

Abstract
We created a registry of Danish-born citizens of Denmark with incident International Classification of Diseases (10th ed.; ICD-10) severe stress and adjustment disorder diagnoses between 1995 and 2011. A unique personal identifier was used to retrieve and merge data on demographic characteristics and diagnoses (ICD-10 codes F43.x). Here we report on the incidence of these disorders and the demographic characteristics of the subset of the Danish population who have received 1 of these diagnoses: 111,844 adults and children received a first diagnosis between 1995 and 2011. More women than men (60.1% vs. 39.9%) received a diagnosis. Diagnoses increased during the late teens through early 30s. Adjustment disorder was the most common diagnosis (65.7% of adults and 64% of children). Reaction to severe stress unspecified was the second most common (19.8% of adults and 23.8% of children), and there was a large increase in both, as well as acute stress reaction diagnoses, in 2007 (3,717–5,141, 1,248–2,520, and 348–1,024 in 2006 to 2007, respectively). Findings regarding gender and age of onset are similar to other westernized countries. This registry can be used for future research programs, contributing to the study of stress and trauma.
Posttraumatic stress disorder (PTSD) is associated with psychiatric and physical health comorbidities and suicidal behavior, resulting in heightened interest in the longitudinal course of this disorder (Gradus, Qin, Lincoln, Miller, Lawler, & Lash, 2010; Gradus, Qin, Lincoln, Miller, Lawler, Sorensen, et al., 2010; Greenberg, Rosenfeld, & Ortega, 1995; Kessler, Chiu, Demler, & Walters, 2005; Qureshi, Pyne, Magruder, Schultz, & Kunik, 2009). Although the research to date has contributed to our understanding of disorders resulting from stressful and traumatic experiences—with the exception of PTSD—most studies have been cross-sectional, included small or specific samples and/or a limited set of diagnoses, or relied on retrospective reporting. The paucity of epidemiologic research on severe stress and adjustment disorders is likely due to the challenge of obtaining longitudinal population-based samples. When utilizing primary data collection, such samples are costly and resource intensive to construct. Further, studies requiring longitudinal data collection are often plagued by loss to follow-up.
The goal of the current study was to create a national longitudinal registry of all Danish-born residents of Denmark who had received a new International Classification of Diseases (10th ed.; ICD-10) severe stress or adjustment disorder diagnosis between 1995 and 2011. These diagnoses include acute stress reaction (F43), PTSD (F43.1), adjustment disorder (F43.2), other reaction to severe stress (F43.8), or reaction to severe stress, unspecified (F43.9; Janca, Ustun, van Drimmelen, Dittmann, & Issac, 1994). In the present article, we outline the methodology used to assemble the registry and present the demographic characteristics of the people included within it. Going forward, this registry can be used as a resource for the examination of the longitudinal course of these disorders.
Method
Participants
The base population for the study was Danish-born residents of Denmark who sought treatment at an inpatient or outpatient psychiatric clinic between January 1, 1995 and December 31, 2011. Registry members had to receive at least one incident severe stress or adjustment disorder diagnosis during this time. Anyone with a diagnosis between January 1, 1994 and December 31, 1994 was excluded from the registry. Those diagnosed in 1994, the year these diagnoses were introduced in Denmark, may have been living with the disorder prior to receiving the diagnosis that year (i.e., they were prevalent cases). Prevalent cases may differ from incident cases with regard to disorder etiology (e.g., prevalent cases are impacted by factors associated with disorder maintenance and survival), so these cases were removed from the registry and the current analyses as an extra step to ensure that only incident, newly occurring cases were examined. We defined children as those 15 and younger at diagnosis. In total, 111,844 people (101,663 adults and 10,181 children) received a first severe stress or adjustment disorder diagnosis between 1995 and 2011.
Procedure
Data were obtained from national Danish medical and social longitudinal registers. The 10-digit Civil Registration number, a unique identifier assigned to all residents of Denmark, was used to retrieve and merge individual data. This study was approved by the Institutional Review Board of the Boston University Medical Center.
