

Abstract
Objective
To determine the correlation between portal vein diameter and spleen size (craniocaudal).
Methodology
The study was conducted at the University Ultrasound Clinic, The University of Lahore, Lahore Pakistan from 1st January to 1st July 2013. All the individuals who referred for abdominal sonographic examination, including male, female, older and younger were conveniently included in the study, voluntarily, irrespective of the disease state. Ultrasonographic measurements of the caudocranial length of the spleen and portal vein were carried out on all of the one thousand subjects. The subject position for spleen was supine or right posterior oblique during suspended inspiration and right anterior oblique position for portal vein diameter with quiet respiration. The correlation between the splenic length and portal vein diameter was evaluated.
Result
A total of 1000 subjects; 36.9% females and 63.1% males aged from 4 to 79 years. The mean splenic length was 10.29 ± 1.89 cm. The mean portal vein diameter was 10.27 ± 1.78 mm. A statistically significant correlation was found between the spleen size and portal vein diameter; the Pearson correlation was significant at the 0.01 level.
Conclusion
Portal vein diameter is directly correlated to splenic caudocranial length. A regression formula was developed to measure the splenic length from the calculation of portal vein diameter.
Keywords: spleen, portal vein, portal hypertension, chronic liver parenchymal disease, splenomegaly
Introduction
The left upper quadrant is most frequently assessed with sonography in patients with enlarged spleen or in the case of trauma(1). The advantages of sonography over other imaging modalities include: portability of the equipment, which allows the sonographer for rapid evaluation of the patient at the bedside, the non-invasive nature of ultrasound, negligible bioeffects, etc.(1) The rapid development and modernization of modalities is another great advantage of ultrasonography(2). Apart from all other advantages, the sonographic examination is interactive, real-time and dynamic(3). Patients could easily be maneuvered, moved, deep breathed, compressed and other provocative measures may be applied. Transducer approach could also be changed, more superficial access could be achieved from deeper access(4). Ultrasound is a multiplanar modality, multiple planes could be acquired instead of relying on a single plane(5). Therefore, the importance of ultrasound grows day by day with regard to the evaluation of superficial musculoskeletal structures, nerves, and deep gynecological, obstetrical and abdominal structures(6). Sonography can easily differentiate abdominal structures like liver, gall bladder, pancreases, intestinal walls, abdominal vasculature and spleen, etc.(3) The normal texture of the spleen is very homogeneous, slightly more echogenic than the texture of the liver; therefore, pathology or blood collection secondary to a splenic rupture is usually easily identified. We may also examine portal vein status by means of sonography with regard to the portal vein diameter, hypertension, obstruction, thrombus and collaterals(3,7,8).
The spleen is the largest single mass of lymphoid tissue and part of the reticuloendothelial system, it is located in the left upper quadrant of the abdomen, just below the diaphragm(9,10). In embryonic and early fetal life, it actively participates in blood formation (hematopoiesis), however, blood formation activity decreases gradually by the 5th to 6th month of pregnancy, when the spleen discontinues its hematopoietic activities and assumes its adult characteristics(11,12). The spleen plays a major role in the defensive mechanism of the body (reticuloendothelial system)(13). The spleen rarely become the primary site of disease however it is often affected by systemic disease processes(14). Sonographically, like hepatic parenchyma, the splenic parenchyma appears to have a fine uniform homogeneous mid to low-level echo-pattern(15). The texture of the spleen is actually considered to be more echogenic than the one of the liver(16). Like all other abdominal organs, the echogenicity of the spleen increases with development, maturation and enlargement(17,18).
