

Abstract
Purpose:
To examine the role of radiation oncology (RO) graduates’ application patterns and personal preferences in current labor concerns.
Methods and Materials:
An anonymous, voluntary survey was distributed to 665 domestic RO graduates from 2013 to 2017. Questions assessed graduates’ regional (Northeast [NE]; Midwest [MW]; South [SO]; West [WT]) job type and population size preferences. Top regional choice was compared across other categorical and numerical variables using the χ2 test and analysis of variance, respectively.
Results:
Complete responses were obtained from 299 (45.0% response rate) participants: 82 (27.4%), 74 (24.7%), 85 (28.4%), and 58 (19.4%) graduated from NE, MW, SO, and WT programs. The most to least commonly applied regions were SO (69.2%), MW (55.9%), and then NE/WT (55.2% each). The first and last regional choices were the WT (29.4%) and MW (15.7%), respectively. The most and least common application and top choice preferences were consistent in terms of city size: >500,000 (86.0% and 64.5%, respectively) and <100,001 (26.1% and 7.0%, respectively). The majority of applicants applied to both academic and nonacademic positions (60.9%), with top job type choice being equally split. The majority of respondents independently received a job offer in their preferred region (75.3%), city population size (72.6%) or job type (81.9%). Additionally, 52.5% received a job offer that included all three preferences. Those who underwent residency training (44.3% vs 62.0%−83.6%, P < .001) or medical schooling (50.7% vs 56.3%−75.6%, P < .001) or grew up in the MW (60.8% vs 70.0%−74.7%, P < .001) were least likely to choose this region as their top regional choice compared with other regions.
Conclusions:
The MW and jobs in smaller cities are less appealing to RO graduates, even if they receive training in the MW, which may contribute to current job market concerns. Nonetheless, the majority of respondents received a job offer in the region, population size, and job type of their top choice. Assessing prospective candidates’ city size and geographic preferences and prioritizing applicants who are compatible with positions may help address potential job market discrepancies.
Summary
In this survey of radiation oncology graduates’ applications patterns and personal preferences, we found recent graduates demonstrate a strong preference for working in large cities (>500,000) and had less interest in practicing in the Midwest (MW). Those with ties to the MW (residency training, medical schooling, raised in the MW) chose to practice in the MW less frequently than those with ties to other regions, which may contribute to job market concerns/disparity.
Introduction
There are significant concerns regarding the domestic radiation oncology (RO) labor market.1,2 In the 2017 American Society of Radiation Oncology (ASTRO) Workforce Survey,3,4 59.8% of respondents noted difficulty in procuring a position, citing lack of positions in “desired areas” and overall practice opportunities.3 Conversely, others suggest there is a problem of RO job maldistribution rather than a worsening job market.5–7
To date, no study has defined or investigated applicant opinions on job “desirability” in terms of region, population size, or job type. Therefore, we explored domestic RO graduates’ application patterns and personal preferences, which are potential confounders when assessing the health of the job market.
Methods and Materials
Survey design
An anonymous, internet-based survey (survey questions in Appendix E1; available online at https://doi.org/10.1016/j.ijrobp.2018.12.026) was developed to assess domestic RO graduates’ job application patterns and regional, population size, and job type preferences. This study was granted an exception by the institutional review board.
Regional designations were consistent with US Census Bureau8 definitions. Subset regions were consolidated into larger geographic regions (Northeast [NE], Midwest [MW], South [SO], and West [WT]) for statistical analysis. Jobs were categorized as either academic (medical center/hospital with residency training programs) or nonacademic (all others).
Participants and survey distribution
Graduates from Accreditation Council for Graduate Medical Education (ACGME) accredited RO programs in 2013 to 2017 were identified through (1) Association of Residents in Radiation Oncology directories, (2) ASTRO member directory, (3) institutional websites, and (4) Internet searches. Valid e-mail addresses for 665 graduates (90.7%) were obtained.
