

Abstract
Background
Robot assisted procedures have evolved during the last years, today many surgical, units perform laparoscopic procedures with DaVinci on a regular Basis. The major advantages of Robot assisted procedures comprise technical factors and improved visualization. In Spinal surgery endoscopic stabilization of fractures has become a Standard for many.
Purpose
We have employed DaVinci as an access tool for a retroperitoneal lumbar approach followed by a DaVinci assisted corpectomy and cage implantation to treat a fracture of L3.
Study design
A single operation as proof of concept and demonstration of the method was performed.
Methods
The whole procedure was video recorded. Time factors and clinical outcome were documented.
Results
The procedure was performed safely with no complications. The operating time was longer than usual but within reasonable limits. The postoperatrive outcome did not differ from the usual procedure. The visualization of critical structure during preparation of the vertebral body was superior along with superior soft tissue management with DaVinci.
Conclusion
An endoscopic robotic instrument can be used for endoscopic access surgery. Despite major advantages in visualization and handling of the endoscopic instruments all bone and cartilage preparation must be performed in a traditional endoscpic way because no appropriate instruments are available at present. In order to perform full robotic assisted procedures, new instruments need to be developed.
Keywords: DaVinci, Endoscopic spine surgery, Minimally invasive spine surgery, Retroperitoneal approach
1. Introduction
Robot assisted procedures have evolved during the last years, today many surgical, gynaecological and urologic units perform laparoscopic procedures with DaVinci on a regular Basis. Despite some additional preparation and setup requirements operations can be performed within reasonable time frames. The major advantages of Robot assisted procedures comprise mechanical i.e. technical factors and improved visualization. With respect to surgical technique the device provides very steady instrument movement, and greater Range of motion of the surgical Instrument. With the use of a DaVinci four arms can be supplied with different tools and all arms can be operated separately. Visualization through a three dimensional Video System offers improved visual orientation.
Since the endoscopic treatment of spinal pathology has gained popularity in orthopaedics and neurosurgery, endoscopic stabilization of fractures has become a Standard for many.1,2 Endoscopic treatment is typically possible for stabilization of fractures from the mid-thoracic level down to L4. For Most of fractures a thoracoscopic approach is possible, the lower the fracture the more frequently a so called diaphragm Split is performed. For lower lumbar fractures endoscopic retroperitoneal approaches have been established.3 These retroperitoneal approaches are usually Used in urologic cases.3,4
We have employed DaVinci as an access tool for a retroperitoneal lumbar approach followed by a DaVinci assisted corpectomy and cage implantation to treat a fracture of L3.
2. Methods
Consent was obtained by the patient for publication of the reported method. A Da Vinci Xi system was used for the operation. In brief, DaVinci consists of four robotic arms that can be loaded with various endoscopic instruments i.e. „wirst“, „hook“, „suction“. All arms have 6° of freedom and are operated by the surgeon through the Console that is located outside the sterile field of surgery (Fig. 1).
Fig. 1.
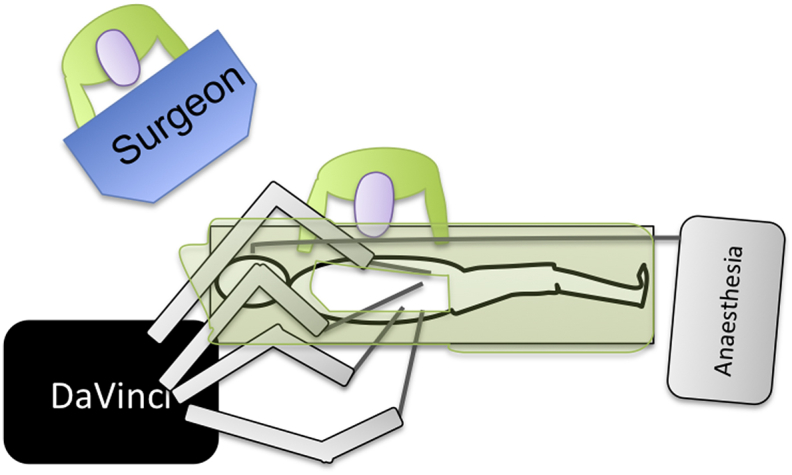
Schematic drawing of the DaVinci system. The operating robot employs 4 arms. The surgeon controls the movement through the console away from the patient. Within the console a 3D vision is presented whereas the screens for assitant and staff are 2D.
First a 3 cm skin incision was made on the left flank region. A blunt dissection of the subcutaneous tissue and perforation of the abdominal fascia and muscle sheath was followed by the insertion of a trocar. A balloon dilator was inserted next to open the retroperitoneal space. Then a second incision was made caudal and anterior to the established portal and a light source and camera were introduced. The dilation of the balloon was visible and inflation was continued until the perirenal fat and the psoas fascia were seen. Two more portals were established under vision in due course anterior and cranial (Fig. 2). The insertion points vary from the ones usually used for endoscopic approaches if DaVinci is used because of a different range of motion of the robot arms. Because the instruments used here are comparably long, the insertion points ly far further apart than for a standard endoscopy. The cavity was then instilled with CO2.
Fig. 2.

