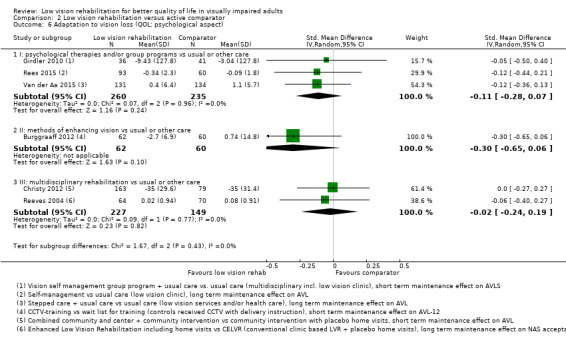
Comparison 2 Low vision rehabilitation versus active comparator, Outcome 6 Adaptation to vision loss (QOL: psychological aspect).
Depression
Nine studies investigated group I psychological therapies and/or group programmes on the effects on depression (short‐term maintenance effects by Bryan 2014: expressive writing intervention versus non‐emotional topic writing task; Kamga 2017: short‐term direct effect of a cognitive behavioural therapy‐based self‐care tool versus usual care; Girdler 2010 and Tey 2019: self‐management programmes plus usual care versus usual care; Rovner 2007: PST versus usual care by an ophthalmologist; Rovner 2013: PST versus standardised psychological nondirective treatment; Rovner 2014: behavioural activation versus standardised psychological nondirective treatment; and long‐term maintenance effects of Rees 2015: low vision self‐management group programme; and Van der Aa 2015: stepped‐care plus usual care compared to usual care). Overall results were suggestive of small benefits that were imprecisely estimated (SMD ‐0.14, 95% CI ‐0.25 to ‐0.04; participants = 1334; studies = 9; I2 = 0%). The certainty of this evidence was moderate due to risk of bias (‐1).
There were two studies in the group II methods for enhancing vision (short‐term maintenance effect by Burggraaff 2012: standardised CCTV training programme versus usual instruction by the supplier and a short‐term direct effect by Jackson 2017: provision of CCTV in addition to optical aids versus optical aids only). Results suggested some benefits but were imprecisely estimated. (SMD ‐0.22, 95% CI ‐0.59 to 0.15; participants = 162; studies = 3; I2 = 12%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
In group IV, other programmes, Gleeson 2014 (120 participants) compared the Alexander technique to improve balance in people with vision loss with usual Guide Dog care (charity foundation) and found no difference (very low‐certainty evidence).
Self‐efficacy or self‐esteem
Four studies investigated group I psychological therapies and/or group programmes on the effects on self‐efficacy or self‐esteem (Analysis 2.5): Girdler 2010 and Tey 2019: short‐term maintenance effects of self‐management interventions plus usual care versus usual care; Kamga 2017: short‐term direct effect of a cognitive behavioural therapy‐based self‐care tool versus usual care; Rees 2015: long‐term maintenance effects of a low vision self‐management group programme versus multidisciplinary team). Results suggested a small and imprecisely estimated benefit and included no benefit (SMD ‐0.06, 95% CI ‐0.26 to 0.15; participants = 427; studies = 4; I2 = 13%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
In the group III, multidisciplinary programmes, Reeves 2004 compared home visits from a rehabilitation officer in addition to conventional low vision rehabilitation versus conventional low vision rehabilitation as a long‐term maintenance effect and found no benefit (very low‐certainty evidence).
Adaptation to visual loss
Six studies investigated the effect of several interventions on adaptation to visual loss (Analysis 2.6) against an active comparator.
Three studies investigated group I psychological therapies and/or group programmes (Girdler 2010: short‐term maintenance effect of a self‐management intervention plus usual care versus usual care which was an individual case management model and multidisciplinary work; and long‐term maintenance effects by Rees 2015: low vision self‐management group programme versus multidisciplinary team; and Van der Aa 2015: stepped‐care plus usual care compared to usual care). The meta‐analysis suggested a small or no benefit on this dimension (SMD ‐0.11, 95% CI ‐0.28 to 0.07; participants = 495; studies = 3; I2 = 0%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
One study in group II, methods for enhancing vision group, which investigated short‐term maintenance effects (Burggraaff 2012: standardised CCTV training programme versus usual instruction by the supplier) found no benefit (very low‐certainty evidence).
Two studies in group III, multidisciplinary rehabilitation, both investigated long‐term maintenance effects (Christy 2012: different methods of multidisciplinary rehabilitation versus centre‐based services with non‐interventional community visits; Rees 2015: low vision self‐management group programme versus multidisciplinary team) and found no additional benefit (SMD ‐0.02, 95% CI ‐0.24 to 0.19; participants = 376; studies = 2; I2 = 0%). The certainty of this evidence was very low due to risk of bias (‐1) and imprecision (‐2).
Social aspect of quality of life
Although the studies by Brunnström 2004, Bryan 2014, and Gleeson 2014 used some measure to investigate effects of an intervention versus an active comparator on a social aspect of QOL, these were not feasible for entering in a meta‐analysis.
Adverse events and serious adverse events
Only a few studies reported data on adverse events (AEs) or serious adverse events (SAEs). Nollet 2016 reported two AEs of which one was related to pharmacological treatment of depression rather than to rehabilitation and 10 SAEs which were unrelated to study interventions. Acton 2016 reported 19 AEs that were probably unrelated to treatment, mainly worsening of depression. Stelmack 2017 reported 10 AEs that were not treatment‐related. Stelmack 2008, Kamga 2017, Waterman 2016, Burggraaff 2012 and Van der Aa 2015 reported no (S)AEs that were treatment‐related. For all other studies, no data were available.
Discussion
Summary of main results
In this review, we have taken a broad perspective to map and summarise the evidence from RCTs in which several types of rehabilitation interventions were evaluated and which aimed to improve QOL of adults with low vision. We adopted both HRQOL and VRQOL as primary outcomes, because general and disease‐specific measures are both used across medical specialities in order for policy makers to make informed decisions about resources.
The interpretation of the results of this review are complicated by the fact that low vision rehabilitation is not a standard process, as interventions are highly individually tailored and can vary in different settings, where a mixture of different optometric or therapeutic components are used. For this reason, we grouped the study interventions in four broad categories. Unlike several other Cochrane Reviews, which present results by comparison, in the main text we have presented effects on an outcome basis, which allows us to explore the consistency of the effects of several types of low vision rehabilitation intervention on each QOL, VRQOL or related outcome. In order to offer a different perspective, the following summary will be comparison‐based, that is, the effects for all outcomes will be described for each comparison.
Psychological therapies and/or group programmes compared to no care showed an effect towards improvement of VRQOL, but this estimate was not sufficiently precise to exclude small benefit and the evidence was of very low‐certainty. No effect was found in a single, small study on VRQOL. Instead, a large effect was found on depression and self‐efficacy or self‐esteem but these were imprecisely estimated, although significant, and the certainty of the evidence was very low. Psychological therapies and/or group programmes compared to usual care or active control showed a small benefit on HRQOL and VRQOL with imprecise estimates that may have included no benefit, with low‐certainty evidence. A small effect of moderate‐certainty was found on depression and low‐certainty evidence of some benefit was also found on activities of daily living. Effects on self‐efficacy or self‐esteem were still positive but very uncertain and with low‐certainty of evidence.
Methods for enhancing vision compared to no care showed moderate‐certainty evidence of small effects for VRQOL and very low‐certainty evidence of effects directed towards benefit for HRQOL and depression but estimates were imprecise. Methods for enhancing vision compared to usual or other care also showed effects towards benefit for HRQOL, VRQOL and depression, but estimates were very imprecise with low‐ or very low‐certainty of evidence.
Multidisciplinary rehabilitation compared to no care showed no effect on HRQOL, and two heterogeneous studies showed a large effect on VRQOL, where the larger trial at low risk of bias was using intensive treatment; the small trial showed a small effect on VRQOL. Imprecise estimates of benefit were detected for adaptation to vision loss and no effect on activities of daily living. All evidence was of low‐ or very low‐certainty. Multidisciplinary rehabilitation compared to usual or other care showed imprecisely estimated effects in the direction of benefit for HRQOL and no benefit for VRQOL, for self‐efficacy or self‐esteem and adaptation to vision loss. All evidence was of low‐ or very low‐certainty.
Three heterogeneous studies evaluated other programmes and readers should refer to each study for this evidence.
The summary made above has no direct interpretation due to the heterogeneity in the interventions, even within subgroups, but it suggests that small effects of several types of low vision rehabilitation may exist for different QOL and related outcomes, especially VRQOL and depression.
The effect size of low vision rehabilitation was small (below 0.5 standard deviation (SD) units and probably around 0.20 SD units) for most intervention types and outcome intersection, except for the effect of psychological therapies on depression. However, larger effects are seldom achieved using QOL tools as outcome measurement instruments, including when effective treatments are assessed. As an example, in participants with diabetic macular oedema, Bressler 2014 found a 2‐year difference in best‐corrected visual acuity (BCVA) increase by 9.7 (SD: 14.5) Early Treatment Diabetic Retinopathy Study (ETDRS) letters for monthly ranibizumab 0.5 mg compared to sham, which is an effect size of 0.67, while the increase in QOL (NEI‐VFQ 25 composite score) was 5.4 (SD: 13.5), corresponding to an effect size of 0.4, meaning that even an intensive and long‐term active pharmacological treatment that improves vision in one eye had a small or moderate impact on QOL, a figure that changed little whether the treatment was applied to the better or the worse eye. We think that small or moderate effects of low vision rehabilitation on VRQOL could be valuable and should be evaluated in further studies including their cost‐effectiveness. Moreover, the intensity of the intervention matters, since effects were recorded for several low vision rehabilitation interventions compared to both no care and usual or other active care. This may have been the reason why the largest benefit for multidisciplinary rehabilitation programmes (versus no care) was recorded in Stelmack 2008, the LOVIT study conducted in the USA, which used an intensive rehabilitation scheme.
Overall completeness and applicability of evidence
Our review offers a broad picture of evidence of RCTs on several types of low vision rehabilitation to improve QOL and related outcomes. Apart from the obvious challenge in discussing the applicability of this heterogeneous evidence in different settings, it must be noted that only a few studies investigated long‐term maintenance effects on QOL or related outcomes, so we do not know whether any benefit persists. Studies were generally focused on short‐term maintenance (within six months) or direct effects of interventions (within one month of intervention completion). Adverse events, or the lack of, were rarely reported in studies. In the few studies reporting on adverse events, these seemed to be related to associated treatments, e.g. antidepressants, rather than directly to the interventions studied. In addition, some interventions were not standard 'low vision rehabilitation' such as prism glasses in AMD (Smith 2005), or tango dance lessons (Pinninger 2013). All studies were conducted in North America; Europe or Australia and only four in Asia, but none in South America or Africa.
With respect to the larger effects of psychological therapies, or group programmes, or both, we only synthesised data on depressive symptomatology, self‐efficacy and self‐esteem and adaptation to vision loss for its close relatedness to the psychological aspect of QOL. The effect of preventive interventions on the incidence of depression and/or anxiety disorders in visually impaired (older) adults was disregarded, as these reflect serious medical conditions. Still, we believe that, since depression and anxiety are a problem in increasing numbers of older visually impaired adults, these preventive interventions may be considered another important development within low vision rehabilitation settings. Examples are interventions specifically developed to prevent depression and anxiety disorders or reduce symptoms (e.g. Nollet 2016; Rees 2015; Rovner 2014 and Van der Aa 2015).
Although most studies in the current review focused on psychological therapies and/or group interventions and showed a positive effect, this does not imply that these therapies are better than methods of enhancing vision or multidisciplinary care to improve QOL. It is possible, though, that methods to enhance vision target VRQOL more directly than psychological interventions which might target the psychological outcomes better, such as depression or self‐esteem.
Nonetheless, there was some evidence of potential benefit on several outcomes for both these interventions. Future evidence may clear up this issue thus research is needed to confirm that methods to enhance (residual) vision should be made accessible to all, taking into account both effectiveness and cost. Apart from that, multidisciplinary approaches, which might include psychological therapies or group programmes, or both, may further enhance QOL and related outcomes as was shown in several studies, even when having usual care as a comparator, which sometimes included rehabilitation services. In addition, it could be observed in the current review that some low vision rehabilitation interventions aim to stimulate patient empowerment leading to increased self‐esteem in our vulnerable group of patients. This is encouraging and following important developments in healthcare (Samoocha 2010) should receive more attention in rehabilitation settings or future studies as well. More high‐quality studies are needed to prove the effect of low vision rehabilitation interventions in improving activities of daily living (e.g. occupational therapy) and to enhance adaptation to vision loss. Adaptation to vision loss may be a long process, however, it may be influenced by group interventions, peer support or psychological interventions aiming to increase insight into the acceptance of living with a disability. Whether these types of interventions are accessible to patients is unclear. Lessons learned from other fields in healthcare could be used as an inspiration to develop new treatments focusing on adaptation to visual disability.
Referring patients to low vision rehabilitation requires customisation of the various available interventions which should be tailored to the individual patient’s wishes and needs. Gaining the medical and functional history of a patient or assessing the patient's needs from his/her own perspective, for example, using the Activity Inventory (Massof 2005) are promising developments to efficiently refer patients to the right intervention. In turn, more prospective studies are needed to predict which patients benefit most from a specific service. The complexity and diversity of patients' needs may indicate a need to adapt any rehabilitation programme to individual patient profiles. Research should be conducted on prognostic factors to develop those patient profiles for specific rehabilitation programmes. Also, there is little evidence yet on dose‐response relations between the intensity of treatment needed and the outcomes studied. Of interest, a landmark study conducted by US Veterans, the LOVIT study (Stelmack 2008), adopted an intensive rehabilitation programme and yielded a very large benefit on VRQOL. If feasible, RCTs addressing differences between intensive versus less intensive models should be set up. In addition, there are only a few studies that report on cost‐effectiveness and/or cost‐utility of low vision rehabilitation interventions (e.g. Stroupe 2008; Eklund 2008, Van der Aa 2015 and Stelmack 2017). A limitation of our findings is that included studies were mainly conducted on participants with AMD living in high‐income countries. Studies are needed in middle and low‐income countries if low vision services are available. Other ‘forgotten’ subgroups which should be separately addressed are young and working‐age adults. Only one and unfortunately rather low‐quality RCT was found addressing work‐related issues in living with vision loss. As the prevalence of visual impairment in working age adults and children is low, we encourage collaboration with other (inter)national research groups for organising properly powered trials providing more and stronger evidence for the effect of rehabilitation programmes. Apart from QOL in younger adults, these outcomes should focus on return to work. Other subgroups should receive more attention as well in the implementation and studies into effective interventions, e.g. people with multiple disabilities, such as intellectual disabilities or concurrent hearing disabilities. The latter have been studied in two Dutch RCTs by Vreeken 2013 and Roets‐Merken 2015 which studied the effect of dual‐sensory loss interventions in older adults. Finally, in clinical practice, training in the use of modern devices such as specific ‘visually impaired user‐friendly’ computer software, tablets and smartphones are increasingly offered. These interventions may have the potential to increase participation in society but trials are needed to evaluate their effectiveness and cost‐effectiveness.
User groups need to be empowered to be more vocal and create the demand for more and better research and the funding for it. with the aim of designing and conducting high‐quality RCTs in rehabilitation programmes that are up to date with respect to patients' needs.
Quality of the evidence
The certainty of the evidence that aimed to assess the effectiveness of low vision rehabilitation interventions on QOL or related outcomes was generally low or very low. Only the certainty of the effect of psychological therapies and/or group programmes versus usual care on depression was moderate.
Reasons for downgrading assessments using GRADE were mostly because of imprecision due to few participants in the comparisons with wide confidence intervals, often suggesting a benefit but including no effect. Moreover, many studies were at unclear risk of bias for allocation concealment and masking. Because rehabilitation is generally impossible to mask, one could argue whether downgrading the certainty of the evidence for this item is fair in this field. We also suggest that research should be conducted to disentangle true benefit from socially desirable responses. Therefore, in view of the subjectivity of QOL outcomes which might be prone to response bias, we encourage researchers to use at least masked outcome assessors and also to develop outcome measures which can be assessed without knowing the intervention status of the participant. Some of the more recent studies which can be found in this review should be used as examples in the field to improve the methodological quality of obtaining evidence of low vision rehabilitation interventions.
Potential biases in the review process
Although all relevant literature databases were searched which led to over 11,000 hits and additional searches were performed on reference lists of relevant studies, conference proceedings and journals, we cannot be certain that we included all available studies. Compared with the review of Binns 2012, the seven trials that were found in that study were also identified in our literature search. In contrast to Binns 2012, nonrandomised trials (NRCT) or observational studies were excluded in this review, however, some of the RCTs included in this study had considerable risk of bias. In a future version of this review, it may be worth including non‐randomised studies with a robust assessment of risk of bias to get a more complete picture of all the relevant evidence.
A potential limitation of the methodology in this review is represented by the use of the SMD, which is the most common pooling method used when instruments use different scales. Various alternatives are available to interpret a meta‐analysis using the SMD (Higgins 2017). We decided to adopt a simple rule of thumb to interpret the magnitude of the effect sizes: 0.2 represents a small effect, 0.5 a moderate effect, and 0.8 a large effect. Using the data extracted for Brody 2002 as an example, this study found a total score difference of ‐0.95 (95%CI: ‐2.84, 0.94) between the self‐management programme and a waiting list using the NEI‐VFQ questionnaire, for which a clinically significant important difference is commonly believed to be five points. The corresponding SMD we found was ‐0.13 (‐0.40, 0.14), which is consistent with the interpretation of the raw NEI‐VFQ estimates of no difference both for the point estimate and its uncertainty.
Agreements and disagreements with other studies or reviews
Binns 2012 concluded from their comprehensive review, in which they included seven RCTs and over fifty observational studies, that rehabilitation services resulted in improved clinical and functional ability outcomes, but that the effects on mood, VRQOL and HRQOL were less clear. We found it difficult to compare our results to those of Binns 2012 due to different inclusion criteria. Binns 2012 was a broad purpose review and we referred to it for a thorough assessment of methodological issues in current low vision research, including a discussion of choice of QOL tools, and other issues regarding study design.
Authors' conclusions
Implications for practice.
In this Cochrane Review, no evidence was found of benefit of diverse types of low vision rehabilitation interventions on HRQOL. We found low‐ and moderate‐certainty evidence of a small benefit on VRQOL in studies comparing psychological therapies or methods for enhancing vision with usual or other care, respectively. Multidisciplinary rehabilitation was found to add little to standard care, but this finding is difficult to interpret due to the variability of the interventions and considering the large benefit for VRQOL recorded in Stelmack 2008, which delivered intensive rehabilitation compared to no care, suggesting a dose‐response may exist. Evidence of moderate‐certainty from several small studies was consistent for psychological therapies to treat depression and to improve self‐efficacy or self‐esteem, which was a secondary outcome in this review.
The type of rehabilitation varied among studies, even within intervention groups, and their intensity probably influenced effects, since benefits were detected compared to usual care or active control.
Implications for research.
Despite these limitations, the consistent direction of the effects in this review towards benefit justifies the conduction of further research of better methodological quality and longer follow‐up on several types of low vision rehabilitation using QOL outcomes, especially VRQOL. Although there are quite a few high‐quality studies with upcoming results, future studies are needed to obtain more evidence in the field of low vision, especially on which type of rehabilitation is more effective for which patients, as well as studies in low‐ and middle‐income countries.
Evidence from this Cochrane Review supports the use of VRQOL tools to compare different types of low vision rehabilitation interventions. More and better research is also needed on the effect of different types of psychological therapies on mental health in people with low vision. Finally, new standards in our ageing society require not only a focus on patient‐reported outcomes, but also on cost‐effectiveness of single or multidisciplinary low vision interventions from a societal perspective.
Acknowledgements
We would like to thank all the study authors who responded to requests for additional information. We are grateful to the Information Specialist, Iris Gordon (IG) for updating the search strategies and running them. We would also like to thank Jennifer Evans and Anupa Shah for their active involvement in finishing the review, but also John Lawrenson, Gianfrancesco Villani, Catey Bunce and Tianjing Li for their peer review comments on the analyses, manuscript and protocol and/or for their earlier peer reviews. Financial support was provided in part by the A.F. Deutman Ophthalmic Research Foundation, Nijmegen, the Netherlands.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor Vision Disorders #2 MeSH descriptor Visually Impaired Persons #3 (low* or handicap* or subnormal* or impair* or partial* or disab*) near/3 (vision or visual* or sight*) #4 (#1 OR #2 OR #3) #5 MeSH descriptor Rehabilitation #6 (rehabilitat* or assess*) near/4 (low vision) #7 MeSH descriptor Activities of Daily Living #8 MeSH descriptor Risk Assessment #9 MeSH descriptor Risk Factors #10 MeSH descriptor Risk Management #11 MeSH descriptor Safety Management #12 (home near/3 safet*) #13 (hazard*) near/3 (home or environment*) #14 MeSH descriptor Home Care Services #15 MeSH descriptor Occupational Therapy #16 MeSH descriptor Exercise Therapy #17 MeSH descriptor Physical Therapy Modalities #18 behavio* near/3 modif* #19 (program*) near/3 (home or exercise* or modif*) #20 MeSH descriptor Cognitive Therapy #21 MeSH descriptor Behavior Therapy #22 (#5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21) #23 (#4 AND #22)
Appendix 2. MEDLINE Ovid search strategy
1. randomized controlled trial.pt. 2. (randomized or randomised).ab,ti. 3. placebo.ab,ti. 4. dt.fs. 5. randomly.ab,ti. 6. trial.ab,ti. 7. groups.ab,ti. 8. or/1‐7 9. exp animals/ 10. exp humans/ 11. 9 not (9 and 10) 12. 8 not 11 13. exp low vision/ 14. exp vision disorders/ 15. exp visually impaired persons/ 16. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$ or disorder$ or loss$ or limit$) adj3 (vision or visual$ or sight$)).tw. 17. or/13‐16 18. rehabilitation/ 19. rehabilitation centres/ 20. (rehabilitat$ adj3 (navigat$ or mobility or travel$ or walk$ or moving or movement or driv$ or teach$ or train$)).tw. 21. patient care team/ 22. self care/ 23. self management.tw. 24. (wait adj1 list).tw. 25. health promotion/ 26. (health$ adj4 (promot$ or programme$ or educat$)).tw. 27. (intervention adj4 (standard or usual or programme$ or target$ or period$)).tw. 28. activities of daily living/ 29. adl.tw. 30. occupational therapy/ 31. occupational therap$.tw. 32. exercise therapy/ 33. physical therapy modalities/ 34. (programme$ adj3 (home or exercise$ or modif$)).tw. 35. Cognitive Therapy/ 36. Behavior Therapy/ 37. (cognitive behavio$ therapy or CBT).tw. 38. (cognitive adj3 (intervention$ or skill$ or train$ or session$)).tw. 39. (behavioural adj3 (intervention$ or skill$ or train$ or session$)).tw. 40. Psychotherapy, Group/ 41. psychotherap$.tw. 42. (psychoeducat$ or patient education).tw. 43. ((intervention$ or therap$ or treat$) adj2 psychological).tw. 44. ((intervention$ or therap$ or treat$) adj2 psychosocial).tw. 45. counseling/ 46. (counseling or counselling).tw. 47. Problem Solving/ 48. problem solving.tw. 49. stress management.tw. 50. coping skills.tw. 51. optometry/ 52. exp sensory aids/ 53. (closed adj3 circuit$).tw. 54. (cctv$ or video$ or computer$ or scanner$).tw. 55. (telescop$ or magnif$ or aid$ or device$).tw. 56. (reading adj3 aid$).tw. 57. ((aid$ or device) adj1 low vision).tw. 58. LVA.tw. 59. Canes/ 60. (cane$ adj3 (long or support)).tw. 61. (orientat$ or mobili$).tw. 62. (way adj3 find$).tw. 63. or/18‐62 64. 17 and 63 65. 12 and 64
The search filter for trials at the beginning of the MEDLINE strategy is from the published paper by Glanville 2006.
