

Abstract
Objectives
To investigate veterinary technician burnout and associations with frequency of self‐reported medical error, resilience, and depression and job‐related risk factors.
Design
Cross‐sectional observational study using an anonymous survey conducted between November 2017 and June 2018.
Setting
Four referral teaching hospitals in the United States and Canada.
Subjects
A total of 344 veterinary technicians were invited to participate. Response rate was 95%. Overall 256 surveys were ultimately analyzed.
Interventions
Burnout, depression, and resilience were measured using validated instruments. Respondents reported perceptions of workload, working environment, and medical error frequency. Associations between burnout and factors related to physical work environment, workload and schedule, compensation package, interpersonal relationships, intellectual enrichment, and exposure to ethical conflicts were analyzed.
Measurements and Main Results
Burnout, characterized by high emotional exhaustion, depersonalization, and low sense of personal accomplishment was common, and was positively associated with perceived medical errors, desire to change career, and depression. Burnout levels on all 3 burnout subscales were higher in this population than previously reported for a contemporaneous group of trauma nurses working with human patients (P < 0.05). Burnout was negatively associated with resilience. Respondents’ feelings of fear or anxiety around supervisor communications, perception that patient load was too high to allow for excellent patient care, and perceived lack of available assistance during sudden workload increases were all associated with burnout.
Conclusions
Burnout in veterinary technicians is common and is associated with numerous undesirable outcomes. Work‐related interventions to reduce burnout should focus on improving supervisor relationships and maintaining an appropriate patient:caregiver ratio.
Keywords: depression, emotional exhaustion, medical errors, resilience, staff turnover
Abbreviations
- CDRISC
Connor Davidson Resilience Scale
- CI
confidence interval
- DP
depersonalization
- EE
emotional exhaustion
- HADS
Hospital Anxiety and Depression Scale
- IQR
interquartile range
- MBI
Maslach Burnout Inventory
- PA
personal accomplishment
1. INTRODUCTION
Burnout has been defined as a psychological state typified by emotional exhaustion, depersonalization, or cynicism toward patients and colleagues, and a reduced sense of personal accomplishment.1 Burnout syndrome has been documented in a wide range of health care professions,2 and job stress is recognized as the principal cause of burnout.3 Burnout syndrome has been associated with decreased quality of care, increased risk of medical errors,4 increased risk of nosocomial infection,5 and increased costs related to staff absenteeism and high turnover6 among medical professionals caring for human patients. Burnout has been associated with symptoms of depression, poor quality of personal well‐being, and increased work conflicts.2, 7 Thus, burnout is associated with multiple negative consequences for caregivers, patients, and hospital revenue.
Within the veterinary hospital setting, there has been recent increased focus on the difficulty of hiring and retaining veterinary technician staff.1 Previous studies of veterinary technicians in the primary care setting have found high Maslach Burnout Inventory (MBI) scores on the emotional exhaustion and cynicism subscales to be associated with low job satisfaction and increased perception of a toxic work environment.8 Conversely, positive associations between supportive interpersonal relationships and higher job satisfaction have been identified.9 However, there are no reports focusing on veterinary technicians working in a specialty referral hospital setting. Job‐related risk factors associated with burnout have not been identified in this arena, and the potential for negative sequela of burnout such as depression and increased medical errors has not been assessed. This information deficit has resulted in a limited evidence base to guide both prioritization of this issue at a management level and decision‐making regarding interventions directed at burnout reduction.
Psychological resilience is recognized as an important factor associated with enhanced ability to provide high‐quality care and increased sustainability of the health care workforce. Resilience is defined as the ability to respond to stress in a healthy way with minimal psychological cost.10 Resilience skills can be taught, and this has been suggested as a potential avenue to reduce burnout prevalence.10 The relationship between resilience and burnout has not been evaluated in veterinary technicians.
The purpose of this exploratory study was to investigate burnout among veterinary technicians working in a specialty hospital setting. The study goal was to investigate associations between burnout and frequency of self‐reported medical error, resilience, and depression in this population, with the hypotheses that burnout in veterinary technicians would be different than levels previously reported for medical professionals caring for human patients, positively associated with medical errors and depression and negatively associated with resilience. An additional goal was to perform an analysis of job‐related risk factors associated with burnout, with the hypothesis that there would be associations between potentially modifiable job‐related factors and burnout. This information could then provide a framework for future research focused on measures to reduce burnout.