Portal vein (PV) is formed by the joining of superior mesenteric vein and splenic vein while forming porto--splenic confluence, posterior to the pancreas at the level of L2(19). Portal vein is located 5 to 7 cm from porto-splenic confluence to the bifurcation in right and left portal vein at porta-hepatis(20,21). The portal vein courses posteriorly to the first portion of the duodenum and then between the layers of the lesser omentum to the porta-hepatis. It bifurcates in the liver into its right and left portal veins and then successively bifurcates to give raise to its terminal branches in the hepatic sinusoids(20,22). Blood of the gastrointestinal tract, (from the lower end of the esophagus to the upper end of the anal canal), pancreas, gallbladder, bile ducts, and spleen is drained by the portal vein to the liver and finally to IVC through hepatic veins(10). The portal vein has an anastomosis with the esophageal veins, rectal venous plexus, and superficial abdominal veins. The liver receives a dual blood supply from the portal vein and the hepatic artery(23). The portal triad contains branches of the portal vein, hepatic artery, and bile duct. These structures are enclosed within a connective tissue sheath that gives the portal vein an echogenic wall appearance on sonography(24).
The splenic vein is formed by the union of several veins at the splenic hilum. It is subsequently joined by the short gastric and left gastroepiploic veins(25). The splenic vein runs along the posteromedial border of the pancreas. It joins the superior mesenteric vein posterior to the neck of the pancreas to form the portal vein. Additional veins from the pancreas and inferior mesenteric vein drain into the splenic vein(10,26). The splenic vein drains blood from the stomach, spleen, and pancreas into the portal vein(27). In the case of hepatic congestion, resistance occurs in the blood flow of portal vein and ultimately splenic vein(28,29). Pressure build-up in the portal vein due to the excessive amount of blood pooling which causes portal hypertension and ultimately increases in portal vein diameter(30). On the other hand, blood congestion in the spleen causes splenomegaly, therefore splenomegaly is correlated to portal vein diameter(31). Apart from the hepatic fibrosis and congestion, splenomegaly could be caused by a number of diseased conditions, suchas: hematologic disorder, Rheumatologic disorders, infectious diseases, and infiltrative disorders(10). However, hepatic congestion is the most common cause of splenomegaly and portal hypertension(28,32). Therefore, we observed that raises in Portal vein diameter increase the splenic caudocranial length at the same ratio. However, this research was intended to test the hypothesis of a correlation between splenic caudocranial length and portal vein diameter.
Methodology
A cross-sectional analytical study was performed from 1st January 2013 to 1st July 2013, at the University Ultrasound Clinic, University of Lahore, Gilani Ultrasound Center Lahore, Pakistan, and Shah Doppler Ultrasound Clinic, Pubi (Peshawar), Pakistan. One thousand subjects were enrolled, with no limits as to the age, gender and disease restrictions, except for liver transplant and gastric varices. All the participants were enrolled in this study voluntarily, the procedure was explained to them and written informed consent was obtained. Pre-approval was obtained from the institutional review board (IRB) and the ethical committee of the University of Lahore. Toshiba (Xario) with Convex transducer frequency ranging 3.0–6.0 MHz, having Color & Power Doppler and Tissue harmonics imaging facilities, Toshiba (Nemio-17) with Convex transducer frequency ranging 3.5–6.0 MHz, having Color & Power Doppler and Tissue harmonics imaging facilities, and Aloka (SSD 3500) with Convex transducer frequency 3.5 MHz, having Color & Power Doppler with Tissue harmonics facilities were applied. Data was collected during the allocated period. The spleen size was measured in the longitudinal plane while the patient was lying in supine or right posterior oblique position and scanned during suspended inspiration. Portal vein measurement has been carried out in longitudinal section in supine and right anterior oblique position. The portal vein diameter was measured in quiet respiration at porta hepatis (near Porta hepatis). The diameter was measured by putting the two cursors in the lumen of the portal vein; the walls of the portal vein were excluded from the measurement.
Statistical Package for the Social Sciences (SPSS) version 24 (SPSS 24, IBM, Armonk, Ny, United States of America) software was used for the evaluation of data and formation of graphs. The results were summarized in the form of graphs, tables, and charts. Descriptive data is explained in the form of frequency, mean and standard deviation. The data was analyzed via Pearson correlation and linear regression analysis.
