

Abstract
Background
The diagnostic yield of 24-hour ECG Holter monitoring (24H) is currently overcome by alternative ECG monitoring techniquesand it needs to be optimized. The recognition of inter-atrial block (IAB) has emerged as a reliable indicator of patients at risk of atrial fibrillation relapses, and its role enhancing the yield of 24H is yet to be determined. We hypothesized that a presumably low yield of 24H may be ameliorated by means of incorporating the assessment for IAB.
Methods
We retrospectively analyzed 1017 consecutive 24H registers performed in a Multidisciplinary Integrated Health Care Institution, in which a restrictive definition of diagnostic 24H findings was used. A univariate and multivariate regression analysis served to determine the variables associated with a higher 24H’s yield, including the requesting medical specialty, type of indication and a number of clinical, echocardiographic and ECG variables, including IAB.
Results
The mean age of our population was 62 ± 17 years (55% males). The majority of 24H were indicated from the Cardiology department (48%). The overall yield was 12.8%, higher for the assessment of the integrity of the electrical conduction system (26.1%) and poorer for the assessment of syncope (3.2%) and cryptogenic stroke (4.6%). The variables associated with higher diagnostic performance were indication from Cardiology (p < 0.001), IAB (p = 0.004), structural heart disease (p = 0.008) and chronic renal failure (p = 0.009). Patients ≤ 50 years old only retrieved a 7% yield. In the multivariate analysis, indication from Cardiology and IAB remained significant predictors of higher 24H’s yield. In a secondary analysis including echocardiographic data, only identification of IAB remained statistically significant.
Conclusions
The recognition of IAB and the type of indication are major determinants of a higher 24H’s diagnostic yield and may help to optimize the selection of candidates.
Keywords: 24-hour ECG Holter monitoring, Inter-atrial block, Atrial fibrillation
Introduction
Twenty-four hour ECG Holter monitoring (24H) is useful for the documentation of brady- and tachy-arrhythmias. Regardless of its suboptimal yield and the implementation of alternative and more efficient monitoring techniques, the 24H remains as a first-line indication during the diagnostic work out of several cardiac disorders. This is probably due to a widespread access to the technique and its relatively low cost[1-5].
The reported diagnostic yield of 24 Hranges from 1-2% to 46% of cases [1-12]. Regardless of scarce direct comparative data, it can be assumed that both the type of indication and several underlying conditions (abnormal baseline 12-lead ECG, structural heart disease, advanced age and other) account to justify such highly variable diagnostic yield [6-8]. Furthermore, the definition of a diagnostic 24H is highly heterogeneous in the literature, with only a minority of series that find it compelling to establish a strict chronological relationship between symptoms and the 24H findings and/or to provide an unequivocal diagnosis with an impact on the patient’s therapeutic management [10,13-16].The influence of the medical specialty that requests the 24H in the diagnostic yield of the technique is also unknown.
The recognition of inter-atrial block (IAB) has been introduced in the clinical practice in the recent years, especially for the prediction of new-onset or recurrent atrial fibrillation (AF) and stroke [17,18]. Its impact on the diagnostic yield of 24H is unknown.
In this study we sought to analyze the variables associated with a highest diagnostic performance of 24H monitoring (including IAB) from a Multidisciplinary Integrated Health Care Institution, in which all medical specialties have equal access to this diagnostic tool, using a preliminarily defined and restrictive definition of diagnostic 24H’s results.
Material and Methods
Study Population
A retrospective cohort study was undertaken including all consecutive patients undergoing 24H in our Institution the years 2012 to 2018. All patients signed informed consent for the use of their clinical data. The following baseline variables were collected: type of indication, the requesting medical specialty, age, hypertension, underlying structural heart disease, chronic renal disease, sleep apnea, the longest PR interval on 12-lead ECG (if sinus rhythm was documented), sinus P-wave duration, QRS complex width, bifascicular and/or atrio-ventricular (AVB) block. Inter-atrial block (IAB) was defined as a sinus P-wave of > 120 ms, following standard criteria[17]. Left ventricular ejection fraction (EF) and left atrial diameter (LAD) were collected among the patients in whom the 24H was performed the years 2016 and 2017 and had previously undergone 2-D echocardiography at least one year before the Holter register. Left ventricular dysfunction was defined as an EF of < 50% (Simpson). Left atrial dilation was defined as a LAD of > 40 mm. Patients in whom the 24H could not be adequately interpreted due to a poor register’s quality were excluded from the study.
24-hour Holter Monitoring: Technical Specifications
The 3-channel 24H register was obtained by positioning 7 electrodes at the thoracic surface: two at both infra-clavicular spaces, one at the superior sternal aspect, one at the right 4th inter-costal space at the mid-axillary axis, one at the right precordial region, one at the sub-xiphoid space and the last one (neutral electrode) at the right inferior costal area. The electrodes were connected to a Seer Light® recorder(General Electric, Milwaukee, Wi, US).
Type of Indication and Definition of Diagnostic Yield
The type of indication was preliminarily determined before data collection and classified into 8 categories: 1) Etiological study of syncope/pre-syncope; 2) Non-documented palpitations; 3) Integrity of the sinus and/or AV conduction upon clinical suspicion of sinus dysfunction and/or advanced/complete AVB; 4) Assessment of rate control in patients with permanent AF; 5) Cryptogenic stroke or systemic embolism; 6) Assessment of sudden death risk among patients with underlying arrhythmogenic cardiomyopathy; 7) Determination of the arrhythmia burden in patients with paroxysmal AF undergoing rhythm control strategy; 8) Other indications.