2. MATERIALS AND METHODS
2.1. Study overview
This was a cross‐sectional census survey study conducted in 4 veterinary specialty teaching hospitals (Cornell University Hospital for Animals, University of Guelph Ontario Veterinary College, Angell Animal Medical Center, and the University of Florida College of Veterinary Medicine) between November 30, 2017 and June 30, 2018. The electronic survey2 was administered during personal meeting or by individual electronic link to be completed at a later time, at the respondent's preference. Participation was voluntary and data were de‐identified. Standardized interviews to administer the survey were conducted by 7 individuals across the 4 settings. The study was assessed by the institutional review boards at Cornell University and University of Florida and considered exempt (Protocol ID# 1710007488 and 201800438) and was approved by the Research Ethics Board at the University of Guelph (REB# 18‐03‐037) and the Clinical Studies Committee at Angell Animal Medical Center. The Maslach Burnout Inventory (MBI)11 was used to quantify burnout syndrome in this study and is the most widely accepted tool for measuring burnout in research on the syndrome.7 The MBI is constructed on 3 subscales, and high burnout is characterized as high emotional exhaustion (EE), high depersonalization (DP), and low personal accomplishment (PA). The MBI‐HSS (Maslach Burnout Inventory Health Services Scale) uses the term “recipients” to refer to “the particular people for whom the respondent provides service, care or treatment.” The MBI‐HSS questions were modified to reflect the veterinary work environment by replacing the term “recipients” with “patients, patients’ owners, and co‐workers” as applicable. The Connor Davidson Resilience Scale (CD‐RISC)12 is a validated instrument that was used to measure psychological resilience. The Hospital Anxiety and Depression Scale (HADS) is a validated instrument that was used to measure depression.13
Comparison data on mean burnout subscale scores from a contemporaneous and age‐ and gender‐matched group of United States nurses caring for human patients were obtained from a study investigating perceived stress and job satisfaction among human trauma nurses.14
2.2. Study respondents
A list of all eligible veterinary technicians employed within each teaching hospital was obtained from the Human Resources department. All listed individuals were contacted individually either in person or by email and asked if they would be willing to participate in a survey investigating burnout and working conditions. If they indicated willingness to participate, they were then either emailed a link to the electronic survey or the survey was administered by personal interview, depending on their preference. Respondents were considered eligible if: they had graduated from a formal veterinary technician training program and were certified or licensed as a veterinary technician within their state or province of employment; had graduated at least 6 months prior; were working more than 20 h/wk as a veterinary technician and were not in solely managerial or administrative positions; and were able to read, write, or converse in English.
2.3. Study measures
Information was collected on participant demographics (age, gender), years in the profession, professional qualifications, field of work (eg, small animal internal medicine, large animal surgery), and self‐reported frequency of making medical errors, as well as burnout, depression, and resilience. Medical error frequency was considered “high” if reported as occurring a few times a month or more. Burnout was measured using the MBI‐HSS. The authors do not recommend using cut‐points on the 3 subscales to diagnose burnout and indicate that subscale quantification on a continuous scale to compare populations and associations between risk factors and burnout is preferred. Depression was assessed using the HADS. This is an internationally recognized questionnaire that screens for anxiety and depression and demonstrates good levels of internal consistency and test‐retest reliability, with a factor structure that has been confirmed in multiple populations.15 The depression subscale measures 7 items. Per recommended scoring, respondents were classified as meeting the criteria for depression if they scored ≥11 (HADS manual). Resilience was measured using the CD‐RISC. The CD‐RISC has been extensively used in observational studies and clinical trials and has excellent test‐retest reliability.16 It is a 25‐item self‐reporting scale that ranges from 0 to 100. Per recommended scoring, resilience was defined as a CD‐RISC score >80, and high resilience was scored as CD‐RISC ≥92.16
Candidate exposures to be explored as potentially protective against burnout were selected based on previous studies of burnout and resilience in the fields of health care, teaching, and the military.2, 10, 17 They were grouped under categories of respondent personal characteristics and lifestyle, compensation package, workload and schedule, interpersonal relationships, exposure to intellectual enrichment, exposure to ethical conflicts, and physical characteristics of the work environment. Exposures were quantified as binary (for example, “My employer provides me with paid sick leave:” yes/no), continuous numerical (for example, “The maximum number of days that I work consecutively on a regular basis is…”), or ordinal in terms of frequency of the exposure (for example, “I work weekends never/rarely or a few times per year/seldom or once a month or less/often or a few times per month/frequently or once a week/always or daily”). Details on the specific exposures investigated are shown in Table 1.
Table 1.
Candidate exposure categories and exposures explored for associations with burnout
| Exposure category | Exposures assessed |
|---|---|
| Personal characteristics and lifestyle | Gender, age, time in career, weekly exercise duration (h), specialty affiliation, holding technician specialty certification |
| Compensation package | Hourly wage, health insurance, dental insurance, maternity leave, sick leave, retirement plan, continuing education support, pet health care subsidy, premium for specialty tech qualification, premium for increased experience |
| Workload and schedule | Weekly hours, night work, weekend work, ability to self‐schedule breaks, ability to schedule time off, number of consecutive days worked, shift duration, working more or less hours than contracted, help availability during workload peaks, perceptions of patient load versus patient care, performing janitorial tasks |
| Interpersonal relationships | Size of work unit, respect received from clinicians, supervisor accessibility, supervisor approachability, receiving positive feedback, level of staff turnover, exposure to positive co‐worker relationships, exposure to disagreement among clinical team, respondents feelings of appreciation from upper management |
| Intellectual enrichment | Acquisition of new technical skills, acquisition of new medical knowledge, participating in patient rounds, participation in clinical research, assuming a teaching role, problem solving |
| Ethical conflict exposures | Exposure to patient death/euthanasia, assisting with euthanasia causing discomfort to patients as part of their care, implementing care decisions the respondent disagrees with |
| Physical characteristics of work environment | Designated break location available, environmental temperature, environmental noise levels, exposure to natural daylight, basic equipment availability, support with lifting/ walking heavy patients, ability to nap while on break |
Finally, respondents were asked to state whether they were considering changing their career and, if that was the case, they were asked to rank reasons for this within categories of job satisfaction, compensation, and work environment.