Measures
The Danish Civil Registration System contains information on birthdate, gender, residence, parent–child relationships, vital status, and emigration data for all persons legally residing in Denmark (Pedersen, Gotzsche, & Moller, 2006). We utilized data on birthdate, gender, and citizenship status for the current study.
The Psychiatric Central Register has collected data on psychiatric inpatient and outpatient diagnoses since 1995. This register contains diagnosis dates, and up to 20 diagnoses per entry with primary diagnoses specifically noted. We used this register to obtain incident severe stress and adjustment disorder diagnoses.
Data Analysis
We explored the proportion of incident severe stress and adjustment disorder diagnoses by adult/child status, gender, primary/secondary diagnosis, age, and year of diagnosis. To compare registry members to the general population with regard to gender and age, we calculated the weighted average of the general population person-time within these variables over the study period. For age, this calculation was performed by dividing each individual’s person-time into subgroups according to age and calendar year and summing across years and then dividing by the total person-time for the entire registry over the entire study period and across all ages. The comparable calculation was conducted for gender. A kernel smoothing procedure was used to graph diagnoses by age (Greenland, 2008). Finally, we calculated the incidence rate of all disorders during the study period.
Results
Adjustment disorder was the most common diagnosis, followed by unspecified reaction to severe stress. In 90.5% of cases, the severe stress or adjustment disorder diagnosis was the primary diagnosis (i.e., the diagnosis was not secondary to another disorder such as major depression). Approximately 17.6%(19,696/111,844) of registry members received a different second diagnosis within the category of severe stress or adjustment disorder (e.g., a PTSD diagnosis following an acute stress reaction diagnosis). Incidence rates for each diagnosis are displayed in Table 1. More women than men received severe stress and adjustment disorder diagnoses (Table 2; 60.1% and 39.9%, respectively) and women were over-represented among those with diagnoses (60% of adults and 60.1% of children) as compared to the general population during this period (49.2% adult male, 50.8% adult female, 51.3% male children and 48.7% female children).
Table 1.
Incidence Rate of Severe Stress and Adjustment Disorder Diagnoses Among Danish-Born Adults and Children from 1995–2011
| Variable | Adults (n = 101,663) |
Children (n = 10,181) |
Incidence rate | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | Incidence rate | n | % | Incidence rate | ||||
| ASR | 9,182 | 9.0 | 13.3 | 527 | 5.2 | 3.0 | 11 | ||
| PTSD | 3,786 | 3.7 | 5.5 | 243 | 2.4 | 1.4 | 4.7 | ||
| AD | 66,823 | 65.7 | 97 | 6,511 | 64 | 37.6 | 85 | ||
| ORSS | 1,692 | 1.7 | 2.5 | 473 | 4.6 | 2.7 | 2.5 | ||
| RSSU | 20,180 | 19.8 | 29.3 | 2,427 | 23.8 | 14 | 26 | ||
Note. Children defined as those aged 15 and younger. Proportion calculation is the proportion of specific diagnoses within the registry, stratified by adult/child status. Incidence rates were calculated using the person time from all Danish born residents of Denmark and are displayed per 100,000 person-years. ASR = acute stress reaction; PTSD = posttraumatic stress disorder; AD = adjustment disorder; ORSS = other reactions to severe stress; RSSU = reactions to severe stress unspecified.
Table 2.
