

Abstract
The use of medical cannabis in children is rapidly growing. While robust evidence currently exists only for pure cannabidiol (CBD) to treat specific types of refractory epilepsy, in most cases, artisanal strains of CBD-rich medical cannabis are being used to treat children with various types of refractory epilepsy or irritability associated with autism spectrum disorder (ASD). Other common pediatric disorders that are being considered for cannabis treatment are Tourette syndrome and spasticity. As recreational cannabis use during youth is associated with serious adverse events and medical cannabis use is believed to have a relatively high placebo effect, decisions to use medical cannabis during childhood and adolescence should be made with caution and based on evidence. This review summarizes the current evidence for safety, tolerability, and efficacy of medical cannabis in children with epilepsy and in children with ASD. The main risks associated with use of Δ9-tetrahydrocannabinol (THC) and CBD in the pediatric population are described, as well as the debate regarding the use of whole-plant extract to retain a possible “entourage effect” as opposed to pure cannabinoids that are more standardized and reproducible.
Keywords: Autism, cannabis, CBD, children, epilepsy, THC
NEUROACTIVITY OF CANNABIS
The cannabis plant has a substantial effect on social behavior in humans.1 It enhances interpersonal communication2 and decreases hostile feelings.3 Similar to other plants, cannabis contains hundreds of compounds, including terpenes and flavonoids, many of which have a known or presumed neurological effect.4 Cannabis also contains over a hundred unique compounds called phytocannabinoids (plant-derived cannabinoids).
The two main phytocannabinoids are cannabidiol (CBD) and Δ9-tetrahydrocannabinol (THC). These compounds were characterized in 1963 and 1964, respectively, by Professor Raphael Mechoulam and colleagues from Israel.5,6 Mechoulam found that THC is the plant’s main psychoactive component, responsible for the feeling of a “high.” This effect in the brain is mediated by an abundant G-protein-coupled receptor, which he named cannabinoid type 1 receptor (CB1R). A second receptor that is also directly activated by THC was isolated later from macrophages in the spleen and was named cannabinoid type-2 receptor (CB2R).7 Accordingly, the main effect mediated by CB2R is immunomodulation. This receptor is not significantly expressed in the brain under normal conditions but can be found on glial cells in various brain pathologies.
The two main endogenous ligands of the cannabinoid receptors (“endocannabinoids”) are N-arachidonoylethanolamine (AEA or anandamide) and 2-arachidonoylglycerol (2-AG).
Figure 1 demonstrates the endocannabinoid system. Endocannabinoids are produced “on demand” in postsynaptic neurons and act as retrograde signaling messengers in overactive brain circuits. By activating CB1R in presynaptic neurons, they modulate the synaptic release of neurotransmitters into the synaptic cleft and attenuate the synaptic activity in that circuit.8 After reuptake of the endocannabinoids to the presynaptic neuron by the endocannabinoid membrane transporter, they are immediately hydrolyzed.
Figure 1.
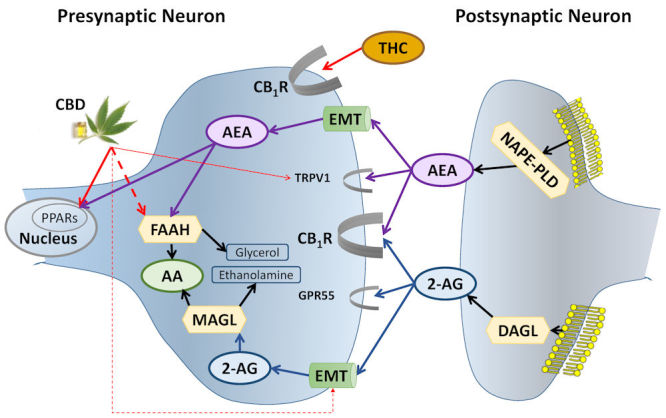
Biosynthesis, Degradation, and Receptor Binding of AEA and 2-AG.
AEA is synthesized from membrane phospholipids in the postsynaptic neuron by NAPE-PLD. It crosses the synapse “against the traffic” and activates CB1R and TRPV1 on the presynaptic neuron. Following reuptake to the presynaptic neuron by the EMT, AEA activates nuclear receptors—PPARs—and is degraded by FAAH.
THC directly activates CB1R; CBD inhibits FAAH and EMT (increasing AEA levels), the endogenous ligand of CB1R. Like AEA, CBD activates PPARs and TRPV1.
2-AG, 2-arachidonoylglycerol (blue ellipses and related lines); AA, arachidonic acid (green ellipses); AEA, anandamide (purple ellipses and related lines); CB1R, cannabinoid type 1 receptor; CBD, cannabidiol; DAGL, diacylglycerol lipase; EMT, endocannabinoid membrane transporter (green tubes); FAAH, fatty acid amide hydrolase; GPR55, G protein-coupled receptor 55; MAGL, monoacylglycerol lipase; NAPE-PLD, N-acylphosphatidylethanolamine-specific phospholipase D; PPARs, peroxisome proliferator-activated receptors; THC, Δ9-tetrahydrocannabinol; TRPV1, transient receptor potential channels of vanilloid type-1. Broken lines = inhibition; half ellipses (
 ) = receptors; hexagons = enzymes; yellow mesh = cell membrane. Thicker lines and half ellipses are of greater importance than the thinner ones. Black lines, other pathways; red lines, phytocannabinoid pathways.
) = receptors; hexagons = enzymes; yellow mesh = cell membrane. Thicker lines and half ellipses are of greater importance than the thinner ones. Black lines, other pathways; red lines, phytocannabinoid pathways.
While THC directly activates the endocannabinoid system through CB1R, CBD does not activate CB1R directly and is not psychoactive.9 Cannabidiol has a relatively high toxicity threshold and appears to have anxiolytic, antipsychotic, and neuroprotective properties that may be mediated through receptors such as serotonin 5-HT1A, glycine α3 and α1, TRPV1, GPR55, and PPARγ, and by inhibiting adenosine reuptake.10–13 Cannabidiol also inhibits the enzyme fatty acid amide hydrolase (FAAH) that degrades anandamide, the endogenous ligand of CB1R, and hence can indirectly activate the endocannabinoid system (Figure 1).
While 99% pure cannabinoids are more reproducible and standardized than whole-plant extract and thus preferred as a study drug, several studies suggest a synergistic effect for the numerous cannabis compounds in the whole-plant extract.4,14–19 This so-called “entourage effect” remains controversial.20
Future studies should directly assess the effects of pure cannabinoids versus whole-plant extracts in various disorders among different target populations.