Cartography of the portals employed.
When a succer, diaphragm retractor, cauterization hook and a wrist were established, the psoas fascia was opened. Care was taken not to injure the ureter and lumbar plexus. Bluntly dissecting the anterior third of the psoas muscle the lateral aspec to the vertebral body was dissected. The succer and the retractor were now used to retract the psoas muscle and a vascular clipper () was introduced. The segmental vessel was easily visualized under good 3D video control and clipped proximally and distally.
Now a mini-lumbotomy was performed directly over the fractured vertebra. The incision was 4 cm long. After blunt dissection of the subcutaneous tissue the muscle was divided and an Alexis ring was inserted (Fig. 3). Through the seal of the ring four long K-wires were inserted into the disc spaces above and below the fractured vertebra. A standard resection of the vetebra was then performed with a long endoscopic chisel leaving the cranial and caudal end plate intact. After measuring the dimensions of the space created an expandible cage was inserted and expanded under endoscopic vision (Fig. 4). Correct placement and achievment of sufficient lordosis was confirmed by x-ray in two planes (Fig. 5). Wound closure comprised insertion of a retroperitoneal drain and suture of all layers in a standard manner.
Fig. 3.

Intraoperative image of the retroperitoneal space.
Fig. 4.

Insertion of the cage.
Fig. 5.