Distribution and Incidence Rates of Incident Severe Stress and Adjustment Disorder ICD-10 Diagnoses by Gender from 1995–2011
| Variable | Adults |
Children |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Males (n = 40,594) |
Females (n = 61,069) |
Males (n = 3,993) |
Females (n = 6,188) |
||||||||||||
| n | % | Incidence rate | n | % | Incidence rate | n | % | Incidence rate | n | % | Incidence rate | ||||
| ASR (F43.0) | 4,078 | 44.4 | 12 | 5,104 | 55.6 | 14.6 | 188 | 35.7 | 2.1 | 339 | 64.3 | 4.0 | |||
| PTSD (F43.1) | 1,514 | 40 | 4.5 | 2,272 | 60 | 6.5 | 104 | 42.8 | 1.2 | 139 | 57.2 | 1.6 | |||
| AD (F43.2) | 26,330 | 39.4 | 77.7 | 40,493 | 60.6 | 115.6 | 2,627 | 40.3 | 29.6 | 3,884 | 59.7 | 46 | |||
| ORSS (F43.8) | 585 | 34.6 | 1.7 | 1,107 | 65.4 | 3.2 | 204 | 43.1 | 2.3 | 269 | 56.9 | 3.2 | |||
| RSSU (F43.9) | 8,087 | 40.1 | 23.9 | 12,093 | 59.9 | 34.5 | 870 | 35.8 | 9.8 | 1,557 | 64.2 | 18.4 | |||
Note. Children are defined as those aged 15 and under. Proportion calculation is the proportion of specific diagnoses within the registry, stratified by adult/child status and gender. Incidence rates were calculated using the person time from all Danish born residents of Denmark and are displayed per 100,000 person-years. ICD = International Classification of Diseases; ASR = acute stress reaction; PTSD = posttraumatic stress disorder; AD = adjustment disorder; ORSS = other reactions to severe stress; RSSU = reactions to severe stress unspecified.
The highest proportion of new diagnoses was during the late teenage years, with smaller proportions starting in the 20s (Figure 1). A shallower increase in the proportion of diagnoses begins in the late 20s, and these proportions remain relatively steady until the early 40s, when all diagnoses begin a decline that lasted throughout old age.
Figure 1.
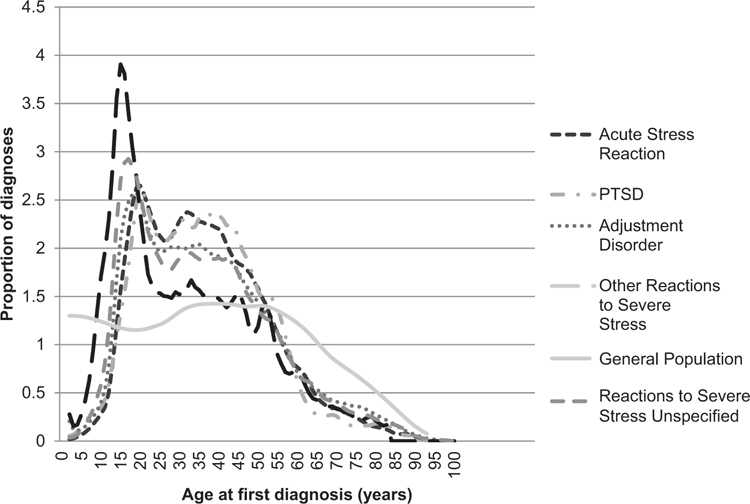
Proportion of incident severe stress and adjustment disorder diagnoses (within each diagnosis) by age at first diagnosis (n = 111,844), 1995–2011.
With regard to calendar year of first diagnoses (Figure 2), there was a large increase in acute stress reaction, adjustment disorder, and unspecified reactions to severe stress diagnoses in 2007 (348–1,024, 3,717–5,141, and 1,248–2,520 in 2006 to 2007, respectively). PTSD and other reactions to severe stress diagnoses had shallower increases over the study period.
Figure 2.
