

Abstract
Nearly half of adolescents experience depressive or aggressive symptoms that impair their functioning at some point in adolescence. Experiencing intense difficult emotions and difficulties regulating such emotions may lead to these depressive and aggressive symptoms. However, existing work largely investigates how adolescent emotions at a single time point predict adolescent depressive or aggressive symptoms months or years later. New investigations are needed to capture the dynamic, changing nature of adolescents’ daily experiences of emotions and symptoms of mental distress. Such investigations would further understanding of how emotions affect mental health in adolescents’ everyday lives. Answering this call, the present study investigated how emotion dysregulation moderated and mediated daily associations between sadness and depressive symptoms and between anger and aggression utilizing ecological momentary assessment in a community sample of 103 Italian adolescents (Mage = 16.77, SD = 0.78, range: 15–18 years old; 47% female). The results revealed that if an adolescent experienced higher-than-usual sadness or anger on a particular day, then they also experienced higher than usual depressive or aggressive symptoms, respectively. Emotion dysregulation mediated and moderated these associations. Adolescents with higher anger had greater difficulties regulating their anger, which led to higher aggressive symptoms (a mediating effect). If adolescents’ sadness was higher than usual on a given day, their depressive symptoms were more severe than usual if they also had higher than usual difficulties regulating sadness (a moderating effect). The findings contribute to understanding of how emotions impact mental distress on a daily basis for adolescents, emphasize the importance of examining specific adolescent emotions, and shed new light on how emotional regulatory capacities influence emotions and mental health in adolescents’ everyday lives.
Keywords: ecological momentary assessment, daily diary, sadness, anger, emotion regulation, depressive symptoms, aggression
Introduction
At some point in adolescence, nearly half of all adolescents experience depressive or aggressive symptoms that impair their mental and physical health, and social, academic, or cognitive functioning (Schacter & Margolin, 2018). Developmental scientists have found that adolescents experience more frequent and intense emotions than younger children or adults (Silk, Steinberg, & Sheffield Morris, 2003), and that the experience of difficult emotions in adolescence predicts the emergence of adolescent depressive and aggressive symptoms (Maciejewski, van Lier, Branje, Meeus, & Koot, 2017). However, several gaps remain in understanding how emotional experiences affect these symptoms of mental distress in adolescence. First, most existing work has examined how differences in emotions experienced by adolescents at one time point predict differences in mental health between adolescents at another time months or years later (Kovacs & Yaroslavsky, 2014). However, adolescent emotions are dynamic in nature and change on a daily basis (Bai & Repetti, 2018). Consequently, existing studies do not reveal how everyday emotional experiences lead to immediate adolescent mental distress (Bai & Repetti, 2018). Therefore, developmental scientists have called for studies to examine how emotions impact symptoms of mental distress within adolescents on a daily basis, to understand how emotions impact adolescents’ mental health in their everyday lives (Lennarz, Hollenstein, Lichtwarck-Aschoff, Kuntsche, & Granic, 2019). Second, most existing work examines associations between adolescent emotions and mental health by combining several emotions (e.g., sadness, anger, etc.) into single measures of negative affectivity (Maciejewski, van Lier, Branje, Meeus, & Koot, 2017). However, different emotions emerge more or less frequently within adolescents on a daily basis, and therefore might affect adolescent symptoms of mental distress differently (Maciejewski et al., 2017). Therefore, investigations need to determine whether specific emotions affect adolescent mental health in different ways on a daily basis (South & Miller, 2014). Third and finally, developmental scientists posit that the daily effects of difficult emotions on adolescent mental health often depend on how well adolescents are able to regulate, or control, these emotions (South & Miller, 2014). However, no studies have tested this hypothesis on a day-to-day basis (Kovacs & Yaroslavsky, 2014). Uncovering how adolescents’ emotion regulation abilities alter associations between adolescents’ emotions and mental distress would aid in the design of interventions that prevent the daily effects of difficult emotions from leading to long-term adolescent mental health problems (Lennarz et al., 2019). The present study fills all three of these gaps in existing literature by examining the daily associations among emotions (sadness and anger), emotion dysregulation and mental distress symptoms (depressive and aggressive symptoms) in a sample of Italian adolescents.
Daily Associations Between Emotions and Symptoms of Mental Distress
Numerous longitudinal investigations have utilized adolescent samples to demonstrate that sadness experienced during one year predicts the emergence of depressive symptoms experienced months or years later, and that anger experienced during one year predicts the emergence of aggressive symptoms months or years later (Maciejewski et al., 2017). Such studies identify between-person associations (i.e., adolescents with higher overall levels of sadness are likely to experience higher overall levels of depressive symptoms), but they do not identify within-person, daily associations. For example, such studies cannot answer the following question: When an adolescent experiences higher sadness on a given day than usual, does that lead to an adolescent experiencing more depressive symptoms on that day than usual (Bolger & Laurenceau, 2013)? Examining such within-person, daily associations is essential to understanding how emotional experiences lead to the emergence of mental distress symptoms within adolescents in everyday life. Study designs utilizing daily diary or ecological momentary assessments (EMA) wherein adolescents report on their emotions and mental distress symptoms in “real-time,” throughout the day are well-suited for investigating such within-person associations (Maciejewski et al., 2017).
Yet, comparatively few daily diary/EMA studies of daily associations between specific emotions and mental distress exist (South & Miller, 2014). Most daily diary studies that do examine such associations in adolescence do not examine discrete emotions, but instead combine multiple difficult emotions (e.g., anger, sadness, guilt, fear) into larger “negative affect” composite scores (South & Miller, 2014). Furthermore, these investigations primarily examine associations between negative affect and depressive symptoms, as opposed to aggressive or other externalizing symptoms (Kovacs & Yaroslavsky, 2014). These studies find that higher daily negative affect is associated with greater daily depressive symptoms (Kovacs & Yaroslavsky, 2014). Though negative affect studies have been vitally important in jump-starting EMA work, investigators have increasingly called for daily diary investigations of associations between discrete emotions and mental distress during adolescence (Maciejewski et al., 2017). This is especially important given that a growing body of work links sadness with depression and anger with aggression in the adolescent treatment literature (e.g., Kovacs & Yaroslavsky, 2014) and that sadness and anger have shown differential courses of development over adolescence (Maciejewski et al., 2017).
Only one EMA study has investigated associations between specific emotions and specific forms of mental distress in adolescents. This study (Silk et al., 2003) utilized an EMA framework over a 7-day period with 14-year-olds and found that greater sadness was associated with greater depressive symptoms, and greater anger was associated with more problem behavior, in adolescents over the entire 7-day period (i.e., between-person effects). However, within-person, daily associations were not examined. Therefore, despite adolescence being a period where discrete emotions are experienced especially intensely, and change especially rapidly, on a daily basis (Maciejewski et al., 2017) existing literature cannot speak to how daily fluctuations in adolescent emotions lead to the emergence of symptoms of mental distress. The present study fills this knowledge gap by utilizing an EMA framework to examine both between- and within-person, daily associations between specific discrete emotions (i.e., sadness and anger) and the symptoms of mental distress with which they have been longitudinally linked in existing literature (i.e., depressive and aggressive symptoms, respectively).
Emotion Dysregulation Alters Associations Between Emotions and Symptoms of Mental Distress
As associations between emotional experiences and mental distress symptoms have been increasingly identified longitudinally, researchers have sought to identify potential moderating and mediating mechanisms that may help explain whether and how emotions convey their effects on symptoms of mental distress (Silk et al., 2003). One prime candidate that has emerged in numerous studies is emotion regulation (Bai & Repetti, 2018). Emotion regulation is a multifaceted construct that has many definitions, but essentially consists of the core processes responsible for monitoring, evaluating, and modifying emotional reactions to accomplish one’s goals (Lennarz et al., 2019).