Postoperative x-ray.
3. Result
The drain was removed 24hrs after the procedure. The patient was mobilized on the first postoperative day. She was discharged after 5 days with clean and dry wounds. She was seen for removal of skin sutures after 12 days at which point she was not taking any pain medication any more. Six weeks post operation x-rays showed good implant position and clinically the patient did report no problems. She was fully mobile and advised to stay of heavy lifting and sports for another 6 weeks. X-rays after 6 months showed osseous integration of the cage.
4. Discussion
Endoscopic retroperitoneal approaches for general and urologic surgical procedures have long been implemented for several indications. In spinal trauma surgery many still prefer a mini open access mainly because insertion of comarably large cages make an incision of 4–6 cm necessary in any way. Nevertheless there are some distinct advantages that can make an endoscopic technique appealing-for the trained surgeon the vision of the operative field is by far better with modern optical devices and the incision as such can be kept to the absolute minimal size. Therefore access morbidity may be reduced in experienced hands. It is worth mentioning that it is of major importance that surgeons need to be familiar with the conventional open technique to control possible complications like severe bleeding and visceral injury. Finley and Lee have reported very promising results of their operations performed in comparable cases, hence the endoscopic approach can be regarded as established.5,6
The DaVinci system takes most of the advantages of endoscopic procedures one step further: The visualization through a three dimensional system is superior to standard 2D and control of the instruments is far more accurate and the range of motion of the instruments is bigger. One possible further advantage is the control of four arms by one surgeon. In a conventional endoscopy part of the control of the operation lies in the hands of an assistant whereas with the DaVinci system all instruments can be operated by one surgeon. There are some reports on previous spinal procedures with DaVinci. In an animal experiment a thoarcoscopic vertebrectomy was performed succesfully.6 On youtube a video report on a lumber spinal intervention is presented by an inidan team (https://www.youtube.com/watch?v=bRy0mEtCwM4). To our knowledge no documentation exists of a retroperitoneal spinal procedure so far.
One of the immediate critisizms regarding our procedure may be the time invested in the technique. Of course the preparation time was longer than for the usual open procedure. The actual operating time was yet acceptable (2:45 h). The surgical outcome of the procedure was favourable for the patient and did not differ from the usual course.
Many different operation techniques have evolved during the last years i.e. the lateral, far lateral or extreme lateral and the endoscopic transeritoneal approach in order to address the disc or the vertebra of the lumbar spine aneriorly. The main concern with such procedures is visceral injury and injury to the lumbosacral plexus. When lateral or far lateral access is used nerve monitoring can provide some assurance not to damage critical structures, but injury to the ureter can only be prevented by direct sight. The DaVinci with three dimensional visualization in great magnification may help to overcome some uncertainty here because even small anatomic variants will be identified during acces surgery. As in standard endoscopic procedures one main advantage is the ability to share the sight on the anatomic situation with all staff and personnel in the operating room as there are at least three screen within one theatre. This aspect of such procedures may not be neglected especially since training is one of the most important aspects of surgical work in a teaching hospital. With a second console, a so called co-pilot, even the three dimensional impression can be shared amongst trainer and trainee. In the case presented here the segmental vessel that can be a cause of severe bleeding if not identified, was clipped with great confidence due to the visualization with DaVinci.
Regarding the surgical preparation DaVinci proved to be versatile and operating the instruments was by far more intuitive than in a conventional endoscopic procedure. Movements of the instruments in conventional procedures require a complex perception and translation into hand movement as all instruments are moving counterwise under cameravision compared to real hand and arm movements. The robotic system is different in that all movements are translated by the system in such way that actual movements of the handle lead to directly corresponding movement of the instrument. Therefore, although for procedures with DaVinci special training is certainly necessary, the handling of the instruments is easier than in a conventional procedure.
One key feature of a robotic endoscopic device is that the freedom of movement of various instruments is greater than in a conventional procedure. The construction of DaVinci allows 360° movement of most instruments including „Wrist“ and „hook“. In a standard endoscopy these instruments can only move according to the range of motion of the surgeon holding the device. In addition all instruments can be locked in certain positions and there is no need for an assistant to steadily hold a camera or a retractor.
One issue that has been discussed by many surgeons using robotic endoscopy is tactile feedback of the instruments, especially „wrist“. At present there is no surgical robot that privides adequate tactile feedback for the preparation of bone (Features of haptic, Friedrich DT) (). Nevertheless Our experience shows that the combination of optical information and experience with the system at least partially outweighs this problem. In the case presented here no obstacles arose from a lack of tactile feedback.
5. Conclusion
Here we present the performance of one of the first DaVinci assisted spinal procedures. The procedure required more time than a standard open corpectomy and cage implantation. The procedure was safely performed and DaVinci was used for the access and preparation of the vertebra and for visualization thoughout the case. No complications were recorded and the outcome was favourable for the patient. Although DaVinci does not offer any option for the preparation of hard tissue like bone the procedure was performed with minimal access under superior vision. This procedure demonstrates the capablities of a commercial robotic system and raises the desire for robotic devices that can fully assist orthopaedic operations.
Declaration of competing interest
The authors declare that no conflict of interest exists.
References
- 1.Regan J.P., Cattey R.P., Henry L.G., Robbins S. Laparoscopically assisted retroperitoneal spinal surgery. J Soc Laparoendosc Surg : J Soc Laparoendosc Surg. 2006;10:493–495. [PMC free article] [PubMed] [Google Scholar]
- 2.Elhadi A.M., Zehri A.H., Zaidi H.A., Almefty K.K., Preul M.C. Surgical efficacy of minimally invasive thoracic discectomy. J Clin Neurosci : Off J Neurosurg Soc Australas. 2015;22:1708–1713. doi: 10.1016/j.jocn.2015.05.013. [DOI] [PubMed] [Google Scholar]
- 3.Rajkumar J.S., Ganesh D., Anirudh J.R., Akbar S., Kishore C.M. Laparoscopic excision of retroperitoneal schwannoma. J Clin Diagn Res : J Clin Diagn Res. 2015;9:PD05–07. doi: 10.7860/JCDR/2015/13792.6762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Benoit T., Peyronnet B., Roumiguie M., Verhoest G., Beauval J.B. Laparoscopic nephrectomy for polycystic kidney: comparison of the transperitoneal and retroperitoneal approaches. World J Urol. 2015;4 doi: 10.1007/s00345-015-1739-5. [DOI] [PubMed] [Google Scholar]
- 5.Finley D., Sherman J.H., Avila E., Bilsky M. Thorascopic resection of an apical paraspinal schwannoma using the da Vinci surgical system. J Neurol Surg A Cent Eur Neurosurg. 2014;75:58–63. doi: 10.1055/s-0033-1345687. [DOI] [PubMed] [Google Scholar]
- 6.Lee J.Y., Bhowmick D.A., Eun D.D., Welch W.C. Minimally invasive, robot-assisted, anterior lumbar interbody fusion: a technical note. J Neurol Surg A Cent Eur Neurosurg. 2013;74:258–261. doi: 10.1055/s-0032-1330121. [DOI] [PubMed] [Google Scholar]