2.4. Statistical methods
Continuous descriptive data were analyzed and presented as mean ± SD where normal, or median (interquartile range [IQR]) where not normal. Normality was assessed using the Shapiro–Wilk test. Categorical data were presented as percentages and 95% confidence intervals (CI). Ordinal data were dichotomized. Associations between categorical data were assessed using the chi‐square test or Fisher's exact test where cell counts ≤5. Differences between group means were assessed using the Students’ t‐test with Satterthwaite's correction for unequal variances, where applicable. Associations between the EE, DP, and PA subscores and binary outcomes of interest were tested with univariable logistic regression to obtain odds ratios (ORs). Independent associations between candidate exposures and the EE, DP, and PA subscores were assessed initially using univariable linear regressions. Ordinal variables were treated as indicator variables or dichotomized for the purposes of analysis. The assumptions of the regression models were checked using visual plots to evaluate linearity, the Cook–Weisberg test to assess homoscedasticity, and qq plots together with the Shapiro–Wilk test to assess for normality of the residuals. Where departures from normality in the residuals were identified, robust standard errors were used. The relationships between factors associated with EE, DP, and PA within each exposure category were explored in a series of Venn diagrams. Variables that had a univariable association with all 3 MBI‐HSS scores within each exposure category were assessed for correlation using Spearman's rank correlation coefficient and entered into multivariable models against the EE, DP, and PA subscores. A manual build was performed with evaluation of interaction terms where biologically plausible. Model assumptions were checked as above. Collinearity was evaluated during the model build using variance inflation factors. The adjusted R 2 was calculated for each model. The adjusted R 2 is a measure of the explanatory power of the model for the data after adjustment for the number of variables within the model. The level of significance was set at P < 0.05. All statistical analyses were performed using Stata 15.3
3. RESULTS
Details of survey participation are shown in Figure 1. Of the 344 technicians invited to participate, 327 provided either partial or full responses (95%). After exclusion criteria were applied (n = 31) and surveys with incomplete data were removed (n = 40), 256 surveys remained for analysis. Respondents were recruited from 4 centers: Ontario Veterinary College (n = 65), Angell Animal Medical Center (n = 63), University of Florida (n = 61), and Cornell University (n = 67). The survey took a median of 28.3 minutes to complete (IQR, 16.8). The survey population gender was 94% female (n = 241), 5% male (n = 14), and 0.03% lesbian/gay/bisexual/transsexual (n = 1). The median age was 36 years (IQR, 15). The respondents worked predominantly with small animals (91%, n = 234) with the remainder split between large animals (5%, n = 14) and exotic/wildlife species (3%, n = 8). Median career duration was 12 years (IQR, 13). Fifty‐nine percent of respondents (n = 152) held academic or professional qualifications in addition to their primary veterinary technician qualification.
Figure 1.
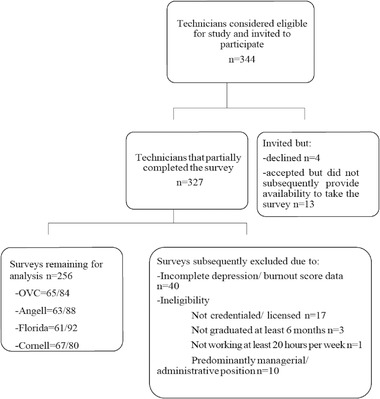
Flow diagram illustrating the survey responses acquired from technicians working at 4 veterinary specialty teaching hospitals and subsequent exclusions
The results for the MBI‐HSS EE, DP, and PA subscales are shown in Table 2. Participating veterinary technicians scored higher on the EE and DP subscales and lower on the PA subscales than a contemporaneous comparison group of trauma nurses.
Table 2.
Results of MBI‐HSS EE, DP, and PA subscale assessment and comparisons with trauma nurses
| MBI subscale | Veterinary technicians (n = 256) | Trauma nurses at Level 1 US trauma center (n = 79)14 | P‐value |
|---|---|---|---|
| Emotional exhaustion | 30.73 (±10.71) | 23.80 (±12.76) | P < 0.0001 |
| Depersonalization | 8.25 (±5.82) | 6.72 (±5.18) | P = 0.0370 |
| Personal accomplishment | 32.39 (±7.37) | 35.31 (±7.53) | P = 0.0024 |
Mean (SD).
The mean HADS depression score was 5.70 ± 3.94; 12.9% (n = 33, 95% CI, 9.0%‐17.6%) of the study population met the classification for depression as defined by HADS screening. Depression was positively associated with the MBI‐HSS EE (OR, 1.18, 95% CI, 1.12%–1.25%, P < 0.001) and DP (OR, 1.17, 95% CI, 1.09%‐1.24%, P < 0.001) subscales. Depression was negatively associated with the PA subscale (OR, 0.90, 95% CI, 0.86%‐0.95%, P < 0.001). EE, DP, and PA subscale scores and prevalence of depression did not differ significantly by center.