Appendix 3. Embase Ovid search strategy
1. exp randomized controlled trial/ 2. exp randomization/ 3. exp double blind procedure/ 4. exp single blind procedure/ 5. random$.tw. 6. or/1‐5 7. (animal or animal experiment).sh. 8. human.sh. 9. 7 and 8 10. 7 not 9 11. 6 not 10 12. exp clinical trial/ 13. (clin$ adj3 trial$).tw. 14. ((singl$ or doubl$ or trebl$ or tripl$) adj3 (blind$ or mask$)).tw. 15. exp placebo/ 16. placebo$.tw. 17. random$.tw. 18. exp experimental design/ 19. exp crossover procedure/ 20. exp control group/ 21. exp latin square design/ 22. or/12‐21 23. 22 not 10 24. 23 not 11 25. exp comparative study/ 26. exp evaluation/ 27. exp prospective study/ 28. (control$ or prospectiv$ or volunteer$).tw. 29. or/25‐28 30. 29 not 10 31. 30 not (11 or 23) 32. 11 or 24 or 31 33. visual disorder/ 34. exp low vision/ 35. exp visual impairment/ 36. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$ or disorder$ or loss$ or limit$) adj3 (vision or visual$ or sight$)).tw. 37. or/33‐36 38. rehabilitation/ 39. rehabilitation centers/ 40. (rehabilitat$ adj3 (navigat$ or mobility or travel$ or walk$ or moving or movement or driv$ or teach$ or train$)).tw. 41. patient care/ 42. self care/ 43. self management.tw. 44. (wait adj1 list).tw. 45. health promotion/ 46. (health$ adj4 (promot$ or program$ or educat$)).tw. 47. (intervention adj4 (standard or usual or program$ or target$ or period$)).tw. 48. exp daily life activity/ 49. adl.tw. 50. occupational therapy/ 51. occupational therap$.tw. 52. exercise/ 53. (program$ adj3 (home or exercise$ or modif$)).tw. 54. cognitive Therapy/ 55. behavior Therapy/ 56. (cognitive behavio$ therapy or CBT).tw. 57. (cognitive adj3 (intervention$ or skill$ or train$ or session$)).tw. 58. (behavioural adj3 (intervention$ or skill$ or train$ or session$)).tw. 59. psychotherapy/ 60. psychotherap$.tw. 61. (psychoeducat$ or patient education).tw. 62. ((intervention$ or therap$ or treat$) adj2 psychological).tw. 63. ((intervention$ or therap$ or treat$) adj2 psychosocial).tw. 64. counseling/ 65. (counseling or counselling).tw. 66. Problem Solving/ 67. problem solving.tw. 68. stress management.tw. 69. coping skills.tw. 70. optometry/ 71. exp sensory aids/ 72. (closed adj3 circuit$).tw. 73. (cctv$ or video$ or computer$ or scanner$).tw. 74. (telescop$ or magnif$ or aid$ or device$).tw. 75. (reading adj3 aid$).tw. 76. ((aid$ or device) adj1 low vision).tw. 77. LVA.tw. 78. cane/ 79. (cane$ adj3 (long or support)).tw. 80. (orientat$ or mobili$).tw. 81. (way adj3 find$).tw. 82. or/38‐81 83. 37 and 82 84. 32 and 83
Appendix 4. CINAHL EBSCO search strategy
S42 S40 and S41 S41 (MH "Aged+") OR (MH "Aged, 80 and Over") OR (MH "Frail Elderly") S40 S12 and S39 S39 S20 and S38 S38 S21 or S22 or S23 or S24 or S25 or S26 or S27 or S28 or S29 or S30 or S31 or S32 or S33 or S34 or S35 or S36 or S37 S37 (MH "Behavior Therapy+") OR (MH "Behavior Therapy (Iowa NIC) (Non‐Cinahl)") S36 (MH "Cognitive Therapy") OR (MH "Cognitive Therapy (Iowa NIC) (Non‐Cinahl)") S35 TX ((program* n3 home) or (program* n3 exercise) or (program* n3 modif*)) S34 TX behavio* n3 modif* S33 (MH "Physical Therapy") S32 (MH "Exercise Therapy: Ambulation (Iowa NIC)") OR (MH "Exercise Therapy: Balance (Iowa NIC)") S31 (MH "Occupational Therapy+") S30 (MH "Home Health Care") S29 TX ((hazard* n3 home) or (hazard* n3 environment*)) S28 TX home n3 safety* S27 (MH "Risk Management") OR (MH "Risk Management (Iowa NIC) (Non‐Cinahl)") S26 (MH "Risk Factors") S25 (MH "Risk Assessment") OR (MH "Fall Risk Assessment Tool") S24 (MH "Activities of Daily Living+") OR (MH "Activities of Daily Living (Saba CCC)") OR (MH "Activities of Daily Living Alteration (Saba CCC)") OR (MH "Instrumental Activities of Daily Living (Saba CCC)") OR (MH "Instrumental Activities of Daily Living Alteration (Saba CCC)") OR (MH "Altered Activities of Daily Living (NANDA) (Non‐Cinahl)") OR (MH "Self Care: Activities of Daily Living (Iowa NOC)") OR (MH "Self‐Care: Instrumental Activities of Daily Living (Iowa NOC)") S23 TX assess* n4 vision* S22 TX rehabilitat* n4 vision* S21 (MH "Rehabilitation of Vision Impaired+") S20 S13 or S14 or S15 or S16 or S17 or S18 or S19 S19 TX ((disab* n3 vision) or (disab* n3 visual*) or (disab* n3 sight)) S18 TX ((partial* n3 vision) or (partial* n3 visual*) or (partial* n3 sight)) S17 TX ((impair* n3 vision) or (impair* n3 visual*) or (impair* n3 sight)) S16 TX ((subnormal* n3 vision) or (subnormal* n3 visual*) or (subnormal* n3 sight)) S15 TX ((handicap* n3 vision) or (handicap* n3 visual*) or (handicap* n3 sight)) S14 TX ((low* n3 vision) or (low* n3 visual*) or (low* n3 sight)) S13 (MH "Vision Disorders+") S12 S1 or S2 or S3 or S4 or S5 or S6 or S7 or S8 or S9 or S10 or S11 S11 TX allocat* random* S10 (MM "Quantitative Studies") S9 (MM "Placebos") S8 TX placebo* S7 TX random* allocat* S6 (MM "Random Assignment") S5 TX randomi* control* trial* S4 TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) S3 TX clinic* n1 trial* S2 PT Clinical trial S1 (MH "Clinical Trials+")
Appendix 5. PsychINFO Ovid search strategy
1. Clinical Trials/ 2. Treatment Effectiveness Evaluation/ 3. random$.tw. 4. ((clin$ or control$ or compar$ or evaluat$ or prospectiv$) adj25 (trial$ or studi$ or study)).tw. 5. ((singl$ or doubl$ or trebl$ or tripl$) adj6 (blind$ or mask$)).tw. 6. (cross‐over or crossover).tw. 7. (assign$ or allocat$).tw. 8. or/1‐7 9. exp Vision/ 10. exp Vision Disorders/ 11. exp Eye Disorders/ 12. exp Blind/ 13. exp Partially Sighted/ 14. ((low$ or handicap$ or subnormal$ or impair$ or partial$ or disab$ or disorder$ or loss$ or limit$) adj3 (vision or visual$ or sight$)).tw. 15. or/10‐14 16. exp Rehabilitation/ 17. exp Rehabilitation Centers/ 18. (rehabilitat$ adj3 (navigat$ or mobility or travel$ or walk$ or moving or movement or driv$ or teach$ or train$)).tw. 19. exp Self Care Skills/ 20. self management.tw. 21. (wait adj1 list).tw. 22. exp Health Promotion/ 23. (health$ adj4 (promot$ or program$ or educat$)).tw. 24. (intervention adj4 (standard or usual or program$ or target$ or period$)).tw. 25. activities of daily living/ 26. adl.tw. 27. exp Occupational Therapy/ 28. occupational therap$.tw. 29. exp Exercise/ 30. exp Physical Activity/ 31. (program$ adj3 (home or exercise$ or modif$)).tw. 32. Cognitive Techniques/ 33. Cognitive Therapy/ 34. Behavior Therapy/ 35. (cognitive behavio$ therapy or CBT).tw. 36. (cognitive adj3 (intervention$ or skill$ or train$ or session$)).tw. 37. (behavioural adj3 (intervention$ or skill$ or train$ or session$)).tw. 38. Group Psychotherapy/ 39. psychotherap$.tw. 40. (psychoeducat$ or patient education).tw. 41. ((intervention$ or therap$ or treat$) adj2 psychological).tw. 42. ((intervention$ or therap$ or treat$) adj2 psychosocial).tw. 43. exp Counseling/ 44. exp Psychotherapeutic Counseling/ 45. (counseling or counselling).tw. 46. Relaxation Therapy/ 47. ((group or therap$ or treat$) adj2 relaxation).tw. 48. Problem Solving/ 49. problem solving.tw. 50. Stress Management/ 51. stress management.tw. 52. self management.tw. 53. exp Coping Behavior/ 54. coping skills.tw. 55. exp Optometry/ 56. exp Optical Aids/ 57. (closed adj3 circuit$).tw. 58. (cctv$ or video$ or computer$ or scanner$).tw. 59. (telescop$ or magnif$ or aid$ or device$).tw. 60. (reading adj3 aid$).tw. 61. ((aid$ or device) adj1 low vision).tw. 62. LVA.tw. 63. (cane$ adj3 (long or support)).tw. 64. (orientat$ or mobili$).tw. 65. (way adj3 find$).tw. 66. or/16‐65 67. 15 and 66 68. 8 and 67 69. limit 68 to human 70. visual analog$.tw. 71. 69 not 70 72. (paediatric$ or pediatric$).tw. 73. (newborn or neonate or infan$ or baby or babies or toddler$ or boy$ or girl$).tw. 74. (nurser$ or kindergarten$ or preschool$ or (pre adj1 school$)).tw. 75. (schoolchild$ or schoolage$ or (school adj1 age$)).tw. 76. ((primary or elementary or secondary or high) adj2 school$).tw. 77. (juvenil$ or underage$ or teen or teens or teenage$ or adolescen$ or youth or youths).tw. 78. or/72‐77 79. 71 not 78
Appendix 6. ISRCTN search strategy
(Visual Impairment OR Low Vision) AND Rehabilitation
Appendix 7. ClinicalTrials.gov search strategy
(Visual Impairment OR Low Vision) AND Rehabilitation
Appendix 8. WHO ICTRP search strategy
Visual Impairment AND Rehabilitation OR Low Vision AND Rehabilitation
Data and analyses
Comparison 1. Low vision rehabilitation versus waiting list or no care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Health‐related quality of life | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 I: psychological therapies and/or group programs vs waiting list or no care | 1 | 54 | Std. Mean Difference (IV, Random, 95% CI) | 0.26 [‐0.28, 0.80] |
| 1.2 III: multidisciplinary rehabilitation vs waiting list or no care | 2 | 183 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.08 [‐0.37, 0.21] |
| 2 Vision‐related quality of life | 9 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 I: psychological therapies and/or group programs vs waiting list or no care | 2 | 285 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.53, 0.08] |
| 2.2 II: methods of enhancing vision vs waiting list or no care | 5 | 262 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.54, 0.15] |
| 2.3 III: multidisciplinary rehabilitation vs waiting list or no care | 2 | 193 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.04 [‐2.24, 0.17] |
| 3 Activities of daily living (QOL physical aspect) | 2 | Std. Mean Difference (IV, Random, 95% CI) | Totals not selected | |
| 3.1 II: methods of enhancing vision vs waiting list or no care | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 III: multidisciplinary rehabilitation vs waiting list or no care | 1 | Std. Mean Difference (IV, Random, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Depression (QOL: psychological aspect) | 9 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 I: psychological therapies and/or group programs vs waiting list or no care | 5 | 456 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.23 [‐2.18, ‐0.28] |
| 4.2 II: methods of enhancing vision vs waiting list or no care | 2 | 44 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.86 [‐1.50, ‐0.23] |
| 4.3 III: multidisciplinary rehabilitation vs waiting list or no care | 2 | 193 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.44, 0.13] |
| 5 Self‐efficacy or self‐esteem (QOL: psychological aspect) | 5 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 I: psychological therapies and/or group programs vs waiting list or no care | 5 | 550 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.85 [‐1.48, ‐0.22] |
| 6 Adaptation to vision loss (QOL: psychological aspect) | 2 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 III: multidisciplinary rehabilitation vs waiting list or no care | 2 | 97 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.54, 0.26] |
Comparison 2. Low vision rehabilitation versus active comparator.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Health‐related quality of life | 9 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 I: psychological therapies and/or group programs vs usual or other care | 4 | 600 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.39, 0.20] |
| 1.2 II: methods of enhancing vision vs usual or other care | 2 | 443 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.28, 0.09] |
| 1.3 III: multidisciplinary rehabilitation vs usual or other care | 2 | 375 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.10 [‐0.31, 0.12] |
| 1.4 IV: other programs vs usual or other care | 1 | 43 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.05 [‐0.70, 0.60] |
| 2 Vision‐related quality of life | 19 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 I: psychological therapies and/or group programs vs usual or other care | 7 | 1245 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.11 [‐0.24, 0.01] |
| 2.2 II: methods of enhancing vision vs usual or other care | 7 | 660 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.24 [‐0.40, ‐0.08] |
| 2.3 III: multidisciplinary rehabilitation vs usual or other care | 3 | 464 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.18, 0.20] |
| 2.4 IV: other programs vs usual or other care | 2 | 163 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.21 [‐0.53, 0.10] |
| 3 Activities of daily living (QOL physical aspect) | 3 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 3.1 I: psychological therapies and/or group programs vs usual or other care | 2 | 208 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.39 [‐0.67, ‐0.12] |
| 3.2 IV: other programs vs usual or other care | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | 0.11 [‐0.25, 0.47] |
| 4 Depression (QOL: psychological aspect) | 13 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 I: psychological therapies and/or group programs vs usual or other care | 9 | 1334 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.25, ‐0.04] |
| 4.2 II: methods of enhancing vision vs usual or other care | 3 | 162 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐0.59, 0.15] |
| 4.3 IV: other programs vs usual or other care | 1 | 120 | Std. Mean Difference (IV, Random, 95% CI) | 0.03 [‐0.33, 0.39] |
| 5 Self‐efficacy or self‐esteem (QOL: psychological aspect) | 5 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 I: psychological therapies and/or group programs vs usual or other care | 4 | 427 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.06 [‐0.26, 0.15] |
| 5.2 III: multidisciplinary rehabilitation vs usual or other care | 1 | 133 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐0.56, 0.12] |
| 6 Adaptation to vision loss (QOL: psychological aspect) | 6 | Std. Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 6.1 I: psychological therapies and/or group programs vs usual or other care | 3 | 495 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.11 [‐0.28, 0.07] |
| 6.2 II: methods of enhancing vision vs usual or other care | 1 | 122 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.30 [‐0.65, 0.06] |
| 6.3 III: multidisciplinary rehabilitation vs usual or other care | 2 | 376 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.02 [‐0.24, 0.19] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Acton 2016.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes RCT‐pilot with two arms evaluating a home visit‐based visual rehabilitation intervention on self‐reported visual function, psychosocial and QOL outcomes Exclusions after randomisation: none Loss to follow‐up: 4 participants (6%) Follow‐up period: 6 months after baseline, appr 4 months maintenance effect |
|
| Participants | Country: UK (Wales) Inclusion period: Oct 2014 ‐ Oct 2015 Number randomised: 71 participants Number analysed: 67 participants Age: mean 75.2 years Sex: female 54% Eye disorder(s): In 58% the primary cause of visual impairment was macular degeneration. VA: mean logMAR = 0.9 in control group; 1.0 in treatment group Inclusion criteria: (1) requirement for low vision rehabilitation; (2) distance VA < 6/12 and/or near acuity < N6 or significant contraction of visual field; (3) age 18 or older Exclusion criteria: (1) Live in area outside catchment of rehabilitation officer; (2) Ineligible for rehabilitation officer; (3) Those with significant need (fast‐track waiting list); (4) A score of < 27/30 on the MMSE indicating cognitive problems; (5) Unable to use telephone e.g. caused by very poor hearing; (6) Unable to understand English; (7) Previous recipient of low vision rehabilitation via a rehabilitation officer within the last 12 months and no relevant change in circumstances; (8) planned cataract extraction in the next 6 months |
|
| Interventions | 1) Treatment: 1 to 8 sessions/home visits from a visual rehabilitation officer. Areas assessed by the officer were emotional issues, low vision function, lighting, personal care, medication management, kitchen tasks, household chores, entitlements, orientation and mobility, communication. 2) Control group: waiting list receiving no care. Study participants received care sooner than non‐participants. |
|
| Outcomes | Primary outcome: ‐ VA LV VFQ‐48: VRQOL or difficulty in performing daily activities, consisting of mobility, visual motor skills, reading, visual information processing scales and an overall score Secondary outcomes: ‐ WEMWBS: mental well being ‐ AVL‐12: psychosocial adaptation to age‐related vision loss ‐ PHQ‐9: depressive symptoms ‐ UCLA: loneliness ‐ EQ‐5D: generic measure of health status or HRQOL |
|
| Notes | Clinical Trial Register: IRCTN44807874 Adverse events: 19 participants (12 intervention; 7 controls) were referred to their GP with depressive symptoms. Funding: the study was supported by Sight Cymru. Declaration of interest: authors declared having no conflict of interest. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated schedule, permuted blocks of two, random variation of the blocking number, stratified by age (older or younger than 65 years) |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Participants were reminded not to reveal their group allocation to outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low percentage loss to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Retrospectively registered in trial register. Protocol paper and outcome paper published in same year |
Bradley 2005.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT‐pilot with two arms to study peer group support and information provision to help people newly diagnosed to adjust to macular degeneration Exclusions after randomisation: none Loss to follow‐up: none Follow‐up period: 6 weeks after baseline (direct effect) |
|
| Participants | Country: United Kingdom Inclusion period: Oct. 2001 ‐ late 2002 Number randomised: 12 Number analysed: 12 Age: mean 76 years Sex: female 50% Eye disorder(s): AMD VA: not reported Inclusion criteria: newly diagnosed with macular degeneration Exclusion criteria: not reported |
|
| Interventions | 1) Intervention: group‐based peer support and information provision, discussion groups, 6 leaflets with information were distributed in 6 weekly topic‐specific sessions of 1.5 hours led by people experienced in living with AMD. 2) Control: waiting list, intervention delayed for 6 weeks |
|
| Outcomes | MacDQOL, selected QOL items 12‐item Well‐being Questionnaire |
|
| Notes | Funding: UK Macular Disease Society Declaration of interest: not reported Adverse events: not reported Small sample (pilot study), no baseline imbalances |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No loss to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | Trial registration and protocol not available |
Brody 1999.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to assess whether a self‐management programme focusing on behavioural skills training for older adults with AMD improves mood, self‐efficacy and activity Exclusions after randomisation: 6 participants from the waiting list control group were excluded from analyses for receiving the intervention too early. Loss to follow‐up: 38 Follow‐up period: 6 weeks follow‐up within 4 weeks after intervention (direct) |
|
| Participants | Country: USA Inclusion period: Nov. 1994 ‐ Jul. 1997 Number randomised: 92 Number analysed: 54 Age: mean 79 years (SD 5.79; range 65 to 91 years; N = 54) Sex: female 50% Eye disorder(s): AMD VA: mean logMAR intervention group: 1.04, mean logMAR control group: 1.24 Inclusion criteria: (1) diagnosis of macular degeneration by an ophthalmologist; (2) best corrected vision meets criteria for legal blindness (20/200) in at least one eye and is no better than 20/60 in the better eye; (3) no vision loss due to other eye diseases; (4) age 60 or greater; (5) no overt psychiatric conditions or cognitive impairment; (6) able to respond to the interview protocol Exclusion criteria: none reported |
|
| Interventions | 1) treatment: self‐management group focused on behavioural skills training for elderly adults with AMD who were legally blind in one or both eyes. Six sessions of 2 hours in groups of 7‐10 participants 2) waiting list controls: participants on the waiting list did not receive treatment. | |
| Outcomes | POMS (primary outcome) QWBS AMD‐SEQ Health and impact Questionnaire |
|
| Notes | ‐ This publication is an independent pilot study to Brody 2002. ‐ Primary analyses were conducted on N = 54, instead of N = 102, which was necessary for an adequate power of 0.8. ‐ The waiting list control group received a late intervention and received a follow‐up measurement. No real cross‐over design, but cross‐over analyses were additionally performed. ‐ During phases of the trial, investigators experimented with alternate forms of some of their measures; this resulted in missing or incomplete data on the final measures for participants who in all other ways successfully completed the trial. ‐ Differences in follow‐up length between groups ‐ Baseline imbalance: participants in the waiting list control group had significantly lower vision compared to the intervention group, but this was not related to the outcome. ‐ Cross‐over data could not be used in the meta‐analysis. ‐ Funding: not reported ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information to permit judgement, not clear in which way randomisation took place |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear who measured the outcomes, not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Per protocol analyses were performed (6 waiting listers receiving an intervention were excluded from analyses), intention‐to‐treat not reported Differences in length of follow‐up period for intervention versus control group (4.3 months versus 2.3 months). May induce bias |
| Selective reporting (reporting bias) | Unclear risk | Some outcomes not reported, e.g. QWBS. Unclear when measured |
Brody 2002.
| Methods |
Intervention type I: psychological therapies and/or group programmes In three publications, the outcome of an RCT with 3 arms was described, aiming to test a self‐management programme in improving QOL (2002) and social support (2005) in people with AMD, and depression in a subgroup of depressed trial participants (2006) Exclusions after randomisation: 21 participants declined participation after baseline measurement due to personal reasons. Follow‐up: 6 weeks and 6 months after baseline appr. 4.5 months maintenance effect Loss to follow‐up (Brody 2002): none reported at 6 weeks follow‐up Loss to follow‐up (Brody 2005): 17 participants declined participation at 6‐month measurements. Loss to follow‐up (Brody 2006): only a subgroup of participants was taken into account (N = 32) at this 6‐month measurement. |
|
| Participants | Country: USA Inclusion period: Feb. 1998 ‐ Sep. 2000 Number randomised: 252 Number analysed: 231 (2002), 214 (2005), 32 (2006) Age: mean 80.9 years (SD 6.1) (2002), 80.8 years (SD 6.1) (2005), 81.5 years (SD 7.5) (2006) Sex: female 66.2% (2002), 67.8% (2005), 65.6% (2006) Eye disorder(s): AMD VA: mean logMAR 1.11 (2002), 1.11 (2005), 1.26 (2006) Inclusion criteria (2002, 2005 and 2006): (1) diagnosis of AMD by an ophthalmologist and confirmed by fundus photographs; (2) VA of 20/60 or worse in the better eye and 20/100 or worse in the other eye with habitual correction (i.e. current glasses); (3) no other unstable eye diseases or vision loss due to other eye disease; (4) age 60 years or older; (5) adequate hearing, with a hearing aid if necessary, to complete the interview and to respond in normal conversation; (6) physical ability to come to an interview if wheelchairs access transportation was provided; (7) no cognitive impairment as assessed by the Orientation‐Memory Concentration test; (8) no current alcohol abuse as assessed by the Short Michigan Alcoholism Screening Test Exclusion criteria: none reported Additional inclusion criterion for data analysis in the 2006 study: meeting SCID for major or minor depressive disorder and a GDS‐15 score of > 5 |
|
| Interventions | 1) Treatment: Self‐management group intervention in which 8‐10 participants had six 2‐hour sessions led by an experienced professional in public health and behavioural medicine. The intervention was composed of both cognitive and behavioural components and focused on health education and enhancement of problem‐solving skills. 2) Control: Tape intervention: to control for the provision of education information in the intervention group, the tape control group received a series of 12 hours of audiotapes of health lectures on AMD and healthy ageing, which they could listen to during a period of 6 weeks. Waiting list control: participants on the waiting list did not receive care. | |
| Outcomes | Brody (2002) and Brody (2005): ‐ POMS (primary outcome) ‐ NEI‐VFQ mediators ‐ AMD‐SEQ ‐ DSSI ‐ LOT‐R Brody (2006): ‐ GDS‐15: extent of depressive symptoms (primary outcome) ‐ NEI‐VFQ ‐ DSSI, LOT‐R and AMD‐SEQ were taken into account as mediator variables. |
|
| Notes | ‐ Subgroup measurements for POMS, NEI‐VFQ and AMD‐SEQ also reported to assess the difference between depression status (2006) ‐ Power of 0.8 for N = 102 (2005, 2006) ‐ Subgroup analysis; power of 0.6, probably not enough (2006) ‐ Subgroup analyses reported in 2006 could have been done within the larger sample (differential analyses implemented in the full model in 2005). ‐ No SMDs calculated, no SD or SE given ‐ Not clear if waiting list controls crossed over to the intervention before the 6‐month measurement (as the name waiting list would imply). Since this was not mentioned, we assumed it has not crossed over before measurements (2005 and 2006). ‐ No baseline imbalances, no significant differences between participants and dropouts ‐ Funding: NEI, USA ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation cards |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered, individual, sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Interviews conducted by clinical psychologists and trained researchers. Procedures in place to keep treatment assignment unknown to the interviewers |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low risk was based on the Brody (2002) and (2005) reports. ‐ Only N = 21 excluded after baseline, no missing data (2002) ‐ Dropout rate was only 15.1%. Dropouts were not significantly different from participants that remained in the study. Main reported reasons for dropout were personal reasons (2005). ‐ Brody (2006): subgroup analyses, not enough power |
| Selective reporting (reporting bias) | Unclear risk | Protocol or trial registration not available |
Brunnström 2004.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to evaluate the effect of additional light adaptation in the living room on top of basic light adjustments on ADL, QOL and well‐being Exclusions after randomisation: none reported (46 randomised) Loss to follow‐up: from 56 eligible participants, 10 did not complete the study. Follow‐up period: 6 months after baseline (maintenance effect) |
|
| Participants | Country: Sweden Inclusion period: not reported Number randomised: 46 Number analysed: 46 Age: mean 76 years (range 20 to 90 years) Sex: unknown Eye disorder(s): dry macular degeneration (N = 12), wet macular degeneration (N = 16), RP (N = 2), glaucoma (N = 5), other diagnoses, not further explained (N = 11) VA: mean VA not reported, only stated that visual impairment was stated at VA <= 0.3 Inclusion criteria: (1) visually impaired people visiting the low vision clinic in Göteborg and selected for adjustment of domestic lighting Exclusion criteria: none reported |
|
| Interventions | 1) Treatment: improved lighting in the living room in addition to usual/basic lighting adjustments in other rooms (kitchen, bathroom and hall) 2) Control: only usual, basic lighting adjustments in other rooms (kitchen, bathroom and hall), no improved lighting in living room | |
| Outcomes | ‐ Three dimensions in the psychological and general well‐being scale (PGWB = HRQOL questionnaire): well‐being, vitality and depression. PGWB questionnaire was reported to be validated, but questions on well‐being, depression and vitality seemed to be single questions. Unclear if these were validated
‐ Factors on perceived QOL: loneliness, health, humour, self‐esteem, physical fitness, appetite, contact with relatives and others ‐ Daily activities |
|
| Notes | The total number of participants randomised in the study was unclear. Baseline imbalance: the control group had already higher scores on depressed mood and well‐being, compared to the intervention group. Funding: Board of Health and Social Welfare, De Blindas Vänner foundation Sweden Declaration of interest: not reported Adverse events: none mentioned |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation in blocks of four |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear who performed the interviews and thus unclear if the interviewer was aware of the treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ There was not much information available to assess attrition. ‐ Unclear if the used questionnaires were valid and reliable ‐ Statistical analyses were incomplete: no between‐group comparison, just within‐group comparison |
| Selective reporting (reporting bias) | Unclear risk | Protocol not available, unclear if all prespecified and expected outcomes of interest were reported Intention‐to‐treat also unclear |
Bryan 2014.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms in which an expressive writing intervention was studied among people with Stargardt’s disease and compared to a neutral writing condition in the participant's homes Exclusions after randomisation: unknown Loss to follow‐up: 46 (57%) Follow‐up period: 3 and 6 weeks after the 1‐week intervention, 6 weeks maintenance effect |
|
| Participants | Country: USA. Inclusion period: Oct. 2011 ‐ Apr. 2012 Number randomised: 81 participants Number analysed: 35 Age: mean 42 years, range 20‐74 years Sex: female 69% Eye disorder(s): Stargardt’s disease (juvenile AMD) VA: unknown Inclusion criteria: > 18 years, fluent in reading and writing English, diagnosed with Stargardt’s disease Exclusion criteria: none reported |
|
| Interventions | 1) Intervention: expressive writing intervention, expressing emotions through written disclosure of a post‐traumatic experience for 20 min on three separate days during a 1‐week period, participants were instructed by the researchers. 2) Control: neutral writing intervention, however, similar in dose and intensity |
|
| Outcomes | Primary outcomes: CES‐D PSS NEI‐VFQ, mental health subscale Secondary outcomes: Social support Physical symptoms, NEI‐VFQ for VRQOL |
|
| Notes | Dropouts were more depressed and stressed at baseline. No baseline imbalances Funding: no specific grant was received from any funding agency. Declaration of interest: not reported Adverse events: not reported Means and SDs of trial arms obtained through personal communication with Dept of Ophthalmology Amsterdam UMC |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computerised random number‐generator was used. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcomes obtained electronically directly from participants |
| Incomplete outcome data (attrition bias) All outcomes | High risk | High dropout rates (57%) |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
Burggraaff 2012.