Atrial fibrillation was defined as an irregular atrial rhythm with a rate of > 300 bpm lasting more than 30 seconds, and non-sustained ventricular tachycardia as a ventricular rhythm of > 120 bpm lasting ≥ 3 beats and < 30 seconds. Supraventricular or ventricular tachycardia lasting < 30 seconds was not considered a diagnostic finding, unless a clear chronological relationship with the clinical symptoms was established.
In our Institution, a restrictive definition of a diagnostic 24H is used [Table 1]. In short, at least one of the following criteria needs to be met: 1) The finding encompasses a change in the patient’s therapeutic management; 2) It provides a straight answer to a specific clinical question it is made; 3) The clinical symptomatology that promoted the indication for 24H appears during the ECG register (an exact chronological correlation between symptoms and ECG findings being compelling in the case of non-documented palpitations); 4) The following ECG findings are considered diagnostic regardless of an unclear symptom-ECG correlation: Mobitz-II 2nd degree AVB, advanced AVB (≥ 2 consecutive blocked P waves), complete AVB and sustained supra-ventricular or ventricular tachycardia (> 30 seconds).
Table 1. Definition of diagnostic 24H with respect to the type of indication.
AF = Atrial fibrillation; AVB = Atrio-ventricular block; AVN = Atrio-ventricular node; PAC = Premature atrial contraction; PVC = Premature ventricular contraction; VT = Ventricular tachycardia.
| Indication | Diagnostic Finding |
|---|---|
| Cryptogenic stroke | AF or atrial flutter paroxysm (> 30 seconds) |
| Sinus/AVN conduction disturbance | > 3-second sinus pauses during wakefulness or documentation of advanced/complete AVB |
| Syncope/pre-syncope | Any ECG register obtained during a clinical relapse or ≥ 3 seconds of asystolic pause |
| Non-documented Palpitations / | Any ECG register obtained during a clinical relapse of the symptomatic palpitations |
| AF: Rhythm control | AF recurrence or atrial flutter documentation |
| Pacemaker dysfunction suspicion | Any sensing or pacing failure documented |
| Silent myocardial ischemia | ST-segment elevation or depression |
| Arrhythmogenic Cardiomyopathy | Documentation of sustained/non-sustained VT |
| Non-sustained arrhythmias | PAC/PVC count > 20% of the total beats or any sustained atrial/ventricular tachycardia |
When 24H is indicated for the assessment of the ventricular rate control in AF patients, the test may always be considered diagnostic (yield of 100%), as it provides a straight answer to the clinical question (criterion number “2”). For this reason, the type of indication was not incorporated into our regression analysis, since it could distort our logistic regression model. A descriptive analysis of the influence of the type on indication in the yield of 24H was performed instead.
Statistical Analysis
Continuous variables were defined as mean ± standard deviation. Discrete variables were expressed as absolute number and percentage. A chi square and a t-test were performed to evaluate differences between groups in discrete and quantitative variables, respectively. In those patients in whom the 24H was performed the years 2016-2017 (from whom clinical, ECG and echocardiographic variables were available), a descriptive comparative analysis was performed to assess for differences in baseline clinical characteristics and diagnostic yield of the 24H in Cardiology versus other specialties as the source of 24H indication. A univariate logistic regression analysis was performed in this population to determine the baseline variables associated with a diagnostic 24H. The variables obtaining a P value of < 0.10 in the univariate analysis (along with age and sex irrespective of their P value) were incorporated into a multivariate logistic regression model to identify independent predictors of diagnostic 24H. A secondary logistic regression analysis was performed in the 143 patients from whom echocardiographic data (including EF and LAD) was available. A bilateral P value of < 0.05 was considered statistically significant. The statistical analysis was performed with the 15.0 STATA software (StataCorp; Texas, US).
Results
Study Population
During the study period (2012-2018), a total number of 1017 24H were performed in 933 patients (mean age 62 ± 17 years, 515 -55%-male, range 1to 5 24H per patient). A total of 486 24H (48%) were indicated from the Cardiology department, 347 (34%) from General Medicine, 143 (14%) from Neurology and the remaining 41 (4%) from other departments.During the years 2016 and 2017, 212 24H registers corresponding to 210 patients (age 65 ± 17 years, 109 -51%- male) were included. The baseline clinical, ECG and echocardiographic characteristics of the latter study subpopulation are summarized in [Table 2]. Of note, the patients proceeding from the Cardiology department had a higher prevalence of structural heart disease (50% vs. 23.4%, p < 0.001), greater LAD (44.6 ± 9 mm vs. 40 ± 6 mm; 64% vs. 38% patients with LAD of > 40 mm, p = 0.001), longer sinus P-wave duration and higher prevalence of IAB (117.2 ± 23 ms vs. 109.6 ± 18 ms and 49% vs. 30%,respectively; p = 0.02), longer PR interval (187.5 ± 52 ms vs. 170 ± 36 ms,p = 0.02)and a statistical trend toward a higher likelihood of underlying baseline AVB of any degree (26.1% vs. 16.1%, p = 0.08).
Table 2. Patient baseline clinical characteristics with respect to the medical specialty that indicates the 24H register.
