

Abstract
Recruiting schools for intervention research can be daunting. This study examined the experiences of researchers recruiting public high schools for a randomized controlled trial to reduce suicide disparities for sexual and gender minority (SGM) youth by implementing evidence-based strategies to enhance school environments. We enrolled 42 schools throughout New Mexico between August 2016 and April 2017. Based on qualitative analysis of recruitment efforts, three groups of factors affected enrollment: (1) non-SGM-specific factors, (2) SGM-specific factors, and (3) facilitating factors. Non-SGM-specific factors negatively impacted the willingness or ability to participate (e.g., demanding staff workloads and beliefs that “outsiders” should not assist with school-based interventions). Notable SGM-specific factors centered on influences in socially conservative community environments and beliefs that schools lacked SGM students. Advocacy, leveraging relationships, and persistence were facilitating factors for overcoming recruitment obstacles. Our findings have implications for researchers and school nurses interested in school-based interventions, especially those focused on SGM youth.
Keywords: high school, school nurse characteristics, sexual and gender minority, recruitment, qualitative research, youth
Decreasing youth suicide in the United States is a national public health priority (National Action Alliance for Suicide Prevention Research Prioritization Task Force, 2014), and students who are sexual and gender minority (SGM) are at particularly high risk (Grossman, Park, & Russell, 2016; Stone et al., 2014). The abbreviation SGM refers to people who are lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ), have varying sexual orientations or gender identities, or identify as two-spirit, asexual, gender-nonconforming, gender fluid, or intersex (National Institutes of Health Sexual and Gender Minority Research Coordinating Committee, 2016). In terms of importance for suicide prevention, a safe and supportive school environment is second only to a safe and supportive home (Centers for Disease Control and Prevention [CDC], 2009; Ethier, Harper, & Dittus, 2018). School nurses are ideally positioned to advocate for SGM youth and for policies and practices providing for the safety of all students (Bradley et al., 2013). We initiated a 5-year study, “Implementing School Nursing Strategies to Reduce LGBTQ Adolescent Suicide” (RLAS), to facilitate adoption and scale-up of evidence-based strategies to improve high school environments for SGM youth (Willging, Green, & Ramos, 2016). Recommended by the CDC, these strategies include adopting bullying and harassment prohibitions, enhancing access to community health and mental health providers who are SGM-sensitive, developing school staff professionally, and incorporating SGM-specific information into health education curricula (Brener et al., 2017). The strategies also center on having “safe spaces” on campus, such as SafeZones and Genders and Sexualities Alliances (or Gay-Straight Alliances). Such initiatives foster SGM inclusivity and exert positive effects on student health (Brener et al., 2017; Marx & Kettrey, 2016; Poteat, Heck, Yoshikawa, & Calzo, 2017; Poteat, Yoshikawa, Calzo, Russell, & Horn, 2017). Finally, this study capitalizes on the role of school nurses and other school personnel in leading implementation of the strategies as part of a 5-year cluster-randomized trial occurring in 42 public high schools in New Mexico, a rural and ethnically diverse state.
Recruitment is a challenge in any school-based study. However, research regarding stigmatized populations may pose greater challenges due to possible prejudice in communities. Schools are complex institutions situated in state-, district-, and community-level systems that can influence involvement in research (Hooper & Britnell, 2012; Stinch-field & Zyromski, 2010). Although gaining access to these institutions for study purposes differs across districts and individual schools, the literature points to several considerations for researchers. For example, participation in research is typically not a top priority for schools (Befort et al., 2008; Cupp, Zimmerman, Massey, Howell, & Swan, 2006; Olds & Symons, 1990; Renes, Ringwalt, Clark, & Hanley, 2007). Rather, the academic mission of schools is generally the first concern for administrators (Befort et al., 2008), especially in the face of state-mandated student assessments, overworked staff, and time constraints (Blinn-Pike, Berger, & Rea-Holloway, 2000; Harrell, Bradley, Dennis, Frauman, & Criswell, 2000; Hooven, Walsh, Willgerodt, & Salazar, 2011; Petosa & Goodman, 1991; Renes et al., 2007). In this light, researchers must make participation attractive to schools and their personnel, which can be accomplished by making the advantages of their involvement explicit, fully communicating expectations prior to enrollment, minimizing burdens on staff, using local advocates to facilitate inclusion, and establishing relationships with major decision makers (Blinn-Pike et al., 2000; Bosma et al., 2010; Hooper & Britnell, 2012; Hooven et al., 2011; Petosa & Goodman, 1991; Stinchfield & Zyromski, 2010).