MAIN RISKS OF CANNABIS IN CHILDREN
The current knowledge on the long-term side-effects of cannabinoids is based mainly on longitudinal follow-up of recreational cannabis users.21–23 Several large studies have demonstrated that the main risks of decreased motivation,24–26 addiction,27 mild cognitive decline,23,25,28,29 and schizophrenia25,30–32 are directly related to the THC and CBD concentrations in the strain used,33 i.e. the higher the ratio of THC to CBD, the greater the risk. The risk is also elevated among those with younger onset of use (<18 years) and in the presence of other risk factors, such as a family history of schizophrenia and concomitant use of alcohol and tobacco.33,34 Notably, these studies contained very few participants under 10 years old and did not assess daily use of medical cannabis.
Longitudinal follow-up studies in children with epilepsy receiving pure CBD suggest high tolerability and safety,35–37 but these studies included very few participants younger than 5 years old.
Animal studies suggest that using pure CBD and its analogue cannabidivarin (CBDV) during early development is relatively safe38,39 while the use of THC, with or without CBD, during early development was found to impair brain structure and function.40–43
Short-term adverse events of pure CBD or CBD-rich whole-plant extracts include somnolence, weight loss, and increased liver transaminases.35,36,44–47
MEDICAL CANNABIS FOR CHILDREN WITH EPILEPSY
Epilepsy is a common neurological disorder, affecting 0.5%–1% of the world’s population.48 Despite the availability of many effective antiepileptic drugs, about one-third of epileptic patients will continue to have treatment-refractory seizures.49 If a patient continues to have seizures despite appropriate treatment trials with three medications, the probability of achieving seizure freedom with subsequent medications is less than 3.5%.49 In such cases, treatment options include epileptic surgery, vagal nerve stimulation, or ketogenic diet. However, for the numerous patients who are not eligible for surgery or do not respond to these treatments, medical cannabis may offer more hope for seizure reduction compared with other pharmacological interventions.
Cannabis treatment for seizures has a long history; it has been used as an anticonvulsant in the ancient Middle East and India for at least 4000 years.50 More recently, leading nineteenth-century neurologists Sir John Russell Reynolds and Sir William Richard Gowers sporadically used THC-rich cannabis to treat seizures. The use of cannabis for epilepsy gradually ceased following the introduction of phenobarbitone in 1912 and phenytoin in 1937. Small studies, mainly of THC-rich cannabis for children with epilepsy, re-emerged in the 1970s with mixed results. Following the discovery of the endocannabinoid system in the 1990s and its major role in neuromodulation, including the attenuation of overactive brain circuits, studies in animal models and anecdotes of successful treatment in refractory epilepsy cases began to accumulate. However, larger-scale clinical studies of cannabinoids in epilepsy were only conducted in recent years.50 These studies focus on the safer cannabinoid, CBD, which seems to have more of an antiepileptic effect than THC in preclinical studies.
A plant-derived pure CBD compound (brand name: Epidiolex) was approved by the US Food and Drug Administration (FDA) in 2018 for treating two severe forms of epilepsy—Dravet and Lennox–Gastaut syndromes51—following a series of successful safety and efficacy studies.36,52–54
A recent systematic review and meta-analysis of the efficacy and tolerability of pure CBD and CBD-rich medical cannabis revealed that CBD is more effective than placebo for treatment-resistant epilepsy, regardless of the etiology of the epileptic syndrome.37 Adverse events included somnolence, decreased appetite and weight, irritability, increased seizure frequency, and diarrhea (in some of the studies). Laboratory abnormalities included elevation of liver transaminases in patients who also received valproic acid. Short-term adverse events were found to be similar for pure CBD and CBD-rich medical cannabis. Adverse events were more frequent at treatment onset compared with long-term follow-up.37 Clinicians should also be aware of cross-reactivity between CBD or CBD-rich medical cannabis and antiepileptic medications that are also metabolized by the cytochrome P450 complex. Notably, active metabolites of benzodiazepines significantly increase with concomitant use of CBD and CBD-rich medical cannabis.
MEDICAL CANNABIS FOR CHILDREN WITH AUTISM SPECTRUM DISORDER
Autism spectrum disorder (ASD) affects up to 2.5% of children worldwide and is a major public health challenge.55 Individuals with ASD have social and communication difficulties, stereotyped or repetitive behaviors and interests, sensory problems, and, in many cases, cognitive impairment and disruptive behaviors. These deficits are present in early childhood and lead to significant disability.56
Approximately 50% of children and adolescents with ASD demonstrate behavioral difficulties, including tantrums, non-compliance, aggression, and self-injury.57–59 This rate is higher than in any other neurodevelopmental disorder.60–65 The behavioral difficulties of children with ASD increase their social isolation66,67 and often cause more distress to caregivers than the core autistic symptoms.68–70 Maladaptive behaviors also limit the child’s ability to benefit from intervention efforts, thereby impairing the long-term prognosis.71
Standard treatment for these problems is based on behavioral interventions71–75 combined with medications,76,77 particularly atypical antipsychotics78–84 and mood stabilizers.85 However, both the efficacy and tolerability of pharmacotherapy in children with ASD are less favorable than among typically developing children with similar symptoms.86
As a result, despite extensive behavioral and medical treatment, 40% of the children and youth with ASD suffer from maladaptive behavior87 that severely impacts their quality of life and takes a heavy toll on their families.69,88 The frustration from current medical treatment leads to an exceptionally high percentage of parents seeking help from complementary and alternative medicine.89,90
Epilepsy is one of the most common comorbid conditions in ASD, affecting 10%–30% of children and youth with ASD,91 and several pathophysiological processes are implicated in both disease processes.92 Hence, the positive effect of cannabinoids in refractory patients is relevant for individuals with ASD.
The CB1R is highly expressed in the frontal cortex and subcortical areas associated with social functioning.93,94 The CB1 receptors and their endogenous ligands anandamide and 2-AG regulate social play and social anxiety in animal models95–100 and in humans.101–103
Activation of the endocannabinoid system in the nucleus accumbens (anandamide mobilization and consequent activation of CB1 receptors) driven by oxytocin, a neuropeptide that reinforces social bonding, was demonstrated to be necessary and sufficient to express the rewarding properties of social interaction.104 Reduced endocannabinoid activity was demonstrated in several animal models of ASD,105 including monogenic (fragile-X,106 neuroligin 3107), polygenic (BTBR105), and environmental (rat valproic acid108) models. Activation of the endocannabinoid system105–108 and administration of CBD105 have been shown to restore social deficits in some models. A single oral administration of 600 mg CBD to 34 men (17 neurotypicals and 17 with ASD) increased prefrontal gamma-aminobutyric acid (GABA) activity in neurotypicals and decreased GABA activity in those with ASD.109 Additionally, children with ASD have been found to have lower peripheral endocannabinoid levels.110,111
Therefore, dysregulation of the endocannabinoid system may play an important role in ASD pathophysiology and may represent a target for pharmacological intervention.112
Four uncontrolled case-series, including 60, 188, 53, and 18 children with ASD and severe behavioral problems, reported high tolerability and efficacy of artisanal CBD-rich cannabis strains.44–47 In the largest cohort, data collection was partial, and there was also an unknown overlap between the first three cohorts. Most participants were followed for at least 6 months, and the retention rate was about 80%.