Systematic reviews of between-person associations have identified that adolescents with higher levels of overall sadness (Kovacs & Yaroslavsky, 2014) or irritability (Brotman, Kircanski, Stringaris, Pine, & Leibenluft, 2017) also experience greater difficulties regulating their emotions. Moreover, between-person studies have also found that greater difficulties with emotion regulation predict greater likelihood of depressive symptoms and externalizing behaviors (including aggression) cross-sectionally and longitudinally (Eisenberg, Spinrad, & Eggum, 2010). Collectively, these studies suggest that emotion dysregulation might mediate associations between the emotions adolescents experience one year and the depressive and aggressive symptoms they experience months or years later (Eisenberg, Spinrad, & Eggum, 2010).
No studies have examined this mediational pathway at the within-person level, where daily fluctuations in emotion dysregulation may mediate the association between emotions and depressive/aggressive symptoms adolescence experience every day. Several within-person EMA studies have examined associations between adolescent emotions and emotion regulation capacities. Specifically, two different EMA studies of American youth age 9–13 (Tan et al., 2012) and 12–15 (Silk et al., 2003) found that more frequent use of several emotion regulation strategies (e.g., avoidance, distraction, and problem solving) was associated with lower levels of momentary anger and sadness (Tan et al., 2012) and general negative affect (Silk et al., 2003) in youth. Additionally, in an EMA study of Dutch adolescents ages 12–17, current negative affect (a measure combining nine difficult emotions including anger and sadness) was lower when adaptive emotion regulation strategies (e.g., problem-solving, acceptance, and reappraisal) were utilized compared to the maladaptive emotion regulation strategy of rumination (Lennarz et al., 2019). Associations between greater negative affect and more difficulty regulating emotions on a daily basis have also been found in EMA investigations of undergraduates (Brockman, Ciarrochi, Parker, & Kashdan, 2017).
These within-person, daily EMA studies build on between-person studies by providing critical evidence that adolescent emotion states can be altered by emotional regulatory capacities on a day-to-day basis (Lennarz et al., 2019). However, these EMA investigations have yet to investigate the mediating effects of emotion regulation by simultaneously examining daily links between emotion states and emotion regulation, and emotion regulation and depressive/aggressive symptoms. Developmental scientists have called for future investigations to do so (South & Miller, 2014). Nevertheless, evidence from both between-person and within-person analyses indicates that daily adolescent experiences of sadness and anger might be associated with daily fluctuations in emotion dysregulation. Moreover, evidence from between-person analyses indicates that emotion dysregulation may mediate the associations between sadness and depressive symptoms, and anger and aggressive symptoms.
Though rarer, some between-person investigations have also investigated whether emotion dysregulation moderates the association between anger and aggression symptoms, and sadness and depressive symptoms, respectively. With regards to anger and aggression associations, a series of studies by Eisenberg and colleagues found that effective emotion regulation buffered the effect of moderate or high negative emotionality on conduct problems, and that higher mother-reported anger and low regulation predicted child membership in a group high in externalizing symptoms (Eisenberg et al., 2001). However, these studies were conducted in elementary-aged children, not adolescents. The only study to examine these questions in an adolescent sample found that during instances where adolescents regulated their anger or sadness more effectively, they were less likely to report depressive symptoms or disruptive problem behavior as a result of sadness or anger (Silk et al., 2003). Importantly, however, this study investigated these moderating effects across particular moments of adolescent-reported emotional experiences in cluster analyses, and did not investigate whether such moderating effects varied within individuals on a day-to-day basis (Silk et al., 2003).
Thus, some evidence from existing between-person investigations indicates that emotion regulation may have both mediating and moderating effects on anger-aggression and sadness-depressive symptoms associations. However, fewer investigations have examined how these associations among emotions, emotion regulation, and mental distress symptoms play out within adolescents on a daily basis. Most within-person EMA studies only examine one of these sets of associations on a daily basis (e.g., just associations between emotions and emotion regulation; Kovacs & Yaroslavsky, 2014). Though there is currently a dearth of empirical evidence, researchers have posited that difficulties regulating emotions may mediate or moderate associations between emotions and symptoms of mental distress on a daily basis (Silk et al., 2003). Stronger emotions than one typically feels on a particular day may lead to more difficulty regulating emotions, which might lead to greater mental distress symptoms felt on that day (a mediating process; Silk et al., 2003). Additionally, the extent to which stronger emotional experiences on a given day lead to the emergence of greater mental distress on that day might depend upon a person’s ability to regulate emotions (a moderating process; Kovacs & Yaroslavsky, 2014).
Identifying whether daily difficulties regulating emotions mediate or moderate associations between emotions and mental distress symptoms would advance understanding of the etiology by which daily emotions lead to daily mental health difficulties and has been called for by clinical (Kovacs & Yaroslavsky, 2014) and developmental (Silk et al., 2003) scientists alike. If adolescents’ daily emotion regulation strategies can be improved, then the daily links between difficult emotions and daily mental distress can be disrupted before such distress becomes chronic and less amenable to change (Kovacs & Yaroslavsky, 2014). Therefore, the present study fills the gap in current knowledge about the daily effects of adolescent emotion dysregulation by examining whether difficulties with regulating sadness or anger mediate or moderate associations between sadness and depressive symptoms and between anger and aggressive symptoms, respectively, on a daily basis.
Anger Versus Sadness-Related Processes
Perhaps due to the widespread use of composite negative affect variables, no EMA studies have examined associations between daily adolescent experiences of specific emotions (e.g., sadness or anger), specific emotion dysregulation (e.g., difficulties regulating sadness or anger), and specific symptoms of mental distress (e.g., depressive symptoms or aggression; Maciejewski et al., 2017). Therefore, it is currently unknown whether emotion dysregulation consistently mediates or consistently moderates associations between daily emotions and mental distress symptoms, or whether such mediation or moderation effects differ depending on the emotions studied. Several leading EMA researchers suspect that the role emotion dysregulation plays depends on the specific emotion-mental distress symptom combination studied, and have called for future investigations to examine this possibility (Maciejewski et al., 2017). The present study adds to existing literature by answering this call. Specifically, the present study compares the mediating or moderating role of emotion dysregulation in associations among adolescent daily sadness, sadness dysregulation, and depressive symptoms on the one hand, and associations among adolescent daily anger, anger dysregulation, and aggressive symptoms on the other.
Current Study
The current study sought to fill three gaps in existing literature. First, moving beyond the investigation of between-person differences in emotions and symptoms of mental distress at single time points months or years apart, the present study utilized EMA analyses to examine the within-person, daily associations between emotions and mental distress symptoms that characterize adolescents’ everyday experiences. Second, moving beyond the investigation of emotions in a single aggregate construct, the present study examined unique effects of specific emotions (sadness and anger) on adolescent symptoms of mental distress (depressive and aggressive symptoms). Third, building upon existing theoretical work that had yet to be examined empirically, the present study explored the mechanisms by which daily adolescent emotion regulation alters associations between adolescent emotions and adolescent symptoms of mental distress.
The present study fills these gaps in existing literature by examining three hypotheses. The first hypothesis, based on (and adding to) findings from existing longitudinal examinations of between-person differences, was that greater sadness would be associated with more depressive symptoms, and greater anger would be associated with more aggressive symptoms, both between adolescents over the entire two week study assessment period, and within-adolescents on a daily basis (Hypothesis 1). Second, extant literature examining primarily between-person effects demonstrated that emotion dysregulation both mediates and moderates associations between negative emotionality and internalizing and externalizing problems. Therefore, the second hypothesis was that adolescent sadness dysregulation could moderate and/or mediate the association between sadness and depressive symptoms, and adolescent anger dysregulation could mediate and/or moderate the association between anger and aggressive symptoms (Hypothesis 2). Existing literature identifies emotion regulation as a mediator and moderator at the between-person level; these same processes were hypothesized to emerge at the within-person, daily level (as posited by other EMA researchers; Kovacs & Yaroslavsky, 2014). Third and finally, the study explored whether the nature of emotion dysregulation mediation or moderation might differ based on the specific emotion-mental distress symptom associations examined (i.e., sadness/depressive associations versus anger/aggressive associations; Hypothesis 3).