| Methods |
Intervention type II: methods of enhancing vision Multicentre RCT with two arms aiming to investigate the effect of a standardised CCTV training programme on vision‐related QOL and other subjective outcomes (2012, 2012 and 2013) Exclusions after randomisation: 11 Loss to follow‐up: 8 Of 122 randomised participants, 111 filled in the baseline and 92 the follow‐up questionnaire, of which three did not have baseline measurements. Therefore, analysis were performed on data of 114 participants (which is feasible with maximum likelihood estimation). Follow‐up period: 3 months after baseline, appr. 2 months maintenance effect |
|
| Participants | Country: Netherlands Inclusion period: Feb. 2008 ‐ Jul. 2009 Number randomised: 122 participants Number analysed: 114 participants Age: mean 77.4 years Sex: female 58.2% Eye disorder(s): In 67.8% primary cause of visual impairment was macular degeneration. VA: logMAR intervention: 0.89, controls: 0.85. mean logMAR = 0.87 Inclusion criteria:(1) visually impaired with an indication for a (stand mounted ) CCTV; (2) aged >= 18 years; (3) good understanding of Dutch language Exclusion criteria: (1) cognitive deficits |
|
| Interventions | 1) Treatment: Usual instructions from supplier when CCTV was delivered combined with training sessions in the use of the device from a low vision therapist. Training sessions were once a week, with a duration of 60 minutes. Participants were trained until they had practiced with every assignment or until no further improvement in reading ability was to be expected (mean number of training sessions was 2, range 1‐7). 2) Control: Received only usual instructions from the supplier who delivered the CCTV |
|
| Outcomes | ‐ Reading speed (main outcome total study): Radner Reading Charts ‐ LVQOL (primary outcome in 2012 study): VRQOL, with 3 domains 'basic aspects', 'adaptation' and 'reading and fine work'. Secondary outcomes (2012): ‐ AVL: psychosocial adaptation to age‐related vision loss ‐ CES‐D: depressive symptoms ‐ EQ‐5D: generic measure of health status or HRQOL ‐ Task‐performance (Dutch ICF Activity Inventory reading questions + diary with information on daily use of CCTV and reading, 2013). |
|
| Notes | ‐ Intentention‐to‐treat analysis and per protocol analysis performed. ‐ Mixed‐models were used to assess outcomes, within and between group effects. ‐ SMDs of difference between treatment group and control group: Basic aspects LVQOL (‐0.34); Adaptation LVQOL (‐0.30); Reading and fine work LVQOL (‐0.32); CES‐D (‐0.24); AVL (0.36); EQ‐5D (0.26) ‐ Task performance on item level, could not be compared to other studies. ‐ Bias was introduced by recruiter who invited relatively good participants, however, in the analyses it turned out this had no effect on the primary outcome. ‐ Funding: ZonMw Inzicht (Netherlands Organisation for Health Research and Development) ‐ Declaration of interest: the authors declared having no conflict of interest. ‐ Adverse events: there were none (personal communication). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated allocation scheme, based on blocks of two, stratified by nine sites (rehabilitation centre locations) |
| Allocation concealment (selection bias) | Low risk | Allocation was performed by research personnel not involved in the study. Random assignments were sent by mail to rehabilitation centres. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme CCTV suppliers were not aware of the study, which means that their instructions were not bounded to a protocol. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The main investigators who rated the CCTV performance and treatment effect were masked to treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data analysis on intention‐to‐treat principle, in addition also per protocol analyses. Loss to follow‐up (N = 8) seemed low, however, sample size calculations based on the primary outcome (reading speed) provided a power of 0.85. |
| Selective reporting (reporting bias) | Low risk | Protocol was available (Burggraaff 2012, 2010 citation) and all prespecified outcomes of interest to the review were reported in a prespecified way. |
Christy 2012.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes A randomised trial of methods of low vision service delivery for children (8+ years) and adults (16+ years) RCT with four arms aiming to determine whether specific post‐interventional differences in QOL existed among persons who received these different rehabilitation services. Loss to follow‐up: 43 participants Follow‐up period: 9 months after baseline, appr. 4‐5 months maintenance effect |
|
| Participants | Country: India Inclusion period: Oct. 2006 ‐ Mar. 2008 Number randomised: 436 of which 347 were adults (16+) Number analysed: 311 adults Age (adult group): mean 43.7 range [16‐86 years] Sex (female, total group): 30% Eye disorder(s): Different eye disorders, AMD was most common cause for 31.6% of the participants VA (distance, best eye corrected): < 6/60 Inclusion criteria: 1) first time referral to the low vision services; 2) BCVA of less than 6/12 to light perception, or a visual field, less than 20 degrees from the point of fixation in the better eye measured using a logMAR VA chart; 3) permanent resident of Ranga Reddy or Hyderabad districts; 4) aged 8 years or older at baseline assessment; 5) having a single disability (visual impairment) Exclusion criteria: (1) not agreed to a comprehensive ophthalmic examination; (2) mental illness or dementia or was otherwise cognitively impaired and unable to understand the instructions of the rehabilitation professional; (3) unable to comprehend Telugu or English |
|
| Interventions | 1) Centre‐based service delivery: in vision rehabilitation centres, including a clinical assessment and prescription of low vision devices. A qualified rehabilitation professional trained all individuals in independent living skills, based on their individual needs, for three consecutive days (4 to 6 hours per day); 6‐12 follow‐up visits (2‐5 hours per visit) at the centre. 2) Community‐based service delivery: trained community‐based rehabilitation workers provided rehabilitation at participants' home environment. Three consecutive days, 4‐6 hours a day. Additional training was provided during 6‐12 follow‐up visits (2‐5 hours per visit) at participant's homes. Family members and neighbours were involved in training. 3) Centre‐ and community‐based service delivery: individuals were trained in needs‐based independent living skills on a one‐to‐one basis for three consecutive days, 4‐ 6 hours a day, at the centre by a rehabilitation professional. Additional training was provided at participant's home by a community‐based rehabilitation worker during 6‐12 follow‐up visits (2‐5 hours per visit). Family members and neighbours were involved in training. 4) Centre‐based with non‐interventional community visits: low vision intervention similar to the model of centre‐based service delivery, however no additional follow‐up training was provided at the rehabilitation centre and home visits made by community workers were non‐interventional. |
|
| Outcomes | For this review, only two questionnaires were used since other questionnaires also involved children. IVI‐Adult: Assessed difficulties in the participation of daily activities, for adults only (in this study, adults were 16+ years old) WHO‐QOL for HRQOL |
|
| Notes | ‐ Study also included children; we only took adults into account in the review. ‐ Within‐subgroup analyses, no between‐group analyses. No mixed model was used. ‐ Intention‐to‐treat analysis was done but not reported in thesis. ‐ Difficult to analyse other outcomes since they were 'biased' with data of children. ‐ Also a few children aged 16‐18 years were involved in analyses of adults, since these were taken into account in IVI‐Adults instead of IVI‐C. ‐ Dropout and baseline imbalance (age), however unclear if it was related to the outcome ‐ Funding: Vision Cooperative Centre, Sydney, Australia ‐ Declaration of interest: the authors declared they had no financial interest relating to the study. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Blocked randomisation by using randomisation codes |
| Allocation concealment (selection bias) | Low risk | Codes allocated to participants based on software, generated by a statistician who was not involved in the recruitment |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported, unclear if research assistant was aware of the allocation |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | N = 311 adults (16+) completed the intervention. 11.6% dropouts (36 adults). For the sample size of 436 adults (including children), a power of 0.9 was estimated with 10% assumed loss to follow‐up. Dropout rate was slightly higher than 10%, however power was high, probably no problem. |
| Selective reporting (reporting bias) | Low risk | Trial registration available, included were participants over 80 years, but register stated an exclusion criterion for participants > 80; this did not influence the comparison with other studies. No bias expected |
Conrod 1998.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with 4 arms aiming to investigate the effects of perceptual training and psychological counselling (both individual and group) on adjustment to vision loss Loss to follow‐up: 20 participants Follow‐up period: appr. 7‐8 weeks after baseline (direct effect) |
|
| Participants | Country: Canada Inclusion period: not reported. Number randomised: 49 adults with low vision (comparison group consisted of 50 adults who were fully sighted with a mean age of 70) Number analysed: 29 Age: mean age 70 years Sex: not reported Eye disorder(s): not reported VA: not reported, but inclusion criteria required all low vision participants to have a score of 40 or less on distance‐acuity measure Inclusion criteria: 1) aged 30 years or older; 2) vision loss that interferes with the ability to function normally in daily activities (equivalent to a score of 40 or less on the distance acuity measure); 3) adequate physical health, sufficiently mobile to attend sessions at university; 4) adequate psychological functioning |
|
| Interventions | 1) Perceptual training: five weekly individual one‐hour training sessions in which participants, under supervision, followed a perceptual training protocol manual 2) Individual counselling: five weekly one‐hour training sessions 3) Group counselling: five weekly one‐hour training sessions 4) Control group: no training 5) Comparison group (not randomised): fully sighted persons, no training |
|
| Outcomes | Distance and near acuity Frostig Figure Ground test: perceptual functioning Coping (designed questionnaires for the study) ‐ Activity level (activities) ‐ Cognitive strategies and beliefs regarding vision loss (beliefs) ‐ Personal assessment of residual vision ‐ Expectations of the ability to cope with in the future (expectations) |
|
| Notes | ‐ It was a 4‐arm trial in a small sample, N = 49. ‐ Two repeated measures MANOVAs ‐ Questionnaires designed for the purpose of this study, not validated ‐ Baseline imbalance unclear on dependent measures ‐ Non‐randomised comparison group with fully sighted persons not relevant for the current review ‐ Funding: Le Conseil Québecois de la Recherche Sociale; La Formaton de Chercheurs et l'Aide à la Recherche, Canada ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Unclear in which way randomisation took place |
| Allocation concealment (selection bias) | Unclear risk | Unclear in which way randomisation took place, people with relatively adequate psychological functioning were recruited, which might have introduced selection bias. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Treatment personnel were trained in three treatment options (contamination risk). Masking of participants also impossible due to recognisable rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Unclear who performed outcome assessments and if they were masked or not |
| Incomplete outcome data (attrition bias) All outcomes | High risk | N = 20 dropouts (40.8%) and distribution of attrition across 4 arms was unclear. Intention‐to‐treat not reported and unclear |
| Selective reporting (reporting bias) | Unclear risk | No protocol available Only 'beliefs' used, due to contribution to effect |
Draper 2016.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes Two‐arm RCT to compare clinic‐based versus home‐based vision rehabilitation in African‐American adults Exclusions after randomisation: none Loss to follow‐up: 7 participants Follow‐up period: 2‐3 months post intervention and after baseline (direct effect) |
|
| Participants | Country: USA Inclusion period: Dec 2010 ‐ Oct 2013 Number randomised: 55 participants Number analysed: 48 Age: mean 63‐66 years Sex: female 54% Eye disorder(s): low vision not defined VA: Inclusion criteria: (1) availability of eye exam from within one year; (2) VA between 20/70 and 20/400 or 20/50 and 20/70 but with central scotoma; (3) no past home‐based vision rehabilitation; (4) 40 years or older; (5) self‐identification of African‐American; (6) adult onset of vision loss; (7) willingness to receive home‐visits Exclusion criteria: (1) significant peripheral visual field loss to < 20 degrees in the eye used for reading; (2) eye movement disorder, e.g. nystagmus interfering with reading; (3) uncorrectable diplopia; (4) scheduled medical treatment or surgery; (5) scheduled eye treatment or surgery to improve vision; (6) low vision instructions in past 24 months; (7) not willing to complete low vision treatment within 3 months |
|
| Interventions | Five visits over 2‐3 months, including low vision aids prescription and training, home adaptations 1) Clinic‐based low vision rehabilitation: visit 1 to 5 in clinic 2) Home‐based low vision rehabilitation: visit 1, 3, 5 in clinic; visit 2, 4 at home |
|
| Outcomes | VRQOL: VFQ‐48 | |
| Notes | People with large field defects were excluded Trial registration: none Financial support: Pennsylvania Department of Health Declaration of interest: none mentioned Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Permuted block randomisation with a variable block size of four or six; stratified for baseline central visual deficit |
| Allocation concealment (selection bias) | Unclear risk | Allocation list provided on a list with two strata, concealment procedure not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme. However, the optometrist involved was masked. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The outcome was assessed by other person than the rehabilitation worker. Statisticians doing analyses were unaware of the allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ Intention‐to‐treat analysis ‐ Attrition 13% ‐ Relatively small study (N = 55) |
| Selective reporting (reporting bias) | Unclear risk | No trial registration or protocol paper |
Dunbar 2013.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to investigate the effectiveness of a standard hospital‐based low vision rehabilitation for people with diabetic eye disease Exclusions after randomisation: none reported Loss to follow‐up: 8 (4 in each arm) Follow‐up: parallel short‐term, 3 months after baseline, appr. 2.5 months maintenance effect (and cross‐over to 6 months measurement) |
|
| Participants | Country: United Kingdom Inclusion period: Jan. 2009 ‐ Feb. 2011 Number randomised: 100 Age: mean: 57 years Sex: male 62% Eye disorder(s): DR logMAR distance acuity: between 0.8 and 0.0 Inclusion criteria: 1) people with Diabetes Mellitus attending Moorfields medical retina clinics; 2) people with gradable DR of at least R1 in the better eye Exclusion criteria: 1) people under the age of 18; 2) people who were not fluent in English; 3) people with serious hearing impairment; 4) people with concomitant eye disease (other than mild cataract); 5) people who had previously attended a low vision clinic; 6) people with poor mobility or in poor general health; 7) people who were hospital inpatients, lived in nursing homes or who were otherwise non‐independent |
|
| Interventions | 1) Immediate intervention: low vision assessment, within 2 weeks of enrolment 2) Control group: intervention, low vision assessment, 3 months after enrolment, providing information, discussing aids and services and dispensing prescribed low vision aids |
|
| Outcomes | Difference in mean change in Activity Inventory (visual ability) after 3 months (primary) and after 6 months (secondary) | |
| Notes | ‐ Relatively good vision of participants ‐ Analysis of covariance (implemented in intention‐to‐treat analysis), adjusted for prognostic variables used in the minimisation process (distance VA, disease severity, sex, age) and additional secondary analyses were done. ‐ Delayed effect of interventions was not the aim of the current review, therefore 6 months follow‐up data were not synthesised for the review. ‐ Randomisation occurred before the baseline measurement which may have influenced responses to the questionnaire (AI). ‐ Funding: Fight for Sight Clinical Fellowship, UK ‐ Declaration of interest: the authors reported that they had no conflict of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Minimisation procedure, with 4 weighted factors |
| Allocation concealment (selection bias) | Low risk | Access to minimisation procedure was held by a statistician within the research and development department of the hospital. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The research assistant who administered the questionnaires was masked and reminded participants not to reveal any information about their allocation. N = 18 (6%) revealed their allocation and these masking violations were reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ High power and sample size adequately met ‐ 8% loss to follow‐up, seemed low; dropouts equal between groups and reasons for dropout similar ‐ Intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Low risk | Trial register and protocol available (Dunbar 2013, Dunbar 2012 citation). Reported in prespecified way |
Eklund 2008.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to investigate the impact of a health education programme on perceived security in performance of daily occupation 4 months (Eklund 2008, Dahlin 2002 citation), 28 months (Eklund 2008, Eklund 2004 citation) and QOL outcomes 28 months post‐intervention (Eklund 2008) Exclusions after randomisation: none reported (2002, 2004); in Eklund (2008), 15 persons refused the allocated intervention (12 from the health programme and 3 from the individual intervention programme). Loss to follow‐up: ‐ In Dahlin (2002), 66 persons dropped out of the study (36 from the individual intervention programme and 30 from the health programme). ‐ In Eklund (2004), 98 persons dropped out of the study (47 from the individual intervention programme and 51 from the health programme). ‐ In Eklund (2008), 98 persons dropped out of the study (47 from the individual intervention programme and 34 from the health programme). Follow‐up period: 4 and 28 months maintenance effect after the 6 month‐intervention |
|
| Participants | Country: Sweden Inclusion period: Jan 1996 ‐ Dec 1997 Number randomised: 253 (Dahlin 2002) and 229 reported in Eklund (2004) Number analysed: 187 (Dahlin 2002) and 131 (Eklund 2004) Age: median 79 years (range 66‐94, 2002), 78 (66‐91, 2004 and 2008) Sex: female 74% (Eklund 2004) Eye disorder(s): AMD VA: median 0.3 Inclusion criteria: (1) 65 years of age or older; (2) living at home; (3) diagnosed AMD as the primary condition; (4) a distance VA of the better eye with best correction no lower than 0.10; (5) ability to participate in group discussions Exclusion criteria: none reported |
|
| Interventions | 1) Treatment: Health education programme 'Discovering new ways', with groups of 4‐6 participants. Two hours a week, with a total duration of 8 weeks; programme was led by an occupational therapist and its main focus was on information providing and skills training. 2) Control: Individual intervention programme, standard programme for the target group at the low vision clinic. Prescription of low vision aids and information about lighting was provided. If requested, additional information about the disease could be received. Programme mainly consisted of 1‐2 one‐hour sessions at the clinic followed by telephone contact. |
|
| Outcomes | Perceived security in performing daily activities on 29 items (validated questionnaire) (Dahlin 2002, Eklund 2004) Eklund (2008): ‐ ADL staircase: dependence level in ADL based on instrumental activities (primary outcome) ‐ SF‐36: general HRQOL ‐ Self‐reported health problems |
|
| Notes | ‐ Median VA was 0.3, but relatively normal VA was allowed. ‐ Analyses on item‐level; nonparametric statistical approach, developed for evaluation of change in ordered categorical data ‐ Unclear why fewer participants were reported to be randomised in Eklund (2004), i.e. N = 229, instead of N = 253 as in Dahlin (2002) ‐ Although the SF‐36 is a general HRQOL measure, the outcomes of the study were difficult to interpret (Eklund 2008). ‐ Dropouts differed significantly on perceived health compared to participants. ‐ Mixed effects model used to analyse data, however, no effect sizes or SDs shown ‐ Funding: Synfrämjandets Research Found, KMA and Vårdal Foundation, Sweden ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Occupational therapists who were not involved in the treatment collected the data, which sounded positive. However, in the discussion part, the authors reported that participants involuntarily revealed allocated intervention while answering the questions. This could be a sign of bias, although this could also be the case for other studies in which this 'bias' is not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ N = 66/253 dropouts, of which 36 were in the intervention group, 30 in the control group (Dahlin 2002) ‐ N = 98/229 dropouts seemed relatively high. ‐ Per‐protocol analyses instead of intention‐to‐treat analyses (reported in Eklund 2008) ‐ Power analyses and sample size calculations not available |
| Selective reporting (reporting bias) | Unclear risk | No real protocol available; there was a feasibility study/focus group study prior to the trial. Unclear if all outcomes were measured in a prespecified way |
Girdler 2010.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with 2 arms aiming to evaluate the effects of usual care and usual care plus vision self‐management on health and participation outcomes of older adults with age‐related vision loss. Exclusions after randomisation: 7 Loss to follow‐up: 2 Follow‐up period: 12 weeks after baseline, appr. 4 weeks maintenance effect |
|
| Participants | Country: Australia Inclusion period: not reported Number randomised: 77 Number analysed: 77 Age: mean: 79.1 years Sex: female 64.9% Eye disorder(s): age‐related vision disorders, 79.2% AMD. VA: mean logMAR VA 0.98 Inclusion criteria: 1) age 65 or over, 2) diagnosis age‐related vision loss by ophthalmologist, 3) best corrected vision at Snellen equivalent of 6/12 or less in both eyes, 4) living in independent accomodation, 5) sufficient physical stamina, mental functioning, hearing and communication ability to attend the group intervention and 6) newly referred to the agency or had recontacted the agency after significant deterioration in vision Exclusion criteria: none reported |
|
| Interventions | 1) Intervention: usual care plus vision self‐management, including self‐efficacy and a group model based on service delivery theories and principles, 8‐week (24 h) structured programme of welcome and warm‐up exercises, learning sessions (including learning and practice activities) and homework assignments plus revisions. Intervention was delivered in a group environment with 6‐10 participants, and led by an occupational therapist and a social worker. 2) Control: usual care, which was based on a one‐to‐one case management model. Initial interview in client’s home by service coordinator to discuss service needs and to jointly develop a service plan. Visual assessment at low vision clinic by optometrists and orthoptists; prescription of low vision aids; aids provided on a trial basis; referral to internal (occupational therapy, orthoptist support, social work, orientation and mobility training, low vision technology) and external service providers. |
|
| Outcomes | Activity Card Sort (ACS): participation levels (primary outcome) Secondary outcomes: ‐ SF‐36: physical & mental component summary scores (HRQOL) ‐ GDS: geriatric depression scale ‐ GSES: generalised self‐efficacy scale ‐ AVLS: adaptation to vision loss scale ‐ AMD‐SEQ: vision specific self‐efficacy |
|
| Notes | ‐ Pilot study reported in Packer (2009) ‐ The authors stated that the self‐management programme was provided in addition to usual care. It is possible that the effectiveness of the programme lies in the interaction between these two models of service delivery. ‐ Funding: in kind contributions from the Association for the Blind of Western Australia (ABWA Inc); Australian Postgraduate Award; Freemasons Postgraduate Scholarship ‐ Declaration of interest: purchase by the ABWA of services from the last author, however, it was declared that the last author had no personal gain from this arrangement ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random assignment via computer‐generated random numbers table |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Interview assessor was masked to participants' group allocation, although participants often inadvertently revealed their allocation during post‐test and follow‐up interviews. Within this study, the authors reported the possible allocation disclosure but we assume this probably happened in more studies, without reporting. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intention‐to‐treat analysis, no dropouts |
| Selective reporting (reporting bias) | Unclear risk | No protocol available. Pilot study was available but did not provide insight into the RCT. |
Gleeson 2014.
| Methods |
Intervention type IV: other programmes RCT with 2 arms aiming to improve balance and other relevant outcomes by teaching visually impaired older adults a specific technique 'the Alexander Technique' plus usual care versus usual care. Exclusion after randomisation: 0 Loss to follow‐up: 9 Follow‐up time: 12 months after baseline with a 9 month maintenance effect |
|
| Participants | Country: Australia Inclusion period: Aug. 2010 ‐ Aug. 2011 Number randomised: 120 Number analysed: 111 Age: mean 75 years (SD 11) Sex: female 71% Eye disorder(s): community‐dwelling visually impaired older adults VA: appr. 80% 6/18 or lower Inclusion criteria: between 50‐90 years, received mobility training < 5 years, no interpreter needed, metropolitan area Exclusion criteria: no independent mobility, clinically diagnosed dementia or low score on short screener, no conversational English, cataract surgery within 12 months |
|
| Interventions | 1) Alexander Technique to improve balance + usual care by 'guide dogs' and community services with 12 weekly sessions 2) Usual care by 'guide dogs' and community services |
|
| Outcomes | Primary outcomes: physical measures, falls, balance, mobility Secondary outcomes: ‐ GDS‐5: 5‐item geriatric depression scale ‐ PANAS: Positive and negative affect scale ‐ IVI: Impact of vision impairment ‐ emotional well being subscale ‐ PVAS: perceived visual ability scale (mobility) ‐ KAP: Keele assessment of participation ‐ Socialisation: frequency of contact with others |
|
| Notes | ‐ 488 eligible participants ‐ Funding: in kind support by Guide Dogs NSW/ACT; Australian Society of Teachers of the Alexander Technique; FM Alexander Trust (UK); Australian Postgraduate Award Scholarship, Australian Federal Government; Australian National Health and Research Council; Australian Research Council ‐ Declaration of interest: the authors declared they had no conflict of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation, computer‐generated list performed by a centre‐based investigator who had no contact with participants |
| Allocation concealment (selection bias) | Low risk | Participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Due to the study design, participants and the intervention providers could not be masked. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All outcome assessors remained masked to group allocation for all assessments, and participants were asked not to reveal their allocation status. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Loss to follow‐up was low and similar for both groups. Between‐group differences were not statistically significant. |
| Selective reporting (reporting bias) | Low risk | Protocol was available, was amended in 2012 and is up‐to‐date. |
Goldstein 2007.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to describe the development of the educational video and to determine the effectiveness of the video in achieving people's self‐efficacy with regard to obtaining and using assistive devices and other rehabilitation resources. Exclusion after randomisation: 2 out of N = 156 baseline interviews Loss to follow‐up: 5 over 2 follow‐up measurements Follow‐up period: 2 weeks and 3 months after baseline (maintenance effect) |
|
| Participants | Country: USA Inclusion period: winter 2002 Number randomised: 154 Number analysed: 151 Age: median 77.5 years (range 39‐92) Sex: female 64.2% Eye disorder(s): not reported VA: not reported Inclusion criteria: 1) having low vision (as defined by the National Eye Institute, US); 2) understand English; 3) have access to a VCR and television; 4) be able to hear well enough to participate in a telephone survey Exclusion criteria: not reported |
|
| Interventions | 1) Video group: educational video which addressed educational, emotional and motivational needs associated with low vision. Participants had 2 weeks of time to watch the video. 2) Control group: waiting list, received no care |
|
| Outcomes | Knowledge Attitude Behaviour (self‐efficacy and emotional response) Willingness to use devices |
|
| Notes | ‐ Participants who completed the study were paid a small stipend. ‐ Possible ceiling effect in knowledge, participants were recruited at a seminar in which they had already acquired some knowledge of disease and rehabilitation (however, no problem due to randomisation), still an effect on knowledge. ‐ Baseline imbalance on main outcomes unknown ‐ ANCOVAs used to examine effects between baseline and 2 follow‐up time points ‐ Unclear if questionnaires were validated ‐ Funding: NIH grants, USA ‐ Declaration of interest: the authors declared that they had no proprietary interest in the video. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised block design with block size 4 |
| Allocation concealment (selection bias) | Low risk | Interview software automatically assigned participants to control or intervention group. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Survey centre staff was not masked to the assigned group of participants. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Sample size calculation: 128 needed, 64 in each group. N = 156 included to account for possible attrition, 5 participants lost to follow‐up, which is a low dropout rate. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
Jackson 2017.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms comparing regular comprehensive vision rehabilitation (VR) to access to a video magnifier (VM) + VR on reading performance, VRQOL and mental health. Only one‐month follow‐up outcomes reported Exclusions after randomisation: none Loss to follow‐up: 6 at 1 month Follow‐up period: 1 month after enrolment (direct effect; 2 months and one year not reported) |
|
| Participants | Country: USA Inclusion period: Feb 2010 ‐ May 2011 Number randomised: 37 participants Number analysed: 31 participants Age: mean 71 years Sex: female 49% Eye disorder(s): 73% AMD or juvenile MD VA: logMAR 0.72 treatment; 0.79 controls Inclusion criteria: (1) age 40 years or older; (2) central visual field loss; (3) no disease affecting peripheral retina; (4) VA < 20/40 of the best eye; (5) MMSE score > 20; (6) sufficient hearing Exclusion criteria: (1) dementia; (2) clinical depression; (3) vision rehabilitation or video magnification experience |
|
| Interventions | 1) usual comprehensive vision rehabilitation with optical aids of preference 2) usual comprehensive vision rehabilitation with optical aids of preference, plus access to a desk model video magnifier |
|
| Outcomes | ‐ Reading speed in words per minute: International Reading Speed Texts ‐ IVI: vision‐related QOL, with 3 domains reading, mobility and well‐being ‐ DASS: depression, anxiety and stress ‐ AI‐reading subscale |
|
| Notes | ‐ Small population, N = 37, intention in trial register: N = 120 ‐ Follow‐up period up to one year, will not be reported by authors (personal communication) ‐ Repeated measures of variance were used to analyse study effects. ‐ Funding: devices provided by Optelec USA ‐ Declaration of interest: authors reported that they had no conflict of interest. ‐ Adverse events: not reported ‐ Trial register: NTC016770643 ‐ Data obtained from authors after personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomisation according to computer‐generated scheme, and after inclusion of half of the participants, an adaptive design was adopted to ensure the groups were comparable regarding VA (stratification). |
| Allocation concealment (selection bias) | Unclear risk | Not reported how allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Assessor was masked to group assignment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Loss to follow‐up 16% in a relatively small study (N = 37), however, no significantly different characteristics of participants lost to follow‐up No sample size calculation, intention was N = 120 participants |
| Selective reporting (reporting bias) | High risk | Trial register report available, however, 1 year outcomes were not reported and are possibly not going to be reported. |
Kaltenegger 2019.