The mean CD‐RISC was 68.8 (± 13.1); 19.1% (n = 49, 95% CI, 14.5%‐24.5%) of the population was classified as resilient (score >80) and 2.7% (n = 7, 95% CI, 1.1%‐5.5%) as highly resilient (score ≥92) using the CD‐RISC. Resilience was negatively associated with the MBI‐HSS EE (OR, 0.96, 95% CI, 0.93%‐0.99%, P = 0.006) and DP (OR, 0.95, 95% CI, 0.89%‐0.99%, P = 0.042) subscales. Resilience was positively associated with the PA subscale (OR, 1.18, 95% CI, 1.11%‐1.25%, P < 0.001). Prevalence of resilience did not differ significantly by center.
In the analysis of possible associations between burnout and medical errors, 5.1% (n = 13, 95% CI, 2.7%‐8.5%) of respondents reported a medical error rate of several per month or higher. A high medical error rate (errors reported as occurring a few times a month or more) was positively associated with the MBI‐HSS EE (OR, 1.09, 95% CI, 1.02%‐1.16%, P = 0.007) and DP (OR, 1.20, 95% CI, 1.09%‐1.31%, P < 0.001) subscales, and negatively associated with the PA subscale (OR, 0.93, 95% CI, 0.86%‐0.99%, P = 0.034). A high medical error rate was negatively associated with the CD‐RISC score (OR, 0.95, 95% CI, 0.91‐0.99%, P = 0.026).
In the analysis of possible associations between burnout and career change, 18.4% (n = 47, 95% CI, 13.9%‐23.7%) of respondents considered a career change on at least a weekly basis. Frequent consideration of career change was positively associated with the MBI‐HSS EE (OR, 1.11, 95% CI, 1.07%‐1.15%, P < 0.001) and DP (OR, 1.12, 95% CI, 1.06%‐1.18%, P < 0.001) subscales, and negatively associated with the PA subscale (OR, 0.94, 95% CI, 0.90%‐0.98%, P = 0.005). Frequent consideration of career change was negatively associated with the CD‐RISC score (OR, 0.98, 95% CI, 0.95%‐0.99%, P = 0.045).
The analysis of associations between work environment risk factors and MBI‐HSS burnout subscales identified factors within the categories of personal characteristics and lifestyle, compensation package, workload and schedule, interpersonal relationships, intellectual enrichment, ethical conflict exposures, and physical characteristics of work environment that showed univariable association at P < 0.05 on the EE, DP, and PA subscales. These factors and the overlap between the subscales are shown in Figures 2 and 3, with data from the univariable models shown in Supporting Information Appendix 1. The exposures investigated within the compensation package category showed the fewest associations and only with the EE subscale. The personal characteristics and lifestyle category was also relatively unfruitful, with no exposures showing associations on more than 1 subscale. The categories of workload and schedule, interpersonal relationships, intellectual enrichment, and physical characteristics of work environment all contained variables that showed associations with all 3 burnout subscales. These variables and categories were then put forward for multivariable analysis. Results are shown in Figure 4. The adjusted R 2 for models within each variable category and subscale are shown in Table 3. Based on this analysis, the categories of workload and schedule and interpersonal relationships had the greatest explanatory power on all 3 burnout subscales. Within these categories, the factors with the strongest associations with the burnout subscales were respondent feelings of fear or anxiety around communications with their supervisor, the respondent perception that patient load was inconsistent with their ability to provide excellent patient care, and the respondent perception that assistance was inconsistently or never available during sudden workload increases (Figure 4). Respondent perception that co‐worker relationships were not always positive also showed a relatively strong negative association with the personal accomplishment subscale, as did the perception that they were seldom or never able to implement their solutions to problems. Seldom or never having support staff available to help lift or walk heavy patients also had a strong positive association with depersonalization.
Figure 2.