Methods
Sample
The 103 adolescent participants in the current study (Mage = 16.77, SD = 0.78, range: 15–18 years old; 53% male, 100% Italian) were recruited from Rome, Italy. All adolescents in the sample had entered puberty. All of the girls had experienced first menarche, and all the boys had developed body hair, facial hair, and voice deepening. Adolescents came from families where parents had 13.2 years of education on average (SD = 4.14). 72% of families included married or cohabitating parents, and 28% of families included divorced, separated, never-married, or widowed parents.
Procedure
Participants were recruited through letters sent from schools. Socioeconomic status and attendance at private versus public schools were both sampled in proportions representative of Rome. After obtaining parental informed consent and child assent, an online assessment methodology called mobile ecological momentary assessment (mEMA; Wen, Schneider, Stone, & Spruijt-Metz, 2017) was employed to collect study data. The mEMA was used to collect data from the adolescents during the course of their daily activities. For 15 consecutive days, adolescents received three e-mails per day (in the morning, afternoon, and evening) on their mobile phones between 8:00 a.m. and 12:00 a.m. Each e-mail was personalized and contained a URL linked to a questionnaire that comprised questions concerning the participants’ current emotional experience. Specifically, first, the adolescents were presented with questions about how much they were feeling specific emotions (e.g., anger, sadness). Then, they were presented with questions about the frequency with which they engaged in specific strategies to handle a specific emotional experience (e.g., anger, sadness). The presented order of questions about anger- and sadness-related mechanisms was randomized at each occasion. Participants had to access the supplied URL and complete the questionnaire within 30 minutes. On average each data completion took 5 minutes. Taken together, the adolescents received 4530 emails. The mEMA protocol was completed 4086 times (90.2% completion rate). This is a very good completion rate considering that a recent review reported that the average compliance rate in adolescent mEMA studies was 78% (Wen et al., 2017). The procedure was approved by Sapienza University of Rome’s Institutional Review Board.
Measures
Anger and sadness.
Adolescents were asked 3 times a day how angry and sad they felt at the moment on a scale of 1 = “very slightly or not at all” to 5 = “extremely.” Anger (“angry,” “mad,” “irritable”) and sadness (“sad,” “discouraged,” “dejected”) were each assessed by separate ratings of 3 items. Both anger (M = 1.27, SD = 0.63, n = 4086) and sadness (M = 1.31, SD = 0.68, n = 4086) items were averaged to create composite scores capturing emotional experience at each time point. High internal reliabilities and significant associations among anger (α = .87, rs = .65 to .72, p < .01) and sadness (α = .85, rs = .63 to .70, p < .01) items supported composite score creation.
Anger and sadness emotion dysregulation.
If adolescents reported a score above 1 in response to any of the anger and sadness items (i.e., if they felt any of the 3 anger or sadness items at least “a little”), they were directed to answer 5 questions adapted from the Difficulties in Emotion Regulation scale (DERS; Gratz & Roemer, 2004). DERS items captured adolescent reports of their difficulties with five different aspects of emotion regulation in response to their anger or sadness. Because the 41-item DERS was too long to include in the brief mEMA assessments used in the current study, a 5-item measure that included each item that loaded highest on each of the 5 DERS categories was utilized (Gratz & Roemer, 2004).
Adolescents were asked to report on how much they were experiencing difficulties on a 1 = “very slightly or not at all” to 5 = “extremely” scale. The items from each of the 5 DERS categories included nonacceptance of emotional responses (“I feel ashamed with myself for feeling angry/sad”), limited access to emotion regulation strategies (“Because I am angry/sad, it is taking me a long time to feel better”), low emotional awareness (“I am acknowledging that I feel angry/sad”; reverse-scored), and problems engaging in both goal-directed behavior (“Because I’m angry/sad, I am having difficulty focusing on other things”) and controlling impulses (“Because I’m angry/sad, my behavior is becoming out of control”). Given high correlations and internal consistency among each of the 5 DERS anger (rs = .18 − .65, ps < .01; α = .76) and sadness (rs = .23 − .58, ps < .01; α = .76) items (i.e., across the 5 types of difficulty in emotion regulation), the items were averaged to create composite scores capturing overall emotion dysregulation related to anger (M = 2.14, SD = 0.77) and sadness (M = 2.13, SD = 0.78). Higher scores indicated greater emotion dysregulation.
Depressive and aggressive symptoms.
Each evening, adolescents reported whether they experienced depressive or aggressive symptoms at some point since the start of the day. Depressive symptoms were measured using three items (e.g., “cried a lot,” “felt worthless or inferior,” “thought that no one loves me”) from the Withdrawn/Depressed subscale, and aggressive symptoms were measured using six items from the Aggression subscale (e.g., “got in many fights,” “teased others”) of the Youth Self Report (YSR; Achenbach & Rescorla, 2001). Items chosen from each subscale represented the items that loaded highest on each subscale in factor analyses utilized in other studies with the same sample. Adolescents reported whether it was 0 = “not true” to 2 = “very true or often true” that they had experienced depressive or aggressive symptoms over the course of the day. Given high correlations and internal consistency among each of the 3 depressive (rs = .32 − .67, ps < .01; α = .70) and 6 aggressive (rs = .16 − .49, ps < .01; α = .71) items, items were averaged to create composite scores capturing severity of daily depressive (M = 0.11, SD = 0.29, n = 1498) or aggressive (M = 0.10, SD = 0.21, n = 1498) symptoms. Higher scores indicated greater symptom severity.
Demographic covariates (gender and age).
Adolescents reported their age in years, and their gender, coded as 0 = girl, 1 = boy.
Analytic Plan
Multilevel modeling (MLM) is a recommended analytic framework when analyzing EMA data (Bolger & Laurenceau, 2013). A key advantage of MLM is its ability to take full advantage of the daily nature of EMA data by disaggregating variance in outcomes due to between-person differences in predictors over time (i.e., differences in adolescents’ depressive and aggressive symptom trajectories over the entire 15-day period) from variance in outcomes attributable to within-person, daily effects (i.e., time-specific differences from an adolescent’s average, or usual, level of depressive or aggressive symptoms). Without accounting for both of these sources of variance, model estimates can be inaccurate and inferences can be subject to the ecological fallacy (Curran & Bauer, 2011).
MLM via the PROC MIXED procedure in SAS 9.4 was used to evaluate study hypotheses. Restricted maximum likelihood estimation procedures were utilized to account for positive skew and leptokurtosis in some study variables, and to maintain statistical power and legitimacy of inferences in the presence of missing data (Bolger & Laurenceau, 2013). A spatial-power covariance structure was utilized to account for serial correlation among daily residuals in dependent variables (Curran & Bauer, 2011). Two MLM models were computed, one examining sadness and sadness regulation as predictors of depressive symptoms (Table 1), and one examining anger and anger regulation as predictors of aggressive symptoms (Table 2). Following expert recommendations (Curran & Bauer, 2011) independent variables (i.e., sadness, sadness emotion dysregulation, anger, anger emotion dysregulation) were grand-mean centered to predict the between-person effects on dependent variable trajectories (i.e., depressive and aggressive symptom intercepts and slopes) and were person-mean centered to predict within-person effects of daily, time-specific alterations to these trajectories. Aligning with expert recommendations (Bolger & Laurenceau, 2013), between- and within-person mediational effects of emotion regulation variables were examined by the calculation of indirect effects, and between- and within-person moderation effects of emotion regulation variables were examined via the creation of interaction terms between emotion variables and emotion dysregulation variables. If a mediational pathway or interaction term was not significant, it was trimmed from the final model in the interest of parsimony. In all models, demographic covariates (i.e., adolescent gender and age) were included as predictors of the intercept and slope of dependent variables.