The treatment was reported to substantially decrease the irritability and anxiety in most of the participants and to improve the social deficits in about half of the subjects, but these results should be interpreted cautiously.
Cannabinoid treatment is associated with a relatively high placebo effect, compared with other pharmacological treatments.113 Placebo effect is expected to be even higher in ASD studies which use subjective behavioral assessments.114 Hence, placebo-controlled studies are required even for a preliminary assessment of efficacy. To date, only one controlled study was completed (NCT02956226) and another is ongoing (NCT03202303).
NCT02956226 was a phase 2, proof-of-concept trial, conducted in a single referral center, Shaare Zedek Medical Center, Jerusalem, Israel. In this double-blind, placebo-controlled trial, 150 children (age 5–21 years) with ASD and behavioral problems (Clinical Global Impression of Severity ≥4), were randomized (in a 1:1:1 ratio) to receive either placebo or one of two cannabinoid solutions for 12 weeks. The cannabinoid solutions were: (1) whole-plant cannabis extract containing cannabidiol (CBD) and Δ9-tetrahydrocannabinol (THC) in a 20:1 ratio; and (2) purified CBD and THC in the same ratio and dose, without other components of the cannabis plant such as minor cannabinoids, terpenes, and flavonoids which may also contribute to the therapeutic effect in an entourage effect.4 The rationale for THC use was previous experience with similar cannabis strains in open-label studies44–46 and the known effects of THC on social behavior.115 The taste, smell, and texture of the three study interventions were carefully adjusted for similarity, which was approved by a professional taster. Participants received either placebo or cannabinoids for 12 weeks to test efficacy, followed by a 4-week washout, and crossed-over to receive another treatment for 12 weeks to further assess tolerability. The treatments were given orally as an add-on to any pre-existing treatment, with an average CBD dose of 5.5 mg/kg/day, divided into three daily doses. There were no serious treatment-related adverse events. The most prevalent adverse events were somnolence and loss of appetite. In some of the measures, cannabinoids reduced the irritability and even the core symptoms of autism significantly more than placebo, with no advantage of the whole-plant extract over the pure cannabinoids.
MEDICAL CANNABIS FOR CHILDREN WITH SPASTICITY AND OTHER INDICATIONS
An open-label study of 25 children (age 1–17 years) with a complex motor disorder116 demonstrated improvement in spasticity and dystonia, sleep difficulties, pain severity, and quality of life. The participants received one of two artisanal strains of CBD-rich cannabis for 5 months: either a 20:1 CBD:THC ratio or a 6:1 ratio. No significant differences were found between the two strains. Two case series, one with 12 children with treatment-refractory spasticity related to developmental disorders117 and one with 7 children with pantothenate kinase-associated neurodegeneration (PKAN),118 reported improvement in the spasticity and dystonia in some of the children after treatment with dronabinol, a synthetic form of THC (spasticity) or various cannabis strains (PKAN). Case reports of children who received cannabis for other indications119 included cases of: neuropathic pain and comorbid major depressive disorder (dronabinol, n=2), anxiety and sleep in PTSD (CBD, n=1), and Tourette syndrome (THC, n=1). Larger open-label studies and randomized studies are required prior to clinical use of cannabis for these indications.
DISCUSSION
Public interest in cannabis-based treatment is rapidly growing, especially in disorders with substantial unmet needs such as pediatric ASD and refractory epilepsy. This review summarizes current knowledge on the neuroactivity of cannabinoids, potential risks, and evidence of efficacy and tolerability in epilepsy and ASD. While most patients receive a variety of artisanal strains, only pure CBD for epilepsy has been rigorously evaluated in controlled trials thus far, with modest but significant improvement in motor seizures and acceptable tolerability. Adverse events included somnolence and reduced appetite. Important interactions with antiepileptic drugs include an increased risk of hepatotoxicity with valproic acid and an increased level of active metabolites with benzodiazepines, contributing to somnolence and potentially to efficacy.
While some studies suggest that artisanal strains with a very high ratio of CBD:THC (e.g. 20:1) are as safe and potent as pure CBD, this issue should be evaluated in future studies. Notably, artisanal preparations, if used, should be obtained from government-controlled sources (preferably good manufacturing practices-approved) as several studies demonstrated significant inconsistency between product labels and actual content in many cases.
In ASD, the gap between published evidence and public beliefs is much wider. Preclinical studies and case series, reporting successful treatment with artisanal CBD-rich cannabis strains in children with ASD and severe irritability, have triggered widespread use of various cannabis strains in children with ASD, despite a lack of published controlled studies. Moreover, parents often request medical cannabis to treat the core autistic symptoms—not the associated irritability—and this request often comes from parents of children younger than 5 years. Some parents prefer to try medical cannabis for irritability as a first-line treatment, as it is perceived as natural and hence safer, compared with the FDA-approved antipsychotics, risperidone and aripiprazole. Many families are interested in products with a relatively high content of THC, which carries a higher risk of severe neurobehavioral comorbidities in this vulnerable population compared with the general population.
In our opinion, the use of medical cannabis in ASD should be currently limited to clinical trials and highly selected cases of treatment-resistant severe irritability.
Abbreviations
- ASD
autism spectrum disorder
- CBD
cannabidiol
- THC
Δ9-tetrahydrocannabinol.
Footnotes
Conflict of interest: Adi Aran reports receiving personal fees and stock options for advisory roles at BOL Pharma. No potential conflict of interest relevant to this article was reported for Dalit Cayam-Rand.
