

Abstract
Chronic sleep deprivation may worsen many medical and mental health conditions, causing difficulty in the ability to function at work. Job stress may be a factor that directly correlates with the poorer sleep quality of nurses from different departments in a general hospital. However, epidemiological evaluations of sleep problems among community nurses in China are scarce, and an association between sleep problems and occupational stress has not been investigated. This study investigated the association between nurses’ job stress and sleep quality in a community hospital in China. This cross-sectional study was conducted from September to November 2017 and involved 180 nurses who had worked for more than 1 year in 12 community hospitals. The Job Stress Questionnaire was administered to evaluate occupational stress. The Pittsburgh Sleep Quality Index was used to evaluate sleep disorder status. Logistic regression was performed to investigate the association between job stress and sleep disorder among these community nurses in China. For the 155 nurses who completed the study, the job stress score was 58 ± 18, and 72 nurses (46%) had a Pittsburgh Sleep Quality Index (PSQI > 7). The type of nurse contract and total job stress scores were related to sleep disturbances within the previous month. The job stress scores were negatively associated with sleep quality; in other words, the higher the job stress scores were, the worse the quality of sleep. The logistic regression analysis showed that the type of nurse contract and self-reported job stress were significant factors affecting sleep quality. Sleep disturbances in nurses were highly associated with job difficulty factor, doctor-patient relationships, psychosomatic state, environment or events, promotion or competition and total pressure scores. Sleep problems were prevalent among clinical nurses in community hospitals in China. Occupational stress negatively affects sleep quality in Chinese community nurses; the higher the stress is, the worse the sleep quality.
Keywords: community nurses, correlation, occupational stress, sleep quality
1. Introduction
The topic of sleep has been given considerable attention as an important reference guide of psychological health.[1,2] Chronic sleep deprivation may worsen many medical and mental health conditions, causing difficulty in the ability to function at work. The American Academy of Sleep Medicine has declared that 30% to 35% of the general adult population in the United States have brief symptoms of insomnia. Insomnia is also common in nurses due to long work shifts. It has been reported that 35.5% of Chinese nurses suffer from sleep disorders.[3,4] Nurses may be required to maintain all-night vigils and work several consecutive 12 hour shifts. Nocturnal shift work is a primary cause of sleep disorders, and 57% of night shift nurses reportedly have a sleep disorder.[5] Long-term sleep deprivation may lead to serious thought retardation, memory loss, slow response, fatigue, irritability, and even potential depression and suicidal ideation.[6,7] Furthermore, night shift work can affect not only nurses’ personal health but also the quality of their work and their patients’ psychological health and treatment, even result in errors and accidents.[8,9] Previous studies suggest that job stress may be a factor that directly correlates with the poorer sleep quality of nurses from different departments in a general hospital.[10,11] The pressures of the nursing occupation include heavy responsibility and high risk, with constant encounters with disease, trauma, and even death.[12] A chronic state of job stress can lead to lassitude, anxiety, depression, and other psychological problems that affect sleep quality.[13,14]
Preventing and controlling occupational injuries are concerns in the field of public health. [15] In recent years, the occupational health and safety committees at medical institutions have emphasized that it is important for all medical staff should comply with legal and company requirements.[16] Due to the uncertainty and particularity of their work, the expectations of medical workers, the profession, and society can result in unhealthy behaviors and lifestyles, including lack of sleep, standing for long periods of time, lack of exercise, and excessive work pressure. [17] It has been reported that sleep disorders are prevalent among Chinese clinical nurses in general hospitals, and occupational stress can lead to clinical sleep problems.[18] However, epidemiological evaluations of sleep problems among community nurses in mainland China are scarce, and an association between sleep problems and occupational stress has not been investigated. Types of nurse contracts in public hospitals (including community hospitals) in China are divided into two types: authorized strength nurses and contract nurses. Furthermore, contract nurses are divided into those with fixed contracts and those without fixed contracts. Authorized strength nurses’ personal monthly income and job stability are usually higher than contract nurses’ personal monthly income and job stability. Compared with nurses in first level, second level, and third level hospitals, community nurses have lower career incentives, insufficient labor, tedious tasks, and low wages.[19] Compared with the income of doctors of the same age, the personal monthly income of nurses is generally much lower; personal monthly income is also a factor influencing the sleep quality of nurses.[10,19]
Most research on the sleep quality of nurses comes from tertiary level hospitals in China. The order of departments that may lead to nurses’ sleep disturbance most easily is as follows: ICU, emergency department, and department of gynecology and obstetrics.[10] A relation was observed between the levels of stress and the sleep quality of nurses who work in different departments; the ICU and the emergency department are generally connected with higher job stress and poor sleep quality than the internal medicine wards are.[20,21] Nurses working at community hospitals are therefore more likely to experience lower wages for their efforts, leading to increased stress and sleep disorders. The present study investigated an association between sleep quality and job stress in community hospitals in mainland China.
