

Abstract
Purpose:
The effectiveness of Accredited Social Health Activists (ASHAs) with and without monetary incentive in uptake of diabetic retinopathy (DR) screening at community health center (CHC) was compared in South Gujarat, India.
Methods:
In this non-randomized controlled trial, ASHAs were incentivized to refer people with diabetes mellitus (PwDM) from their respective villages for DR screening after people were sensitized to DM and DR. The minimum sample size was 63 people in each arm.
Results:
Of 162, 50.6% were females, 80.2% were literate, 56.2% were >50 years, 54.3% had increased random blood sugar (RBS), and 59.9% had diabetes for 5 years. The percentage of screening was significantly higher [relative risk (RR) = 4.37, 95% confidence interval (CI) 2.79, 6.84] in ASHA incentive group and health education (HE) group (RR = 3.67, 95% CI 2.35, 5.75) compared with baseline. Providing incentive to ASHAs was not found to be of extra advantage (RR = 1.19, 95% CI 0.89, 1.57). The likelihood of uptake of screening was higher among uncontrolled PwDM, poor literacy, and higher duration of diabetes in incentive phase (P < 0.001) compared with HE. The results show that age (P = 0.017), education (P = 0.015) and level of RBS (P = 0.001) of those referred were significantly associated with incentives to ASHAs.
Conclusion:
ASHAs can be used effectively to refer known PwDM for DR screening especially when DR screening program is introduced in population with low awareness and poor accessibility. When incentives are planned, additional burden on resources should be kept in mind before adapting this model of care.
Keywords: Accredited Social Health activist (ASHA), diabetic retinopathy, health education, incentive, India, screening
The burden of diabetes mellitus (DM) and its consequent morbidities is increasing globally. According to the World Health Organization (WHO), globally there are 422 million people with DM (PwDM) in 2014.[1] In India, there are 72.9 million PwDM in 2017and the numbers would rise to approximately 100 million by the year 2030.[2] The major cause of blindness due to DM is diabetic retinopathy (DR) which is a specific microvascular complication of DM. It is estimated that 10%–25% of the population with diabetes have DR[2] and others have the potential to develop over the period of time.[3,4,5] In India, 12 million PwDM are estimated to have DR. Effective programs for prevention of blindness from DR require good uptake of screening among known PwDM for timely treatment.
In India, tele-ophthalmology has been found to be cost-effective for DR screening where fundus images are read remotely and treatment offered.[6] This newer technique is being used to screen for DR at our vision centers located in tribal areas. Mobilizing PwDM for DR screening to the location where the fundus camera is placed was a challenge. This could be potentially increased with help of village-level health workers. The Accredited Social Health Activist (ASHA) volunteers are one such category personnel who could be engaged to increase DR screening in rural India because they are already performing several health promotion activities and specifically cataract case detection in ophthalmology.[7,8] ASHA volunteers often work on incentives, usually fixed by the Government of India. In this study, we examined the impact of the ASHA volunteers for DR screening promotion with and without incentives.
Methods
This was a nonrandomized controlled trial study that was conducted in two phases at a base hospital in the tribal area of South Gujarat. In the first phase, 55 ASHA volunteers were trained at the base hospital to educate people on DM and DR using the printed information-education-communication (IEC) materials. In the second phase, the same ASHAs were given case-specific incentive for PwDM facilitated for DR screening. The difference was then analyzed to gauge the effect of these two interventions on the uptake of referrals for DR screening at CHC.
A minimum sample size of 274 diabetic patients from the tribal area (α = 0.05, power = 80%, maximum difference = 20%) was required to detect differences in the uptake of screening between three phases (calculated using sample size for two proportions adjusted for alpha). We assumed an attrition rate of 10%.
All PwDM above age 15 years were included. People with juvenile diabetics and those with terminal illness were excluded from the study. Ethical committee of Divyajyoti Trust, Mandvi-Surat approved the study. The study followed the tenets laid down under the Declaration of Helsinki.
After 2 months of baseline screening of PwDM reporting at CHC, the first phase of intervention was implemented after a meeting of ASHAs was convened in April 2018. They were oriented to motivate PwDM to the community health center (CHC) where a fundus camera was installed for DR screening. ASHA volunteers were given the printed IEC materials in local language (Gujarati) and requested to use them for increasing awareness among PwDM in the village. People referred by the ASHA workers were identified from the specific referral slip from the ASHA volunteers of that particular population area. The uptake of referrals for DR screening at CHC was documented.