REFERENCES
- 1.Tart CT. Marijuana intoxication common experiences. Nature. 1970;226:701–4. doi: 10.1038/226701a0. [DOI] [PubMed] [Google Scholar]
- 2.Salzman C, Kochansky GE, Van Der Kolk BA, Shader RI. The effect of marijuana on small group process. Am J Drug Alcohol Abuse. 1977;4:251–5. doi: 10.3109/00952997709002763. [DOI] [PubMed] [Google Scholar]
- 3.Salzman C, Van Der Kolk BA, Shader RI. Marijuana and hostility in a small-group setting. Am J Psychiatry. 1976;133:1029–33. doi: 10.1176/ajp.133.9.1029. [DOI] [PubMed] [Google Scholar]
- 4.Russo EB. The case for the entourage effect and conventional breeding of clinical cannabis: no “strain,” no gain. Front Plant Sci. 2018;1969;9 doi: 10.3389/fpls.2018.01969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gaoni Y, Mechoulam R. Isolation, structure and partial synthesis of an active constituent of hashish. J Am Chem Soc. 1964;86:1646–7. doi: 10.1021/ja01062a046. [DOI] [Google Scholar]
- 6.Mechoulam R, Shvo Y. Hashish–I: The structure of cannabidiol. Tetrahedron. 1963;12:2073–8. doi: 10.1016/0040-4020(63)85022-X. [DOI] [PubMed] [Google Scholar]
- 7.Munro S, Thomas KL, Abu-Shaar M. Molecular characterization of a peripheral receptor for cannabinoids. Nature. 1993;365:61–5. doi: 10.1038/365061a0. [DOI] [PubMed] [Google Scholar]
- 8.Guerrero-Alba R, Barragán-Iglesias P, González-Hernández A, et al. Some prospective alternatives for treating pain: the endocannabinoid system and its putative receptors GPR18 and GPR55. Front Pharmacol. 2018;9:1496. doi: 10.3389/fphar.2018.01496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Szkudlarek HJ, Desai SJ, Renard J, et al. Δ-9-Tetrahydrocannabinol and cannabidiol produce dissociable effects on prefrontal cortical executive function and regulation of affective behaviors. Neuropsychopharmacology. 2019;44:817–25. doi: 10.1038/s41386-018-0282-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Campos AC, Fogaça MV, Scarante FF, et al. Plastic and neuroprotective mechanisms involved in the therapeutic effects of cannabidiol in psychiatric disorders. Front Pharmacol. 2017;8:269. doi: 10.3389/fphar.2017.00269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McGuire P, Robson P, Cubala WJ, et al. Cannabidiol (CBD) as an adjunctive therapy in schizophrenia: a multicenter randomized controlled trial. Am J Psychiatry. 2018;175:225–31. doi: 10.1176/appi.ajp.2017.17030325. [DOI] [PubMed] [Google Scholar]
- 12.Devinsky O, Cilio MR, Cross H, et al. Cannabidiol: pharmacology and potential therapeutic role in epilepsy and other neuropsychiatric disorders. Epilepsia. 2014;55:791–802. doi: 10.1111/epi.12631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Iannotti FA, Hill CL, Leo A, et al. Nonpsychotropic plant cannabinoids, cannabidivarin (CBDV) and cannabidiol (CBD), activate and desensitize transient receptor potential vanilloid 1 (TRPV1) channels in vitro: potential for the treatment of neuronal hyperexcitability. ACS Chem Neurosci. 2014;5:1131–41. doi: 10.1021/cn5000524. [DOI] [PubMed] [Google Scholar]
- 14.Ben-Shabat S, Fride E, Sheskin T, et al. An entourage effect: inactive endogenous fatty acid glycerol esters enhance 2-arachidonoyl-glycerol cannabinoid activity. Eur J Pharmacol. 1998;353:23–31. doi: 10.1016/s0014-2999(98)00392-6. [DOI] [PubMed] [Google Scholar]
- 15.Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol. 2011;163:1344–64. doi: 10.1111/j.1476-5381.2011.01238.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sanchez-Ramos J. The entourage effect of the phytocannabinoids. Ann Neurol. 2015;77:1083. doi: 10.1002/ana.24402. [DOI] [PubMed] [Google Scholar]
- 17.Blasco-Benito S, Seijo-Vila M, Caro-Villalobos M, et al. Appraising the “entourage effect”: Antitumor action of a pure cannabinoid versus a botanical drug preparation in preclinical models of breast cancer. Biochem Pharmacol. 2018;157:285–93. doi: 10.1016/j.bcp.2018.06.025. [DOI] [PubMed] [Google Scholar]
- 18.Ferber SG, Namdar D, Hen-Shoval D, et al. The “entourage effect”: Terpenes coupled with cannabinoids for the treatment of mood disorders and anxiety disorders. Curr Neuropharmacol. 2020;18(2) doi: 10.2174/1570159X17666190903103923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Namdar D, Voet H, Ajjampura V, et al. Terpenoids and phytocannabinoids co-produced in Cannabis sativa strains show specific interaction for cell cytotoxic activity. Molecules. 2019;24 doi: 10.3390/molecules24173031. pii:E3031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Santiago M, Sachdev S, Arnold JC, McGregor IS, Connor M. Absence of entourage: terpenoids commonly found in Cannabis sativa do not modulate the functional activity of Δ9-THC at human CB1 and CB2 receptors. Cannabis Cannabinoid Res. 2019;4:165–76. doi: 10.1089/can.2019.0016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schrot RJ, Hubbard JR. Cannabinoids: medical implications. Ann Med. 2016;48:128–41. doi: 10.3109/07853890.2016.1145794. [DOI] [PubMed] [Google Scholar]
- 22.Levine A, Clemenza K, Rynn M, Lieberman J. Evidence for the risks and consequences of adolescent cannabis exposure. J Am Acad Child Adolesc Psychiatry. 2017;56:214–25. doi: 10.1016/j.jaac.2016.12.014. [DOI] [PubMed] [Google Scholar]
- 23.Krebs MO, Kebir O, Jay TM. Exposure to cannabinoids can lead to persistent cognitive and psychiatric disorders. Eur J Pain. 2019;23:1225–33. doi: 10.1002/ejp.1377. [DOI] [PubMed] [Google Scholar]
- 24.Morgan CJ, Freeman TP, Schafer GL, Curran HV. Cannabidiol attenuates the appetitive effects of delta 9-tetrahydrocannabinol in humans smoking their chosen cannabis. Neuropsychopharmacology. 2010;35:1879–85. doi: 10.1038/npp.2010.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Morgan CJ, Gardener C, Schafer G, et al. Sub-chronic impact of cannabinoids in street cannabis on cognition, psychotic-like symptoms and psychological well-being. Psychol Med. 2012;42:391–400. doi: 10.1017/S0033291711001322. [DOI] [PubMed] [Google Scholar]