The survey was distributed using SurveyPlanet (https://surveyplanet.com). The survey was voluntary, participants remained anonymous, and responses were confidential. Three email notifications were sent from October 9, 2017 through November 6, 2017,9 and data collection concluded on November 15, 2017.
Statistical analysis
Descriptive statistics were generated for categorical and numeric variables. Top choice region was compared with other categorical variables using χ2 tests, and numeric variables were compared using analysis of variance. Statistical analyses were performed with SAS software (version 9.4; SAS Institute, Cary, NC).
Results
Demographics
Complete responses were obtained from 299 of 665 (45.0%) invited graduates. Table 1 highlights the characteristics of the respondents and compares the distribution to the entire ACGME RO resident cohort from 2013 to 2017.
Table 1.
Demographic information about sample population
| Variable | Current study | ACGME total | P value |
|---|---|---|---|
| Sex | 1.0 | ||
| Male | 202 (67.6%) | 515 (70.3%) | |
| Female | 81 (27.1%) | 209 (28.5%) | |
| No response | 16 (5.4%) | 9 (1.2%) | |
| Relationship status | - | - | |
| Single | 53 (17.7%) | ||
| Spouse/partner | 127 (42.5%) | ||
| Spouse/partner/family | 119 (39.8%) | ||
| Year of graduation | .354 | ||
| 2013 | 48 (15.9%) | 132 (17.3%) | |
| 2014 | 44 (14.6%) | 144 (18.9%) | |
| 2015 | 55 (18.9%) | 150 (19.7%) | |
| 2016 | 76 (25.6%) | 166 (21.8%) | |
| 2017 | 75 (24.9%) | 171 (22.4%) | |
| Region of residency | .793 | ||
| Training | |||
| Northeast | 82 (27.4%) | 218 (28.6%) | |
| Midwest | 74 (24.7%) | 193 (25.3%) | |
| South | 85 (28.4%) | 224 (29.4%) | |
| West | 58 (19.4%) | 128 (16.8%) | |
| Region of medical school | - | - | |
| Northeast | 93 (31.1%) | ||
| Midwest | 71 (23.7%) | ||
| South | 85 (28.4%) | ||
| West | 46 (15.4%) | ||
| Other | 4 (1.3%) | ||
| Region of origin | - | - | |
| Northeast | 73 (24.4%) | ||
| Midwest | 56 (18.7%) | ||
| South | 85 (28.4%) | ||
| West | 74 (24.7%) | ||
| Other | 11 (3.7%) | ||
| Spouse region of origin | - | - | |
| Northeast | 60 (20.1%) | ||
| Midwest | 58 (19.4%) | ||
| South | 62 (20.7%) | ||
| West | 44 (14.7%) | ||
| Other | 17 (5.7%) | ||
| Declined to Answer | 58 (19.4%) |
Abbreviation: ACGME = Accreditation Council for Graduate Medical Education.
Survey demographics comparisons based on information derived from National Resident Matching Program Results and ACGME Data Resource Book.
Job application patterns
Of the 299 respondents, 55.2% (n = 165), 55.9% (n = 167), 69.2% (n = 207), and 55.2% (n = 165) applied to a position in the NE, MW, SO, and WT. Top regional choice was as follows: NE, 22.1% (n = 66); MW, 15.7% (n = 47); SO, 27.4% (n = 82); WT, 29.4% (n = 88); and no regional preference, 5.4% (n = 16). Table E1 (available online at https://doi.org/10.1016/j.ijrobp.2018.12.026) shows top subset regional choices. Two hundred and twenty-five (75.3%) applicants received a job offer in their preferred region; 197 (87.6%) accepted the position.
Respondents applied most frequently to jobs in cities with a population >500,000 (n = 257; 86.0%), whereas only 26.1% (n = 78) applied to a city with a population of 0 to 100,000. The majority (64.5%, n = 193) chose >500,000 as their top population size choice, whereas only 7.0% (n = 21) preferred a city size of 0 to 100,000. The majority (n = 217, 72.6%) of applicants received a job offer in a location with their top city population size, of whom 88.5% (n = 192) accepted the position.