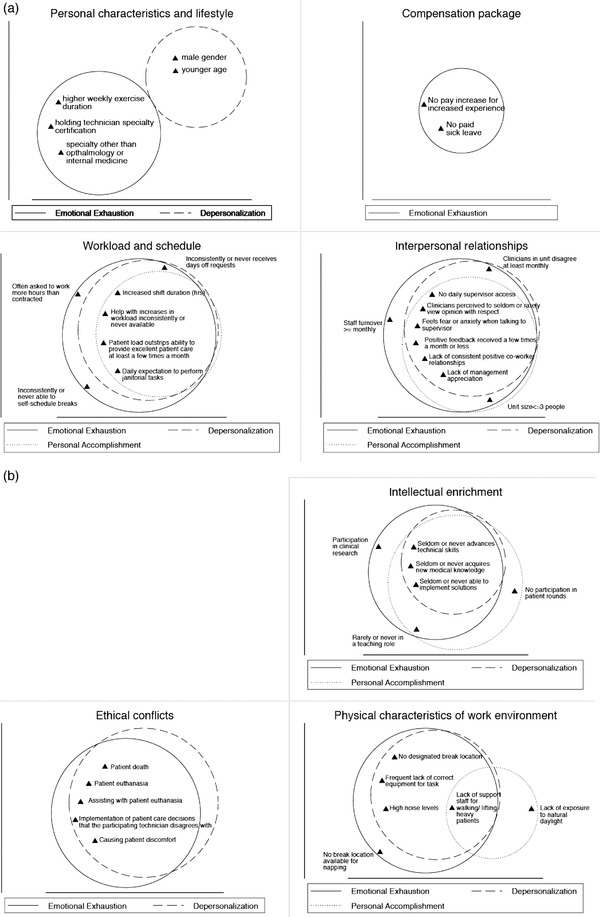
A and B, Venn diagrams showing the variables within the 7 exposure categories identified in Table 1 that were identified as having a univariable association at P < 0.05 with increased severity of burnout on the Maslach emotional exhaustion, depersonalization, or personal accomplishment subscales. Variables identified to have univariable associations with all 3 subscales were then put forward for entry into a multivariable model of each exposure category against each subscale. Univariable models are detailed in full in Supporting Information Appendix 1
Figure 3.
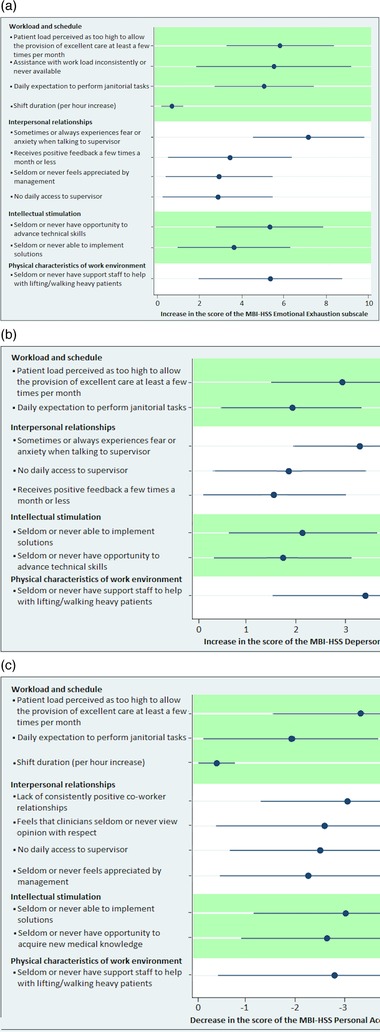
A–C, Figures showing beta coefficients and 95% CI for risk factors retained in multivariable models of exposure category vs Maslach emotional exhaustion, depersonalization, or personal accomplishment subscales at P < 0.05. Multivariable models are detailed in full in Appendix 2. An example of interpretation would be “A technician who perceives patient load as too high to allow provision of excellent patient care a few times a month or more often will have a Maslach EE score that is on average increased by 5.8 units compared with a technician who perceives patient load as too high to allow provision of excellent patient care less frequently than a few times a month, after controlling for the effects of shift duration, availability of assistance with workload, and frequency of performing janitorial tasks”
Figure 4.
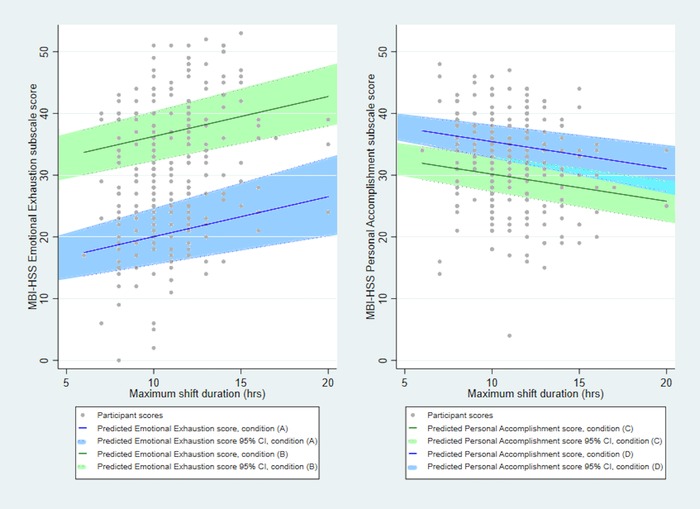
A and B, Graphs showing the associations between maximum shift duration (hours), Maslach EE and Maslach PA scores derived from the multivariable models. Line B shows the association between emotional exhaustion and shift duration (P = 0.015) when respondents were expected to perform janitorial tasks on a daily basis (P < 0.001), had assistance with workload inconsistently or never available (P = 0.004), and perceived patient load to be too high to allow excellent patient care at least a few times a month or more often (P < 0.001). Line A shows the association between emotional exhaustion and shift duration when respondents were expected to perform janitorial tasks on a less than daily basis, had assistance with workload often or always available, and perceived patient load to be too high to allow excellent patient care less often than a few times a month. Line D shows the association between personal accomplishment and shift duration (P = 0.018) when respondents were expected to perform janitorial tasks on a daily basis (P = 0.032) and perceived patient load to be too high to allow excellent patient care at least a few times a month or more often (P < 0.001). Line C shows the association between personal accomplishment and shift duration when respondents were expected to perform janitorial tasks on a less than daily basis and perceived patient load to be too high to allow excellent patient care less often than a few times a month
Table 3.