For randomized controlled trials, successful recruitment of schools may also depend on making the control condition attractive (Befort et al., 2008; Petosa & Goodman, 1991). School administrators or staff may choose not to take part in trials if they perceive no direct benefit to their institutions. To mitigate this concern, establishing a delayed intervention condition in place of a nonintervention control condition or comparing the focal intervention against an established pro-gram are optimal choices that may maintain the continued interest of school-based participants, including those assigned to control conditions (Harrington et al., 1997). For these reasons, the RLAS study randomized schools into either an intervention group receiving immediate technical assistance to implement the evidence-based strategies or a delayed-intervention group that will be given this assistance after a 3-year waiting period.
School administrators also weigh the credibility of the study and its research staff along with levels of controversy associated with the research topic in their decisions to participate. Anticipating that the research will be viewed negatively in conservative communities or contribute to parental upset may also bear upon the decisions of school administrators (Befort et al., 2008). Such barriers are likely germane to research on SGM youth in communities considered to be socially conservative or otherwise less accepting of such populations.
Method
The purpose of the current study is to examine issues impacting the inclusion of schools in research pertaining to SGM students. We draw upon qualitative analysis of detailed recruitment logs compiled by research staff engaged in enrolling schools into the RLAS study. This study was reviewed and approved by the Pacific Institute for Research and Evaluation Institutional Review Board (IRB) and school district research review boards as appropriate.
Recruitment Process
Following IRB approval, recruitment occurred between August 2016 and April 2017. Utilizing a purposive sampling framework, research team members collaborated with the health and public education departments of the State of New Mexico to develop a comprehensive contact list of public high school nurses statewide. Initial e-mail invitations were distributed to these nurses, followed by phone calls to share information about the study and determine the school’s eligibility to participate. During these calls, the school personnel we contacted verbally agreed to speak with our research staff about reasons for or against participating in the study.
Eligibility was initially limited to schools that had at least one half-time nurse on site and had taken part in the 2015 New Mexico Youth Risk and Resiliency Survey (NMYRRS). The NMYRRS is the New Mexico iteration of the CDC’s Youth Risk Behavior Surveillance Survey (YRBSS), a population-based survey of high school students administered by state, territorial, tribal, and local agencies in most states biennially. The NMYRRS provides the RLAS study with essential baseline and outcome data. We later expanded recruitment to public and charter schools with less than half-time nurses and to those that had professional providers at school-based health centers and then reinvited the schools previously deemed ineligible. On-reservation public schools were excluded due to time line considerations in pursuing research approval. To increase interest, a school health official from the state government circulated a sup-port letter to school administrators throughout New Mexico. We also obtained assistance from our community advisory board, representing stakeholders in the fields of health, nursing, education, and youth advocacy. The board members guided study efforts and helped with outreach to schools.
The recruitment process often required multiple contacts with school nurses and other personnel to address concerns raised in each school and to schedule in-person appointments to share study information. Once meetings were scheduled, a researcher met with school nurses or designated team leads and administrators (e.g., principals) to answer questions about the study, verify the school’s eligibility and willingness to participate, and complete school enrollment using procedures described in a separate publication (Willging et al., 2016). Over 900 contacts were made at 145 public high schools. A total of 42 schools (28.9% of those contacted) enrolled in the study (see Figure 1). For nonparticipating schools, the average time between initial contact and declination was 82 days (range = 2–209). For those schools that enrolled, the average time between initial contact and agreement was 129 days (range = 6–252). Of the final sample of schools, 64% were in urban areas and 36% in rural areas. On average, the size of the student body for each school that agreed to participate was 1,014 (range = 25–2,507).
Figure 1.