2. Subjects and methods
2.1. Study design
A cross-sectional study design was used.
2.2. Participant demographic
All nurses who worked in community hospitals in Chengdu, China, between September and November 2017 were initially considered for inclusion in this study. Twelve community hospitals in the city of Chengdu with inpatient departments were randomly selected. During the pre-investigation, there were 17 to 25 nurses engaged in clinical nursing in each community hospital, 15 nurses were selected from each community hospital as participants, and a total of 180 nurses were invited to participate in the survey.
To be included in the study, each nurse had a signed labor contract with a community hospital, a nurse's license, current practice in clinical care, and one or more years of work experience in their current job position. Nurses were excluded if they were on leave for illness, marriage, maternity, or other personal affairs; had sleep affected by disease, alcohol, or pharmacotherapy; had a family history of sleep disorders; or were not willing to participate in the survey.
Members of the research team interviewed each participant at their respective work location. The investigator explained the purpose, significance, and relevant instructions before administering the questionnaire, and then the respondents completed the questionnaires by themselves.
2.3. Data collection
For data collection, three questionnaires were given to each participant: a demographic survey, the Job Stress Questionnaire, and the Pittsburgh Sleep Quality Index (PSQI). For the demographic data, each participant provided a self-report of his or her formal education history, marital status, health status, years of work experience, work shift, job title, manager position, type of nurse contract, monthly personal income and monthly family income.
The database was built using EpiData3.1 software (EpiData– Comprehensive Data Management and Basic Statistical Analysis System, EpiData Association, Odense, Denmark). The data entry was checked by two people, and incomplete questionnaires (>20% missing data) were eliminated.
2.3.1. Demographic data
The demographic data collected were self-designed after a literature review. According to the results of the survey, the demographic data were classified into the following categories: formal education history (polytechnic school, college, undergraduate), marital status (unmarried, married, divorced, widowed), health status (healthy, ill), work shift (day, night), job title (registered nurse, primary nurse, intermediate nurse, deputy senior), manager position (no, nurse group leader, head nurse), type of nurse contract (no fixed contract, fixed contract, authorized strength contract), years of work experience, monthly personal income and monthly family income.
2.3.2. Job stress questionnaire
The Job Stress Questionnaire (JSQ) was designed to measure the perceptions of job-related stress and the sources of stress in the workplace, as proposed by previous studies.[22] Briefly, this questionnaire comprises 7 parts (23 items) as follows: job strength (5 items); job difficulty factor (4 items); doctor-patient relationships (3 items); psychosomatic state (4 items); disgusting environment or events (3 items); interpersonal relationships (2 items); and promotion or competition ( items). The items were measured using a five-point Likert-type scale (1 through 5), with higher values indicating greater distress. The scores of the seven parts were summed to obtain a total score of stress. The coefficient of internal consistency was Cronbach's α = 0.778. [22]
2.3.3. Pittsburgh sleep quality index (PSQI)
The Chinese version of the Pittsburgh Sleep Quality Index (PSQI) was used to assess subjective sleep quality. The PSQI was prepared by Liu et al,[23] who translated and verified its reliability and validity. The coefficient of internal consistency was Cronbach's α = 0.845.[23] The PSQI is a scored 18-item self-reported questionnaire with commentary items to characterize sleep patterns and quantify sleep quality over the previous month. The 18 items were grouped into seven clinically derived component scores: sleep quality; sleep latency; sleep duration; habitual sleep efficiency; sleep disturbance; usage of sleep medication; and daytime dysfunction. Each component was scored on a four-point Likert-type scale (0 to 3), weighted equally with higher scores indicating worse sleep quality. The seven component scores were summed to obtain a total score ranging from 0 to 21. Chinese scholars have confirmed that a PSQI ≤ 7 as the reference threshold for sleep quality problems is more suitable for Chinese individuals.[23] Because the subjects of this study were Chinese, we used a PSQI ≤ 7 instead of PSQI < 5. Thus, in the present study, normal sleep quality was defined as a PSQI ≤ 7, and poor sleep quality was defined as a PSQI > 7.
