

Abstract
Background
Policies to improve healthy food retail have been recognized as a potential means of reducing diet-related health disparities. The revised 2014 Minneapolis Staple Foods Ordinance instituted minimum stocking standards for healthy, staple foods. The objective of this study was to examine retailer compliance with the policy, and whether compliance varied by neighborhood and store characteristics.
Methods
In this natural experiment, audits were conducted annually pre- and post-ordinance (2014–2017) in 155 small/nontraditional stores in Minneapolis, MN and a comparison city (St. Paul, MN). Compliance measures for 10 product categories included: (1) met requirements for ≥8 categories; (2) 10-point scale (one point for each requirement met); and (3) carried any item in each category. Store characteristics included store size and ownership status. Neighborhood characteristics included census-tract socioeconomic status and low-income/low-access status. Analyses were conducted in 2018.
Results
All compliance measures increased in both Minneapolis and St. Paul from pre- to post-policy; Minneapolis increases were greater only for carrying any item in each category (p < 0.01). In Minneapolis, corporate (vs. independent) stores were generally more compliant. No differences were found by neighborhood characteristics.
Conclusions
Overall trends suggest broad movement among Minneapolis stores towards providing a minimum level of staple foods. Increases were greater in corporate stores. Trends do not suggest neighborhood-level disparities in compliance.
Study registration
ClinicalTrials.gov NCT02774330, retrospectively registered May 17, 2016.
Keywords: Food access, Policy, Small food store, Stocking standards, Neighborhood disparities
Background
Disparities in the healthfulness of local food environments are evident across the U.S. [1, 2] High-minority and low-income neighborhoods are less likely to have supermarkets and more likely to have small food stores [1–3]. Small and non-traditional stores, such as corner stores, gas-marts, dollar stores, and pharmacies, have consistently demonstrated a limited selection of healthy food items [4–6], with managers of these stores citing challenges in procuring, stocking, and selling health food [7–10]. Unequal access to healthy food is associated with disparities in diet-related health outcomes, including obesity [11–15].
Policies to improve healthy food retail have been recognized as a potential means of reducing diet-related health disparities [16]. Some policies, such as the 2010 Healthy Food Financing Initiative, focus on geographic areas defined by the U.S. Department of Agriculture (USDA) as low-income areas with low access to healthy food [17, 18]. Other types of retailer policies are not focused on particular geographic areas, but aim to increase healthy food in retail settings that serve low-income groups at risk of poor diet, such as the 2009 revision of retailer standards for the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) [19–21]. The WIC policy change resulted in improved availability and variety of healthy foods in WIC-authorized stores [19–21]. A similar proposed policy strategy at the local level is creating minimum stocking requirements for healthy foods in all types of food stores as a condition of business licensing [22].
In 2008, the City Council of Minneapolis, MN passed the first Staple Foods Ordinance in the U.S., requiring licensed grocery stores to carry a basic minimum of healthy, staple foods. In 2014, the ordinance was revised to better align the policy with the Dietary Guidelines for Americans and stocking requirements for retailers participating in WIC [23, 24]. Revisions established minimum stocking requirements in 10 product categories, including fruits and vegetables, whole grain rich products, and low-fat dairy. The revised Staple Foods Ordinance had few exemptions; it applied not only to traditional large and medium-sized grocery stores, but also smaller non-traditional stores (such as gas-marts, dollar stores, and pharmacies) that sold food and participated in government food assistance programs like the Supplemental Nutrition Assistance Program (SNAP). The intention of the ordinance was to address disparities in food access within the city, recognizing the lack of universal access to supermarkets and the need to “ensure that everyone has access to healthy foods no matter where they shop” [25].
The revised Staple Foods Ordinance was first implemented in April 2015 with a one-year period without enforcement to address compliance concerns from retailers. During this year, the Minneapolis Health Department implemented the policy by assessing retailers’ understanding of policy requirements, conducting training on product procurement/marketing, offering resources like merchandising kits for infrastructure enhancements, and conducting meetings with corporate chain store representatives. Enforcement began in 2016 and was carried out through routine health inspections in which inspectors were given the authority to issue warning letters, citations, and fines for non-compliance.
An evaluation of the Minneapolis Staple Foods Ordinance in small and non-traditional stores revealed challenges with the implementation of the ordinance [26]. By 2017, only 9.6% of small and non-traditional food stores were fully compliant with the requirements, and changes in compliance during the study period (2014–2017) were not statistically different from analogous changes in inventory among stores in the comparison city (St. Paul, MN). However, while not statistically different from St. Paul, stores in Minneapolis showed significant improvements in compliance and healthy food availability over the study period. Looking at more detailed changes in store stocking using difference compliance indicators can contribute a better understanding of implementation successes and challenges.
The ability of stores to comply with the Staple Foods Ordinance could be affected by store and neighborhood factors that influence the ability to stock healthy food. Research has shown that small food stores in low-income/low-access neighborhoods have dense networks of unhealthy food suppliers [27], and major food distributors may avoid deliveries to smaller and independently-owned stores [7, 10]. The smallest stores tend to stock less healthy food than even slightly larger ones, perhaps due to difficulty in healthy food procurement among the smallest stores [4]. Stores with fewer supports for supplying healthy food could be less likely to comply with the policy, resulting in an unintended exacerbation of disparities in healthy food access.
Given the trends toward compliance noted in our previous study, the objectives of this study were to: 1) assess three distinct indicators of movement towards compliance, described in detail below, and 2) assess compliance in different stores and neighborhoods. We hypothesized that larger and corporately-owned stores (versus smaller and independently-owned stores) would demonstrate larger increases in compliance from baseline, as would stores located in higher-SES or outside low-income/low-access areas (versus those in lower-SES areas or in low-income/low-access areas).