Values are expressed as mean ± standard deviation unless otherwise stated. * p value of < 0.05 comparing Cardiology versus other medical specialties. AVB = Atrio-ventricular block; CRD = Chronic renal disease; EF = Left ventricular ejection fraction; HT = Hypertension; IVCD = Intra-ventricular conduction delay (QRS width of > 120 ms); LAD = Left atrial diameter; SA = Sleep apnea; SHD = Structural heart disease.
| Total (n = 212) | Cardiology (n = 88) | Other (n = 124) | P | |
|---|---|---|---|---|
| Age | 65,3 ± 17 | 66,2 ± 16 | 64,8 ± 18 | 0,57 |
| Gender (female), % | 49,1% | 48,9% | 49,2% | 1 |
| HT, % | 60,4% | 62,5% | 58,9% | 0,67 |
| SHD | 34,4% | 50% | 23,4% | < 0,001 * |
| EF (%, n = 143) | 59,4 ± 8 | 59,7 ± 10 | 59,1 ± 7 | 0,68 |
| LAD (n = 143) | 41,9 ± 8 | 44,2 ± 9 | 40 ± 6 | 0,001 * |
| SA, % | 8,9% | 10,2% | 8% | 0,63 |
| CRD, % | 22,6% | 27,3% | 19,4% | 0,19 |
| P-wave duration | 113,1 ± 20 | 117,2 ± 23 | 109,6 ± 18 | 0,02 * |
| PR interval | 178,1 ± 45 | 187,5 ± 52 | 170 ± 36 | 0,02 * |
| QRS width | 100,5 ± 20 | 102 ± 21 | 99 ± 19 | 0,34 |
| AVB, % | 20,3% | 26,1% | 16,1% | 0,08 |
| IVCD, % | 11,8% | 14,8% | 9,7% | 0,29 |
The type of indication was also different depending on the petitionary medical specialty (p < 0.05), being the assessment of the cardiac conducting system the most frequent indication from Cardiology(24%), the evaluation of non-documented palpitations from General Medicine (63%), the etiological study of cryptogenic stroke from Neurology (55%) and the study of syncope from other departments (37%; [Table 3]).Other indications included asymptomatic frequent premature atrial (PAC) or ventricular (PVC) contractions (58%), unspecific dizziness episodes (15%) and pre-excitation syndrome (8%). No 24H was indicated for documentation of myocardial ischemia by means of ST segment analysis, with only one 24H indicated upon suspicion of pacemaker dysfunction.
Table 3. Type of 24H indication with respect to the petitionary medical specialty.
Values are expressed as absolute number (percentage with respect to the corresponding specialty). AF (HRR) = Atrial fibrillation: Heart rate response; CM = Cardiomyopathy (assessment of sudden cardiac deatch risk); NDP = Non-documented palpitations; Parox AF = Paroxysmal atrial fibrillation (assessment of AF burden); Sinus/AVN = Assessment of the integrity of the sinus and atrio-ventricular node conducting system.
| Cardiology (n = 486) | General Medicine (n = 347) | Neurology (n = 143) | Other (n = 41) | Total (n = 1017) | |
|---|---|---|---|---|---|
| Syncope/presyncope | 85 (17,5) | 69 (20) | 21 (15) | 15 (37) | 190 (19) |
| NDP | 89 (18,3) | 216 (63) | 5 (3,5) | 10 (24) | 320 (32) |
| Sinus/AVN | 114 (23,5) | 23 (6,7) | 37 (26) | 2 (5) | 176 (17) |
| AF (HRR) | 75 (15,4) | 6 (1,7) | 0 (0) | 7 (17) | 88 (8,7) |
| Cryptogenic stroke | 4 (0,8) | 3 (0,8) | 79 (55) | 1 (2) | 87 (8,6) |
| CM (SCD risk) | 40 (8,2) | 0 (0) | 0 (0) | 1 (2) | 41 (4) |
| Parox AF | 41 (8,4) | 5 (1,4) | 0 (0) | 2 (4) | 48 (4,7) |
| Other | 38 (7,8) | 25 (7,2) | 1 (0,7) | 3 (7) | 67 (6,7) |
Diagnostic Yield of 24-hour Holter Monitoring
The diagnostic yield of the 24H was 20.16% (205 out of the 1017 24H). After excluding the assessment of ventricular rate in permanent AF patients (n = 88), the yield decreased to 12.8% of cases (119 out of 929 registers).
Differences in the yield of 24H regarding the type of indication are depicted in [Figure 1]. As expected, assessment of the ventricular rate in permanent AF patients achieved the highest diagnostic yield (86 out of 88 cases, 98%), not reaching a 100% percentage due to the performance of 2 consecutive 24H in 2 different patients, without additional diagnostic benefit of the second register. Assessment of the cardiac conducting system was accompanied by the second highest yield (46/176 cases, 26.1%). In 21 of these 46 patients, advanced and/or complete AVB was documented, a pacemaker being implanted in 15 of them. All 21 patients had some degree of baseline AVB (1st or 2nd degree AVB), and thus no diagnostic 24H was registered in patients with bifascicular block but without baseline AVB. Thirteen out of the 46 patients were diagnosed from sinus dysfunction, (pacemaker implantation in 7). Baseline sinus bradicardia/pauses had been documented in all these patients.
Figure 1. Diagnostic yield of 24H on the basis of the type of indication.

Values are expressed as proportion and percentage in each type of indication.
AF (HRR) = Atrial fibrillation: Heart rate response; CM = Cardiomyopathy (assessment of sudden cardiac deatch risk); NDP = Non-documented palpitations; Parox AF = Paroxysmal atrial fibrillation (assessment of AF burden); Sinus/AVN = Assessment of the integrity of the sinus and atrio-ventricular node conducting system.
Importantly, the 2 indications achieving the highest diagnostic yield (ventricular rate control in permanent AF and assessment of cardiac conducting system) more frequently proceeded from the Cardiology department as compared to other sources: 85.2% vs. 14.8% and 64.8% vs. 35.2%, respectively.