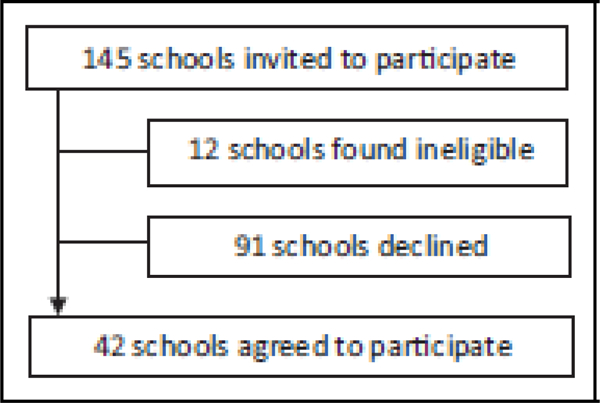
Overview of recruitment efforts.
Data Collection and Analysis
We documented each contact or attempted contact in a recruitment log maintained in the form of written field notes. The field notes included information regarding the person contacted and their position, topics discussed, plans for future engagement, the outcomes of each contact, and team member impressions of the interaction. The field notes were then coded by hand using open and focused coding techniques to analyze responses to our recruitment efforts for each school contacted. Codes were developed around themes identified in the broader literature, that is, demanding staff workloads, time constraints, and state-mandated student assessments. In addition, research staff created new codes according to themes that had emerged within the field notes, that is, conservative community environments and beliefs that schools did not have SGM students or already had sufficient supports in place for such students. Open coding captured both a priori and emergent themes. Next, focused coding was used to refine code assignments and themes and determine which themes were most prevalent and which represented infrequent concerns or were isolated to individual schools. Two team members independently coded the field notes, organized codes into overarching sets of factors affecting participation, and shared their work with the larger team for review (Corbin & Strauss, 2008; Glaser & Strauss, 1967).
Results
We identified three groups of factors affecting school participation: non-SGM-specific challenges, SGM-specific challenges, and facilitating factors. Non-SGM-specific challenges were general school environment factors inducing impediments to participation, while SGM-specific challenges surfaced as factors complicating participation in an explicitly SGM-focused initiative. Facilitating factors were those either enabling or helping to overcome barriers to school participation. We must also note that many of the reasons that school personnel (particularly administrators) provided for not participating were nonspecific, such as the study not being “a fit for our school at this time,” or a very simple but final “the answer is no.” Motivations underlying declinations are difficult to discern from these types of responses.
Non-SGM-Specific Factors
Non-SGM-specific factors were present across most schools. School personnel were often charged with demanding workloads that included the performance of duties falling outside their typical job descriptions. Especially in smaller school districts, administrators and staff undertook work that would normally be assigned to multiple personnel in a larger district. Across the state, school nurses—originally conceptualized by researchers as the main implementers for the strategies—covered one or more schools or were assigned to very large schools with com-plex caseloads without sufficient support. Many school nurses and other staff approached about the study expressed concerns about having the time to participate. School administrators frequently echoed this sentiment, indicating that they did not want to “overburden” staff.
Second, some school personnel did not want to be in a study led by a team outside their school, district, or community. Summing up this view, one nurse said, “Our principal doesn’t want someone coming into our school to implement policy or provide training.” The same principal and others expressing similar concerns simply declined to meet with researchers.
SGM-Specific Factors
Some factors impacting school participation were more unambiguously related to the focus on SGM students. Among the schools we approached, it was common for personnel to claim that they already had sufficient supports in place for SGM students. This sentiment was expressed primarily in larger school districts in metropolitan areas where some SGM resources or services were available, although personnel in smaller districts also asserted that they were “very inclusive and supportive of diverse students.” Narratives that all students should be treated equally (Willging, Salvador, & Kano, 2006) were often invoked by school personnel to politely excuse themselves from participation, regardless of the presence or absence of SGM resources.
School staff concerns about the conservative nature of surrounding communities also influenced participation. Such concerns were mostly raised in small rural communities where school personnel worried about being socially ostracized for becoming involved in the study. Staff feared resistance to initiatives concerning SGM students that fell outside of the hetero/cis-normative worldviews imputed to members of the community. Some staff also offered examples to team members that accentuated concerns about their community’s conservatism, for instance, observing resistance to the presence of a school-based health center that provided sexual and reproductive health services. One individual cited a prominent local leader who publicly stoked fear about “the homosexual agenda” within their community. Personnel across many schools identified religious or cultural backgrounds of the community as a major source of this tension.