Of the respondents, 248 (82.9%), 233 (77.9%), and 182 (60.9%) applied to academic, nonacademic, and both job types. Top job choice was evenly split: academic at 150 (50.2%) versus nonacademic at 149 (49.8%). The majority of applicants received (n = 245; 81.9%) and accepted (n = 222; 90.6%) a job offer for their preferred job type.
Top regional choice analysis
Table 2 demonstrates factors that correlate with top regional choice when controlling by various covariates. Importantly, the MW was least likely to be chosen as the top region to practice compared with other regions, regardless of graduates receiving residency training (44.3% vs 62.0%−83.6%, P < .001) or medical schooling (50.7% vs 56.3%−75.6%, P < .001) or being raised in the MW (60.8% vs 70.0%−74.6%, P < .001) (Fig. 1). Additionally, those whose spouse grew up in the MW (55.6% vs 70.7%−83.7%) were least likely to choose the MW as their top region to practice.
Table 2.
Top regional choice analysis
| Covariate | Level | Top choice region | P-value | |||
|---|---|---|---|---|---|---|
| Northeast (N = 66) | Midwest (N = 47) | South (N = 82) | West (N = 88) | |||
| Sex | Male (N = 195) | 23.1% | 17.4% | 25.1% | 34.4% | .093 |
| Female (N = 73) | 23.3% | 13.7% | 39.7% | 23.3% | ||
| Year of graduation | 2013 (N = 43) | 14.0% | 16.3% | 44.2% | 25.6% | .534 |
| 2014 (N = 44) | 22.7% | 20.5% | 29.5% | 27.3% | ||
| 2015 (N = 50) | 28.0% | 18.0% | 18.0% | 36.0% | ||
| 2016 (N = 72) | 26.4% | 16.7% | 23.6% | 33.3% | ||
| 2017 (N = 74) | 23.0% | 13.5% | 32.4% | 31.1% | ||
| Residency training location | Northeast (N = 79) | 62.0% | 5.1% | 11.4% | 21.5% | <.001 |
| Midwest (N = 70) | 7.1% | 44.3% | 24.3% | 24.3% | ||
| South (N = 79) | 13.9% | 12.7% | 63.3% | 10.1% | ||
| West (N = 55) | 1.8% | 3.6% | 10.9% | 83.6% | ||
| Medical school Location | Northeast (N = 87) | 56.3% | 5.7% | 12.6% | 25.3% | <.001 |
| Midwest (N = 69) | 11.6% | 50.7% | 11.6% | 26.1% | ||
| South (N = 80) | 8.8% | 5.0% | 68.8% | 17.5% | ||
| West (N = 45) | 4.4% | 6.7% | 13.3% | 75.6% | ||
| Other (N = 2) | 0.0% | 0.0% | 100.0% | 0.0% | ||
| Region of origin | Northeast (N = 70) | 70.0% | 5.7% | 11.4% | 12.9% | <.001 |
| Midwest (N = 51) | 7.8% | 60.8% | 5.9% | 25.5% | ||
| South (N = 82) | 7.3% | 8.5% | 72.0% | 12.2% | ||
| West (N = 71) | 8.5% | 7.0% | 9.9% | 74.6% | ||
| Other (N = 9) | 11.1% | 0.0% | 55.6% | 33.3% | ||