Intermediate diagnostic yields were obtained for the study of paroxysmal AF in patients undergoing AF rhythm control, for the sudden cardiac death risk assessment in patients with underlying cardiomyopathy and for the evaluation of non-documented palpitations. In the evaluation of palpitations (yield of 36/320 cases, 11.3%), 10 cases were diagnosed from frequent PVCs/NSVT, 9 from sustained supraventricular tachycardia, 9 from non-sustained atrial tachycardia and 3 from frequent PACs. Normal sinus rhythm was never documented during symptomatic palpitations.
The indications yielding a poorer diagnostic performance were the etiological study of cryptogenic stroke and syncope (4.6% and 3.2%, respectively). No patient presented syncope recurrences during 24H registering.
Without considering permanent AF’s rate control, the 24H derived from Cardiology had a diagnostic yield of 20.2% (83 out of 411 registers), higher than that obtained from General Medicine (9.1% -31 out of 341-), Neurology (3.5%) and other departments (2.9% -1 out of 34-).Importantly, patients proceeding from Cardiology also had a higher prevalence of structural heart disease (50% vs. 23%, p < 0,001), LA enlargement (64% vs. 38%, p = 0.001) and IAB (49% vs. 30%, p = 0.02) than those from other medical specialties.
Among the 212 patients undergoing a complete cardiologic assessment (including 2-D echocardiography), only 9 of them (4%) had documented AF relapses leading to anticoagulant and/or anti-arrhythmic drug therapy initiation. Seven out of the 9 episodes corresponded to newly diagnosed AF relapses. Interestingly, 7 out of these 9 patients (78%) had IAB.
Univariate and Multivariate Analyses
In our univariate analysis, the variables associated with a better diagnostic performance of the 24H register were indication from the Cardiology department (p < 0.001), underlying structural heart disease (p = 0.008), chronic renal failure (p = 0.009) and identification of IAB (p = 0.004; [Table 4]).Descriptively, the yield was manifestly low among patients ≤ 50 years old (7% as compared to a 24% percentage among patients > 50 years old), although not reaching statistical significance.Categorization of age by decades did not add relevant statistical significance.
Table 4. Univariate and multivariate logistic regression analysis of predictors of a higher diagnostic performance of 24H monitoring.
AVB = Atrio-ventricular block; BFB = Bifascicular block; CA = Cardiology department; CI = Confidence Interval; CRD = Chronic renal disease; EF = Left ventricular ejection fraction; HT = Hypertension; IAB = Inter-atrial block; IVCD = Intra-ventricular conduction delay (QRS width of > 120 ms); LAD = Left atrial diameter; OR = Odds Ratio; SA = Sleep apnea; SHD = Structural heart disease. Model #1: Mutivariate analysis performed over the total study population (n=1017); Model #2: Secondary analysis performed after incorporating echocardiographic variables (n=143).
| Univariate | |||
|---|---|---|---|
| Variable | OR | CI 95% | P |
| Age > 50 years | 1,53 | [0,56 – 4,23] | 0,41 |
| Gender (Female) | 0,56 | [0,26 – 1,18] | 0,13 |
| HT | 0,98 | [0,47 – 2,06] | 0,96 |
| SHD | 2,70 | [1,29 – 5,66] | 0,008 |
| EF | 0,97 | [0,92 – 1,01] | 0,16 |
| LAD > 40 mm | 1,08 | [1,03 – 1,14] | 0,004 |
| SA | 0,57 | [0,13 – 2,59] | 0,48 |
| CRD | 2,80 | [1,29 – 6,07] | 0,009 |
| IAB | 5,07 | [1,69 – 15,21] | 0,004 |
| PR interval | 0,99 | [0,99 – 1,01] | 0,98 |
| Baseline AVB | 1,84 | [0,74 – 4,61] | 0,19 |
| QRS width | 1,01 | [0,99 – 1,03] | 0,291 |
| QRS > 120 ms | 1,57 | [0,61 – 3,98] | 0,37 |
| BFB | 0,96 | [0,31 – 2,99] | 0,94 |
| Medical specialty (CA) | 5,36 | [2,36 – 12,15] | < 0,001 |
| Multiivariate | |||
| Model #1 | OR | CI 95% | P |
| IAB | 4,14 | [1,28 – 13,43] | 0,018 |
| CA | 4,11 | [1,20 – 14,04] | 0,024 |
| Model #2 | OR | IC 95% | P |
| IAB | 3,71 | [1,03 – 13,3] | 0,044 |
In our multivariate analysis, the 24H indication from Cardiology (OR = 4.11; CI 95% [1.2 – 14.0]; p = 0.024) and the identification of IAB (OR = 4.14; CI 95% [1.3 – 13.4]; p = 0.018) remained as independent predictors of a higher diagnostic performance (Table4).The sensitivity/specificity/positive/negative predictive values for indication from Cardiology and IAB were 70%/59%/20%/93% and 61%/74%/26%/93%, respectively. More specifically, the recognition of IAB yielded sensitivity/specificity/positive/negative predictive values of 78%/73%/17%/98% in the identification of AF relapses prompting anticoagulant and/or anti-arrhythmic drug therapy initiation.In a secondary analysis to which the echocardiographic EF and LAD variables were incorporated (n=143),only IAB persisted as statistically significant(OR 3.71, CI 95% 1.03 – 13.3; p=0.044).