Methods
Study Design
This natural experiment involved 4 annual time points of data collection (T1-T4) from 2014 to 2017 in stores in Minneapolis, MN (where the Staple Foods Ordinance was being implemented) and St. Paul, MN (the comparison community).
Study sample
The study sample and store recruitment process has been described previously [5, 6, 26, 28–33]. Stores exempted from the ordinance (including those that would not reasonably be expected to stock a minimal amount of foods and stores located the core downtown commercial district) were excluded from the evaluation in Minneapolis and St. Paul. The evaluation study targeted retailers that were not already expected to meet the new minimum stocking requirements; thus supermarkets, mass-merchandizers, and stores participating in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) were excluded from the sample. Finally, stores with invalid licensing addresses were excluded.
Of 255 eligible stores, 180 were randomly selected to participate. After visiting these stores to collect data at baseline (T1), 23 were identified as ineligible (e.g., due to new participation in WIC), and an additional 17 refused to participate. At the three subsequent data collection time points, study staff re-visited stores that refused to participate at T1 to attempt data collection. The final analytic sample had 155 unique stores (n = 140 at T1, 139 at T2, 137 at T3, and 127 at T4). Among the eligible sample, all stores were categorized as corner stores, gas-marts, dollar stores, pharmacies, or general retailers at T1. The study was approved by the Institutional Review Board at University of Minnesota.
Measures
Store environment was assessed using a tool modified from the Rudd Center for Food Policy and Obesity that was developed to evaluate changes in WIC policy revisions in small food stores in 2009 [20]. The tool, described previously [5, 6, 26, 28], is similar in format to Nutrition Environment Measure Survey in Stores (NEMS-S), but modified to align with the 10 Minneapolis Staple Food Ordinance requirements.
From the data generated using the store assessment tool, three indicators of ordinance compliance were generated:
80% compliance with ordinance requirements: the percent of stores that met at least 8/10 of the product category requirements of the ordinance (yes/no).
10-point scale: the total number of ordinance requirements met by stores (range 0–10), presented as an average across stores.
Carrying any food in each of the 10 categories: whether stores had any food in each of the categories required by the ordinance, even if the food was not in the appropriate package size, form, or quantity required by the ordinance (e.g., eggs sold in dozen containers were required by the ordinance, but eggs packed in half-dozen containers met the criteria for any eggs). The indicator is presented as the percent of stores that had any in all 10 categories (yes/no).
Store size (small/larger) was measured during the assessment as the number of cash registers in the store. Small stores had 1–2 cash registers and larger stores had at least 3 cash registers.
Store ownership status (corporate/independent) was determined during an interviewer-administered survey with store managers in which they were asked whether the store was independently-owned, corporately-owned, or part of a franchise. Franchise and corporately-owned stores were combined into a single category. In stores where ownership status was not available from the manager survey, two study team members (CEC and MNL) determined status based on publicly available information about the store (e.g., name, number of locations). Stores that were part of well-known chains were assigned corporate status; stores that had only one location were deemed independent.
Neighborhood data were obtained from 5-year American Community Survey estimates (ACS, 2009–2015) [34] and attributed to stores based on census tract location. Store census tracts were classified into lower-socioeconomic status (SES) or higher-SES. Lower-SES census tracts had > 50% of residents at or below 185% of the federal poverty income guidelines [35].
Using the USDA Food Access Research Atlas [17], stores were classified as low-income/low-access if the census tract they were located in was both low-income and low-access. Low-income tracts met any of the following criteria: [1] median family income ≤80% of the state-wide of the metropolitan area’s median family income [2]; poverty rate > 20%. Low-access tracts had ≥100 households located > 1/2 mile from the nearest supermarket and had no access to a vehicle.
Statistical analyses
Descriptive statistics were computed for store and neighborhood characteristics at baseline for Minneapolis and St. Paul separately, expressed as number and percentage of stores/neighborhoods. We also computed chi-square tests to compare the store and neighborhood characteristics across the two cities. Using data from T1-T4 from both cities, a mixed regression model for each of the three compliance outcome measures was conducted to examine the overall movement towards compliance in Minneapolis compared with the control condition in St. Paul. For each model, we tested an overall time-by-city interaction, adjusted for neighborhood race/ethnicity (the only significant covariate in bivariate city comparisons).
Subsequent analyses were limited to stores in Minneapolis only, to compare magnitude of changes in compliance within different stores and neighborhoods of the policy area. A mixed regression model was computed for each compliance outcome with store (size, ownership status) and neighborhood characteristics (SES, low-income/low-access status) as independent variables. Models tested the interaction between time and store/neighborhood characteristic (3 degrees of freedom) for each outcome. For interactions that reached statistical significance, we tested changes between baseline and each time point (T1 to T2, T1 to T3, and T1 to T4). All models were adjusted for repeated measures over time. All analyses were conducted in SAS (SAS/STAT Version 9.4).
Results
Table 1 presents store characteristics in Minneapolis and St. Paul. Most stores were corner/convenience stores or food-gas marts (75% in Minneapolis vs. 73% in St. Paul). The remainder were dollar stores, pharmacies, and one general retailer in Minneapolis. The majority of stores in both cities were smaller, located in higher SES neighborhoods, and located outside of low-income/low-access neighborhoods. There were more independent stores in Minneapolis (55%) vs. St. Paul (41%). Correlations between store and neighborhood characteristics were small, except store size and ownership status was moderately correlated (r = 0.6).
Table 1.