| Methods |
Intervention type II: methods of enhancing vision Cross‐over RCT with two arms comparing reading training to placebo training doing crossword puzzles Exclusions after randomisation: none Loss to follow‐up: 10 Follow‐up period: 12 weeks after enrolment, however, this review used only the direct effect 6 weeks after baseline |
|
| Participants | Country: Germany Inclusion period: Nov 2012 ‐ Jun 2015 Number randomised: 37 participants (treatment N = 25, control N = 12) Number analysed: 27 participants Age: median 72 years (IQR 67.5 ‐ 79) Sex: female 57% Eye disorder(s): AMD VA: not reported, see inclusion criteria Inclusion criteria: (1) Dry AMD with an absolute central scotoma (2) non‐foveal (parafoveal or eccentric) fixation, (3) magnification requirement 1.25 – 10‐fold, (4) VA 0.2–1.1 logMAR (decimal 0.08–0.60), (5) previous adaptation to the use of magnifying aids of at least 6 weeks Exclusion criteria: (1) Any other eye disease, (2) exudative AMD, (3) simultaneous anti‐VEGF or other treatments, (4) reduced emotional and cognitive status |
|
| Interventions | 1) Reading training with sequentially presented text (RSVP) in addition to magnifying aids 2) Control group: placebo training (doing crossword puzzles) in addition to magnifying aids Both groups performed the training exercises at home for 6 weeks, 5 days/week, 30 min/day. |
|
| Outcomes | ‐ Reading speed ‐ Fixation stability and preferred retinal locus ‐ MADRS: Montgomery–Åsberg Depression Rating Scale ‐ DemTect: cognitive status ‐ IVI: vision‐related QOL |
|
| Notes | ‐ Follow‐up cross‐over period not assessed in this review ‐ Funding: Governmental funding: Ministerium für Soziales und IntegrationBaden‐Württemberg, and foundations: Tistou & Charlotte Kerstan Stiftung, Paul Lechler Stiftung ‐ Declaration of interest: authors reported that they had no conflict of interest. ‐ Adverse events: not reported ‐ Data on depression and vision‐related QOL requested and received for meta‐analysis, medians available in publication ‐ Additional data and information on study procedures received by personal communication. They reported that there were no adverse events. ‐ German Clinical Trials Register: DRKS00015609 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation according to predefined tables |
| Allocation concealment (selection bias) | Unclear risk | The PI explained study procedures and concealed the group allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Researchers performed the outcome assessments, not clear if they were masked |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition seemed high (32%) for QOL‐related outcomes in a small study with unequal trial arms (N = 27 treatment, N = 10 controls). |
| Selective reporting (reporting bias) | Unclear risk | Trial registration of protocol after study ending. The placebo training was changed because of the inaccessible format for people with low VA. No other changes reported |
Kaluza 1996.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to determine whether acute stress reactivity of Intraocular pressure (IOP) to a short‐term achievement‐related stressor can be influenced by relaxation procedures in open angle glaucoma Exclusions after randomisation: none reported Loss to follow‐up: unclear Follow‐up period: unclear, training duration was 8 weeks (possibly direct effect) |
|
| Participants | Country: Germany Inclusion period: not reported Number randomised: 23 Number analysed: 23 Age: median age 52 years (range 20‐68) Sex: female 78.2% Eye disorder(s): primary angle glaucoma VA: not reported Inclusion criteria: 1) ophthalmologic diagnosis of primary open‐angle glaucoma; 2) no other major medical or psychiatric condition and 3) capable of speaking and writing the German language Exclusion criteria: none reported |
|
| Interventions | 1) Training group: training to support peoples' coping with the threats and demands of the disease and to enable them to self‐regulate stress‐induced elevated IOP levels. Eight weekly 90‐minute sessions in group format conducted by an experienced clinical psychologist. Training in standard autogenic relaxation. Furthermore, participants were encouraged to practice exercises at home regularly. 2) Control group: waiting list control group |
|
| Outcomes | Intraocular pressure (IOP) Psychological strain (KAB) Heart rate |
|
| Notes | ‐ Small population, N = 23 ‐ Baseline imbalance on age, not on main outcomes ‐ Unclear follow‐up period ‐ Three factorial mixed‐model analyses of variance, MANOVA ‐ Funding: not reported. ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported in which way randomisation took place |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme. Contamination, 11 participants in total (from which 8 in the control group) earlier received relaxation training and the knowledge of participants in control group that study was about relaxation effects |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not clear who measured psychological strain. For heart rate, it was clear that students were masked. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ‐ 3 dropouts of 23 participants = 13% (from 11 to 9 in treatment group, from 12 to 11 in control group) ‐ Unclear follow‐up period and if intention‐to‐treat analysis was performed |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
Kamga 2017.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms, focusing on reducing depressive symptoms in people with retinal disease in a home‐based setting Exclusions after randomisation: none Loss to follow‐up: 10 Follow‐up: 8 weeks after baseline (direct effect) |
|
| Participants | Country: Canada Inclusion period: Nov 2014 ‐ Dec 2015 Number randomised: 80 Mean age: 76 years Sex: female 62% Eye disorder(s): 55% macular degeneration, 45% DR VA: mean logMAR VA 0.37 (20/50 or 6/15) Inclusion criteria: (1) age > 50 years, (2) clinical diagnosis of late‐stage macular degeneration or DR, (3) PHQ‐9 depression score 5 or > indicating mild symptoms, (4) VA > 20/200, (5) adequate cognition Exclusion criteria: (1) already receiving cognitive behavioural therapy, (2) suicidal intent, (3) ocular surgery during study, (4) cognitive impairment, (5) inability to speak or understand English or French, (6) profound hearing impairment |
|
| Interventions | 1) Intervention: cognitive behavioural therapy‐based self‐care tool intervention (antidepressant skills workbook, mood monitoring tool, DVD on depression) plus up to three coaching 10‐minute phone calls by a trained former nurse 2) Controls: 'usual care' defined as waiting list control group receiving the intervention after follow‐up with one phone call |
|
| Outcomes | Primary outcome: ‐ PHQ‐9: depressive symptoms Secondary outcomes: ‐ GAD‐7: generalised anxiety symptoms ‐ Life Space assessment questionnaire ‐ Self‐efficacy scale |
|
| Notes | ‐ Treatment fidelity was assessed by recording coach phone calls. ‐ Intention‐to‐treat using multiple imputation was carried out for the primary outcome, but also complete case for the secondary outcomes and subgroup analyses were performed. ‐ Funding: Fonds de Recherche en Sante du Quebec, Vision Health Research Network, Antoine Turmel Foundation ‐ Declaration of interest: authors declared having no conflict of interest; funding organisations had no role in design or conduct of the study. ‐ Adverse events: recorded, but none mentioned ‐ Trial register: NCT02261194 ‐ Note: Small baseline imbalances included differences in VA, use of antidepressants and use of psychotherapy between groups, but they were not harmful. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Website‐based random number generator with a block size of four |
| Allocation concealment (selection bias) | Low risk | Assignments in sealed envelopes and opened in front of participants |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Telephone interviewers were masked to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Loss to follow‐up 12.5%, power analyses and sample size calculation based on numbers analysed |
| Selective reporting (reporting bias) | Low risk | Protocol available and reported according to expectations |
Leat 2017.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to investigate the effects of closed‐circuit television versus eccentric viewing training to enhance reading and VRQOL Exclusions after randomisation: none Loss to follow‐up: 4 Follow‐up period: 6 weeks after baseline (direct effect) |
|
| Participants | Country: Canada Inclusion period: appr. 2010 ‐ 2013 Number randomised: 14 (out of planned 30) Mean age: 82 years Sex: female 20% Eye disorder(s): AMD VA: between 20/160 and 20/400 and later extended to 20/630 Inclusion criteria: (1) diagnosis of AMD and VA between 20/160 and 20/630 in the better eye, (2) first‐time patient of blind institute, (3) age > 50 years, (4) able to read English, (5) helper at home to help with intervention Exclusion criteria: (1) no anticipated ocular treatment during trial (except anti‐VEGF), (2) reading was not a goal, (3) cognitive impairment, (4) other ocular disease reducing vision |
|
| Interventions | (1) Treatment: closed‐circuit television delivered and set up within one week after randomisation at home. Participants were asked to practice for 6 weeks 2 times 10 minutes everyday. (2) Treatment: eccentric viewing training within one week after randomisation 1.5‐2 hrs and then home training with an observer giving feedback on accuracy. Participants were asked to practice for 3 weeks 2 times 10 minutes everyday. After that, a phone call was made to check compliance and training and home work was repeated. |
|
| Outcomes | Primary outcomes: ‐ Reading accuracy and reading speed and performance Secondary outcomes: ‐ Reading behaviour inventory ‐ VFQ‐25: VRQOL ‐ GDS: depression |
|
| Notes | ‐ Trial register: NCT00971464 ‐ Funding: Lawson Research institute, Foundation‐Jarmain Family Fund. Optelec funded CCTVs. ‐ Declaration of interest: none declared ‐ Adverse events: not reported ‐ Data obtained from authors after personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random sequence generation mode not reported. Randomisation was stratified by VA group. |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment procedure not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessors could not be masked. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Small sample: N = 14 were included, with N = 4 lost to follow‐up. Intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | Trial registration available: an initial sample of N = 30 was aimed, secondary outcomes were requested for meta analysis and sent. |
McCabe 2000.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes RCT with two arms aiming to evaluate a multidisciplinary model of outpatient vision rehabilitation, including optometry, occupational therapy and social work interventions and to assess whether involving families in the rehabilitation process further enhances the participant's level of functioning Exclusion after randomisation: 12 people changed their mind about participating. Loss to follow‐up: 13 participants dropped out for reasons not specifically related to the study. Follow‐up: no follow‐up period reported, seems to be directly after the intervention |
|
| Participants | Country: USA Inclusion period: 20 months, not reported exactly when Number randomised: 97 Mean age 69 years, median 76 years, range 19 to 91 years Sex: female 52 (53.6%) Eye disorder(s): predominant ophthalmic diagnosis was macular degeneration (64%). Other diagnoses included DR, other retinal diseases, optic neuropathy, glaucoma and cataracts. VA: 20/100 or worse in the better eye, 50% of the participants had a VA lower than 20/200 Inclusion criteria: (1) 19 years or older; (2) BCVA of 20/100 or worse in the better eye; (3) mental competence; (4) ability to communicate in English by telephone; (5) probability of completing the intervention; (6) participant's willingness to include a family member, neighbour or friend Exclusion criteria: (1) terminal illness; (2) plans to leave the area; (3) distance from the hospital |
|
| Interventions | All participants in the study received the Infirmary's standard vision rehabilitation programme to help them learn to use their remaining vision to its fullest capacity. Rehabilitation included training in the use of prescribed optical and non‐optical devices, instruction in adaptive techniques, and adjustment counselling. 1) Treatment: family rehabilitation intervention. Family members were included in all stages of the rehabilitation process. Time was spent educating family members about the ophthalmic condition and the rehabilitation process. Families also used simulators to understand the nature of the participant's vision loss. The social work interview included an exploration of the meaning of vision loss for the family unit and the ways the family members worked together to adapt to the loss. 2) Control: individual rehabilitation intervention, which focused solely on the participant. Family members were excluded from all sessions. | |
| Outcomes | ‐ Self‐reported Functional Assessment Questionnaire (FAQ), a) evaluation of specific visual functions by asking participants to rate the difficulty they had in performing 40 visual skills, using a three‐point scale (easy, moderate, hard); b) evaluation of the functional independence by asking participants to rate the extent to which they used assistance from others in performing 40 activities, using a three‐point scale (never, sometimes, always) ‐ Observer‐rated Functional Visual Performance Test (FVPT) |
|
| Notes | ‐ There was no control group receiving no intervention or waiting list control.
‐ Change score for total group and separate arms reported. No mixed effects models used to analyse data ‐ FAQ validated, FVPT designed for this study and validated, good properties ‐ Funding: Robert Wood Johnson Foundation USA ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were assigned by a randomisation process but unclear in which way |
| Allocation concealment (selection bias) | Unclear risk | Not reported, only reported that participants were 'immediately assigned' |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The self‐report questionnaire was administered over the telephone by research assistants who were masked to the intervention protocol. Functional vision was observed by an occupational therapist; unclear if outcome assessor was masked (less relevant measure for current review) |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ Intention‐to‐treat analysis ‐ 23% dropout, sample size requirements: 50 in each group with a power of 0.7; power to detect effects may be low. |
| Selective reporting (reporting bias) | Unclear risk | No protocol or trial registration available |
Mielke 2013.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to investigate the effects of professional visual rehabilitation on developing a secondary depressive disorder as well as on cognitive status and QOL Exclusions after randomisation: none reported Loss to follow‐up: 6 for VRQOL measurement Follow‐up period: 3 months after baseline (appr. 2.5 months maintenance effect) |
|
| Participants | Country: Germany Inclusion period: not reported Number randomised: 20 Number analysed: 14 for VRQOL, however, different numbers for different parameters Age: mean 79 years (range 65‐85 years) Sex: female 65% Eye disorder(s): AMD VA: distance: mean 0.125 (SD 0.08); near: mean 0.08 (SD 0.1) Inclusion criteria: 1) age 65‐85 years; 2) diagnosed with AMD; 3) first request for low vision aids within the university clinic Tübingen (Germany); 4) decimal VA in best eye between 0.05‐0.2; 5) potential to increase reading ability Exclusion criteria: 1) severe musculoskeletal impairment; 2) manifest dementia; 3) not able to handle magnification aids; 4) severe depression, with psychotic or suicidal symptomatology |
|
| Interventions | 1) Treatment (N = 9): rehabilitation measures: provision of magnifying visual aids and training 2) Control (N = 11): waiting list, rehabilitation possible after 3 months | |
| Outcomes | GDS: Geriatric depression scale ADS‐L: German version of CES‐D DemTecT: Dementia detection test MMS: Mini Mental Status (cognitive functioning) NEI‐VFQ 25: National Eye Intstitute Visual Functioning questionnaire IREST: Reading speed, continuous text reading chart |
|
| Notes | ‐ Small sample, N = 20 ‐ There seemed to be a baseline imbalance on the VRQOL questionnaire. ‐ Distance and near VA and magnification needed did not change over the three‐month period. ‐ Analysis of variance with repeated measurements ‐ Funding: Ministerium für Arbeit und Soziales des Landes Baden‐Württemberg, Germany ‐ Declaration of interest: the authors declared that they had no conflict of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported, although impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported, just that data gathering was in cooperation with the Department of Psychiatry and Psychotherapy from the Tübingen University clinic |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ‐ Participants analysed for QoL outcome, NEI‐VFQ unclear ‐ Per protocol analysis ‐ High dropout rate in data related to QOL |
| Selective reporting (reporting bias) | Unclear risk | ‐ No protocol or trial registration available |
Mozaffar Jalali 2014.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms, focusing on increasing psychological well‐being in a low vision rehabilitation or non‐governmental organisation setting Exclusions after randomisation: none Loss to follow‐up: none Follow‐up: 1 month after baseline (direct effect) |
|
| Participants | Country: Iran Inclusion period: not reported Number randomised: 60 Mean age: 20‐40 years Sex: not reported Eye disorder(s): blind VA: unknown Inclusion criteria: 60 persons were chosen out of 1300 from rehabilitation/NGO settings Exclusion criteria: unknown |
|
| Interventions | 1) Intervention: group‐based rational emotive behavioural therapy which is a comprehensive, active‐directive psychotherapy focusing on resolving emotional and behavioural problems 2) Control: no training |
|
| Outcomes | Primary outcome: DASS Secondary outcomes: Jones irrational beliefs questionnaire Eysenck’s self‐esteem inventory |
|
| Notes | ‐ Number of sessions and duration unclear, background of therapists unclear ‐ No power analysis, possible selection bias (60 participants were 'chosen'), baseline characteristics not reported ‐ Funding: not reported ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes obtained in groups, masking of outcome assessors not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There was no attrition, complete dataset |
| Selective reporting (reporting bias) | Unclear risk | No protocol available, unknown |
Nollet 2016.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with three arms to determine whether PST and/or a referral to the general practitioner would diminish depressive symptoms DEPVIT Exclusions after randomisation: 1 referral arm and 5 in PST arm Loss to follow‐up: 8 unable or not willing to continue Follow‐up period: 6 months after baseline, appr. 4 months maintenance effect |
|
| Participants | Country: United Kingdom Inclusion period: not reported Number randomised: 85 Mean age: 70 years Sex: female 50 (59%) Eye disorder(s): low vision, not otherwise specified VA: unknown Inclusion criteria: adults 18 years and older, attending low vision services, GDS‐15 > 6. Exclusion criteria: low vision assessment within previous 12 months, referral to service in error, already receiving depression treatment, not able to understand English, unable to use telephone due to poor hearing, severe medical illness, suicidal ideation, outside catchment area, low score on cognitive/memory scale |
|
| Interventions | 1) Problem‐solving treatment: trained therapists delivered a seven‐step cognitive behavioural therapy to approach problems participants wanted to address. Sessions took place in the participant's own home or at the low vision service; large print self‐help materials were used as well. 2) Referral to general practitioner: within two weeks after randomisation, a standardised letter was sent to the general practitioner informing them of the positive screening on clinically significant depressive symptoms and asking them to provide stepped‐care according to NICE guidelines. 3) Waiting list control: no intervention other than a 6‐week low vision assessment |
|
| Outcomes | Primary outcomes: depressive symptoms BDI‐II: Beck depression inventory GDS‐15: geriatric depression scale Secondary outcomes: visual functioning, VRQOL LV VFQ‐48: reading ability NEI‐VFQ: 7‐item visual functioning EQ‐5D: Euroqol 5 dimensions, health status/HRQOL Cost‐effectiveness |
|
| Notes | ‐ UK trial register: ISRCTN46824140 ‐ Modest number of participants. Intervention not always delivered as intended ‐ Two adverse events: one fall due to dizziness after antidepressants; ten serious adverse events unrelated to trial; one withdrawal in the control group due to suicidal ideation ‐ Funding: Guide Dogs UK ‐ Declaration of interest: the authors declared that they had no conflict of interest. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was performed by using permuted blocks of varying sizes. |
| Allocation concealment (selection bias) | Low risk | Allocation was performed by a data manager, who was not included in any other part of the study. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants were not masked, therapists were not masked, but general practitioners were not aware of the trial. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessors were masked. Masking violations were recorded, however, these results were not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Reasons for missing outcome data balanced in numbers across intervention groups, with similar reasons |
| Selective reporting (reporting bias) | Low risk | Study protocol was available and all of the study’s prespecified outcomes that were of interest in the review have been reported. |
Pankow 2004.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes RCT with two arms aiming to test the effectiveness of a vision rehabilitation programme in enabling older adults with visual impairment to achieve rehabilitation goals to improve independent function and psychological well‐being Exclusions after randomisation: none reported Loss to follow‐up: not clear Follow‐up: 4‐6 weeks after service ended as a maintenance effect which is 3 to 3.5 months after baseline |
|
| Participants | Country: USA Inclusion period: not reported Number randomised: 30 Number analysed: 30, however not clear Age: mean 77.8 years (range 65 to 90 years) Sex: female 56.7% Eye disorder(s): most frequent cause of vision loss was macular degeneration, next hemianopia (33%), VA: not reported, however 60% of study participants were blind. Inclusion criteria: (1) age 55 years or more; (2) seeking vision rehabilitation services for the first time; (3) sufficient cognitive function to meaningfully answer interview questions; (4) stable acquired visual impairment demonstrated by best corrected acuity of 20/50 or less in each eye and/or a visual field of 20 degrees or less in each eye or homonymous hemianopia or quadrantopia or any combination of these characteristics Exclusion criteria: none reported |
|
| Interventions | Treatment: orientation & mobility training and/or blind rehabilitation teaching and/or low vision evaluation Control: waiting list (education regarding ocular disease) | |
| Outcomes | NAS2: Nottingham Adjustment Scale (primary outcome) FIMBA: Functional Independence Measure for Blind Adults ‐ performance with respect to living skills ‐ orientation and mobility skills | |
| Notes | ‐ Small sample, N = 30 ‐ Participants had maximal waiting period of 8 weeks. ‐ Multidisciplinary rehabilitation; it was not possible to compare the effectiveness of separate interventions. ‐ Fluctuating follow‐up time points. Outcome not validated ‐ ANCOVAs with pretest scores as covariates, means and SDs provided, difference between pretest and post‐test within group or difference between post‐test of treatment and control group ‐ Funding: Corning Medical Optics; Designs for Vision donated optical aids to participants ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were assigned in yoked pairs in a random fashion to treatments and control groups. Not reported explicitly how |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme. Evaluators were also trainers and researchers; this may indicate contamination. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Evaluators were aware who was in treatment and control group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Unclear if participants dropped out, not reported |
| Selective reporting (reporting bias) | Unclear risk | No protocol or trial registration available |
Patodia 2017.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to investigate the effects of available low vision devices on visual ability and QOL of glaucoma participants Exclusions after randomisation: none Loss to follow‐up: none Follow‐up period: 4 weeks after baseline (direct effect) |
|
| Participants | Country: Canada Inclusion period: not reported Number randomised: 16 Number analysed: 16 Age: not reported Sex: not reported Eye disorder(s): glaucoma Inclusion criteria: (1) primary or secondary open angle glaucoma stable 1 year, (2) BCVA > 20/400 and < 20/70, (3) no surgical or laser procedures in the last 6 months, (4) retained visual field < 20 degrees Exclusion criteria: (1) no telephone access, (2) unable to speak Engish, (3) received low vision aids before, (4) various health conditions that would interfere with measurements |
|
| Interventions | Treatment: low vision outpatient treatment including examination, prescription of low vision devices for 4‐week use to determine which would be most beneficial and single training session, i.e. binocular and monocular telescopes, telemicroscopes, magnifiers, portable CCTV and absorptive filters Control: low vision examination, but no intervention |
|
| Outcomes | VA LV VFQ‐48: VRQOL, visual ability | |
| Notes | Small sample, N = 16 Paired and two‐samples t‐tests used to analyse data ‐ Funding: in part by Canadian National Institute for the Blind and Glaucoma Research Society of Canada ‐ Declaration of interest: authors reported no conflicts of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated allocation scheme was used; allocation not dependent on sample size |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Telephone interviewers were masked to treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in the analyses, intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | No protocol available, but it seemed there were no other analyses intended |
Pearce 2011.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to investigate the effect of adding further low vision device training on top of consultation with an optometrist Exclusions after randomisation: none reported Loss to follow‐up: 24 participants, 12 in each group Follow‐up period: 1 and 3 months follow‐up after baseline (maintenance 2.5 months) |
|
| Participants | Country: United Kingdom Inclusion period: not reported Number randomised: 120 Number analysed: 96 Age: mean 73.1 years Sex: male 37.5% Eye disorder(s): not reported VA: mean logMAR VA 0.67 Inclusion criteria: 1) all first time attendees to the low vision clinic, 2) age 18 years or older Exclusion criteria: 1) not being independent, 2) not fluent in English, 3) hospital inpatients, 4) previously attending a low vision assessment elsewhere, 5) serious hearing impairment; 6) VA better than 6/12; 7) no significant visual field loss in better eye |
|
| Interventions | 1) Intervention: a 1‐hour appointment with a low vision support worker 2 weeks after the initial low vision assessment, reviewing handling of low vision devices, discussing daily issues at home, focusing on low vision devices. Conventional low vision assessment with follow‐up 2) Control group: received a well‐person check with a nurse, only measuring weight, height, vision and blood pressure. Conventional low vision assessment |
|
| Outcomes | Massof Activity Inventory (MAI): assesses vision‐related activities of daily living, social and recreational (visual ability). Manchester Low Vision Questionnaire (MLVQ): low vision device handling |
|
| Notes | ‐ T‐tests on change scores; no mixed models were used. ‐ People should be able to have remaining vision to be recruited in the study. No inclusion of severe visually impaired ‐ Funding: Special Trustees of Moorfields Eye Hospital, UK ‐ Declaration of interest: the authors declared that they had no competing interests. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation reported to be randomised, but not explained in which way; insufficient information to permit judgement |
| Allocation concealment (selection bias) | Low risk | A sealed envelope technique was used; all investigators were masked to the randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All investigators were masked to randomisation. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ Intention‐to‐treat analyses performed ‐ Number randomised was 120 (48 were needed per arm); number analysed was 96. |
| Selective reporting (reporting bias) | Low risk | Trial registration; importance of outcomes on Massof's AI was planned, however the outcome chosen may not have been appropriate. Difficult to measure an effect on importance of items in AI |
Pinninger 2013.
| Methods |
Intervention type IV: other programmes RCT with two arms aiming to investigate the feasibility, acceptability and adherence to a tango programme for individuals with AMD in improving well‐being Exclusions after randomisation: none reported Loss to follow‐up: none Follow‐up: 4 weeks after baseline (direct effect) |
|
| Participants | Country: Australia Inclusion period: not reported Number randomised: 17 Number analysed: 17 Age: mean 79.4 years Sex: female: 100% (all participants female) Eye disorder(s): AMD VA: not reported, < 6/48 Inclusion criteria: 1) People diagnosed with AMD (acuity of 6/48–6/120), 2) 65 years or older, 3) experiencing feelings of sadness or depression, 4) wishing to improve mood and well‐being Exclusion criteria: 1) unstable cardiovascular conditions, history of stroke, walking or balance problems (e.g. vertigo, leg weakness) that might affect the capacity to participate in the activity, 2) auditory or cognitive disorders that could significantly affect mobility or the ability to follow instructions, 3) other significant ocular disorders, such as cataracts or glaucoma |
|
| Interventions | 1) Intervention: tango dance group programme; sessions of 1.5 hrs, twice a week, during 4 weeks. Tango lesson started with warming up, dance instructions and available time to share experiences or ask questions. 2) Control: waiting list, only 'post test' interview conducted |
|
| Outcomes | NEI VFQ‐25: National Eye Institute Visual Functioning Questionnaire SWL scale: Satisfaction With Life, global perceptions of well‐being and contentment with life GDS‐short version: Geriatric Depression Scale Rosenberg self‐esteem scale |
|
| Notes | ‐ Feasibility study, therefore a small study sample (N = 17) ‐ Although not an inclusion or exclusion criterion, the study population consisted of women only. ‐ Baseline characteristics were not explicitly reported; VFQ25 no differences ‐ ANCOVA analyses with baseline scores as covariates ‐ Study effects not fully explained, no table of results before and after. Difficult to interpret ‐ Funding: grants form McGill University Montreal, Canada ‐ Declaration of interest: the authors declared that they had no conflict of interest. ‐ Adverse events: not reported ‐ No response to data request |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation process: numbers drawn from a hat |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment was not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to the recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Volunteers assisted in completion of the pre‐ and post‐test questionnaires. The questionnaires for participants in the waiting list control group was conducted via telephone, whereas the questionnaires for tango participants were administered after a tango session, face‐to‐face. This indicated that these volunteers were aware of the treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ All participants randomised were analysed (no dropouts). ‐ An intention‐to‐treat analysis was performed. |
| Selective reporting (reporting bias) | High risk | ‐ Study protocol was not available to identify any other unreported outcomes. ‐ The outcome measure VFQ‐25 was reported incompletely. No interpretation possible for estimation of the effect after the treatment period |
Rees 2015.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms in which a group‐based self‐management intervention was compared to usual care to diminish depressive symptoms Exclusions after randomisation: 5 Loss to follow‐up: 19 (16%) Follow‐up period: 1 and 6 months post‐intervention which was appr. 8 months after baseline (6 months maintenance effect) |
|
| Participants | Country: Australia Inclusion period: retrospectively recruited between 2007 and 2008 Number randomised: 153 Mean age: 80 years (SD = 8) Sex: female (60%) Eye disorder(s): 70% AMD, 6.6% glaucoma, 6.6% DR, 17% other VA: 87% > logMAR 0.5 Inclusion criteria: received a low vision assessment in the previous 12 months, VA of < 6/12 and > 6/480 in the better eye with habitual correction, age > 55 years, living independently (not in a nursing home), English speaking, adequate hearing to respond to normal conversation, no cognitive impairment (assessed by screener) Exclusion criteria: opposite of inclusion |
|
| Interventions | 1) Intervention: group‐based self‐management programme focusing on coping with illness and disability. Weekly 3‐hour sessions for 8 weeks offered by two low vision rehabilitation counsellors and guest speakers. 2) Control: usual care provided by a low vision rehabilitation service, initial assessment by multidisciplinary team, optometric assessment and prescription of optical aids, further training provided by the multidisciplinary team |
|
| Outcomes | Primary outcomes: DASS: Depressive, Anxiety and Stress Symptoms IVI: Impact of Vision Impairment ‐ emotional well‐being subscale Secondary outcomes: GSES: self‐efficacy AVL: adaptation to Age‐related Vision Loss IVI: Impact of Vision Impairment, VRQOL |
|
| Notes | Trial register: ACTRN12607000399493 ‐ Response rate seemed low (18%). ‐ Funding: Australian Research Council Linkage grant; The Centre for Eye Research Australia receives Operational Infrastructure Support from the Victorian Government. ‐ Declaration of interest: the authors declared that they had no conflict of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random allocation scheme was used. |
| Allocation concealment (selection bias) | Low risk | Opaque sealed envelopes were used. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Masked and independent research assistants administered questionnaires. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rate was low (16%). |
| Selective reporting (reporting bias) | Unclear risk | Trial was registered retrospectively and the timing of reported outcomes did not seem to match the protocol. |
Reeves 2004.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes RCT with 3 arms aiming to investigate the (cost) effectiveness of different strategies of low vision rehabilitation for people with newly diagnosed AMD Exclusions after randomisation: none reported Loss to follow‐up: 32 participants were lost to follow‐up. There was some indication of differential loss to follow‐up across arms (21%, 15%, and 7% respectively for CLVR, ELVR, and CELVR); reasons for loss to follow‐up were distributed similarly in all groups. Follow‐up: 12 months after baseline (6‐9 months maintenance effect) |
|
| Participants | Country: United Kingdom Inclusion period: Nov. 1997 ‐ Aug. 1999 Number randomised: 226 Number analysed: 194 Age: median 81 years Sex: female 150 (66.4%) Eye disorder(s): AMD VA: mean logMAR VA 0.77 Inclusion criteria: (1) newly referred to low vision clinic; (2) primary diagnosis of AMD; (3) VA worse than 6/18 (> 0.5 logMAR) in both eyes and equal or better than 1/60 (=< 1.8 logMAR) in the better eye Exclusion criteria: (1) living in a residential or a nursing home; (2) suffering from mental illness of dementia; (3) not proficient in English |
|
| Interventions | 1) Treatment: conventional low vision rehabilitation (CLVR) provided by the hospital eye service. Follow‐up contact at appr. 3 months. 2) Treatment: enhanced low vision rehabilitation (ELVR): CLVR enhanced with home visits from a rehabilitation officer for the visually impaired. Follow‐up contact at appr. 4‐6 months 3) Control: controlled trial arm for additional contact time (CELVR): CLVR supplemented with home visits, from a community care worker, which did not include rehabilitation (CELVR). Follow‐up contact at appr. 4‐6 months | |
| Outcomes | ‐ VCM1: VRQOL core measure
‐ SF‐36: physical and mental component summary score HRQOL
‐ NAS: Nottingham Adjustment Scale ‐ Measured task performance ‐ LVA (Low Vision Aid) use |
|
