

Abstract
Background:
Objective dynamic assessments are central to the evaluation of facial rejuvenation treatments. This study used three-dimensional digital stereophotogrammetry to generate a quantitative dynamic assessment of facial strain and hyaluronic acid filler efficacy.
Methods:
Thirty women (aged 41 to 65 years) with moderate to severe bilateral nasolabial folds and marionette lines received Restylane Refyne, Restylane Defyne, or both, and were compared to a “younger” untreated group (n = 20; aged 25 to 35 years). Three-dimensional videos were collected at baseline and at day 42. Dynamic strain was analyzed at the marionette lines and nasolabial folds as subjects went from a neutral position through a series of facial expressions.
Results:
Baseline nasolabial folds and marionette lines showed statistically significant (p ≤ 0.05) differences in the level of stretch between younger and older untreated subjects, with higher stretch profiles observed in the older cohort. In the older cohort, filler treatment reduced peak strain (stretch) in the nasolabial folds and marionette lines compared with baseline across all tested expressions, resembling the youthful strain profile of the younger untreated control group. Treatment was well tolerated.
Conclusions:
Quantitative dynamic strain analysis is an innovative method for evaluating the dynamic face following dermal fillers and provides objective evidence that such treatment results in stretch levels resembling a younger phenotype in areas prone to the effects of facial aging. The strain reduction following filler treatment objectively conveys a dermal tightening effect, likely secondary to the volumization of treated areas. Additional studies will refine the technology and associated procedures to optimize quantitative dynamic strain analysis for treatment planning and patient outcome optimization.
CLINICAL QUESTION/LEVEL OF EVIDENCE:
Therapeutic, IV.
Facial expressions convey emotions and indicate characteristics such as age and quality of life.1,2 Facial rejuvenation treatments must maintain or enhance expressions for optimal outcomes,2 and therefore facial dynamics should be central to the evaluation of rejuvenation treatments to produce natural-appearing results. The perioral area, which is especially mobile and prone to significant rhytide formation and volume loss, specifically requires precise dynamic evaluation.3
Facial dynamics arise from the complex interplay of the skin’s physiomechanical properties, underlying soft tissue, skeletal volume, and muscle activity. Three-dimensional digital stereophotogrammetry (Canfield Scientific, Inc., Parsippany, N.J.) uses a Vectra (Canfield Scientific) three-dimensional camera system and algorithms to quantitatively analyze video of facial dynamic changes by tracking hundreds of points within a defined area of interest, such as the nasolabial folds. Results are presented as color-coded “heat-map” images and precisely quantitate the degree of stretch and compression (referred to as dynamic strain) of the skin surface as the subject moves from a neutral to maximum expression.3–6
The goal of this study was to evaluate whether quantitative analysis of facial dynamic strain can objectively measure aging-related facial changes and ascertain the effectiveness of dermal hyaluronic acid filler treatment of the nasolabial folds and marionette lines. The study further aimed to determine whether hyaluronic acid filler treatment of the nasolabial folds and marionette lines results in facial dynamics that resemble a younger phenotype. This study used the highly flexible hyaluronic acid gel fillers Restylane Refyne and Restylane Defyne (both from Q-Med AB/Galderma, Uppsala, Sweden), which are transparent, sterile, particulate gels composed of cross-linked sodium hyaluronate of bacterial origin and are both approved in the United States for the treatment of moderate to severe facial wrinkles and folds.7–12 This dynamic strain analysis is part of a larger study of Restylane Refyne and Restylane Defyne, which is reported separately [registered under the name “Emervel for the Correction of Lower Face Wrinkles & Folds,” ClinicalTrials.gov registration number NCT02718040 (https://clinicaltrials.gov/ct2/show/NCT02718040)].13
PATIENTS AND METHODS
The protocol was approved by a central institutional review board (Quorum Review IRB, Columbia, Md.). The study was conducted according to the International Conference on Harmonization and Good Clinical Practice principles, the U.S. Food and Drug Administration Code of Federal Regulations, and federal and local regulatory requirements. Figure 1 summarizes the study design.
Fig. 1.
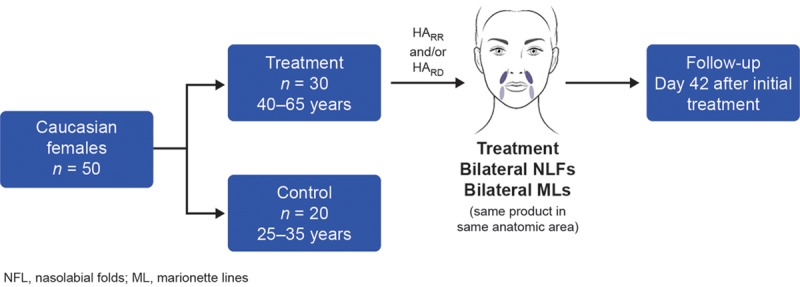
Summary of study design. HARR, Restylane Refyne; HARD, Restylane Defyne.