2.4. Statistical analysis
SPSS 20.0 software (IBM, Armonk, NY) was used for the statistical analyses. Quantitative data such as the JSQ score and PSQI score are presented as the arithmetic mean and standard deviations and compared with the t-test, analysis of variance, or nonparametric test among different groups. Qualitative data such as the proportion of PSQI > 7 are represented by percentages. Multiple logistic regression was performed to estimate the association between the sleep quality (poor sleep quality, PSQI > 7) and job stress scores, and the relevant factors (such as age, education, marital status, health status, work shift, years of work experience, job title, manager position, contract and income) that are considered to probably be associated with sleep quality were entered with a forward method that introduced the variables into the model; the variable was deleted if it had been in the model with P > .05 after a new variable was pulled in the model. The odds ratios and 95% confidence intervals (CIs) were calculated by logistic regression. A P value < .05 was considered statistically significant.
3. Results
3.1. Subjects
Of the 180 subjects, 15 were excluded due to missing items on the questionnaire, and 10 were excluded due to inconsistency. Thus, 155 subjects composed the final study group. All 155 subjects were women, ranging in age from 21 to 54 years old. The rate of validity of the questionnaires for this study was 86.1% (Table 1). The average age of the 155 nurses was 31 ± 8 years. There were 66 (43%) nurses aged 25 to 34 years, and 92 (59%) nurses had completed college. One hundred (65%) nurses were married, and 53 (34%) nurses had a shift work schedule.
Table 1.
Demographic characteristics of participants and total scores for job stress.
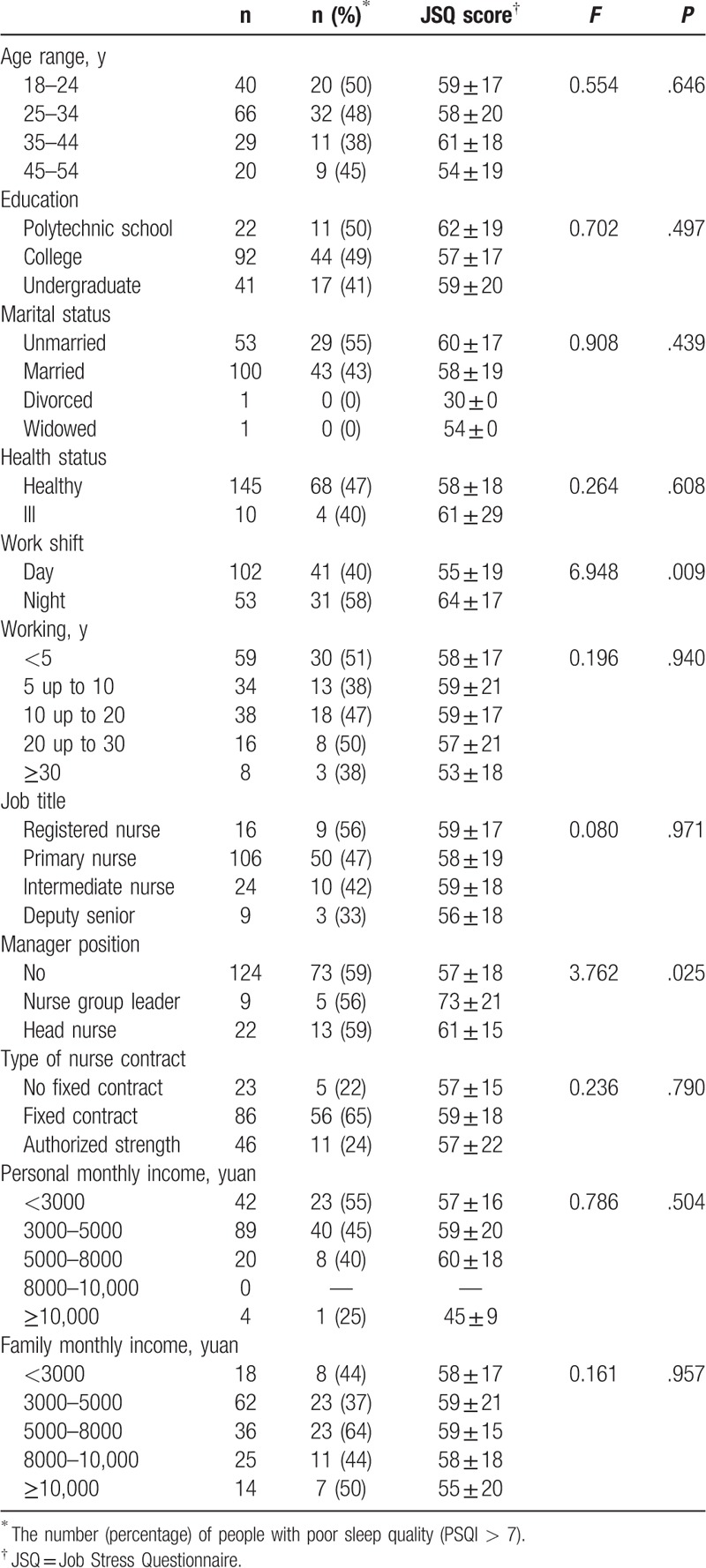
3.2. Demographic characteristics of participants and total scores for job stress
The basic characteristics of the subjects and the job stress scores are summarized in Table 1. The overall job stress score was 59 ± 9, and 72 nurses (46%) had a PSQI >7 (median, 7). Nurse managers and nurses with a night shift work schedule had greater job pressure scores than non-manager nurses and nurses working a day shift, respectively (manager position, F = 3.762, degrees of freedom = 154, P = .025; work shift, F = 6.948, degrees of freedom = 154, P = .009). No significant difference was observed in other variables, as indicated in Table 1.