| Notes | ‐ All SMDs for each outcome measure were reported in 3 ways: ELVR vs CLVR, ELVR vs CELVR, CELVR vs CLVR. No standard deviations were reported. ‐ Funding: North West Regional Health Authority; Manchester Royal Eye Hospital Research Endowment Fund, UK ‐ Declaration of interest: the authors declared that they had no conflict of interest. ‐ Adverse events: not reported ‐ Data obtained from authors after personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A blocked randomisation procedure was used with blocks of unequal length. |
| Allocation concealment (selection bias) | Low risk | Allocation codes were generated by the computer before the start of the study and were concealed in sealed opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Allocation secret to researcher who measured the outcomes, however, 5% were guessed correctly by the outcome assessor; this did not influence the measured effects. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intention‐to‐treat analyses with a low dropout rate of approximately 14.4% after 1 year, however different across arms |
| Selective reporting (reporting bias) | Low risk | Protocol available (Russell 2001); all outcomes were reported in a prespecified way. Only costs were not analysed. |
Rovner 2007.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to investigate effects of problem‐solving treatment in preventing depressive disorders in AMD participants Exclusions after randomisation: none reported Loss to follow‐up: 17 participants dropped out of the study (9 treatment, 3 control). Follow‐up: 2 and 6 months after baseline (appr. 4 month maintenance effect) |
|
| Participants | Country: USA Inclusion period: Dec 2001 ‐ Jul 2005 Number randomised: 206 Number analysed: 204 (2 months), 190 (6 months) Age: mean years 81.2 Sex: female 144 (69.9%) Eye disorder(s): AMD VA: mean logMAR VA 0.6 Inclusion criteria: 1) ≧ 64 years; 2) having neovascular macular degeneration in one eye diagnosed within the preceding 6 months and preexisting AMD in the fellow eye Exclusion criteria: 1) DSM‐IV diagnosis of a depressive disorder or current treatment for depression; 2) cognitive impairment; 3) other eye conditions |
|
| Interventions | 1) Problem‐solving treatment (PST): teaching problem‐solving skills, in addition to care‐as‐usual. Six PST sessions, provided by trained therapists, at participant's home, with a duration of 45‐60 minutes, for a period of 8 weeks. PST group also received care‐as‐usual from their ophthalmologists and/or other health care providers. 2) Control: usual care, provided by ophthalmologist or other health care providers |
|
| Outcomes | DSM‐IV diagnosis of depression (primary outcome) HDRS: Hamilton Depression Rating Scale, depressive symptoms VA Contrast sensitivity NEI VFQ‐17: National Eye Institute Visual Functioning Questionnaire |
|
| Notes | ‐ Study and its belonging effects also reported as Rovner 2008, however, publication of 2007 provided more information about the study design. ‐ Mixed effects model used to analyse data ‐ Funding: National Institute for Mental Health; National Eye Institute; Farber Institute for Neurosciences of Thomas Jefferson University, USA ‐ Declaration of interest: the authors declared that they had no financial interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table and a fixed randomisation scheme with a permuted random block design |
| Allocation concealment (selection bias) | Low risk | Random numbers table and sealed envelopes containing treatment assignments were used. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were unaware of the participant's treatment assignment; 18% of the participants revealed their allocation to the assessor, but no difference was found in the presence of depression. This indicated that no significant bias could be detected. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ Intention‐to‐treat analyses on available cases ‐ Dropout rate of 8.3% seemed low; large sample size ‐ However, sample size calculation was not reported. |
| Selective reporting (reporting bias) | Unclear risk | ‐ Trial registration available ‐ 12 months follow‐up seemed to not have been reported, however, 6 months follow‐up showed no effect. |
Rovner 2013.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms aiming to compare the immediate and longer term efficacy of problem‐solving therapy (PST) with supportive therapy to improve 'targeted visual functioning' and VRQOL for AMD participants Exclusions after randomisation: none Loss to follow‐up: 26 Follow‐up: 3 and 6 months after baseline, appr. 4 months maintenance effect |
|
| Participants | Country: USA Inclusion period: Oct 2006 ‐ Feb 2010 Number randomised: 241 Number analysed: 228 at 3 months and 215 at 6 months Age: mean: 82 years Sex: female 63.5% Eye disorder(s): AMD, 87.6% neovascular disease; remainder had bilateral geographical atrophy VA: mean logMAR distance acuity: 0.58, mean logMAR near: 0.62 Inclusion criteria: 1) people from retina clinics associated with Wills Eye Institute in Philadelphia; 2) ≧ 65 years; 3) bilateral AMD (neovascular and/or geographic atrophy); 4) best‐corrected VA between 20/70 and 20/400 inclusive in the better‐seeing eye and no lower acuity limit in the fellow eye and 5) moderate difficulty in ≧ 1 valued vision‐function goal (e.g. reading mail, attending social activities) Exclusion criteria: 1) presence of uncontrolled glaucoma, DR or planned cataract surgery within 6 months; 2) cognitive impairment on an abbreviated version of the Mini‐Mental Status Examination that omitted vision‐dependent items; 3) presence of a medical condition that would preclude participation and 4) residence in a skilled nursing facility |
|
| Interventions | 1) Intervention: problem‐solving therapy teaches problem‐solving skills in a structured way to enable a participant to identify his problems, generate and select a solution. PST therapist and participants discussed their functional problems due to their vision loss and used problem‐solving steps to reduce difficulties. The training programme consisted of workshops, review and discussion of the treatment manuals and supervision of 5 training cases at the participant's home. 2) 'Placebo': supportive therapy is a standardised psychological treatment. It is nondirective and supportive. The ST therapists informed participants that its purpose was to explore the impact of vision loss on their lives. In contrast with PST, there was no discussion of vision function goals, problem‐solving or low vision rehabilitative strategies. The training programme consisted of workshops, review and discussion of the treatment manuals and supervision of 5 training cases at the participant's home. |
|
| Outcomes | TVF: Targeted Vision Function (primary outcome) NEI VFQ 25 + supplement: National Eye Institute Visual Functioning Question AI: Massof's activity inventory Physical health status: chronic disease score PHQ: Patient Health Questionnaire, depression |
|
| Notes | ‐ Behaviour Activation for Depression Scale (BADS) only reported in protocol. ‐ Interventions were well‐protocolised and checked for fidelity. ‐ Appropritate statistical methods used, i.e. mixed‐effect and other longitudinal models. ‐ Funding: National Eye Institute, USA ‐ Declaration of interest: the authors declared that they had no financial, proprietary or commercial interest. ‐ Adverse events: not reported ‐ Means and SDs of trial arms obtained through personal communication with Dept of Ophthalmology VUmc |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table,with a permuted random block design, stratified by severity of AMD |
| Allocation concealment (selection bias) | Low risk | Serially numbered, sealed, opaque envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The research nurse who performed the interviews was masked to the treatment assignment. The authors reported that she became unmasked to 9 participants who revealed their allocation. This seemed like a slight detection bias, however, not significant enough to influence data |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ 26/241 participants were lost to follow‐up (11%). ‐ Sample size requirements were clear (200 + 20% to account for loss to follow‐up). Intention‐to‐treat analyses |
| Selective reporting (reporting bias) | Low risk | Study protocol was available; outcomes were measured in prespecified way, although some measures were excluded in this study. E.g. BADS was not taken into account in the full report; instead it was reported as a primary and secondary control scale. Furthermore, general QOL measured by MOS‐6 was not (yet) reported. |
Rovner 2014.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms comparing behavioural activation plus low vision rehabilitation versus supportive therapy in addition to low vision rehabilitation to investigate its effectiveness in reducing depression Exclusions after randomisation: none Loss to follow‐up: 25 (13%) Follow‐up: 4 months after baseline, 2 months maintenance effect |
|
| Participants | Country: USA Inclusion period: Jul. 2009 ‐ Feb. 2013 Number randomised: 188 Mean age: 84 years (SD 7.0) Sex: female 70% Eye disorder(s): AMD VA: best eye < 20/70 Inclusion criteria: age > 65 years, bilateral AMD, best‐corrected VA < 20/70 in the better seeing eye, > 5 antiangiogenic injections if the better eye had neovascular disease, or no injections in the previous 3 months, moderate difficulty performing a valued vision‐dependent activity, and subthreshold depressive symptoms (PHQ‐9 score > 5), or depressed mood or anhedonia several days per week Exclusion criteria: ongoing or anticipated antiangiogenic treatment, current DSM IV‐defined depressive disorder, uncontrolled glaucoma, DR, corneal dystrophy or anticipated cataract surgery, and screener‐based cognitive impairment |
|
| Interventions | 1) Treatment: in home behavioural activation which focuses on targeting behaviours that might maintain/worsen depression (six in home 1‐hour sessions over 8 weeks, offered by 1 of 5 occupational therapists) + low vision rehabilitation 2) Control: in‐home supportive therapy (similar in dose and intensity) controlling for the nonspecific effects of attention + low vision rehabilitation |
|
| Outcomes | Primary outcomes: PHQ‐9: Patient Health Questionnaire; 9 items for depressive disorder. NEI‐VFQ: National Eye Institute Visual Function Questionnaire for mental health (subscale) Secondary outcomes: AI: Activity Inventory NEI‐VFQ‐25 plus: National Eye Institute Vision Function Questionnaire–25 plus Supplement and NEI‐VFQ QOL |
|
| Notes | Trial Register: NCT00769015 ‐ Small baseline imbalances found; no difference between responders and non‐responders ‐ Funding: National Eye Institute, USA ‐ Declaration of interest: the authors declared that they had no proprietary or commercial interest. ‐ Adverse events: not reported ‐ Means and SDs of trial arms obtained through personal communication with Dept. of Ophthalmology VUmc ‐ Data obtained from authors after personal communication ‐ Participants in both study arms received an incentive of 350 USD for a basic set of optical devices. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A random numbers table was used by an independent statistician. |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes were used; allocation was done with a 1:1 ratio and stratification to severity of vision loss. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Independent and masked research assistants administering questionnaires at participants' homes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low dropout rate (13%); high power |
| Selective reporting (reporting bias) | Low risk | Trial registration and protocol available; all predefined outcomes were reported. |
Rumrill 1999.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with 2 arms aiming to describe the effects of an expanded 'Three I' training programme for employed people with visual impairment and blindness Exclusions after randomisation: none reported Lost to follow‐up: 2 Follow‐up period: 16 weeks: 8‐week maintenance effect after an 8‐week 'follow along' visit |
|
| Participants | Country: USA Inclusion period: not reported Number randomised: 48 Number analysed: 46 Age: mean: 43.6 years (range 16‐69) Sex: female 64.6% Eye disorder(s): not reported VA: 17% totally blind; 54% legal blindness: VA range 20/200‐20/800; and 29% visual impairment: VA range 20/80‐ 20/200 Inclusion criteria: not reported Exclusion criteria: not reported |
|
| Interventions | 1) Three I intervention: two sessions and one follow along visit after 8 weeks, training by a rehabilitation professional: participants were assisted in 1) identifying their needs for reasonable accommodations, receiving detailed information about 'Title I' provision and national accomodation resources. Participants completed an intensive social competence and self‐advocacy programme including role play to develop skills in requesting on‐the‐job accommodations from their employers. 2) Control: waiting list control |
|
| Outcomes | Accomodation self‐efficacy Accomodation activity Americans with Disabilities Act knowledge Work Experience Survey |
|
| Notes | ‐ Only employed adults ‐ Post‐test only: no interpretation of enhancement in comparison to before intervention possible ‐ Matching was used; when one participant dropped out, the other matched participant was also excluded. ‐ No mixed effects models used. Instead it was stated that paired t‐tests were used to compare differences between groups, which should be independent samples t‐tests. ‐ Funding: Research and Creativity Award from the Kent State University Research Council, USA ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Matching procedure used by the researcher to pair participants according to age, gender and degree of visual impairment; matched pairs were randomised. |
| Allocation concealment (selection bias) | Unclear risk | Not reported, insufficient information to permit judgement |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Rehabilitation professional providing training also completed outcome interviews. This indicated an 'unblinded' situation. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ‐ Disadvantage of matching was that when 1 participant dropped out, the other matched participant was not analysed; this happened once (slight deviation from intention‐to‐treat analysis). ‐ Small sample (requirements unknown) ‐ Post‐test only |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
Scanlan 2004.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to determine the outcomes of a low vision service assisting participants with AMD to use low vision devices and by giving them an extended period of education. Exclusions after randomisation: none reported Loss to follow‐up: deteriorating vision participants were replaced to maintain sample size. Follow‐up: 12 weeks after baseline, with a maintenance effect of 7 weeks |
|
| Participants | Country: Canada Inclusion period: not reported Number randomised: 64 Number analysed: 64 Age: mean: 81 years Sex: female 64.1% Eye disorder(s): AMD, newly referred by ophthalmologist or optometrist Inclusion criteria: 1) diagnosis of AMD, 2) BCVA in the better eye of 20/60 to 20/400, 3) relatively good health and 4) sufficient motivation to participate in the study Exclusion criteria: not reported |
|
| Interventions | 1) Intervention: extended teaching programme in reading with microscopes, consisting of five one‐hour sessions at the low vision clinic. There was also a focus on activities of daily living. 2) Control: traditional teaching session of one hour in reading with microscopes at the low vision clinic. |
|
| Outcomes | NEI‐VFQ: National Eye Institute Visual Functioning Questionnaire, separate items Pepper Visual Skills for Reading Test: reading ability |
|
| Notes | ‐ Relatively small sample, sample size calculation unclear ‐ Participants who suffered a significant vision loss during the study were removed from the study and additional clients were recruited to ensure that there were 32 participants in each group. ‐ Seemed as if mixed models were used to analyse data ‐ VRQOL outcome was validated but not used as such since only a selection of items of NEI VFQ were used. ‐ Funding: not reported ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation not described |
| Allocation concealment (selection bias) | Unclear risk | Randomly allocated using concealed assignment; not further explained in which way |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants due to rehabilitation programmes that were recognisable. In addition, the low vision rehabilitation (LVR) worker was aware of the allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | LVR worker administered the outcome measures and was aware of the allocation. In addition, he was the same person who gave the treatment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | ‐ No intention‐to‐treat analyses: participants with deteriorated vision were replaced |
| Selective reporting (reporting bias) | Unclear risk | ‐ Study protocol was not available to identify any other unreported outcomes ‐ Not all subscales of NEI VFQ reported, only some items |
Seiple 2011.
| Methods |
Intervention type II: methods of enhancing vision A multicentre study of reading rehabilitation in macular disease comparing different reading strategy training to a waiting list control group in a cross‐over trial (excluding the waiting list) Exclusions after randomisation: none reported Loss to follow‐up: none reported Follow‐up: 18 weeks after baseline (direct effect) |
|
| Participants | Country: USA Inclusion period: Number randomised: 36 Number analysed: 36 Age: median 79 years (intervention group, N = 30), mean 78.5 (controls, N = 6) Sex: female 50% (in intervention group, for controls unknown) Eye disorder(s): AMD VA: mean 0.8 logMAR Inclusion criteria: diagnosis of dry nonexudative AMD and VA greater than 20/400 in the better eye Exclusion criteria: other major ophthalmologic or neurologic disease, choroidal neovascularisation as a result of wet AMD, moderate to severe media opacities, and cognitive impairment |
|
| Interventions | Reading rehabilitation training exercises were derived from the literature and from the laboratory’s curriculum: 1) Visual awareness and eccentric viewing 2) Control of reading eye movements 3) Reading practice with sequential presentation of lexical information 4) Control group: delayed treatment for 18 weeks |
|
| Outcomes | Reading performance, VRQOL, HRQOL, depressive symptoms, adaptation to vision loss | |
| Notes | ‐ Clinical Trials register: NCT00746668 and ClinicalTrials.gov number: NCT00125632 ‐ Funding: US Veterans Administration Rehabilitation Research and Development, The Foundation Fighting Blindness, and Hope for Vision ‐ Declaration of interest: the authors declared that they had no conflict of interest. ‐ Adverse events: not reported ‐ Fewer participants included than was aimed for in the original protocol: power could be an issue and control group was very small. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | A research associate masked to the training module order administered the reading assessment battery, for the questionnaire assessment; this was not reported clearly. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No attrition, but power could be an issue (e.g. control group was small). |
| Selective reporting (reporting bias) | Unclear risk | In the protocol, other outcome measures were reported as well, such as HRQOL and adaptation to vision loss. The publication reported on visual functioning items in addition to the main outcome. |
Smith 2005.
| Methods |
Intervention type II: methods of enhancing vision RCT with 3 arms aiming to investigate the effectiveness of prism spectacles in people with AMD Exclusions after randomisation: not reported Loss to follow‐up: 18 (10 custom, 6 standard, 2 placebo) Follow‐up: 3 months after baseline, maintenance effect of prescription of prisms |
|
| Participants | Country: United Kingdom Inclusion period: Jul. 2001 ‐ Mar. 2003 Number randomised: 243 Number analysed: 225 Age: median age 81 years Sex: female 64.6% Inclusion criteria: 1) referred to low vision clinics of hospital; 2) bilateral AMD; 3) VA of at least 1/60 (1.78 logMAR) but no better than 6/18 (0.48 logMAR) in the better eye; 4) free of mental illness, dementia and severe physical limitations; 5) proficient in English and literate; 6) not a resident in a hospital or a nursing home Exclusion criteria: 1) resident in a hospital or nursing home; 2) Mini‐Mental State Examination score < 16 out of 22 |
|
| Interventions | 1) Custom treatment: incorporating bilateral prisms to match participants' preferred power and base direction 2) Standard treatment: incorporating standard bilateral prisms (6 prism diopters base for logMAR VA of 0.48‐1.00 and 10 diopters base for logMAR VA of 1.02‐1.68) 3) Control: placebo, consisting of spectacles matched in weight and thickness to prism spectacles but without the prism | |
| Outcomes | logMAR VA MNRead: Reading speed performance NEI‐VFQ‐25: National Eye Institute visual functioning questionnaire, 9 items Melbourne Low Vision ADL Index (MLVAI) part I & II: activities of daily living performance Manchester Low Vision Questionniare (MLVQ): helpfulness and use of test spectacles |
|
| Notes | ‐ ANCOVA analyses corrected for baseline outcomes ‐ No SDs reported ‐ Funding: The Health Foundation, UK ‐ Declaration of interest: the authors declared that they had no financial interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation codes prepared in advance |
| Allocation concealment (selection bias) | Low risk | Randomisation and the ordering of spectacles were performed by a principal investigator who had no contact with participants during the study. Dispensing opticians were aware that participants must not find out their group allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | It was a placebo‐controlled trial. The participants were masked. Randomisation and the ordering of spectacles were performed by a principal investigator who had no contact with participants during the study. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The investigators who collected all outcome data were masked to the treatment allocations. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ Intention to treat analyses ‐ 7% lost to follow‐up, no difference in numbers for loss to follow‐up between groups |
| Selective reporting (reporting bias) | Unclear risk | No protocol available; unclear if all outcome measures were used in a predefined way |
Stelmack 2008.
| Methods |
Intervention type III: multidisciplinary rehabilitation programmes RCT with two arms aiming to evaluate the effectiveness of an outpatient low vision rehabilitation programme for veterans with moderate and severe vision loss due to macular diseases LOVIT I: Low Vision Intervention Trial Exclusions after randomisation: 2 persons from the treatment group did not receive low vision rehabilitation as assigned and withdrew consent. Loss to follow‐up: 7 persons from the treatment group discontinued study prior to completion of low vision rehabilitation. Follow‐up: 4 months for QOL after baseline appr. two weeks after intervention (direct), 2 months follow‐up for reading outcomes |
|
| Participants | Country: USA Inclusion period: Nov. 2004 ‐ Jul. 2006 Number randomised: 126 Number analysed: 117 Age: mean 78.9 years Sex: male 98% Eye disorder(s): macular degeneration, macular dystrophy, macular hole, or inflammatory disease of the macula VA: mean logMAR VA 1.1 Inclusion criteria: (1) primary eye diagnosis in the better‐seeing eye of macular degeneration, macular dystrophy, macular hole, or inflammatory disease of the macula; (2) VA in the better‐seeing eye worse than 20/100 and better than 20/500; (3) eligibility for VA benefits Exclusion criteria: (1) no access to telephone; (2) inability to speak English; (3) previous recipient of comprehensive low vision services; (4) English literacy less than fifth‐grade level; (5) Telephone Interview for Cognitive Status score of 30 or lower; (6) history of stroke with aphasia; (7) other health condition that would preclude follow‐up; (8) inability or unwillingness to attend clinic visits required for the study; (9) severe hearing impairment that interferes with participation in telephone questionnaires; (10) vitreous haemorrhage, serious or hemorrhagic detachment of the macula, clinically significant macular edema, or cystoid macular edema; (11) cataract extraction planned within the next 6 months |
|
| Interventions | 1) Treatment: 5 weekly sessions (approximately 2 hours per session) at the low vision clinic to learn strategies for more effective use of remaining vision and use of low vision devices. In addition, 1 home visit was provided to teach environmental adaptations and to set up low vision devices so that participants could practice using them in their homes. Each participant was assigned 5 hours of homework per week after each therapy session to practice performing everyday tasks. 2) Control: treatment was delayed for 4 months. Participants received bimonthly telephone calls from the low vision therapists during the 4 months they were waiting. The purpose of these calls was to keep participants engaged in the study to present attrition and to report adverse events. |
|
| Outcomes | Veterans Affairs Low Vision Visual Functioning Questionnaire‐48: change in visual reading ability (primary outcome) Other domains of VA LV VFQ‐48 :mobility, visual information processing, visual motor skills and overall visual ability SF‐36: HRQOL CES‐D: depressive symptoms |
|
| Notes | ‐ Generalisability: mostly male participants (98%); slight imbalance in reading ability between study arms ‐ No mixed models were used. Instead of that, paired t‐tests were conducted. ‐ Also 1‐year follow‐up results have been reported by the authors (Stelmack 2012). However, participants in the control group also received a rehabilitation programme after the four months waiting list. In the follow‐up study, both arms were treated as separate cohorts. These additional analyses were not according to the protocol and were therefore not reported in the current review. ‐ SMDs reported slightly deviate from effect sizes in the review due to different analyses strategy. ‐ Funding: Department of Veterans Affairs Rehabilitation Research and Development, Department of Veterans Affairs Prosthetics Service (low vision aids) ‐ Declaration of interest: the authors reported none. ‐ Adverse events: no (serious) adverse events were judged to be related to the study. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | ‐ A computer‐generated allocation schema based on permuted blocks of random sizes ‐ Randomisation was stratified by distance VA less than 20/500 to 20/250 and better than 20/250 but less than 20/100, and by study site. |
| Allocation concealment (selection bias) | Low risk | A co‐ordinating centre staff member communicated each participant's assignment to the sites by telephone. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Interviewer was masked. In addition, participants were informed not to reveal their allocation. No disclosures were tracked. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | ‐ Intention‐to‐treat analyses performed in addition to as‐treated analyses ‐ Low dropout rate (7%); however dropout was only in the treatment group. |
| Selective reporting (reporting bias) | Low risk | Protocol available; all outcomes were measured in prespecified way. |
Stelmack 2017.
| Methods |
Intervention type II: methods of enhancing vision RCT with two arms aiming to determine the value of adding low vision rehabilitation with a therapist to low vision aids compared with low vision aids provision without intervention for veterans with macular diseases LOVIT II: Low Vision Intervention Trial Exclusions after randomisation: none Loss to follow‐up: N = 19 (6%) Follow‐up: 4 months after baseline, appr. 3 to 3.5 months maintenance effect |
|
| Participants | Country: USA Inclusion period: Sep. 2010 ‐ Jul 2014 Number randomised: N = 323 Number analysed: N = 323 Age: mean 80 years (SD 10.5) Sex: male 314 (97%) Eye disorder(s): macular diseases VA: mean logMAR 0.6 (SD 0.2) Inclusion criteria: eligible for VA benefits, diagnosis of any macular disease, and BCVA better‐eye of 20/50 to 20/200 Exclusion criteria: no access to telephone, adequate English level, no vision loss since previous low vision rehabilitation, cognitively unable, unable or unwilling to attend clinic visits, hearing impairment that interferes with telephone questionnaires, visual field better‐eye less than 20° in diameter, vitreous haemorrhage affecting line of sight, cataract extraction planned within 4 months, receiving macular disease treatment expected to improve vision, participating in another study that does not allow dual enrolment |
|
| Interventions | 1) Treatment: low vision devices with a rehabilitation therapist providing instruction and homework on the use of low vision devices, eccentric viewing, and environmental modification 2) Control: receiving low vision devices with no therapy |
|
| Outcomes | Primary outcomes: VA‐VFQ: Veterans Affairs Low Vision Visual Functioning Questionnaire for VRQOL on 4 functional domains (reading, visual information, visual motor, and mobility) MNREAD: reading speed, critical print size, and reading acuity SF‐36: Short Form‐36 for HRQOL EQ‐5D: Euroqol‐5 dimensions for HRQOL |
|
| Notes | ‐ Trial registration: NCT00958360 ‐ Funding: Department of Veterans Affairs Rehabilitation Research and Development grant; Department of Veterans Affairs Prosthetics Service (for low vision services provided to participants) ‐ Declaration of interest: authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported. ‐ Adverse events: eleven adverse events unrelated to the intervention were reported. ‐ Means and SDs of trial arms obtained through personal communication with Dept. of Ophthalmology VUmc ‐ Data obtained from authors after personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The co‐ordinating centre created a computer‐generated permutated block randomisation with random block sizes. |
| Allocation concealment (selection bias) | Low risk | Study site co‐ordinators received assignments from the online randomisation system and informed participants and clinical staff of the treatment assignments. Preplanned stratification was by participating site and BCVA better‐eye (20/50 to 20/63 and worse than 20/63 to 20/200). |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Certified and masked interviewers read a script to inform participants that questionnaire responses and treatment assignments were anonymous and confidential. Outcomes data were not shared with investigators or clinical staff until the study's end. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low attrition rate (6%); intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Low risk | Protocol available and predefined outcomes were reported. |
Sun 2012.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms to observe the influence on the psychological condition of participants with glaucoma after psychological therapy versus physical therapy in a clinical (hospital) setting Exclusions after randomisation: none Loss to follow‐up: none Follow‐up: 6 months after baseline, direct effect |
|
| Participants | Country: China Inclusion period: 2009 ‐ 2010 Number randomised: 100 Mean age: 62 years, range 25‐75 years Sex: not reported Eye disorder(s): glaucoma VA: not reported Inclusion criteria: first time diagnosis of glaucoma Exclusion criteria: not reported |
|
| Interventions | 1) Intervention: psychological therapy, however, specific content unclear (during 6 months, number of sessions unclear; provided by psychiatrists and specialist nurses) + physical therapy by an ophthalmologist 2) Control: physical therapy, however, specific content unclear |
|
| Outcomes | SDS: Self‐rating Depression Scale SAS: Self‐rating Anxiety Scale SCL‐90: Symptom CheckList 90 items for personality domains | |
| Notes | ‐ Funding: not reported ‐ Declaration of interest: not reported ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants enrolled in the trial provided outcome data, there was no attrition. |
| Selective reporting (reporting bias) | Unclear risk | No protocol available |
Taylor 2017.
| Methods |
Intervention type II: methods of enhancing vision Randomised cross‐over trial studying the (cost) effectiveness of portable electronic in addition to optical magnifiers for near vision activities Exclusions after randomisation: none Loss to follow‐up: 18 Follow‐up: 2 and 4 months after intervention's active use (direct effect) |
|
| Participants | Country: United Kingdom Inclusion period: between May 2013 and Nov 2014 Number randomised: 100 Mean age: 71 years Sex: female 62% Eye disorder(s): AMD (61%), other (39%) VA: mean binocular distance VA 0.96 Inclusion criteria: (1) adults 18+ years, (2) using optical devices only, (3) stable visual impairment, (4) BCVA > 0.7 logMAR and/or log contrast sensitivity 1.2 or worse, (5) adequate hearing, (6) English speaking Exclusion criteria: (1) physical disability preventing operating electronic device, (2) cognitive impairment |
|
| Interventions | 1) Treatment: portable electronic device on top of nonelectronic optical devices 2) Control: nonelectronic optical devices |
|
| Outcomes | Primary outcomes: Reading measurements: MNRead, frequency of device usage, MLVQ, IReST Secondary outcomes: 5‐TIADLs: instrumental activities of daily living NV‐VFQ‐15: near vision items of the VFQ‐48 EQ‐5D: HRQOL VISQOL WHO‐5: well‐being Economic evaluation: cost‐effectiveness and cost‐utility analyses from a societal perspective |
|
| Notes | Stratification: age and VA Trial identifier: NCT01701700 Analyses: (mixed effect) linear models, t‐tests to account for treatment, period and carry‐over effects Funding: National Institute of Health Research ‐ Research for Patient Benefit programme Conflict of interest: authors reported no conflicts of interest and had no proprietary interest in the optical devices. Adverse events: not reported Data obtained from authors after personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not clear how sequence generation took place |
| Allocation concealment (selection bias) | Unclear risk | Not clear how allocation was concealed |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Study researcher was masked to group allocation when baseline assessments were carried out, but not at subsequent measurements. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition slightly higher than expected (18%), however, no indication that it had an effect on power |
| Selective reporting (reporting bias) | Low risk | Protocol paper and trial registration available, no deviations from protocol |
Tey 2019.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms to compare a self‐management programme 'living successfully with low vision', with usual care (low vision aid training) Exclusions after randomisation: 27 Loss to follow‐up: 37 (22%) Follow‐up: 2 weeks and 6 months post‐intervention as a maintenance effect |
|
| Participants | Country: Singapore Inclusion period: Jan 2013 and Jul 2015 Number randomised: 165 Mean age: 60.2 (SD 11.3) Sex: female 36.2% Eye disorder(s): glaucoma (20%), DRP (20%), RP (12.5%), pathologic myopia (10%), other (37.5%) VA: mean 0.73 logMAR (SD 0.36) Inclusion criteria: English or Mandarin speaking; > 21 years; low vision (VA =< 6/12 to >= 6/480 in the better eye after best correction or central scotoma or visual field loss < 20 degrees); able to participate in normal conversation and free of cognitive impairment (6‐item Cognitive impairment test); living independently in the community |
|
| Interventions | 1) Low vision self‐management programme on top of usual care in which participants picked a goal they wished to achieve, focus on learning process of new techniques to enhance activities of daily living, providing information, exploring experiences with low vision and developing problem‐solving skills including positive self‐talk, use of other senses (touch and hearing). Four times 3.5‐hour weekly group sessions (6‐8 participants) for sharing and practicing ADLs 2) Usual care: standard ophthalmologic care and low vision aid training and referral to occupational or mobility training at the participant's request |
|
| Outcomes | Primary outcome: IVI‐28: VRQOL Secondary outcomes: DASS: mental health and emotional distress including depression, anxiety and stress GSES: self‐efficacy EQ‐5D and SF‐12: HRQOL |
|
| Notes | Clinical Trial register: NCT01879501 ‐ Funding: Ministry of Health (Singapore) ‐ Health Services Research Grant [nr 0026/2012]. They had no role in any part of the study. ‐ Declaration of interest: authors disclosed no conflict of interest. ‐ Adverse events: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Telephone randomisation by a consent‐taking research officer calling a separate randomisation officer for treatment allocation linked to a participant's ID |
| Allocation concealment (selection bias) | Low risk | Allocation concealment by an independent research officer |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Treatment allocation was masked for the outcome assessor. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low attrition rate compared to baseline measurements (2%) but higher compared to numbers randomised (22%) |
| Selective reporting (reporting bias) | High risk | Some other criteria were used in the outcome report compared to the trial protocol (age, eye disorder, visual field, hearing loss, follow‐up time; measurement instruments were not specified in protocol). |
Van der Aa 2015.
