

Abstract
Background
Infants in the neonatal intensive care unit (NICU) are subjected to stress, including sound of high intensity. The sound environment in the NICU is louder than most home or office environments and contains disturbing noises of short duration and at irregular intervals. There are competing auditory signals that frequently challenge preterm infants, staff and parents. The sound levels in NICUs often exceed the maximum acceptable level of 45 decibels (dB), recommended by the American Academy of Pediatrics. Hearing impairment is diagnosed in 2% to 10% of preterm infants versus 0.1% of the general paediatric population. Noise may cause apnoea, hypoxaemia, alternation in oxygen saturation, and increased oxygen consumption secondary to elevated heart and respiratory rates and may, therefore, decrease the amount of calories available for growth. Elevated levels of speech are needed to overcome the noisy environment in the NICU, thereby increasing the negative impacts on staff, newborns, and their families. High noise levels are associated with an increased rate of errors and accidents, leading to decreased performance among staff. The aim of interventions included in this review is to reduce sound levels to 45 dB or less. This can be achieved by lowering the sound levels in an entire unit, treating the infant in a section of a NICU, in a 'private' room, or in incubators in which the sound levels are controlled, or reducing the sound levels that reaches the individual infant by using earmuffs or earplugs. By lowering the sound levels that reach the neonate, the resulting stress on the cardiovascular, respiratory, neurological, and endocrine systems can be diminished, thereby promoting growth and reducing adverse neonatal outcomes.
Objectives
Primary objective
To determine the effects of sound reduction on growth and long‐term neurodevelopmental outcomes of neonates.
Secondary objectives
1. To evaluate the effects of sound reduction on short‐term medical outcomes (bronchopulmonary dysplasia, intraventricular haemorrhage, periventricular leukomalacia, retinopathy of prematurity).
2. To evaluate the effects of sound reduction on sleep patterns at three months of age.
3. To evaluate the effects of sound reduction on staff performance.
4. To evaluate the effects of sound reduction in the neonatal intensive care unit (NICU) on parents' satisfaction with the care.
Search methods
We searched the Cochrane Central Register of Controlled Trials (The Cochrane Library), MEDLINE, EMBASE, CINAHL, abstracts from scientific meetings, clinical trials registries (clinicaltrials.gov; controlled‐trials.com; and who.int/ictrp), Pediatric Academic Societies Annual meetings 2000 to 2014 (Abstracts2ViewTM), reference lists of identified trials, and reviews to November 2014.
Selection criteria
Preterm infants (< 32 weeks' postmenstrual age (PMA) or < 1500 g birth weight) cared for in the resuscitation area, during transport, or once admitted to a NICU or a stepdown unit.
Data collection and analysis
We performed data collection and analyses according to the Cochrane Neonatal Review Group.
Main results
One small, high quality study assessing the effects of silicone earplugs versus no earplugs qualified for inclusion. The original inclusion criteria in our protocol stipulated an age of < 48 hours at the time of initiating sound reduction. We made a deviation from our protocol and included this study in which some infants would have been > 48 hours old. There was no significant difference in weight at 34 weeks postmenstrual age (PMA): mean difference (MD) 111 g (95% confidence interval (CI) ‐151 to 374 g) (n = 23). There was no significant difference in weight at 18 to 22 months corrected age between the groups: MD 0.31 kg, 95% CI ‐1.53 to 2.16 kg (n = 14). There was a significant difference in Mental Developmental Index (Bayley II) favouring the silicone earplugs group at 18 to 22 months corrected age: MD 14.00, 95% CI 3.13 to 24.87 (n = 12), but not for Psychomotor Development Index (Bayley II) at 18 to 22 months corrected age: MD ‐2.16, 95% CI ‐18.44 to 14.12 (n =12).
Authors' conclusions
To date, only 34 infants have been enrolled in a randomised controlled trial (RCT) testing the effectiveness of reducing sound levels that reach the infants' ears in the NICU. Based on the small sample size of this single trial, we cannot make any recommendations for clinical practice. Larger, well designed, conducted and reported trials are needed.
Plain language summary
Sound reduction management in the neonatal intensive care unit for preterm or very low birthweight infants
Background: Infants in the neonatal intensive care unit (NICU) are subjected to stress, including high intensity sound. The sound environment in the NICU is louder than most home or office environments and contains disturbing noises of short duration and at irregular intervals. There are competing sound signals that frequently challenge preterm infants, staff, and parents. The sound levels in NICUs range from 7 dB to 120 dB, often exceeding the maximum acceptable level of 45 dB, recommended by the American Academy of Pediatrics. Hearing impairment is diagnosed in 2% to 10% of preterm infants versus 0.1% of the general paediatric population. Noise may cause apnoea, hypoxaemia, alternation in oxygen saturation, and increased oxygen consumption secondary to elevated heart and respiratory rates and may, therefore, decrease the amount of calories available for growth. Elevated levels of speech are needed to overcome the noisy environment in the NICU, thereby increasing the negative impacts on staff, newborns, and their families. High noise levels are associated with an increased rate of errors and accidents, leading to decreased performance among staff. The aim of all interventions considered for inclusion in this review is to reduce the sound levels that reach the individual neonate to 45 dB or less. This can be achieved by lowering the sound levels in an entire unit, treating the infant in a section of a NICU or in a 'private' room, or in incubators in which the sound levels are controlled, or reducing the sound levels that reaches the individual infant by using earmuffs or earplugs. By lowering the sound levels that reach the neonate, the resulting stress can be diminished, thereby promoting growth and reducing adverse neonatal outcomes.
Results: This review identified only one small, high quality study that used earplugs to reduce the sound level that reached the newborn infant. There was a trend for better growth at 34 weeks postmenstrual age (PMA). The Mental Developmental Index at 18 to 22 months was higher in the silicone earplug group that included six infants compared to the control group that included six infants.
Conclusions: To date only 34 preterm infants have been enrolled in a single randomised controlled trial (RCT) studying the effects of noise reduction and no recommendations for clinical practice can be made. Further research is needed.
Background
Pathophysiology
Sound is defined as a vibration in air that has intensity, frequency, periodicity, and duration (AAP 1997). The frequency of sound is measured in Hertz (Hz). The normal human ear hears between 20 Hz and 20,000 Hz (Morris 2000). The pressure of sound is expressed using decibels (dB). Noise is defined as an undesirable sound that interferes with communication of voice or music and causes pain or disorder in the ear (Kawada 2004).
The acoustic environment of the foetus is rich and varied and sounds below 200 Hz to 300 Hz are transmitted to the foetus. Foetuses respond to sound as manifested by changes in behavioural state variables, such as heart rate variability, and eye and breathing movements (Abrams 2000). In one prospective observational study of working military women, a significant effect of noise exposure on preterm labour (P = 0.001) but not on preterm birth (P = 0.300) was identified (Magann 2005). Five of the fourteen women exposed to noise for greater than 28 weeks had preterm labour compared with 61 out of 800 for the rest of the women (P = 0.003). This difference did not reach significance for preterm birth (P = 0.104) (Magann 2005).
Infants in the neonatal intensive care unit (NICU) are subjected to stress, including sound of high intensity (Anagnostakis 1980; Lotas 1992). The sound environment in the NICU is louder than most home or office environments and contains disturbing noises of short duration and at irregular intervals (Lasky 1995). There are competing auditory signals that frequently challenge preterm infants, staff, and parents (Gray 2004). The sound levels in NICUs range from 7 dB to 120 dB (Anagnostakis 1980; Philbin 2000; Chang 2001; Kent 2002; Johnson 2003), often exceeding the maximum acceptable level of 45 dB, recommended by the American Academy of Pediatrics (AAP 1997). The maximum acceptable level of 45 dB by the American Academy of Pediatrics was based on a report by the Environmental Protection Agency, Office of Noise Abatement and Control (EPA 1974).
Preterm infants are susceptible to negative effects of environmental stimuli due to central nervous system immaturity (Blackburn 1998), and decreased autonomic and self regularity abilities to deal with stress (Bowden 2000). They are unable to co‐ordinate autonomic responses to environmental and tactile stimulation until 32 to 34 weeks' postmenstrual age (PMA) (Bowden 2000). As a result of excessive stimuli, neurons may form alternative pathways between the cerebral cortex and the brainstem (Catlett 1990). Preterm infants born before 28 weeks' PMA have an immature auditory system (Birnholz 1983; Lary 1985; Philbin 1999). Myelination of the auditory pathway continues after birth (Letko 1992). Microscopic analyses of the cochlea of neonates have shown that hair cells are still in a process of differentiation (Beckham 1982; Rubel 1985; Kent 2002).
Burden of illness
Hearing impairment is diagnosed in 2% to 10% of preterm infants versus 0.1% of the general paediatric population (Carter 1991). There is evidence for synergy between noise, hypoxia, apnoea and hyperbilirubinaemia in causing hearing impairment (Stennert 1978; Winkel 1978; Anagnostakis 1982). Stennert 1978 demonstrated that 52% of infants treated in incubators had abnormal audiograms suggestive of noise‐induced hearing impairment. Outer hair cell damage has been shown in young guinea pigs exposed to noise levels above 80 dB (Douek 1976).
Description of the condition
Noise‐induced stress reactions in the infant
Two narrative reviews on physiological effects of sound/noise on newborns treated in the NICU were conducted 10 years apart (Morris 2000; Wachman 2011). The cardiac response to acoustic stimulation depends on behavioural state, history of previous sound exposure, predisposing conditions of the central nervous system, antenatal and perinatal events, postnatal age of the infant and PMA at birth. High intensity noise may cause either bradycardia or tachycardia. In low birth weight infants, both high‐ and low‐frequency sound stimulation result in a 10 mm Hg increase in systolic and diastolic blood pressure above baseline (Morris 2000; Wachman 2011).
Noise may cause apnoea, hypoxaemia, alternation in oxygen saturation and increased oxygen consumption secondary to elevated heart and respiratory rates and may, therefore, decrease the amount of calories available for growth (Morris 2000; Wachman 2011).
