

Abstract
In India, more than 72 million people have diabetes. Diabetic retinopathy (DR), a vision-threatening complication of people with diabetes, is an important cause of avoidable blindness. The delay in the detection of DR is due to lack of awareness and shortage of ophthalmologists trained in the management of DR. With this background, in 2015, we initiated a capacity-building program “Certificate Course in Evidence Based Management of Diabetic Retinopathy (CCDR)” with an objective to build the skills and core competencies of the physicians across India in the management of diabetes and DR. The program has completed four cycles and 578 physicians have been trained. The course elicited an excellent response, which reflects the much-felt need for skill improvement in DR diagnosis and management for physicians in India. This model demonstrates an innovative modality to address DR-related avoidable blindness in a resource-restraint country like India.
Keywords: Diabetes, diabetic retinopathy, training
Worldwide, the burden of diabetes and its complications is on the rise. In India, more than 72 million people have diabetes.[1] The prevalence of diabetic retinopathy (DR), a vision-threatening complication and an important cause of avoidable blindness and visual impairment in people with diabetes, has been reported to be 17.6%–28.2% in India.[2] The duration of diabetes, hyperglycemia, and hypertension are considered important risk factors for progression of vision loss in people with diabetes.[3] Studies have documented the importance of glycemic and blood pressure control in the progression of DR and vision loss.[4] The delay in the detection of DR is due to lack of awareness and shortage of ophthalmologists trained in the management of DR. In developing countries like India, primary care physicians (PCPs) are the frontline carers for people with diabetes.[5] Therefore, there is a need to improve the capacity of PCPs by updating their clinical knowledge and skills in the management of DR through an evidence-based scientific knowledge enhancement program. This will improve the early diagnosis, timely referrals, and reduce the overall burden of DR.
With this background, in 2015, the Public Health Foundation of India (PHFI) in collaboration with Dr Mohan's Diabetes Education Academy (DMDEA), Chennai, India, the Aravind Eye Care System, Madurai, India, and the Centre for Chronic Disease Control (CCDC), New Delhi, India, initiated a pan India capacity-building program titled “Certificate Course in Evidence Based Management of Diabetic Retinopathy (CCDR).” The Queen Elizabeth Diamond Jubilee Trust (QEDJT) provided the educational grant, with additional supplemental funding from the Leona M. and Harry B. Helmsley Charitable Trust through the London School of Hygiene & Tropical Medicine (LSHTM).[6] The fundamental objective of CCDR was to enhance knowledge, skills, and core competencies of PCPs to prevent and manage DR and to build their network with other PCPs and specialists. The CCDR program was an on-the-job training course with unique features [Table 1]. The four modular course was conducted as once-a-month contact session, with hands-on-skill training and an exit examination. The curriculum covered various aspects of DR with the aim of strengthening PCPs capacity of screening, referral, and management of diabetes and risk factors for complications. The curriculum was developed by the academic partners DMDEA and Aravind Eye Care System and vetted by a panel of eight national experts (diabetologists and retina specialists) [Fig. 1]. The eligibility criterion for PCPs to enrol was a graduate medical degree (MBBS) with clinical experience of more than 3 years. The course comprised of didactic lectures, case studies, and instructional videos and was delivered by 42 regional faculties in 20 centers across 13 states and 1 union territory of India.
Table 1.
Salient features of the certificate course in evidence-based management of diabetic retinopathy
| Evidence-based learning | The focus of teaching is on evidence-based learning with one-to-one interaction with experts of the field. |
| Program curriculum | Updated curriculum is prepared by the academic partner on the basis of inputs by 50 experts across the country. Curriculum is updated annually with inputs from all stakeholders and in context to the latest advancements (didactic lectures, case studies, instructional videos, group exercises, etc.) with hands-on training at premier retina institutes. |
| On-the-job training | The training is conducted once a month on designated weekends to ensure that routine activities of all the stakeholders are not affected. |
| Networking | The program establishes a network between national experts, regional faculty, and primary care physicians, which strengthens referral mechanisms. |
| Advancements in the field of diabetic retinopathy | Participants are offered special packages to attend various conferences and workshops and other training programs across the country. |
| Robust monitoring and evaluation | Robust internal and external monitoring and supervision activities. This enables a standard teaching protocol throughout the country. |
Figure 1.