| Methods |
Intervention type I: psychological therapies and/or group programmes RCT with two arms to compare stepped‐care with usual care for preventing the onset of major depressive, dysthymic and anxiety disorders in older people with visual impairment and subthreshold depression and/or anxiety in a low vision rehabilitation setting Exclusions after randomisation: 5 no show Loss to follow‐up: 34% after 2 years Follow‐up: 3, 6, 9, 12, 18, 24 months after baseline, at least 12 months maintenance effect |
|
| Participants | Country: Netherlands and Belgium Inclusion period: Jul. 2012 ‐ Apr. 2013 Number randomised: 265 Mean age: 74 years Sex: female 185 (70%) Eye disorder(s): 46% AMD, 17% glaucoma, 3% DR, 6% CVA, 40% other VA: 91% logMAR > 0.3 Inclusion criteria: decimal VA of ≤ 0.3 and/or a visual field of ≤ 30° around the central point of fixation and/or an evident request for help for which options in regular ophthalmic practice are not adequate, such as contrast sensitivity or glare, having subthreshold depression and/or anxiety (HADS‐A score ≥ 8 and/or CES‐D score ≥ 16); speak Dutch language adequately Exclusion criteria: meeting the diagnostic criteria of a major depressive, dysthymic, and/or anxiety disorder according to the DSM‐IV measured with the Mini International Neuropsychiatric Interview (MINI), severe cognitive impairment (short screener) |
|
| Interventions | 1) Intervention: stepped‐care (+ usual care) by supervised occupational therapists, social workers, and psychologists from low vision rehabilitation organisations who delivered the programme, which comprised watchful waiting, guided self‐help based on cognitive behavioural therapy, problem‐solving treatment, and referral to a GP. Participants moved to the next step in the care programme if the former step did not sufficiently diminish depressive and/or anxiety symptoms under cut‐off. 2) Control: usual care by rehabilitation centre or any other healthcare service |
|
| Outcomes | Primary outcome: Cumulative incidence of depression and anxiety disorder after 24 months measured with the MINI diagnostic interview (including measurements at 3, 6, 9, 12, 18 and 24 months) Secondary outcomes: CES‐D HADS‐A LVQOL for VRQOL EQ‐5D for HRQOL depression and anxiety symptoms, VRQOL, HRQOL AVL: Adaptation to age‐related vision loss questionnaire Cost‐effectiveness |
|
| Notes | ‐ Netherlands trial register: NTR3296 ‐ Funding: ZonMw InZicht, the Dutch Organisation for Health Research and Development‐InSight Society, the Netherlands ‐ Declaration of interest: All authors completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declared: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. ‐ Adverse events: no (serious) adverse events, however, participants with a study diagnosis of major depression (study end point) were sent to their GP according to protocol. ‐ Participants who volunteered for joining the study might have differed from other eligible individuals, i.e. responders were younger and had fewer cognitive and physical problems and might have better access to health care. ‐ Dropout rates were higher than expected, therefore, more participants were recruited. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation based on computerised random number generator, performed by an independent researcher. The scheme was based on blocks of two and stratified by 17 locations of three outpatient low vision rehabilitation organisations in the Netherlands and Belgium. |
| Allocation concealment (selection bias) | Low risk | Only when guidance needed to be offered in step two or three of the programme were the clinical staff directly informed by the independent researcher as to which participant to treat. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme. Participants were registered as being a participant of the study in their records at the rehabilitation centres. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | At the outset of the study and at the start of each telephone interview, participants were told not to reveal the nature of their treatment. Masking was guessed correctly in 38% of cases by independent interviewers, indicating that masking was effective. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Loss to follow‐up, and reasons for loss to follow‐up were similar for the control group and the intervention group: N = 45 in the intervention group lost to follow‐up, N = 46 in the usual care group. |
| Selective reporting (reporting bias) | Low risk | Study protocol was available and all prespecified outcomes of interest were reported in a prespecified way. |
Waterman 2016.
| Methods |
Intervention type IV: other programmes Three‐arm RCT comparing social visits, a home safety programme and a home safety plus home exercise programme in order to prevent falls in visually impaired persons Exclusions after randomisation: none Loss to follow‐up: 6 Follow‐up: 3 and 6 months (direct effect considering the contact that was kept in the extended programme) |
|
| Participants | Country: United Kingdom Inclusion period: Mar ‐ Oct 2012 Number randomised: 49 Mean age: 81 years, range 65‐96 Sex: females 65% Eye disorder(s): 57% AMD VA: mean logMAR between 1.05 and 1.17 Inclusion criteria: (1) BCVA > 0.6 and/or moderate visual field loss, (2) 65 years or older, (3) independently living in the community, (4) able to walk in their residence, (5) cognitively able to participate Exclusion criteria: (1) receiving occupational therapy, physiotherapy, or exercise interventions |
|
| Interventions | 1) Treatment: home safety programme by occupational therapist visiting twice and making safety modifications plus one phone call 2) Treatment: home safety plus home exercise programme stressing strength and balance, at least 3 times every week for 30 min, walking twice per week by occupational therapists who visited two times, the peer mentors three times and phoned twice 3) Control: usual care from NHS three social visits, two telephone calls by trained lay visitors/volunteers |
|
| Outcomes | Primary outcomes: Falls and injurious falls Physical activity Secondary outcomes: SF‐12: QOL VCM1: visual disability, VRQOL AFRIS Short FES‐I: fear of falling, falls self‐efficacy Economic evaluation: direct and indirect costs |
|
| Notes | Analysis: General linear mixed models Adverse events: There were no serious adverse events related to the study. Funding: National Institute of Health Research ‐ Research for Patient Benefit programme Conflict of interest: two authors are directors of a not‐for‐profit training company. Other authors reported no conflict of interest. Note: Due to low response, aimed sample size of N = 193 not reached, therefore not powered for significant results |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Via a web‐based secure randomisation service |
| Allocation concealment (selection bias) | Low risk | Clinical trial unit allocated group assignment. Baseline imbalance for gender and psychotropic drug use |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Impossible to mask participants and providers of the programmes due to recognisability of the rehabilitation programme |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Research assistant and statistician were masked to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intention‐to‐treat analysis, relatively low attrition rates (12%) |
| Selective reporting (reporting bias) | Unclear risk | Trial registration, protocol available but retrospectively registered |
ABWA: Association for the Blind of Western Australia ACS: activity card sort ADL: activities of daily living ADS‐L: Allgemeinen Depressionsskala ‐ Lang AFRIS: Attitudes to Falls‐Related Interventions Scale AI: activity inventory AMD: age‐related macular degeneration AMD‐SEQ: age‐related macular degeneration ‐ self efficacy questionnaire ANCOVA: analysis of covariance appr: approximately AVL: adaptation to vision loss AVL‐12: adaptation to vision loss ‐ 12‐item questionnaire AVLS: adaptation to vision loss scale BADS: Behaviour Activation for Depression Scale BCVA: best corrected visual acuity BDI‐II: Beck Depression Inventory ‐ II CCTV: closed‐circuit television CELVR: Control [group] Enhanced Low Vision Rehabilitation CES‐D: Center for Epidemiologic Studies ‐ Depression scale CLVR: conventional low vision rehabilitation CVA: cerebral vascular accident DASS: Depression Anxiety and Stress Symptoms scale DemTect: Demenzdetektionstest DEPVIT: Depression in Visual Impairment Trial DR: diabetic retinopathy DSM‐IV: Diagnostic and Statistical Manual ‐ 5th version DSSI: Duke Social Support Index DVD: digital versatile disc ELVR: enhanced low vision rehabilitation EQ‐5D: EuroQol ‐ 5 Dimensions questionnaire FAQ: functional assessment questionnaire FES‐I: Falls Efficacy Scale ‐ International FIMBA: Functional Independence Measure for Blind Adults FVPT: functional visual performance test GAD‐7: Generalized Anxiety Disorder 7‐item questionnaire GDS (‐5 or ‐15): Geriatric Depression Scale (5‐ or 15‐item versions) GP: General Practitioner GSES: generalised self‐efficacy scale HADS‐A: Hospital Anxiety Depression Scale ‐ Anxiety subscale HDRS: Hamilton Depression Rating Scale HRQOL: health‐related quality of life IOP: intraocular pressure IQR: Interquartile range IResT: International Reading speed Texts IVI: Impact of Visual Impairment profile IVI‐Adult: Impact of Visual Impairment profile ‐ Adult version IVI‐C: Impact of Visual Impairment profile ‐ Child version IVI‐28: Impact of Visual Impairment profile ‐ 28‐item version KAP: Keele's assessment of participation logMAR: logarithm of the Minimal Angle of Resolution LOT‐R: Life Orientation Test‐Revised LOVIT‐I and ‐II: Low Vision Intervention Trial LV: low vision LVA: low vision aid LVQOL: low vision quality of life questionnaire LVR: low vision rehabilitation MacDQOL: macular degeneration quality of life questionnaire MADRS: Montgomery–Åsberg Depression Rating Scale MAI: Massof's Activity Inventory MANOVA: Multivariate Analysis Of Variance MD: macular degeneration min: minutes MINI: Mini‐International Neuropsychiatric Interview MLVAI: Melbourne Low Vision Activities of daily living Index MLVQ: Manchester Low Vision Questionnaire MMSE: Mini‐Mental State Examination MNRead: Minnesota Reading acuity charts MOS‐6: Medical Outcomes Study social support survey ‐ 6‐items NAS/NAS2: Nottingham Adjustment Scale NEI: National Eye InstitutE NEI‐VFQ: National Eye Institute Visual Functioning Questionnaire NHS: National Health Service NV: near vision PANAS: Positive And Negative Affect Scale PGWB: Psychological and General Well‐Being scale PHQ: Patient Health Questionnaire PHQ‐9: Patient Health Questionnaire ‐ 9‐item version POMS: profile of mood states PSS: perceived stress scale PST: Problem Solving Treatment PVAS: Perceived Visual Ability Scale QOL: quality of life QWBS: Quality of Well‐Being Scale R1: Diabetic Retinopathy Grading 1 (mild form) RCT: randomised controlled trial RP: retinitis pigmentosa RSVP: Rapid Serial Visual Presentation SAS: Self‐rating Anxiety Scale SCID: Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders SCL‐90: Symptom Checklist 90‐items SD: standard deviation SDS: Self‐rating Depression Scale SE: standard error SF‐12/SF‐36: Short‐Form 12‐item or 36‐item version SMD: standardised mean difference SPSS: Statistical Package for the Social Sciences ST: supportive therapy SWL: Satisfaction With Life scale 5‐TIADL: Five Timed Instrumental Activities of Daily Living questionnaire TVF: targeted vision function UCLA: University of California Los Angeles loneliness scale VA: visual acuity VCM1: vision‐related quality of life Core Measure ‐ 1 VCR: video cassette recorder VEGF: vascular endothelial growth factor VFQ (‐15, ‐17, ‐25, ‐48): Visual Functioning Questionnaire (15‐, 17‐, 25‐ and 48‐item versions) VISQOL: vision‐related quality of life VM: video magnifier VR: vision rehabilitation VRQOL: vision‐related quality of life vs: versus WEMWBS: Warwick‐Edinburgh Mental‐Wellbeing Scale WHO‐5: World Health Organization ‐ 5‐item questionnaire version
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aimola 2014 | RCT on reading and exploration computer training (visual field expansion‐related) |
| Antonucci 1995 | RCT on neglect rehabilitation, no QOL outcomes |
| Ballinger 1996 | NRCT comparing optical aids, no QOL outcomes |
| Bhatlawande 2014 | RCT but in laboratory experimental environment (obstacle course) |
| Birk 2004 | NRCT comparing psychosocial intervention versus controls |
| Boehm 1985 | NRCT, echolocalisation intervention, comparison between visually impaired and blindfolded persons, no QOL outcomes |
| Bowman 2017 | NRCT in low vision rehabiltation; safety crossing streets |
| Campbell 2005 | RCT on prevention of falls and costs, no QOL outcomes |
| Cavanaugh 2017 | NRCT in visual field enhancement |
| Chebat 2015 | NRCT on maze walking with an eye cane comparing visually impaired versus (blind‐folded) normally sighted persons |
| Chen 2012 | RCT on Tai Chi versus control in low vision residential home, no QOL outcomes |
| Coco‐Martin 2017 | NRCT comparing a reading training program to controls on efficacy and QOL |
| Coleman 2006 | RCT; healthy and AMD patients got a voucher for eye glasses, magnifiers or both |
| Connors 2014 | RCT on virtual environment and navigation skills, directed instruction versus video‐game based approaches, no QOL outcomes |
| Court 2011 | NRCT on community versus hospital‐based low vision intervention |
| Culham 2009 | q‐RCT on optical aids preferences, no rehabilitation intervention or proper assessment of QOL outcomes possible |
| Dae Shik Kim 2014 | RCT studying cane techniques among sighted persons, no QOL outcomes |
| Dae Shik Kim 2016 | RCT repeated measures latin‐square design on preference of 4 different cane tip designs for traveling on snow, no QOL outcomes |
| Dannenbaum 2010 | RCT on home‐based balance exercises, no QOL outcomes |
| De Haan 2015 | RCT on compensatory scanning training |
| Elliot 2014 | RCT on cognitive speed of processing training in visually impaired versus healthy controls, no QOL outcomes |
| Elshout 2016 | Cross‐over trial in vision rehabilitation in chronic cerebral blindness |
| Elshout 2018 | RCT in vision restoration for people with hemianopia |
| Flores 2015 | NRCT comparing a vibrotactile belt to audio information for wayfinding in low vision |
| George 2011 | RCT protocol on visual‐restoration type intervention study |
| Gopinath 2017 | Protocol for RCT to study multimodal support service for caregivers of AMD patients |
| Griffin‐Shirley 1994 | NRCT on community or centre‐based low vision rehabilitation vs controls |
| Grue 2008 | NRCT on visual cue training, no QOL outcomes |
| Hackney 2015 | NRCT comparing adapted tango versus fall proof lessions in visually impaired persons |
| Ivanov 2013 | Cross‐over RCT in visual exploration training for tunnel vision in RP |
| Ivanov 2016 | RCT after saccade or reading training on obstacle course outcomes |
| Kasten 1995 | NRCT comparing vision‐restoration therapy versus control, no QOL outcomes |
| Kerkhoff 2014 | NRCT comparing eye‐movement versus visual scanning training, no QOL outcomes |
| La Grow 2004 | NRCT comparing comprehensive low vision rehabilitation versus a matched control group |
| Lipkova 2008 | NRCT comparing aerobic exercise with controls, no QOL outcomes (anxiety) |
| Lundqvist 2014 | RCT on physiotherapy intervention (Feldenkrais method) versus no therapy to reduce neck pain in visually impaired persons, no QOL outcomes |
| Nelles 2001 | NRCT comparing fixating and exploring visual compensation therapy in hemianopia versus healthy subjects |
| Nguyen 2011 | RCT comparing rapid serial visual presentation versus sensomotoric training, no QOL outcomes |
| Peterson 2003 | RCT comparing optical aids, no low vision rehabilitation intervention or QOL outcomes |
| Plow 2012 | RCT comparing transcranial direct current stimulation and vision restoration therapy |
| Riley 2015 | NRCT comparing CCTV versus tablet for reading in low vision |
| Riley 2016 | NRCT comparing CCTV versus tablet for reading in low vision |
| Robinson 2018 | RCT comparing light therapy delivered via a light‐emitting mask to no treatment on the progression of AMD |
| Roentgen 2012 | NRCT comparing different mobility devices and canes, no QOL outcomes |
| Rossi 1990 | RCT comparing prisma versus control in hemianopia |
| Roth 2009 | RCT comparing saccade training versus flicker stimulation in hemianopia |
| Rowe 2014 | RCT protocol comparing prisms versus other training for vision restoration in hemianopia |
| Sabel 2014 | RCT on computer‐based vision restoration training vs placebo in glaucoma patients |
| Schinzel 2012 | RCT comparing visual restoration therapy versus saccadic training in neuritis optica |
| Seki 2011 | NRCT comparing no training versus virtual reality training, versus mobility training |
| Soong 2001 | NRCT comparing orientation and mobility training versus no training, no QOL outcomes |
| Stelmack 2002 | NRCT comparing intense versus less intense low vision rehabilitation |
| Stelmack 2012 | NRCT comparing inpatient versus outpatient low vision rehabilitation |
| Stroupe 2008 | NRCT comparing inpatient versus outpatient low vision rehabilitation on cost‐effectiveness |
| Szlyk 1998 | NRCT comparing orientation and mobility training and bioptics for driving versus waiting list, no QOL outcomes |
| Szlyk 2000 | RCT comparing bioptics and training versus lenses and training versus lenses, no QOL outcomes |
| Taylor 2011 | NRCT comparing systematic treatment targeting visual functioning versus conventional treatment after stroke |
| Trozzolino 2003 | NRCT comparing a psychoeducational group therapy program versus controls |
| Ueda 2013 | NRCT comparing a living skills program versus controls |
| Van Nispen 2010 | NRCT comparing optometric versus multidisciplinary services |
| Vreeken 2013 | RCT on occupational therapy intervention in dual sensory loss |
| Vukicevic 2009 | NRCT comparing eccentric viewing training versus controls |
| Wahl 2006 | RCT: patients randomised to two similar intervention groups, but controls were selected nonrandomly |
| West 2003 | RCT comparing vision screening in nursing homes versus usual care, no QOL outcomes, only baseline results |
| Wittich 2018 | Pre‐post single arm study of the effects of the eSight Eyewear to enhance vision. |
AMD: age‐related macular degeneration CCTV: closed‐circuit television NRCT: nonrandomised controlled trial QOL: quality of life q‐RCT: quasi‐ randomised controlled trial RCT: randomised controlled trial RP: retinitis pigmentosa
Characteristics of ongoing studies [ordered by study ID]
Keay 2018.
| Trial name or title |
Intervention type IV: other studies PlaTFORM: Preventing falls through specialist orientation and mobility training |
| Methods | RCT |
| Participants | 500 older adults with vision impairment or blindness |
| Interventions | 1) Lifestyle integrated functional exercise fall prevention programme 2) Usual care |
| Outcomes | Fall rate over 12 months, physical activity, impact of falls, QOL |
| Starting date | March 2017 |
| Contact information | lkeay@georgeinstitute.org.au |
| Notes | ANZCTR12616001186448, process evaluation protocol published (Dillon 2018) |
Lamoureux 2015.
| Trial name or title |
Intervention type II: methods of enhancing vision The Residential Ocular Care Study |
| Methods | RCT |
| Participants | 395 older adults in residential care, not necessarily visually impaired |
| Interventions | 1) Refraction and spectacle provision or cataract surgery or low vision rehabilitation or referral to ophthalmologist 2) Usual care which may include mobile optometric service |
| Outcomes | Near and distance vision, impact of vision impairment for VRQOL |
| Starting date | June 2014 |
| Contact information | ecosse@unimelb.edu.au |
| Notes | ACTRN12615000587505, study protocol published in 2018, data will soon be analysed and published (personal communication 2019) |
NCT00545220.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes Effectiveness of problem‐solving training on emotional health |
| Methods | RCT |
| Participants | 430 |
| Interventions | 1) Problem‐solving training 2) Sham attention intervention |
| Outcomes | Depressive symptoms |
| Starting date | October 2007 |
| Contact information | University of Alabama at Birmingham, USA |
| Notes | Clinical Trials register: NCT00545220. December 2014 final data collection date Study closed since recruitment of participants did not work out as expected (personal communication 2019) |
NCT00971464.
| Trial name or title |
Intervention type II: methods of enhancing vision Low vision study comparing eccentric viewing training versus closed circuit television use for AMD rehabilitation |
| Methods | RCT |
| Participants | 10 older adults with AMD |
| Interventions | 1) Eccentric viewing training 2) CCTV training |
| Outcomes | Reading speed and accuracy, VRQOL, depressive symptoms |
| Starting date | September 2009 |
| Contact information | Dr. Hodge, Lawson Health Research Institute, Canada |
| Notes | Clinical Trials register: NCT00971464 Relevant outcomes not published yet and are not expected anymore (personal communication 2019) |
NCT02457884.
| Trial name or title |
Intervention type II: methods of enhancing vision Effectiveness of training in reading rehabilitation for patients with diabetic macular oedema |
| Methods | RCT |
| Participants | 152 macular oedema participants |
| Interventions | 1) Visual processing training 2) Spatial visual span training 3) Visual processing speed and visual span training 4) Leisure reading activities |
| Outcomes | Visual processing speed, visual span size, reading performance, fixation stability, impact of visual impairment for VRQOL, participation in daily living |
| Starting date | May 2015 |
| Contact information | allen.my.cheong@polyu.edu.hk |
| Notes | Trial registration: NCT02457884 |
NCT03065907.
| Trial name or title |
Intervention type III: multidisciplinary rehabilitation programmes Timing of low vision rehabilitation in anti‐vascular endothelial growth factor (VEGF) therapy: TRAVIT |
| Methods | RCT |
| Participants | 44 neovascular AMD adults (50 years or older) |
| Interventions | 1) Vision rehabilitation within 1 month of randomisation 2) Vision rehabilitation within 7 months of randomisation |
| Outcomes | Consent rate, retention rate, crossing over from group 2 to 1 |
| Starting date | Jan 2018 |
| Contact information | Johns Hopkins University: Dr. X Guo, xguo11@jhi.edu |
| Notes | Trial registration: NCT03065907, estimated study completion date December 1, 2019 |
NCT03560765.
| Trial name or title |
Intervention type II: methods of enhancing vision Training in the use of smart phones and tablets to improve quality of life in visual impairment ‐ Mobile electronic devices for visual impairment (MED4VI) |
| Methods | RCT |
| Participants | 200 |
| Interventions | 1) training course only in the use of mobile electronic devices (e.g. tablet, smart phone) 2) buddy (a local university student) who can provide continuing assistance with using the devices by visiting the participant at home |
| Outcomes | VRQOL, depressive symptoms, acceptance, everyday activities |
| Starting date | August 2018 |
| Contact information | chris.dickinson@manchester.ac.uk; ahalya.subramanian.1@city.ac.uk |
| Notes | Clinical Trials register: NCT03560765, expected study completion date July 1, 2020 |
nl/trial/7764.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes E‐nergEYEze: Cost‐effectiveness of a self‐management ‐ cognitive behavioural therapy ‐ social worker supported e‐health intervention to reduce fatigue in visually impaired patients |
| Methods | RCT |
| Participants | 176 visually impaired adults |
| Interventions | 1) E‐nergEYEze e‐health intervention 2) Usual care |
| Outcomes | Fatigue, QOL, VRQOL, depression |
| Starting date | November 2019 |
| Contact information | Amsterdam UMC, Ophthalmology, Vrije Universiteit, Amsterdam, the Netherlands, Dr. van Nispen: r.vannispen@amsterdamumc.nl |
| Notes | Trial registration: NTR7764, data available in 2022 |
Rees 2013.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes Integrated depression management trial |
| Methods | RCT |
| Participants | Appr 180 visually impaired older adults from low vision rehabilitation services |
| Interventions | 1) Problem‐solving treatment in primary care 2) Usual care referral to general practitioner |
| Outcomes | Depressive symptoms and behaviours |
| Starting date | 2012 |
| Contact information | grees@unimelb.edu.au |
| Notes | No publication found yet |
Riazi 2014.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes POSITIVE: problem‐solving treatment for visual impairment |
| Methods | RCT pilot |
| Participants | 120 recently diagnosed partially sighted or blind persons |
| Interventions | 1) Problem‐solving treatment + usual care 2) Usual care |
| Outcomes | Psychological well‐being, symptoms of distress, mobility, QOL |
| Starting date | 2014 |
| Contact information | Afsane.riazi@rhul.ac.uk |
| Notes | RCT supported by PRIMENT UK‐CRC Registered Clinical Trials Unit No publication found yet |
Rubin 2011.
| Trial name or title |
Intervention type II: methods of enhancing vision EFFECT: eccentric fixation from enhanced clinical training |
| Methods | RCT |
| Participants | 200 AMD hospital patients from the UK |
| Interventions | 1) Hospital‐based low vision service 2) Enhanced rehabilitation programme including eccentric viewing |
| Outcomes | Visual ability, VRQOL, HRQOL, reading speed |
| Starting date | April 2011 |
| Contact information | g.rubin@ucl.ac.uk |
| Notes | Clinical Trials register: NCT01499628. December 2014 final data collection date |
Skelton 2016.
| Trial name or title |
Intervention type IV: other programmes Visually Impaired OLder people's Exercise programme for falls prevenTion: VIOLET |
| Methods | Randomised controlled feasibility trial |
| Participants | 80 visually impaired older adults |
| Interventions | 1) Falls management exercise programme 2) Usual activity |
| Outcomes | Fear of falling, QOL |
| Starting date | 2016 |
| Contact information | Dr. Bailey, Newcastle upon Tyne, UK: catherine.bailey@northumbria.ac.uk |
| Notes | Trial registration: ISRCTN16949845 Feasibility report available (Adams 2018) in which it was concluded that continuing with the RCT was feasible |
Sörensen 2015.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes MADAS: macular degeneration and aging study |
| Methods | RCT |
| Participants | 250 AMD participants |
| Interventions | 1) Preventive problem‐solving treatment 2) Life and health review |
| Outcomes | Psychological well‐being, preparation for future care |
| Starting date | May 2009 |
| Contact information | Silvia Sorensen, University of Rochester, NY, USA |
| Notes | Trial registration: NCT02224963, data will soon be analysed and published (personal communication 2019) |
Van der Aa 2017.
| Trial name or title |
Intervention type I: psychological therapies and/or group programmes E‐PsEYE: Economic evaluation of an e‐mental health intervention for patients with retinal exudative diseases who receive intraocular anti‐VEGF injections |
| Methods | RCT |
| Participants | 174 participants with retinal exudative diseases receiving anti‐VEGF treatment |
| Interventions | 1) E‐PsEYE: online cognitive behavioural therapy intervention supported by social workers from rehabilitation service in addition to usual care 2) Usual care |
| Outcomes | Depression, anxiety, quality‐adjusted life years |
| Starting date | June 2017 |
| Contact information | Amsterdam UMC, Ophthalmology, Vrije Universiteit, Amsterdam, the Netherlands. Dr. van der Aa: h.vanderaa@amsterdamumc.nl |
| Notes | Participants do not necessarily have low vision. Trial registration: NTR6337, data available in 2020 |
Zijlstra 2009.
| Trial name or title |
Intervention type III: multidisciplinary rehabilitation programmes Evaluation of a standardised orientation and mobility training in older adults with low vision |
| Methods | RCT |
| Participants | 190 visually impaired older adults |
| Interventions | 1) Standardised orientation and mobility training 2) Usual orientation and mobility training |
| Outcomes | Activities of daily life, distance and mobility activities, depression and anxiety symptoms, social support, VRQOL, HRQOL, concerns about falling |
| Starting date | July 2010 (see other outcomes in additional table by Ballemans 2012) |
| Contact information | Dr. Schouten, Maastricht University, CAPHRI School for Public Health and Primary Care |
| Notes | Clinical Trials register: NCT00946062. Relevant outcomes not published yet and are not expected anymore (personal communication) |
AMD: age‐related macular degeneration CCTV: closed‐circuit television EFFECT: eccentric fixation from enhanced clinical training HRQOL: health‐related quality of life MADAS: macular degeneration and aging study MED4VI: MED4VI POSITIVE: Problem‐Solving Treatment for Visual impairment QOL: quality of life RCT: randomised controlled trial TRAVIT: Timing of low vision Rehabilitation in Anti‐Vascular endothelial growth factor Therapy VEGF: vascular endothelial growth factor VIOLET: Visually Impaired Older people's Exercise programme for falls prevention VRQOL: vision‐related quality of life
Differences between protocol and review
Since the study protocol was published (Langelaan 2008), the team of authors has expanded (RvN, GV, JK, JEEK, GvR) and now includes authors from three academic centres in the Netherlands and Italy.
The title has changed from 'Multidisciplinary rehabilitation and monodisciplinary rehabilitation for visually impaired adults'. The focus on monodisciplinary versus multidisciplinary rehabilitation was not feasible because of clinical diversity; organising studies into two types of monodisciplinary rehabilitation (1) psychological therapies and/or group interventions; 2) methods of enhancing vision), 3) multidisciplinary rehabilitation and 4) other types of interventions that could also be considered part of rehabilitation, was a more logical categorisation.
Finally, more patient‐reported outcome measures that were closely related to QOL were added as secondary outcomes, such as 'physical outcomes' (activities of daily living), 'psychological outcomes' (depression, adaptation to vision loss, self‐esteem) and 'social outcomes' (participation). These may be considered deviations from protocol in which we also wanted to focus on satisfaction with the use of low vision aids, mobility, orientation and reading.
We had planned to use the fixed‐effects model If there were fewer than three trials in a certain comparison. However, this is not possible when a single forest plot is produced for several subgroups. Thus, we always used random‐effects models and we chose pragmatically to comment on individual studies when heterogeneity was apparent due to poor overlapping of 95% CIs of two studies in a subgroup.
Some studies presented both short‐ and long‐term data as trial outcomes. Since long‐term outcomes were scarce and were considered a possible threat to homogeneity of the data, we originally planned to first analyse data using short‐term outcomes only and if long‐term data were available, to enter them in the analyses and report separately if differences with only short‐term outcomes were relevant. However, given the small number of studies in each subgroup and the limitation in data reporting, we analysed the data as available.
We originally planned sensitivity analyses by excluding studies from the analysis if they presented unclear and/or high risk of bias on at least four out of seven domains on which risk of bias was assessed, or in case of outliers. However, as reported above, given the small number of studies in each subgroup, with unclear or high risk of bias in at least one domain, we did not conduct such analyses.
In the protocol, we stated that quasi‐randomised studies would be eligible, but in the review, they have now been excluded.
In the protocol, we did not mention whether studies that did not report certain outcomes would be excluded, but in the review studies were excluded if they did not report a quality of life outcome.
We did not consider data on reading, mobility, anxiety, satisfaction with rehabilitation, or other patient perceptions regarding rehabilitation which were mentioned in the initial protocol, but stayed closer to the concept of QOL.