The electrical activity of the central nervous system changes in response to acoustic stimulation in the range between 36 dB and 90 dB. Increases in intracranial pressure and electromyographic and behavioural changes have been noted in newborns in response to sudden noise. Excessive sound may influence the neuroendocrine system and may have an indirect effect on immunity (Morris 2000; Wachman 2011).
The stress responses listed above, including bradycardia or tachycardia, increase in systolic and diastolic blood pressure, apnoea, hypoxaemia, alteration in oxygen saturation, increased oxygen consumption and increase in intracranial pressure, could potentially increase the risk for adverse outcomes such as poor growth, abnormal sleep patterns, hearing impairment, bronchopulmonary dysplasia, retinopathy of prematurity, intraventricular haemorrhage, periventricular leukomalacia, and developmental delay. Schell et al noted that animal studies have established that noise is a stressor and that animal growth is inhibited by noise exposure. They suggested that stress affects growth through the endocrine system. Stress from noise activates the hypothalamic‐pituitary‐adrenal axis, and causes growth‐inhibiting effects possibly through the action of corticosteroids. Birth weights among humans have been shown to be reduced in relation to noise exposure (Schell 2006). Perlman states: "Many clinical factors, (i.e. chronic lung disease, recurrent apnoea and bradycardia, transient hyperthyroxinaemia of prematurity, hyperbilirubinaemia, nutritional deficiencies, glucocorticoid exposure), as well as stressful environmental conditions, including infant–provider interaction, constant noise, and bright light, may act in combination to impact on the developing brain, even in the absence of overt haemorrhage and/or ischemia" (Perlman 2001). It thus seems plausible that a reduction in the noise levels that reach a preterm infant while in the NICU might reduce these adverse outcomes.
Noise‐induced stress reactions among staff
Efforts have been made to characterise noise that interferes with communication and work, and that are annoying and distracting for adults (Lasky 1995). Elevated levels of speech are needed to overcome the noisy environment in the NICU, thereby increasing the negative impacts on staff, newborns and their families (Lasky 1995). High noise levels are associated with an increased rate of errors and accidents leading to decreased performance among staff (Hétu 1994; Lasky 1995).
In one meta‐analysis of 31 studies of nurses' job satisfaction, Zangaro 2007 examined the relationships between job satisfaction and autonomy, job stress, and nurse‐physician collaboration among registered nurses working in staff positions. Job satisfaction was most strongly negatively correlated with job stress.
Noise has been recognised as a risk factor for work‐related stress in Her Majesty's Coastguard (Kingdom 2011). Blomkvist 2005 studied the acoustics and psychosocial environment in an intensive coronary critical care unit in Sweden. The aim of the study was to examine the influence of different acoustic conditions on the work environment and the staff in the coronary critical care unit. Psychosocial work environment data from the start and end of each individual shift were obtained from morning, afternoon and night shifts for a one‐week baseline period and for two four‐week periods during which either sound‐reflecting or sound‐absorbing tiles were installed. Reverberation times and speech intelligibility improved during the study period when the ceiling tiles were changed from sound‐reflecting tiles to sound‐absorbing ones of identical appearance. Improved acoustics positively affected the work environment; the afternoon shift staff experienced significantly lower work demands and reported less pressure and strain. The authors concluded that important gains in the psychosocial work environment of health care can be achieved by improving room acoustics. According to the authors: "The study points to the importance of further research on possible effects of acoustics in health care on staff turnover, quality of patient care, and medical errors" (Blomkvist 2005). Poor communication among intensive care unit nurses and doctors has been found to be a common causal factor underlying critical incidents in intensive care (Reader 2007).
Description of the intervention
The aim of all interventions included in this review is to reduce the sound levels that reach the individual neonate to 45 dB or less. This can be achieved by lowering the sound levels in an entire unit (to be studied in cluster randomised trials ‐ the individual NICU is the unit of randomisation), treating the infant in a section of a NICU, or in a 'private' room, or in incubators in which the sound levels are controlled, or reducing the sound levels that reaches the individual infant by using earmuffs or earplugs (to be studied in RCTs in which the unit of randomisation is the individual patient).
In 1997, the American Academy of Pediatrics (AAP 1997) recommended sound levels not to exceed 45 dB in NICUs (which frequently occurs in current practice) (Lasky 2009). The maximum acceptable level of 45 dB was based on a report by the Environmental Protection Agency, Office of Noise Abatement and Control (EPA 1974). The interventions included in this review are aimed at reducing the sound levels to below 45 dB for 24 hours or shorter periods of a day/night shift and continued over weeks (at least to 34 weeks' PMA) at the level of the NICU or the individual neonate.
Reduction in sound levels in general in an entire NICU or in a separate part of a NICU
Reductions in sound levels can be achieved in an entire NICU or in an individual patient room by architectural remodelling (Philbin 2002). Interventions include education of caregivers and parents to achieve behavioural changes to decrease sound levels (Philbin 2002; Ramesh 2009). Sound levels can be monitored and electronically recorded for long periods of time using a sound level meter with computing and data storage capabilities (dosimeter) (Philbin 2002). As sound levels vary by location and over 24 hours in a NICU (Ramesh 2009; Matook 2010), it is important that the monitoring is ongoing in various locations of the NICU, including inside the incubators (Pinheiro 2011). Environmental changes in the NICU aimed at reducing the sound levels might even increase decibel levels as described by Brandon et al after installation of motion‐sensing motorised paper towel dispensers and the introduction of a new communication system (Brandon 2007). It is of note that two centres, using primarily human behaviour noise reduction strategies, were unable to demonstrate measurable improvements in sound levels within the occupied open‐unit design NICU (Liu 2010). A single‐family room level 3 NICU is a quieter, less loud environment compared with the open‐unit level 3 NICU when the patient is supported on room air, high flow nasal cannula, bubble continuous positive airway pressure and conventional ventilation. High‐frequency ventilation results in similar measurements to the open‐unit level 3 bedside NICU (Liu 2012). In our experience, the sound levels in the resuscitation area can be very high, especially when several neonates are resuscitated simultaneously. We have not been able to identify any study that measured the sound levels in that area. Any innovative, developmentally sensitive intervention should start at birth in the resuscitation room, where neonates are exposed to excessive noise and light levels and painful/stressful stimuli to body parts (mouth, nose, throat, larynx and hands) represented by large areas in the sensory cortex (Ohlsson 2009). The sensory receptor in the minute cochlea occupies an area of the cortex comparable to that occupied by an area as large as the skin of the whole face. The cortex in this area, measuring about 3 mm in depth, is thicker than in other sensory fields (Fisch 1983).
In a prospective cohort study 136 preterm infants (< 30 weeks PMA) were assigned to a bed space in an open ward or in a private room within the same hospital, based on space and staffing availability (Pineda 2014). The infants remained in the location to which they were first assigned for the whole duration of their hospital stay. The primary outcome was developmental performance at two years of age measured using the Bayley Scales of Infant and Toddler Development, 3rd Edition. Eighty‐six infants returned for testing (83% of survivors). At age two years, infants cared for in private rooms had lower language scores (average difference in Bayley score ‐8.3; 95% CI ‐14.2 to ‐2.4) and a trend toward lower motor scores (average difference in Bayley score ‐6.3; 95% CI ‐11.7 to ‐0.99) compared to infants cared in an open ward. The differences persisted after adjustment for potential confounders (Pineda 2014). The authors concluded that "these findings raise concerns that highlight the need for further research into the potential adverse effects of different amounts of sensory exposure in the NICU environment" (Pineda 2014). In an accompanying editorial in The Journal of Pediatrics, Dr. Jobe wrote: "The optimal types and frequencies of stimulations for development of the very preterm brain are unknown, but isolation of these infants in relatively dark and quiet private rooms may be going in the wrong direction" (Jobe 2014). Commonly recommended interventions as part of the Newborn Individualized Developmental Care and Assessment Program (NIDCAP®) include incubator covers and lowering of sound levels in the NICU, which have not been shown to be effective in improving developmental outcomes (Ohlsson 2013).
Reduction in sound levels for an individual infant
Reduction in sound levels that reach the individual neonate only can be achieved by the use of earmuffs/earplugs or by the use of sound‐reducing incubator covers. Sound levels in an incubator during actual flight conditions in four common medically configured aircrafts were measured (Sittig 2011). The incubator provided a 6 dB decrease in noise exposure from that in the crew cabin, but the average noise level in the incubator was still close to 80 dB (Sittig 2011).
Initiation and duration of the intervention
Ideally the sound reducing intervention should start at birth and be implemented during resuscitation, during transport from a referring hospital to a NICU and during the stay in a Level III or II unit to at least 34 weeks' PMA, but ideally to 36 weeks' PMA.
Reduction in sound levels in the NICU ‐ effects on nursing staff and parents
As high noise levels are associated with an increased rate of errors and accidents leading to decreased performance among staff (Hétu 1994; Lasky 1995), lowering the noise levels could improve staff performance and parental satisfaction with the care. Voluntary anonymous reporting of medical errors for NICUs is feasible and has the potential of enhancing patient safety (Suresh 2004). Nurses' working experience and satisfaction with care following the implementation of the Newborn Individualized Developmental Care and Assessment Program (NIDCAP®) has been measured using questionnaires (Westrup 2003).
At least five parent satisfaction questionnaires have been developed (the Parent Feedback Questionnaire, Neonatal Index of Parent Satisfaction, Inpatient Parent Satisfaction‐Children's Hospital Minneapolis, Picker Institute‐Inpatient Neonatal Intensive Care Unit Survey, and the Neonatal Intensive Care Unit‐Parent Satisfaction Form) (Mitchell‐Dicenso 1996; Conner 1999). These instruments have not been fully tested and validated (Conner 1999), but may have been used in studies to be included in this review.
How the intervention might work
By lowering the sound levels that reach the neonate, the resulting stress on the cardiovascular, respiratory, neurological and endocrine systems can be diminished, thereby promoting growth and reducing adverse neonatal outcomes.
There are many possible interventions to decrease the noise level in a NICU/Level II unit. The changes/interventions may aim at the NICU as a whole or a section or at the individual neonate.