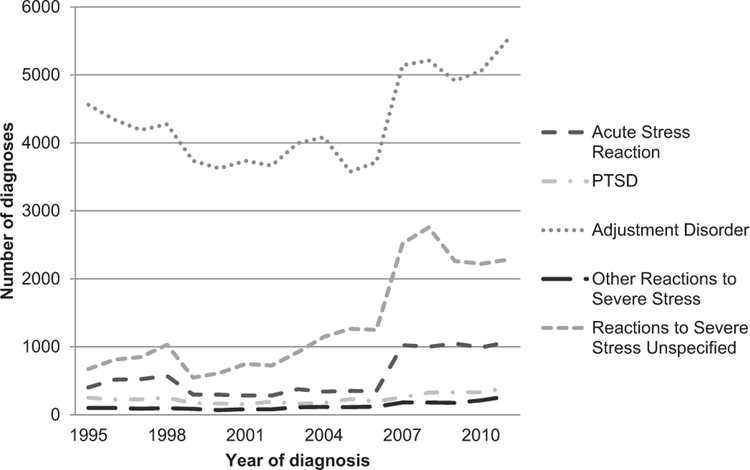
Number of incident severe stress and adjustment disorder diagnoses by calendar year (n = 111,844), 1995–2011.
Discussion
Here we summarized incident ICD-10 severe stress and adjustment disorder diagnoses in Denmark from 1995 through 2011, obtained from a newly constructed longitudinal registry. Adjustment disorder was the most common diagnosis, perhaps indicative of this diagnosis being used as a catch-all for vague symptomatology or for those experiencing mild to moderate symptomatology following a stressful life event. Unspecified reaction to severe stress was the second most common, perhaps capturing patients with symptomatology who do not meet ICD-10 criteria for a specific disorder (e.g., the time since event). Future research should explore the symptom profile of patients with this diagnosis.
Consistent with gender differences literature, women received PTSD and other diagnoses more frequently than men (Breslau, Davis, Andreski, Peterson, & Schultz, 1997; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Factors impacting the female to male ratio of PTSD diagnoses in other countries include women’s greater willingness to report mental health symptoms and women more frequently experiencing traumatic events that lead to a posttrauma diagnosis. These factors may explain the increased frequency of PTSD and other severe stress and adjustment disorder diagnoses among women in Denmark (Tolin & Foa, 2006). Age at diagnosis also showed a pattern consistent with other Westernized cultures (Bunting, Murphy, O’Neill, & Ferry, 2012; Kessler et al., 2005).
Among the most interesting findings was the sudden increase in acute stress reaction, adjustment disorder, and unspecified reaction to severe stress in 2007. Many factors could have led to this increase including changes in diagnostic practices or an event (e.g., natural disaster) that acted as a stressor or trauma to many people simultaneously. We know of no mass trauma that impacted Denmark on a national scale in 2007; however, a congress for Danish psychiatrists and psychologists that year explored when psychological help following trauma is most beneficial, perhaps shifting clinical attention towards these disorders. This finding serves as an example of the dynamic nature of prevalence and incidence, and highlights the import of examining disorders longitudinally.
The current study is not without limitations. We excluded diagnoses from somatic treatment facilities because disorder etiology may differ from diagnoses made at psychiatric facilities. Additionally, this study included people who sought psychiatric treatment. It is possible that there are people who have not sought treatment or who were treated by private psychiatrists, despite access to free healthcare in Denmark. These people would not be included, although the majority of people with psychiatric disorders eventually make treatment contact (Wang, Berglund, Olfson, & Kessler, 2004). Although all data are collected prospectively in the longitudinal Danish national registries, our assessment of these disorders occurred at one point in time. Finally, most individuals with mild/moderate psychiatric disorders are treated by general practitioners or private psychiatrists and psychologists in Denmark, so they may not be in the Psychiatric Central Register (Mors, Perto, & Mortensen, 2011); therefore, this study may only include moderate/severe cases.
This study makes a contribution to the literature by exploring severe stress and adjustment disorder diagnoses in a population-based sample. In addition, the registry that was created for this project can be used for future projects that could contribute important advances to the study of stress and trauma by examining multiple predictors and sequelae of these disorders in a longitudinal population-based sample.
