

Abstract
Background
Pain ratings reported by patients with cancer continue to increase, and numerous computer and phone apps for managing cancer-related pain have been developed recently; however, whether these apps effectively alleviate patients’ pain remains unknown.
Objective
This study aimed to comprehensively evaluate the role of mobile apps in the management of cancer pain.
Methods
Literature on the use of apps for cancer pain management and interventions, published before August 2019, was retrieved from the following databases: MEDLINE, Embase, Cochrane, CINAHL, Scopus, and PsycINFO. The effects of apps on cancer pain were evaluated using RevMan5.3 software, and the rates of adverse drug reactions were analyzed using the R Statistical Software Package 3.5.3.
Results
A total of 13 studies were selected for the analysis: 5 randomized controlled trials (RCTs), 4 before-after studies, 2 single-arm trials, 1 prospective cohort study, and 1 prospective descriptive study. The 5 RCTs reported data for 487 patients (240 patients in the intervention group and 247 patients in the control group), and the remaining studies reported data for 428 patients. We conducted a meta-analysis of the RCTs. According to the meta-analysis, apps can significantly reduce pain scores (mean difference [MD]=–0.50, 95% CI –0.94 to –0.07, I2=62%, P=.02). We then used apps that have an instant messaging module for subgroup analysis; these apps significantly reduced patients’ pain scores (MD=–0.67, 95% CI –1.06 to –0.28, I2=57%, P<.01). Patients using apps without an instant messaging module did not see a reduction in the pain score (MD=0.30, 95% CI –1.31 to 1.92, I2=70%, P=.71). Overall, patients were highly satisfied with using apps. Other outcomes, such as pain catastrophizing or quality of life, demonstrated greater improvement in patients using apps with instant messaging modules compared with patients not using an app.
Conclusions
The use of apps with instant messaging modules is associated with reduced pain scores in patients with cancer-related pain, and patient acceptance of these apps is high. Apps without instant messaging modules are associated with relatively higher pain scores. The presence of an instant messaging module may be a key factor affecting the effect of an app on cancer pain.
Keywords: mobile apps, cancer pain, meta-analysis, instant messaging
Introduction
Cancer Pain Management
According to the 2018 global cancer statistics, there were approximately 18.19 million new cases of cancer [1]. The number of new cancer cases is increasing rapidly every year and is expected to exceed 20 million by 2030 [2]. Further, the incidence of persistent cancer pain during treatment has also increased [3]. According to reports, approximately 69% of patients with cancer worldwide experience pain during their daily activities, which may have serious psychosocial consequences, including anxiety and depression [4].
Due to differences in treatment levels, cancer pain that is not adequately controlled is still widespread in developing countries [5]. According to reports, only 25% of patients with advanced cancer have pain that can be relieved, especially out-of-hospital patients, who have a lower pain relief rating than patients in the hospital. This is primarily caused by disjointed management of patients after discharge, resulting in reduced patient compliance, poor control of side effects, and outbreaks of pain [6].
Apps for Cancer Pain Management
With the development of the Internet, the number of health-related apps is growing rapidly, including apps for monitoring and managing diseases [5,7-9]. Apps for pain management are also gradually entering the market [10-12]. There are currently 283 pain-related apps in China and abroad, but only 8.2% of these apps include medical professionals in the development process, and none are scientifically proven to be effective. Therefore, whether apps can improve pain relief for patients remains unknown. Among the available pain apps, none are comprehensive for pain management, and most only contain a pain diary module [13,14].
Aim of the Study
It is not clear whether using an app to manage cancer pain can improve pain relief rating or which module type is the most effective in terms of app usability and pain management. Therefore, we conducted a systematic review and meta-analysis of studies of apps intended to manage cancer-related pain to explore whether these apps can improve pain relief ratings for patients with cancer and identify which modules increase the app’s effectiveness for managing pain.
Methods
Literature Search
Eligible studies were identified by searching Medline, Embase, Cochrane, CINAHL, psycINFO, and other relevant databases, and the results were combined using the literature traceability method. Searches were conducted on August 1, 2019. Search keywords included “cancer pain+,” “cancer pain management+,” “mobile phone,” “+,“ ”Mobile Devices,“ ”Mobile Apps,“ and ”mHealth.“ Search strategies are detailed in Multimedia Appendix 1. Only articles written in English were considered. There were no restrictions regarding publication date.
Inclusion and Exclusion Criteria
Inclusion Criteria
Studies were included when they (1) focused on patients with cancer pain, (2) involved an intervention using apps downloaded and registered on either a mobile phone or computer for the management of cancer pain, (3) used the numeric rating scale to assess pain, (4) included patients that were followed up for more than a week, and (5) reported the results in English.
Exclusion Criteria
Studies were excluded when (1) the study type was a review, model study, literature review, or conference summary; (2) the results of the study used scales other than the numeric rating scale or did not report the pain score; (3) the study intervention was a telephone conversation; or (4) the study was a duplicate report.
Document Screening and Data Extraction
All reference titles and abstracts were initially screened for relevance by two reviewers. Afterward, full-text analysis for eligibility was independently performed by Caiyun Zheng and Lizhu Weng. Disagreements were resolved by discussion and consensus or third-party arbitration.
The required data were extracted by a researcher using a literature data extraction table, and another researcher confirmed the accuracy and authenticity of the data. The extracted content included study information (research topic, author, date), baseline characteristics of the study subjects (sample size, median age), specific details of the app intervention, pain scores for up to 12 months of intervention, and other outcome indicators (quality of life, side effects).