Multivariable model adjusted R 2 results for each category of exposures explored for associations with burnout
| Category | EE model adj R 2 | DP model adj R 2 | PA model adj R 2 |
|---|---|---|---|
| Workload and schedule | 0.243 | 0.098 | 0.097 |
| Interpersonal relationships | 0.236 | 0.165 | 0.156 |
| Intellectual enrichment | 0.100 | 0.056 | 0.083 |
| Physical characteristics of work environment | 0.051 | 0.054 | 0.022 |
The maximum hours worked per shift showed a positive association with emotional exhaustion and negative association with personal accomplishment in multivariable analysis.
Finally, when considering respondent prioritization of job‐related factors, respondents who considered changing their career at least a few times per year (n = 168, 65.6%) ranked concerns regarding insufficient compensation (mean rank = 1.9) above lack of job satisfaction (mean rank = 2.2) and problems with working conditions (mean rank = 2.5) as the prompt for change. When then asked to rank different components of each of these categories in order of importance to them, the prioritized top 3 of 6 subcategories for each category were as follows: for compensation: hourly pay (mean rank = 1.4), health benefits (mean rank = 2.7), sick leave (mean rank = 3.5). For job satisfaction: lack of upward mobility (mean rank = 2.2), lack of respect from veterinarians (mean rank = 2.9), and lack of supported continuing education (mean rank = 3.0). For working conditions: understaffing (mean rank = 1.7), physical demands of the job (mean rank = 3.8), and lack of supervisor support (mean rank = 3.9).
4. DISCUSSION
The results of this multicenter study indicate that concerns regarding veterinary technician burnout are valid, that burnout and depression are strongly associated in this population, and burnout can be associated with increased medical errors and desire for career change. This is likely to have negative consequences for the quality of hospital care and hospital staffing costs. There are a number of potential areas of intervention that may be protective against burnout, providing avenues for prospective interventional research.
Burnout among health care workers has been the subject of extensive previous investigation.2, 15, 17, 18 The level of burnout reported in this study suggests that burnout prevalence among veterinary technicians is higher than in other medical occupations.19 The level of emotional exhaustion was also higher, and the level of personal accomplishment lower, than that recently reported for veterinarians,20 as well as veterinary technicians in primary care practice.8 The reasons for this are likely multifactorial. The population reported here was almost entirely women (94% female), and female gender has been reported as a risk factor for burnout syndrome; similarly, burnout among nursing staff has been reported to be higher in teaching hospitals compared with other facilities,2 and all our hospitals were teaching hospitals. We also speculate that lack of societal awareness of the key role of the veterinary technician in animal medical care, and the lack of an established professional identity with clear boundaries (as evidenced by the proportion of qualified veterinary technicians performing janitorial tasks) may also be contributing factors to the identified high burnout prevalence. This interpretation would account for the increased burnout found in this technician group compared with a comparison group of trauma nurses that had a similar age and gender composition to this group.
A positive association between burnout and depression was identified in this population, which is in agreement with the literature.21 It has been hypothesized that there is a reciprocal causality between the 2 syndromes; burnout may be a phase in the development of depression and, equally, depression may exacerbate negative aspects of the work experience and lead to burnout. Conceptually, burnout is considered to be job‐specific, while depression is context‐free,22 and factor analysis has suggested they are related, but distinct, constructs.3 Clinically, depression is a distinct mental illness for which diagnostic criteria are available, while burnout is not clinically defined.21 With respect to the results of this study, we might infer that much of the stress experienced by this population appears to be job‐specific (as described by the prevalence of burnout), and that the prevalence of clinical depression in this population is likely increased by these job‐specific stressors.
In addition to the impact on individual quality of life, medical professional burnout has been found to increase the rate of medical errors, lower care quality, and reduce productivity.23, 24 Burnout is also associated with a decrease in empathy25 and effective communication between care provider and recipients.26 The reduced level of care provided by workers experiencing burnout is likely to contribute further to their own decreased satisfaction with their work, as evidenced by the strong negative association between the personal accomplishment subscale and patient loads, which impedes excellent care provision. Reduced career satisfaction, in turn, reduces staff retention.27
A reduction in job performance and increase in turnover stemming from burnout can have significant economic impact on the veterinary industry,28 as well as the individual practices experiencing staff shortages. When skilled technicians leave the profession, the industry as a whole suffers from a reduced experience pool. The veterinary practice itself loses the investment made in that employee and incurs the costs of overtime for the remaining employees, advertising and interviewing for new hires, as well as orienting and training new employees. Finally, the loss of a valued team member can result in reduced morale in the remaining employees and even result in further resignations.29
Interpersonal relationships, workload, and work scheduling characteristics were strongly associated with aspects of burnout in the present study. These areas have previously been identified as significant areas of stress for veterinary support staff30 and represent areas for protective strategies to be implemented and assessed. Limiting the hourly duration of shifts, reducing the need for technicians to perform janitorial tasks, and limiting patient load per technician may all be protective against burnout. Routine, positive interactions with co‐workers and supervisors are also likely to be protective against burnout and its sequelae. These interpersonal interventions could take the form of regular staff meetings and employee reviews, with emphasis placed on positive feedback, problem‐solving, and the respectful interaction of all members of the veterinary team, including clinicians. Continuing education that focuses on positive, effective communication skills and team building may also yield benefit. In the veterinary hospital setting, supervisory staff who may themselves be experiencing burnout are frequently promoted from “floor” positions with minimal or no training in supervisory skills or tools helpful in maintaining positive interpersonal relationships at the supervisor level. Addressing this skill deficit may have a positive effect on burnout levels. Given the high rate of occupational injury and illness already experienced by veterinary staff,31 limitations should also be recommended for the size and weight of patients that technicians are expected to lift or move without assistance.