3.3. The comparison of PSQI scores with different demographic characteristics of participants
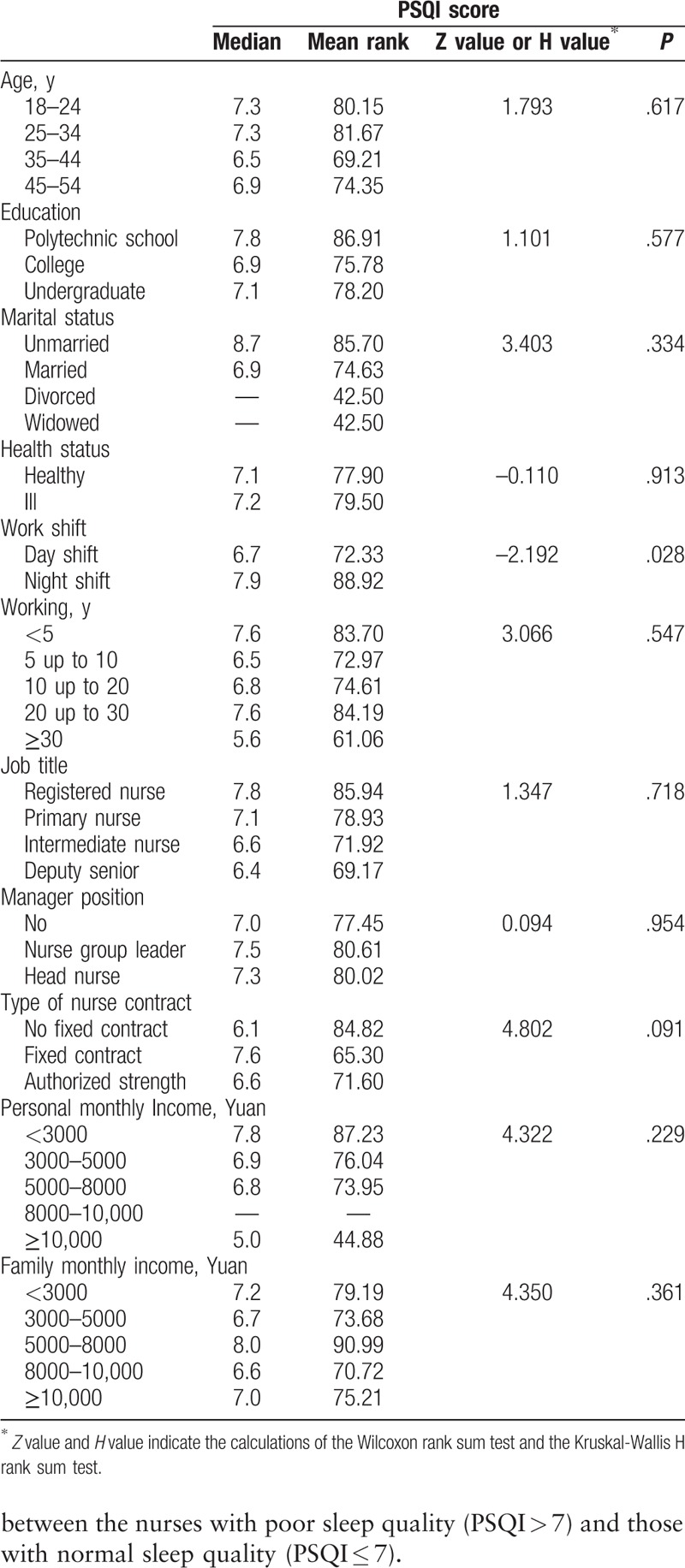
Sleep quality was significantly related to shift work (P = .028 of the Wilcoxon rank sum test, Table 2). Other factors, such as age, marital status, educational background, managerial position, and income, were not significantly related to sleep quality with P > .05 for the Wilcoxon rank sum test or the Kruskal-Wallis H rank sum test (Table 2).
Table 2.
The comparison of PSQI scores with different demographic characteristics of participants.