The architecture and the interior design of a NICU contribute to the sound levels in the unit. Less sound is produced in a unit that consists of pods (as an example designated pods 1, 2, and 3, with ten beds in each pod that surround a central medication area) compared to a unit that consists of one large room (Maragakis 2008). Sound levels can be reduced by installing sound absorbing materials and minimising conversations among the staff (Bremmer 2003). A renovated NICU was found to be 4 dB to 6 dB quieter across all environmental conditions than a comparable non‐renovated room (Byers 2006). Choice of equipment is important as different transport incubators, incubators, ventilators and other essential equipment produce varying sound levels (Byers 2006). As an example, noise intensities generated by the neonatal helmet continuous positive airway pressure (CPAP) are significantly higher than those registered while using a conventional nasal CPAP system (Trevisanuto 2011). These aspects of sound management, except for minimising conversations among staff, will not be the focus of this review.
In a children's surgical ward the mean noise levels were higher in cots (57 dB) than in incubators (51 dB) (Elander 1995). Following an education and awareness programme among staff about sound levels there was a significant reduction in the mean noise level for cots (49 dB), but not for incubators (52 dB) (Elander 1995). Taheri et al studied 31 preterm infants in a NICU with no sound restrictions for one hour between 12:00 to 13:00 and for one hour between 14:30 to 15:30 when the noise level was reduced to ≤ 45 dB (staff were asked to lower their voices, to minimise the telephone ring sound and the hospital matron was asked not to page during the intervention period). The mean oxygen saturation for the infants during the quiet hour was significantly higher compared to when sound levels were not decreased (Taheri 2010).
At the level of the individual neonate, the sound exposure can be decreased by covering the incubator with sound‐absorbing fabrics or by providing earplugs or earmuffs.
Why it is important to do this review
No systematic review according to Cochrane methodology has been performed on the topic of sound reduction in the NICU and its effect on growth and development, thereby justifying this review.
Objectives
Primary objective
To determine the effects of sound reduction on growth and long‐term neurodevelopmental outcomes of neonates.
Secondary objectives
To evaluate the effects of sound reduction on short‐term medical outcomes (bronchopulmonary dysplasia, intraventricular haemorrhage, periventricular leukomalacia, retinopathy of prematurity).
To evaluate the effects of sound reduction on sleep patterns at three months of age.
To evaluate the effects of sound reduction on staff performance.
To evaluate the effects of sound reduction in the neonatal intensive care unit (NICU) on parents' satisfaction with the care.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) or quasi‐RCTs. We planned to include trials if the randomisation was either at the individual patient level or by cluster (an entire NICU or a separate ward of a NICU was the unit of randomisation). The intervention could start in the resuscitation area, during initial transport to a NICU or in the NICU. The intervention should have continued to at least 34 weeks' postmenstrual age (PMA). It is possible that some studies have looked at both reductions in sound levels and light levels. We planned to consider for inclusion such studies if a group that received only sound reduction and a control group that received neither sound nor light reduction could be identified. Exposing neonates to cycled light has been reviewed separately (Morag 2011).
Types of participants
Preterm infants (< 32 weeks' PMA or < 1500 g birth weight) cared for in the resuscitation area, during transport, or once admitted to a NICU or a stepdown unit.
Types of interventions
Comparisons
Reduction in sound levels below 45 dB in individual NICUs (and the resuscitation area) compared to no sound (noise) reduction in other NICUs (the entire NICU is randomised ‐ cluster randomisation). The sound levels could be reduced by the architectural design of the NICU, by reducing the sound from necessary equipment and alarms, by educating the staff to reduce the sound levels they create (from radios, talking etc.), or a combination of these.
Reduction in sound levels below 45 dB in individual ('isolated') rooms compared to rooms in the same NICU with no attempts at reducing the sound levels (the individual infant was randomised to a quiet or a 'non‐quiet' room in the same NICU).
The use of earmuffs versus no earmuffs (randomisation of the individual patient) during transport and in a NICU.
The use of earplugs versus no earplugs (randomisation of the individual patient) during transport and in a NICU.
The interventions should ideally be applied in a NICU, including the resuscitation area, and later in the stepdown unit. The intervention may cover 24 hours of a day/night period or a certain number of hours out of 24 hours. Interventions applied only during neonatal transport would not be included unless they formed part of interventions that continued during the hospital stay. The intervention should start within the first 48 hours after birth. The intervention should continue at least to 34 weeks' PMA.
In a deviation from the protocol we included one study in which the intervention started at < 7 days. Some infants in that study would have been older than 48 hours (our predetermined cut‐off age).
Types of outcome measures
Primary outcomes
Growth (g/kg/day or g/day or mean weight gain since birth) at 34 weeks' postmenstrual age (PMA), at 36 weeks' PMA, at discharge, or a combination.
Long‐term outcomes: growth (weight (kg), height (cm), body mass index and neurodevelopmental outcomes including visual and auditory outcomes (impairments) at 18 months' corrected age or later, using standardised and validated tests).
Secondary outcomes
Growth (g/kg/day or g/day or mean weight gain since birth) at one and three months' corrected age.
Auditory functioning at discharge and at three months' corrected age (measured using automated auditory brainstem response or otoacoustic emissions, or both (Hall 2000)). Reported as normal or abnormal.
Sleep patterns ‐ time spent in quiet sleep at discharge and at one and three months' corrected age (number of hours spent sleeping in 24 hours).
Time to full oral or nasogastric feeds (days).
Days of assisted ventilation.
Days in supplemental oxygen.
Bronchopulmonary dysplasia (oxygen requirement at 28 days of age or at 36 weeks' PMA, or both).
Retinopathy of prematurity; any stage and stages ≥ 3.
Intraventricular haemorrhage; all grades and grades 3 and 4 (diagnosed by ultrasound, computerised tomography (CT) scan or magnetic resonance imaging (MRI)).
Periventricular leukomalacia (diagnosed by ultrasound, CT‐scan or MRI).
Days of initial hospitalisation.
Staff performance (frequency of errors, efficiency, fatigue, concentration, ability to communicate) as measured by a validated assessment tool. Medical errors assessed by voluntary anonymous reporting (Suresh 2004).
Carers' satisfaction with the intervention as measured by a validated assessment tool (Zangaro 2007) or by questionnaires (Westrup 2003).
Parental reactions, stress and satisfaction measured by validated assessment tools (Mitchell‐Dicenso 1996; Conner 1999).
In a deviation from the protocol, we included the following outcomes that were not predetermined at the protocol stage.
Primary outcomes
Weight (g) at 34 weeks PMA.
Secondary outcomes
Fronto‐occipital circumference (cm) at 18 to 22 months of age.
All‐cause mortality during initial hospital stay.
Irritation to the ears (during the treatment period).
Search methods for identification of studies
See: Cochrane Neonatal Review Group (CNRG) search strategy.
Electronic searches
We used the standard search strategy of the CNRG as outlined in The Cochrane Library. This included electronic searches of the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library 2014, Issue 12), MEDLINE (1966 to December 2014), EMBASE (1980 to December 2014), and CINAHL (1982 to December 2014). For details see Appendix 1.
We searched abstracts published online from the annual meetings of the Pediatric Academic Societies (2000 to 2014 Abstracts2View™ Online Archives*).
We searched the following clinical trials registries for ongoing or recently completed trials (clinicaltrials.gov; controlled‐trials.com; anzctr.org.au; who.int/ictrp).
We searched Google for the first 200 hits on Google Scholar™ to identify grey literature.
We did not apply any language restrictions.
Searching other resources
We searched the reference lists of identified trials to identify potential articles for inclusion. We did not seek unpublished data. We planned to contact authors of the one identified published trial to clarify or provide additional information if needed (e.g. to clarify how the randomisation sequence was created, to resolve differences between number of patients randomised and number of patients for which outcomes were reported, to clarify definitions for outcomes reported such as bronchopulmonary dysplasia, to clarify deviations between protocol and the published report, etc.). Review authors screened the retrieved articles to identify articles eligible for inclusion in this review.
Data collection and analysis
We used the standardised review methods of the CNRG to assess the methodological quality of studies. The review authors assessed all abstracts and published full reports identified as potentially relevant by the literature search for inclusion in the review. Each author extracted data separately using predesigned data abstraction forms and then compared results. One review author (AO) entered the data into Review Manager 5 (RevMan 2014) and the other review author cross‐checked the printout against his own data abstraction forms. We corrected any errors by consensus. We planned to contact the primary authors of the studies identified as abstracts, if the full paper was not identified in an electronic database search, to ascertain whether a full publication was available. We obtained information from the primary author if the published article provided inadequate information for the review. Review authors conducted quality assessments of the retrieved articles and we were not blinded to authors, institution or journal of publication.
Selection of studies
We independently assessed study eligibility for inclusion in this review using preset inclusion and exclusion criteria. We listed excluded studies in the table 'Characteristics of excluded studies'.
Data extraction and management
We independently extracted data from the full‐text articles and abstracts using specifically designed customised forms to manage information. We used these forms to decide trial inclusion/exclusion, to extract data from eligible trials and for requesting additional information from authors of the original report. We entered and cross‐checked data using RevMan 5 software (RevMan 2014). We compared the extracted data for any differences. We resolved differences by mutual discussion and consensus. We planned to consult a third person as an arbitrator if necessary.
Assessment of risk of bias in included studies
The following headings and associated questions (based on the questions in the 'Risk of bias' table) were evaluated by the two review authors and entered into the 'Risk of bias' table.
Selection bias (random sequence generation and allocation concealment)
Adequate sequence generation
For the one included study, we categorised the risk of selection bias as:
low risk ‐ adequate (any truly random process e.g. random number table; computer random number generator);
high risk ‐ inadequate (any non‐random process e.g. odd or even date of birth; hospital or clinic record number);
unclear risk ‐ no or unclear information provided.
Allocation concealment
For the one included study, we categorised the risk of bias regarding allocation concealment as:
low risk ‐ adequate (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk ‐ inadequate (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk ‐ no or unclear information provided.