Store and neighborhood characteristics at baseline, Minneapolis and St. Paul, MN, 2014
| Store and neighborhood characteristics | Minneapolis (n = 77) |
St. Paul (n = 63) |
|
|---|---|---|---|
| n (%) | n (%) | p-value a | |
| Store type | 0.49 | ||
| Corner stores, convenience stores, small groceries | 34 (44) | 20 (32) | |
| Food-gas marts | 24 (31) | 26 (41) | |
| Dollar stores | 7 (9) | 6 (10) | |
| Pharmacies | 11 (14) | 11 (17) | |
| General retailers | 1 (1) | 0 (0) | |
| Store size | 0.39 | ||
| Smaller size (1–2 registers) | 53 (69) | 39 (62) | |
| Larger size (3+ registers) | 24 (31) | 24 (38) | |
| Store ownership status | 0.12 | ||
| Corporate | 35 (45) | 37 (59) | |
| Independent | 42 (55) | 26 (41) | |
| Neighborhood SES | 0.28 | ||
| Lower SES (< 185% of poverty) | 26 (34) | 16 (25) | |
| Higher SES (> = 185% of poverty) | 51 (66) | 47 (75) | |
| Neighborhood low-income/low-access status | 0.11 | ||
| Store located in low-income/low-access area | 23 (30) | 27 (43) | |
| Store not located in low-income/low-access area | 54 (70) | 36 (57) |
a Chi-square tests
Table 2 presents the results of models for the three compliance indicators by city, as well as change in these measures over the four time points. All indicators were higher in Minneapolis than St. Paul at every time point, and all indicators demonstrated a net increase between T1 to T4 in both cities. Changes were only statistically significant for the percent of stores that carried any food in each of the 10 categories (p = 0.01) in Minneapolis (27.6 to 75.1%), compared to St. Paul (12.3 to 19.1%).
Table 2.
Compliance in Minneapolis vs. St. Paul
| Compliance Outcome | City | Pre-policy (2014) Mean (SE) | Implementation only (2015) Mean (SE) | Early initiation of enforcement (2016) Mean (SE) | Continued monitoring (2017) Mean (SE) | Overall Effect (time-by-city) P (df = 3) |
|---|---|---|---|---|---|---|
| Met 80% of ordinance standards (% of stores) | Minneapolis (Policy) | 24.4 (4.9) | 40.7 (5.6) | 31.0 (5.2) | 50.5 (5.9) | 0.83 |
| St. Paul (Control) | 3.2 (2.2) | 11.6 (4.1) | 6.7 (3.2) | 14.4 (4.7) | ||
| 10 point scale (0–10; 1 point for each standard met) | Minneapolis (Policy) | 5.7 (0.3) | 6.4 (0.3) | 6.6 (0.2) | 7.1 (0.2) | 0.30 |
| St. Paul (Control) | 4.4 (0.2) | 4.7 (0.3) | 4.9 (0.3) | 5.3 (0.3) | ||
| Have any food in each of 10 categories (% of stores) | Minneapolis (Policy) | 27.6 (5.2) | 39.0 (5.5) | 51.1 (5.8) | 75.1 (5.1) | 0.01 |
| St. Paul (Control) | 12.3 (4.1) | 12.7 (4.2) | 16.3 (4.7) | 19.1 (5.2) | ||
| p-net | p = 0.27 | p = 0.13 | p = 0.0009 |
Note: Regression models are adjusted for repeated measures over time and for neighborhood race/ethnicity (the only covariate that was significant in bivariate comparisons between Minneapolis and St. Paul); p-net values refer to changes in time-by-city effect from pre-policy to implementation only, from pre-policy to early initiation of enforcement, from pre-policy to continued monitoring respectively bolded values: p ≤ .05
Table 3 presents the results of models and significance testing for the three compliance indicators in Minneapolis alone by store size and ownership status; Figs. 1 and 2 visually present trends in compliance by these store factors over time. Compared with smaller-sized stores, larger stores had lower compliance on all indicators at T1, but by T4 surpassed smaller-sized stores on every indicator. However this increase was only statistically significant for the 10 point scale (p = 0.03), for which smaller stores initially had a greater gain from T1 to T2 than larger stores, but this gain was subsequently surpassed by larger stores at T4. Corporate stores (versus independent stores) had lower compliance for all indicators at baseline, but had significantly surpassed independent stores at T4 for all indicators.
Table 3.
Compliance by store characteristics (Minneapolis only)
| Compliance Outcome | Store characteristic | Pre-policy (2014) Mean (SE) | Implementation only (2015) Mean (SE) | Early initiation of enforcement (2016) Mean (SE) | Continued monitoring (2017) Mean (SE) | Overall Effect (time-by-characteristic) p (df = 3) |
|---|---|---|---|---|---|---|
| Met at least 8 of 10 ordinance standards (% of stores) | Larger size (3+ registers) | 8.3 (5.6) | 21.4 (7.8) | 17.9 (7.2) | 53.6 (9.4) | 0.08 |
| Smaller size (1–2 registers) | 32.1 (6.4) | 52.0 (7.1) | 38.8 (7.0) | 48.8 (7.6) | ||
| Corporate | 5.7 (3.9) | 18.0 (6.1) | 20.5 (6.5) | 57.9 (8.0) | <.0001 | |
| Independent | 40.5 (7.6) | 64.1 (7.7) | 42.1 (8.0) | 42.4 (8.6) | ||
| p-net | 0.66 | 0.09 | 0.0002 | |||
| 10 point scale (0–10; 1 point for each category where standard met) | Larger size (3+ registers) | 5.4 (0.3) | 5.5 (0.4) | 6.4 (0.3) | 7.3 (0.3) | 0.03 |
| Smaller size (1–2 registers) | 5.7 (0.4) | 7.0 (0.4) | 6.7 (0.3) | 7.1 (0.3) | ||
| p-net | 0.03 | 0.94 | 0.43 | |||
| Corporate | 5.0 (0.3) | 5.5 (0.3) | 6.4 (0.3) | 7.3 (0.3) | 0.0008 | |
| Independent | 6.1 (0.5) | 7.4 (0.4) | 6.8 (0.4) | 7.0 (0.4) | ||
| p-net | 0.08 | 0.16 | 0.01 | |||
| Have any food in each of 10 categories (% of stores) | Larger size (3+ registers) | 8.3 (5.6) | 17.9 (7.2) | 35.7 (9.1) | 78.6 (7.8) | 0.08 |
| Smaller size (1–2 registers) | 35.9 (6.6) | 50.0 (7.1) | 59.2 (7.0) | 72.1 (6.8) | ||
| Corporate | 8.6 (4.7) | 10.3 (4.9) | 38.5 (7.8) | 76.3 (6.9) | 0.002 | |
| Independent | 42.9 (7.6) | 66.7 (7.5) | 63.2 (7.8) | 72.7 (7.8) | ||
| p-net | 0.25 | 0.12 | 0.006 |
Note: All models adjusted for repeated measures over time; p-net values refer to changes in time-by-characteristic effect from pre-policy to implementation only, from pre-policy to early initiation of enforcement, from pre-policy to continued monitoring respectively; bolded values: p ≤ .05
Fig. 1.