Contributions of authors
‐ Conceiving the review: ML ‐ Designing the review: ML, RvN, GvR ‐ Co‐ordinating the review: RvN ‐ Data collection for the review: IG ‐ Designing search strategies: IG ‐ Undertaking searches: IG ‐ Screening search results: RvN, MH, ML, GV ‐ Organising retrieval of papers: MH ‐ Screening retrieved papers against inclusion criteria: RvN, MH, ML, GV ‐ Appraising quality of papers: RvN, MH, ML ‐ Extracting data from papers: RvN, MH, GV ‐ Writing to authors of papers for additional information: RvN, GV ‐ Providing additional data about papers: RvN, GV ‐ Obtaining and screening data on unpublished studies: RvN, MH ‐ Data management for the review: RvN, GV ‐ Entering data into RevMan: RvN, GV ‐ Analysis of data: RvN, GV ‐ Interpretation of data: RvN, GV ‐ Writing the review: RvN, GV, MH, ML, GvR, JK, JEEK
Sources of support
Internal sources
No sources of support supplied
External sources
A.F. Deutman Ophthalmic Research Foundation, Nijmegen, Netherlands.
-
National institute for Health Research (NIHR), UK.
o Richard Wormald, Co‐ordinating Editor for Cochrane Eyes and Vision (CEV) acknowledges financial support for his CEV research sessions from the Department of Health through the award made by the National Institute for Health Research to Moorfields Eye Hospital NHS Foundation Trust and UCL Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology. o This review was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the CEV UK editorial base.
The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, or the Department of Health.
Declarations of interest
The authors have no conflict of interest with respect to the studies reviewed.
These authors contributed equally to this work
These authors contributed equally to this work
New
References
References to studies included in this review
Acton 2016 {published data only}
- Acton JH, Molik B, Binns A, Court H, Margrain TH. Effect of rehabilitation worker input on visual function outcomes in individuals with low vision: study protocol for a randomised controlled trial. Trials 2016;17:Article number: 105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Acton JH, Molik B, Court H, Margrain TH. Effect of a home visit‐based low vision rehabilitation intervention on visual function outcomes: an exploratory randomized controlled trial. Investigative Ophthalmology and Visual Science 2016;57(15):6662‐7. [DOI] [PubMed] [Google Scholar]
Bradley 2005 {published data only}
- Bradley P, Mitchell J, Bradley C. Peer support for people newly diagnosed with macular degeneration: a pilot study. International Congress Series 2005;1282:211‐5. [Google Scholar]
Brody 1999 {published data only}
- Brody BL, Williams RA, Thomas RG, Kaplan RM, Chu RM, Brown SI. Age‐related macular degeneration: a randomized clinical trial of a self‐management intervention. Annals of Behavioral Medicine 1999;21(4):322‐9. [DOI] [PubMed] [Google Scholar]
Brody 2002 {published data only}
- Brody BL, Roch‐Levecq AC, Gamst AC, Maclean K, Kaplan RM, Brown SI. Self‐management of age‐related macular degeneration and quality of life: a randomized controlled trial. Archives of Ophthalmology 2002;120(11):1477‐83. [DOI] [PubMed] [Google Scholar]
- Brody BL, Roch‐Levecq AC, Kaplan RM, Moutier CY, Brown SI. Age‐related macular degeneration: self‐management and reduction of depressive symptoms in a randomized, controlled study. Journal of the American Geriatrics Society 2006;54(10):1557‐62. [DOI] [PubMed] [Google Scholar]
Brunnström 2004 {published data only}
- Brunnstrom G, Sorensen S, Alsterstad K, Sjostrand J. Quality of light and quality of life ‐ the effect of lighting adaptation among people with low vision. Ophthalmic and Physiological Optics 2004;24(4):274‐80. [DOI] [PubMed] [Google Scholar]
Bryan 2014 {published data only}
- Bryan JL, Lu Q. Vision for improvement: expressive writing as an intervention for people with Stargardt’s disease, a rare eye disease. Journal of Health Psychology 2016;21(5):709‐19. [DOI] [PubMed] [Google Scholar]
Burggraaff 2012 {published data only}
- Burggraaff MC. Contribution to Evidence in Low‐Vision Rehabilitation: Effects of CCTV Training in Visually Impaired Patients. Chapter 7 of Effects of CCTV Training on Task Performance [Thesis]. Amsterdam (NETHERLANDS): VU University, 2013. [Google Scholar]
- Burggraaff MC, Nispen RM, Knol DL, Ringens PJ, Rens GH. Randomized controlled trial on the effects of CCTV training on quality of life, depression, and adaptation to vision loss. Investigative Ophthalmology and Visual Science 2012;53(7):3645‐52. [DOI] [PubMed] [Google Scholar]
- Burggraaff MC, Nispen RMA, Hoeben FP, Knol DL, Rens GHMB. Randomized controlled trial on the effects of training in the use of closed‐circuit television on reading performance. Investigative Ophthalmology and Visual Science 2012;53(4):2142‐50. [DOI] [PubMed] [Google Scholar]
- Burggraaff MC, Nispen RMA, Melis‐Dankers BJM, Rens GHMB. Effects of standard training in the use of closed‐circuit televisions in visually impaired adults: design of a training protocol and a randomized controlled trial. BMC Health Services Research 2010;10:62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Christy 2012 {published data only}
- Christy B. A Randomized Trial of Methods of Low Vision Service Delivery [Thesis]. Sydney, Australia: The University of New South Wales, 2012. [Google Scholar]
- Christy B, Keeffe JE, Nirmalan PK, Rao GN. A randomized controlled trial assessing the effectiveness of strategies delivering low vision rehabilitation: design and baseline characteristics of study participants. Ophthalmic Epidemiology 2010;17(4):203‐10. [DOI] [PubMed] [Google Scholar]
Conrod 1998 {published data only}
- Conrod BE, Overbury O. The effectiveness of perceptual training and psychosocial counseling in adjustment to the loss of vision. Journal of Visual Impairment and Blindness 1998;92(7):464‐82. [Google Scholar]
Draper 2016 {published data only}
- Draper E, Feng R, Appel SD, Graboyes M, Engle E, Ciner EB, et al. Low vision rehabilitation for adult African Americans in two settings. Optometry and Vision Science 2016;93(7):673‐82. [DOI] [PubMed] [Google Scholar]
Dunbar 2013 {published data only}
- Dunbar HM, Crossland MD, Bunce C, Egan C, Rubin GS. The effect of low vision rehabiltation in diabetic eye disease: a randomised controlled trial protocol. Ophthalmic and Physiological Optics 2012;32(4):282‐293. [DOI] [PubMed] [Google Scholar]
- Dunbar HMP. Visual Disability in Diabetic Eye Disease and its Rehabilitation [Thesis]. London (UK): UCL Institute of Ophthalmology, 2013. [Google Scholar]
Eklund 2008 {published data only}
- Dahlin Ivanoff S, Sonn U, Svensson E. A health education program for elderly persons with visual impairments and perceived security in the performance of daily occupations: a randomized study. American Journal of Occupational Therapy 2002;56(3):322‐30. [DOI] [PubMed] [Google Scholar]
- Dahlin‐Ivanoff S, Klepp KI, Sjostrand J. Development of a health education programme for elderly with age‐related macular degeneration: a focus group study. Patient Education Counseling 1998;34(1):63‐73. [DOI] [PubMed] [Google Scholar]
- Eklund K, Dahlin‐Ivanoff S. Low vision, ADL and hearing assistive device use among older persons with visual impairments. Disability and Rehabilitation 2007;2(6):326‐34. [DOI] [PubMed] [Google Scholar]
- Eklund K, Sjostrand J, Dahlin‐Ivanoff S. A randomized controlled trial of a health‐promotion programme and its effect on ADL dependence and self‐reported health problems for the elderly visually impaired. Scandinavian Journal of Occupational Therapy 2008;15(2):68‐74. [DOI] [PubMed] [Google Scholar]
- Eklund K, Sonn U, Dahlin‐Ivanoff S. Long‐term evaluation of a health education programme for elderly persons with visual impairment. A randomized study. Disability Rehabilitation 2004;26(7):401‐9. [DOI] [PubMed] [Google Scholar]
- Eklund K, Sonn U, Nystedt P, Dahlin‐Ivanoff S. A cost‐effectiveness analysis of a health education programme for elderly persons with age‐related macular degeneration: a longitudinal study. Disability Rehabilitation 2005;27(20):1203‐12. [DOI] [PubMed] [Google Scholar]
Girdler 2010 {published data only}
- Girdler SJ, Boldy DP, Dhaliwal SS, Crowley M, Packer TL. Vision self‐management for older adults: a randomised controlled trial. British Journal of Ophthalmology 2010;94(2):223‐8. [DOI] [PubMed] [Google Scholar]
Gleeson 2014 {published data only}
- Gleeson M, Sherrington C, Borkowski E, Keay L. Improving balance and mobility in people over 50 years of age with vision impairments: can the Alexander Technique help? A study protocol for the VISIBILITY randomised controlled trial. Injury Prevention 2014;20(1):e3. [DOI] [PubMed] [Google Scholar]
- Gleeson M, Sherrington C, Lo S, Keay L. Can the Alexander Technique improve balance and mobility in older adults with visual impairments? A randomized controlled trial. Clinical Rehabilitation 2015;29(3):244‐60. [DOI] [PubMed] [Google Scholar]
- Keay LJ, Gleeson MG, Lo S, Sherrington C. Can the Alexander Technique improve balance and mobility in adults over 50 years of age with visual impairments? A single‐blind randomized controlled trial. Investigative Ophthalmology and Visual Science 2014; Vol. 55:ARVO E‐abstract 4579.
Goldstein 2007 {published data only}
- Goldstein RB, Dugan E, Trachtenberg F, Peli E. The impact of a video intervention on the use of low vision assistive devices. Optometry and Vision Science 2007;84(3):208‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jackson 2017 {published data only}
- Jackson ML, Schoessow KA, Selinova A, Wallis J. Adding access to a video magnifier to standard vision rehabilitation: initial results on reading performance and well‐being from a prospective, randomized study. Digital Journal of Ophthalmology 2017;23(1):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kaltenegger 2019 {published data only}
- Kaltenegger K. Reading training in dry AMD improves reading ability and prevents secondary depression. Investigative Ophthalmology and Visual Science 2016;57:ARVO E‐abstract 5168. [Google Scholar]
- Kaltenegger K, Stephan Kuester S, Altpeter‐Ott E, Eschweiler GW, Cordey A, Ivanov IV, et al. Effects of home reading training on reading and quality of life in AMD—a randomized and controlled study. Graefe's Archive for Clinical and Experimental Ophthalmology 2019;257(7):1499–512. [DOI] [PubMed] [Google Scholar]
Kaluza 1996 {published data only}
- Kaluza G, Strempel I, Maurer H. Stress reactivity of intraocular pressure after relaxation training in open‐angle glaucoma patients. Journal of Behavioral Medicine 1996;19(6):587‐98. [DOI] [PubMed] [Google Scholar]
Kamga 2017 {published data only}
- Kamga H, McCusker J, Yaffe M, Sewitch M, Susman T, Strumpf E, et al. Self‐care tools to treat depressive symptoms in patients with age‐related eye disease: a randomized controlled clinical trial. Clinical and Experimental Ophthalmology 2017;45(4):371‐8. [DOI] [PubMed] [Google Scholar]
Leat 2017 {published data only}
- Leat SJ, Si FF, Gold D, Pickering D, Gordon K, Hodge W. The experience of a randomized clinical trial of closed‐circuit television versus eccentric viewing training for people with age‐related macular degeneration. Journal of Visual Impairment and Blindness 2017;111(4):354‐68. [Google Scholar]
McCabe 2000 {published data only}
- McCabe P, Nason F, Demers TP, Friedman D, Seddon JM. Evaluating the effectiveness of a vision rehabilitation intervention using an objective and subjective measure of functional performance. Ophthalmic Epidemiology 2000;7(4):259‐70. [DOI] [PubMed] [Google Scholar]
Mielke 2013 {published data only}
- Mielke A, Wirkus K, Niebler R, Eschweiler G, Nguyen NX, Trauzettel‐Klosinski S. The influence of visual rehabilitation on secondary depressive disorders due to age‐related macular degeneration. A randomized controlled pilot study. Ophthalmologe 2013;110(5):433‐40. [DOI] [PubMed] [Google Scholar]
Mozaffar Jalali 2014 {published data only}
- Mozaffar Jalali MD, Moussavi MS, Amin Yazdi SA, Salehi Fadardi J. Effectiveness of rational emotive behavior therapy on psychological well‐being of people with late blindness. Journal of Rational ‐ Emotive and Cognitive ‐ Behavior Therapy 2014;32(4):23‐47. [Google Scholar]
Nollet 2016 {published data only}
- Margrain TH, Nollett C, Shearn J, Stanford M, Tudor Edwards R, Ryan B, et al. The DEPression in Visual Impairment Trial (DEPVIT): trial design and protocol. BMC Psychiatry 2012;12:Article number: 57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nollet CL, Bray N, Bunce C, Casten RJ, Edwards RT, Hegel MT, et al. Depression in visual impairment trial (DEPVIT): a randomized clinical trial of depression treatments in people with low vision. Investigative Ophthalmology & Visual Science 2016;57:4247‐54. [DOI] [PubMed] [Google Scholar]
Pankow 2004 {published data only}
- Pankow L, Luchins D, Studebaker J, Chettleburgh D. Evaluation of a vision rehabilitation program for older adults with visual impairment. Topics in Geriatric Rehabilitation 2004;20(3):223‐32. [Google Scholar]
Patodia 2017 {published data only}
- Patodia Y, Golesic E, Mao A, Hutnik CML. Clinical effectiveness of currently available low‐vision devices in glaucoma patients with moderate‐to‐severe vision loss. Clinical Ophthalmology 2017;11:683‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pearce 2011 {published data only}
- Pearce E, Crossland MD, Rubin GS. The efficacy of low vision device training in a hospital‐based low vision clinic. British Journal of Ophthalmology 2011;95(1):105‐8. [DOI] [PubMed] [Google Scholar]
Pinninger 2013 {published data only}
- Pinniger R, Brown RF, Thorsteinsson EB, McKinley P. Tango programme for individuals with age‐related macular degeneration. British Journal of Visual Impairment 2013;31(1):47‐59. [Google Scholar]
Rees 2015 {published data only}
- Rees G, Xie J, Chiang PP, Larizza MF, Marella M, Hassell JB, et al. A randomised controlled trial of a self‐management programme for low vision implemented in low vision rehabilitation services. Patient Education and Counseling 2015;98(2):174‐81. [DOI] [PubMed] [Google Scholar]
Reeves 2004 {published data only}
- Reeves BC, Harper RA, Russell WB. Enhanced low vision rehabilitation for people with age related macular degeneration: a randomised controlled trial. British Journal of Ophthalmology 2004;88(11):1443‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell W, Harper R, Reeves B, Waterman H, Henson D, McLeod D. Randomised controlled trial of an integrated versus an optometric low vision rehabilitation service for patients with age‐related macular degeneration: study design and methodology. Ophthalmic and Physiological Optics 2001;21(1):36‐44. [DOI] [PubMed] [Google Scholar]
Rovner 2007 {published data only}
- Rovner BW, Casten RJ. Preventing late‐life depression in age‐related macular degeneration. American Journal of Geriatric Psychiatry 2008;16:454‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rovner BW, Casten RJ, Hegel MT, Leiby BE, Tasman WS. Preventing depression in age‐related macular degeneration. Archives of General Psychiatry 2007;64(8):886‐92. [DOI] [PubMed] [Google Scholar]
Rovner 2013 {published data only}
- Rovner BW, Casten RJ, Hegel MT, Massof RW, Leiby BE, Ho AC, et al. Improving function in age‐related macular degeneration ‐ a randomized controlled trial. Ophthalmology 2013;120(8):1649‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rovner BW, Casten RJ, Hegel MT, Massof RW, Leiby BE, Tasman WS. Improving function in age‐related macular degeneration: design and methods of a randomized clinical trial. Contemporary Clinical Trials 2011;32(2):196‐203. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rovner 2014 {published data only}
- Casten R, Rovner BW, Fontenot JL. Targeted vision function goals and use of vision resources in ophthalmology patients with age‐related macular degeneration and comorbid depressive symptoms. Journal of Visual Impairment and Blindness 2016;110(6):413‐24. [Google Scholar]
- Deemer AD, Massof RW, Rovner BW, Casten RJ, Piersol CV. Functional outcomes of the low vision depression prevention trial in age‐related macular degeneration. Investigative Ophthalmology and Visual Science 2017;58(3):1514‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rovner BW, Casten RJ, Hegel MT, Massof RW, Leiby BE, Ho AC, et al. Low vision depression prevention trial in age‐related macular degeneration: a randomized clinical trial. Ophthalmology 2014;121(11):2204‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rumrill 1999 {published data only}
- Rumrill PD. Effects of a social competence training program on accommodation request activity, situational self‐efficacy, and Americans with Disabilities Act knowledge among employed people with visual impairments and blindness. Journal of Vocational Rehabilitation 1999;12(1):25‐31. [Google Scholar]
Scanlan 2004 {published data only}
- Scanlan JM, Cuddeford JE. Low vision rehabilitation: a comparison of traditional and extended teaching programs. Journal of Visual Impairment and Blindness 2004;98(10):601‐11. [Google Scholar]
Seiple 2011 {published data only}
- Seiple W, Grant P, Szlyk JP. Reading rehabilitation of individuals with AMD: relative effectiveness of training approaches. Investigative Ophthalmology and Visual Science 2011;52(6):2938–44. [DOI] [PubMed] [Google Scholar]
Smith 2005 {published data only}
- Smith HJ, Dickinson CM, Cacho I, Reeves BC, Harper RA. A randomized controlled trial to determine the effectiveness of prism spectacles for patients with age‐related macular degeneration. Archives of Ophthalmology 2005;123(8):1042‐50. [DOI] [PubMed] [Google Scholar]
Stelmack 2008 {published data only}
- Stelmack JA, Tang C, Reda DJ, Rinne S, Mancil RM, Massof RW. Outcomes of the Veterans Affairs Low Vision Intervention Trial (LOVIT). Archives of Ophthalmology 2008;126(5):608‐17. [DOI] [PubMed] [Google Scholar]
- Stelmack JA, Tang XC, Reda DJ, Moran D, Rinne S, Mancil RM, et al. The Veterans Affairs Low Vision Intervention Trial (LOVIT): design and methodology. Clinical Trials 2007;4(6):650‐60. [DOI] [PubMed] [Google Scholar]
Stelmack 2017 {published data only}
- Stelmack JA, Tang XC, Reda DJ, Stroupe KT, Rinne S, Massof RW. VA LOVIT II: a protocol to compare low vision rehabilitation and basic low vision. Ophthalmic and Physiological Optics 2012;32(6):461‐71. [DOI] [PubMed] [Google Scholar]
- Stelmack JA, Tang XC, Wei Y, Wilcox DT, Morand T, Brahm K, et al. Outcomes of the Veterans Affairs Low Vision Intervention Trial II (LOVIT II): a randomized clinical trial. JAMA Ophthalmology 2017;135(2):96‐104. [DOI] [PubMed] [Google Scholar]
- Stroupe KT, Stelmack JA, Tang XC, Wei Y, Sayers S, Reda DJ, et al. Economic evaluation of low‐vision rehabilitation for veterans with macular diseases in the US Department of Veterans Affairs. JAMA Ophthalmology 2018;136(5):524‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sun 2012 {published data only}
- Sun W, Wu F, Kong J, Nakahara Y, Xuan D, Li SY, et al. Analysis on the psychological factors of glaucoma and the influence of the psychological therapy after the education on the Glaucoma Club. International Eye Science 2012;12(9):1619‐22. [Google Scholar]
Taylor 2017 {published data only}
- Bray N, Brand A, Taylor J, Hoare Z, Dickinson C, Edwards RT. Portable electronic vision enhancement systems in comparison with optical magnifiers for near vision activities: an economic evaluation alongside a randomized crossover trial. Acta Ophthalmologica 2017;95(5):e415‐e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor J, Bambrick R, Dutton M, Harper R, Ryan B, Tudor‐Edwards R, et al. The p‐EVES study design and methodology: a randomised controlled trial to compare portable electronic vision enhancement systems (p‐EVES) to optical magnifiers for near vision activities in visual impairment. Ophthalmic and Physiological Optics 2014;34(5):558‐72. [DOI] [PubMed] [Google Scholar]
- Taylor JJ, Bambrick R, Brand A, Bray N, Dutton M, Harper RA. Effectiveness of portable electronic and optical magnifiers for near vision activities in low vision: a randomised crossover trial. Ophthalmic and Physiological Optics 2017;37(4):370‐84. [DOI] [PubMed] [Google Scholar]
Tey 2019 {published data only}
- Tey CS, Man REK, Fenwick EK, Aw AT, Drury V, Chiang PPC, et al. Effectiveness of the "living successfully with low vision" self‐management program: results from a randomized controlled trial in Singaporeans with low vision. Patient Education and Counseling 2019;102(6):1150‐6. [DOI] [PubMed] [Google Scholar]
Van der Aa 2015 {published data only}
- Aa HPA, Krijnen‐de Bruin E, Rens GHMB, Twisk JWR, Nispen RMA. Watchful waiting for subthreshold depression and anxiety in visually impaired older adults. Quality of Life Research 2015;24(12):2885‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aa HPA, Rens GHMB, Bosmans JE, Comijs HC, Nispen RMA. Economic evaluation of stepped‐care versus usual care for depression and anxiety in older adults with vision impairment: randomized controlled trial. BMC Psychiatry 2017;17:Article number: 280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aa HPA, Rens GHMB, Comijs HC, Bosmans JE, Margrain TH, Nispen RMA. Stepped‐care to prevent depression and anxiety in visually impaired older adults ‐ design of a randomised controlled trial. BMC Psychiatry 2013;13:Article number: 209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aa HPA, Rens GHMB, Comijs HC, Margrain TH, Gallindo‐Garre F, Twisk JWR, et al. Stepped care for depression and anxiety in visually impaired older adults: multicentre randomised controlled trial. BMJ 2015;351:h6127. [DOI: 10.1136/bmj.i1995] [DOI] [PMC free article] [PubMed] [Google Scholar]
Waterman 2016 {published data only}
- Waterman H, Ballinger C, Brundle C, Castin S, Gae H, Harper R, et al. A feasibility study to prevent falls in older people who are sight impaired: the VIP2UK randomised controlled trial. Trials 2016;17:Article number: 464. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Aimola 2014 {published data only}
- Aimola L, Lane AR, Smith DT, Kerkhoff G, Ford GA, Schenk T. Efficacy and feasibility of home‐based training for individuals with homonymous visual field defects. Neurorehabilitation and Neural Repair 2014;28(3):207‐18. [DOI] [PubMed] [Google Scholar]
Antonucci 1995 {published data only}
- Antonucci G, Guariglia C, Judica A, Magnotti L, Paolucci S, Pizzamiglio L, et al. Effectiveness of neglect rehabilitation in a randomized group study. Journal of Clinical and Experimental Neuropsychology 1995;17(3):383‐9. [DOI] [PubMed] [Google Scholar]
Ballinger 1996 {published data only}
- Ballinger R, Lalle P, Maino J, Stelmack J, Tallman K, Wacker R. Veterans Affairs multicenter low vision enhancement system (LVES) study: clinical results. Optometry 1996;71(12):764‐74. [PubMed] [Google Scholar]
Bhatlawande 2014 {published data only}
- Bhatlawande S, Mahadevappa M, Mukherjee J, Biswas M, Das D, Gupta S. Design, development, and clinical evaluation of the electronic mobility cane for vision rehabilitation. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2014;22(6):1148‐59. [DOI] [PubMed] [Google Scholar]
Birk 2004 {published data only}
- Birk T, Hickl S, Wahl HW, Kammerer A, Miller D, Holz F, et al. A psychosocial training program for elderly patients with age‐related macular degeneration: findings of a pilot evaluation study. Zeitschrift fur Gerontologie und Geriatrie 2004;37(5):363‐5. [DOI] [PubMed] [Google Scholar]
- Birk T, Hickl S, Wahl HW, Miller D, Kammerer A, Holz F, et al. Development and pilot evaluation of a psychosocial intervention program for patients with age‐related macular degeneration. Gerontologist 2004;44(6):836‐43. [DOI] [PubMed] [Google Scholar]
Boehm 1985 {published data only}
- Boehm RG. The use of echolocation as an aid in mobility for blind persons [Thesis]. Vancouver (CANADA): The University of British Columbia, 1985. [Google Scholar]
Bowman 2017 {published data only}
- Bowman EL, Liu L. Individuals with severely impaired vision can learn useful orientation and mobility skills in virtual streets and can use them to improve real street safety. PLOS One 2017;12:e0176534. [DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell 2005 {published data only}
- Campbell AJ, Robertson MC, Grow SJ, Kerse NM, Sanderson GF, Jacobs RJ, et al. Randomised controlled trial of prevention of falls in people aged >=75 with severe visual impairment: the VIP trial. BMJ 2005;331:817. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cavanaugh 2017 {published data only}
- Cavanaugh MR, Huxlin KR. Visual discrimination training improves Humphrey perimetry in chronic cortically induced blindness. Neurology 2017;88(19):1856‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chebat 2015 {published data only}
- Chebat DR, Maidenbaum S, Amedi A. Navigation using sensory substitution in real and virtual mazes. PLOS One 2015;10:e0126307. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chen 2012 {published data only}
- Chen EW, Fu ASN, Chan KM, Tsang WWN. The effects of Tai Chi on the balance control of elderly persons with visual impairment: a randomised clinical trial. Age and Aging 2012;41(2):254‐9. [DOI] [PubMed] [Google Scholar]
Coco‐Martin 2017 {published data only}
- Coco‐Martin MB, López‐Miguel A, Cuadrado R, Mayo‐Iscar A, Herrero AJ, Pastor JC, et al. Reading performance improvements in patients with central vision loss without age‐related macular degeneration after undergoing personalized rehabilitation training. Current Eye Research 2017;42(9):1260‐8. [DOI] [PubMed] [Google Scholar]
Coleman 2006 {published data only}
- Coleman AL, Yu F, Keeler E, Mangione CM. Treatment of uncorrected refractive error improves vision‐specific quality of life. Journal of the American Geriatrics Society 2006;54(6):883‐90. [DOI] [PubMed] [Google Scholar]
Connors 2014 {published data only}
- Connors EC, Chrastil ER, Sanchez J, Merabet LB. Virtual environments for the transfer of navigation skills in the blind: a comparison of directed instruction vs. video game based learning approaches. Frontiers in Human Neuroscience 2014;8:223. [DOI] [PMC free article] [PubMed] [Google Scholar]
Court 2011 {published data only}
- Court H, Ryan B, Bunce C, Margrain TH. How effective is the new community‐based Welsh low vision service?. British Journal of Ophthalmology 2011;95(2):178‐84. [DOI] [PubMed] [Google Scholar]
Culham 2009 {published data only}
- Culham LE, Chabra A, Rubin GS. Users' subjective evaluation of electronic vision enhancement systems. Ophthalmic and Physiological Optics 2009;29(2):138‐49. [DOI] [PubMed] [Google Scholar]
Dae Shik Kim 2014 {published data only}
- Dae Shik Kim, Emerson RW. Effect of cane technique on obstacle detection with the long cane. Journal of Visual Impairment and Blindness 2014;108(4):335‐40. [PMC free article] [PubMed] [Google Scholar]
Dae Shik Kim 2016 {published data only}
- Dae Shik Kim, Wall Emerson R, Gaves E. Travel in adverse winter weather conditions by blind pedestrians: effect of cane tip design on travel on snow. Journal of Visual Impairment and Blindness 2016;110(1):53‐8. [PMC free article] [PubMed] [Google Scholar]
Dannenbaum 2010 {published data only}
- Dannenbaum E, Kairy D, Fung J. Benefits of home‐based balance exercises for visually impaired seniors. Archives of Physical Medicine and Rehabilitation 2010;91(10):e49‐e50. [Google Scholar]
De Haan 2015 {published data only}
- Haan GA, Melis‐Dankers BJM, Brouwer WH, Tucha O, Heutink J. The effects of compensatory scanning training on mobility in patients with homonymous visual field defects: a randomized controlled trial. PLOS One 2015;10:e0134459. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elliot 2014 {published data only}
- Elliott AF, O'Connor ML, Edwards JD. Cognitive speed of processing training in older adults with visual impairments. Ophthalmic and Physiological Optics 2014;34(5):509‐18. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elshout 2016 {published data only}
- Elshout JA, Asten F, Hoyng CB, Bergsma DB, Berg AV. Visual rehabilitation in chronic cerebral blindness: a randomized controlled crossover study. Frontiers in Neurology 2016;7:92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elshout 2018 {published data only}