- 26.Zlebnik NE, Cheer JF. Beyond the CB1 receptor: is cannabidiol the answer for disorders of motivation? Annu Rev Neurosci. 2016;39:1–17. doi: 10.1146/annurev-neuro-070815-014038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hurd YL, Yoon M, Manini AF, et al. Early phase in the development of cannabidiol as a treatment for addiction: opioid relapse takes initial center stage. Neurotherapeutics. 2015;12:807–15. doi: 10.1007/s13311-015-0373-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Morgan CJ, Schafer G, Freeman TP, Curran HV. Impact of cannabidiol on the acute memory and psychotomimetic effects of smoked cannabis: naturalistic study. Br J Psychiatry. 2010;197:285–90. doi: 10.1192/bjp.bp.110.077503. [DOI] [PubMed] [Google Scholar]
- 29.Lorenzetti V, Solowij N, Yücel M. The role of cannabinoids in neuroanatomic alterations in cannabis users. Biol Psychiatry. 2016;79:e17–31. doi: 10.1016/j.biopsych.2015.11.013. [DOI] [PubMed] [Google Scholar]
- 30.Iseger TA, Bossong MG. A systematic review of the antipsychotic properties of cannabidiol in humans. Schizophr Res. 2015;162:153–61. doi: 10.1016/j.schres.2015.01.033. [DOI] [PubMed] [Google Scholar]
- 31.Silva TB, Balbino CQ, Weiber AF. The relationship between cannabidiol and psychosis: a review. Ann Clin Psychiatry. 2015;27:134–41. [PubMed] [Google Scholar]
- 32.Ortiz-Medina MB, Perea M, Torales J, et al. Cannabis consumption and psychosis or schizophrenia development. Int J Soc Psychiatry. 2018;64:690–704. doi: 10.1177/0020764018801690. [DOI] [PubMed] [Google Scholar]
- 33.Volkow ND, Baler RD, Compton WM, Weiss SR. Adverse health effects of marijuana use. N Engl J Med. 2014;370:2219–27. doi: 10.1056/NEJMra1402309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.French L, Gray C, Leonard G, et al. Early cannabis use, polygenic risk score for schizophrenia and brain maturation in adolescence. JAMA Psychiatry. 2015;72:1002–11. doi: 10.1001/jamapsychiatry.2015.1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Laux LC, Bebin EM, Checketts D, et al. Long-term safety and efficacy of cannabidiol in children and adults with treatment resistant Lennox-Gastaut syndrome or Dravet syndrome: expanded access program results. Epilepsy Res. 2019;154:13–20. doi: 10.1016/j.eplepsyres.2019.03.015. [DOI] [PubMed] [Google Scholar]
- 36.Szaflarski JP, Bebin EM, Comi AM, et al. Long-term safety and treatment effects of cannabidiol in children and adults with treatment-resistant epilepsies: expanded access program results. Epilepsia. 2018;59:1540–8. doi: 10.1111/epi.14477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.de Carvalho Reis R, Almeida KJ, da Silva Lopes L, de Melo Mendes CM, Bor-Seng-Shu E. Efficacy and adverse event profile of cannabidiol and medicinal cannabis for treatment-resistant epilepsy: systematic review and meta-analysis. Epilepsy Behav. 2019;102 doi: 10.1016/j.yebeh.2019.106635. 106635. [DOI] [PubMed] [Google Scholar]
- 38.Huizenga MN, Sepulveda-Rodriguez A, Forcelli PA. Preclinical safety and efficacy of cannabidivarin for early life seizures. Neuropharmacology. 2019;148:189–98. doi: 10.1016/j.neuropharm.2019.01.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Ceprián M, Vargas C, Garcia-Toscano L, et al. Cannabidiol administration prevents hypoxia-ischemia-induced hypomyelination in newborn rats. Front Pharmacol. 2019;10:1131. doi: 10.3389/fphar.2019.01131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Scheyer AF, Borsoi M, Wager-Miller J, et al. Cannabinoid exposure via lactation in rats disrupts perinatal programming of the gamma-aminobutyric acid trajectory and select early-life behaviors. Biol Psychiatry. 2019 doi: 10.1016/j.biopsych.2019.08.023. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Scheyer AF, Melis M, Trezza V, Manzoni OJJ. Consequences of perinatal cannabis exposure. Trends Neurosci. 2019;42:871–84. doi: 10.1016/j.tins.2019.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Thorpe HHA, Hamidullah S, Jenkins BW, Khokhar JY. Adolescent neurodevelopment and substance use: receptor expression and behavioral consequences. Pharmacol Ther. 2019 doi: 10.1016/j.pharmthera.2019.107431. 107431. [DOI] [PubMed] [Google Scholar]
- 43.Schonhofen P, Bristot IJ, Crippa JA, et al. Cannabinoid-based therapies and brain development: potential harmful effect of early modulation of the endocannabinoid system. CNS Drugs. 2018;32:697–712. doi: 10.1007/s40263-018-0550-4. [DOI] [PubMed] [Google Scholar]
- 44.Aran A, Cassuto H, Lubotzky A, Wattad N, Hazan E. Brief report: Cannabidiol-rich cannabis in children with autism spectrum disorder and severe behavioral problems-a retrospective feasibility study. J Autism Dev Disord. 2019;49:1284–8. doi: 10.1007/s10803-018-3808-2. [DOI] [PubMed] [Google Scholar]
- 45.Barchel D, Stolar O, De-Haan T, et al. Oral cannabidiol use in children with autism spectrum disorder to treat related symptoms and co-morbidities. Front Pharmacol. 2019;9:1521. doi: 10.3389/fphar.2018.01521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Bar-Lev Schleider L, Mechoulam R, Saban N, Meiri G, Novack V. Real life experience of medical cannabis treatment in autism: analysis of safety and efficacy. Sci Rep. 2019;9:200. doi: 10.1038/s41598-018-37570-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Fleury-Teixeira P, Caixeta FV, Ramires da Silva LC, Brasil-Neto JP, Malcher-Lopes R. Effects of CBD-enriched Cannabis sativa extract on autism spectrum disorder symptoms: an observational study of 18 participants undergoing compassionate use. Front Neurol. 2019;10:1145. doi: 10.3389/fneur.2019.01145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ngugi AK, Bottomley C, Kleinschmidt I, Sander JW, Newton CR. Estimation of the burden of active and life-time epilepsy: a meta-analytic approach. Epilepsia. 2010;51:883–90. doi: 10.1111/j.1528-1167.2009.02481.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Chen Z, Brodie MJ, Liew D, Kwan P. Treatment outcomes in patients with newly diagnosed epilepsy treated with established and new antiepileptic drugs: a 30-year longitudinal cohort study. JAMA Neurol. 2018;75:279–86. doi: 10.1001/jamaneurol.2017.3949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Russo EB. Cannabis and epilepsy: an ancient treatment returns to the fore. Epilepsy Behav. 2017;70:292–7. doi: 10.1016/j.yebeh.2016.09.040. [DOI] [PubMed] [Google Scholar]
- 51.U.S. Food and Drug Administration. FDA news release: FDA approves first drug comprised of an active ingredient derived from marijuana to treat rare, severe forms of epilepsy. [accessed January 9, 2020]. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm611046.htm.