Additionally, a very small number of school administrators and staff stated that there were no SGM students at their school, thus not warranting involvement of their institution in an initiative concentrating on such students. From other data sources like the NMYRRS, we know this absence to be unlikely. In some cases, administrators or staff reported not knowing any SGM students, and in one case, a school nurse stated that she did not think there were “many of those students at school, and those that are don’t usually come out until after they have graduated.” This invisibility or erasure of SGM students and the acknowledgment that those who do exist only choose to come out after graduation provided impetus for further conversation between research staff and schools, although efforts to secure participation were unsuccessful.
Finally, some school personnel expressed opinions that focusing on SGM students was “inappropriate.” Several principals indicated that their main rationale for not allowing their schools to take part in this study was the focus on SGM students, rather than the entire student population. Further exploration revealed a belief in “treating everyone the same” and perceptions that other issues adversely affecting students were equally or more important to address.
Facilitating Factors
Despite the many hurdles to participation, 42 schools agreed to take part in the RLAS study. For these schools, we identified the presence of one or more facilitating factors as positively influencing decisions to participate. The three facilitating factors that emerged were (1) advocacy, (2) relationships, and (3) persistence. First, self-identified advocates stepped forward to support the study and enroll their schools. In some cases, despite resistance at administrative or district levels, the passion that individuals in schools had for the study led to successful recruitment. For example, the efforts of one school nurse who self-identified as a former “mental health nurse and strong advocate for students” were critical to enrolling a school in a particularly conservative community. Elsewhere, the school nurse was “very interested” yet apprehensive because she was new to her school and community. With support from staff of the local school-based health center, and persistence on her part, she garnered administrative approval for the study. In several other schools, nurses who were “supportive” but unable to participate due to workload were vital to identifying others, such as social workers, counselors, and health educators, to become champions at their schools. Finally, having a family member or close friend who was SGM engendered buy in and commitment from various school personnel.
The second key facilitating factor centered on the role of relationships. Professional relationships were leveraged in the recruitment process to navigate potential challenges detailed in the literature. Several recruited schools were ones where the research team already had a professional relationship with a school nurse, counselor, social worker, or administrator. For example, one social worker explained that once she saw the names of study staff, she knew it was “legit” and “wanted in” based on previous studies. The endorsement of, and strong partnership with, the New Mexico School Nurses Association was also pivotal in establishing credibility with school nurses in the field. Further, colleagues from the state government were crucial in identifying and reaching out to individuals at high schools whom they thought might be interested in the study. Several school administrators commented on their increased interest when contacted personally by a study advisory board member affiliated with the state government. Another structural relationship that facilitated participation was having a direct supervisor who was enthusiastic about the study from the outset. Indeed, by garnering buy in from a district school nurse supervisor, the study enrolled four schools in the same district.
A third key facilitating factor was persistence. Even for schools with staff supportive of the study, time constraints and workloads made final enrollment and eventual participation in data collection (e.g., qualitative interviews) problematic; yet participants expressed gratitude for the research team’s patience and tenacity. Many school nurses indicated that they were “just too busy” at the beginning of the school year, but follow-up e-mails and phone calls resulted in several of them either enrolling their schools or identifying other staff. One principal (who ultimately agreed to participate) voiced her appreciation for the “pleasant persistence” of our researchers in following up when she had not returned phone calls. In another case, a school-based health center coordinator offered to take on the study while the principal was still skeptical, even after initially agreeing to allow the school to participate. After multiple attempts over several months to interview the principal, the research staff was finally able to sit down with him, adjusted interview tactics (no recording, only notes, modifying number of questions and their ordering) to address his hesitancies, and spoke openly to address his concerns. The patience, persistence, and flexibility of research staff was critical to finalizing his school’s enrollment and maintaining engagement in the beginning stages of implementation.