Performance bias
Blinding of participants and personal
For the one included study, we categorised the methods used to blind study personnel from knowledge of which intervention a participant received (as our study population consisted of neonates they would all be blinded to the study intervention):
low risk ‐ adequate for personnel (a placebo that could not be distinguished from the active drug was used in the control group);
high risk ‐ inadequate; personnel aware of group assignment;
unclear risk ‐ no or unclear information provided.
Detection bias
Blinding of outcome assessment
For the one included study, we categorised the methods used to blind outcome assessors from knowledge of which intervention a participant received. (As our study population consisted of neonates they would all be blinded to the study intervention). Blinding was assessed separately for different outcomes or classes of outcomes. We categorised the methods used with regards to detection bias as:
low risk ‐ adequate; follow‐up was performed with assessors blinded to group;
high risk ‐ inadequate; assessors at follow‐up were aware of group assignment;
unclear risk ‐ no or unclear information provided.
Attrition bias
Incomplete outcome data addressed
For the one included study and for each outcome, we described the completeness of data including attrition and exclusions from the analysis. We noted whether attrition and exclusions were reported, the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported or supplied by the trial authors, we re‐include missing data in the analyses. We categorised the methods with respect to the risk attrition bias as:
low risk ‐ adequate (< 10% missing data);
high risk ‐ inadequate (≥ 10% missing data);
unclear risk ‐ no or unclear information provided.
Reporting bias
Free of selective reporting
For the one included study, we described how we investigated the risk of selective outcome reporting bias and what we found. We compared what the researchers stated in a published protocol if available (clinicaltrials.gov; controlled‐trials.com; anzctr.org.au; who.int/ictrp or a peer‐reviewed journal). We assessed the methods as:
low risk ‐ adequate (where it is clear that all of the study's prespecified outcomes and all expected outcomes of interest to the review have been reported);
high risk ‐ inadequate (where not all the study's prespecified outcomes have been reported; one or more reported primary outcomes were not prespecified; outcomes of interest are reported incompletely and so cannot be used; study fails to include results of a key outcome that would have been expected to have been reported);
unclear risk ‐ no or unclear information provided (the study protocol was not available).
Other bias
Free of other bias
For the one included study, we described any important concerns we have about other possible sources of bias (e.g. whether there was a potential source of bias related to the specific study design or whether the trial was stopped early due to some data‐dependent process). We assessed whether each study was free of other problems that could put it at risk of bias as:
low risk ‐ no concerns of other bias raised;
high risk ‐ concerns raised about multiple looks at the data with the results made known to the investigators, difference in number of patients enrolled in abstract and final publications of the paper;
unclear ‐ concerns raised about potential sources of bias that could not be verified by contacting the authors.
Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We assessed the likely magnitude and direction of the bias and whether we considered it is likely to impact on the findings. We planned to explore the impact of the level of bias through undertaking sensitivity analyses if at least two trials using the same intervention reported on the same outcome (see 'Sensitivity analysis').
Measures of treatment effect
We followed the statistical analyses recommended by the CNRG using the RevMan 5 software (RevMan 2014). The estimates of the treatment effects include typical risk ratio (RR), typical risk difference (RD), number needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) for dichotomous outcomes, and mean difference (MD) for continuous outcomes. We reported all estimates of treatment effects with 95% confidence intervals (CIs). We used a fixed‐effect model for meta‐analyses. We used the standardised mean difference (SMD) to combine trials that measured the same outcome but used different scales.
Unit of analysis issues
The unit of analysis was the individual infant if individuals were randomised and for cluster‐RCTs the unit of analysis would be the cluster (individual NICUs randomised to a quiet or a control group).
We planned to include cluster‐RCTs in the analyses along with trials that randomised individual patients. We planned to analyse them using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) using an estimate of the intra‐cluster correlation coefficient (ICC) derived from the trial (if possible), or from another source. We planned to report this and to conduct sensitivity analyses to investigate the effect of variation in the ICC if ICCs from other sources were used. We planned to synthesise the relevant information if we identified both cluster‐RCTs and patient‐level randomised trials. We considered it reasonable to combine the results from both if there was little heterogeneity between the study designs and if interaction between the effect of intervention and the choice of randomisation unit was unlikely.
Dealing with missing data
We planned to request additional data from authors of each trial if necessary (e.g. to resolve differences between number of patients randomised and number of patients for which outcomes were reported, to clarify definitions for outcomes reported such as bronchopulmonary dysplasia). We planned to include the infants for which outcomes were reported and to examine the effect of losses in a sensitivity analysis according to study quality when data were still missing. The analysis was an intention‐to‐treat analysis. We obtained, from the senior author Dr. Lasky, means and SDs for the outcomes reported in the only included trial (Abou Turk 2009). In the published report the results are reported as the mean difference between the groups (Abou Turk 2009).
Assessment of heterogeneity
Only one trial was included in the analysis and therefore tests for heterogeneity were not applicable. We planned to perform heterogeneity tests including the calculation of the I2 statistic to assess the appropriateness of pooling the data if at least two studies were included in a meta‐analysis.
We planned to use RevMan 5 software (RevMan 2014) to assess heterogeneity of treatment effects between trials. We planned to use the following two formal statistics.
The Chi2 test, to assess whether observed variability in effect sizes between studies is greater than would be expected by chance. Since this test has low power when the number of studies included in the meta‐analysis is small, we planned to set the probability at the 10% level of significance.
The I2 statistic to ensure that pooling of data is valid. We planned to grade the degree of heterogeneity as: none, low, moderate and high for I2 values of < 25%, 25% to 49%, 50% to 74% and ≥ 75%, respectively (Higgins 2003). Where there is evidence of apparent or statistical heterogeneity, we planned to assess the source of the heterogeneity using sensitivity and subgroup analyses looking for evidence of bias or methodological differences between trials.
Assessment of reporting biases
We planned to assess reporting and publication bias by examining degree of asymmetry of a funnel plot in RevMan 5 (RevMan 2014) if a meta‐analysis included at least 10 trials.
Data synthesis
We performed statistical analyses according to the recommendations of the CNRG. We analysed all infants randomised on an intention‐to‐treat basis. We analysed treatment effects in the individual trial. We used a fixed‐effect model for meta‐analysis to combine the data. As only one study was included in the analyses, tests for heterogeneity were not applicable. In the future, when more than one trial is included in an analysis for a certain outcome, we plan to examine the potential cause of any heterogeneity in subgroup and sensitivity analyses. In the future, when we judge meta‐analysis to be inappropriate, we plan to analyse and interpret individual trials separately. We used the Mantel‐Haenszel method for estimates of RR and RD. We used the inverse variance method for measured quantities.
Subgroup analysis and investigation of heterogeneity
The following subgroup analyses were prespecified.
Gestational age (< 28 weeks, 28 to 32 weeks).
Birth weight (< 1000 g, 1000 to < 1500g.
Sensitivity analysis
We planned to perform a sensitivity analysis to determine if the findings were affected by including only studies of adequate methodology, defined as adequate randomisation and allocation concealment, blinding of intervention and measurement, and < 10% losses to follow‐up.
We planned to perform further sensitivity analyses depending on the results from the meta‐analyses.
Results
Description of studies
Results of the search
We identified one study for inclusion (Abou Turk 2009) from the literature search conducted in January 2013 and excluded three studies (Mann 1986; Zahr 1995; Li 2009). We identified two other potential studies (Aita 2013; Abdeyazdan 2014) in the November 2014 updated search, but excluded these.
Included studies
The study by Abou Turk et al (Abou Turk 2009) was a single centre study conducted at the University of Texas Medical School at Houston, Center for Clinical Research and Evidence‐Based Medicine, Houston, Texas, USA.
Objective: To determine whether very low birth weight newborns (< 1500 g) wearing silicone earplugs grow larger and perform better on developmental exams than controls.
Population: 34 very low birth weight infants (< 1500 g birth weight), < 1 week of age. Exclusion criteria included terminal illness, congenital anomalies and syndromes associated with hearing loss. Eighteen infants were randomised to earplugs and 16 infants to no earplugs. Twenty‐four infants survived (11 in the earplug group and 13 in the control group).
Intervention: very low birth weight newborns (n = 34) were randomised to wearing earplugs or not. Earplugs were positioned at the time of randomisation and worn continuously until the infants were 35 weeks postmenstrual age (PMA) or discharged (whichever came first). Earplugs were removed for medical or social reasons (e.g. parental visits). Newborns in the control group received standard care. The neonatal intensive care unit (NICU) nurses were given in‐service training regarding the intervention. They were instructed how to shape the plugs and insert them into the concha of the newborn in order to maintain a tight acoustic seal. If the earplugs were properly positioned when spot random checks were made, nurses were given tokens. Four tokens were rewarded with a USD 20 gift certificate.
Outcomes: Short‐term outcomes included mortality during hospital stay, weight at 34 weeks PMA, length of stay in the NICU, time on ventilator, passing a hearing screen and irritation to the ear. Long‐term outcomes included anthropometric measurements, cerebral palsy, and Bayley II (Mental Developmental Index) and Psychomotor Development Index outcomes for the extremely low birth weight (< 1000 g) infants at 18 to 22 months. Twenty‐four of 34 randomised infants survived to discharge. Fourteen of 15 surviving extremely low birth weight infants had follow‐up exams and of these 12 had Bayley II assessments.
Notes: The original inclusion criteria in our protocol stipulated an age of < 48 hours at the time of initiating sound reduction. We made a deviation from our protocol and included this study in which some infants would have been > 48 hours old. In the published report the results are reported as the MD between the groups. Dr. Robert Lasky (senior author of the study) kindly provided us with outcome data as per the silicone earplug group and the no earplug group for all outcomes included in this review. In addition he informed us that: "This study was a preliminary study for a larger RCT. Our [institutional review board] IRB would not approve the larger RCT mostly because they were concerned newborns would be deprived of speech input". Because of funding restraints only the extremely low birth weight infants could be followed at 18 to 22 months corrected age.