Results
A total of 1000 patient, 369 (36.9%) female and 631 (63.1%) male participants were included in the study. Patients’ ages ranged between 4 and 79 years with the mean of 32.92±16.8, and the rest of descriptive measurements are specified in table 1. A statistically strong correlation was found between the caudocranial length of the spleen and portal vein diameter with P-value (0.000), the correlation was significant at less than 0.01 level and R-value (0.98), which is near to 1, represents a strong positive relationship (Tab. 2, Fig. 1). Regression between Splenic caudocranial length and portal vein diameter was calculated at 95% confidence interval, the values of coefficients, intercept and slope (alpha and beta) and standard deviations with upper and lower limits are presented in Tab. 3.
Tab. 1.
Age, Spleen caudocranial length, and portal vein diameter
| Variable | N | Range | Minimum | Maximum | Mean | Standard deviation | Standard error |
|---|---|---|---|---|---|---|---|
| Age in years | 1000 | 75.00 | 4.00 | 79.00 | 32.5600 | 16.80 | 1.680 |
| Spleen size (cm) | 1000 | 10.16 | 6.84 | 17.00 | 10.2918 | 1.8908 | 0.18 |
| Portal vein (mm) | 1000 | 9.20 | 6.80 | 16.00 | 10.2759 | 1.7875 | 0.17 |
Tab. 2.
Correlations between spleen size and portal vein diameter
| Variables | Correlation | Spleen in cm | Portal vein in mm |
|---|---|---|---|
| Spleen size in cm | Pearson correlation | 1 | 0.990** |
| Sig. (2-tailed) | 0.000 | ||
| Number of subjects | 8 | 8 |
Correlation is significant at the 0.01 level (2-tailed).
Fig. 1.
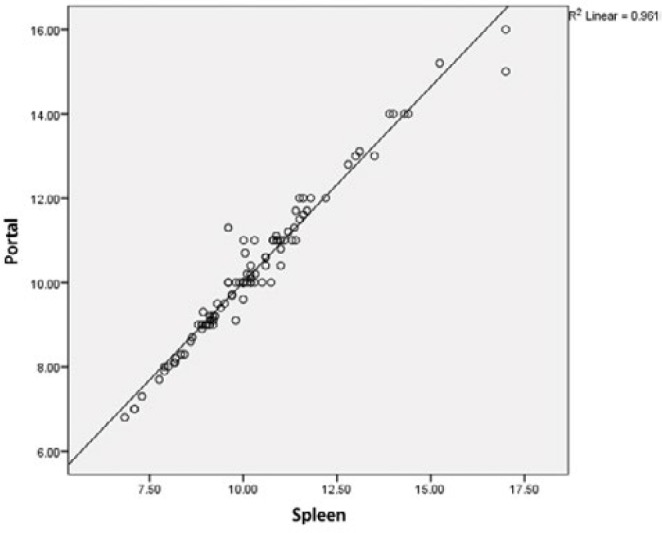
Scatterplot shows correlation of spleen size in (cm), portal vein diameter in (mm)
Tab. 3.
Coefficients for the regression model of splenic size and portal vein diameter
| Model | Unstandardized coefficients | Standardized coefficients | t | Sig | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| 1 | (Constant) | 0.737 | 0.197 | 3.742 | 0.000 |
| Spleen | 0.927 | 0.19 | 0.980 | 49.199 | 0.000 |
a. Dependent variable: portal vein
The formula for the calculation of portal vein diameter:
To calculate portal vein diameter from the measurement of splenic caudocranial length, the following formula is derived from a simple regression modal as shown in Tab. 3, Fig. 1.
| (1) |
where “y” represents portal vein diameter and “x” represents Splenic craniocaudal length, whereas “ᾴ” is intercept 0.737 and “ß” slope is 0.927.
When putting these values in equation 1, the following equation will be obtained.
| (2) |
Portal vein diameter could easily be calculated from the above equation simply by adding the value of Caudocranial length of the spleen.