Interestingly, the results of this study suggested that although burnout may be an individual problem, the causes of burnout appear to be manifesting at a population level and are predominantly related to the hospital structuring of workflow and hospital team function. None of the individual level risk factors assessed (compensation package characteristics, personal characteristics, and lifestyle) showed associations with more than a single burnout subscale. Resilience skills training has been suggested as a tool that individuals can acquire to protect themselves against environment induced burnout and this study identified a positive association between increased resilience and decreased burnout. The concept of resilience training was originally developed in the military environment for soldiers on active service to reduce the incidence of posttraumatic stress disorder following active deployment.10 A notable difference is that the armed conflict zone of the military working environment is inherently uncontrolled, unlike the hospital environment, which is open to control and modification by management. While resilience training may be an appropriate short‐term intervention for employees experiencing burnout, addressing some of the root management causes of burnout suggested by this study at the hospital level may be a more rewarding long‐term path to take.
This study had a number of limitations. The cross‐sectional nature of the study did not allow for interpretation of a causal relationship between the factors studied and burnout severity. An additional limitation of occupational research is the “healthy worker effect,”32 which suggests that individuals who are unwell will tend to leave a job, resulting in an overall “healthy” bias in the remaining working population. Only veterinary technicians working at specialty referral practices were included in this study, which may limit the generalizability of results to technicians in primary care practices. In line with the concept of an exploratory study with the goal of identifying avenues to guide prospective interventional research, we evaluated multiple risk factors for consistent associations with all 3 burnout subscales. Such an approach carries the risk of type I error, which we tried to limit by following a strictly hypothesis‐driven approach and insisting on repeatability through sections of the analysis. Finally, our investigation of medical errors was perceived rather than documented. It is possible that individuals with burnout perceive themselves to be more likely to be making medical errors, whether this is actually the case or not.
In conclusion, burnout in veterinary technicians working in a specialty hospital setting is worryingly high, positively associated with depression and medical error rates, and negatively associated with resilience. Limiting exposure to excess workload (in particular high patient load that limits patient care with no additional staff to help) and negative interpersonal relationships (particularly with supervisors) may be promising avenues for further research targeting burnout reduction measures.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
Supporting information
Supporting information
Supporting informatiom
Hayes GM, LaLonde‐Paul DF, Perret JL et al. Investigation of burnout syndrome and job‐related risk factors in veterinary technicians in specialty teaching hospitals: a multicenter cross‐sectional study. J Vet Emerg Crit Care. 2020;30:18–27. 10.1111/vec.12916
Presented in abstract form at the 25th International Veterinary Emergency and Critical Care Symposium, Washington, DC, September 2019.
Funding information
Supported by the President's Council of Cornell Women Affinito‐Stewart Grant.
ENDNOTES
Qualtrics, Provo, UT.
Stata, College Station, TX.