Table 1.
Multilevel Model Predicting Depressive Symptoms from Sadness and Sadness Emotion Dysregulation
| Model Including Only Sadness | Model Including Sadness and Sadness Emotion Dysregulation | |||
|---|---|---|---|---|
| Predictors | B | SE | B | SE |
| Between Person Effects | ||||
| Intercept | 0.14** | 0.02 | 0.27** | 0.04 |
| Linear Slope | 0.00 | 0.00 | 0.00 | 0.00 |
| Gender | −0.05 | 0.03 | −0.14 | 0.08 |
| Gender X Time Interaction | 0.00 | 0.00 | 0.00 | 0.01 |
| Age | 0.02 | 0.02 | 0.01 | 0.05 |
| Age X Time Interaction | 0.00 | 0.00 | 0.00 | 0.01 |
| Sadness1 | 0.21** | 0.03 | 0.26* | 0.13 |
| Sadness Emotion Dysregulation1 | N/A | N/A | 0.12 | 0.07 |
| Sadness1 X Sadness Emotion Dysregulation1 Interaction | N/A | N/A | −0.29* | 0.15 |
| Within Person Daily Effects | ||||
| Sadness2 | 0.19** | 0.03 | 0.09* | 0.04 |
| Sadness Emotion Dysregulation2 | N/A | N/A | 0.00 | 0.04 |
| Sadness2 X Sadness Emotion Dysregulation2 Interaction | N/A | N/A | 0.14** | 0.03 |
Note:
Grand-mean centered,
Person-mean centered
p ≤ .05.
p ≤ .01.
Table 2.
Multilevel Model Predicting Aggressive Symptoms from Anger and Anger Emotion Dysregulation
| Model Including Only Anger | Model Including Anger and Anger Emotion Dysregulation | |||
|---|---|---|---|---|
| Predictors | B | SE | B | SE |
| Between Person Effects | ||||
| Intercept | 0.12** | 0.02 | 0.15** | 0.04 |
| Linear Slope | −0.004** | 0.002 | −0.004 | 0.01 |
| Gender | −0.01 | 0.03 | 0.10 | 0.06 |
| Gender X Time Interaction | 0.00 | 0.00 | −0.01 | 0.01 |
| Age | 0.05* | 0.02 | 0.10** | 0.04 |
| Age X Time Interaction | −0.003* | 0.001 | −0.007** | 0.00 |
| Anger1 | 0.12** | 0.03 | −0.06 | 0.06 |
| Anger Emotion Dysregulation1 | N/A | N/A | 0.15** | 0.05 |
| Within Person Daily Effects | ||||
| Anger2 | 0.08** | 0.02 | 0.05 | 0.03 |
| Anger Emotion Dysregulation2 | N/A | N/A | 0.05 | 0.04 |
Note:
Grand-mean centered,
Person-mean centered
p ≤ .05.
p ≤ .01.
Results
Missing Data Analyses
Missingness was minimal; 9.6% of entries (N = 444) were skipped entirely, and therefore missing all reports. Of entries that were completed (N = 4086), less than 1% (N = 11) were missing reports of anger or sadness dysregulation. Moreover, of the 1545 possible reports of depressive and aggressive problems (because these problems were only assessed once per day), only 9 (0.20%) were missing. Entries skipped entirely, and therefore missing all variables, obviously could not be compared on differences in emotions, dysregulation, or mental distress symptoms reported. However, skipped versus completed entries did not systematically differ by adolescent gender (X2(1) = .00, p = .99). Entries with versus without missing reports of anger dysregulation did not differ on sadness, anger, sadness dysregulation, depressive symptoms or aggressive symptoms. Entries with versus without missing reports of sadness dysregulation did not differ on sadness, anger, anger regulation, depressive symptoms, or aggressive symptoms. Entries with versus without missing reports of depressive and aggressive symptoms did not significantly differ on sadness, anger, or anger dysregulation though they did differ on sadness dysregulation, with the 4 applicable reports missing depressive symptoms but reporting sadness dysregulation reporting higher sadness dysregulation, when compared to completed reports of depressive symptoms (2.9 to 2.13, t(1241) = −1.97, p = .05). Though systematic differences in missing data were few, out of an abundance of caution restricted information maximum likelihood estimation procedures were used to account for missing data (further detailed below).
Sadness/Depressive Symptoms Models
Testing direct effects of sadness on depressive symptoms (hypothesis 1).
First, the direct between- and within-person associations between sadness and depressive symptoms were modeled to test hypothesis 1 (Table 1). In this model, the intra-class correlation (ICC; r = .32, p < .01) was significant, indicating approximately 68% of variability in depressive symptoms existed at the within-person, daily level. Adolescents reported being at least “a little” sad 30.4% of the time (n = 1243 out of 4086 total reports), and reported that they experienced at least one depressive symptom on 16.62% of days, or 2.50 out of 15 days.
In accordance with expert recommendations (Bolger & Laurenceau, 2013), three competing models (a linear growth curve model with a random intercept only, a linear growth curve model with a random intercept and random slope, and a quadratic growth curve model with a random intercept and random linear slope) were compared to determine which model best captured change in adolescent depressive symptoms over the entire 15-day period. Chi-square testing revealed that a linear growth curve model with a random intercept and slope best characterized change in adolescent depressive symptoms over the 15-day period, even though the average slope over all participants was non-significant. This model indicated that, on average, adolescents reported their depressive symptoms to be 0.14 (so between “not true” and “sometimes true”) on the morning of the study’s first day, and symptoms remained at approximately that level over the entire course of the study. With regards to demographic covariates, neither child gender nor age were significantly associated with the intercept or slope of depressive symptoms (Table 1). Supporting hypothesis 1, both between- and within-person sadness predicted depressive symptom scores (Table 1).
The significant between-person effect indicated that adolescents who reported more overall sadness over the entire 15-day study also experienced more severe overall depressive symptoms over the course of the study, even after controlling for adolescent gender and age. The significant within-person effect of sadness indicated that, on any given study day, if an adolescent experienced higher-than-usual sadness, they also experienced higher-than-usual depressive symptoms (Table 1). Additionally, significant random effects indicated unexplained variance across individuals remained in depressive symptoms experienced on the study’s first day (Intercept Estimate = .01, p < .01) and in the effect of daily sadness on daily depressive symptoms (Estimate = .04, p < .01). These effects indicate that, though the effects of sadness on depressive symptoms were significant, adolescents still varied from one another in their depressive symptoms on the study’s first day after accounting for such effects, and that the impact of daily sadness on daily depressive symptoms varied across individuals.
Testing sadness emotion dysregulation as a mediator and/or moderator (hypothesis 2).
Next, the between and within-person effects of sadness emotion dysregulation were added to the model to explore how emotion dysregulation moderated or mediated between- and within-person associations of sadness and depressive symptoms (Table 1). Demographic covariates (i.e., gender, age) were not significantly associated with the intercept or slope of depressive symptoms.
Moderating effects of sadness emotion dysregulation were tested first. Although the direct between- and within-person effects of sadness emotion dysregulation were non-significant, significant interaction terms (Table 1) indicated that sadness and sadness emotion dysregulation significantly interacted at both the between- and within-person levels to predict depressive symptoms. Therefore, both of these interactions were probed further in simple slopes analyses using the online calculator and accompanying recommendations provided by Preacher, Curran, and Bauer (2006). The between-person interaction was probed first; the association between overall sadness and overall depressive symptoms across the entire 15-day study was investigated at one standard deviation below average (low), average, and one standard deviation above average (high) overall sadness emotion dysregulation (Figure 1). In adolescents where sadness was below average (B = .24, p = .01) over the entire 15-day period, greater sadness emotion dysregulation predicted higher depressive symptoms. However, when adolescents had average (B = .12, p = .11) or high (B = −.01, p = .92) depressive symptoms over the entire 15-day period compared to their peers, the level of sadness emotion dysregulation did not significantly predict depressive symptoms. In other words, greater emotion dysregulation exacerbated the effects of sadness on depressive symptoms in adolescents with low, but not average or high levels of sadness compared to their peers across the entire 15-day period.