Inclusion and Exclusion Criteria
Two cohorts were enrolled. The “older” group (aged 41 to 65 years) sought bilateral treatment for moderate or severe nasolabial folds (Wrinkle Severity Rating Scale: moderate, 2 to 3; severe, 3 to 4) and marionette lines (Wrinkle Assessment Scale: moderate, 2 to 3; severe, 3 to 4). Subjects received Restylane Refyne, Restylane Defyne, or both, according to the licensed indication. A “younger” untreated group (aged 25 to 35 years) served as “youthful phenotype” controls. All subjects gave written consent to participate. Subjects of childbearing potential agreed to use contraception during and for 30 days after the study. The exclusion criteria included subjects with nasolabial folds or marionette lines that required other treatments (e.g., lasers or chemical peels) and those who had undergone facial surgery, tissue-augmenting therapy or contouring with any filler, revitalization treatment with neurotoxin or laser or light, mesotherapy, chemical peeling, or dermabrasion below the zygomatic arch within 6 months before the study.
Treatment
Treated subjects received bilateral Restylane Refyne, Restylane Defyne, or both depending on the severity of nasolabial folds and marionette lines. If subjects received both fillers, Restylane Refyne or Restylane Defyne was injected into separate anatomical locations. Restylane Refyne and Restylane Defyne were injected using a needle in the mid to deep dermis using either serial puncture or linear threading at the investigator’s discretion, with optional additional local anesthesia. Treatment location was standardized (medial to the fold) to avoid confounding posttreatment strain assessments. Subjects were treated to optimal correction as agreed by the investigator and subject. Total recommended injection volumes for each treatment session were up to 2 ml for each nasolabial fold and 1 ml for each marionette line. A touch-up treatment could be performed at day 15, for optimal correction.
Three-Dimensional Digital Stereophotogrammetry
Full details of three-dimensional digital stereophotogrammetry are published elsewhere.3,4,6 In previous studies, white foundation and black speckle makeup were applied to the subject’s face. The subject then made a facial expression and the digital camera tracked and measured the movement of the speckles across the entire face and, specifically, in areas of interest, such as nasolabial folds and marionette lines. This study used a novel, speckle-free, dynamic three-dimensional digital technology developed by Canfield Scientific. Three-dimensional images were collected at baseline for both control and treated subjects, and at day 42 for treated subjects (Fig. 2). [See Video 1 (online), which shows three-dimensional video imaging (stereophotogrammetry) of facial dynamics showing heat-map images of the degree of dynamic strain on the skin surface as the subjects move from a neutral to a maximum expression. A comparative example of two-dimensional videos and three-dimensional dynamic strain video imaging on day 1 and day 42 in an older treated subject showing a closed smile at maximum contraction is shown. See Video 2 (online), which shows three-dimensional video imaging (stereophotogrammetry) of facial dynamics showing heat-map images of the degree of dynamic strain on the skin surface as the subjects move from a neutral to a maximum closed smile expression. An older subject is shown at day 1 and day 42, in comparison to a younger, untreated, subject at day 1.] Central imaging analysis and reporting of dynamic strain was conducted by Canfield Scientific. Computer software combined left and right sides for both nasolabial fold and marionette line analyses. Strain was reported for four expressions as the percentage change as each subject went from rest (neutral position) to fully expressing closed smile (mouth closed), open smile (showing teeth), lip pursing (kissing position), and grimace (pulling down corners of mouth with lips together). Strain results were presented as positive (surface stretch) or negative strain (surface compression) along two principal axes:
Fig. 2.
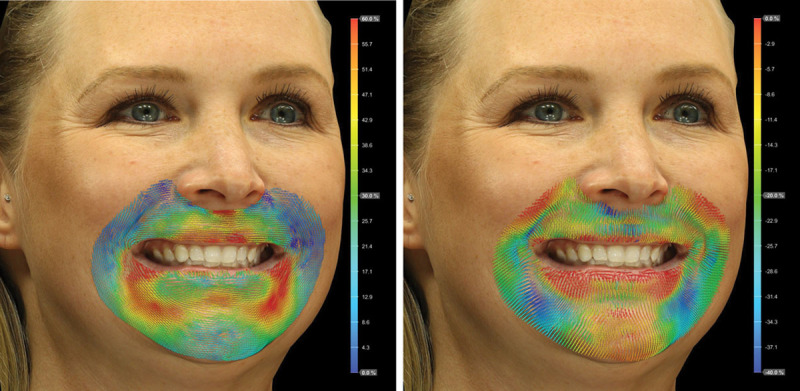
Three-dimensional digital stereophotogrammetry. The three-dimensional digital stereophotogrammetry system uses computer-vision technology to track facial surface deformations for a given area of interest, through an expression, to quantify stretch (percentage) and compression (percentage). (Left) Positive strain is an indication of surface stretch, with red indicating areas with the greatest degree of stretch and blue indicating areas with the least amount of stretch. (Right) Negative strain is an indication of surface compression, with blue indicating areas with the greatest degree of compression and red indicating areas with the least amount of compression. (Courtesy of Canfield Scientific, Inc.)