Discussion
Main Findings
To our knowledge, the present study is the largest unrestricted series of patients undergoing 24H monitoring in the literature. In contrast to prior series, 1) we newly incorporated all possible indications in a sole series of patients undergoing 24H monitoring; 2) we exhaustively analyzed the clinical, ECG and echocardiographic variables associated with a better diagnostic performance of the test, including IAB; 3) a rigorous and restrictive definition of diagnostic 24H was homogeneously and preliminary utilized; and 4) our Multidisciplinary Health Care Institution allowed for assessing for the differences in the yield of 24H related with the medical specialty indicating this diagnostic test.
Currently, alternative prolonged heart rhythm monitoring techniques have proven superior to the 24H in their diagnostic yield. It therefore becomes compelling to optimize the selection of the adequate candidates to 24H monitoring. Our univariate and multivariate analyses identifieda number of clinical, ECG and echocardiographic variables that were associated witha highest diagnostic performanceof this technique, with finally IAB becoming a major predictor of a high 24H’s yield.
The yield of 24H was 12.8%, a percentage that was raised to 20.16% when permanent AF’s rate control was included as an indication. Our study further identified the indications showing a manifestly low diagnostic yield: the etiological study of cryptogenic stroke and syncope. The indications for 24H derived from the Cardiology department and the presence of IAB were identified as predictors of a higher diagnostic performance in our multivariate analysis, although the former lost statistical significanceonce the echocardiographic variables were incorporated into our model. It is suggested by this that a thorough cardiologic evaluation (either performed or not by a cardiologist) should be undertaken prior to the indication of 24H. Such evaluation should incorporate a rigorous analysis of the clinical symptoms, the 12-lead ECG and suspicion and/or characterization of the underlying cardiac disease, if any.
Prior Data
The notorious discrepancy among series with regard to the diagnostic yield of the 24H (ranging from a 1%to a 46%) appears justified by 3 reasons. First, the definition of a diagnostic 24H is not homogeneous. In the setting of non-documented palpitations, a very distinct criterion of diagnostic 24H findings is used, including a highly variable PAC/PVC/non-sustained tachycardia burden and a more or less exigent chronological correlation of such arrhythmias with the clinical symptoms [7,9,11,13,14]. In our study, such chronological correlation was considered compelling, without establishing a minimum arrhythmia burden above which a positive 24H result would be determined. Second, the source of patients derived for 24H monitoring is also variable among prior series, with a majority of them proceeding from non-multidisciplinary institutions. Finally, in the vast majority of prior studies only one or two types of indications of 24H are represented. Our study corroborates that the type of indication for 24H has a dramatic impact on its diagnostic performance.
Contemporary Role of 24H Monitoring in the Era of the Implantable Loop Recorder
Prolonged ECG monitoring, especially with implantable loop recorders, has proven to be superior and highly efficient as compared to 24H in different clinical scenarios, with a percentage of positive tests of up to 84% for the assessment of non-documented palpitations and up to 34% for the etiological study of syncope [11,19,20].Parallel to this, the number of 24H indications seems not to decrease, probably due to the low cost and easy access to this test. Unnecessary indications may lead to an increment of the 24H patient’s waiting list to unacceptable delays, with even a theoretical prognostic impact in patients with syncope, AV conduction disturbanceor underlying cardiomyopathy. Suchdelay should be overcome by means of an accurate patient selection of candidates to 24H monitoring. Our study definitely helps to restrict the indications of 24H to selected indications and clinical scenarios that facilitate the 24H’s diagnostic yield.
The assessment of ventricular rate control in patients with permanent AF was considered almost always efficient in our study (98% of cases), since it provides a straight answer to the clinical question. Regardless of the apparently optimal diagnostic yield of this indication, alternative tests (especially a stress test) may provide a more ‘physiological’ characterization of the functional repercussion of permanent AF. Also considering that a more lenient AF’s heart rate control is currently allowed, a restrictive use of 24H in this settingappears reasonable [21].
The acceptable yield of 24H for the assessment of the sinus/AV conduction (26.1%) appears grounded in a strong clinical/ECG suspicion of significant conducting system disturbance, as inferred from the observation of baseline sinus bradycardia, sinus pauses and/or 1st-2nd degree AVBamong patients with positive 24H results in our series. In contrast, the presence of bifascicular block as an isolated finding (without additional AVB of any degree) did not enhance a higher diagnostic performance. We therefore believe that, among asymptomatic patients, the sole finding of baseline bifascicular block should not become an indication for 24H in the search of advanced AVB.
The assessment of sudden death risk in patients with arrhythmogenic cardiomyopathyand of the arrhythmia burden in AF patients undergoing a rhythm-control strategy (yield of 14.6% and 16.6% in our series, respectively)is generally accepted, and we thus do not recommend revisiting such indication. Periodical 24H monitoring may indeed increase the ability of the technique to pick up AF relapses to up to 40% of cases [22].
In patients with non-documented palpitations (yield of 11.3%), alternative techniques to 24H should be considered, restricting initial 24H monitoring to patients with frequent (daily) symptoms. Otherwise, the primary use of external loop recorders or direct electrophysiological study (in selected patients with underlying cardiomiopathy, > 5-min episodes and sudden termination)is encouraged [23,24].
The 24H’s diagnostic performance in the etiological study of syncope (3.2%) and cryptogenic stroke (4.6%) is unacceptably poor, and alternative diagnostic tools appear mandatory, from a sole carotid sinus massage (which has a higher performance than 24H in unselected patients with syncope) up to the indication of an electrophysiological study and/or implantable loop recorder implantation [3-5,7,14-17,20,25].