- 52.Devinsky O, Marsh E, Friedman D, et al. Cannabidiol in patients with treatment-resistant epilepsy: an open-label interventional trial. Lancet Neurol. 2016;15:270–8. doi: 10.1016/S1474-4422(15)00379-8. [DOI] [PubMed] [Google Scholar]
- 53.Devinsky O, Cross JH, Laux L, et al. Trial of cannabidiol for drug-resistant seizures in the Dravet syndrome. N Engl J Med. 2017;376:2011–20. doi: 10.1056/NEJMoa1611618. [DOI] [PubMed] [Google Scholar]
- 54.Devinsky O, Patel AD, Cross JH, et al. Effect of cannabidiol on drop seizures in the Lennox-Gastaut syndrome. N Engl J Med. 2018;378:1888–97. doi: 10.1056/NEJMoa1714631. [DOI] [PubMed] [Google Scholar]
- 55.Xu G, Strathearn L, Liu B, et al. Prevalence and treatment patterns of autism spectrum disorder in the United States, 2016. JAMA Pediatr. 2019;173:153–9. doi: 10.1001/jamapediatrics.2018.4208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, Virginia: American Psychiatric Publishing; 2013. Autism Spectrum Disorder, 29900 (F840) pp. 50–5. [DOI] [Google Scholar]
- 57.Hartley SL, Sikora DM, McCoy R. Prevalence and risk factors of maladaptive behaviour in young children with autistic disorder. J Intellect Disabil Res. 2008;52:819–29. doi: 10.1111/j.1365-2788.2008.01065.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Mukaddes NM, Fateh R. High rates of psychiatric co-morbidity in individuals with Asperger’s disorder. World J Biol Psychiatry. 2010;11:486–92. doi: 10.1080/15622970902789130. [DOI] [PubMed] [Google Scholar]
- 59.Kanne SM, Mazurek MO. Aggression in children and adolescents with ASD: prevalence and risk factors. J Autism Dev Disord. 2011;41:926–37. doi: 10.1007/s10803-010-1118-4. [DOI] [PubMed] [Google Scholar]
- 60.Green J, Gilchrist A, Burton D, Cox A. Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. J Autism Dev Disord. 2000;30:279–93. doi: 10.1023/a:1005523232106. [DOI] [PubMed] [Google Scholar]
- 61.Bradley EA, Summers JA, Wood HL, Bryson SE. Comparing rates of psychiatric and behavior disorders in adolescents and young adults with severe intellectual disability with and without autism. J Autism Dev Disord. 2004;34:151–61. doi: 10.1023/b:jadd.0000022606.97580.19. [DOI] [PubMed] [Google Scholar]
- 62.Gadow KD, DeVincent CJ, Pomeroy J, Azizian A. Psychiatric symptoms in preschool children with PDD and clinic and comparison samples. J Autism Dev Disord. 2004;34:379–93. doi: 10.1023/b:jadd.0000037415.21458.93. [DOI] [PubMed] [Google Scholar]
- 63.Eisenhower AS, Baker BL, Blacher J. Preschool children with intellectual disability: syndrome specificity, behaviour problems, and maternal well-being. J Intellect Disabil Res. 2005;49:657–71. doi: 10.1111/j.1365-2788.2005.00699.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Brereton AV, Tonge BJ, Einfeld SL. Psychopathology in children and adolescents with autism compared to young people with intellectual disability. J Autism Dev Disord. 2006;36:863–70. doi: 10.1007/s10803-006-0125-y. [DOI] [PubMed] [Google Scholar]
- 65.Hill J, Furniss F. Patterns of emotional and behavioural disturbance associated with autistic traits in young people with severe intellectual disabilities and challenging behaviours. Res Dev Disabil. 2006;27:517–28. doi: 10.1016/j.ridd.2005.07.001. [DOI] [PubMed] [Google Scholar]
- 66.Scahill L, McDougle CJ, Aman MG, et al. Effects of risperidone and parent training on adaptive functioning in children with pervasive developmental disorders and serious behavioral problems. J Am Acad Child Adolesc Psychiatry. 2012;51:136–46. doi: 10.1016/j.jaac.2011.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Maskey M, Warnell F, Parr JR, Le Couteur A, McConachie H. Emotional and behavioural problems in children with autism spectrum disorder. J Autism Dev Disord. 2013;43:851–9. doi: 10.1007/s10803-012-1622-9. [DOI] [PubMed] [Google Scholar]
- 68.Hastings RP, Kovshoff H, Ward NJ, degli Espinosa F, Brown T, Remington B. Systems analysis of stress and positive perceptions in mothers and fathers of pre-school children with autism. J Autism Dev Disord. 2005;35:635–44. doi: 10.1007/s10803-005-0007-8. [DOI] [PubMed] [Google Scholar]
- 69.Lecavalier L, Leone S, Wiltz J. The impact of behaviour problems on caregiver stress in young people with autism spectrum disorders. J Intellect Disabil Res. 2006;50:172–83. doi: 10.1111/j.1365-2788.2005.00732.x. [DOI] [PubMed] [Google Scholar]
- 70.Hayes SA, Watson SL. The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J Autism Dev Disord. 2013;43:629–42. doi: 10.1007/s10803-012-1604-y. [DOI] [PubMed] [Google Scholar]
- 71.Horner RH, Carr EG, Strain PS, Todd AW, Reed HK. Problem behavior interventions for young children with autism: a research synthesis. J Autism Dev Disord. 2002;32:423–46. doi: 10.1023/a:1020593922901. [DOI] [PubMed] [Google Scholar]
- 72.Dretzke J, Davenport C, Frew E, et al. The clinical effectiveness of different parenting programmes for children with conduct problems: a systematic review of randomised controlled trials. Child Adolesc Psychiatry Ment Health. 2009;3:7. doi: 10.1186/1753-2000-3-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Reichow B, Barton EE, Boyd BA, Hume K. Early intensive behavioral intervention (EIBI) for young children with autism spectrum disorders (ASD) Cochrane Database Syst Rev. 2012;10:CD009260. doi: 10.1002/14651858.CD009260.pub2. [DOI] [PubMed] [Google Scholar]
- 74.Oono IP, Honey EJ, McConachie H. Parent-mediated early intervention for young children with autism spectrum disorders (ASD) Cochrane Database Syst Rev. 2013;4:CD009774. doi: 10.1002/14651858.CD009774.pub2. [DOI] [PubMed] [Google Scholar]