Figure 1.
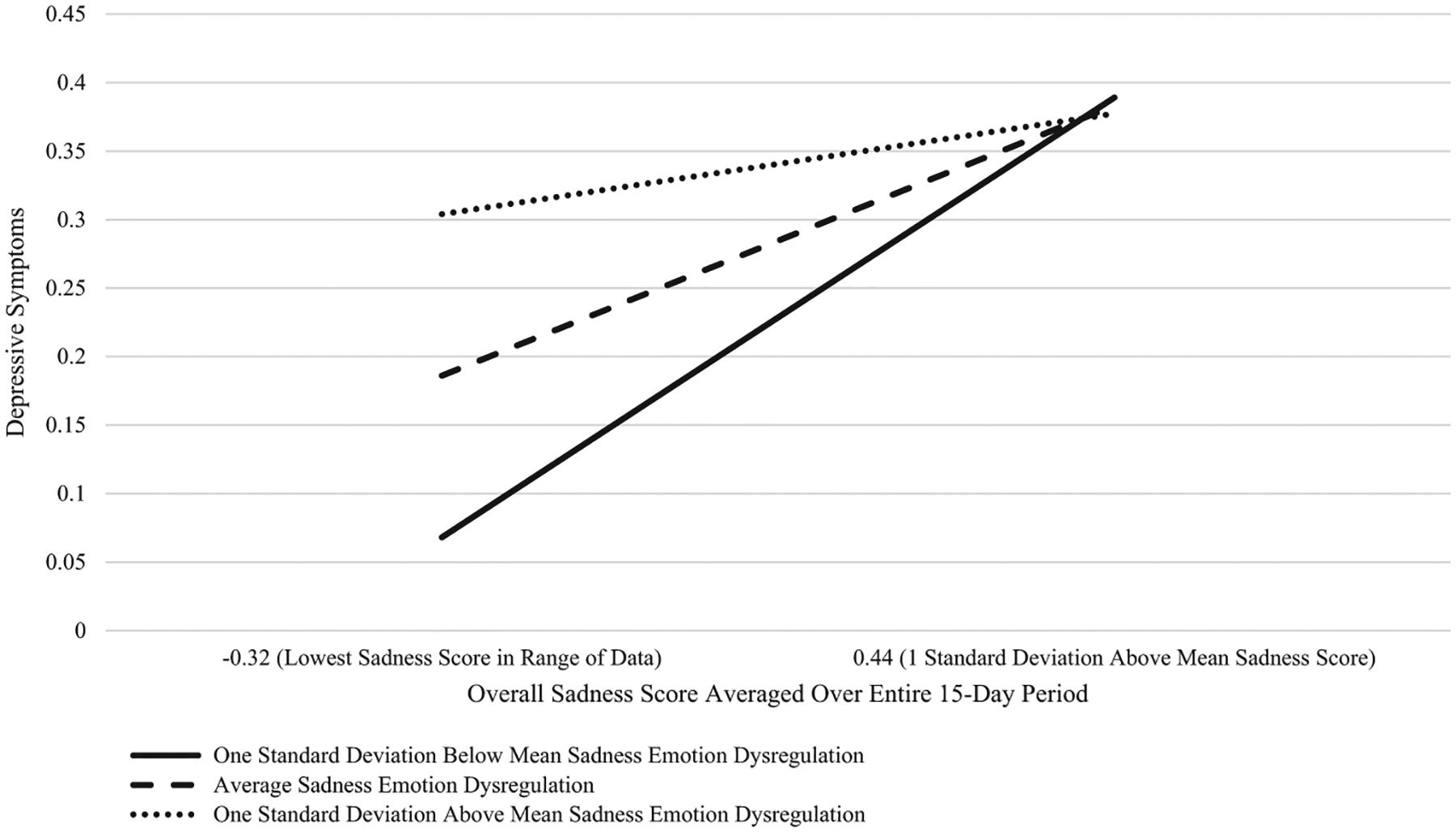
Between person effect of sadness on depressive symptoms at one standard deviation below mean, average, and one standard deviation above mean levels of sadness emotion dysregulation. The original plots were intended to be at 1 standard deviation above mean and below mean sadness scores. However, a one standard deviation below mean sadness score (i.e., −0.44) was beyond the range of the data, so instead interactions are plotted at the lowest sadness score (−0.32) and at 1 standard deviation above mean sadness (0.44).
The within-person interaction term was also probed. The association between daily sadness and daily depressive symptoms was investigated at one standard deviation below average (low), average, and one standard deviation above average (high) daily sadness emotion dysregulation (Figure 2). Results revealed that if an adolescent’s sadness was higher than usual on a given day, then an adolescent’s depressive symptoms were also more severe than usual on a given day if their sadness emotion dysregulation was also higher than usual (B = .16, p < .01), or typical for them (B = .09, p = .01), but not if it was lower than usual (B = .01, p = .74). In other words, on a given day, if adolescents experienced higher than usual emotion dysregulation, then the deleterious effects of their higher-than-usual sadness on their depressive symptoms were exacerbated. However, if their emotion dysregulation was lower than usual, than higher than usual sadness symptoms did not predicted elevated depressive symptoms.
Figure 2.
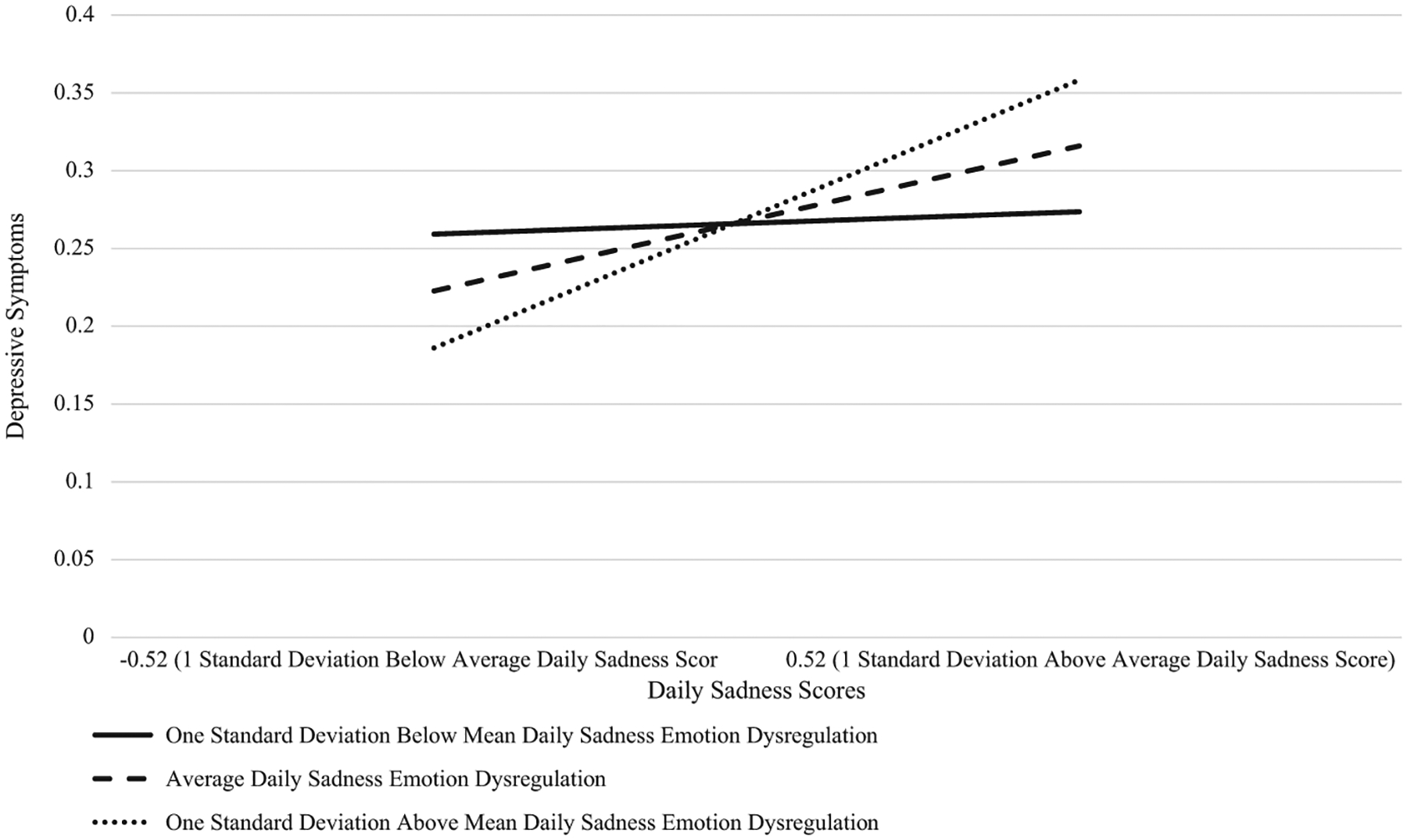
Within person effect of sadness on depressive symptoms at one standard deviation below mean, average, and one standard deviation above mean levels of sadness emotion dysregulation.