Example: If the spleen caudocranial length is 10.0 cm, then the PV diameter will be calculated as follows: 0.737 + 0.927 × 10 = 10.0 mm
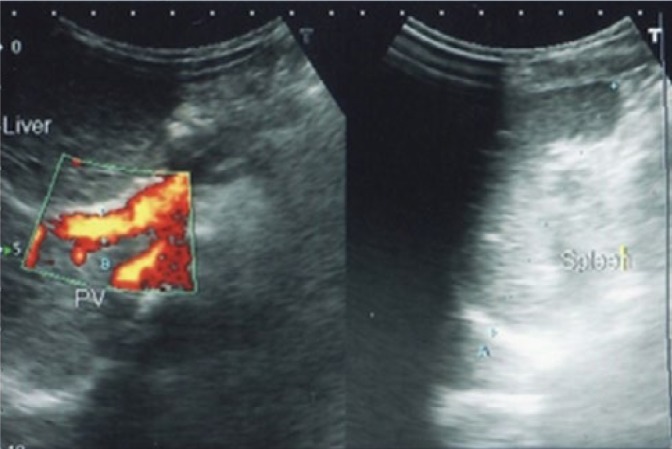
It is obvious that portal vein diameter increases with an increase in splenic size as shown in a series of ultrasound images (Fig. 2, Fig. 3).
Fig. 2.
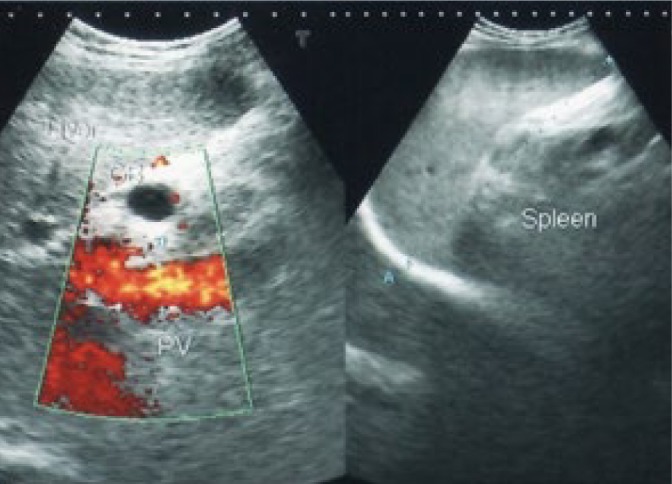
Spleen size = 15.24 cm, portal vein diameter = 15.2 mm
Fig. 3.
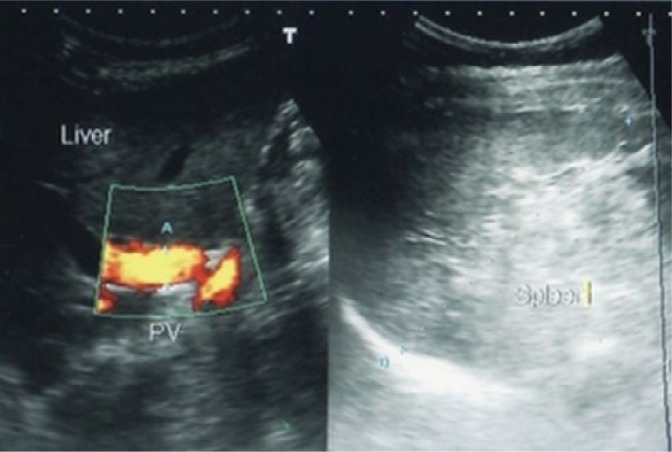
Spleen size = 10.01 cm, portal vein diameter = 11 mm
Discussion
It was an analytical study; the purpose of this research work was to sonographically assess the relationship between spleen craniocaudal length and portal vein diameter that has been observed frequently in ultrasound practice. Real-time sonography is the most accurate and reliable method of assessing the portal vein diameter. Ultrasound is frequently used to examine the spleen to assess its size and texture, it is an easy and non-invasive technique and can be used safely at any age. Studies have proved the high reliability and accuracy of ultrasound in the measurement of the diameter of the portal vein and size of the spleen. The size may inform on the diagnosis and prognosis of disease courses, while the portal vein diameter is useful in evaluating splenic-portal conditions as shown in a series of ultrasound Fig. 2, Fig. 3, Fig. 4.