| Spouse/partner/family when applying | Spouse/Partner (N = 123) | 26.0% | 16.3% | 32.5% | 25.2% | .508 |
| Spouse/Partner/Family (N = 114) | 22.8% | 16.7% | 27.2% | 33.3% | ||
| No (N = 46) | 17.4% | 17.4% | 23.9% | 41.3% | ||
| Spouse region of origin | Northeast (N = 58) | 70.7% | 5.2% | 15.5% | 8.6% | <.001 |
| Midwest (N = 54) | 13.0% | 55.6% | 9.3% | 22.2% | ||
| South (N = 60) | 6.7% | 1.7% | 73.3% | 18.3% | ||
| West (N = 43) | 7.0% | 2.3% | 7.0% | 83.7% | ||
| Other (N = 17) | 11.8% | 23.5% | 47.1% | 17.6% | ||
| Number of regions applied | Mean | 2.61 | 1.96 | 2.18 | 2.47 | .006 |
| Median | 3 | 2 | 2 | 2 | ||
| Top job type choice | Academic (N = 140) | 30.7% | 15.0% | 26.4% | 27.9% | .037 |
| Non-academic (N = 143) | 16.1% | 18.2% | 31.5% | 34.3% | ||
| Top city population size choice | 0–100,000 (N = 21) | 14.3% | 33.3% | 33.3% | 19.0% | .003 |
| 100,001–200,000 (N = 29) | 24.1% | 34.5% | 34.5% | 6.9% | ||
| 200,001–500,000 (N = 49) | 26.5% | 20.4% | 28.6% | 24.5% | ||
| >500,000 (N = 184) | 23.4% | 10.9% | 27.7% | 38.0% | ||
Percentages derived by using number of responses per each respective top choice region as numerator and total responses in corresponding row (covariate column) as denominator.
Bold was used to signify statistical significance (P < 0.05).
Fig. 1.
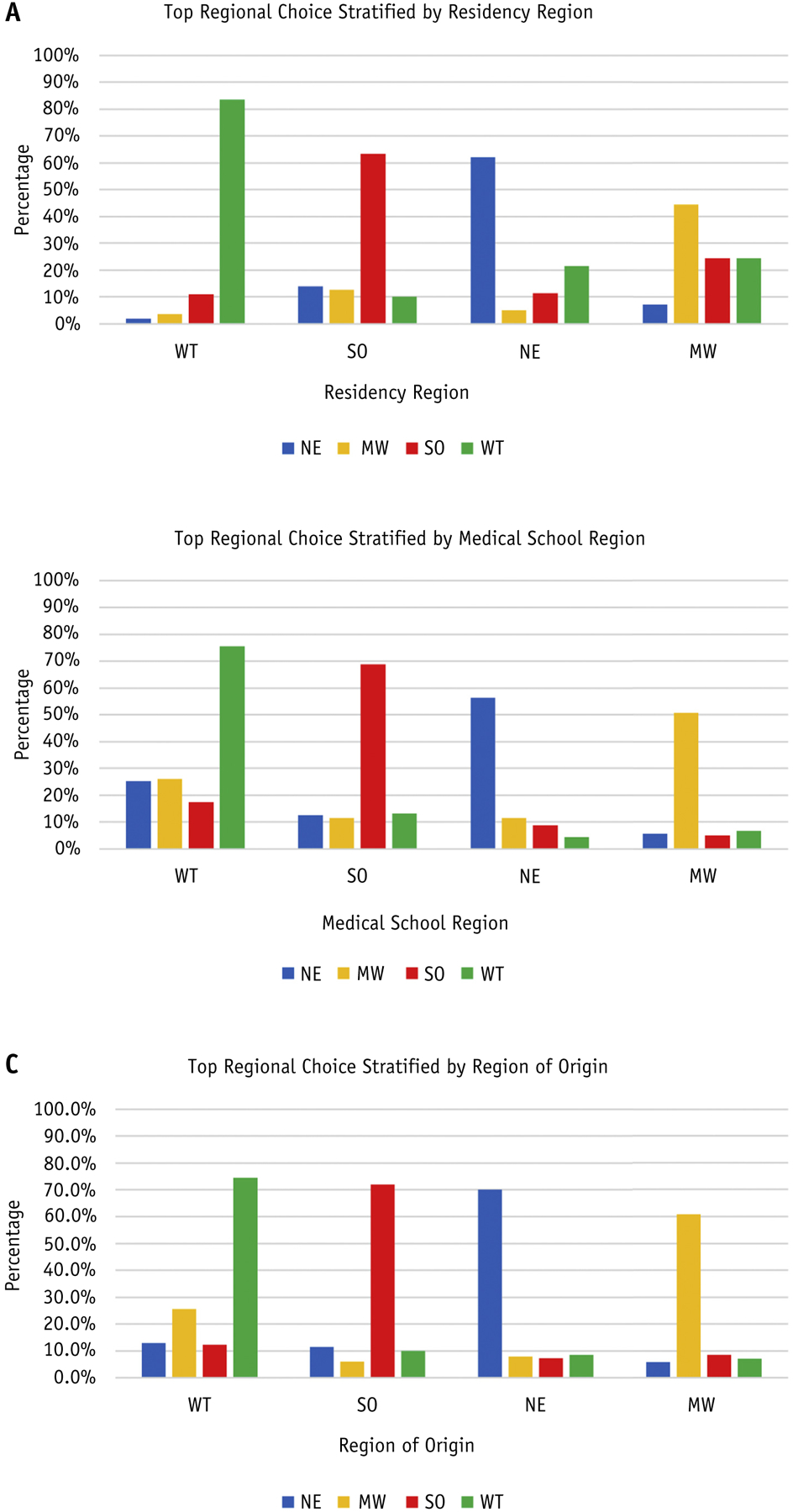
Respondents’ top regional choice (columns) stratified by (A) region of residency training, (B) region of medical schooling, and (C) region of origin (defined as where one self-reports being raised).
When controlling for top choice region Table E2 (available online at https://doi.org/10.1016/j.ijrobp.2018.12.026), we find that the WT is the most likely region to be preferred by both those with and without ties to the WT. A similar pattern is seen when assessing spousal regional ties. Those who prefer the MW applied to the least number of regions and had a higher preference for smaller city positions (0–200,000: 36.2% vs 6.8%−20.7%). Only those who preferred the NE were more likely to prefer an academic job (65.2% vs 44.2%−45.1%, P = .003).
Discussion