Video 1. This video shows three-dimensional video imaging (stereophotogrammetry) of facial dynamics showing heat-map images of the degree of dynamic strain on the skin surface as the subjects move from a neutral to a maximum expression. A comparative example of two-dimensional videos and three-dimensional dynamic strain video imaging on day 1 and day 42 in an older treated subject showing a closed smile at maximum contraction is shown.
Video 2. This video shows three-dimensional video imaging (stereophotogrammetry) of facial dynamics showing heat-map images of the degree of dynamic strain on the skin surface as the subjects move from a neutral to a maximum closed smile expression. An older subject is shown at day 1 and day 42, in comparison to a younger, untreated, subject at day 1.
Major strain (stretch): Measurement axis with the greater value.
Minor strain (typically compression): Measurement axis with the lesser value.
Each strain parameter was reported as percentage change during expression: mean, median, peak (95th percentile), and minimum (fifth percentile). A post hoc global dynamic assessment analysis was conducted to estimate the average strain for each expression.
Statistical Analyses
Mean changes from baseline to day 42 for the four strain metrics for each expression were examined using paired two-tailed t tests. Baseline strain metrics were compared between the treated cohort and untreated controls using a two-sample two-tailed t test. A significant p value was defined as p ≤ 0.05. The analysis focused on peak strain, which conveys maximum strain, the most clinically significant metric.
Safety
Adverse events are reported in detail elsewhere.13 Treatment-emergent adverse events were collected throughout the study. Predefined injection-related events are expected following dermal aesthetic procedures and were not captured as adverse events unless ongoing 14 days after treatment.
RESULTS
Demographics and Subject Disposition
Thirty subjects were enrolled in the treatment group and 20 subjects were enrolled in the control group. Table 1 summarizes the demographics. All enrolled subjects completed the study. An equal number of subjects received Restylane Refyne, Restylane Defyne, or both. Overall, 27 subjects received touch-up treatment.
Table 1.
Demographics and Baseline Characteristics
| Variable | Control | Treated |
|---|---|---|
| No. of subjects | 20 | 30 |
| Age, yr | ||
| Mean ± SD | 28.7 ± 3.01 | 55.0 ± 6.01 |
| Range | 25–35 | 41–65 |
| Female sex, % | 100 | 100 |
| Caucasian, % | 100 | 100 |
| BMI, kg/m2 | ||
| Mean ± SD | 23.68 ± 2.919 | 24.92 ± 2.874 |
| Range | 18.9–29.8 | 20.6–29.9 |
BMI, body mass index.
Peak Metric Analysis Reveals Overall Improved Peak Metrics following Hyaluronic Acid Treatment
Baseline peak results showed statistically significant variation in the degree of strain (stretch, p ≤ 0.05), with overall higher peak values observed in the older cohort before treatment compared to the younger controls. There were a few parameters in which the younger cohort had either a higher observed peak strain (stretch) or there was no statistically significant difference between the two groups (Fig. 3). At baseline, most expressions showed higher peak compression values in the controls compared with the older subjects.
Fig. 3.
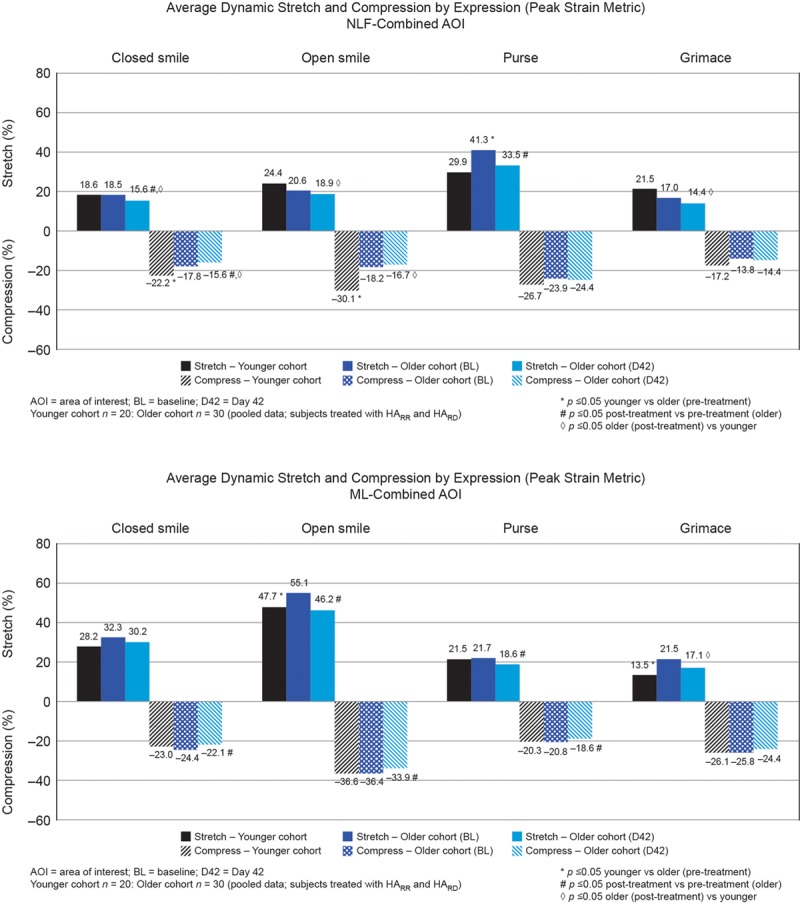
Objective facial dynamic results (three-dimensional stereophotogrammetry) by individual expressions and (above) nasolabial fold (NLF) and (below) marionette line (ML) areas of interest (AOI). HARR, Restylane Refyne; HARD, Restylane Defyne.