Fig. 4.
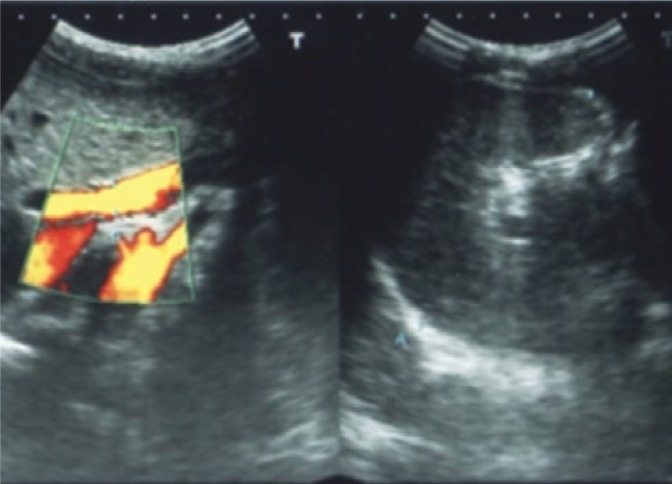
Spleen size = 8.64 cm, portal vein diameter = 8.7 mm
A study by Rosenberg et al. was carried out to determine the clinical significance of splenic size(33). The authors found that a simple measurement of splenic length served as a guide to spleen size. The authors proposed the upper normal limit of splenic length at 12 cm for girls aged 15 or older and at 13 cm for boys aged 15 or older; in another study performed by Dittrich et al., it was observed that there was an approximately linear increase in spleen size, as measured on sonography, in the course of development in the pediatric population and that spleen size correlated best with the body height(34). Konus et al. conducted a study on the pediatric population of 307 subjects and they found that height is correlated best with spleen length(35). In a study on adults, Frank et al. used conventional sonography to evaluate 793 healthy subjects (17–82 years) and found that 95% of patients had a splenic length of less than 11 cm, a width (transverse dimension) of less than 7 cm, and a thickness of less than 5 cm(36). Niederau et al. studied 915 healthy subjects using sonography and determine the mean longitudinal and transverse diameters of the spleen to be 5.8 ± 1.8 cm and 5.5 ± 1.4 cm, respectively. These dimensions are much smaller than those obtained in other studies, as the authors did not measure the maximal length of the spleen as authors did in other studies, but rather the true superior to inferior length. This study further found that spleen size correlated poorly with height in the general population(37,38). To determine normal spleen dimensions, Hosey RG, et al. conducted a study in 2006, in British journal of sports(11). For this purpose, they recruited 631 athletes from the Division I university. It was observed that the mean spleen length was 10.65 cm and mean width equaled to 5.16 cm. They correlated the size of the spleen of men with the spleens in women and found a significant correlation of spleen size with gender. Men had larger spleens than women had. They further determine the correlation of white-American with African-American individuals. There was also a significant correlation among the spleen size of the white individual and African individuals. White-American population had significantly larger spleens than African-American subjects had. Baik and Kim, published their work in 2018, to determine the role of Doppler ultrasound in the diagnosis of chronic liver parenchymal disease.10 Various factors, including the liver size, liver surface nodularity, spleen length, and splenic vein respiratory variation and portal vein blood flow velocity, showed a diagnostic accuracy ranging from 73% for the diagnosis of significant fibrosis, to 84% for severe fibrosis(39).