Acknowledgments
This work was funded by a National Institute of Mental Health grant: “Constructing a Danish Reaction to Severe Stress Cohort” (1R21MH094551-01A1), Jaimie Gradus, Principal Investigator.
References
- Breslau N, Davis GC, Andreski P, Peterson EL, & Schultz LR (1997). Sex differences in posttraumatic stress disorder. Archives of General Psychiatry, 54, 1044–1048. doi: 10.1001/archpsyc.1997.01830230082012 [DOI] [PubMed] [Google Scholar]
- Bunting BP, Murphy SD, O’Neill SM, & Ferry FR (2012). Lifetime prevalence of mental health disorders and delay in treatment following initial onset: Evidence from the Northern Ireland Study of Health and Stress. Psychological Medicine, 42, 1727–1739. doi: 10.1017/50033291711002510 [DOI] [PubMed] [Google Scholar]
- Gradus JL, Qin P, Lincoln AK, Miller M, Lawler E, & Lash TL (2010). The association between adjustment disorder diagnosed at psychiatric treatment facilities and completed suicide. Clinical Epidemiology, 2, 23–28. doi: 10.1093/ije/dyq112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gradus JL, Qin P, Lincoln AK, Miller M, Lawler E, Sorensen HT, & Lash TL (2010). Posttraumatic stress disorder and completed suicide. American Journal of Epidemiology, 171, 721–727. doi: 10.1093/aje/kwp456 [DOI] [PubMed] [Google Scholar]
- Greenberg WM, Rosenfeld DN, & Ortega EA (1995). Adjustment disorder as an admission diagnosis. American Journal of Psychiatry, 153, 759–461. [DOI] [PubMed] [Google Scholar]
- Greenland S (2008). Analysis of ploytomous exposures and outcomes In Rothman KJ, Greenland S & Lash TL (Eds.), Modern epidemiology (3rd ed.). Philadelphia PA: Lippincott Williams & Wilkins. [Google Scholar]
- Janca A, Ustun TB, van Drimmelen J, Dittmann V, & Issac M (1994). ICD-10 symptom checklist for mental disorders, Version 1.1]. Geneva, Switzerland: World Health Organization, Division of Mental Health. [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593–602. doi: 10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- Kessler RC, Chiu WT, Demler O, & Walters EE (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 617–627. doi: 10.1001/archpsyc.62.6.617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Sonnega A, Bromet E, Hughes M, & Nelson CB (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52, 1048–1060. doi: 10.1001/archpsyc.1995.03950240066012 [DOI] [PubMed] [Google Scholar]
- Mors O, Perto GP, & Mortensen PB (2011). The Danish Psychiatric Central Research Register. Scandinavian Journal of Public Health, 39, 54–57. doi: 10.1177/1403494810395825 [DOI] [PubMed] [Google Scholar]
- Pedersen CB, Gotzsche H, & Moller J (2006). The Danish civil registration system. A cohort of eight million persons. Danish Medical Bulletin, 53, 441–449. [PubMed] [Google Scholar]
- Qureshi SU, Pyne JM, Magruder KM, Schultz LR, & Kunik ME (2009). The link between post-traumatic stress disorder and physical comorbidities: A systematic review. Psychiatric Quarterly, 80, 87–97. doi: 10.1007/s11126-009-9096-4 [DOI] [PubMed] [Google Scholar]
- Tolin DF, & Foa EB (2006). Sex differences in trauma and posttraumatic stress disorders: A quantitative review of 25 years of research. Psychological Bulletin, 132, 959–992. doi: 10.1037/0033-2909.132.6.959 [DOI] [PubMed] [Google Scholar]
- Wang PS, Berglund PA, Olfson M, & Kessler RC (2004). Delays in initial treatment contact after first onset of a mental disorder. Health Services Research, 39, 393–415. doi: 10.1111/j.1475-6773.2004.00234 [DOI] [PMC free article] [PubMed] [Google Scholar]