Discussion
Meticulous logging of each contact in field notes allowed us to identify factors affecting the recruitment of schools for intervention research on SGM youth, underscoring the critical importance of advocates in schools, building and lever-aging of relationships, and persistence. For some schools, a combination of background constraints, such as demanding school staff workloads, socially conservative environments, and beliefs that “outsiders” should not assist with school-based interventions, in the absence of facilitating factors influenced declinations. For others, the combined difficulties presented by demanding workloads, beliefs that sufficient supports for SGM students were already in place locally, and a socially conservative community environment were in themselves enough to limit participation. Findings from this statewide effort confirm the work of other scholars on the difficulties of recruiting for school-based research studies (Befort et al., 2008; Blinn-Pike et al., 2000; Cupp et al., 2006; Harrell et al., 2000; Hooven et al., 2011; Olds & Symons, 1990; Petosa & Goodman, 1991; Renes et al., 2007), particularly randomized clinical trials (Petosa & Smith, 2018). In addition, scholars recently contemplating the benefits and challenges of conducting research in school settings highlight similar themes, including the relevance of relationship building and trust in the research team, logistics (e.g., demanding workloads and time constraints), and perceived sensitivity and importance of the research topic (Bartlett et al., 2017). Because the topic itself can influence receptivity to research among school personnel, it behooves researchers to do their homework ahead of time, learning as much as possible about philosophies or ideologies prevailing in the targeted schools and surrounding communities to tailor their outreach approach accordingly. This research sought to understand how to facilitate recruitment even in instances when the topic may not align well with school and community priorities. Barriers to participation described in the literature still hold, and the SGM focus of our research likely contributed to difficulties recruiting schools. How-ever, our study also points to the vital roles that researchers, school nurses, and other champions can play in maintaining steadfastness, leveraging relationships, and advocating for the well-being of a stigmatized youth population, to successfully enroll schools in research to improve the health of SGM students despite the presence of obstacles to recruitment.
Implications for School Nursing and School Health Services Research
School nursing implications.
The 2016 National School Nurse Association (NASN) position statement on the role of the school nurses in supporting SGM students clearly states that school nurses are leaders who should work to foster a safe and supportive school environment for SGM youth (National Association of School Nurses, 2016). This position statement emphasizes that school nurses are uniquely qualified to understand health inequities for SGM students and to collaborate with school and community members to improve outcomes. Additionally, the position statement points to the role of the school nurse as an advocate for policies and practices to support SGM students. There is currently a need for rigorous research to understand how to best support SGM students (Heck, Poteat, & Goodenow, 2016). Such research must rely on the collaborations and advocacy fundamental to the role of the school nurse (Wain-wright, Thomas, & Jones, 2000). Our results point to the role of advocacy and relationships in facilitating school participation in research on SGM youth. The NASN suggests that school nurses can be best prepared as advocates by developing relationships with key stakeholders, including regularly attending meetings of the local board of education or parent–teacher association/organizations. The use of anecdotes about interactions with SGM students and the need to find evidence-based ways to reduce disparities can also serve effectively as advocacy tools for school nurses, particularly when shared with opinion leaders and decision makers (National Association of School Nurses, n.d.). By engaging with researchers and heartily promoting the merits and production of a solid evidence base to strengthen sup-port for and protect SGM students, school nurses can lead both their schools and the nation in reducing devastating disparities for this often marginalized population.
Research implications.
Our results also have implications for research and surveillance initiatives aiming to include queries regarding SGM status. For example, as more states and territories begin to include questions on their local iterations of the nationwide YRBSS to collect vital information related to the sexual orientation and gender identity of students, they may experience many of the struggles we faced in recruiting schools for the RLAS study. Greater under-standing of the challenges and facilitating factors encountered in the current study may enhance efforts to enroll public high schools for this important national surveillance of adolescent health risk behaviors.
Research recruitment in schools requires detailed planning, time, and perseverance, particularly when the research topic may be perceived as sensitive or even opposed by others. School nurses and academic researchers who are prepared to address the challenges and highlight the advantages of research related to SGM students are crucial to addressing the overall public health urgency for SGM-focused research to reduce health disparities.