To determine the clinical application of ultrasound, O’Donohue et al. conducted a study on 45 patients with chronic liver parenchymal disease and 49 healthy individuals(9). They established a normal reference value for spleen size and portal vein diameter from the normal controls. The mean spleen size was 10.7 cm in normal, it was significantly associated with height and weight but not with body mass and age. In male patients, spleen was significantly larger than in female patients. The mean portal vein diameter was 9.6 mm. The mean spleen size was 16.0 cm in patients with chronic liver parenchymal disease, which is significantly larger than in normal individuals. The mean portal vein diameter in cirrhotic patients with standard deviation was 10.8 mm. They concluded that spleen size and portal vein diameter increase with liver congestion. Subash Bhattarai, et al. observed 150 patients with chronic liver parenchymal disease, to determine the role of portal vein diameter and spleen size in the prognosis of gastroesophageal varices(40). They observed mean portal vein diameter to be 10.800 mm in patients who do not suffer from varices, and 13.731 mm in patients with varices. Mean spleen size of patients with no varices was 12.67 cm and 15.367 cm in participant with varices. There was 92.72 % sensitivity and 90 % specificity for the portal vein diameter of 12.25 mm, and 94.5 % sensitivity, 75% specificity for the spleen size of 13.9 cm, to predict gastro-esophageal varices. Our hypothesis was based on the concept of splenic length increase with an increase in portal vein diameter, the relation is shown in the scatterplot (Fig. 1). We observed similar results as obtained in previous studies, howeverwe correlated splenic size with portal vein diameter as shown in a series of figures (Fig. 2, Fig. 3, Fig. 4, Fig. 5). As there was a linear correlation between portal vein diameter and splenic length, therefore we present a logistic regression model and an example for elaboration (Formula in results).
Fig. 5.
Spleen size = 6.84 cm, portal vein diameter = 6.8 mm
Conclusion
Portal vein diameter and splenic craniocaudal length are linearly correlated. An increase in the spleen size may linearly predict an increase in the portal vein diameter in the case of chronic liver parenchymal disease (liver congestion).
Footnotes
Conflict of interest
Authors do not report any financial or personal connections with other persons or organizations, which might negatively affect the contents of this publication and/or claim authorship rights to this publication.
References
- 1.Richards JR, McGahan JP: Focused Assessment with Sonography in Trauma (FAST) in 2017: what radiologists can learn. Radiology 2017; 283: 30–48. [DOI] [PubMed] [Google Scholar]
- 2.Postema A, Idzenga T, Mischi M, Frinking P, de la Rosette J, Wijkstra H: Ultrasound modalities and quantification: developments of multipara-metric ultrasonography, a new modality to detect, localize and target prostatic tumors. Curr Opin Urol 2015; 25: 191–197. [DOI] [PubMed] [Google Scholar]
- 3.Manzoor I, Bacha R, Gilani SA: Diagnostic accuracy of sonoelastography in different diseases. J Ultrason 2018; 18: 29–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bacha R, Gilani SA: Ultrasound diagnosis of spontaneous nephrocutaneous fistula. Ultrasound Q 2017; 33: 293–295. [DOI] [PubMed] [Google Scholar]
- 5.Gilani SA: An overview of musculoskeletal ultrasound – A thirteen years experience in Pakistan. Perspectives in Medicine 2012; 1: 427–430. [Google Scholar]
- 6.Gilani SA: Musculoskeletal ultrasound. Cerebrovascular Diseases 2011; 31: 2–3. [Google Scholar]