Predictors of a Higher Diagnostic 24H Yield: Role of Inter-Atrial Block
Three aspectsjustify the identification of IAB as a predictor of a higher 24H’s diagnostic performance. First, the prevalence of IAB is associated with aging andwith underlying structural heart disease, two conditions that favor a higher incidence of both bradi- and tachy-arrhythmias. Second, IAB is indicative of an underlying impaired inter- and intra-atrial conduction as a consequence of an electrical/structural atrial remodeling process. Such pathological process specifically predisposes to the development of AF as the cause of palpitations, as it was demonstrated in our series by 7 out of the 9 documented AF relapses showing IAB with fair sensitivity (78%), specificity (73%) and negative predictive values (98%). The positive predictive value was, however, very low (17%), probably due to the somewhat low prevalence of IAB and, specially, the very low incidence of “de novo”AF documentation by means of 24H in our patient population. [17]. Finally, IAB is commonly linked to sinus dysfunction and/or AVB, and therefore the identification of IAB indirectly increments the likelihood of registering significant sinus dysfunction or advanced AVB. Our findings suggest that IAB identifies a subpopulation of patients in whom the likelihood of a positive 24H is higher. However, considering the prior evidence, the indication for 24H should also be settled on a strong clinical suspicion of significant bradi- or tachy-arrhythmias. The overall principle of a low diagnostic yield of 24H in the diagnosis of AF should, in our opinion, be maintained, since IAB not only “predicted” AF documentation, but it especially was accompanied by an overall higher diagnostic yield irrespective of the 24H’s findings. We thus believe our findings should not prompt indication of 24H in the search of AF relapses on a routine basis, with the possible exception of patients undergoing AF ablation, in whom routine post-procedural 24H is the rule.
In our multi-variate analysis, the source of 24H indication (Cardiology department) determined a higher diagnostic yield of the technique. In our secondary analysis in which echocardiographic variables were included, however, it was confirmed that such apparent ‘superiority’ of the diagnostic performance of 24H proceeding from Cardiology is inherent to a selection bias of patients with a higher prevalence of underlying cardiomyopathy (p < 0.001), LAD (p = 0.001) and IAB (p = 0.02). It should be further noted that the type of indications that yielded a higher diagnostic performance (AF’s rate control and assessment of sinus/AV conduction) were more frequently processed from Cardiology. Finally, although not becoming statistically significant in our series, a manifestly low yield of 24H in patients ≤ 50 years old (7% in our study) is in agreement with prior series. It therefore appears reasonable to encourage the use of this technique only in highly selected patients when age is under 50 years.
Altogether, an approximated suggested algorithm to guide the use of 24H taking into account all variables associated with an optimized diagnostic yield of this technique in our series (thus incorporating the identification of IAB) is provided in [Figure 2].
Figure 2. A suggested algorithm to guide indication for 24H monitoring.
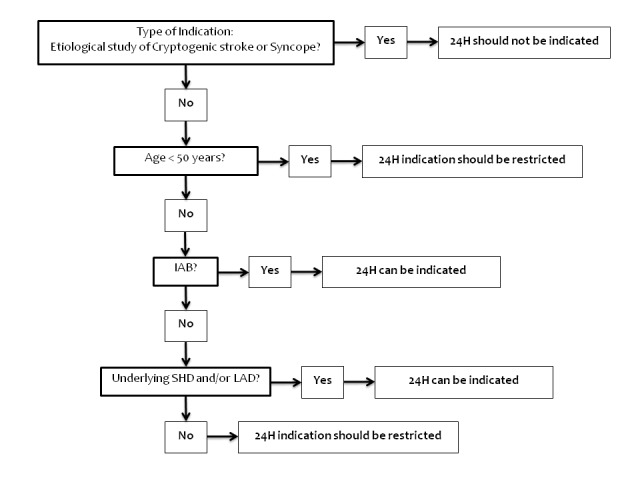
On the basis of the results obtained in this study, a simplified stepwise algorithm is provided in order to optimize the diagnostic yield of 24H monitoring by means of a more accurate and restrictive selection of candidates.
IAB = Inter-atrial block; LAD = Left atrial dilatation; SHD = Structural heart disease.
Limitations
This single-center study may have the limitations inherent to generalization of results from a single source of patients. Regardless of the inclusion of consecutive patients, the retrospective nature of this study may also be considered a significant limitation. Non-systematic echocardiographic data collection may have influenced the analysis of the predicting role of the variables EF and LAD. Although the vast majority of patients with AF documentation prompting a therapeutic change had underlying IAB (7 out of 9, 78%), a correlation analysis between IAB and AF documentation was not performed due to the very low incidence of AF during 24H registering. Finally, the assessment of silent myocardial ischemia and pacemaker dysfunction was not adequately analyzed in our study due to underrepresentation of both indications.
Conclusion
The type of indication and the identification of IAB dramatically influence the diagnostic performance of 24H, with other additional clinical, ECG and echocardiographic variables worthwhile to be considered in order to enhance an optimal patient selection of candidates to this diagnostic tool. The diagnostic yield of 24H for the etiological study of syncope and cryptogenic stroke is prohibitively low. The apparent higher efficiency of the test when it is indicated from a Cardiology department appears to be essentially influenced by an indirect selection of patients in whom the 24H’s diagnostic yield is particularly high.