Excluded studies
We excluded five studies (Mann 1986; Zahr 1995; Li 2009; Aita 2013; Abdeyazdan 2014) as they did not fulfil our inclusion criteria.
The Li 2009 study randomised 47 infants to the earmuff group; however 24 infants weighed 1501 g to 2500 g and 26 infants had a postmenstrual age (PMA) of 32 to 35 weeks. They randomised 43 infants to the control group; however 20 cases weighted 1501 g to 2500 g and 25 cases had a PMA of 32 to 35 weeks. The outcomes for infants with a birth weight (< 1500 g or a PMA of < 32 weeks) at entry were not reported separately. The majority of the infants did not meet our weight and PMA inclusion criteria (Li 2009). The intervention in the Mann 1986 study was a combination of light and noise reduction. The study did not include a group that was exposed to noise reduction only. Most of the 17 infants in the Zahr 1995 study were enrolled at a PMA beyond 32 weeks, and the study reported only on physiological measures.
From the updated search in November 2014, we identified and excluded two other potential studies (Aita 2013; Abdeyazdan 2014). Abdeyazdan 2014 placed earmuffs on infants for only two days and included infants up to 37 weeks PMA. Also, only physiological/motor outcomes were reported. Aita 2013 performed a RCT in which the intervention was a reduction in both light and noise levels. The authors included only physiological outcomes and no outcomes of interest for this review were reported.
Risk of bias in included studies
Although small, the only included study comparing silicone earplugs to no earplugs was well designed and executed (Abou Turk 2009). The randomisation sequence was created by a random number generator and group assignment was indicated in sequentially numbered opaque sealed envelopes. The infants' healthcare providers and families were not blinded to intervention status because earplugs were clearly visible. There were incentives in place for nursing compliance that may have promoted additional care in the earplug group. The research staff that collected medical record data and assessed the participants at 18 to 22 months follow‐up were blinded to intervention status. All randomised infants were accounted for. Because of funding restraints only the extremely low birth weight infants could be followed at 18 to 22 months corrected age. This study was registered on Clinical Trials.gov (NCT00565357). There do not seem to be any deviations from the protocol. We considered the overall risk of bias to be low.
Effects of interventions
The use of earplugs versus no earplugs in a NICU was the only noise reducing intervention that we could identify in a RCT, that met our inclusion criteria.
As we only identified one study (Abou Turk 2009), we were unable to apply any tests for heterogeneity for any of the outcomes reported below.
Silicone earplugs versus no earplugs (comparison 1)
Primary outcomes
Growth (g/kg/day or g/day or mean weight gain since birth) at 34 weeks' postmenstrual age (PMA), at 36 weeks' PMA, at discharge, or a combination. These outcomes were not reported in the only included study (Abou Turk 2009).
However, weight (g) at 34 weeks PMA was reported and we decided in a deviation from the protocol to include this outcome as a primary outcome.
Long‐term outcomes
Growth (weight (kg), height (cm), body mass index and neurodevelopmental outcomes including visual and auditory outcomes (impairments) at 18 months' corrected age or later using standardised and validated tests). Several of these outcomes were reported in the included trial (Abou Turk 2009), as follows.
Primary outcomes
The following outcomes were not predefined in the protocol: weight (g) at 34 weeks PMA, fronto‐occipital circumference (cm) at 18 to 22 months corrected age.
Weight (g) at 34 weeks PMA
The one included study reported this outcome in 23 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD 111 g, 95% CI ‐151 g to 374 g) (Analysis 1.1) (Figure 1).
1.1. Analysis.
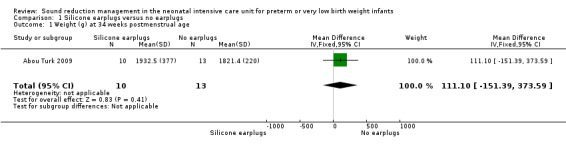
Comparison 1 Silicone earplugs versus no earplugs, Outcome 1 Weight (g) at 34 weeks postmenstrual age.
1.

Forest plot of comparison: 1 Silicone earplugs versus no earplugs, outcome: 1.1 Weight (g) at 34 weeks postmenstrual age.
Weight (kg) at 18 to 22 months corrected age
The one included study reported on this outcome in 14 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD 0.31 kg, 95% CI ‐1.53 kg to 2.16 kg) (Analysis 1.2).
1.2. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 2 Weight (kg) at 18 to 22 months corrected age.
Height (cm) at 18 to 22 months corrected age
The one included study reported on this outcome in 14 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD 2.7 cm, 95% CI ‐3.1 cm to 8.5 cm) (Analysis 1.3).
1.3. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 3 Height at 18 to 22 months corrected age.
Fronto‐occipital circumference (cm) at 18 to 22 months corrected age
The one included study reported on this outcome in 14 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD 1.9 cm, 95% CI ‐0.4 cm to 4.1 cm) (Analysis 1.4).
1.4. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 4 Fronto‐occipital circumference (cm).
Cerebral palsy at 18 to 22 months corrected age
The one included study reported on this outcome in 14 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (RR 3.0, 95% CI 0.13 to 63.15), (RD 0.14, 95% CI ‐0.18 to 0.46) (Analysis 1.5).
1.5. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 5 Cerebral palsy at 18 to 22 months corrected age.
Mental Developmental Index (Bayley II) at 18 to 22 months corrected age
The one included study reported on this outcome in 12 infants. The mean scores on the Mental Developmental Index were significantly higher in infants managed with earplugs than in control infants (MD 14.00, 95% CI 3.13 to 24.87) (Analysis 1.6) (Figure 2).
1.6. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 6 Mental Developmental Index (Bayley II) at 18 to 22 months corrected age.
2.

Forest plot of comparison: 1 Silicone earplugs versus no earplugs, outcome: 1.6 Mental Developmental Index (Bayley II) at 18 to 22 months corrected age.
Psychomotor Development Index (Bayley II) at 18 to 22 months corrected age
The one included study reported on this outcome in 12 infants. The mean scores on the Psychomotor Development Index were not significantly different in infants managed with earplugs compared to control infants (MD ‐2.16, 95% CI ‐18.44 to 14.12) (Analysis 1.7).
1.7. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 7 Psychomotor Development Index (Bayley II) at 18 to 22 months corrected age.
Secondary outcomes
The following outcomes were not predefined in the protocol: all‐cause mortality during hospital stay, irritation to the ears.
Length of stay (days)
The one included study reported on this outcome in 24 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD 1.4 days, 95% CI ‐31.0 days to 33.8 days) (Analysis 1.8).
1.8. Analysis.

Comparison 1 Silicone earplugs versus no earplugs, Outcome 8 Length of stay (days).
Days on assisted ventilation
The one included study reported on this outcome in 24 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (MD ‐1.4 days, 95% CI ‐23.3 days to 20.4 days) (Analysis 1.9).
1.9. Analysis.
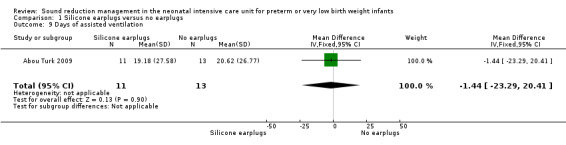
Comparison 1 Silicone earplugs versus no earplugs, Outcome 9 Days of assisted ventilation.
Passed auditory brainstem response (auditory evoked response) test while in hospital
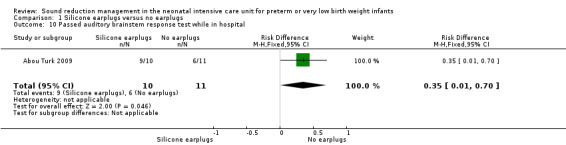
The one included study reported on this outcome in 21 infants. There was no significant difference in this outcome between infants managed with earplugs and control infants for risk ratio: (RR 1.65, 95% CI 0.93 to 2.94), but for risk difference the difference was significantly different (RD 0.35, 95 % CI 0.01 to 0.70); (NNTB 3, 95% CI 1 to 100) (Analysis 1.10) (Figure 3).
1.10. Analysis.
Comparison 1 Silicone earplugs versus no earplugs, Outcome 10 Passed auditory brainstem response test while in hospital.
3.

Forest plot of comparison: 1 Silicone earplugs versus no earplugs, outcome: 1.10 Passed auditory brainstem response test while in hospital.
All‐cause mortality during hospital stay
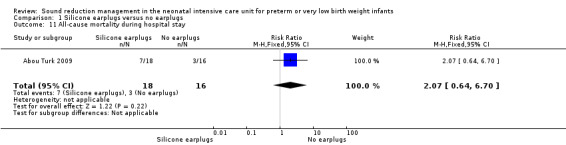
The one included study reported on all‐cause mortality in all 34 randomised infants. There was no significant difference in this outcome between infants managed with earplugs and control infants (RR 2.07, 95% CI 0.64 to 6.70), (RD 0.20, 95% CI ‐0.09 to 0.50) (Analysis 1.11).
1.11. Analysis.
Comparison 1 Silicone earplugs versus no earplugs, Outcome 11 All‐cause mortality during hospital stay.
Potentially adverse effects
Irritation to the ears
The one study reported no irritation to the ears in all 34 randomised infants.
The one included study (Abou Turk 2009) did not report on the following predetermined outcomes.
Primary outcomes
Growth (g/kg/day or g/day or mean weight gain since birth) at 34 weeks' PMA, at 36 weeks' PMA, at discharge, or a combination.
Long‐term outcomes: visual and auditory outcomes (impairments) at 18 months' corrected age or later using standardised and validated tests.
Secondary outcomes
Growth (g/kg/day or g/day or mean weight gain since birth) at one and three months' corrected age.
Auditory functioning at three months' corrected age (measured using automated auditory brainstem response or otoacoustic emissions, or both (Hall 2000). Reported as normal or abnormal.
Sleep patterns ‐ time spent in quiet sleep at discharge and at one and three months' corrected age (number of hours spent sleeping in 24 hours).
Time to full oral or nasogastric feeds (days).
Days of assisted ventilation.
Days in supplemental oxygen.