Mediational effects were also examined. No significant mediational effects emerged at the between-person level. However, a significant mediational effect did emerge at the within-person level. Specifically, daily sadness emotion dysregulation significantly mediated the association between daily sadness and daily depressive symptoms (Indirect Effect B = .04, p < .01). In other words, when an adolescent experienced higher sadness than usual, that higher-than-usual sadness predicted the emergence of higher-than-usual difficulties handling sadness, which led to more severe depressive symptoms than usual. Thus, sadness emotion dysregulation had a moderating effect at the between-person level, and both moderating and mediating effects at the within-person daily level, on adolescent depressive symptoms in this study.
Anger/Aggression Models
Testing direct effects of anger on aggressive symptoms (hypothesis 1).
First, the direct between- and within-person associations between anger and aggression were modeled to test the first hypothesis (Table 2). In this model, the intra-class correlation (ICC; r = .32, p < .01) was significant, indicating approximately 68% of variability in aggressive symptoms existed at the within-person, daily level. Adolescents reported being at least “a little” angry 24.28% of the time (n = 1243 out of 4086 total reports), and reported that they experienced at least one aggressive symptom on 28.17% of days, or 4.23 out of 15 days.
In accordance with expert recommendations (Curran & Bauer, 2011), three competing models (a linear growth curve model with a random intercept only, a linear growth curve model with a random intercept and random slope, and a quadratic growth curve model with a random intercept and random linear slope) were compared to determine which model best captured change in adolescent aggressive symptoms over the entire 15-day period. Chi-square testing revealed that a linear growth curve model with random intercept and slope was the best fit to the aggression data. This model indicated that, on average, adolescents reported their aggressive symptoms to be 0.12 (so between “not true” and “sometimes true”) on the morning of the study’s first day, and decreased slightly over time at a rate of 0.004 units per day. Supporting hypothesis 1, both between- and within-person anger predicted aggression scores (Table 2).
The significant between-person effect indicated that adolescents who reported more overall anger over the entire 15-day study also experienced more severe overall aggressive symptoms over the course of the study. Notably, this effect remained stable over time (i.e., the between-person interaction between anger and time was non-significant and trimmed from the model). The significant within-person effect of anger indicated that, on any given study day, if an adolescent experienced higher-than-usual anger, they also experienced higher-than-usual aggressive symptoms (Table 2). Additionally, significant random effects indicated significant unexplained variance across individuals remained in aggressive symptoms experienced on the study’s first day (Intercept Estimate = .01, p < .01) and the effect of daily anger on aggressive symptoms (Estimate = .01, p < .01).
Additionally, child age was found to be a significant between-person predictor of the intercept and slope of aggressive symptoms (Table 2). Older children experienced higher levels of aggressive symptoms at the beginning of the study (the intercept effect), and experienced greater decreases in aggressive symptoms over the 15-day course of the study (the slope effect). Child gender, however, was not a significant predictor of intercept or slope.
Testing anger emotion dysregulation as a mediator and/or moderator (hypothesis 2).
Next, the between- and within-person effects of anger emotion dysregulation were added to the model to explore how emotion dysregulation moderated or mediated between- and within-person associations of anger and aggression (Table 2). The effect of child age on the intercept, but not slope, of aggressive symptoms remained significant in this new model, and the effects of gender remained non-significant. Moreover, once anger emotion dysregulation was added to the model, the between- and within-person effects of anger on aggressive symptoms were no longer significant. Additionally, the main effect of anger emotion dysregulation at the between-person, but not the within-person, level was significant. Adolescents with more difficulties handling their anger over the entire 15-day study period experienced greater aggressive symptoms over the entire study period.
Additionally, the mediating and moderating effects of anger emotion dysregulation were explored. Interestingly, no significant moderating effects were found, and only one significant mediating effect was found. Specifically, at the between-person level, overall anger emotion dysregulation over the entire study completely mediated the association between overall anger over the course of the study and aggressive symptoms (Indirect Effect B = .10, p < .01). Adolescents with higher overall anger had greater overall difficulties regulating their anger (B = .63, p < .01), which subsequently led to higher overall aggressive symptoms across the course of the study (B = 0.15, p < .01). Given that the direct between-person effect of anger on aggressive symptoms was no longer significant (B = −.06, p = .32), it appears the entire effect of anger on aggression at the between-person level was mediated by difficulties with anger regulation.
Sensitivity Analyses/Alternate Model Analyses
Several sensitivity and alternate model analyses were conducted to ensure the robustness of study results. Specifically, all models reported above were examined after removing non-significant effects of demographic covariates (i.e., gender and age), to ensure that such non-significant covariate effects were not masking significant between- or within-person associations among substantive study variables. When the demographic covariates were removed, all substantive study results were unchanged and all significant associations were retained (if interested, contact first author for results from these alternative models).
Discussion
Depressive and aggressive symptoms are a leading cause of adolescent impairment and disability, with nearly half of all adolescents experiencing symptoms at some time (Schacter & Margolin, 2018). Extant investigations demonstrate that adolescents with more intense difficult emotions compared to their peers during one year have more severe depressive and aggressive symptoms compared to their peers the next year (Maciejewski et al., 2017). However, existing work typically does not examine how daily experiences of emotions give rise to mental distress in adolescents’ everyday lives (Kovacs & Yaroslavsky, 2014), does not separately examine specific difficult emotions (i.e., sadness versus anger; South & Miller, 2014), and does not examine how emotion dysregulation impacts these daily associations between difficult emotions and mental distress (Lennarz et al., 2019). The current study filled these gaps in existing literature by utilizing an EMA design to test daily associations among adolescent emotions and mental distress, by examining two specific difficult emotions (sadness and anger), and by investigating whether emotion dysregulation mediates or moderates daily associations between sadness and depressive symptoms, and anger and aggressive symptoms. The results indicate that daily experiences of emotions do indeed impact depressive and aggressive symptoms experienced by adolescents in everyday life (hypothesis 1), that emotion dysregulation does alter these associations via mediating and moderating pathways (hypothesis 2), and that examining specific difficult emotions is important, because the effects of emotion dysregulation vary depending on whether adolescent sadness or anger is examined (hypothesis 3).