References
- 1.Knoebel S B, Crawford M H, Dunn M I, Fisch C, Forrester J S, Hutter A M, Kennedy H L, Lux R L, Sheffield L T, Fisch C. Guidelines for ambulatory electrocardiography. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Ambulatory Electrocardiography). Circulation. 1989 Jan;79 (1):206–15. doi: 10.1161/01.cir.79.1.206. [DOI] [PubMed] [Google Scholar]
- 2.Crawford M H, Bernstein S J, Deedwania P C, DiMarco J P, Ferrick K J, Garson A, Green L A, Greene H L, Silka M J, Stone P H, Tracy C M, Gibbons R J, Alpert J S, Eagle K A, Gardner T J, Gregoratos G, Russell R O, Ryan T J, Smith S C. ACC/AHA guidelines for ambulatory electrocardiography: executive summary and recommendations. A report of the American College of Cardiology/American Heart Association task force on practice guidelines (committee to revise the guidelines for ambulatory electrocardiography). Circulation. 1999 Aug 24;100 (8):886–93. doi: 10.1161/01.cir.100.8.886. [DOI] [PubMed] [Google Scholar]
- 3.Koudstaal P J, van Gijn J, Klootwijk A P, van der Meche F G, Kappelle L J. Holter monitoring in patients with transient and focal ischemic attacks of the brain. Stroke. 1986 Mar 1;17 (2):192–5. doi: 10.1161/01.str.17.2.192. [DOI] [PubMed] [Google Scholar]
- 4.Ziegler Paul D, Rogers John D, Ferreira Scott W, Nichols Allan J, Sarkar Shantanu, Koehler Jodi L, Warman Eduardo N, Richards Mark. Real-World Experience with Insertable Cardiac Monitors to Find Atrial Fibrillation in Cryptogenic Stroke. Cerebrovasc. Dis. 2015;40 (3-4):175–81. doi: 10.1159/000439063. [DOI] [PubMed] [Google Scholar]
- 5.Ritter Martin A, Kochhäuser Simon, Duning Thomas, Reinke Florian, Pott Christian, Dechering Dirk G, Eckardt Lars, Ringelstein E Bernd. Occult atrial fibrillation in cryptogenic stroke: detection by 7-day electrocardiogram versus implantable cardiac monitors. Stroke. 2013 May;44 (5):1449–52. doi: 10.1161/STROKEAHA.111.676189. [DOI] [PubMed] [Google Scholar]
- 6.Shen Win-Kuang, Sheldon Robert S, Benditt David G, Cohen Mitchell I, Forman Daniel E, Goldberger Zachary D, Grubb Blair P, Hamdan Mohamed H, Krahn Andrew D, Link Mark S, Olshansky Brian, Raj Satish R, Sandhu Roopinder Kaur, Sorajja Dan, Sun Benjamin C, Yancy Clyde W. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2017 Aug 01;136 (5):e60–e122. doi: 10.1161/CIR.0000000000000499. [DOI] [PubMed] [Google Scholar]
- 7.Locati Emanuela T. New directions for ambulatory monitoring following 2017 HRS-ISHNE expert consensus. J Electrocardiol. 2017 Sep 21;50 (6):828–832. doi: 10.1016/j.jelectrocard.2017.08.009. [DOI] [PubMed] [Google Scholar]
- 8.Gibson T C, Heitzman M R. Diagnostic efficacy of 24-hour electrocardiographic monitoring for syncope. Am. J. Cardiol. 1984 Apr 01;53 (8):1013–7. doi: 10.1016/0002-9149(84)90628-3. [DOI] [PubMed] [Google Scholar]
- 9.Reiffel James A, Schwarzberg Robert, Murry Maria. Comparison of autotriggered memory loop recorders versus standard loop recorders versus 24-hour Holter monitors for arrhythmia detection. Am. J. Cardiol. 2005 May 01;95 (9):1055–9. doi: 10.1016/j.amjcard.2005.01.025. [DOI] [PubMed] [Google Scholar]
- 10.Sivakumaran Soori, Krahn Andrew D, Klein George J, Finan Jane, Yee Raymond, Renner Suzanne, Skanes Allan C. A prospective randomized comparison of loop recorders versus Holter monitors in patients with syncope or presyncope. Am. J. Med. 2003 Jul;115 (1):1–5. doi: 10.1016/s0002-9343(03)00233-x. [DOI] [PubMed] [Google Scholar]
- 11.Hoefman E, Bindels P J E, van Weert H C P M. Efficacy of diagnostic tools for detecting cardiac arrhythmias: systematic literature search. Neth Heart J. 2010 Nov;18 (11):543–51. doi: 10.1007/s12471-010-0831-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shafqat S, Kelly P J, Furie K L. Holter monitoring in the diagnosis of stroke mechanism. Intern Med J. 2004 Jun;34 (6):305–9. doi: 10.1111/j.1444-0903.2004.00589.x. [DOI] [PubMed] [Google Scholar]