- Elshout J, Bergsma DP, Sibbel J, Baars‐Elsinga A, Lubbers P, Asten F, et al. Improvement in activities of daily living after visual training in patients with homonymous visual field defects using Goal Attainment Scaling. Restorative Neurology and Neuroscience 2018;36(1):1‐12. [DOI] [PubMed] [Google Scholar]
Flores 2015 {published data only}
- Flores G, Kurniawan S, Manduchi R, Martinson E. Vibrotactile guidance for wayfinding of blind walkers. IEEE Transactions of Haptics 2015;8:306‐17. [DOI] [PubMed] [Google Scholar]
George 2011 {published data only}
- George S, Hayes A, Chen C, Crotty M. The effect of static scanning and mobility training on mobility in people with hemianopia after stroke: a randomized controlled trial comparing standardized versus non‐standardized treatment protocols. BMC Neurology 2011;11:87. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gopinath 2017 {published data only}
- Gopinath B, Craig A, Kifley A, Liew G, Bloffwitch J, Vu KV, et al. Implementing a multi‐modal support service model for the family caregivers of persons with age‐related macular degeneration: a study protocol for a randomised controlled trial. BMJ 2017;7(8):e018204. [DOI] [PMC free article] [PubMed] [Google Scholar]
Griffin‐Shirley 1994 {published data only}
- Griffin‐Shirley N. The effect of rehabilitation training of visually impaired older adults on self‐efficacy, depression, activities of daily living, attitudes about blindness, and social support networks [abstract]. Dissertation Abstracts International Section A: Humanities and Social Sciences 1994;54:2805. [Google Scholar]
Grue 2008 {published data only}
- Grue EV, Kirkevold M, Mowinchel P, Ranhoff A. Sensory impairment in hip‐fracture patients 65 years or older and effects of hearing/vision interventions on fall frequency. Journal of Multidisciplinary Healthcare 2009;2:1‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hackney 2015 {published data only}
- Hackney ME, Hall CD, Echt KV, Wolf SL. Multimodal exercise benefits mobility in older adults with visual impairment: a preliminary study. Journal of Aging and Physical Activity 2015;23(4):630‐9. [DOI] [PubMed] [Google Scholar]
Ivanov 2013 {published data only}
- Ivanov I. Is visual exploration training beneficial in tunnel vision?. Investigative Ophthalmology and Visual Science 2013;54:ARVO E‐abstract 2769. [Google Scholar]
Ivanov 2016 {published data only}
- Ivanov I, Mackeben M, Vollmer A, Martus P, Nguyen NX, Trauzettel‐Klosinski S. Eye movement training and suggested gaze strategies in tunnel vision ‐ a randomized and controlled pilot study. PLOS One 2016;11:e0157825. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kasten 1995 {published data only}
- Kasten E, Sabel BA. Visual field enlargement after computer training in brain‐damaged patients with homonymous deficits: an open pilot trial. Restorative Neurology and Neuroscience 1995;8(3):113‐27. [DOI] [PubMed] [Google Scholar]
Kerkhoff 2014 {published data only}
- Kerkhoff G, Bucher L, Brasse M, Leonhart E, Holzgraefe M, Volzke V, et al. Smooth pursuit "bedside" training reduces disability and unawareness during the activities in daily living in neglect: a randomized controlled trial. Neurorehabilitation and Neural Repair 2014;28(6):554‐63. [DOI] [PubMed] [Google Scholar]
La Grow 2004 {published data only}
- Grow SJ. The effectiveness of comprehensive low vision services for older persons with visual impairments in New Zealand. Journal of Visual Impairment and Blindness 2004;98(11):679‐92. [Google Scholar]
Lipkova 2008 {published data only}
- Lipkova J, Gregor T, Kyselovicova O, Skodova M. The effect of aerobic exercises on the ocular parameters and the psychic state of glaucoma patients. Activitas Nervosa Superior 2008;50(1‐2):15‐7. [Google Scholar]
Lundqvist 2014 {published data only}
- Lundqvist LO, Zetterlund C, Richter HO. Effects of Feldenkrais method on chronic neck/scapular pain in people with visual impairment: a randomized controlled trial with one‐year follow‐up. Archives of Physical Medicine and Rehabilitation 2014;95(9):1656‐61. [DOI] [PubMed] [Google Scholar]
Nelles 2001 {published data only}
- Nelles G, Esser J, Ecksein A, Tiede A, Gerhard H, Diener HC. Compensatory visual field training for patients with hemianopia after stroke. Neuroscience Letters 2001;306(3):189‐92. [DOI] [PubMed] [Google Scholar]
Nguyen 2011 {published data only}
- Nguyen NX, Stockum A, Hahn GA, Trauzettel‐Klosinkski S. Training to improve reading speed in patients with juvenile macular dystrophy: a randomized study comparing two training methods. Acta Ophthalmologica 2011;89(1):e82‐e8. [DOI] [PubMed] [Google Scholar]
Peterson 2003 {published data only}
- Peterson RC, Wolffsohn JS, Rubinstein M, Lowe J. Benefits of electronic vision enhancement systems (EVES) for the visually impaired. American Journal of Ophthalmology 2003;136(6):1129‐35. [DOI] [PubMed] [Google Scholar]
Plow 2012 {published data only}
- Plow AB, Obretenova SN, Fregni F, Pascual‐Leone A, Merabet LB. Comparison of visual field training for hemianopia with active versus sham transcranial direct cortical stimulation. Neurorehabilitation and Neural Repair 2012;26(6):616‐26. [DOI] [PubMed] [Google Scholar]
Riley 2015 {published data only}
- Riley SK. Low vision reading speed comparison of CCTV and iPad. Investigative Ophthalmology and Visual Science 2017;56:ARVO E‐abstract 4793. [Google Scholar]
Riley 2016 {published data only}
- Riley SK. Apple iPad and CCTV reading performance comparison in persons with low vision. Investigative Ophthalmology and Visual Science 2016;57:ARVO E‐abstract 5169. [Google Scholar]
Robinson 2018 {published data only}
- McKeague C, Margrain T, Bailey C, Binns AM. Low‐level night‐time light therapy for age‐related macular degeneration (ALight): study protocol for a randomized controlled trial. Trials 2014;15:246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson DG, Margrain TH, Dunn MJ, Bailey C, Binns AM. Low‐level nighttime light therapy for age‐related macular degeneration: a randomized clinical trial. Investigative Ophthalmology and Visual Science 2018;59(11):4531–41. [DOI] [PubMed] [Google Scholar]
Roentgen 2012 {published data only}
- Roentgen UR, Gelderblom GJ, Witte LP. User evaluation of two electronic mobility aids for persons who are visually impaired: a quasi‐experimental study using a standardized mobility course. Assistive Technology 2012;24(2):110–20. [DOI] [PubMed] [Google Scholar]
Rossi 1990 {published data only}
- Rossi PW, Kheyfets S, Reding MJ. Fresnel prisms improve visual perception in stroke patients with homonymous hemianopia. Neurology 1990;40(10):1597‐9. [DOI] [PubMed] [Google Scholar]
Roth 2009 {published data only}
- Roth T, Sokolov AN, Messias A, Roth P, Weller M, Trauzettel‐Klosinski S. Comparing explorative saccade and flicker training in hemianopia. Neurology 2009;72(4):324‐31. [DOI] [PubMed] [Google Scholar]
Rowe 2014 {published data only}
- Rowe F, Drummond A, Sackley CM, Pollock A, Bedson E, Breen R, et al. A randomized controlled trial comparing the effectiveness of prism glasses, visual search training and standard care to improve visual field for people with hemianopia post stroke. International Journal of Stroke 2015;10(4):12‐13. [Google Scholar]
- Rowe FJ, Barton PG, Bedson E, Breen R, Conroy EJ, Cwiklinski E, et al. A randomised controlled trial to compare the clinical and cost‐effectiveness of prism glasses, visual search training and standard care in patients with hemianopia following stroke: a protocol. BMJ Open 2014;4(7):e005885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe FJ, Barton PG, Bedson E, Breen R, Conroy EJ, Cwiklinski E, et al. Randomized controlled trial results of prism therapy versus visual scanning training versus standard care for homonymous hemianopia. Neuro‐Ophthalmology 2015;39(6):S47. [Google Scholar]
- Rowe FJ, Conroy EJ, Barton PG, Bedson E, Cwiklinski E, Dodridge C, et al. A randomised controlled trial of treatment for post‐stroke homonymous hemianopia: screening and recruitment. Neuro‐Ophthalmology 2016;40(1):1‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rowe FJ, Conroy EJ, Bedson E, Cwiklinski E, Drummond A, García‐Fiñana M, et al. A pilot randomized controlled trial comparing effectiveness of prism glasses, visual search training and standard care in hemianopia. Acta Neurologica Scandinavica 2017;136(4):310‐21. [DOI] [PubMed] [Google Scholar]
Sabel 2014 {published data only}
- Sabel BA, Gudlin J. Vision restoration training for glaucoma: a randomized clinical trial. JAMA Ophthalmology 2014;132(4):381‐9. [DOI] [PubMed] [Google Scholar]
Schinzel 2012 {published data only}
- Schinzel J, Schwarzlose L, Dietze H, Bartusch K, Weiss S, Ohlraun S, et al. Efficacy of vision restoration therapy after optic neuritis (VISION study): study protocol for a randomized controlled trial. Trials 2012;13:94. [DOI] [PMC free article] [PubMed] [Google Scholar]
Seki 2011 {published data only}
- Seki Y, Sato T. A training system of orientation and mobility for blind people using acoustic virtual reality. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2011;19(1):95‐104. [DOI] [PubMed] [Google Scholar]
Soong 2001 {published data only}
- Soong GP, Lovie‐Kitchin JE, Brown B. Does mobility performance of visually impaired adults improve immediately after orientation and mobility training?. Optometry and Vision Science 2001;78(9):657‐66. [DOI] [PubMed] [Google Scholar]
Stelmack 2002 {published data only}
- Stelmack JA, Stelmack TR, Massof RW. Measuring low‐vision rehabilitation outcomes with the NEI VFQ‐25. Investigative Ophthalmology and Visual Science 2002;43(9):2859‐68. [PubMed] [Google Scholar]
Stelmack 2012 {published data only}
- Stelmack JA, Tang XC, Wei Y, Massof RW. The effectiveness of low‐vision rehabilitation in 2 cohorts derived from the Veterans Affairs low‐vision intervention trial. Archives of Ophthalmology 2012;130(9):1162‐8. [DOI] [PubMed] [Google Scholar]
Stroupe 2008 {published data only}
- Stroupe KT, Stelmack JA, Tang XC, Reda DJ, Moran D, Rinne S, et al. Economic evaluation of blind rehabilitation for veterans with macular diseases in the department of Veterans Affairs. Ophthalmic Epidemiology 2008;15(2):84‐91. [DOI] [PubMed] [Google Scholar]
Szlyk 1998 {published data only}
- Szlyk JP, Seiple W, Laderman DJ, Kelsch R, Ho K, McMahon R. Use of bioptic amorphic lenses to expand the visual field in patients with peripheral loss. Optometry and Vision Science 1998;75(7):518‐24. [DOI] [PubMed] [Google Scholar]
Szlyk 2000 {published data only}
- Szlyk JP, Seiple W, Laderman DJ, Kelsch R, Stelmack J, McMahon T. Measuring the effectiveness of bioptic telescopes for persons with central vision loss. Journal of Rehabilitation Research and Development 2000;37(1):101‐8. [PubMed] [Google Scholar]
Taylor 2011 {published data only}
- Taylor L, Poland F, Harrison P, Stephenson R. A quasi‐experimental feasibility study to determine the effect of a systematic treatment programme on the scores of the Nottingham Adjustment Scale of individuals with visual field deficits following stroke. Clinical Rehabilitation 2011;25(1):43‐50. [DOI] [PubMed] [Google Scholar]
Trozzolino 2003 {published data only}
- Trozzolino L, Thompson PS, Tansman MS, Azen SP. Effects of a psychoeducational group on mood and glycemic control in adults with diabetes and visual impairments. Journal of Visual Impairment and Blindness 2003;97(4):230‐9. [Google Scholar]
Ueda 2013 {published data only}
- Ueda Y, Tsuda A. Differential outcomes of skill training, group counselling, and individual cognitive therapy for persons with acquired visual impairment. Japanese Journal of Psychological Research 2013;55(3):229‐40. [Google Scholar]
Van Nispen 2010 {published data only}
- Boer MR, Terwee CB, Vet HCW, Moll AC, Volker‐Dieben HJM, Rens GHMB. Evaluation of cross‐sectional and longitudinal construct validity of two vision‐related quality of life questionnaires: the LVQOL and VCM1. Quality of Life Research 2006;15(2):233‐48. [DOI] [PubMed] [Google Scholar]
- Boer MR, Twisk J, Moll AC, Volker‐Dieben HJM, Vet HCW, Rens GHMB. Outcomes of low‐vision services using optometric and multidisciplinary approaches: a non‐randomized comparison. Ophthalmic and Physiological Optics 2006;26(6):535‐44. [DOI] [PubMed] [Google Scholar]
- Nispen RMA, Knol DL, Langelaan M, Boer MR, Terwee CB, Rens GHMB. Applying multilevel item response theory to vision‐related quality of life in Dutch visually impaired elderly. Optometry and Vision Science 2007;84(8):710‐20. [DOI] [PubMed] [Google Scholar]
- Nispen RMA, Knol DL, Neve HJ, Rens GHMB. A multilevel item response theory model was investigated for longitudinal vision‐related quality‐of‐life data. Journal of Clinical Epidemiology 2010;63(3):321‐30. [DOI] [PubMed] [Google Scholar]
Vreeken 2013 {published data only}
- Vreeken HL, Rens GH, Kramer SE, Knol DL, Festen JM, Nispen RM. Dual sensory loss: development of a dual sensory loss protocol and design of a randomized controlled trial. BMC Geriatrics 2013;13:84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vreeken HL, Rens GH, Kramer SE, Knol DL, Nispen RM. Effects of a dual sensory loss protocol on hearing aid outcomes: a randomized controlled rial. Ear and Hearing 2015;36(4):e166‐75. [DOI] [PubMed] [Google Scholar]
Vukicevic 2009 {published data only}
- Vukicevic M, Fitzmaurice K. Eccentric viewing training in the home environment: can it improve the performance of activities of daily living?. Journal of Visual Impairment and Blindness 2009;103(5):277‐90. [Google Scholar]
Wahl 2006 {published data only}
- Wahl, H, Kammerer A, Holz F, Miller D, Becker S, Kaspar R, et al. Psychosocial intervention for age‐related macular degeneration: a pilot project. Journal of Visual Impairment and Blindness 2006;100(9):533‐43. [Google Scholar]
West 2003 {published data only}
- West SK, Friedman D, Munoz B, Bandeen‐Roche K, Park W, Deremeik J, et al. A randomized trial of visual impairment interventions for nursing home residents: study design, baseline characteristics and visual loss. Ophthalmic Epidemiology 2003;10(3):193‐209. [DOI] [PubMed] [Google Scholar]
Wittich 2018 {published data only}
- Wittich W, Lorenzini MC, Markowitz SN, Tolentino M, Gartner SA, Goldstein JE, et al. The effect of head‐mounted low vision device on visual function. Optometry and Vision Science 2018;95(9):774‐84. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to ongoing studies
Keay 2018 {published data only}
- Dillon L, Clemson L, Coxon K, Keay L. Understanding the implementation and efficacy of a home‐based strength and balance fall prevention intervention in people aged 50 years or over with vision impairment: a process evaluation protocol. BMC Health Services Research 2018;18(1):512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keay L, Dillon L, Clemson L, Tiedemann A, Sherrington C, McCluskey P, et al. PrevenTing Falls in a high‐risk, vision‐impaired population through specialist ORientation and Mobility services: protocol for the PlaTFORM randomised trial. Injury Prevention 2018;24(6):459‐66. [DOI] [PubMed] [Google Scholar]
Lamoureux 2015 {published data only}
- Holloway EE, Constantinou M, Xie J, Fenwick EK, Finkelstein EA, Man REK, et al. Improving eye care in residential aged care facilities using the Residential Ocular Care (ROC) model: study protocol for a multicentered, prospective, customized, and cluster randomized controlled trial in Australia. Trials 2018;19(1):650. [DOI] [PMC free article] [PubMed] [Google Scholar]
NCT00545220 {published data only}
- NCT00545220. Problem solving training and low vision rehabilitation. clinicaltrials.gov/ct2/show/NCT00545220 Vol. (first received 17 October 2007).
NCT00971464 {published data only}
- NCT00971464. Low vision study comparing EV training vs. CCTV for AMD rehabilitation (AMD). clinicaltrials.gov/ct2/show/NCT00971464 (first received 3 September 2009).
NCT02457884 {published data only}
- NCT02457884. Effectiveness of training in reading rehabilitation for patients with diabetic macular oedema. clinicaltrials.gov/show/NCT02457884 (first received 29 May 2015).
NCT03065907 {published data only}
- NCT03065907. Timing of low vision rehabilitation in anti‐vascular endothelial growth factor (VEGF) therapy (TRAVIT). clinicaltrials.gov/ct2/show/NCT03065907 (first received 28 February 2018).
NCT03560765 {published data only}
- NCT03560765. Mobile electronic devices for visual impairment (MED4VI). clinicaltrials.gov/ct2/show/NCT03560765 (first received 18 June 2018).
nl/trial/7764 {published data only}
- nl/trial/7764. Reducing fatigue in visually impaired adults with the E‐nergEYEze intervention. www.trialregister.nl/trial/7764 (first received 28 May 2019).
Rees 2013 {published data only}
- Rees G, Mellor D, Holloway E, Sturrock BA, Hegel MT, Casten R, et al. Integrated depression management: a proposed trial of a new model of care in a low vision rehabilitation setting. Ophthalmic Epidemiology 2013;20(5):321‐9. [DOI] [PubMed] [Google Scholar]
Riazi 2014 {published data only}
- Riazi A, Walters K, Rubin G, Ambler G, Jichi F, Mynors‐Wallis L, et al. A pilot randomised controlled trial of Problem‐Solving Treatment for Visual Impairment (POSITIVE): protocol paper. Ophthalmic and Physiological Optics 2014;34(4):489‐97. [DOI] [PubMed] [Google Scholar]
Rubin 2011 {published data only}
- Brown G, Rubin G. Investigating the impact of Eccentric Viewing Training on reading performance in people with AMD participating in the EFFECT Trial. Investigative Ophthalmology and Visual Science 2016;57:ARVO E‐abstract. [Google Scholar]
- NCT01499628. EFFECT: eccentric fixation from enhanced clinical training. clinicaltrials.gov/ct2/show/NCT01499628 (first received 26 December 2011).
Skelton 2016 {published data only}
- Adams N, Skelton DA, Howel D, Bailey C, Lampitt R, Fouweather T, et al. Feasibility of trial procedures for a randomised controlled trial of a community based group exercise intervention for falls prevention for visually impaired older people: the VIOLET study. BMC Geriatrics 2018;18:307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skelton DA, Bailey C, Howel D, Cattan M, Deary V, Coe D, et al. Visually Impaired OLder people's Exercise programme for falls prevenTion (VIOLET): a feasibility study protocol. BMJ Open 2016;6:e011996. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sörensen 2015 {published data only}
- Sorensen S, White K, Mak W, Zanibbi K, Tang W, O'Hearn A, et al. The macular degeneration and aging study: design and research protocol of a randomized trial for a psychosocial intervention with macular degeneration patients. Contemporary Clinical Trials 2015;42:68‐77. [DOI] [PMC free article] [PubMed] [Google Scholar]
Van der Aa 2017 {published data only}
- Aa HPA, Rens GHMB, Verbraak FD, Bosscha M, Koopmanschap MA, Comijs HC, et al. Economic evaluation of an e‐mental health intervention for patients with retinal exudative diseases who receive intraocular anti‐VEGF injections (E‐PsEYE): protocol for a randomised controlled trial. BMJ Open 2017;7:e018149. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zijlstra 2009 {published data only}
- Ballemans J, Zijlstra GAR, Schouten JSAG, Kempen GIJM. Usefulness and acceptability of a standardised orientation and mobility training for partially‐sighted older adults using an identification cane. BMC Health Services Research 2012;12:141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zijlstra GAR, Rens GHMB, Scherder EJA, Brouwer DM, Velde J, Verstraten PFJ, et al. Effects and feasibility of a standardised orientation and mobility training in using an identification cane for older adults with low vision: design of a randomised controlled trial. BMC Health Services Research 2009;9:153. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Amtmann 2011
- Amtmann D, Cook KF, Johnson KL, Cella D. The PROMIS initiative: involvement of rehabilitation stakeholders in development and examples of applications in rehabilitation research. Archives of Physical Medicine and Rehabilitation 2011;92(Suppl 10):S12‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Barker 2015
- Barker L, Thomas R, Rubin G, Dahlmann‐Noor A. Optical reading aids for children and young people with low vision. Cochrane Database of Systematic Reviews 2015, Issue 3. [DOI: 10.1002/14651858.CD010987.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Binns 2012
- Binns AM, Bunce C, Dickinson C, Harper R, Tudor‐Edwards R, Woodhouse M, et al. How effective is low vision service provision? A systematic review. Survey of Ophthalmology 2012;57(1):34‐65. [DOI] [PubMed] [Google Scholar]
Bookwala 2011
- Bookwala J, Lawson B. Poor vision, functioning, and depressive symptoms: a test of the activity restriction model. Gerontologist 2011;51(6):798‐808. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bourne 2014
- Bourne R, Jonas JB, Flaxman SR, Keeffe JE, Leasher J, Naidoo K, et al. Prevalence and causes of vision loss in high‐income countries and in Eastern and Central Europe: 1990–2010. British Journal of Ophthalmology 2014;98(5):629‐38. [DOI] [PubMed] [Google Scholar]
Bourne 2017
- Bourne RRA, Flaxman SR, Braithwaite T, Cicinelli MV, Das A, Jonas JB, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta‐analysis. Lancet Global Health 2017;5(9):e888‐97. [DOI] [PubMed] [Google Scholar]
Bressler 2014
- Bressler NM, Varma R, Suñer IJ, Dolan CM, Ward J, Ehrlich JS, et al. RIDE and RISE Research Groups. Vision‐related function after ranibizumab treatment for diabetic macular edema: results from RIDE and RISE. Ophthalmology 2014;121(12):2461‐72. [DOI] [PubMed] [Google Scholar]
Brody 2001
- Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, Dolnak D, et al. Depression, visual acuity, comorbidity, and disability associated with age‐related macular degeneration. Ophthalmology 2001;108(10):1893‐900. [DOI] [PubMed] [Google Scholar]
Bruijning 2013
- Bruijning JE, Rens GHMB, Knol DL, Nispen RMA. Psychometric analyses to improve the Dutch ICF Activity Inventory. Optometry and Vision Science 2013;90(8):806‐19. [DOI] [PubMed] [Google Scholar]
Elsman 2019
- Elsman EBM, Al Baaj M, Rens GHMB, Sijbrandi W, Broek EGC, Aa HPA, et al. Interventions to improve functioning, participation, and quality of life in children with visual impairment: a systematic review. Survey of Ophthalmology 2019;64(4):512‐57. [DOI] [PubMed] [Google Scholar]
Glanville 2006
- Glanville JM, Lefebvre C, Miles JN, Camosso‐Stefinovic J. How to identify randomized controlled trials in MEDLINE: ten years on. Journal of the Medical Library Association 2006;94(2):130‐6. [PMC free article] [PubMed] [Google Scholar]
Hayman 2007
- Hayman KJ, Kerse NM, Grow SJ, Wouldes T, Robertson MC, Campbell AJ. Depression in older people: visual impairment and subjective ratings of health. Optometry and Vision Science 2007;84(11):1024‐30. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Deeks JJ (editors). Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Higgins 2017
- Higgins JP, Altman DG, Sterne JAC, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Kempen 2012
- Kempen GIJM, Ballemans J, Ranchor AV, Rens GHMB, Zijlstra GAR. The impact of low vision on activities of daily living, symptoms of depression, feelings of anxiety and social support in community‐living older adults seeking vision rehabilitation services. Quality of Life Research 2012;21(8):1405‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lim 2014
- Lim YE, Vukicevic M, Koklanis K, Boyle J. Low vision services in the Asia‐Pacific region: models of low vision service delivery and barriers. Journal of Visual Impairment and Blindness 2014;108(4):313‐22. [Google Scholar]
Maghami 2014
- Maghami MH, Sodagar AM, Lashay A, Riazi‐Esfahani H, Riazi‐Esfahani M. Visual prostheses: the enabling technology to give sight to the blind. Journal of Ophthalmic and Vision Research 2014;9(4):494‐505. [DOI] [PMC free article] [PubMed] [Google Scholar]
Massof 2001
- Massof RW, Rubin GS. Visual function assessment questionnaires. Survey of Ophthalmology 2001;45(6):531‐48. [DOI] [PubMed] [Google Scholar]
Massof 2005
- Massof RW, Hsu CT, Baker FH, Barnett GD, Park WL, Deremeik JT, et al. Visual disability variables. I: the importance and difficulty for activity goals of a sample of low vision patients. Archives of Physical and Medical Rehabilitation 2005;86(5):946‐53. [DOI] [PubMed] [Google Scholar]
Massof 2007
- Massof RW, Deremeik JT, Park WL, Grover LL. Self‐reported importance and difficulty of driving in a low‐vision clinic population. Ophthalmic Epidemiology 2007;48(11):4955‐62. [DOI] [PubMed] [Google Scholar]
Owsley 2009
- Owsley C, McGwin G, Lee PP, Wasserman N, Searcey K. Characteristics of low vision rehabilitation services in the United States. Archives of Ophthalmology 2009;127(5):681‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pascolini 2012
- Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. British Journal of Ophthalmology 2012;96(5):614‐8. [DOI] [PubMed] [Google Scholar]
Pesudovs 2007
- Pesudovs K. Patient‐centered measurement in ophthalmology ‐ a paradigm shift. BMC Ophthalmology 2007;6:25. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pollock 2011
- Pollock A, Hazelton C, Henderson CA, Angilley J, Dhillon B, Langhorne P, et al. Interventions for disorders of eye movement in patients with stroke. Cochrane Database of Systematic Reviews 2011, Issue 10. [DOI: 10.1002/14651858.CD008389.pub2] [DOI] [PubMed] [Google Scholar]
Roets‐Merken 2015
- Roets‐Merken LM, Draskovic I, Zuidema SU, Erp WS, Graff MJL, Kempen GIJM, et al. Effectiveness of rehabilitation interventions in improving emotional and functional status in hearing or visually impaired older adults: a systematic review with meta‐analyses. Clinical Rehabilitation 2015;29(2):107‐19. [DOI] [PubMed] [Google Scholar]
Samoocha 2010
- Samoocha D, Bruinvels DJ, Elbers NA, Anema JR, Beek AJ. Effectiveness of web‐based interventions on patient empowerment: a systematic review and meta‐analysis. Journal of Medical Internet Research 2010;12(2):e23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Scott 1999
- Scott IU, Smiddy WE, Schiffman J, Feuer WJ, Pappas CJ. Quality of life of low‐vision patients and the impact of low‐vision services. American Journal of Ophthalmology 1999;128(1):54‐62. [DOI] [PubMed] [Google Scholar]
Skelton 2013
- Skelton DA, Howe TE, Ballinger C, Neil F, Palmer S, Gray L. Environmental and behavioural interventions for reducing physical activity limitation in community‐dwelling visually impaired older people. Cochrane Database of Systematic Reviews 2013, Issue 5. [DOI: 10.1002/14651858.CD009233.pub2] [DOI] [PubMed] [Google Scholar]
Stelmack 2001
- Stelmack J. Quality of life of low‐vision patients and outcomes of low‐vision rehabilitation. Optometry and Vision Science 2001;78(5):335‐42. [DOI] [PubMed] [Google Scholar]
Van Nispen 2009
- Nispen RMA, Boer MR, Hoeijmakers JGJ, Ringens PJ, Rens GHMB. Co‐morbidity and visual acuity are risk factors for health related quality of life decline: five months follow‐up EQ‐5D data of visually impaired older patients. Health and Quality of Life Outcomes 2009;7:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
Virgili 2010
- Virgili G, Rubin G. Orientation and mobility training for adults with low vision. Cochrane Database of Systematic Reviews 2010, Issue 5. [DOI: 10.1002/14651858.CD003925] [DOI] [PMC free article] [PubMed] [Google Scholar]
Virgili 2018
- Virgili G, Acosta R, Bentley SA, Giacomelli G, Allcock C, Evans JR. Reading aids for adults with low vision. Cochrane Database of Systematic Reviews 2018, Issue 4. [DOI: 10.1002/14651858.CD003303.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
WHO 2007
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems. www.who.int/classifications/icd/en/ (accessed 28 October 2019), issue 11th revision.
WHO 2013
- World Health Organisation. Universal eye health. A global action plan 2014‐2019. www.who.int/blindness/actionplan/en/ (accessed 28 October 2019).
WHO 2017
- World Health Organisation. International standards for vision rehabilitation: report of the international consensus conference: Rome, 9‐12 December 2015: Universal access to low vision rehabilitation. www.iapb.org/resources/international‐consensus‐conference‐vision‐rehabilitation‐standards/ (accessed 28 October 2019).
References to other published versions of this review
Langelaan 2008
- Langelaan M, Nispen RMA. Multidisciplinary rehabilitation and monodisciplinary rehabilitation for visually impaired adults. Cochrane Database of Systematic Reviews 2008, Issue 4. [DOI: 10.1002/14651858.CD006543] [DOI] [Google Scholar]