In this study, we surveyed RO graduates’ application patterns and job preferences over a 5-year span. The WT (29.4%) and MW (15.7%) were the most and least popular regions to practice. The majority of applicants preferred practicing in cities with >500,000 people (64.5%), with only 7.0% choosing cities with 0 to 100,000 people. Respondents were evenly split in preference for academic versus nonacademic jobs. Overall, >72% of respondents received a job offer in their preferred region, job type, population size or job type (independently). Furthermore, 52.5% received a job offer in their preferred region, city size, and job type (combined). Which this suggests a lower level of concern than suggested in prior reports.
Further examination of factors does suggest that RO trainees’ personal preferences may be contributing to the geographic RO maldistribution. Specifically, we found those with ties to the MW (RO training, medical schooling, raised in MW) preferred to stay in the MW less frequently than people with ties to other regions. Of note, there was a subset of 23 respondents who were from the MW and also underwent both medical schooling and RO training in the MW, of whom 19 (82.6%) chose the MW as their top region to practice. Those who preferred to practice in the MW were more likely to prefer a job in smaller cities (<200,000) than those who preferred other regions. One potential solution to improve maldistribution is for RO programs to prioritize these geographic factors when assessing applicants. Interestingly, those who had a spouse who grew up in the MW were least likely (<60% vs >70% for all other regions) to choose their respective region as their top location to practice. It is possible that the MW poses unique challenges for physicians attempting to balance their personal career choice with those of their spouse.10
Our study does contain some limitations inherent to surveys. To limit selection bias, we compared our survey demographics (sex, year of graduation, residency training region) with those from the ACGME Data Resource Book11 and National Resident Matching Program Results12 and found no significant differences between the samples. To limit nonresponse bias, we compared responses between early and late responders and found no significant differences between the 2 for all questions. Finally, we cannot make formal conclusions regarding applicants’ regional preferences without accounting for salary, practice size, partnership model, and academic time, among others; however, much of this data is not public and was beyond the scope of this project.