- 13.Paudel Badri, Paudel Klara. The diagnostic significance of the holter monitoring in the evaluation of palpitation. J Clin Diagn Res. 2013 Mar;7 (3):480–3. doi: 10.7860/JCDR/2013/4923.2802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sulfi Sreekumar, Balami Dauda, Sekhri Neha, Suliman Abdel, Kapur Akhil, Archbold R Andrew, Ranjadayalan Kulasegaram, Timmis Adam D. Limited clinical utility of Holter monitoring in patients with palpitations or altered consciousness: analysis of 8973 recordings in 7394 patients. Ann Noninvasive Electrocardiol. 2008 Jan;13 (1):39–43. doi: 10.1111/j.1542-474X.2007.00199.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Moya Angel, Sutton Richard, Ammirati Fabrizio, Blanc Jean-Jacques, Brignole Michele, Dahm Johannes B, Deharo Jean-Claude, Gajek Jacek, Gjesdal Knut, Krahn Andrew, Massin Martial, Pepi Mauro, Pezawas Thomas, Ruiz Granell Ricardo, Sarasin Francois, Ungar Andrea, van Dijk J Gert, Walma Edmond P, Wieling Wouter. Guidelines for the diagnosis and management of syncope (version 2009). Eur. Heart J. 2009 Nov;30 (21):2631–71. doi: 10.1093/eurheartj/ehp298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brignole Michele, Vardas Panos, Hoffman Ellen, Huikuri Heikki, Moya Angel, Ricci Renato, Sulke Neil, Wieling Wouter, Auricchio Angelo, Lip Gregory Y H, Almendral Jesus, Kirchhof Paulus, Aliot Etienne, Gasparini Maurizio, Braunschweig Frieder, Lip Gregory Y H, Almendral Jesus, Kirchhof Paulus, Botto Gian Luca. Indications for the use of diagnostic implantable and external ECG loop recorders. Europace. 2009 May;11 (5):671–87. doi: 10.1093/europace/eup097. [DOI] [PubMed] [Google Scholar]
- 17.Tse Gary, Wong Cheuk Wai, Gong Mengqi, Wong Wing Tak, Bazoukis George, Wong Sunny Hei, Li Guangping, Wu William K K, Tse Lap Ah, Lampropoulos Konstantinos, Xia Yunlong, Liu Tong, Baranchuk Adrian. Predictive value of inter-atrial block for new onset or recurrent atrial fibrillation: A systematic review and meta-analysis. Int. J. Cardiol. 2018 Jan 01;250 ():152–156. doi: 10.1016/j.ijcard.2017.09.176. [DOI] [PubMed] [Google Scholar]
- 18.Escobar-Robledo Luis Alberto, Bayés-de-Luna Antoni, Lupón Josep, Baranchuk Adrian, Moliner Pedro, Martínez-Sellés Manuel, Zamora Elisabet, de Antonio Marta, Domingo Mar, Cediel Germán, Núñez Julio, Santiago-Vacas Evelyn, Bayés-Genís Antoni. Advanced interatrial block predicts new-onset atrial fibrillation and ischemic stroke in patients with heart failure: The "Bayes' Syndrome-HF" study. Int. J. Cardiol. 2018 Nov 15;271 ():174–180. doi: 10.1016/j.ijcard.2018.05.050. [DOI] [PubMed] [Google Scholar]
- 19.Moya A, Brignole M, Menozzi C, Garcia-Civera R, Tognarini S, Mont L, Botto G, Giada F, Cornacchia D. Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation. 2001 Sep 11;104 (11):1261–7. doi: 10.1161/hc3601.095708. [DOI] [PubMed] [Google Scholar]
- 20.Burkowitz Jörg, Merzenich Carina, Grassme Kathrin, Brüggenjürgen Bernd. Insertable cardiac monitors in the diagnosis of syncope and the detection of atrial fibrillation: A systematic review and meta-analysis. Eur J Prev Cardiol. 2016 Aug;23 (12):1261–72. doi: 10.1177/2047487316632628. [DOI] [PubMed] [Google Scholar]
- 21.Van Gelder Isabelle C, Groenveld Hessel F, Crijns Harry J G M, Tuininga Ype S, Tijssen Jan G P, Alings A Marco, Hillege Hans L, Bergsma-Kadijk Johanna A, Cornel Jan H, Kamp Otto, Tukkie Raymond, Bosker Hans A, Van Veldhuisen Dirk J, Van den Berg Maarten P. Lenient versus strict rate control in patients with atrial fibrillation. N. Engl. J. Med. 2010 Apr 15;362 (15):1363–73. doi: 10.1056/NEJMoa1001337. [DOI] [PubMed] [Google Scholar]
- 22.Rubín José Manuel, Calvo David, Pérez Diego, Fidalgo Ana, de la Hera Jesús María, Martínez Lidia, Capín Esmeralda, Arrizabalaga Haritz, Carballeira Lidia, García Daniel, Morís Cesar. Characterization of a stepwise approach in cavotricuspid isthmus ablation for typical atrial flutter: A randomized study comparing three catheters. Pacing Clin Electrophysiol. 2017 Oct;40 (10):1052–1058. doi: 10.1111/pace.13170. [DOI] [PubMed] [Google Scholar]
- 23.Ermis Cengiz, Zhu Alan X, Pham Scott, Li Jian Ming, Guerrero Marco, Vrudney Amy, Hiltner Laura, Lu Fei, Sakaguchi Scott, Lurie Keith G, Benditt David G. Comparison of automatic and patient-activated arrhythmia recordings by implantable loop recorders in the evaluation of syncope. Am. J. Cardiol. 2003 Oct 01;92 (7):815–9. doi: 10.1016/s0002-9149(03)00889-0. [DOI] [PubMed] [Google Scholar]
- 24.Vallès Ermengol, Martí-Almor Julio, Bazan Victor, Suarez Fabiola, Cian Debora, Portillo Laura, Bruguera-Cortada Jordi. Diagnostic and prognostic value of electrophysiologic study in patients with nondocumented palpitations. Am. J. Cardiol. 2011 May 01;107 (9):1333–7. doi: 10.1016/j.amjcard.2010.12.047. [DOI] [PubMed] [Google Scholar]
- 25.Locati E T, Moya A, Oliveira M, Tanner H, Willems R, Lunati M, Brignole M. External prolonged electrocardiogram monitoring in unexplained syncope and palpitations: results of the SYNARR-Flash study. Europace. 2016 Aug;18 (8):1265–72. doi: 10.1093/europace/euv311. [DOI] [PMC free article] [PubMed] [Google Scholar]