Emotions Impact Mental Distress In Adolescents’ Everyday Lives (Hypothesis 1)
The first hypothesis, that sadness would be positively associated with depressive symptoms and anger with aggression both between and within individuals, was fully supported. The significant within-person, daily associations deserve special emphasis. These within-person, daily associations move beyond rank-order, between-person effects and emphasize that regardless of an adolescent’s overall level of sadness or anger, on days when adolescents felt more sad or angry than usual, they also felt more severe depressive or aggressive symptoms. These within-person, daily effects highlight a core tenet of developmental psychopathology: that normative and atypical developmental processes mutually inform one another (Silk et al., 2003) such that even children who generally experience “normal” (i.e., average) levels of sadness or anger can still experience deleterious spikes in depressive or aggressive symptoms as a result of momentary, everyday elevations in sadness or anger. If daily spikes in sadness and anger reoccur over and over, the daily elevations in depressive or aggressive symptoms resulting from these spikes have the potential to crystallize into more chronic patterns of depression and aggression (Kovacs & Yaroslavsky, 2014). Such crystallizing effects demonstrate how daily effects of sadness and aggression “add up” over time, and contribute to the etiology of more depressive and aggressive symptoms (Kovacs & Yaroslavsky, 2014). The significance of these within-person daily associations between emotions and mental distress speaks to the potential importance of educating all adolescents (not just those who are chronically sad or angry) on evidence-based, effective ways to identify and cope with sadness or anger.
Emotion Dysregulation Alters Daily Emotion-Mental Distress Associations (Hypothesis 2)
The second hypothesis was partially supported; emotion dysregulation mediated and/or moderated associations between anger and aggression and between sadness and depressive symptoms, albeit in different ways. Within-person, daily mediating and moderating effects were found for sadness, but not anger. The manner in which anger emotion dysregulation affected the association between anger and aggressive symptoms was relatively straightforward; anger regulation served as a complete mediator of the association between anger and aggression, but only at the between-person level. That is, greater anger over the entire 15-day study period predicted greater difficulties controlling anger over the entire study, which predicted greater aggressive symptoms. This sole between-person mediational finding suggests that associations between anger, difficulties regulating anger, and actual aggression demonstrate stability across time and between adolescents, and are less prone to day-to-day fluctuations. Therefore, evidence-based interventions that primarily target associations between adolescent anger and anger regulation, or between adolescent anger regulation and aggressive symptoms, should be especially effective in mitigating the deleterious effects of this mediational pathway.
For instance, behavioral parent training interventions that teach parents to positively reinforce appropriate child responses to anger have demonstrated efficacy in improving emotion regulation in young children (Rothenberg, Weinstein, Dandes, & Jent, 2018) and have been adapted for adolescents (Barkley & Robin, 2014). Additionally, cognitive-behavioral therapy interventions that teach adolescents alternative, effective responses to regulate anger (i.e., via relaxation techniques, thought-challenging, etc.) have already demonstrated efficacy in reducing aggressive symptoms (Brotman et al., 2017).
The manner in which emotion dysregulation mediated and moderated associations between sadness and depressive symptoms was more complex and multi-faceted. At the between-person level, sadness emotion dysregulation moderated the effects of sadness on depressive symptoms at low but not high, levels of sadness (Figure 1). This moderating effect demonstrates that even in adolescents who experience low levels of sadness compared to their peers, such sadness can be associated with increased risk for depressive symptoms if emotion dysregulation strategies are also suboptimal. Results indicate that depressive symptoms do not just emerge in adolescents who are very sad most of the time, but can also emerge in adolescents who do not have the regulatory capacities and skills to cope with the levels of sadness they do experience (even if such sadness is typically relatively low; South & Miller, 2014).
Interestingly, this moderating effect also revealed that level of sadness emotion dysregulation did not differentiate depressive symptoms experienced in adolescents who experienced higher sadness than their peers over the entire 15-day period. Two potential explanations could account for this finding, one substantive and one methodological. With regards to the substantive explanation, in the high-sadness group, the chronic persistence of sadness may eventually “wear out” adolescents’ regulatory capacities, and therefore become associated with high depressive symptoms regardless of adolescents’ capacity to regulate or cope with their sadness. However, this finding could also have arisen due to the methodology for measuring emotion regulation. Specifically, it is notable that the measure of emotion dysregulation only included emotion regulation difficulties (e.g., nonacceptance of emotional responses, low emotional awareness). Therefore low emotion dysregulation scores indicated an absence of emotion regulation difficulties, but do not capture the presence of positive emotion regulation strategies (e.g., active coping, goal-directed problem solving) that can improve the association between affect and depressive symptoms (Friedberg & McClure, 2015). It may be that high-sadness adolescents who engage in positive emotion regulation strategies are less likely to develop depressive symptoms compared to their peers, but the current emotion regulation measure does not capture such positive emotion regulation strategies.
Additionally, at the within-person level sadness dysregulation both mediated and moderated the association between daily sadness and depressive symptoms. Yet, these two findings appear to work in concert with one another; the significant within-person mediational pathway clarifies the mechanism by which the within-person moderating effect emerged. Specifically, it appears that greater-than-usual sadness dysregulation exacerbates the effect of daily sadness on daily depressive symptoms (the moderating effect) because higher-than-usual sadness leads to higher-than-usual difficulties regulating sadness, which leads to more severe depressive symptoms (the mediating effect). Utilizing mediation to explain potential reasons for moderating effects in this way is encouraged by quantitative prevention scientists (Fairchild & MacKinnon, 2009).
These within-person mediating and moderating effects of sadness dysregulation once again speak to the importance of recognizing daily effects even in “typically” developing children. Indeed, these mediating and moderating within-person effects indicate that even well-regulated children can have days where higher-than-usual sadness predicts greater-than-usual difficulty regulating sadness and subsequently increased depressive symptoms. Therefore, as a stronger test of this potential causal pathway, evidence-based strategies from cognitive-behavioral therapeutic (CBT) frameworks could be taught to all adolescents in community settings to ensure they have effective strategies to cope with sadness when it arises. Examples of such daily self-regulation exercises from the CBT literature include daily pleasant activity scheduling, daily mood monitoring (via mood-monitoring phone applications, daily journaling, etc.), and daily check-ins with trusted social supports (such as friends and family members; Friedberg & McClure, 2015).
The Effects of Emotion Regulation Differ Depending On The Emotion (Hypothesis 3)
Exploration of the third hypothesis revealed differences in how emotion regulation mediated or moderated associations between anger and aggression, compared to sadness and depressive symptoms. Specifically, whereas sadness dysregulation had both between- and within-person moderating effects, and a within-person mediating effect, on sadness-depressive symptom associations, anger dysregulation had only between-person mediating effects on anger-aggressiveness associations. Thus, the major difference between these two emotion-mental distress associations was that sadness emotion dysregulation demonstrated both moderating and mediating within-person effects, whereas anger emotion dysregulation had no such within-person, daily meditating or moderating effects. This difference might have emerged for multiple reasons. One possibility could have been greater within-person variation in sadness dysregulation compared to anger dysregulation, and therefore moderating and mediating effects may have emerged at the within-person level for sadness dysregulation simply because there was more day-to-day variability in use of these techniques. Yet the data do not support this explanation, as variations in adolescent endorsement of daily sadness dysregulation and anger dysregulation were identical (SD = 0.53).