The second phase of intervention started after another meeting was convened where the same ASHA workers were informed of the monetary incentive of Indian National Rupees (INR) 30 for referring one patient for DR screening and INR 100 if patients received treatment for DR at the base hospital. This incentive was reimbursed to the ASHA workers only after screening and/or treatment was completed. People referred by the ASHA workers were identified from the specific referral slip from the ASHA volunteers of that particular population area. The uptake of referrals for DR screening at CHC was documented.
Data were analyzed by EpiInfo software after ensuring completeness of data. Chi-square test and two-sample test of proportion were applied to analyze data.
Results
A total of 300 PwDM were included in the study (between May and December 2018). The first phase (no monetary incentive) took 5 months' time to achieve the target number of PwDM and the second phase (monetary incentive) took 3 months to achieve the target population. A total of 22 PwDM were screened in the baseline period, 75 in the health education (HE)-only phase and 65 in the ASHA worker incentive, respectively. The data regarding the screened DM patients (n = 162) were measured and reported.
In 2 months' baseline period, 22 PwDM [68% male, mean age 55.5 years, mean random blood sugar (RBS) 147.5 mg%] reported to the CHC for DR screening [Table 1].
Table 1.
Mean age and random blood sugar in study sample
| Age | Age | Random blood sugar |
|---|---|---|
| Mean±standard deviation (years) | Mean±standard deviation (mg%) | |
| No intervention, n=22 | ||
| Male (n=15) | 55.1±7.49 | |
| Female (n=7) | 56.4±11.81 | |
| Total | 55.5±8.82 | 147±10.4 |
| Health education, n=75 | ||
| Male (n=33) | 52.4±10.09 | |
| Female (n=42) | 55.0±10.21 | |
| Total | 53.9±10.18 | 153±28.4 |
| ASHA incentive, n=65 | ||
| Male (n=32) | 50.1±11.69 | |
| Female (n=33) | 54.3±11.60 | |
| Total | 52.3±11.75 | 195±38.1 |
ASHA=Accredited Social Health Activist
In the first phase, 75 PwDM (33 male, 42 female; average age 53.8 years; RBS 153 mg%) reported for DR screening over 5 months. In the second phase, 65 PwDM (32 male, 33 female; average age 52.3 years; RBS 195 mg%) reported for DR screening over the period of 3 months [Table 1].
A total of 300 (men 172, women 128) PwDM were registered at CHC. In the final analysis, 54% (n = 162) received DR screening [Fig. 1].
Figure 1.
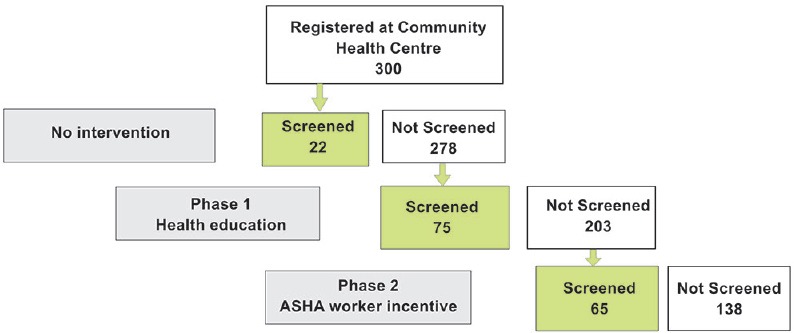
Phase-wise patient distribution along the time period of the study
The average number of PwDM screened per month in each of the three study periods was 11, 15, and 22 in the no intervention, HE, and ASHA worker incentive periods, respectively [Fig. 2].
Figure 2.
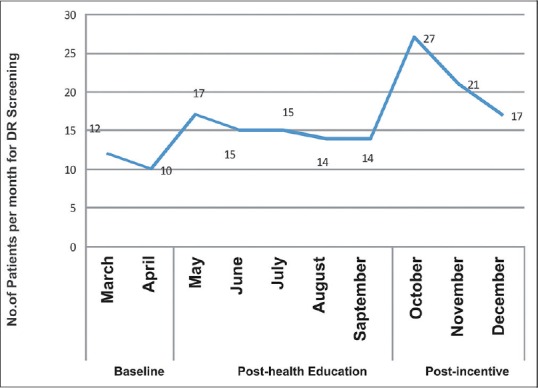
Number screened per month in different phases – pre-intervention, post health education by ASHA workers and post-incentive to ASHA workers
Descriptive statistics of the different characteristics measured are shown in Table 2. Of 162, 50.6% were females, 80.2% were literate, 56.2% were >50 years, 54.3% had uncontrolled RBS, and 59.9% had diabetes for 5 years or more. Statistically significant differences in the proportion of PwDM were observed in different levels of education, RBS, and duration of diabetes compared with three groups.