Treatment with Restylane Refyne, Restylane Defyne, or both generally reduced the degree of stretch and compression in most facial areas and expressions. The peak strain metric analyses specifically demonstrated that treatment with Restylane Refyne, Restylane Defyne, or both resulted in statistically significant reductions (p ≤ 0.05) in peak strain (stretch) values compared to baseline in areas prone to volumetric effects of facial aging such as nasolabial folds and marionette lines (Fig. 3). Three parameters—nasolabial folds, pursed; marionette lines, open smile; and upper lip, pursed (data not shown)—showed no statistically significant difference between controls and treated women at day 42, despite the peak strain (stretch) being statistically significantly different between the two groups before treatment, with higher observed peak strain (stretch) means in the older pretreatment cohort.
Global Dynamic Assessment Metric Analysis Confirms Overall Improved Peak Metrics following Hyaluronic Acid Treatment
The global dynamic assessment metric estimated the average strain for each of the four facial expressions. Peak dynamic stretch was generally higher in the younger controls than in older women at baseline (before treatment, p ≤ 0.05) for each facial area (data not shown). The older cohort (after treatment) showed statistically significant higher peak stretch (p ≤ 0.05) specifically in the marionette lines (Fig. 4). There were no statistically significant differences in marionette line compression metrics between groups before treatment. Peak global dynamic assessment in the nasolabial folds showed a trend toward higher stretch in older untreated subjects at baseline. Statistically significant different degrees of peak global dynamic assessment compression of the nasolabial folds (p ≤ 0.05) were observed, with higher peak values in the controls compared with the pretreatment and posttreatment older cohort.
Fig. 4.
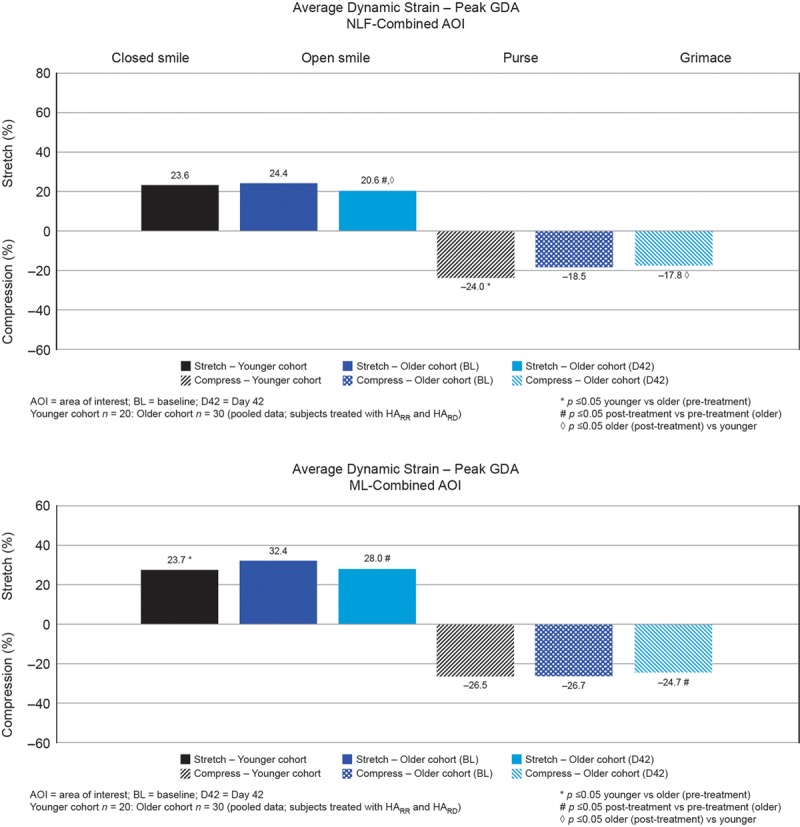
Objective facial dynamic global dynamic assessment (GDA) results (three-dimensional digital stereophotogrammetry) by (above) nasolabial fold (NLF) and (below) marionette line (ML) areas of interest (AOI). HARR, Restylane Refyne; HARD, Restylane Defyne.