REFERENCES
- 1. Aronsson G, Theorell T, Grape T, et al. A systematic review including meta‐analysis of work environment and burnout symptoms. BMC Public Health. 2017;17:264‐277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Poncet MC, Toullic P, Papazian L, et al. Burnout syndrome in critical care nursing staff. Am J Respir Crit Care Med. 2007;175:698‐704. [DOI] [PubMed] [Google Scholar]
- 3. Leiter MP, Durup J. The discriminant validity of burnout and depression: a confirmatory factor analytic study. Anxiety Stress Coping. 1994;7:357‐373. [Google Scholar]
- 4. Christensen JF, Levinson W, Dunn PM. The heart of darkness: the impact of perceived mistakes on physicians. J Gen Intern Med. 1992;7:424‐431. [DOI] [PubMed] [Google Scholar]
- 5. Poghosyan L, Clarke SP, Finlayson M, et al. Nurse burnout and quality of care: cross‐national investigation in six countries. Res Nurs Health. 2010;33:288‐298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Shoorideh FA, Ashktorab T, Yaghmaei F, et al. Relationship between ICU nurses' moral distress with burnout and anticipated turnover. Nurs Ethics. 2015;22:64‐76. [DOI] [PubMed] [Google Scholar]
- 7. Embriaco N, Papazian L, Kentish‐Barnes N, et al. Burnout syndrome among critical care healthcare workers. Curr Opin Crit Care. 2007;13:482‐488. [DOI] [PubMed] [Google Scholar]
- 8. Moore IC, Coe JB, Adams CL, et al. The role of veterinary team effectiveness in job satisfaction and burnout in companion animal veterinary clinics. J Am Vet Med Assoc. 2014;245:513‐524. [DOI] [PubMed] [Google Scholar]
- 9. Kimber S, Gardner DH. Relationships between workplace well‐being, job demands and resources in a sample of veterinary nurses in New Zealand. N Z Vet J. 2016;64:224‐229. [DOI] [PubMed] [Google Scholar]
- 10. Bursch B, Lloyd J, Mogil C, et al. Adaptation and evaluation of military resilience skills training for pediatric residents. J Med Educ Curric Dev. 2017;4:1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Manual. Palo Alto, CA: Consulting Psychologists Press; 1986:56‐102. [Google Scholar]
- 12. Connor KM, Davidson JR. Development of a new resilience scale: the Connor‐Davidson resilience scale (CD‐RISC). Depress Anxiety. 2003;18:76‐82. [DOI] [PubMed] [Google Scholar]
- 13. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361‐370. [DOI] [PubMed] [Google Scholar]
- 14. Munnangi S, Dupiton L, Boutin A, et al. Burnout, perceived stress and job satisfaction among trauma nurses at a level 1 safety‐net trauma center. J Trauma Nursing. 2018;25(1):4–13. [DOI] [PubMed] [Google Scholar]
- 15. Colville GA, Smith JG, Brierley J, et al. Coping with staff burnout and work‐related post traumatic stress in intensive care. Pediatr Crit Care Med. 2017;18:267‐273. [DOI] [PubMed] [Google Scholar]
- 16. Mealer M, Jones J, Newman J, et al. The presence of resilience is associated with a healthier psychological profile in intensive care unit (ICU) nurses: results of a national survey. Int J Nurs Stud. 2012;49:292‐299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Upton D, Mason V, Doran B, et al. The experience of burnout across different surgical specialties in the United Kingdom: a cross‐sectional survey. Surgery. 2012;151:493‐501. [DOI] [PubMed] [Google Scholar]
- 18. Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work‐life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172:1377‐1385. [DOI] [PubMed] [Google Scholar]
- 19. Maslach C, Jackson SE, Leiter MP. The MBI‐Human Sevices Survey. 4th ed Menlo Park, CA: Mind Garden; 2017:12‐24. [Google Scholar]
- 20. Perret J, Best C, Coe J, et al. Prevalence of mental health outcomes among a sample of Canadian veterinarians. J Am Vet Med Assoc. In press. [DOI] [PubMed] [Google Scholar]
- 21. Bianchi R, Schonfeld IS, Laurent E. Burnout‐depression overlap: a review. Clin Psychol Rev. 2015;36:28‐41. [DOI] [PubMed] [Google Scholar]
- 22. Bakker AB, Schaufeli WB, Demerouti E, et al. Using equity theory to examine the difference between burnout and depression. Anxiety Stress Coping. 2000;13:247‐268. [Google Scholar]
- 23. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283:516‐529. [DOI] [PubMed] [Google Scholar]
- 24. Salyers MP, Bonfils KA, Luther L, et al. The relationship between professional burnout and quality and safety in healthcare: a meta‐analysis. J Gen Intern Med. 2017;32:475‐482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Wilkinson H, Whittington R, Perry L, et al. Examining the relationship between burnout and empathy in healthcare professionals: a systematic review. Burn Res. 2017;6:18‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Chang BP, Carter E, Ng N, et al. Association of clinician burnout and perceived clinician‐patient communication. Am J Emerg Med. 2018;36:156‐158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Cowin LS, Johnson M, Craven RG, et al. Causal modeling of self‐concept, job satisfaction, and retention of nurses. Int J Nurs Stud. 2008;45:1449‐1459. [DOI] [PubMed] [Google Scholar]
- 28. Shanafelt T, Goh J, Sinsky C. The business case for investing in physician well‐being. JAMA Intern Med. 2018;177:1826‐1832. [DOI] [PubMed] [Google Scholar]
- 29. Huerkamp MJ. Job dynamics of veterinary professionals in an academic research institution. I. Retention and turnover of veterinary technicians. J Am Assoc Lab Anim Sci. 2006;45:16‐25. [PubMed] [Google Scholar]
- 30. Foster SM, Maples EH. Occupational stress in veterinary support staff. J Vet Med Educ. 2014;41:102‐110. [DOI] [PubMed] [Google Scholar]
- 31. Nienhaus A, Skudlik C, Seidler A. Work‐related accidents and occupational diseases in veterinarians and their staff. Int Arch Occup Environ Health. 2005;78:230‐238. [DOI] [PubMed] [Google Scholar]
- 32. Li CY, Sung FC. A review of the healthy worker effect in occupational epidemiology. Occup Med. 1999;49:225‐229. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information
Supporting informatiom