- 75.Bearss K, Johnson C, Smith T, et al. Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: a randomized clinical trial. JAMA. 2015;313:1524–33. doi: 10.1001/jama.2015.3150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Aman MG, McDougle CJ, Scahill L, et al. Medication and parent training in children with pervasive developmental disorders and serious behavior problems: results from a randomized clinical trial. J Am Acad Child Adolesc Psychiatry. 2009;48:1143–54. doi: 10.1097/CHI.0b013e3181bfd669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Bearss K, Lecavalier L, Minshawi N, et al. Toward an exportable parent training program for disruptive behaviors in autism spectrum disorders. Neuropsychiatry (London) 2013;3:169–80. doi: 10.2217/npy.13.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.McCracken JT, McGough J, Shah B, et al. Risperidone in children with autism and serious behavioral problems. N Engl J Med. 2002;347:314–21. doi: 10.1056/NEJMoa013171. [DOI] [PubMed] [Google Scholar]
- 79.Shea S, Turgay A, Carroll A, et al. Risperidone in the treatment of disruptive behavioral symptoms in children with autistic and other pervasive developmental disorders. Pediatrics. 2004;114:e634–41. doi: 10.1542/peds.2003-0264-F. [DOI] [PubMed] [Google Scholar]
- 80.Research Units on Pediatric Psychopharmacology Autism Network. Risperidone treatment of autistic disorder: longer-term benefits and blinded discontinuation after 6 months. Am J Psychiatry. 2005;162:1361–9. doi: 10.1176/appi.ajp.162.7.1361. [DOI] [PubMed] [Google Scholar]
- 81.Williams SK, Scahill L, Vitiello B, et al. Risperidone and adaptive behavior in children with autism. J Am Acad Child Adolesc Psychiatry. 2006;45:431–9. doi: 10.1097/01.chi.0000196423.80717.32. [DOI] [PubMed] [Google Scholar]
- 82.Loy JH, Merry SN, Hetrick SE, Stasiak K. Atypical antipsychotics for disruptive behaviour disorders in children and youths. Cochrane Database Syst Rev. 2017;(8):CD008559. doi: 10.1002/14651858.CD008559.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Accordino RE, Kidd C, Politte LC, Henry CA, McDougle CJ. Psychopharmacological interventions in autism spectrum disorder. Expert Opin Pharmacother. 2016;17:937–52. doi: 10.1517/14656566.2016.1154536. [DOI] [PubMed] [Google Scholar]
- 84.Levine SZ, Kodesh A, Goldberg Y, et al. Initial severity and efficacy of risperidone in autism: results from the RUPP trial. Eur Psychiatry. 2016;32:16–20. doi: 10.1016/j.eurpsy.2015.11.004. [DOI] [PubMed] [Google Scholar]
- 85.Canitano R. Mood stabilizers in children and adolescents with autism spectrum disorders. Clin Neuropharmacol. 2015;38:177–82. doi: 10.1097/WNF.0000000000000096. [DOI] [PubMed] [Google Scholar]
- 86.Ji N, Findling RL. An update on pharmacotherapy for autism spectrum disorder in children and adolescents. Curr Opin Psychiatry. 2015;28:91–101. doi: 10.1097/YCO.0000000000000132. [DOI] [PubMed] [Google Scholar]
- 87.Adler BA, Wink LK, Early M, et al. Drug-refractory aggression, self-injurious behavior, and severe tantrums in autism spectrum disorders: a chart review study. Autism. 2015;19:102–6. doi: 10.1177/1362361314524641. [DOI] [PubMed] [Google Scholar]
- 88.Rivard M, Terroux A, Parent-Boursier C, Mercier C. Determinants of stress in parents of children with autism spectrum disorders. J Autism Dev Disord. 2014;44:1609–20. doi: 10.1007/s10803-013-2028-z. [DOI] [PubMed] [Google Scholar]
- 89.Salomone E, Charman T, McConachie H, Warreyn P Working Group 4. COST Action ‘Enhancing the Scientific Study of Early Autism’. Prevalence and correlates of use of complementary and alternative medicine in children with autism spectrum disorder in Europe. Eur J Pediatr. 2015;174:1277–85. doi: 10.1007/s00431-015-2531-7. [DOI] [PubMed] [Google Scholar]
- 90.Owen-Smith AA, Bent S, Lynch FL, et al. Prevalence and predictors of complementary and alternative medicine use in a large insured sample of children with autism spectrum disorders. Res Autism Spectr Disord. 2015;17:40–51. doi: 10.1016/j.rasd.2015.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ballaban-Gil K, Tuchman R. Epilepsy and epileptiform EEG: association with autism and language disorders. Ment Retard Dev Disabil Rev. 2000;6:300–8. doi: 10.1002/1098-2779(2000)6:4<300::AID-MRDD9>3.0.CO;2-R. [DOI] [PubMed] [Google Scholar]
- 92.Keller R, Basta R, Salerno L, Elia M. Autism, epilepsy, and synaptopathies: a not rare association. Neurol Sci. 2017;38:1353–61. doi: 10.1007/s10072-017-2974-x. [DOI] [PubMed] [Google Scholar]
- 93.Seeley WW, Zhou J, Kim EJ. Frontotemporal dementia: what can the behavioral variant teach us about human brain organization? Neuroscientist. 2012;18:373–85. doi: 10.1177/1073858411410354. [DOI] [PubMed] [Google Scholar]
- 94.Glass M, Dragunow M, Faull RL. Cannabinoid receptors in the human brain: a detailed anatomical and quantitative autoradiographic study in the fetal, neonatal and adult human brain. Neuroscience. 1997;77:299–318. doi: 10.1016/s0306-4522(96)00428-9. [DOI] [PubMed] [Google Scholar]
- 95.Moreira FA, Kaiser N, Monory K, Lutz B. Reduced anxiety-like behaviour induced by genetic and pharmacological inhibition of the endocannabinoid-degrading enzyme fatty acid amide hydrolase (FAAH) is mediated by CB1 receptors. Neuropharmacology. 2008;54:141–50. doi: 10.1016/j.neuropharm.2007.07.005. [DOI] [PubMed] [Google Scholar]