3.4. Associations between job stress parameters and sleep disturbances
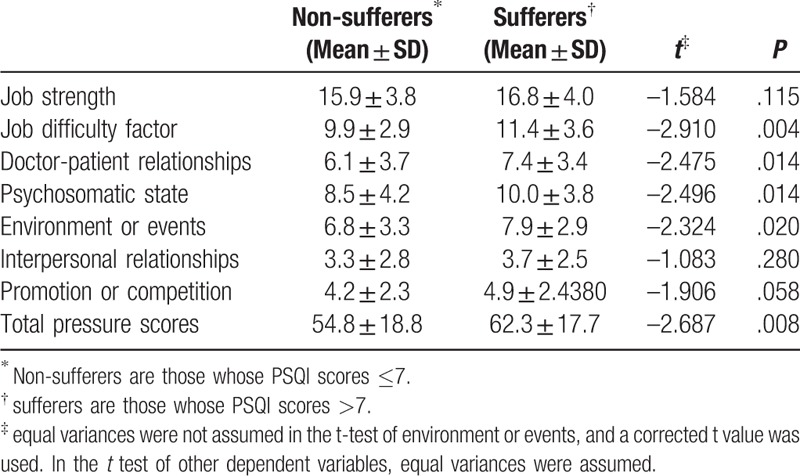
According to the seven parts of the job stress scores, we found that the scores for the job difficulty factor, doctor-patient relationships, psychosomatic state, environment or events, and total pressure scores were significantly different (P ≤ .02, Table 3) between the nurses with poor sleep quality (PSQI > 7) and those with normal sleep quality (PSQI ≤ 7).
Table 3.
Comparison of job stress-related factors by t-test between nurses with poor sleep quality and those with normal sleep quality.
3.5. Logistic regression analysis of multiple factors related to sleep quality
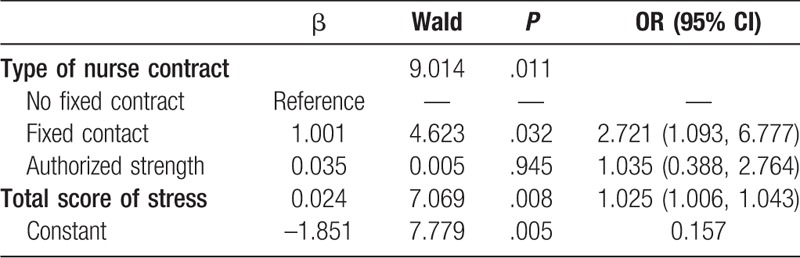
The independent variables included age, education, marital status, health status, work shift, years of work experience, job title, manager position, contract, and income were also screened by this method. The type of nurse contract and total job stress scores were related to sleep disturbances within the previous month. Specifically, the risk factors for sleep disturbances in community nurses were a fixed contract and a high total job stress score (Table 4).
Table 4.
Logistics regression analysis of the total score for stress and relevant factors related to sleep quality.
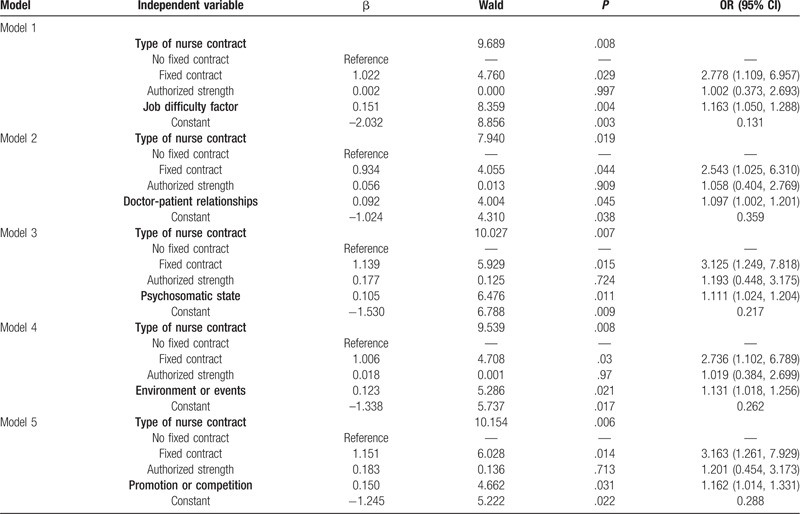
To further evaluate the effect of stress-related factors on sleep, sleep quality was taken as the dependent variable in the logistic regression, and the following seven relevant factors of job stress were considered as the independent variables in the models: job strength, psychosomatic state, doctor-patient relationships, job difficulty factor, environment or events, interpersonal relationships, and promotion or competition. There were seven logistic regression models in total, and the results that were statistically significant are shown in Table 5. The results showed that the type of nurse contract, job difficulty factor, doctor-patient relationships, psychosomatic state, environment or events, and promotion or competition affected the sleep quality of community nurses.