Bronchopulmonary dysplasia (oxygen requirement at 28 days of age or at 36 weeks' PMA, or both).
Retinopathy of prematurity; any stage and stages ≥ 3.
Intraventricular haemorrhage; all grades and grades 3 and 4 (diagnosed by ultrasound, computerised tomography (CT) scan or magnetic resonance imaging (MRI)).
Periventricular leukomalacia (diagnosed by ultrasound, CT‐scan or MRI).
Staff performance (frequency of errors, efficiency, fatigue, concentration, ability to communicate) as measured by a validated assessment tool. Medical errors assessed by voluntary anonymous reporting (Suresh 2004).
Carers' satisfaction with the intervention as measured by a validated assessment tool (Zangaro 2007) or by questionnaires (Westrup 2003).
Parental reactions, stress and satisfaction measured by validated assessment tools (Mitchell‐Dicenso 1996; Conner 1999).
Discussion
We identified only one study that qualified for this review. The study compared silicone earplugs with no earplugs in very low birth weight infants. It was a well designed and conducted study, but with a small sample size. The mortality was high (29%). Infants who died were not candidates to develop the long‐term outcomes. We were not able to ascertain a composite outcome of death or long‐term neurodevelopment impairment. Becasue of funding restraints only the extremely low birth weight infants could be followed at 18 to 22 months corrected age. The study showed two outcomes that favoured the silicone earplugs group: more infants passed the auditory brainstem response test during hospital stay (significant difference for RD but not for RR); and at 18 to 22 months the few infants (n = 6 in each group) that were followed performed significantly better on the Mental Developmental Index (Bayley II). In view of the small sample size, no conclusions can be drawn from this only study that qualified. Large well conducted RCTs studying different aspects of noise reduction are needed.
Authors' conclusions
Implications for practice.
There is lack of evidence from RCTs to inform healthcare or policy decisions.
Implications for research.
Large well designed, conducted and reported RCTs studying different aspects of noise reduction are needed, as a noise reduction to below 45 dB is recommended but has not been achieved in most neonatal intensive care units (NICUs).
What's new
| Date | Event | Description |
|---|---|---|
| 27 January 2020 | Amended | Arne Ohlsson deceased. |
| 27 January 2020 | New citation required but conclusions have not changed | Contact author changed, and contact details updated. |
Acknowledgements
We would like to thank Ms. Elizabeth Uleryk, Chief Librarian at the Hospital for Sick Children, Toronto for her invaluable help in designing the search strategy for the review at the protocol stage. We are grateful to Ms. Yolanda R Brosseau, Managing Editor of the Cochrane Neonatal Review Group, for conducting the literature searches in January, 2013. Dr. Robert Lasky kindly provided us with outcome data as per the silicone earplug group and the no earplug group for all outcomes included in this review.
Ms. Colleen Ovelman, Trials Search Coordinator, Cochrane Neonatal Review Group, updated the literature searches in December, 2014.
Dr. Roberta G. Pineda provided us with clarifications regarding her study Pineda 2014 in January 2015.
Appendices
Appendix 1. MEDLINE search strategy
We searched MEDLINE from 1966 to the time of the full review using the following search strategy.
1 Noise/ 2 Acoustic Stimulation/ 3 hearing loss/ or deafness/ or hearing loss, bilateral/ or hearing loss, conductive/ or hearing loss, functional/ or hearing loss, high‐frequency/ or hearing loss, noise‐induced/ (26183) 4 Sound/ ( 5 1 or 2 or 3 or 4 6 Intensive Care, Neonatal/ 7 intensive care units/ or intensive care units, neonatal/ 8 6 or 7 9 exp Infant, Newborn, Diseases/ 10 8 or 9 11 5 and 10 12 limit 11 to ("newborn infant (birth to 1 month)" and randomised controlled trial) 13 limit 11 to randomised controlled trial 14 13 not 12 15 from 12 keep 5,8 16 limit 11 to ("newborn infant (birth to 1 month)" and controlled clinical trial) 17 limit 11 to ("newborn infant (birth to 1 month)" and clinical trial) 18 17 not (16 or 12) 19 limit 5 to ("newborn infant (birth to 1 month)" and (clinical trial or controlled clinical trial or randomised controlled trial)) (58) 20 19 not (12 or 16 or 17) 21 from 20 keep 4,21,29‐32,35,37,40 22 exp infant, low birth weight/ or infant, premature/ 23 5 and 22 24 limit 23 to (clinical trial or controlled clinical trial or randomised controlled trial) 25 24 not (12 or 16 or 17 or 19) 26 21 or 15
Appendix 2. CINAHL search strategy
We searched the CINAHL (Cumulative Index to Nursing & Allied Health Literature) database from 1982 to the time of the full review using the following search strategy.
1 sound/ or noise/ 2 Acoustic Stimulation/ 3 deafness/ or exp hearing loss, partial/ 4 noise:.mp. 5 or/1‐4 6 Intensive Care, Neonatal/ 7 Intensive Care Units, Neonatal/ 8 or/6‐7 9 5 and 8 10 exp Clinical Trials/ 11 9 and 10 12 (random: or blind or blinds or blinded or bias or biased).mp. 13 (clinical adj25 trial:).mp. 14 (controlled adj25 trial:).mp. 15 or/12‐14 16 9 and 15 17 11 or 16
Appendix 3. EMBASE search strategy
We searched EMBASE from 1980 to the time of the full review using the following search strategy.
1 noise/ or low frequency noise/ or noise reduction/ or noise standard/ or signal noise ratio/ or white noise/ or noise measurement/ or auditory stimulation/ or sound detection/ or sound transmission/ or exp auditory response/ or exp hearing/ or exp otoacoustic emission/ or hearing impairment/ or conduction deafness/ or hearing loss/ (64508) 2 noise:.mp. 3 1 or 2 4 newborn intensive care/ or exp newborn disease/ 5 3 and 4 6 5 and ct.fs. 7 (random: or blind or blinded or bias or controlled or control or controls).hw,mp,tw. 8 double blind procedure/ or latin square design/ or single blind procedure/ or randomised controlled trial/ or "systematic review"/ 9 5 and 8 10 6 or 9 11 environmental factor/ 12 7 or 8 13 5 and 12 14 newborn intensive care/ 15 3 and 12 and 14 16 6 or 15
Data and analyses
Comparison 1. Silicone earplugs versus no earplugs.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Weight (g) at 34 weeks postmenstrual age | 1 | 23 | Mean Difference (IV, Fixed, 95% CI) | 111.10 [‐151.39, 373.59] |
| 2 Weight (kg) at 18 to 22 months corrected age | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | 0.31 [‐1.53, 2.16] |
| 3 Height at 18 to 22 months corrected age | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | 2.70 [‐3.13, 8.53] |
| 4 Fronto‐occipital circumference (cm) | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | 1.86 [‐0.37, 4.09] |
| 5 Cerebral palsy at 18 to 22 months corrected age | 1 | 14 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.14, 63.15] |
| 6 Mental Developmental Index (Bayley II) at 18 to 22 months corrected age | 1 | 12 | Mean Difference (IV, Fixed, 95% CI) | 14.0 [3.13, 24.87] |
| 7 Psychomotor Development Index (Bayley II) at 18 to 22 months corrected age | 1 | 12 | Mean Difference (IV, Fixed, 95% CI) | ‐2.16 [‐18.44, 14.12] |
| 8 Length of stay (days) | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | 1.36 [‐31.03, 33.75] |
| 9 Days of assisted ventilation | 1 | 24 | Mean Difference (IV, Fixed, 95% CI) | ‐1.44 [‐23.29, 20.41] |
| 10 Passed auditory brainstem response test while in hospital | 1 | 21 | Risk Difference (M‐H, Fixed, 95% CI) | 0.35 [0.01, 0.70] |
| 11 All‐cause mortality during hospital stay | 1 | 34 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.07 [0.64, 6.70] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abou Turk 2009.