Acknowledgments
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01HD083399).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
References
- Bartlett R, Wright T, Olarinde T, Holmes T, Beamon ER, & Wallace D (2017). Schools as sites for recruiting participants and implementing research. Journal of Community Health Nursing, 34, 80–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Befort C, Lynch R, James RL, Carroll SL, Nollen N, & Davis A (2008). Perceived barriers and benefits to research participation among school administrators. Journal of School Health, 78, 581–586. doi: 10.1111/j.1746-1561.2008.00349.x [DOI] [PubMed] [Google Scholar]
- Blinn-Pike L, Berger T, & Rea-Holloway M (2000). Conducting adolescent sexuality research in schools: Lessons learned. Family Planning Perspectives, 32, 246–251. doi: 10.1363/3224600 [DOI] [PubMed] [Google Scholar]
- Bosma LM, Sieving RE, Ericson A, Russ P, Cavender L, & Bonine M (2010). Elements for successful collaboration between K-8 school, community agency, and university part-ners: The lead peace partnership. Journal of School Health, 80, 501–507. doi: 10.1111/j.1746-1561.2010.00534.x [DOI] [PubMed] [Google Scholar]
- Bradley B, Kelts S, Robarge D, Davis C, Delger S, & Comp-ton L (2013). NASN position statement: Sexual orientation and gender identity/expression (sexual minority students): School nurse practice. NASN School Nurse, 28, 112–113. [DOI] [PubMed] [Google Scholar]
- Brener ND, Demissie Z, McManus T, Shanklin SL, Queen B, & Kann L (2017). School health profiles 2016: Character-istics of health programs among secondary schools. Atlanta, GA: Centers for Disease Control and Prevention. [Google Scholar]
- Centers for Disease Control and Prevention. (2009). School connectedness: Strategies for increasing protective factors among youth. Atlanta, GA. Retrieved from https://www.cdc.gov/healthyyouth/protective/pdf/connectedness.pdf
- Corbin J, & Strauss A (2008). Basics of qualitative research: Techniques and procedures for developing grounded theory (3rd ed). Thousand Oaks, CA: Sage. [Google Scholar]
- Cupp PK, Zimmerman RS, Massey CS, Howell JR, & Swan R (2006). Using community ties to facilitate school- based prevention research. Health Promotion Practice, 7, 459–466. doi: 10.1177/1524839905278870 [DOI] [PubMed] [Google Scholar]
- Ethier KA, Harper CR, & Dittus PJ (2018). School environment is related to lower health and safety risks among sexual minority middle and high school students. Journal of Adolescent Health, 62, 143–148. doi: 10.1016/j.jadohealth.2017.08.024 [DOI] [PubMed] [Google Scholar]
- Glaser BG, & Strauss AL (1967). The discovery of grounded theory: Strategies for qualitative research. New York, NY: Aldine de Gruyter. [Google Scholar]
- Grossman AH, Park JY, & Russell ST (2016). Transgender youth and suicidal behaviors: Applying the interpersonal psychological theory of suicide. Journal of Gay & Lesbian Mental Health, 20, 329–349. doi: 10.1080/19359705.2016.1207581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harrell JS, Bradley C, Dennis J, Frauman AC, & Criswell ES (2000). School-based research: Problems of access and consent. Journal of Pediatric Nursing, 15, 14–21. doi: 10.1016/S0882-5963(00)80019-6 [DOI] [PubMed] [Google Scholar]
- Harrington KF, Binkley D, Reynolds KD, Duvall RC, Copeland JR, Franklin F, & Raczynski J (1997). Recruit-ment issues in school-based research: Lessons learned from the high 5 Alabama project. Journal of School Health, 67, 415–421. doi: 10.1111/j.1746-1561.1997.tb01287.x [DOI] [PubMed] [Google Scholar]
- Heck NC, Poteat VP, & Goodenow CS (2016). Advances in research with LGBTQ youth in schools. Psychology of Sexual Orientation and Gender Diversity, 3, 381–385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooper LM, & Britnell HB (2012). Mental health research in K-12 Schools: Translating a systems approach to university- school partnerships. Journal of Counseling and Development, 90, 81–90. [Google Scholar]