Compliance with the Minneapolis Staple Foods Ordinance in Larger and Smaller Stores in Minneapolis, MN A: Percent of Stores Meeting 80% of Staple Foods Ordinance Standards; B: 10-Point Scale of Meeting Ordinance Requirements; C: Percent of Stores Stocking Any Food in All 10 Categories; T1 = 2014 (Pre-policy), T2 = 2015 (Implementation only), T3 = 2016 (Early initiation of enforcement), T4 = 2017 (Continued monitoring).
Fig. 2.

Compliance with the Minneapolis Staple Foods Ordinance in Corporate and Independent Stores in Minneapolis, MN A: Percent of Stores Meeting 80% of Staple Foods Ordinance Standards; B: 10-Point Scale of Meeting Ordinance Requirements; C: Percent of Stores Stocking Any Food in All 10 Categories; T1 = 2014 (Pre-policy), T2 = 2015 (Implementation only), T3 = 2016 (Early initiation of enforcement), T4 = 2017 (Continued monitoring)
Table 4 presents the results of models and significance testing for compliance indicators in Minneapolis by neighborhood factors; Figs. 3 and 4 visually present trends in compliance by neighborhood over time. Changes in stores in higher-SES areas were generally similar to changes in lower-SES areas, with no statistically significant differences. In low-income/low-access areas compared with areas that were not low-income/low-access, the magnitude of changes in compliance between T1 and T4 was similar for all outcomes. Outcomes for stores within vs. outside low-income/low-access were similar at T1, and also similar at T4, though overall trends were different for the 10-point scale (p = 0.002) and carrying any items in each of the 10 categories (p = 0.05). Adjusting for store factors (size and ownership status) did not result in substantive changes in neighborhood trends.
Table 4.
Compliance by neighborhood characteristics (Minneapolis only)
| Compliance Outcome | Neighborhood Characteristic | Pre-policy (2014) Mean (SE) | Implementation only (2015) Mean (SE) | Early initiation of enforcement (2016) Mean (SE) | Continued monitoring (2017) Mean (SE) | Overall Effect (time-by-characteristic) p (df = 3) |
|---|---|---|---|---|---|---|
| Met at least 8 of 10 ordinance standards (% of stores) | Lower SES | 26.9 (8.7) | 48.2 (9.6) | 42.3 (9.7) | 44.0 (9.9) | 0.23 |
| Higher SES | 23.5 (5.9) | 37.3 (6.8) | 25.5 (6.1) | 54.4 (7.3) | ||
| Low-income/low-access | 26.1 (9.2) | 59.1 (10.5) | 35.0 (10.7) | 47.1 (12.1) | 0.15 | |
| Not low-income/low-access | 24.1 (5.8) | 33.9 (6.3) | 29.8 (6.1) | 51.9 (6.8) | ||
| 10 point scale (0–10; 1 point for each category where standard met) | Lower SES | 5.9 (0.5) | 6.9 (0.5) | 6.8 (0.4) | 6.7 (0.4) | 0.12 |
| Higher SES | 5.5 (0.4) | 6.3 (0.3) | 6.5 (0.3) | 7.4 (0.3) | ||
| Low-income/low-access | 5.4 (0.6) | 7.4 (0.5) | 6.6 (0.6) | 7.2 (0.5) | 0.002 | |
| Not low-income/low-access | 5.7 (0.3) | 6.1 (0.3) | 6.6 (0.3) | 7.2 (0.3) | ||
| p-net | 0.001 | 0.65 | 0.70 | |||
| Any food in each of 10 categories (% of stores) | Lower SES | 30.8 (9.1) | 44.4 (9.6) | 57.7 (9.7) | 72.0 (9.0) | 0.82 |
| Higher SES | 25.5 (6.1) | 35.3 (6.7) | 47.1 (7.0) | 76.1 (6.3) | ||
| Low-income/low-access | 30.4 (9.6) | 45.5 (10.6) | 40.0 (11.0) | 82.4 (9.2) | 0.05 | |
| Not low-income/low-access | 25.9 (6.0) | 35.7 (6.4) | 54.4 (6.6) | 72.2 (6.1) | ||
| p-net | 0.73 | 0.09 | 0.65 |
Bolded entries: p < 0.05; Low SES: > 50% of residents at 185% of poverty; High SES: ≤50% of residents at 185% of poverty; All models adjusted for repeated measures over time; p-net values refer to changes in time-by-characteristic effect from pre-policy to implementation only, from pre-policy to early initiation of enforcement, from pre-policy to continued monitoring respectively
Fig. 3.