Treatment reduced global dynamic assessment peak strain (stretch and compression), although many of these differences were not statistically significant (data not shown). Statistically significant differences in degrees of peak stretch (p ≤ 0.05) were observed for the nasolabial fold and marionette lines after treatment compared with baseline. Bilateral treatment of the nasolabial folds and marionette lines decreased peak global dynamic assessment stretch to levels that were similar to those of the younger controls (Fig. 4). In Figures 5 and 6, the day-42 strain map for the representative older subject demonstrates less stretch following treatment [see Video 1 (online)]. When comparing the day-42 strain map to the younger untreated subjects, the levels of stretch resemble a younger phenotype, which is consistent with the objective, quantitative global dynamic assessment results, particularly in the marionette line region [see Video 2 (online)].
Fig. 5.
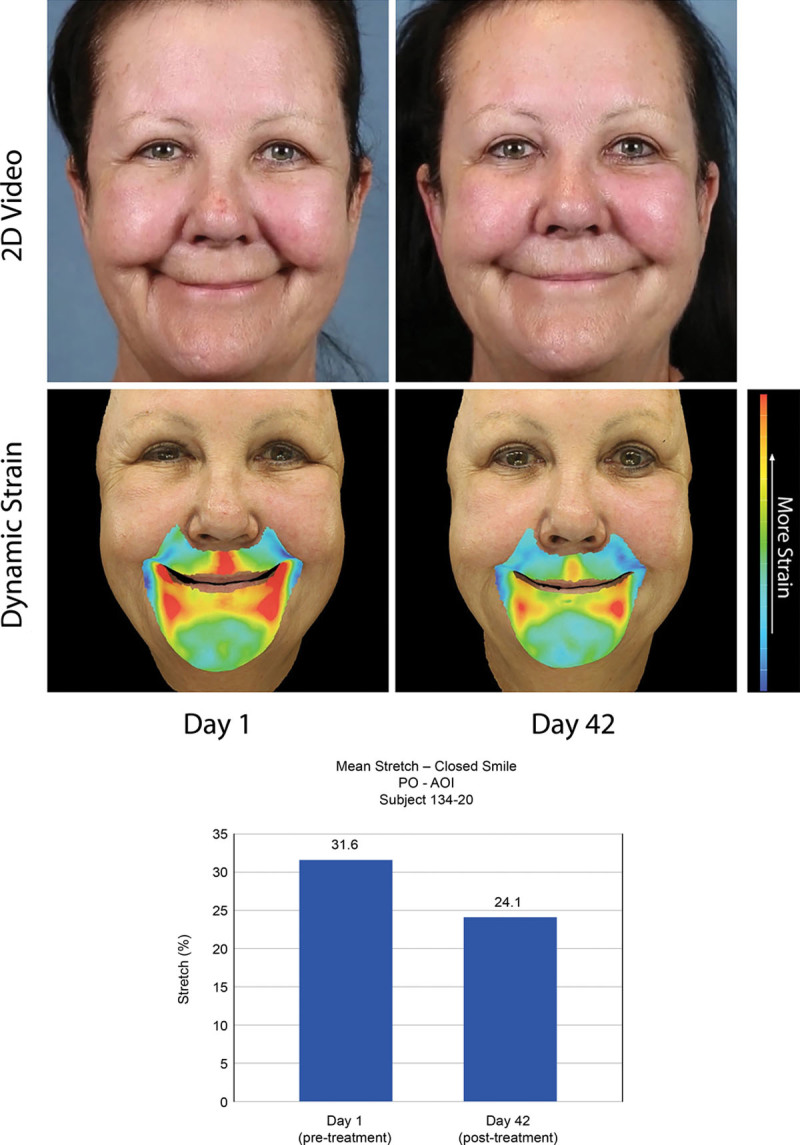
Objective facial dynamic results (three-dimensional stereophotogrammetry) in representative subjects. Subject ID 134-20, aged 58 years, with closed smile (maximum contraction), treated with Restylane Defyne. Total injection volume in nasolabial folds and marionette lines = 4.4 ml (nasolabial fold = 2.5 ml; marionette line = 1.9 ml).
Fig. 6.