- Hooven C, Walsh E, Willgerodt M, & Salazar A (2011). Increasing participation in prevention research: Strategies for youths, parents, and schools. Journal of Child and Adolescent Psychiatric Nursing, 24, 137–149. doi: 10.1111/j.1744-6171.2011.00288.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marx RA, & Kettrey HH (2016). Gay-straight alliances are associated with lower levels of school-based victimization of LGBTQ youth: A systematic review and meta-analysis. Journal of Youth and Adolescence, 45, 1269–1282. [DOI] [PubMed] [Google Scholar]
- National Action Alliance for Suicide Prevention Research Prioritization Task Force. (2014). A prioritized research agenda for suicide prevention: An action plan to save lives. Washington, DC. Retrieved from http://actionallianceforsuicideprevention.org/sites/actionallianceforsuicideprevention.org/files/Agenda.pdf
- National Association of School Nurses. (2016). LGBTQ students: The role of the school nurse (Position Statement). Silver Spring, MD. Retrieved from https://www.nasn.org/advocacy/professional-practice-documents/position-statements/ps-lgbtq
- National Association of School Nurses. (n.d.). Advocacy skill building. Retrieved from https://www.nasn.org/nasn/advocacy/advocacy-skill-building
- National Institutes of Health Sexual and Gender Minority Research Coordinating Committee. (2016). NIH FY 2016–2020 strategic plan to advance research on the health and well-being of sexual and gender minorities. Rockville, MD. Retrieved from https://dpcpsi.nih.gov/sites/default/files/sgmStrategicPlan.pdf
- Olds RS, & Symons CW (1990). Recommendations for obtaining cooperation to conduct school-based research. Journal of School Health, 60, 96–98. [DOI] [PubMed] [Google Scholar]
- Petosa RL, & Goodman RM (1991). Recruitment and retention of schools participating in school health research. Journal of School Health, 61, 426–429. doi: 10.1111/j.1746-1561.1991.tb05991.x [DOI] [PubMed] [Google Scholar]
- Petosa RL, & Smith L (2018). Effective recruitment of schools for randomized clinical trials: Role of school nurses. The Journal of School Nursing, 34, 430–434. doi: 10.1177/1059840517717592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poteat V, Heck NC, Yoshikawa H, & Calzo J (2017). Gay- straight alliances as settings to discuss health topics: Individual and group factors associated with substance use, mental health, and sexual health discussions. Health education research, 32, 258–268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poteat VP, Yoshikawa H, Calzo JP, Russell ST, & Horn S (2017). Gay-straight alliances as settings for youth inclusion and development: Future conceptual and methodological directions for research on these and other student groups in schools. Educational Researcher, 46, 508–516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renes SL, Ringwalt C, Clark HK, & Hanley S (2007). Great minds don’t always think alike: The challenges of conducting substance abuse prevention research in public schools. Journal of Drug Education, 37, 97–105. [DOI] [PubMed] [Google Scholar]
- Stinchfield TA, & Zyromski B (2010). A training model for school, family, and community collaboration. Family Journal, 18, 263–268. [Google Scholar]
- Stone DM, Luo F, Ouyang L, Lippy C, Hertz MF, & Crosby AE (2014). Sexual orientation and suicide ideation, plans, attempts, and medically serious attempts: Evidence from local youth risk behavior surveys, 2001–2009. American Journal of Public Health, 104, 262–271. doi: 10.2105/AJPH.2013.301383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wainwright P, Thomas J, & Jones M (2000). Health promotion and the role of the school nurse: A systematic review. Journal of Advanced Nursing, 32, 1083–1091. [DOI] [PubMed] [Google Scholar]
- Willging CE, Green AE, & Ramos MM (2016). Implementing school nursing strategies to reduce LGBTQ adolescent suicide: A randomized cluster trial study protocol. Implementation Science, 11, 145. doi: 10.1186/s13012-016-0507-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Willging CE, Salvador M, & Kano M (2006). Unequal treatment: Mental health care for sexual and gender minority groups in a rural state. Psychiatric Services, 57, 867–870. doi: 10.1176/appi.ps.57.6.867 [DOI] [PubMed] [Google Scholar]