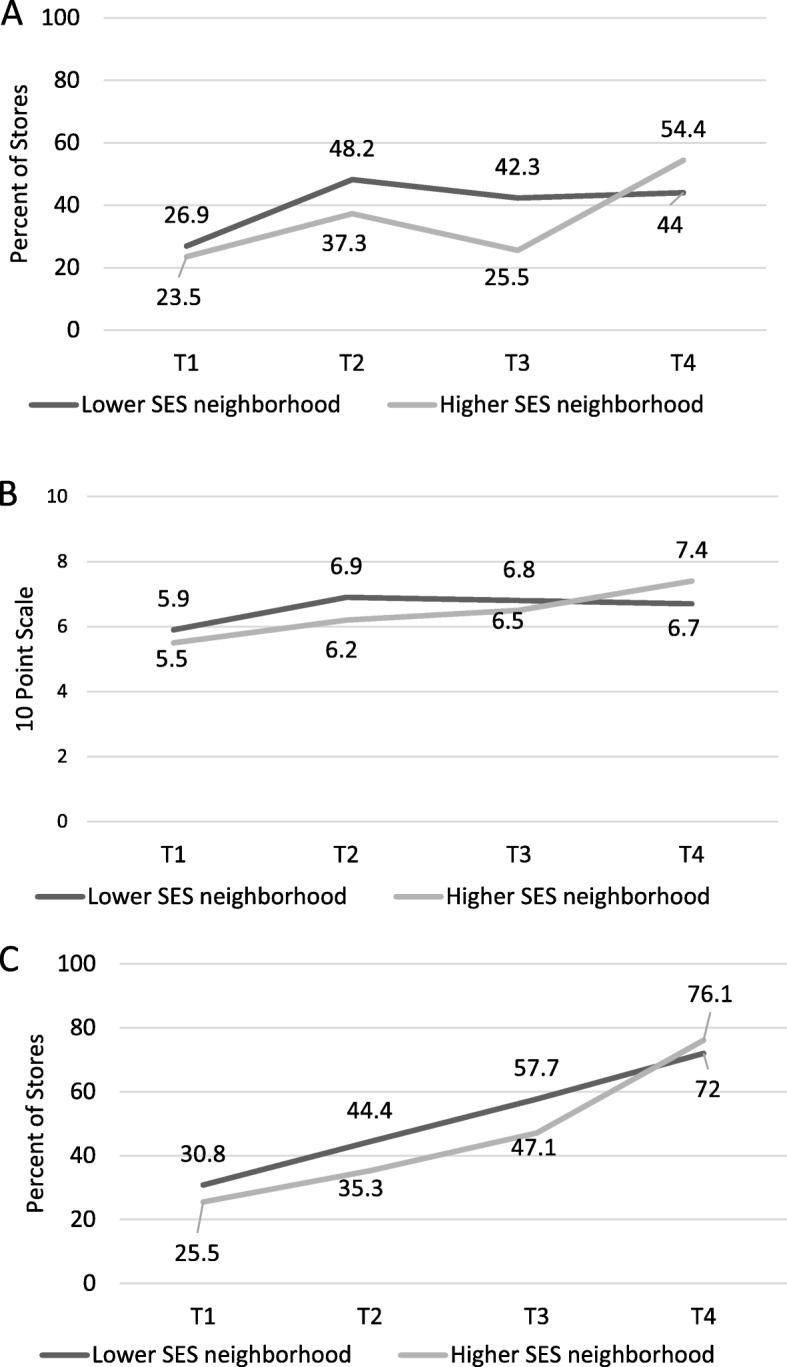
Compliance with the Minneapolis Staple Foods Ordinance in Lower-SES and Higher-SES Stores in Minneapolis, MN A: Percent of Stores Meeting 80% of Staple Foods Ordinance Standards; B: 10-Point Scale of Meeting Ordinance Requirements; C: Percent of Stores Stocking Any Food in All 10 Categories; T1 = 2014 (Pre-policy), T2 = 2015 (Implementation only), T3 = 2016 (Early initiation of enforcement), T4 = 2017 (Continued monitoring)
Fig. 4.

Compliance with the Minneapolis Staple Foods Ordinance in Lower-Income/Access and Higher-Income/Access Stores in Minneapolis, MN A: Percent of Stores Meeting 80% of Staple Foods Ordinance Standards; B: 10-Point Scale of Meeting Ordinance Requirements; C: Percent of Stores Stocking Any Food in All 10 Categories; T1 = 2014 (Pre-policy), T2 = 2015 (Implementation only), T3 = 2016 (Early initiation of enforcement), T4 = 2017 (Continued monitoring)
Discussion
Previous work indicated that compliance with the Minneapolis Staple Foods Ordinance was low, with only 10% of small and non-traditional Minneapolis food retailers meeting full compliance; moreover, Minneapolis was no different from St. Paul in terms of change in full retailer compliance across the study period [26]. The current study adds to that work, with the objective of assessing three indicators of movement towards compliance, and assessing compliance in different stores and neighborhoods. The current study shows that stores in Minneapolis demonstrated robust increases in compliance measures in the 3-year period following ordinance implementation. Minneapolis stores had a greater magnitude increase in carrying any items in all 10 product categories of the ordinance compared with St. Paul stores. In addition, corporate stores may be better equipped to make changes to increase compliance than independent stores, and that there were not meaningful differences in change in compliance between neighborhood types. These findings do not diminish the implementation concerns cited in the previous study, but they do demonstrate movement towards the goal of the ordinance to provide a minimum level of healthy food in stores across the city. However, it is possible that changes observed are attributable to factors other than the ordinance, such as secular trends in the marketplace, changes in food preferences of shoppers, and/or changing demographics of shoppers.