Conclusions
In this study, recent RO graduates demonstrate a strong preference for working in large cities (>500,000) and had less interest in practicing in the MW. Those with ties to the MW (RO training, medical schooling, raised in MW) may prefer to practice in their respective region less frequently than people with ties to other regions. Despite the disparities in regional preference, the majority (75%) of respondents received a job offer in their preferred region. A multifaceted approach to help correct job market deficiencies is needed, involving ASTRO, RO residency programs, and RO trainees.
Supplementary Material
Acknowledgments—
The authors would like to acknowledge and thank all the recent graduates who completed the survey.
Research reported in this publication was supported in part by the Biostatistics and Bioinformatics Shared Resource of Winship Cancer Institute of Emory University and National Institutes of Health/National Cancer Institute under award number P30CA138292. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Conflict of interest: none.
Supplementary material for this article can be found at https://doi.org/10.1016/j.ijrobp.2018.12.026.
References
- 1.Nabavizadeh N, Burt LM, Mancini BR, et al. Results of the 2013–2015 Association of Residents in Radiation Oncology Survey of Chief Residents in the United States. Int J Radiat Oncol Biol Phys 2016;94:228–234. [DOI] [PubMed] [Google Scholar]
- 2.Burt LM, Trifiletti DM, Nabavizadeh N, et al. Supply and demand for radiation oncology in the United States: A resident perspective. Int J Radiat Oncol Biol Phys 2017;97:225–227. [DOI] [PubMed] [Google Scholar]
- 3.Fung CY, Chen E, Vapiwala N, et al. The American Society for Radiation Oncology 2017 Radiation Oncologist Workforce Study. Int J Radiat Oncol Biol Phys 2019;103:547–556. [DOI] [PubMed] [Google Scholar]
- 4.Fung CY. The changing face of the radiation oncology work force Top finding from the ASTRO Workforce Subcommittee’s 2017 Workforce Study. ASTROnews, Vol 20 Arlington, VA: American Society for Radiation Oncology; 2018;13–14. [Google Scholar]
- 5.Aneja S, Smith BD, Gross CP, et al. Geographic analysis of the radiation oncology workforce. Int J Radiat Oncol Biol Phys 2012;82:1723–1729. [DOI] [PubMed] [Google Scholar]
- 6.Chowdhary M, Chhabra AM, Switchenko JM, et al. Domestic job shortage or job maldistribution? A geographic analysis of the current radiation oncology job market. Int J Radiat Oncol Biol Phys 2017;99:9–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chowdhary M, Chhabra AM, Jhaveri J, et al. In reply to Royce. Int J Radiat Oncol Biol Phys 2018;100(2):530–531.. [DOI] [PubMed] [Google Scholar]
- 8.US Census Bureau. Geographic terms and concepts-Census divisions and census regions. Available at: https://www.census.gov/geo/reference/gtc/gtc_census_divreg.html. Accessed September 28, 2017.
- 9.Hoddinott SN, Bass MJ. The Dillman total design survey method. Can Fam Physician 1986;32:2366–2368.. [PMC free article] [PubMed] [Google Scholar]
- 10.Staiger DO, Marshall SM, Goodman DC, et al. Association between having a highly educated spouse and physician practice in rural underserved areas. JAMA 2016;315:939–941. [DOI] [PubMed] [Google Scholar]
- 11.Department of Applications and Data Analysis. ACGME Data Resource Book, Academic Year 2015–2016. Chicago: Accredidation Council for Graduate Medical Education; 2016. Accessed July 20, 2018. [Google Scholar]
- 12.National Resident Matching Program. Data and reports; specialties matching service 2013–2017. Available at: http://www.nrmp.org/match-data/nrmp-historical-reports/. Accessed July 20, 2018.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.