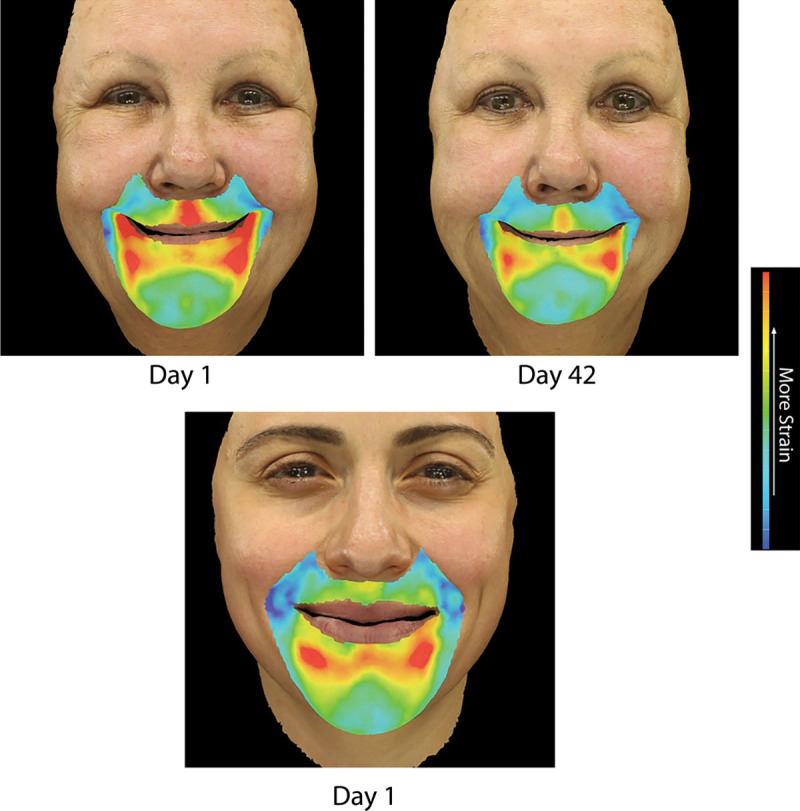
The day-42 strain map for the representative older subject shows less stretch after treatment. When comparing the day-42 strain map to the younger untreated subjects, the levels of stretch resembles a younger phenotype, which is consistent with the objective, quantitative global dynamic assessment results, particularly in the marionette line region. (Above) Subject ID 134-20, aged 58 years, with closed smile (maximum contraction), treated with Restylane Defyne. Total injection volume in nasolabial folds and marionette lines = 4.4 ml (nasolabial fold = 2.5 ml; marionette line = 1.9 ml). Day 1 and day 42. (Below) Subject ID 134-01, aged 35 years, with closed smile (maximum contraction) on day 1 and no treatment (younger cohort).
Safety
Full safety results are reported elsewhere.13 No serious adverse events or treatment-emergent adverse events leading to permanent discontinuation occurred. No treatment-emergent adverse events were reported for subjects treated with Restylane Refyne. Two subjects treated with Restylane Defyne experienced a treatment-emergent adverse event; both were mild and assessed as not related to the study treatment. Twenty-nine subjects experienced at least one mild to moderate injection-related event, which resolved within 2 weeks of treatment.
DISCUSSION
Facial expressions convey emotions that promote and modulate interpersonal relationships, self-esteem, and quality of life.1,2 Therefore, facial dynamic assessment should be central to the evaluation of facial rejuvenation treatments.2 Specifically, the perioral region is subject to significantly increased dynamic strain and volume loss.4,14 In addition to subjective measurements, it is important to objectively define the dynamic strain patterns (stretch and compression) of the aging face phenotype and to evaluate objectively and quantitatively the clinical improvements in facial dynamic strain after treatment with hyaluronic acid fillers.14 By defining the dynamic strain patterns of younger phenotypes and comparing these to older phenotypes before treatment, clinicians can better understand baseline age-related differences in facial dynamic strain patterns and, furthermore, discern whether treatment with hyaluronic acid fillers improves facial dynamic strain profiles to resemble younger patients.
First, this study confirmed that three-dimensional digital stereophotogrammetry gives a precise, quantitative assessment of facial soft-tissue dynamics, with positive strain corresponding to dermal stretch and negative strain reflecting dermal compression, metrics that translate the complex interplay of the underlying subcutaneous tissues to the skin.3–6 Three-dimensional speckle tracking stereophotogrammetry has been used in basic research and in the clinical assessment of neurotoxin efficacy for aesthetic and neuromuscular indications.5,6,14 This technology is sufficiently sensitive to differentiate the effects of onabotulinumtoxinA, abobotulinumtoxinA, and incobotulinumtoxinA.5 The technique further showed that abobotulinumtoxinA plus a filler (Restylane Silk) significantly reduces strain in the perioral region, correlating with high patient satisfaction during follow-up of up to 90 days.14
Second, this study demonstrates that markerless three-dimensional digital stereophotogrammetry can differentiate between older and younger phenotypes in the nasolabial fold and marionette line regions, two areas that are especially prone to volumetric effects with advancing age. Stereophotogrammetry characterizes the dynamic face as a state of simultaneous stretch and compression, for all facial regions and expressions tested in older and younger people. This advanced technology can further discriminate a treatment effect following hyaluronic acid injection, and uniquely elucidated that this treatment restores a younger phenotype in volume-depleted areas. This work is consistent with findings from other studies showing that Restylane Refyne and Restylane Defyne are effective at treating moderate to severe facial wrinkles, folds, and soft-tissue contour deformities.7–12
Importantly, our study confirms previous investigations demonstrating that certain elements of the dynamic face are characterized by significant age-related differences.4 Hsu and colleagues showed that subjects older than 40 years are subject to a statistically significant increase in stretch in the perioral region during lip pursing compared with younger people (58.4 percent and 33.8 percent respectively; p = 0.015). The nasolabial folds stretch (61.6 percent and 32.9 percent, respectively; p = 0.007), and overall strain (61.6 percent and 32.9 percent, respectively; p = 0.007) metrics showed differences in the older group compared with the younger group.4 In our study, the nasolabial fold and marionette line regions demonstrated statistically significant higher stretch in older subjects at baseline compared with the controls. Treatment with Restylane Refyne, Restylane Defyne, or both significantly reduced the observed peak strain levels in most expressions. Three parameters—nasolabial folds, pursed; marionette lines, open smile; and upper lip, pursed—showed no statistically significant differences between untreated controls and the treated cohort at day 42, as these metrics decreased after treatment compared to baseline in the treated cohort. The lack of effect on marionette lines, open smile probably reflects the lack of perioral treatment in areas other than nasolabial folds and marionette lines. The relatively small number of people included in this study may also contribute to the lack of a statistically significant difference in other outcomes.