Table 2.
Descriptive statistics of different characteristics among screened diabetic patients
| Characteristics | Categories | No intervention (n=22) f (%) | Health education (n=75) f (%) | ASHA worker incentive (n=65) f (%) | P |
|---|---|---|---|---|---|
| Gender | Male | 15 (68.2%) | 33 (44%) | 32 (49.2%) | 0.137 |
| Female | 7 (31.8%) | 42 (56%) | 33 (50.8%) | ||
| Education | Low literacy (illiterate and primary education) | 8 (36.4%) | 5 (6.7%) | 19 (29.2%) | <0.001* |
| Literate (>primary education) | 14 (63.6%) | 70 (93.3%) | 46 (70.8%) | ||
| Age (years) | ≤50 | 7 (31.8%) | 35 (46.7%) | 29 (44.6%) | 0.461 |
| >50 | 15 (68.2%) | 40 (53.3%) | 36 (55.4%) | ||
| Random blood sugar (mg/dL)a | Controlled (<160 mg/dL) | 10 (45.5%) | 57 (76%) | 7 (10.8%) | <0.001* |
| Not controlled (≥160 mg/dL) | 12 (54.5%) | 18 (24%) | 58 (89.2%) | ||
| Duration of diabetes (years) | ≤5 | 22 (100%) | 43 (57.3%) | 32 (49.2%) | <0.001* |
| 6-10 | 0 (0%) | 20 (26.7%) | 13 (20%) | ||
| ≥11 | 0 (0%) | 12 (16%) | 20 (30.8%) |
*Statistically significant at 5% level of significance. aRandom blood sugar ≤160 is controlled and >160 was defined uncontrolled. ASHA=Accredited Social Health Activist
The overall percentage of screening was 54%, of which the highest DR screening was observed in the ASHA worker incentive phase. We compared the percentage of screening in the ASHA worker incentive phase and HE-only phase with respect to the baseline [Table 3]. The results indicated that the percentage of screening was significantly higher [relative risk (RR) = 4.37, 95% confidence interval (CI) 2.79, 6.84] in the ASHA worker incentive group and HE group (RR = 3.67, 95% CI 2.35, 5.75) compared with baseline. We also compared the two intervention groups and found no significant difference (RR = 1.19, 95% CI 0.89, 1.57), that is, providing incentives to ASHAs was of no extra advantage. When the characteristics of PwDM reporting for screening across the two intervention groups [Table 1] were compared, the likelihood of uptake of screening was higher among uncontrolled diabetes, poor literacy, and higher duration of diabetes in ASHA incentive phase (P < 0.001) compared with HE-only phase. There was no difference across gender and age in uptake of screening across the two intervention phases. The graded serial nature of intervention suggests that when ASHAs were given incentive, they were able to dedicate more time to motivate and facilitate PwDM who are least likely to get DR screening, to report for screening, that is, poor literacy, poor blood sugar control, and greater duration of diabetes.
Table 3.
Percentage of screening of DR in three different phases of the study
| Screened | Not screening | Total | RR (95% CI) | P | |
|---|---|---|---|---|---|
| No intervention | 22 (7.3%) | 278 (92.7%) | 300 | - | - |
| Health education | 75 (27.0%) | 203 (73%) | 278 | 3.67 (2.35, 5.75)b | <0.001# |
| ASHA worker incentive | 65 (32%) | 138 (68%) | 203 | 4.37 (2.79, 6.84)c | <0.001# |
DR=Diabetic retinopathy; RR=Relative risk; CI=Confidence interval; ASHA=Accredited Social Health Activist. #Statistically significant at 2% level of significance, P value adjusted for Bonferroni correction. bRR of screening comparing health education vs no intervention. cRR of screening comparing incentive to ASHA vs no intervention
Discussion
There are countries where community health workers are employed full-time by the governments with salaries and there are some countries where they are employed as part-time workers with result-oriented incentives. ASHAs fall in the latter category.[9] In India, the ASHA is the cadre which acts as an interface between the community and the health system, as agents of social change for health promotion and are the main pillars of achieving government policy goals at grassroot level.[9]
DR is the sixth major cause of blindness and visual impairment in India.[10] Therefore, DR screening assumes enormous importance by sheer magnitude of the problem in India. This service must be simple and less expensive to be effective in a resource-constrained economy like India. According to Diabetic Retinopathy Study (DRS) and Early Treatment Diabetic Retinopathy Study (ETDRS), 90% of severe visual loss can be reduced by just laser photocoagulation, when performed on time.[11,12]
There are many modalities available for DR screening. The sensitivity of retinal photography by fundus cameras is higher than direct ophthalmoscopy,[13,14] and even single-field retinal photographs read by retinologist or trained ophthalmologists are effective.[13]