Results from different compliance measures offer some insight into the successes and challenges of the ordinance. Gains in carrying any food in each of the 10 required categories indicate stores’ ability to obtain different types of healthy, staple foods. This includes obtaining a supplier or the capacity to self-supply certain types of food, as well as having the basic infrastructure for stocking perishable products. Indeed, capacity to supply and infrastructure to stock a variety of healthy foods has consistently been cited in previous literature as central to the success of small stores in carrying healthy products [7, 8]. Increases in carrying food in each of the 10 categories suggest a promising step in compliance; the statistically significant increase in Minneapolis compared with St. Paul stores suggest that Minneapolis stores may have expanded their network of suppliers and/or capacity to self-supply healthy and staple foods. Stores that carry any food in each of the 10 categories, but do not meet full ordinance requirements, may stock less healthful versions of required foods (e.g., whole/reduced-fat milk instead of low-fat/skim milk) or narrowly miss ordinance requirements while still carrying healthful products (e.g., eggs in ½-dozen containers instead of 1-dozen containers). For such stores, it remains unclear whether the lack of full compliance is due to insufficient retailer understanding about the ordinance, inadequate space to stock required amounts, manager beliefs about the demand for certain products, or a combination of these and other factors.
Corporate stores demonstrated greater gains in compliance during the study period compared with independent stores, respectively. Corporate stores scored considerably lower on all measures at baseline, but had surpassed independent stores on all measures by T4. Corporate stores may be better positioned to bring themselves into alignment with the policy due to economies of scale in purchasing and delivery. Additionally, corporate stores’ centralized decision-making could have facilitated compliance across many stores at once. Given their prominence in the food retail landscape, corporate stores may have had more pressure to comply from those in charge of ordinance implementation. Larger stores may share some characteristics with corporate stores that make it easier to supply healthy food (e.g., economies of scale); indeed, larger stores demonstrated a greater magnitude of change than smaller stores, although these changes were not always statistically significant.
Compliance trends were similar for stores in lower-SES and higher-SES neighborhoods. Progress was more variable over time for stores within versus outside low-income/low-access areas, and increases were not observed at every study time point. However, by T4, total increases in compliance were similar for stores in low-income/low-access areas compared to those outside low-income/low-access areas. Overall, findings do not raise concerns about differences in compliance across these neighborhood characteristics.
In 2018, after our data were collected, concerns were raised about insufficient flexibility of stocking options in the Staple Foods Ordinance, and in December 2018 Minneapolis City Council approved modifications to the ordinance requirements that improved flexibility in providing healthy and culturally-appropriate food that meets customer demand [36]. As of early 2019, the Minneapolis Health Department was continuing to offer education, training, and technical assistance to help assist with compliance, albeit with increasingly limited by budgetary cuts for health inspections. Low compliance with the ordinance remains a concern, despite overall trends suggesting broad movement of Minneapolis stores towards providing a minimum level of healthy food. Meanwhile, there is national interest in minimum stocking requirements policies for improving healthy food in small food retailers. In 2016, the Robert Wood Johnson Foundation published a set of recommendations for healthy stocking criteria for small retail food stores meant to inform similar initiatives [37], and another city recently passed a similar Staple Foods policy [38]. Other cities are actively considering the feasibility of similar policies.
This study has a number of strengths, including hypotheses grounded in a health disparities framework, a well-matched comparison condition, and four time points of objective measurement of small and non-traditional food stores that spanned the period of pre- and post-policy implementation. One limitation of the study is that changes in two of our three indicators did not differ significantly by city, so compliance changes in Minneapolis may be attributable to factors other than the ordinance. Another limitation is that our analysis did not test compliance mediators; while we can glean from previous studies what challenges may have been likely for different kinds of stores [7–9], these were not tested in the current study. Another limitation is the sample size for the Minneapolis-only analyses, which may not have been large enough to detect significant subgroup differences; our conclusions are supported by both visual trends and p-values. Finally, the study observed only one geographic area and enforcement of the ordinance was limited; thus, there may be other circumstances under which to test the feasibility of implementing minimum stocking requirement policies [8].
Conclusions
The experience of Minneapolis in implementing the first Staple Foods Ordinance suggests that the success of implementing minimum stocking requirements in small/non-tradition retailers may depend on store factors related to store capacity, such as ownership status. However, location differences in compliance were not evident, suggesting that the policy did not exacerbate urban food access disparities. Given national interest in minimum stocking requirements for small food stores, additional work is needed to understand implementation challenges in different retail settings.
Acknowledgements
We would like to acknowledge Kristen Klingler and Nora Gordon at the Minneapolis Health Department for their partnership, support and expertise working with local small food stores. We would also like to acknowledge the large data acquisition and data management team, most especially Stacey Moe and Pamela Carr-Manthe.
Abbreviations
- ACS
American Community Survey estimates
- MN
Minnesota
- NEMS-S
Nutrition Environment Measure Survey in Stores
- SES
Socioeconomic status
- SNAP
Supplemental Nutrition Assistance Program
- USDA
U.S. Department of Agriculture
- WIC
Special Supplemental Nutrition Program for Women, Infants and Children
Authors’ contributions
CEC was responsible for formulating research questions, leading manuscript writing and supported carrying out the study from which these data originated; MRW assisted in formulating the research questions, contributed to data interpretation, and contributed to the writing/revision of the manuscript. KL conducted the data analysis and contributed to writing/revision of the manuscript. LH assisted in formulating the research questions, assisted in interpreting result, and contributed to writing and revising the manuscript. DJE guided and provided feedback on the analysis, assisted in interpreting results, gave feedback on analyses and writing/revision of the manuscript. MNL was responsible for leading the overall study from which these data originated, including conception/design, funding acquisition and implementation; she also gave feedback on analyses and contributed to writing/revision of the manuscript. All authors read and approved the final manuscript.
Funding
This research was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (R01DK104348); it was also supported by the Centers for Disease Control and Prevention as a Special Interest Project of the UMN Prevention Research Center (U48DP005022). NIH grant UL1TR000114 from the National Center for Advancing Translational Sciences (NCATS) supported data management. A training grant from the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (T32 DK08325010) supported author MRW. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Funding agencies had no role in the design, analysis or writing of this article.