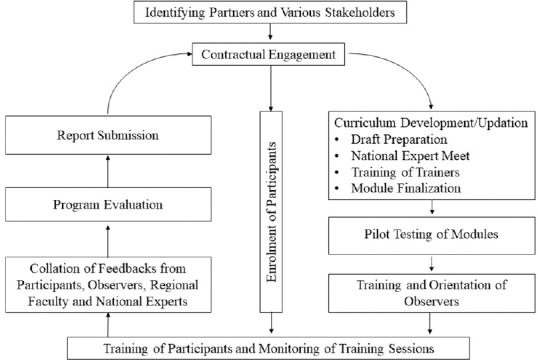
Implementation model of the certificate course in evidence-based management of diabetic retinopathy
A two-member team of physician (internal medicine) and ophthalmologist at each center conducted the sessions. This physician and ophthalmologist combination was unique for bridging the gaps in communication regarding pathogenesis, screening, and management of diabetes mellitus (DM) and DR to the participants. The criteria for certification includes participation in all the four modules (including the pre-test and post-test of each module), submission of course-based assignments, and pass an exit examination with a minimum of 50% score conducted at the end of the course. The program had a robust monitoring and supervision mechanism (onsite/offsite) by 17 observers (public health experts) [Fig. 2]. A final evaluation is being conducted after completion of each cycle, to identify the need for change in the curriculum and course implementation.
Figure 2.
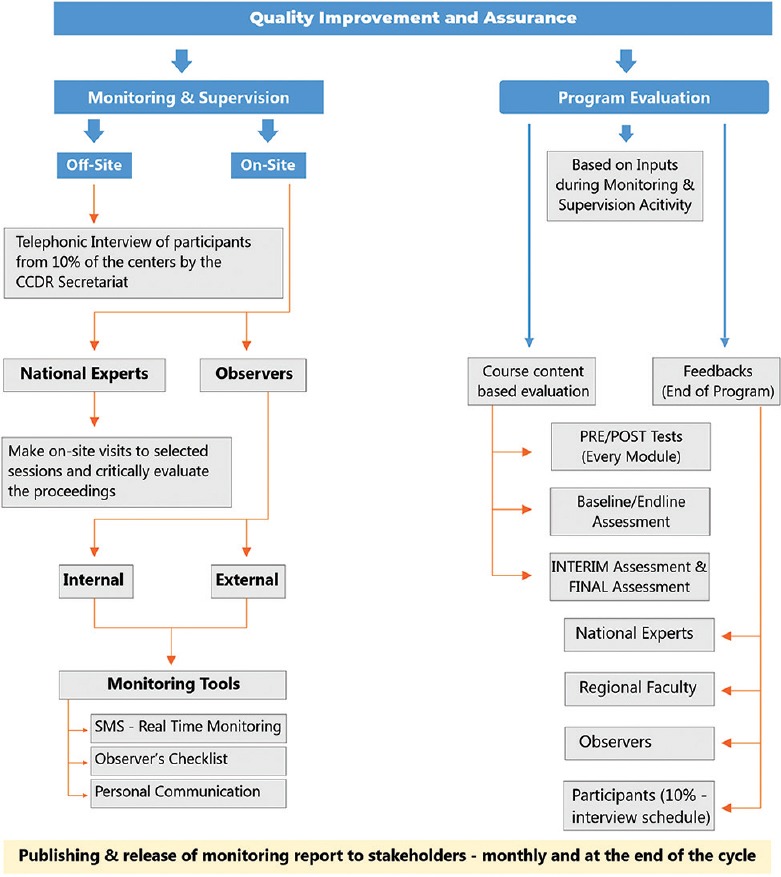
Monitoring and evaluation framework for the certificate course in evidence-based management of diabetic retinopathy
The program has completed four cycles and 578 physicians [profile shown in Table 2] have been trained from 114 districts in India. Seven state governments nominated one-third of the government-affiliated participants from various health facilities [district hospitals, community health centers, primary health centers (PHCs), others]. To assess change in participant's knowledge, a module-based pre/post-test was administered before the start and end of each session which observed an average increase of 1 unit score (on a scale of 10). Based on participant's feedback, 95% agreed that the curriculum was ideal for learning. During the final evaluation, the participants rated the course modules and teaching methodology with an overall score of 9/10 (excellent).
Table 2.