- 7.Vancauwenberghe T, Snoeckx A, Vanbeckevoort D, Dymarkowski S, Vanhoenacker FM: Imaging of the spleen: what the clinician needs to know. Singapore Med J 2015; 56: 133–144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mazur R, Celmer M, Silicki J, Hołownia D, Pozowski P, Międzybrodzki K: Clinical applications of spleen ultrasound elastography – a review. J Ultrason 2018; 18: 37–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.O’Donohue J, Ng C, Catnach S, Farrant P, Williams R: Diagnostic value of Doppler assessment of the hepatic and portal vessels and ultrasound of the spleen in liver disease. Eur J Gastroenterol Hepatol 2004; 16: 147–155. [DOI] [PubMed] [Google Scholar]
- 10.Baik SK, Kim MY: Diagnostic methods for cirrhosis and portal hypertension: imaging: ultrasound and doppler ultrasonography In: Baik SK, Kim MY (ed.): Diagnostic Methods for Cirrhosis and Portal Hypertension. Springer, 2018: 139–147. [Google Scholar]
- 11.Hosey RG, Mattacola CG, Kriss V, Armsey T, Quarles J, Jagger J: Ultrasound assessment of spleen size in collegiate athletes. Br J Sports Med 2006; 40: 251–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Görg C, Eichkorn M, Zugmaier G: The small spleen: sonographic patterns of functional hyposplenia or asplenia. J Clin Ultrasound 2003; 31: 152–155. [DOI] [PubMed] [Google Scholar]
- 13.de Porto AP, Lammers AJ, Bennink RJ, ten Berge IJ, Speelman P, Hoekstra JB: Assessment of splenic function. Eur J Clin Microbiol Infect Dis 2010; 29: 1465–1473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Toma P, Granata C, Rossi A, Garaventa A: Multimodality imaging of Hodgkin disease and non-Hodgkin lymphomas in children. Radiographics 2007; 27: 1335–1354. [DOI] [PubMed] [Google Scholar]
- 15.Chiorean L, Zdrenghea M, Badea R: Ultrasonography of the spleen. Pictorial essay. Med Ultrason 2014; 16: 48–59. [DOI] [PubMed] [Google Scholar]
- 16.Schmidt G: Differential diagnosis in ultrasound imaging: a teaching Atlas Thieme, 2011. [Google Scholar]
- 17.Virmani J, Kumar V, Kalra N, Khandelwal N: Prediction of liver cirrhosis based on multiresolution texture descriptors from B-mode ultrasound. Int J Convergence Computing 2013; 1: 19–37. [Google Scholar]
- 18.Rossi F, Leone VF, Vignoli M, Laddaga E, Terragni R: Use of contrast-enhanced ultrasound for characterization of focal splenic lesions. Vet Radiol Ultrasound 2008; 49: 154–164. [DOI] [PubMed] [Google Scholar]
- 19.Görg C, Riera-Knorrenschild J, Dietrich J: Pictorial review: colour doppler ultrasound flow patterns in the portal venous system. Br J Radiol 2002; 75: 919–929. [DOI] [PubMed] [Google Scholar]
- 20.Park HS, Desser TS, Jeffrey RB, Kamaya A: Doppler ultrasound in liver cirrhosis: correlation of hepatic artery and portal vein measurements with model for end-stage liver disease score. J Ultrasound Med 2017; 36: 725–730. [DOI] [PubMed] [Google Scholar]
- 21.Gareeballah A, Hassan IA, Elzaki M, Ibraheem SS, Abelwahab B, Siddig A et al. : Measurement of normal portal vein using ultrasound in Sudanese. Glob Adv Res J Med Med Sci 2017; 6: 336–340. [Google Scholar]
- 22.Weis J, Schlosser S, Müller-Schilling M: Challenging HCC surveillance in a case with a history of peliosis hepatis and liver cirrhosis CHILD A due to a hypoplastic portal vein. Z Gastroenterol 2018; 56: E2–E89. [Google Scholar]
- 23.Coysh T, Zonoozi S, Jayasooriya N, Cargill Z, Burn-Murdoch A, Yalchin M et al. : PTU-073 Title: is portal vein diameter being reported in abdominal ultrasound scans of decompensated liver cirrhosis patients? Gut 2017; 66: 87–95. [Google Scholar]
- 24.Badi Y, Badro N, Dhawan S: Portal vein thrombosis: the overlooked association between pancreatic cancer and PVT. Oncol Cancer Case Rep 2017; 3: 1–2. [Google Scholar]