Availability of data and materials
The datasets generated during the current study are not publicly available because the investigator team is still actively analyzing and publishing study results, but data are available from the corresponding author on reasonable request. We will reassess making.the data publicly available when current analyses are completed.
Ethics approval and consent to participate
This study was approved by the Intuitional Review Board at the University of Minnesota (study ID 1410S54204) on December 5, 2013. Human subjects involved in this research were consented verbally and provided a study information sheet. Verbal consent only was required because of the study’s low risk and the lack of private information collected; the verbal consent process was approved by the IRB.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Caitlin E. Caspi, Email: cecaspi@umn.edu
Megan R. Winkler, Email: mwinkler@umn.edu
Kathleen M. Lenk, Email: lenk@umn.edu
Lisa J. Harnack, Email: harna001@umn.edu
Darin J. Erickson, Email: erick232@umn.edu
Melissa N. Laska, Email: nels5024@umn.edu
References
- 1.Powell L, Slater S, Mirtcheva D, Bao Y, Chaloupka F. Food store availability and neighborhood characteristics in the United States. Prev Med. 2007;44(3):189–195. doi: 10.1016/j.ypmed.2006.08.008. [DOI] [PubMed] [Google Scholar]
- 2.Larson N, Story M, Nelson M. Neighborhood environments disparities in access to healthy foods in the US. Am J Prev Med. 2009;36(1):74–81. doi: 10.1016/j.amepre.2008.09.025. [DOI] [PubMed] [Google Scholar]
- 3.Bodor JN, Ulmer VM, Dunaway LF, Farley TA, Rose D. The rationale behind small food store interventions in low-income urban neighborhoods: insights from New Orleans. J Nutr. 2010;140(6):1185–1188. doi: 10.3945/jn.109.113266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Laska MN, Borradaile KE, Tester J, Foster GD, Gittelsohn J. Healthy food availability in small urban food stores: a comparison of four US cities. Public Health Nutr. 2010;13(7):1031–1035. doi: 10.1017/S1368980009992771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Laska MN, Caspi CE, Pelletier JE, Friebur R, Harnack LJ. Lack of healthy food in small-size to mid-size retailers participating in the supplemental nutrition assistance program, Minneapolis-St. Paul, Minnesota, 2014. Prev Chronic Dis. 2015;12:E135. doi: 10.5888/pcd12.150171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Caspi CE, Pelletier JE, Harnack L, Erickson DJ, Laska MN. Differences in healthy food supply and stocking practices between small grocery stores, gas-marts, pharmacies and dollar stores. Public Health Nutr. 2015;28:1–8. doi: 10.1017/S1368980015002724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gittelsohn J, Laska MN, Karpyn A, Klingler K, Ayala GX. Lessons learned from small store programs to increase healthy food access. Am J Health Behav. 2014;38(2):307–315. doi: 10.5993/AJHB.38.2.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Karpyn A, DeWeese RS, Pelletier JE, Laska MN, Ohri-Vachaspati P, Deahl-Greenlaw A, et al. Examining the feasibility of healthy minimum stocking standards for small food stores. J Acad Nutr Diet. 2018;118(9):1655–1663. doi: 10.1016/j.jand.2017.12.006. [DOI] [PubMed] [Google Scholar]
- 9.Ayala GX, D’Angelo H, Gittelsohn J, Horton L, Ribisl K, Sindberg LS, et al. Who is behind the stocking of energy-dense foods and beverages in small stores? The importance of food and beverage distributors. Public Health Nutr. 2017;20(18):3333–3342. doi: 10.1017/S1368980016003621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.O’Malley K, Gustat J, Rice J, Johnson CC. Feasibility of increasing access to healthy foods in neighborhood corner stores. J Community Health. 2013;38(4):741–749. doi: 10.1007/s10900-013-9673-1. [DOI] [PubMed] [Google Scholar]
- 11.Cannuscio CC, Weiss EE, Asch DA. The contribution of urban Foodways to health disparities. J Urban Health-Bull N Y Acad Med. 2010;87(3):381–393. doi: 10.1007/s11524-010-9441-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Morland K, Evenson K. Obesity prevalence and the local food environment. Health Place. 2009;15(2):491–495. doi: 10.1016/j.healthplace.2008.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vargas CM, Stines EM, Granado HS. Health-equity issues related to childhood obesity: a scoping review. J Public Health Dent. 2017;77(Suppl 1):S32–S42. doi: 10.1111/jphd.12233. [DOI] [PubMed] [Google Scholar]
- 14.Lovasi GS, Hutson MA, Guerra M, Neckerman KM. Built environments and obesity in disadvantaged populations RID C-2781-2009. Epidemiol Rev. 2009;31(1):7–20. doi: 10.1093/epirev/mxp005. [DOI] [PubMed] [Google Scholar]
- 15.Sallis JF, Glanz K. Physical activity and food environments: solutions to the obesity epidemic. Milbank Q. 2009;87(1):123–154. doi: 10.1111/j.1468-0009.2009.00550.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Story Mary, Kaphingst Karen M., Robinson-O'Brien Ramona, Glanz Karen. Creating Healthy Food and Eating Environments: Policy and Environmental Approaches. Annual Review of Public Health. 2008;29(1):253–272. doi: 10.1146/annurev.publhealth.29.020907.090926. [DOI] [PubMed] [Google Scholar]
- 17.United States Department of Agriculture ERS Food Food Access Research Atlas Documentation [Internet]. Available from: https://www.ers.usda.gov/data-products/food-access-research-atlas/documentation/ [cited 2017 Feb 22].