- 96.Cassano T, Gaetani S, Macheda T, et al. Evaluation of the emotional phenotype and serotonergic neurotransmission of fatty acid amide hydrolase-deficient mice. Psychopharmacology. 2011;214:465–76. doi: 10.1007/s00213-010-2051-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Trezza V, Damsteegt R, Manduca A, et al. Endocannabinoids in amygdala and nucleus accumbens mediate social play reward in adolescent rats. J Neurosci. 2012;32:14899–908. doi: 10.1523/JNEUROSCI.0114-12.2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Trezza V, Baarendse PJ, Vanderschuren LJ. The pleasures of play: pharmacological insights into social reward mechanisms. Trends Pharmacol Sci. 2010;31:463–9. doi: 10.1016/j.tips.2010.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Seillier A, Advani T, Cassano T, Hensler JG, Giuffrida A. Inhibition of fatty-acid amide hydrolase and CB1 receptor antagonism differentially affect behavioural responses in normal and PCP-treated rats. Ing J Neuropsychopharmacol. 2010;13:373–86. doi: 10.1017/S146114570999023X. [DOI] [PubMed] [Google Scholar]
- 100.Seillier A, Martinez AA, Giuffrida A. Phencyclidine-induced social withdrawal results from deficient stimulation of cannabinoid CB1 receptors: implications for schizophrenia. Neuropsychopharmacology. 2013;38:1816–24. doi: 10.1038/npp.2013.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Bergamaschi MM, Queiroz RH, Chagas MH, et al. Rimonabant effects on anxiety induced by simulated public speaking in healthy humans: a preliminary report. Hum Psychopharmacol. 2014;29:94–9. doi: 10.1002/hup.2374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Gunduz-Cinar O, MacPherson KP, Cinar R, et al. Convergent translational evidence of a role for anandamide in amygdala-mediated fear extinction, threat processing and stress-reactivity. Mol Psychiatry. 2013;18:813–23. doi: 10.1038/mp.2012.72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Phan KL, Angstadt M, Golden J, Onyewuenyi I, Popovska A, de Wit H. Cannabinoid modulation of amygdala reactivity to social signals of threat in humans. J Neurosci. 2008;28:2313–19. doi: 10.1523/JNEUROSCI.5603-07.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Wei D, Lee D, Cox CD, et al. Endocannabinoid signaling mediates oxytocin-driven social reward. Proc Natl Acad Sci U S A. 2015;112:14084–9. doi: 10.1073/pnas.1509795112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Zamberletti E, Gabaglio M, Parolaro D. The endocannabinoid system and autism spectrum disorders: insights from animal models. Int J Mol Sci. 2017;18 doi: 10.3390/ijms18091916. pii: E1916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Wang W, Cox BM, Jia Y, et al. Treating a novel plasticity defect rescues episodic memory in Fragile X model mice. Mol Psychiatry. 2018;23:1798–806. doi: 10.1038/mp.2017.221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Hosie S, Malone DT, Liu S, et al. Altered amygdala excitation and CB1 receptor modulation of aggressive behavior in the neuroligin-3R451C mouse model of autism. Front Cell Neurosci. 2018;12:234. doi: 10.3389/fncel.2018.00234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Melancia F, Schiavi S, Servadio M, et al. Sex-specific autistic endophenotypes induced by prenatal exposure to valproic acid involve anandamide signalling. Br J Pharmacol. 2018;175:3699–712. doi: 10.1111/bph.14435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Pretzsch CM, Freyberg J, Voinescu B, et al. Effects of cannabidiol on brain excitation and inhibition systems; a randomised placebo-controlled single dose trial during magnetic resonance spectroscopy in adults with and without autism spectrum disorder. Neuropsychopharmacology. 2019;44:1398–405. doi: 10.1038/s41386-019-0333-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Karhson DS, Krasinska KM, Dallaire JA, et al. Plasma anandamide concentrations are lower in children with autism spectrum disorder. Mol Autism. 2018;9:18. doi: 10.1186/s13229-018-0203-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Aran A, Eylon M, Harel M, et al. Lower circulating endocannabinoid levels in children with autism spectrum disorder. Mol Autism. 2019;10:2. doi: 10.1186/s13229-019-0256-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Krueger DD, Brose N. Evidence for a common endocannabinoid-related pathomechanism in autism spectrum disorders. Neuron. 2013;78:408–10. doi: 10.1016/j.neuron.2013.04.030. [DOI] [PubMed] [Google Scholar]
- 113.Lattanzi S, Brigo F, Trinka E, et al. Efficacy and safety of cannabidiol in epilepsy: a systematic review and meta-analysis. Drugs. 2018;78:1791–804. doi: 10.1007/s40265-018-0992-5. [DOI] [PubMed] [Google Scholar]
- 114.Jones RM, Carberry C, Hamo A, Lord C. Placebo-like response in absence of treatment in children with autism. Autism Res. 2017;10:1567–72. doi: 10.1002/aur.1798. [DOI] [PubMed] [Google Scholar]
- 115.Hindocha C, Freeman TP, Schafer G, et al. Acute effects of delta-9-tetrahydrocannabinol, cannabidiol and their combination on facial emotion recognition: a randomised, double-blind, placebo-controlled study in cannabis users. Eur Neuropsychopharmacol. 2015;25:325–34. doi: 10.1016/j.euroneuro.2014.11.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Libzon S, Schleider LB, Saban N, et al. Medical cannabis for pediatric moderate to severe complex motor disorders. J Child Neurol. 2018;33:565–71. doi: 10.1177/0883073818773028. [DOI] [PubMed] [Google Scholar]
- 117.Kuhlen M, Hoell JI, Gagnon G, et al. Effective treatment of spasticity using dronabinol in pediatric palliative care. Eur J Paediatr Neurol. 2016;20:898–903. doi: 10.1016/j.ejpn.2016.07.021. [DOI] [PubMed] [Google Scholar]
- 118.Wilson JL, Gregory A, Wakeman K, et al. Cannabis use in children with pantothenate kinase-associated neurodegeneration. J Child Neurol. 2019;11 doi: 10.1177/0883073819890516. 883073819890516. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 119.Wong SS, Wilens TE. Medical cannabinoids in children and adolescents: a systematic review. Pediatrics. 2017;140 doi: 10.1542/peds.2017-1818. pii:e20171818. [DOI] [PubMed] [Google Scholar]