Profile of participants attending the certificate course in evidence-based management of diabetic retinopathy
| Characteristics | Female, n (%) | Male, n (%) | Total, n (%) | |
|---|---|---|---|---|
| 205 (35.5) | 373 (64.5) | 578 (100) | ||
| Age (years) | 25-35 | 131 (63.9) | 167 (44.8) | 298 (51.6) |
| Mean: 37 years | 36-45 | 40 (19.5) | 94 (25.2) | 134 (23.2) |
| Median: 34 years | ≥46 | 34 (16.6) | 112 (30) | 146 (25.3) |
| Clinical experience (years) | ≤10 | 158 (77.1) | 244 (65.4) | 402 (69.6) |
| Mean: 9 years | 11-20 | 32 (15.6) | 67 (18) | 99 (17.1) |
| Median: 4 years | ≥21 | 15 (7.3) | 62 (16.6) | 77 (13.3) |
| Highest qualification | MBBS | 129 (63) | 241 (64.6) | 370 (64) |
| DNB | 10 (4.9) | 22 (5.9) | 32 (5.5) | |
| MD/MS | 65 (31.6) | 106 (28.4) | 171 (29.6) | |
| DM | 1 (0.5) | 4 (1.1) | 5 (0.9) | |
| Organizational affiliation | Government | 110 (53.7) | 175 (46.9) | 285 (49.3) |
| Private | 82 (40) | 185 (49.6) | 267 (46.2) | |
| Others | 13 (6.3) | 13 (3.5) | 26 (4.5) | |
| Teaching affiliation | Non-teaching | 194 (94.6) | 334 (89.5) | 528 (91.3) |
| Teaching | 11 (5.4) | 39 (10.5) | 50 (8.7) |
The CCDR program won several awards and accolades, receiving endorsement from reputed bodies that include UK Research and Innovation, Global Challenges Research Fund through Ornate-India and has been endorsed for 3 years (2019–2022) by the All India Ophthalmological Society (AIOS).
To our knowledge, CCDR is probably the first capacity-building program conducted in India in the management of DR for physicians. The course met an excellent response, which reflects the felt need for skill improvement in DR management for physicians in India. Participant's feedback revealed that after CCDR certification, some of the primary care physicians have already included fundus photography as a part of their investigation armamentarium for patients with DM and are referring to ophthalmologist as necessary. This model demonstrated an innovative modality to address DR-related avoidable blindness in a resource-restraint country like India.
In the government's universal health coverage strategy, a major thrust has been given to PHCs, which requires an effort to upskill doctors at a primary level. CCDR course has been adopted by the Government of Tripura and Madhya Pradesh, India for training of 20 and 100 medical officers under National Health Mission (NHM). The CCDR team is taking initiatives to integrate CCDR into National Programme for Control of Blindness and Visual Impairment (NPCB) for training physicians in management of DR. Beyond India, the course has been adopted by the Ministry of Health in Rwanda, Afghanistan, and Myanmar. These offshore tie-ups are further demonstration of the importance and significance of CCDR in the management of DM and DR in countries with similar economy and resources as India. To ensure sustainability and expand the reach, the CCDR course has now been developed into E-learning model in collaboration with Bosch India.[7]
Conclusion
CCDR is a continued effort to align the program as a sustainable training model and designed to be adaptive to the needs of the PCPs, so that its access and impact reaches the far-off areas. The PCPs (including postgraduates) in India have an unmet need for education on the management of DR and the course implements a system that is responsive to the specific needs of the stakeholders.
Financial support and sponsorship
The Queen Elizabeth Diamond Jubilee Trust, London, UK.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors gratefully acknowledge the contribution of national experts, regional faculty, and observers in delivering the training program.
References
- 1.International Diabetes Federation. IDF Diabetes Atlas. 8th ed. Brussels, Belgium: International Diabetes Federation; 2017. [Last accessed 2019 Sep 09]. Available from: http://www.diabetesatlas.org . [Google Scholar]
- 2.Das T, Aurora A, Chhablani J, Giridhar A, Kumar A, Raman R, et al. Evidence-based review of diabetic macular edema management: Consensus statement on Indian treatment guidelines. Indian J Ophthalmol. 2016;64:14–25. doi: 10.4103/0301-4738.178142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis (Lond) 2015;2:17. doi: 10.1186/s40662-015-0026-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Klein BE. Overview of epidemiologic studies of diabetic retinopathy. Ophthalmic Epidemiol. 2007;14:179–83. doi: 10.1080/09286580701396720. [DOI] [PubMed] [Google Scholar]
- 5.Wiggins MN, Landes RD, Bhaleeya SD, Uwaydat SH. Primary care physicians' knowledge of the ophthalmic effects of diabetes. Can J Ophthalmol. 2013;48:265–8. doi: 10.1016/j.jcjo.2013.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Certificate Course in Evidence Based Management of Diabetic Retinopathy [Internet] c2019. [Last cited on 2019 Sep 09, Last accessed on 2019 Sep 09]. Available from: http://www.ccdr.org.in/
- 7.Evidence Based Management of Diabetic Retinopathy [Internet] c2019. [Last cited on 2019 Oct 03, Last accessed on 2019 Oct 03]. Available from: https://blooms.boschlearningsolutions.com/