Table 5.
Logistics regression analysis of job stress and relevant factors related to sleep quality.
4. Discussion
The present study showed that sleep problems were prevalent among clinical nurses in community hospitals in China. In addition, we found that nurses with a night shift work schedule were at a much higher risk of sleep disturbance than nurses working a day shift. More importantly, the study indicated that as nurses’ job stress scores increased, sleep quality became progressively worse.
In community hospitals, nurses are often subject to public health, basic health, and various other special inspections. This contributes to day-to-day uncertainty and higher occupational stress. It has been recognized that job stress affects the sleep quality of nurses[24], especially for those who are on a night shift work schedule.[25]
Our results support previous studies that show that job stress is associated with work shift and a managerial position. The role of nurse managers is one of the most demanding in hospitals, which contributes to job-related stress. One study in 2014 reported that 72% of nurse managers were planning to leave their positions within five years. [26] Our results also showed that nurse managers had higher job pressure than the rest of the staff in a community hospital, which was not shown in reports from general hospitals.
Currently, the need for medical services is increasing with the development of China's economy, especially in community hospitals, and along with it, the frequency of a monthly night shift is also increasing. This work disturbs the internal body clock of nurses and results in irregular sleep patterns.[27,28] The overall prevalence of sleep disturbances in clinical nurses at community hospitals in Mainland China is reportedly 52.0%, which is higher than that found for the general population (26.4%–39.4%).[3,4,25–28]
Previous studies showed that sleep disturbances were more likely to occur among clinical nurses in general hospitals in Mainland China compared with Hong Kong, where the overall rate of insomnia is 11.9%, with women at higher risk than men. [29,30] By contrast, the insomnia rate of clinical nurses in Mainland China was 27.3%, and that of night shift nurses (63.8% to 70.0%) was significantly higher than that of day shift nurses [31–33]. Another study reported that the prevalence of shift-work disorder in nurses was 35.5% to 42.9%, specifically 26.1% for day shift nurses and 42.9% for night shift nurses. [34] This is lower than the results of the present study (46%). However, another study found that the prevalence of nurse sleep disorder was 87.7%, [35] which is much higher than the results of this study. We found that day and night shift nurses suffered from job stress scores that were 55 ± 19 and 64 ± 17, respectively, probably because 40% worked the day shift and 58% worked the night shift and had poor sleep quality. This is consistent with the findings of other researchers.[36,37] Therefore, clinical nurses are prone to sleep disturbances, and nurses working in a community hospital are most vulnerable to sleep disorders.
It is generally considered that temporary employees experience more job insecurity than permanent staff. Job insecurity has been identified as an important occupational stress factor that contributes negatively to the psychological and physical health and well-being of employees.[38–40]
Temporary nurses are more likely to be dismissed from work, so they are more likely to be stressed and work harder to keep their job, which may lead to sleep disorders. However, the present research indicates that nurses with fixed contracts have higher job stress scores than temporary nurses and permanent nurses. A possible reason is that they need to continuously learn new knowledge to improve their ability, meet job requirements and maintain work stability. Our study showed that the sleep quality of nurses with a fixed contract was more easily affected than the sleep quality of their counterparts who had permanent employment. This is inconsistent with other reports.[37–39] This study also showed that a high level of job stress was associated with sleep problems, corroborating previous findings.[19]
This study found that sleep problems were prevalent among clinical nurses in community hospitals in China. Sleep disturbances in nurses were highly associated with job difficulty factor, doctor-patient relationships, psychosomatic state, environment or events, promotion or competition, and total pressure scores. Occupational stress negatively affects sleep quality in Chinese clinical nurses; the higher the stress is, the worse the sleep quality. Sleep disturbance may lead to a lower quality of life and work efficiency of nurses, even leading to errors or medical malpractice. Awareness and interventions are therefore required to reduce job stress in community hospitals. Additional research on this topic is also necessary.
5. Limitations
This study had several limitations that may have affected the outcomes. First, there are no data from different types of hospitals as a control group in the study design to compare the difference in sleep disturbances between different ward/department nurses and community nurses. Second, the recruitment of stratified cluster sampling limits the generalization of the results. Job stress is a subjective experience that can affect sleep quality but it does not affect the professional function of community nurses. It may be important to sample community nurses for serious sleep disorders and determine whether these disorders affect their professional function. Third, the study data were obtained from a single city in southwestern China, and although nurses resided in several different communities, it may not be possible to generalize the findings to other cultures and geographic regions. Fourth, participants were from urban communities, and nurses in rural communities were not included.