However, one tentative explanation emerges when one examines daily variability in aggressive, versus depressive, symptoms. Specifically, it appears that depressive symptoms are much more variable over the course of a day than aggressive symptoms. Despite being on the same 0–2 measurement scale, and having almost the exact same mean, the standard deviation for depressive symptoms (M = 0.11, SD = 0.29), was almost 1/3rd larger than the standard deviation for aggressive symptoms (M = 0.10, SD = 0.21). Additionally, in the final models labeled “Model Including Sadness and Sadness Emotion Dysregulation” (Table 1) and “Model Including Anger and Anger Emotion Dysregulation” (Table 2), aggressive symptoms experienced at the within-person level from one day to the next were highly correlated (r =.70, p < .01), whereas depressive symptoms were not correlated (r = .01, p = .98). This indicates that aggressive symptoms were much more likely to show stability within an individual across multiple days than depressive symptoms. In the face of such day-over-day stability in aggressive symptoms, fluctuations in anger regulation within a person on any specific day may have been a relative “drop in the bucket” and had little effect on aggressive symptom fluctuations. Consequently, mediating and moderating effects of daily anger regulation could be dampened. Another alternative explanation for the lack of within-person anger regulation mediation/moderation may involve the measurement of emotion dysregulation in the current sample. Several items examining emotion dysregulation, including those assessing nonacceptance of emotional responses (“I feel ashamed with myself for feeling angry/sad”), limited access to emotion regulation strategies (“Because I am angry/sad, it is taking me a long time to feel better”), and low emotional awareness (“I am acknowledging that I feel angry/sad”) might be better suited to capture dysregulation related to sadness than anger.
Limitations and Future Directions
Though this study yields several important insights, it is not without limitations that suggest future directions. As with many studies in the EMA field, this study relied completely on adolescent self-reports (Silk et al., 2003), which could lead to reporting bias and limits generalizability of findings. Future studies could combine adolescent and parent, or adolescent and observational reports, in EMA data analyses. Additionally, it could be argued that these data are somewhat cross-sectional. Emotions and emotion dysregulation were examined at three daily time points, and then participants were asked about depressive and aggressive symptoms during the evening, so there is some level of temporal precedence in the data. However, ultimately, the study measures were all reported on during the same day, albeit every day for 15 consecutive days. Therefore, future investigations could consider the best ways to establish temporal precedence among daily emotional experiences, emotion regulation, and symptoms of mental distress, and to examine, in turn, reciprocal effects between these constructs.
Conclusion
Experiencing depressive and aggressive symptoms is common and impairing in adolescence, and past work demonstrates that adolescents who experience more severe difficult emotions and greater emotion dysregulation at one time experience greater depression and aggression months or years later. In accordance with calls from developmental scientists (Bai & Repetti, 2018), the present study moves beyond solely examining these monthly or annually measured between-person associations by also examining how daily fluctuations in difficult emotions give rise to depressive and aggressive symptoms on a daily basis within adolescents. By utilizing an innovative EMA methodology that captures these associations, and a MLM analytic framework that allows the disaggregation of between- and within-person, daily effects, the current study advances understanding of associations between emotions and mental distress throughout adolescents’ everyday lives. Results indicate that even in typically-developing adolescents without mental health disorders, daily spikes in sadness or anger can lead to increased risk for the emergence of depressive or aggressive symptoms. Additionally, results identify adolescent emotion dysregulation as an important mediator and moderator of these associations, and that the nature of such mediating and moderating effects differs across discrete difficult emotions (i.e., sadness versus anger). Collectively, results suggest that strategies for identifying and coping with daily sadness and anger, and strategies for adaptively regulating oneself when faced with such emotions, should be introduced to all adolescents (not just those who are chronically sad, angry, or dysregulated). Ultimately, the present findings advance understanding of how emotions impact mental distress on a daily basis for adolescents, emphasize the importance of examining discrete, specific emotions in adolescents, and shed new light on how emotional regulatory capacities influence emotions and mental health in adolescents’ everyday experiences.
References
- Achenbach TM, & Rescorla LA (2001). Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families. [Google Scholar]
- Bai S, & Repetti RL (2018). Negative and positive emotion responses to daily school problems: Links to internalizing and externalizing symptoms. Journal of Abnormal Child Psychology, 46(3), 423–435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barkley RA, & Robin AL (2014). Defiant adolescents: A clinician’s manual for assessment and family intervention (2nd ed.). New York, NY: Guilford Press. [Google Scholar]
- Bolger N, & Laurenceau J-P (2013). Intensive longitudinal methods: An introduction to diary and experience sampling research. New York, NY: Guilford Press. [Google Scholar]
- Brockman R, Ciarrochi J, Parker P, & Kashdan T (2017). Emotion regulation strategies in daily life: Mindfulness, cognitive reappraisal and emotion suppression. Cognitive Behaviour Therapy, 46(2), 91–113. [DOI] [PubMed] [Google Scholar]
- Brotman MA, Kircanski K, Stringaris A, Pine DS, & Leibenluft E (2017). Irritability in youths: A translational model. The American Journal of Psychiatry, 174(6), 520–532. [DOI] [PubMed] [Google Scholar]
- Curran PJ, & Bauer DJ (2011). The disaggregation of within-person and between-person effects in longitudinal models of change. Annual Review of Psychology, 62, 583–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N, Cumberland A, Spinrad TL, Fabes RA, Shepard SA, Reiser M, … Guthrie IK (2001). The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Development, 72(4), 1112–1134. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Spinrad TL, & Eggum ND (2010). Emotion-related self-regulation and its relation to children’s maladjustment. Annual Review of Clinical Psychology, 6, 495–525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairchild AJ, & MacKinnon DP (2009). A general model for testing mediation and moderation effects. Prevention Science, 10(2), 87–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedberg RD, & McClure JM (2015). Clinical practice of cognitive therapy with children and adolescents: The nuts and bolts, 2nd ed New York, NY: Guilford Press. [Google Scholar]
- Gratz KL, & Roemer L (2004). Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. Journal of Psychopathology and Behavioral Assessment, 26(1), 41–54. [Google Scholar]
- Kovacs M, & Yaroslavsky I (2014). Practitioner review: Dysphoria and its regulation in child and adolescent depression. Journal of Child Psychology and Psychiatry, 55(7), 741–757. 10.1111/jcpp.12172 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lennarz HK, Hollenstein T, Lichtwarck-Aschoff A, Kuntsche E, & Granic I (2019). Emotion regulation in action: Use, selection, and success of emotion regulation in adolescents’ daily lives. International Journal of Behavioral Development, 43(1), 1–11. https://doi-org.proxy.lib.duke.edu/10.1177/0165025418755540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maciejewski DF, van Lier PAC, Branje SJT, Meeus WHJ, & Koot HM (2017). A daily diary study on adolescent emotional experiences: Measurement invariance and developmental trajectories. Psychological Assessment, 29(1), 35–49. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Curran PJ, & Bauer DJ (2006). Computational tools for probing interaction effects in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics, 31, 437–448. [Google Scholar]
- Rothenberg WA, Weinstein A, Dandes EA, & Jent JF (2019). Improving emotion regulation in young children: Effects of Parent-Child Interaction Therapy and emotion coaching strategies. Journal of Child and Family Studies, 28(3), 720–731. [Google Scholar]
- Schacter HL, & Margolin G (2018). When it feels good to give: Depressive symptoms, daily prosocial behavior, and adolescent mood. Emotion. 10.1037/emo0000494.supp (Supplemental) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silk JS, Steinberg L, & Morris AS (2003). Adolescents’ emotion regulation in daily life: Links to depressive symptoms and problem behavior. Child Development, 74(6), 1869–1880. [DOI] [PubMed] [Google Scholar]
- South SC, & Miller ML (2014). Measuring momentary stress, affect, and cognition: Relationships with the internalizing and externalizing spectra. Journal of Psychopathology and Behavioral Assessment, 36(1), 93–104. [Google Scholar]
- Tan PZ, Forbes EE, Dahl RE, Ryan ND, Siegle GJ, Ladouceur CD, & Silk JS (2012). Emotional reactivity and regulation in anxious and nonanxious youth: A cell‐phone ecological momentary assessment study. Journal of Child Psychology and Psychiatry, 53(2), 197–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wen CKF, Schneider S, Stone AA, & Spruijt-Metz D (2017). Compliance with mobile ecological momentary assessment protocols in children and adolescents: A systematic review and meta-analysis. Journal of Medical Internet Research, 19(4), e132. [DOI] [PMC free article] [PubMed] [Google Scholar]