- 25.Roy S, Bhatt S, Rawal R, Tandon A, Meena N: Splenic vein thrombosis as a rare complication of disseminated tuberculosis – imaging diagnosis and case report. Pol J Radiol 2017; 82: 106–109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tokodai K, Miyagi S, Nakanishi C, Hara Y, Nakanishi W, Miyazawa K et al. : The utility of superb microvascular imaging for monitoring low-velocity venous flow following pancreas transplantation: report of a case. J Med Ultrason 2018; 45: 171–174. [DOI] [PubMed] [Google Scholar]
- 27.Christou N, Dib N, Chuffart E, Taibi A, Durand-Fontanier S, Valleix D et al. : Stepwise management of hepatocellular carcinoma associated with Abernethy syndrome. Clin Case Rep 2018; 6: 930–934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Benson CB, Frates MC: Color Duplex Scanning of the Hepatoportal Circulation In: Benson CB, Frates MC (ed.): Noninvasive vascular diagnosis. Springer, 2017: 623–646. [Google Scholar]
- 29.Mills A, Mellnick V: Imaging features of hepatic arterial and venous flow abnormalities. Clin Liver Dis 2018; 11: 27–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Luisa S, Vitale G, Sorbo AR, Maurizio P, Lodovico RG: Hepatic vein transit time of second-generation ultrasound contrast agent: new tool in the assessment of portal hypertension. J Ultrasound 2016; 20: 43–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kievit L, Kræmer P, Hamilton-Dutoit S, Grønbæk H: Adult presentation of noncirrhotic portal hypertension and ascites following treatment for Wilms’ tumor in childhood. Case Rep Gastroenterol 2018; 12: 56–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Endo M, Soroida Y, Sato M, Kobayashi T, Hikita H, Sato M et al. : Ultrasound evaluation of liver stiffness: accuracy of ultrasound imaging for the prediction of liver cirrhosis as evaluated using a liver stiffness measurement. J Med Dent Sci 2017; 64: 27–34. [DOI] [PubMed] [Google Scholar]
- 33.Rosenberg HK, Markowitz RI, Kolberg H, Park C, Hubbard A, Bellah RD: Normal splenic size in infants and children: sonographic measurements. AJR Am J Roentgenol 1991; 157: 119–121. [DOI] [PubMed] [Google Scholar]
- 34.Dittrich M, Milde S, Dinkel E, Baumann W, Weitzel D: Sonographic biometry of liver and spleen size in childhood. Pediatr Radiol 1983; 13: 206–211. [DOI] [PubMed] [Google Scholar]
- 35.Konuş OL, Ozdemir A, Akkaya A, Erbaş G, Celik H, Işik S: Normal liver, spleen, and kidney dimensions in neonates, infants, and children: evaluation with sonography. AJR Am J Roentgenol 1998; 171: 1693–1698. [DOI] [PubMed] [Google Scholar]
- 36.Frank K, Linhart P, Kortsik C, Wohlenberg H: Sonographic determination of spleen size: normal dimensions in adults with a healthy spleen. Ultraschall Med 1986; 7: 134–137. [DOI] [PubMed] [Google Scholar]
- 37.Spielmann AL, DeLong DM, Kliewer MA: Sonographic evaluation of spleen size in tall healthy athletes. AJR Am J Roentgenol 2005; 184: 45–49. [DOI] [PubMed] [Google Scholar]
- 38.Niederau C, Sonnenberg A, Müller JE, Erckenbrecht JF, Scholten T, Fritsch WP. Sonographic measurements of the normal liver, spleen, pancreas, and portal vein. Radiology 1983; 149: 537–540. [DOI] [PubMed] [Google Scholar]
- 39.Aubé C, Oberti F, Korali N, Namour MA, Loisel D, Tanguy JY et al. : Ultrasonographic diagnosis of hepatic fibrosis or cirrhosis. J Hepatol 1999; 30: 472–478. [DOI] [PubMed] [Google Scholar]
- 40.Bhattarai S, Gyawali M, Dewan KR, Shrestha G, Patowary BS, Sharma P: Study of portal vein diameter and spleen size by ultrasonography and their association with gastro-esophageal varices. Nepalese Journal of Radiology 2017; 4: 6-14. [Google Scholar]