Acknowledgments
We are grateful to all the nurses who participated in the study. Data will not be shared because study participants did not give their approval via an informed consent form.
Author contributions
Conceptualization: Ronghua Fang.
Data curation: Xuexue Deng, Xuelian Liu.
Methodology: Xuexue Deng, Ronghua Fang.
Project administration: Ronghua Fang.
Supervision: Ronghua Fang.
Writing – original draft: Xuexue Deng, Xuelian Liu.
Writing – review & editing: Ronghua Fang.
Footnotes
Abbreviations: JSQ = job stress questionnaire, PSQI = Pittsburgh sleep quality index.
How to cite this article: Deng X, Liu X, Fang R. Evaluation of the correlation between job stress and sleep quality in community nurses. Medicine. 2020;99:4(e18822).
All participants signed informed consent forms.
Approval of the research protocol: The ethics committee of West China Hospital of Sichuan University approved this study and its method in August 2017 (approve number 2017 (65)).
The authors have no conflicts of interest to disclose.
References
- [1].Cho KO. Sleep duration and self-rated health are independently associated with physical activity level in the Korean population. Iran J Public Health 2014;435:590–600. [PMC free article] [PubMed] [Google Scholar]
- [2].Zhou XN, Zhao WY, Li NN. The relationship between sleep quality, job burnout and coping style of medical staffs. China J Health Psychol 2013;213:353–5. [Google Scholar]
- [3].Sateia MJ, Doghramji K, Hauri PJ, et al. Evaluation of chronic insomnia. An American academy of sleep medicine review. Sleep 2000;232:243–308. [PubMed] [Google Scholar]
- [4].Liu Y, Chen GN. Nurse's sleep quality in a three level hospital in Guangzhou. China J Health Psychol 2015;237:989–92. [Google Scholar]
- [5].Zhang L, Sun DM, Li CB, et al. Influencing factors for sleep quality among shift-working nurses: a cross-sectional study in China using 3-factor Pittsburgh sleep quality index. Asian Nurs Res 2016;10:277–82. [DOI] [PubMed] [Google Scholar]
- [6].Mieda M, Sakurai T. Orexin (hypocretin) receptor agonists and antagonists for treatment of sleep disorders. Rationale for development and current status. CNS Drugs 2013;27:83–90. [DOI] [PubMed] [Google Scholar]
- [7].Rosado IV, Russo GH, Maia EM. Generating health elicits illness? The contradictions of work performed in emergency care units of public hospitals. Cien Saude Colet 2015;20:3021–32. [DOI] [PubMed] [Google Scholar]
- [8].Feleke SA, Mulatu MA, Yesmaw YS. Medication administration error: magnitude and associated factors among nurses in Ethiopia. BMC Nurs 2015;14:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Kling RN, McLeod CB, Koehoorn M. Sleep problems and workplace injuries in Canada. Sleep 2010;335:611–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Han Y, Yuan Y, Zhang L, et al. Sleep disorder status of nurses in general hospitals and its influencing factors. Psychiatria Danubina 2016;28:176–83. [PubMed] [Google Scholar]
- [11].da Rocha MC, De Martino MM. Stress and sleep quality of nurses working different hospital shifts. Rev Esc Enferm USP 2010;44:279–85. [DOI] [PubMed] [Google Scholar]
- [12].Gao YQ, Pan BC, Sun W, et al. Depressive symptoms among Chinese nurses: prevalence and the associated factors. J Adv Nurs 2012;685:1166–75. [DOI] [PubMed] [Google Scholar]
- [13].Li M, Nie J, Ren Y. Effects of exercise dependence on psychological health of Chinese college students. Psychiatr Danub 2015;274:413–9. [PubMed] [Google Scholar]
- [14].Liu XZ, Xu L, Shi GL, et al. Analysis of occupational stress of nurses in ICUs of 13 class III grade I hospitals. J Nurs 2011;1822:10–4. [Google Scholar]
- [15].Karlberg, Ingvar Is occupational health part of public health? Scand J Public Health 2016;44:333–4. [DOI] [PubMed] [Google Scholar]
- [16].Clare G, Elsa U. Managing work health and safety: recent developments and future directions. Asia Pac J Hum Res 2012;50:227–44. [Google Scholar]
- [17].Hu Q, Peng MJ, Liao HL, et al. Discussion on the construction of occupational safety and health management system in medical institution. China Med Herald 2018;15:147–9. [Chinese]. [Google Scholar]
- [18].Dong H, Zhang Q, Sun Z, et al. Sleep problems among Chinese clinical nurses working in general hospitals. Occup Med 2017;67:534–9. [DOI] [PubMed] [Google Scholar]