Global dynamic assessment analyses further confirmed these findings, showing statistically significant differences in peak strain (stretch and compression) for nasolabial folds and marionette lines in older subjects after treatment versus baseline. Global dynamic assessment analyses may simplify how the dynamic face is objectively characterized by averaging strain for individual expressions, providing a global measure of dynamic strain. Although global dynamic assessment results were similar to the more detailed evaluations of individual expressions, stretch and compression as individual parameters may not optimally characterize the dynamic face for specific expressions and, therefore, global dynamic assessment may be more appropriate. This principle of individual expression versus global expression metrics will be examined further in additional studies.
This study was not designed to identify the underlying reason(s) for age-related differences in dynamic strain that may include volumetric differences, muscle atrophy or imbalance, subcutaneous tissue inconsistency, and variability in the predominant dynamic vector(s). The significant effect produced in the marionette line region is consistent with previous observations that age-related changes in the marionette lines are more dependent on volume loss than age-related changes of the nasolabial fold region.14 The latter is characterized by a more complex interplay of midfacial anatomical factors. The posttreatment reduction in stretch and compression objectively reflects a dermal tightening effect that reinforces prior subjective outcome assessments. We hypothesize that this tightening effect is likely secondary to volume augmentation of treated areas, perhaps in combination with a distal effect on facial musculature activity, and demonstrates that this results in a more youthful facial phenotype.
This study is subject to several limitations. Because of the small sample size, the probability of a nonsignificant p value is higher than would be observed in a higher powered study. The absence of a statistically significant difference does not necessarily indicate that the means were statistically the same. The observations will be confirmed in a larger, more high-powered study. Furthermore, the study enrolled only Caucasian women, who are known to show an overall greater degree of stretch in their lower face than men when pursing their lips.4 The study should therefore be repeated in people of varied ethnic backgrounds, in both sexes, and in people with different body mass indexes to optimize dynamic facial analyses and filler treatments to the face. In addition, the analysis used “defined expressions” to create a wide dynamic range and thus future work may incorporate more natural and fluid expressions and correlate the findings to, for example, changes in quality of life and self-esteem.
Moreover, the benefits of Restylane Refyne and Restylane Defyne persist for at least 6 months to 1 year.7,9,10 Therefore, studies with a longer follow-up may also be insightful for gaining knowledge into the long-term benefits of these interventions and for establishing ideal times for repeated treatment. Although subjects were treated in this study with Restylane Refyne, Restylane Defyne, or both, the small number of subjects prevented filler-specific analyses, and additional work will be required to generate conclusions about the effects of specific fillers in different regions of the face and in relation to subject-specific anatomy.
Finally, additional clinical developments are needed to explore whether a three-dimensional dynamic capture system that uses a single dynamic parameter encompassing stretch and compression may be more clinically relevant and reliable in characterizing the dynamic face. Future technological development and additional clinical studies will help clarify whether combining volumetric and surface-tracking capabilities can optimize clinical utility and help aesthetic physicians use a dynamic capture system to aid in treatment planning, standardization, and optimization of clinical outcomes, and to enhance training.
CONCLUSIONS
This study validates that speckle-free three-dimensional digital stereophotogrammetry can precisely quantify the dynamic face as simultaneous stretch and compression metrics in the nasolabial folds and marionette lines, regardless of facial expression or age. Globally, the nasolabial fold and marionette line regions demonstrated statistically significant higher peak strain (stretch) in older subjects at baseline compared with a younger cohort. Restylane Refyne, Restylane Defyne, or both produced quantified improvement on dynamic stretch and compression profiles, especially in the marionette line region, thereby restoring dynamic strain to resemble a younger phenotype. The reduced peak strain (stretch and compression) provides objective, quantitative support for a clinical tightening effect on the dermis, likely secondary to increased volume after hyaluronic acid filler placement. Further studies in a larger, more diverse population will be conducted to expand on these significant findings.
PATIENT CONSENT
Patients provided written informed consent for the use of their images.
ACKNOWLEDGMENTS
Galderma Laboratories, L.P., Fort Worth, Texas, funded the study. Editorial support was provided by Mark Greener and MedSense Ltd, funded by Galderma. The authors wish to thank Premier Research International LLC for managing the clinical study and providing statistical analysis support. The authors would also like to thank Oleg Bisker from Canfield Scientific, Inc., for technical expertise and input.