- 18.U.S. Department of Health & Human Services . Office of Community Service: Healthy Food Financing Initiative [Internet]. Office of Community Services | ACF. 2017. [Google Scholar]
- 19.Zenk SN, Odoms-Young A, Powell LM, Campbell RT, Block D, Chavez N, et al. Fruit and vegetable availability and selection: federal food package revisions, 2009. Am J Prev Med. 2012;43(4):423–428. doi: 10.1016/j.amepre.2012.06.017. [DOI] [PubMed] [Google Scholar]
- 20.Andreyeva T, Luedicke J, Middleton AE, Long MW, Schwartz MB. Positive influence of the revised special supplemental nutrition program for women, infants, and children food packages on access to healthy foods. J Acad Nutr Diet. 2012;112(6):850–858. doi: 10.1016/j.jand.2012.02.019. [DOI] [PubMed] [Google Scholar]
- 21.Havens EK, Martin KS, Yan J, Dauser-Forrest D, Ferris AM. Federal Nutrition Program Changes and healthy food availability. Am J Prev Med. 2012;43(4):419–422. doi: 10.1016/j.amepre.2012.06.009. [DOI] [PubMed] [Google Scholar]
- 22.ChangeLab Solutions . Licensing for Lettuce: Model Ordinance and Guide for Licensing Healthy Food Retailers. [Internet] 2013. [Google Scholar]
- 23.Dietary Guidelines - health.gov [Internet]. Available from: http://health.gov/dietaryguidelines/ [cited 2016 Jan 13].
- 24.Minesota Department of Health. Minimum Stock Requirements: Resources for WIC Authorized Grocery Stores [Internet]. n.d. Available from: https://www.health.state.mn.us/people/wic/vendor/rqrmnts/minstock.html [cited 2019 Mar 20].
- 25.Minneapolis Health Department: Minneapolis Staple Foods Ordinance Frequently Asked Questions [Internet]. n.d. Available from: http://www.minneapolismn.gov/www/groups/public/@health/documents/webcontent/wcmsp-216179.pdf#page=1&zoom=auto,-73,792 [cited 2019 Mar 20].
- 26.Laska MN, Caspi CE, Lenk K, Moe S, Pelletier JE, Harnack LJ, et al. Evaluation of the first U.S. staple foods ordinance: impact on nutritional quality of small and non-traditional food store offerings, customer purchases and home food environments. Int J Behav Nutr Phys Act. 2019;16(1):83. [DOI] [PMC free article] [PubMed]
- 27.Mui Y, Lee BY, Adam A, Kharmats AY, Budd N, Nau C, et al. Healthy versus unhealthy suppliers in Food Desert neighborhoods: a network analysis of corner stores’ food supplier networks. Int J Environ Res Public Health. 2015;12(12):15058–15074. doi: 10.3390/ijerph121214965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Caspi CE, Lenk K, Pelletier JE, Barnes TL, Harnack L, Erickson DJ, et al. Association between store food environment and customer purchases in small grocery stores, gas-marts, pharmacies and dollar stores. Int J Behav Nutr Phys Act. 2017 05;14(1):76. [DOI] [PMC free article] [PubMed]
- 29.Caspi CE, Lenk K, Pelletier JE, Barnes TL, Harnack L, Erickson DJ, et al. Food and beverage purchases in corner stores, gas-marts, pharmacies and dollar stores. Public Health Nutr. 2016;19:1–11. doi: 10.1017/S1368980015002724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Caspi CE, Pelletier JE, Harnack LJ, Erickson DJ, Lenk K, Laska MN. Pricing of staple foods at supermarkets versus small food stores. Int J Environ Res Public Health. 2017;15:14(8). doi: 10.3390/ijerph14080915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Winkler MR, Lenk KM, Caspi CE, Erickson DJ, Harnack L, Laska MN. Variation in the food environment of small and non-traditional stores across racial segregation and corporate status. Public Health Nutr. 2019;22(9):1624–1634. doi: 10.1017/S1368980019000132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lenk KM, Caspi CE, Harnack L, Laska MN. Customer characteristics and shopping patterns associated with healthy and unhealthy purchases at small and non-traditional food stores. J Community Health. 2018;43(1):70–78. doi: 10.1007/s10900-017-0389-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Barnes TL, Pelletier JE, Erickson DJ, Caspi CE, Harnack LJ, Laska MN. Healthfulness of Foods Advertised in Small and Nontraditional Urban Stores in Minneapolis-St. Paul, Minnesota, 2014. Prev Chronic Dis. 2016;13:E153. doi: 10.5888/pcd13.160149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.U.S. Census Bureau. American Community Survey (ACS) [Internet]. Available from: https://www.census.gov/programs-surveys/acs [cited 2019 Mar 20].
- 35.Poverty Guidelines [Internet]. U.S. Department of Health and Human Services. 2019. Available from: https://aspe.hhs.gov/poverty-guidelines [cited 2019 Nov 19]
- 36.Minneapolis Staple Foods Ordinance: comparison of past to current requirements as of 12/7/18 [Internet]. 2018 Available from: http://www.minneapolismn.gov/www/groups/public/@health/documents/webcontent/wcmsp-216177.pdf [cited 2019 Mar 20].
- 37.Laska MN, Pelletier JE. Minimum Stocking Levels and Marketing Strategies of Healthful Foods for Small Retail Food Stores [Internet]. Minneapolis, MN: Healthy Eating Research; 2016 Feb. Report No.: 1088. Available from: http://healthyeatingresearch.org/wp-content/uploads/2016/02/her_minimum_stocking_final.pdf. [cited 2016 Feb 10]
- 38.City of Passaic, NJ: Chapter 162 Grocery Stores [Internet]. City of Passaic, NJ Code. 2017 Available from: https://ecode360.com/32444965. [cited 2019 Mar 20].
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated during the current study are not publicly available because the investigator team is still actively analyzing and publishing study results, but data are available from the corresponding author on reasonable request. We will reassess making.the data publicly available when current analyses are completed.