| Methods | RCT. Study period June 2002 to March 2003 at the Children's Memorial Hermann NICIU in Houston, Texas, USA | |
| Participants | 34 very low birth weight infants (< 1500 g birth weight), < 1 week of age. Exclusion criteria included terminal illness, congenital anomalies and syndromes associated with hearing loss. 18 infants were randomised to earplugs and 16 infants to no earplugs. 24 infants survived (11 in the earplug group and 13 in the control group) | |
| Interventions | Earplugs were positioned at the time of randomisation and worn continuously until the infants were 35 weeks PMA or discharged (whichever came first). Earplugs were removed for medical or social reasons (e.g. parental visits). Newborns in the control group received standard care. The NICU nurses were given in‐service training regarding the intervention. They were instructed how to shape the plugs and insert them into the concha of the newborn in order to maintain a tight acoustic seal. If the earplugs were properly positioned when spot random checks were made, nurses were given tokens. Four tokens were rewarded by a USD 20 gift certificate | |
| Outcomes | Mortality during hospital stay, weight at 34 weeks PMA, length of stay in the NICU, time on ventilator, and passing a hearing screen. Irritation to the ear.Anthropometric measurements, cerebral palsy, Bayley II (mental and psychomotor index) outcomes for the ELBW infants at 18 to 20 months | |
| Notes | Infants were enrolled at < 1 week of age. Our original inclusion criteria in our protocol stipulated an age < 48 hours. We made a deviation from our protocol and included this study. Because of funding restraints only the ELBW infants could be followed at 18 to 22 months corrected age. Dr. Robert Lasky kindly provided us with outcome data (using means and standard deviations) as per the silicone earplug group and the no earplug group for all outcomes included in this review. In the published report the results are reported as the mean difference between the groups. In addition he informed us that: "This study was a preliminary study for a larger RCT. Our [Institutional Review Board] IRB would not approve the larger RCT mostly because they were concerned newborns would be deprived of speech input" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number generator |
| Allocation concealment (selection bias) | Low risk | Group assignment was indicated in sequentially numbered opaque sealed envelopes |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The subjects' health care providers and families were not blinded to intervention status because earplugs were clearly visible. There were incentives in place for nursing compliance that may have promoted additional care |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The research staff that collected medical record data and assessed the participants at 18 to 22 months follow‐up were blinded to intervention status |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All randomised infants were accounted for |
| Selective reporting (reporting bias) | Low risk | This study was registered on Clinical Trials.gov (NCT00565357). There do not seem to be any deviations from the protocol |
| Other bias | Low risk | The study seems to be free of other bias |
ELBW ‐ extremely low birth weight NICU ‐ neonatal intensive care unit PMA ‐ premenstrual age RCT ‐ randomised controlled trial
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abdeyazdan 2014 | The infants had the intervention (earmuffs) only for two days and there were only physiological/motor outcomes reported. In addition infants were included up to 37 weeks PMA, which is the term population. In the study the infants were 7.1. days (SD 4.2) old |
| Aita 2013 | The intervention in this RCT was a reduction in both light and noise levels. The authors included only physiological outcomes and no outcomes of interest for this review were reported |
| Li 2009 | 47 infants were randomised to the earmuff group; however 24 infants weighed 1501 to 2500 g and 26 infants had a PMA of 32 to 35 weeks. 43 infants were randomised to the control group; however 20 cases weighed 1501 to 2500 g and 25 cases had a PMA of 32 to 35 weeks. The outcomes for infants with a birth weight < 1500 g or a PMA of < 32 weeks at entry were not reported separately. The majority of the infants did not meet our weight and PMA inclusion criteria |
| Mann 1986 | The intervention in this RCT was a reduction in both light and noise levels. The study is included in the Cochrane review on cycled light (Morag 2011) |
| Zahr 1995 | In this study 17 infants were randomised to an experimental (earmuffs) or a control group (no earmuffs). The mean (SD) PMA was 31.0 +/‐ 2.7 weeks in the earmuffs group and 28.9 +/‐ 3.8 weeks in the no earmuffs group. Thus most of the infants did not meet our inclusion criteria of < 32 weeks PMA. The outcomes were physiological measures only |
PMA ‐ postmenstrual age RCT ‐ randomised controlled trial SD ‐ standard deviation
Differences between protocol and review
The only included study enrolled infants who were < 7 days old. Our predetermined age cut‐off was < 48 hours. In a deviation from our protocol we included this study. We report on a number of outcomes that were not included in the protocol.
Contributions of authors
Drs. Al Madhoob and Ohlsson have contributed to all sections of this review.
Dr. Al Madhoob performed the translation from Chinese to English of the Li 2009 study using net based translation programmes.
Sources of support
Internal sources
Mount Sinai Hospital, Canada.
Salmaniya Medical Complex, Ministry of Health, Bahrain.
External sources
-
Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA.
Editorial support of the Cochrane Neonatal Review Group has been funded with Federal funds from the Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA, under Contract No. HHSN275201100016C.
Declarations of interest
Dr. Abdulraoof Almadhoob has no conflict of interest to report.
Dr. Arne Ohlsson has no conflict of interest to report.
Deceased
Edited (no change to conclusions)
References
References to studies included in this review
Abou Turk 2009 {published data only}
- Abou Turk CA, Williams AL, Lasky RE. A randomized clinical trial evaluating silicone earplugs for very low birth weight newborns in intensive care. Journal of Perinatology 2009;29(5):358‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Abdeyazdan 2014 {published data only}
- Abdeyazdan Z, Ghassemi S, Marofi M. The effects of earmuff on physiologic and motor responses in premature infants admitted in neonatal intensive care unit. Iranian Journal of Nursing and Midwifery Research 2014;19(2):107‐12. [PUBMED: 24834077] [PMC free article] [PubMed] [Google Scholar]
Aita 2013 {published data only}
- Aita M, Johnston C, Goulet C, Overlander TF, Snider L. Intervention minimizing preterm infants' exposure to NICU light and noise. Clinical Nursing Research 2013;22(3):337‐58. [PUBMED: 23275433] [DOI] [PubMed] [Google Scholar]
Li 2009 {published data only}
- Li WG, Jiang HB, Gan T, Zhou WX, Chen M. The effect of noise on the auditory system and the intelligence development of premature infants treated in the neonatal intensive care unit. Zhongguo Dang Dai Er Ke Za Zhi 2009;11(12):976‐9. [PubMed] [Google Scholar]
Mann 1986 {published data only}
- Mann NP, Haddow R, Stokes L, Goodley S, Rutter N. Effect of night and day on preterm infants in a newborn nursery: randomised trial. British Medical Journal 1986;293(6557):1265‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zahr 1995 {published data only}
- Zahr LK, Traversay J. Premature infant responses to noise reduction by earmuffs: effects on behavioral and physiologic measures. Journal of Perinatology 1995;15(6):448‐55. [PubMed] [Google Scholar]
Additional references
AAP 1997
- American Academy of Pediatrics (AAP). Committee on Environmental Health. Noise: a hazard for the fetus and newborn. Pediatrics 1997;100(4):724‐7. [PubMed] [Google Scholar]
Abrams 2000
- Abrams RM, Gerhardt KJ. The acoustic environment and physiological responses of the fetus. Journal of Perinatology 2000;20(8 Pt 2):S30‐6. [DOI] [PubMed] [Google Scholar]
Anagnostakis 1980
- Anagnostakis D, Petmezakis J, Messaritakis J, Matsaniotis N. Noise pollution in neonatal units: a potential health hazard. Acta Paediatrica Scandinavica 1980;69(6):771‐3. [DOI] [PubMed] [Google Scholar]
Anagnostakis 1982
- Anagnostakis D, Petmezakis J, Papazissis G, Messaritakis J, Matsaniotis N. Hearing loss in low birth weight infants. American Journal of Diseases of Children 1982;136(7):602‐4. [DOI] [PubMed] [Google Scholar]
Beckham 1982
- Beckham RW, Mishoe SC. Sound levels inside incubators and oxygen hood used with nebulizers and humidifiers. Respiratory Care 1982;27(1):33‐40. [PubMed] [Google Scholar]
Birnholz 1983
- Birnholz JC, Benacerraf BR. The development of human fetal hearing. Science 1983;222(4623):516‐8. [DOI] [PubMed] [Google Scholar]
Blackburn 1998
- Blackburn S. Environmental impact of the NICU on developmental outcomes. Journal of Pediatric Nursing 1998;13(5):279‐89. [DOI] [PubMed] [Google Scholar]
Blomkvist 2005
- Blomkvist V, Eriksen CA, Theorell T, Ulrich R, Rasmanis G. Acoustics and psychosocial environment in intensive coronary care. Occupational and Environmental Medicine 2005;62(3):e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bowden 2000
- Bowden V, Greenberg C, Donaldson N. Developmental care of the newborn. Online Journal of Clinical Innovations 2000;15:1‐77. [Google Scholar]
Brandon 2007
- Brandon DH, Ryan DJ, Barnes AH. Effect of environmental changes on noise in the NICU. Neonatal Network 2007;26(4):213‐8. [DOI] [PubMed] [Google Scholar]
Bremmer 2003
- Bremmer P, Byers JF, Kiehl E. Noise and the premature infant: physiological effects and practice implications. Journal of Obstetric, Gynecologic, and Neonatal Nursing 2003;32(4):447‐54. [DOI] [PubMed] [Google Scholar]
Byers 2006
- Byers JF, Waugh WR, Lowman LB. Sound level exposure of high‐risk infants in different environmental conditions. Neonatal Network 2006;25(1):25‐32. [DOI] [PubMed] [Google Scholar]
Carter 1991
- Carter BS, Wilkening RB. Prevention of hearing disorders: neonatal cause of hearing loss. Seminars in Hearing 1991;12:154‐91. [Google Scholar]
Catlett 1990
- Catlett AT, Holditch‐Davis D. Environmental stimulation of the acutely ill premature infant: physiological effects and nursing implications. Neonatal Network 1990;8(6):19‐26. [PubMed] [Google Scholar]
Chang 2001
- Chang YJ, Lin CH, Lin LH. Noise and related events in a neonatal intensive care unit. Acta Paediatrica Taiwanica 2001;42(4):212‐7. [PubMed] [Google Scholar]
Conner 1999
- Conner JM, Nelson EC. Neonatal intensive care: satisfaction measured from a parent's perspective. Pediatrics 1999;103(1 Suppl E):336‐49. [PubMed] [Google Scholar]
Douek 1976
- Douek E, Dodson HC, Bannister LH, Ashcroft P, Humphries KN. Effects of incubator noise on the cochlea of the newborn. Lancet 1976;2(7995):1110‐3. [DOI] [PubMed] [Google Scholar]
Elander 1995
- Elander G, Hellström G. Reduction of noise levels in intensive care units for infants: evaluation of an intervention program. Heart and Lung 1995;24(5):376‐9. [DOI] [PubMed] [Google Scholar]
EPA 1974
- Environmental Protection Agency, Office of Noise Abatement and Control. Information on levels of environmental noise requisite to protect public health and welfare with an adequate margin of safety (Report No. 5509‐74‐004). Washington, DC: Government Printing Office, 1974. [Google Scholar]
Fisch 1983
- Fisch L. Integrated development and maturation of the hearing system. A critical review article. British Journal of Audiology 1983;17(3):137‐54. [DOI] [PubMed] [Google Scholar]
Gray 2004
- Gray L, Philbin MK. Effects of the neonatal intensive care unit on auditory attention and distraction. Clinics in Perinatology 2004;31(2):243‐60. [DOI] [PubMed] [Google Scholar]
Hall 2000
- Hall JW 3rd. Screening for and assessment of infant hearing impairment. Journal of Perinatology 2000;20(8 Pt 2):S113‐21. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Intervention. Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hétu 1994
- Hétu R. Mismatches between auditory demands and capacities in the industrial work environment. Audiology 1994;33(1):1‐14. [DOI] [PubMed] [Google Scholar]
Jobe 2014
- Jobe AH. Sensory deprivation in private rooms in the NICU. The Journal of Pediatrics 2014;164(1):1. [DOI] [PubMed] [Google Scholar]
Johnson 2003
- Johnson AN. Adapting the neonatal intensive care environment to decrease noise. Journal of Perinatal Neonatal Nursing 2003;17(4):280‐8. [DOI] [PubMed] [Google Scholar]
Kawada 2004
- Kawada T. The effect of noise in the health of children. Journal of Nippon Medical School 2004;71(1):5‐10. [DOI] [PubMed] [Google Scholar]
Kent 2002
- Kent WD, Tan AK, Clarke MC, Bardell T. Excessive noise levels in the neonatal ICU: potential effects on auditory system development. The Journal of Otolaryngology 2002;31(6):355‐60. [DOI] [PubMed] [Google Scholar]
Kingdom 2011
- Kingdom SE, Smith AP. Psychosocial risk factors for work‐related stress in Her Majesty's Coastguard. International Maritime Health 2011;62(3):200‐5. [PubMed] [Google Scholar]
Lary 1985
- Lary S, Briassoulis G, Vries L, Dubowitz LM, Dubowitz V. Hearing threshold in preterm and term infants by auditory brainstem response. Journal of Pediatrics 1985;107(4):593‐9. [DOI] [PubMed] [Google Scholar]
Lasky 1995
- Lasky R. Sound in the NICU and its effects on the newborn. Report of the Tenth Canadian Ross conference in Pediatrics. Montreal: Abbott Laboratories, 1995.