Footnotes
Presented at Plastic Surgery The Meeting 2017, Annual Meeting of the American Society of Plastic Surgeons, in Orlando, Florida, October 6 through 10, 2017; and the 2017 American Society for Dermatologic Surgery Annual Meeting, in Chicago, Illinois, October 5 through 8, 2017.
Disclosure: Dr. Percec is a paid consultant and speaker for Galderma. Drs. Bertucci and Solish are paid consultants, speakers, and clinical trial investigators for Galderma. Mr. Wagner and Drs. Nogueira and Mashburn are employees of Galderma Laboratories, L.P.
Related digital media are available in the full-text version of the article on www.PRSJournal.com.
A “Hot Topic Video” by Editor-in-Chief Rod J. Rohrich, M.D., accompanies this article. Go to PRSJournal.com and click on “Plastic Surgery Hot Topics” in the “Digital Media” tab to watch.
REFERENCES
- 1.Charles Finn J, Cox SE, Earl ML. Social implications of hyperfunctional facial lines. Dermatol Surg. 2003;29:450–455. [DOI] [PubMed] [Google Scholar]
- 2.Michaud T, Gassia V, Belhaouari L. Facial dynamics and emotional expressions in facial aging treatments. J Cosmet Dermatol. 2015;14:9–21. [DOI] [PubMed] [Google Scholar]
- 3.Lin Y, Lin H, Lin Q, et al. A novel three-dimensional smile analysis based on dynamic evaluation of facial curve contour. Sci Rep. 2016;6:22103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hsu VM, Wes AM, Tahiri Y, Cornman-Homonoff J, Percec I. Quantified facial soft-tissue strain in animation measured by real-time dynamic 3-dimensional imaging. Plast Reconstr Surg Glob Open 2014;2:e211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wilson AJ, Chang B, Taglienti AJ, et al. A quantitative analysis of onabotulinumtoxinA, abobotulinumtoxinA, and incobotulinumtoxinA: A randomized, double-blind, prospective clinical trial of comparative dynamic strain reduction. Plast Reconstr Surg. 2016;137:1424–1433. [DOI] [PubMed] [Google Scholar]
- 6.Wilson AJ, Chin BC, Hsu VM, Mirzabeigi MN, Percec I. Digital image correlation: A novel dynamic three-dimensional imaging technique for precise quantification of the dynamic rhytid and botulinum toxin type a efficacy. Plast Reconstr Surg. 2015;135:869e–876e. [DOI] [PubMed] [Google Scholar]
- 7.Rzany B, Bayerl C, Bodokh I, et al. Efficacy and safety of a new hyaluronic acid dermal filler in the treatment of moderate nasolabial folds: 6-month interim results of a randomized, evaluator-blinded, intra-individual comparison study. J Cosmet Laser Ther. 2011;13:107–112. [DOI] [PubMed] [Google Scholar]
- 8.Ascher B, Bayerl C, Brun P, et al. Efficacy and safety of a new hyaluronic acid dermal filler in the treatment of severe nasolabial lines: 6-month interim results of a randomized, evaluator-blinded, intra-individual comparison study. J Cosmet Dermatol. 2011;10:94–98. [DOI] [PubMed] [Google Scholar]
- 9.Cartier H, Trevidic P, Rzany B, et al. Perioral rejuvenation with a range of customized hyaluronic acid fillers: Efficacy and safety over six months with a specific focus on the lips. J Drugs Dermatol. 2012;11(Suppl):s17–s26. [PubMed] [Google Scholar]
- 10.Rzany B, Cartier H, Kestemont P, et al. Full-face rejuvenation using a range of hyaluronic acid fillers: Efficacy, safety, and patient satisfaction over 6 months. Dermatol Surg. 2012;38:1153–1161. [DOI] [PubMed] [Google Scholar]
- 11.Baumann L, Weiss RA, Grekin S, et al. Comparison of hyaluronic acid gel with (HARDL) and without lidocaine (HAJUP) in the treatment of moderate-to-severe nasolabial folds: A randomized, evaluator-blinded study. Dermatol Surg. 2018;44:833–840. [DOI] [PubMed] [Google Scholar]
- 12.Fagien S, Monheit G, Jones D, et al. Hyaluronic acid gel with (HARRL) and without lidocaine (HAJU) for the treatment of moderate-to-severe nasolabial folds: A randomized, evaluator-blinded, phase III study. Dermatol Surg. 2018;44:549–556. [DOI] [PubMed] [Google Scholar]
- 13.Solish N, Bertucci V, Percec I, Wagner T, Nogueira A, Mashburn J.Dynamics of hyaluronic acid fillers formulated to maintain natural facial expression. J Cosmet Dermatol. 2019;18:738–746. [DOI] [PMC free article] [PubMed]
- 14.Chang CS, Chang BL, Lanni M, Wilson AJ, Beer J, Percec I. Perioral rejuvenation: A prospective, quantitative dynamic three-dimensional analysis of a dual modality treatment. Aesthet Surg J. 2018;38:1225–1236. [DOI] [PubMed] [Google Scholar]