- [19].Liu XL, Deng XX, Fang RH. Correlation analysis between sleep quality and work stress of community health. Sichuan Med J 2018;39:341–5. [Google Scholar]
- [20].Trousselard M, Dutheil F, Naughton G, et al. Stress among nurses working in emergency, anesthesiology and intensive care units depends on qualification: a Job Demand-Control survey. Int Arch Occup Environ Health 2016;89:221–9. [DOI] [PubMed] [Google Scholar]
- [21].Bjorvatn B, Dale S, Hogstad-Erikstein R, et al. Self-reported sleep and health among Norwegian hospital nurses in intensive care units. Nurs Crit Care 2012;17:180–8. [DOI] [PubMed] [Google Scholar]
- [22].Lou YY, Wu XR, Chen QY, et al. Investigation and analysis of 320 medical staff's work pressure and its physiological and health self-assessment. Zhejiang Med Educ 2008;7:14–8. [Google Scholar]
- [23].Liu XC, Tang MQ, Hu L, et al. Study of the reliability and validity of the Pittsburgh sleep quality index. Chin J Psychiatry 1996;29:103–7. [Google Scholar]
- [24].Utsugi M, Saijo Y, Yoshioka E, et al. Relationships of occupational stress to insomnia and short sleep in Japanese workers. Sleep 2005;28:728–35. [DOI] [PubMed] [Google Scholar]
- [25].Shan X, Hong XF. Investigation and analysis of the sleep quality of nurses in elderly ward. Chin J Mod Nurs 2010;16:6634–6. [Google Scholar]
- [26].Shao MF, Chou YC, Yeh MY, et al. Sleep quality and quality of life in female shift-working nurses. J Adv Nurs 2010;66:1565–72. [DOI] [PubMed] [Google Scholar]
- [27].Warshawsky NE, Havens DS. Nurse manager job satisfaction and intent to leave. Nurs Econ 2014;32:32–9. [PMC free article] [PubMed] [Google Scholar]
- [28].Zhang HS, Li Y, Mo HY, et al. A community-based cross-sectional study of sleep quality in middle-aged and older adults. Qual Life Res 2017;26:923–33. [DOI] [PubMed] [Google Scholar]
- [29].Korompeli A, Chara T, Chrysoula L, et al. Sleep disturbance in nursing personnel working shifts. Nurs Forum 2013;48:45–53. [DOI] [PubMed] [Google Scholar]
- [30].Dong HY, Zhang Q, Sun ZH. Sleep disturbances among Chinese clinical nurses in general hospitals and its influencing factors. BMC Psychiatry 2017;67:534–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Li RH, Wing YK, Ho SC, et al. Gender differences in insomnia–a study in the Hong Kong Chinese population. J Psychosom Res 2002;53:601–9. [DOI] [PubMed] [Google Scholar]
- [32].Vanden TM, Jonqe J. Managing job stress in nursing: what kind of resources do we need. J Adv Nurs 2008;63:75–84. [DOI] [PubMed] [Google Scholar]
- [33].Chien PL, Su HF, Hsieh PC, et al. Sleep quality among female hospital staff nurses. Sleep Disord 2013;2013:283490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Chan MF. Factors associated with perceived sleep quality of nurses working on rotating shifts. J Clin Nurs 2009;18:285–93. [DOI] [PubMed] [Google Scholar]
- [35].Sadat A, Roodbandi J, Feyzi V, et al. Sleep quality and sleepiness: a comparison between nurses with and without shift work, and University Employees. Int J Occup Hyg 2017;4:230–6. [Google Scholar]
- [36].Sveinsdottir H. Self-assessed quality of sleep, occupational health, working environment, illness experience and job satisfaction of female nurses working different combination of shifts. Scand J Caring Sci 2006;20:229–37. [DOI] [PubMed] [Google Scholar]
- [37].Wang L, Qin P, Zhao Y, et al. Prevalence and risk factors of poor sleep quality among Inner Mongolia medical university students: a cross-sectional survey. Psychiatry Res 2016;244:243–8. [DOI] [PubMed] [Google Scholar]
- [38].Yazdi Z, Sadeghniiat-Haghighi K, Loukzadeh Z, et al. Prevalence of sleep disorders and their impacts on occupational performance: a comparison between shift workers and nonshift workers. Sleep Disord 2014;2014:870320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Burgard SA, Brand JE, House JS. Perceived job insecurity and worker health in the United States. Soc Sci Med 2009;69:777–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].László KD, Pikhart H, Kopp MS, et al. Job insecurity and health: a study of 16 European countries. Soc Sci Med 2010;70:867–74. [DOI] [PMC free article] [PubMed] [Google Scholar]