To our knowledge, this was the first study conducted to determine the impact of incentives to ASHAs for DR care in India. Lack of awareness about DR-related visual impairment and blindness was found to be one of the main reasons in studies conducted in India.[15,16] The ASHAs could bridge this knowledge gap and might act as an agent for nudging more people to avail DR screening at the primary care level at the CHCs. Our study showed an increase in PwDM reporting for DR screening after ASHAs were incentivized, though this increase was only marginal, from an average 15 people a month to 22 people a month. Even though this increase is marginal in number, but qualitatively, incentive to ASHA improved uptake of DR screening among those who were least likely to be screened, for example, uncontrolled PwDM, low literacy group, and those with long duration of diabetes. Similar to other reports, this study also suggested that people with better diabetes control and higher education are more likely to get screened compared with those with poor medication compliance and lower literacy.[17,18,19,20,21,22,23] The number attending each month during the HE period was relatively stable, but after a peak, the number declined in the ASHA worker incentive period. It would be interesting to monitor the monthly DR screening trend for a longer duration post incentive phase.
As far as the limitations of the study are concerned, because the study was embedded in an ongoing program, all the characteristics of interest for all 300 PwDM were not available. The funds available for the study were small, limiting the duration of the study. These factors limited the analysis for likelihood for uptake of screening across the two phases. A study with larger sample size and duration of implementation is required to further understand the impact of ASHA incentives over HE by ASHA for increasing the likelihood of DR screening among PwDM in rural/tribal areas.
Conclusion
Monetary incentives are not sustainable; in the short run, it may be beneficial but in the long run it needs to be phased out and education and self-care by nonincentivized mechanism should drive PwDM for DR screening into the systems but ASHAs can be used effectively to refer known PwDM for DR screening especially when DR screening program is introduced in population with low awareness and poor accessibility to increase uptake of DR screening. This study showed that monetary incentive to the ASHAs has a potential to help a marginal or better yield of people for DR screening. Further studies with comparison design (more variables) and longer duration are required to further understand the sustainability and long-term impact implications.
Financial support and sponsorship
The Queen Elizabeth Diamond Jubilee Trust, London, UK.
Conflicts of interest
There are no conflicts of interest.
References
- 1.The new global estimates on visual impairment and blindness (WHO) [Internet] 2014. [Last accessed on 2019 Feb 02]. Available from: https://www.who.int/diabetes/global-report/en/
- 2.International Diabetes Federation [Internet] 2017. [Last accessed on 2019 Feb 02]. Available from: https://wwwidforg/our-network/regions-members/south-east-asia/members/94-indiahtml .
- 3.Gadkari S, Maskati Q, Nayak B. Prevalence of diabetic retinopathy in India: The all India ophthalmological society diabetic retinopathy eye screening study 2014. Indian J Ophthalmol. 2016;64:38–44. doi: 10.4103/0301-4738.178144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Murthy GVS, Das T. Diabetic care initiatives to prevent blindness from diabetic retinopathy in India. Indian J Ophthalmology. 2016;64:50–4. doi: 10.4103/0301-4738.178152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Raman R, Ganesan S, Pal SS, Kulothungan V, Sharma T. Prevalence and risk factors for diabetic retinopathy in rural India. Sankara Nethralaya diabetic retinopathy epidemiology and molecular genetic study III (SN-DREAMS III), report no 2. BMJ Open Diabetes Res Care. 2014;2:e000005. doi: 10.1136/bmjdrc-2013-000005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vashist P, Singh S, Gupta N, Saxena R. Role of early screening for diabetic retinopathy in patients with diabetes mellitus: An overview. Indian J Community Med. 2011;36:247–52. doi: 10.4103/0970-0218.91324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Guha I, Raut AV, Maliye CH, Mehendale AM, Garg BS. Qualitative assessment of Accredited social health activists (ASHA) regarding their roles and responsibilities and factors influencing their performance in selected villages of Wardha. Int J Adv Med Health Res. 2018;5:21–6. [Google Scholar]
- 8.Nandan D, Jain N, Shrivastava N. Assessment of the functioning of ASHAs under NRHM in Uttar Pradesh. 2007. [Last accessed on 2019 Sep 21]. Available from: http://www.nihfw.org/doc/RAHI-I%20Reports/Lucknow/LUKNOW.pdf .