Lasky 2009
- Lasky RE, Williams AL. Noise and light exposures for extremely low birth weight newborns during their stay in the neonatal intensive care unit. Pediatrics 2009;123(2):540‐6. [DOI] [PubMed] [Google Scholar]
Letko 1992
- Letko MD. Detecting and preventing infant hearing loss. Neonatal Network 1992;11(5):33‐8. [PubMed] [Google Scholar]
Liu 2010
- Liu WF, NIC/Q 2005 Physical Environment Exploratory Group. The impact of a noise reduction quality improvement project upon sound levels in the open‐unit‐design neonatal intensive care unit. Journal of Perinatology 2010;30:489‐96. [DOI] [PubMed] [Google Scholar]
Liu 2012
- Liu WF. Comparing sound measurements in the single‐family room with open‐unit design neonatal intensive care unit: the impact of equipment noise. Journal of Perinatology 2012;32:368‐73. [DOI] [PubMed] [Google Scholar]
Lotas 1992
- Lotas MJ. Effects of light and sound in the neonatal intensive care unit environment on the low‐birth‐weight infants. NAAACOG's Clinical Issues in Perinatal and Womens Health Nursing 1992;3(1):34‐44. [PubMed] [Google Scholar]
Magann 2005
- Magann EF, Evans SF, Chauhan SP, Nolan TE, Henderson J, Klausen JH, et al. The effects of standing, lifting and noise exposure on preterm birth, growth restriction, and perinatal death in healthy low‐risk working military women. The Journal of Maternal‐Fetal and Neonatal Medicine 2005;18(3):155‐62. [DOI] [PubMed] [Google Scholar]
Maragakis 2008
- Maragakis LL, Winkler A, Tucker MG, Cosgrove, SE, Ross T, Lawson E, et al. Outbreak of multidrug‐resistant serratia marcescens infection in a neonatal intensive care unit. Infection Control and Hospital Epidemiology 2008;29(5):418‐23. [DOI] [PubMed] [Google Scholar]
Matook 2010
- Matook SA, Sullivan MC, Salisbury A, Miller RJ, Lester BM. Variation of NICU sound by location and time of day. Neonatal Network 2010;29(2):87‐95. [DOI] [PubMed] [Google Scholar]
Mitchell‐Dicenso 1996
- Mitchell‐Dicenso A, Guyatt G, Paes B, Blatz S, Kirpalani H, Fryers M, et al. A new measure of parent satisfaction with medical care provided in the neonatal intensive care unit. Journal of Clinical Epidemiology 1996;49(3):313‐8. [DOI] [PubMed] [Google Scholar]
Morag 2011
- Morag I, Ohlsson A. Cycled light in the intensive care unit for preterm and low birth weight infants. Cochrane Database of Systematic Reviews 2011, Issue 1. [DOI: 10.1002/14651858.CD006982.pub2] [DOI] [PubMed] [Google Scholar]
Morris 2000
- Morris BH, Philbin MK, Bose C. Physiological effects of sound on the newborn. Journal of Perinatology 2000;20(8 Pt 2):S55‐60. [DOI] [PubMed] [Google Scholar]
Ohlsson 2009
- Ohlsson A. NIDCAP: new controversial evidence for its effectiveness. Pediatrics 2009;124(4):1213‐5. [DOI] [PubMed] [Google Scholar]
Ohlsson 2013
- Ohlsson A, Jacobs SE. NIDCAP: A systematic review and meta‐analyses of randomized controlled trials. Pediatrics 2013;131(3):e881‐93. [DOI] [PubMed] [Google Scholar]
Perlman 2001
- Perlman JM. Neurobehavioural deficits in premature graduates of intensive care ‐ potential medical and neonatal environmental risk factors. Pediatrics 2001;108(6):1339‐48. [DOI] [PubMed] [Google Scholar]
Philbin 1999
- Philbin MK, Robertson A, Hall JW 3rd. Recommended permissible noise criteria for occupied, newly constructed or renovated hospital nurseries. The Sound Study Group of the National Resource Center. Journal of Perinatology 1999;19(8 Pt 1):559‐63. [DOI] [PubMed] [Google Scholar]
Philbin 2000
- Philbin MK. The influence of auditory experience on the behavior of preterm newborns. Journal of Perinatology 2000;20(8 Pt 2):S77‐87. [DOI] [PubMed] [Google Scholar]
Philbin 2002
- Philbin MK, Gray L. Changing levels of quiet in an intensive care nursery. Journal of Perinatology 2002;22(6):455‐60. [DOI] [PubMed] [Google Scholar]
Pineda 2014
- Pineda RG, Neil J, Dierker D, Smyser CD, Wallendorf M, Kidokoro H. Alterations in brain structure and neurodevelopmental outcome in preterm infants hospitalized in different neonatal intensive care unit environments. Journal of Pediatrics 2014;164(1):52‐60. [PUBMED: 24139564] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pinheiro 2011
- Pinheiro EM, Guinsburg R, Nabuco MA, Kakehashi TY. Noise at the neonatal intensive care unit and inside the incubator. Revista Latino‐Americana de Enfermagem 2011;19(5):1214‐21. [DOI] [PubMed] [Google Scholar]
Ramesh 2009
- Ramesh A, Suman Rao PN, Sandeep G, Nagapoornima M, Srilakshmi V, Dominic M, et al. Efficacy of a low cost protocol in reducing noise levels in the neonatal intensive care unit. Indian Journal of Pediatrics 2009;76(5):475‐8. [DOI] [PubMed] [Google Scholar]
Reader 2007
- Reader TW, Flin R, Mearns K, Cuthbertson BH. Interdisciplinary communication in the intensive care unit. British Journal of Anaesthesia 2007;98(3):347‐52. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rubel 1985
- Rubel EW. Strategies and problems for future studies of auditory system development. Acta Otolaryngology 1985;421:114‐28. [DOI] [PubMed] [Google Scholar]
Schell 2006
- Schell LM, Gallo MV, Denham M, Ravenscroft J. Effects of pollution on human growth and development: an introduction. Journal of Physiological Anthropology 2006;25(1):103‐12. [DOI] [PubMed] [Google Scholar]
Sittig 2011
- Sittig SE, Nesbitt JC, Krageschmidt DA, Sobczak SC, Johnson RV. Noise levels in a neonatal transport incubator in medically configured aircraft. International Journal of Pediatric Otorhinolaryngology 2011;75(1):74‐6. [DOI] [PubMed] [Google Scholar]
Stennert 1978
- Stennert E, Schulte FJ, Vollrath M, Brunner E, Frauenrath C. The etiology of neurosensory hearing defects in preterm infants. Archives of Otorhinolaryngology 1978;221(3):171‐82. [DOI] [PubMed] [Google Scholar]
Suresh 2004
- Suresh G, Horbar JD, Plsek P, Gray J, Edwards WH, Shiono PH, et al. Voluntary anonymous reporting of medical errors for neonatal intensive care. Pediatrics 2004;113(6):1609‐18. [DOI] [PubMed] [Google Scholar]
Taheri 2010
- Taheri P, Abbasi E, Abdeyazdan Z, Fathizadeh N. The effects of a designed program on oxygen saturation and heart rate of premature infants hospitalized in neonatal intensive care unit of Al‐Zahra hospital in Isfahan in 2008‐2009. Iranian Journal of Nursing and Midwifery Research 2010;15(2):66‐70. [PMC free article] [PubMed] [Google Scholar]
Trevisanuto 2011
- Trevisanuto D, Camiletti L, Doglioni N, Cavallin F, Udilano A, Zanardo V. Noise exposure is increased with neonatal helmet CPAP in comparison with conventional nasal CPAP. Acta Anaesthesiologica Scandinavica 2011;55(1):35‐8. [DOI] [PubMed] [Google Scholar]
Wachman 2011
- Wachman EM, Lahav A. The effects of noise on preterm infants in the NICU. Archives of Disease in Childhood. Fetal and Neonatal Edition 2011;96(4):F305‐9. [DOI] [PubMed] [Google Scholar]
Westrup 2003
- Westrup B, Stjernqvist K, Kleberg A, Hellström‐Westas L, Lagercrantz H. Neonatal individualized care in practice: a Swedish experience. Seminars in Neonatology 2002;7(6):447‐57. [DOI] [PubMed] [Google Scholar]
Winkel 1978
- Winkel S, Bonding P, Larsen PK, Roosen G. Possible effects of kanamycin and incubation in newborn children with low birth weight. Acta Paediatrica Scandinavica 1978;67(6):709‐15. [DOI] [PubMed] [Google Scholar]
Zangaro 2007
- Zangaro GA, Soeken KL. A meta‐analysis of studies of nurses' job satisfaction. Research in Nursing and Health 2007;30(4):445‐58. [DOI] [PubMed] [Google Scholar]