- 9.Singh D, Negin J, Otim M, Orach CG, Cumming R. The effect of payment and incentives on motivation and focus of community health workers: Five case studies from low- and middle-income countries. Hum Resour Health. 2015;13:58. doi: 10.1186/s12960-015-0051-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Murthy GV, Gupta SK, Bachani D, Jose R, John N. Current estimates of blindness in India. Br J Ophthalmol. 2005;89:257–60. doi: 10.1136/bjo.2004.056937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Photocoagulation treatment of proliferative diabetic retinopathy: Clinical application of Diabetic retinopathy study (DRS) findings, DRS report number 8. Ophthalmology. 1981;88:583–600. [PubMed] [Google Scholar]
- 12.Early photocoagulation for diabetic retinopathy: ETDRS report number 9. Ophthalmology. 1991;98:766–85. [PubMed] [Google Scholar]
- 13.Bawankar P, Shanbhag NS, Smitha K, Dhawan B, Palsule A, Kumar D, et al. Sensitivity and specificity of automated analysis of single-field non-mydriatic fundus photographs by Bosch DR algorithm-comparison with mydriatic fundus photography (ETDRS) for screening in undiagnosed diabetic retinopathy. PLoS One. 2017;12:e0189854. doi: 10.1371/journal.pone.0189854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cunha LP, Figueiredo EA, Araújo HP, Costa-Cunha LV, Costa CF, Neto JM, et al. Non-mydriatic fundus retinography in screening for diabetic retinopathy: Agreement between family physicians, general ophthalmologists, and a retinal specialist. Front Endocrinol (Lausanne) 2018;9:251. doi: 10.3389/fendo.2018.00251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Namperumalsamy P, Kim R, Kaliaperumal K, Sekar A, Karthika A, Nirmalan PK. A pilot study on awareness of diabetic retinopathy among non-medical persons in South India. The challenge for eye care programmes in the region. Indian J Ophthalmol. 2004;52:247. [PubMed] [Google Scholar]
- 16.Rani PK, Raman R, Agarwal S, Paul PG, Uthra S, Margabandhu G, et al. Diabetic retinopathy screening model for rural population: Awareness and screening methodology. Rural Remote Health. 2005;5:350. [PubMed] [Google Scholar]
- 17.Leese GP, Boyle P, Feng Z, Emslie-Smith A, Ellis JD. Screening uptake in a well-established diabetic retinopathy screening program: The role of geographical access and deprivation. Diabetes Care. 2008;31:2131–5. doi: 10.2337/dc08-1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mumba M, Hall A, Lewallen S. Compliance with eye screening examinations among diabetic patients at a Tanzanian referral hospital. Ophthalmic Epidemiol. 2007;14:306–10. doi: 10.1080/09286580701272079. [DOI] [PubMed] [Google Scholar]
- 19.Rothman RL, Malone R, Bryant B, Wolfe C, Padgett P, DeWalt DA, et al. The spoken knowledge in low Literacy in diabetes scale: A diabetes knowledge scale for vulnerable patients. Diabetes Educ. 2005;31:215–24. doi: 10.1177/0145721705275002. [DOI] [PubMed] [Google Scholar]
- 20.Williams MV, Baker DW, Parker RM, Nurss JR. Relationship of functional health literacy to patients' knowledge of their chronic disease. A study of patients with hypertension and diabetes. Arch Intern Med. 1998;158:166–72. doi: 10.1001/archinte.158.2.166. [DOI] [PubMed] [Google Scholar]
- 21.Kashim RM, Newton P, Ojo O. Diabetic retinopathy screening: A systematic review on patients' non-attendance. Int J Environ Res Public Health. 2018;15:157. doi: 10.3390/ijerph15010157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Piyasena MMPN, Murthy GVS, Yip JLY, Gilbert C, Zuurmond M, Peto T, et al. Systematic review on barriers and enablers for access to diabetic retinopathy screening services in different income settings. PLoS One. 2019;14(4):e0198979. doi: 10.1371/journal.pone.0198979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Van-Eijk KN, Blom JW, Gussekloo J, Polak BC, Groeneveld Y. Diabetic retinopathy screening in patients with diabetes mellitus in primary care: Incentives and barriers to screening attendance. Diabetes Res Clin Pract. 2011;96:10–6. doi: 10.1016/j.diabres.2011.11.003. [DOI] [PubMed] [Google Scholar]