Literature Quality Evaluation
Risk assessment of the included RCTs was performed using the Cochrane risk of bias tool based on the Cochrane Systematic Review Manual's literature evaluation criteria.
Statistical Analysis
Meta-analysis of RCTs was performed using RevMan5.3 software. Heterogeneity was assessed using the chi-squared test, and quantitative analysis was performed using I2. Values of P≥.05 and I2 ≤50% were considered to represent no heterogeneity, and a fixed-effect model was used. If P<.05 and I2>50%, a random-effects model was used, followed by subgroup analysis to identify the cause of heterogeneity [15].
Results
Search Results
A total of 11,217 articles were retrieved from the systematic literature search, and 4 articles were retrieved by other means, totaling 11,221 articles. After removing duplicate studies, the remaining 8640 were screened. After reading 40 eligible full-text articles, 27 were excluded, and 13 were selected [16-28]. The systematic search results are shown in Figure 1.
Figure 1.
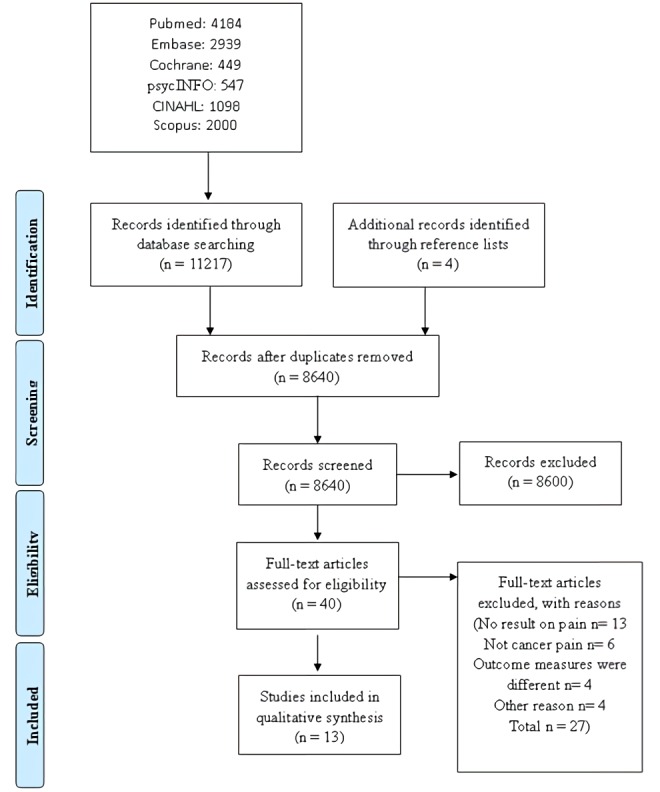
Literature screening and selection flow chart.
Basic Characteristics and Quality Evaluation of the Literature
The 5 RCTs included a total of 487 patients: 240 patients in the intervention group and 247 patients in the control group. The remaining studies reported data for 428 patients. General information from the studies is shown in Table 1. The Cochrane systematic evaluation method was used for quality evaluation, and overall, the included literature had a low risk of bias, as shown in Figure 2.
Table 1.
Summary of the characteristics of the included studies.
| Study | Study design |
Number of participants |
Follow-up (weeks) |
Age (years), mean (SD) |
Description of modules within the app | Instant messaging module |
| Yun, 2012 [17] | RCTa | 273 | 12 | Unknown | Five modules: self-assessment and graphic reports, health advice and online education, enhanced and short message services, caregiver monitoring and support, monitoring by a health professional | Yes |
| Somers, 2016 [23] | RCT | 23 | 1 | 60.00 (11) | Skype | No |
| Sun, 2017 [21] | RCT | 46 | 2 | 67.50 (Unknown) | Four modules: life quality self-evaluation, cancer pain self-evaluation, real-time messaging, standard medication | Yes |
| Smith, 2018 [28] | RCT | 87 | 18 | 56.70 (8.7) | Four modules: Web-based content, required activities including attending one online introductory group meeting, viewing videos to complete cognitive reframing, mind-body exercises | No |
| Yang, 2019 [16] | RCT | 58 | 4 | 52.53 (8.78) | Four modules: pain education, consultation, cancer pain self-evaluation, soothing music | Yes |
| Somers, 2015 [18] | BASb | 25 | 1 | 53.88 (12.59) | Videoconferencing on a tablet computer, eg, Skype | No |
| Jibb, 2017 [24] | BAS | 40 | 4 | 14.20 (1.7) | Questionnaires, real-time self-management recommendations, email alerts | Yes |
| Bae, 2017 [26] | BAS | 100 | 4 | 57.00 (Unknown) | PHRc data gathering, PHR gateway, Web service | No |
| Lengacher, 2017 [25] | BAS | 13 | 6 | 57.00 (9) | iBooks on an iPad | No |
| Stinson, 2015 [22] | Prospective, descriptive study | 92 | 2 | 13.10 (2.9) | Assessment items | No |
| Oldenmenger, 2017 [27] | Prospective, cohort study | 48 | 6 | 59.00 (11) | Three modules: a pain diary, eConsult, patient education | Yes |
| Dorfman, 2018 [19] | Single-arm pilot study | 20 | Unknown | 57.85 (11.72) | Daily access to session content, video clips modeling coping skills, stories about pain experiences from example participants, other materials (eg, relaxation audio) | Yes |
| Parks, 2019 [20] | Prospective, single-arm study | 90 | 12 | 55.10 (8.7) | Three modules: to-do list, individual health information, in-app chat service | Yes |
aRCT: randomized controlled trial.
bBAS: before-after study.
cPHR: personal health record.
Figure 2.
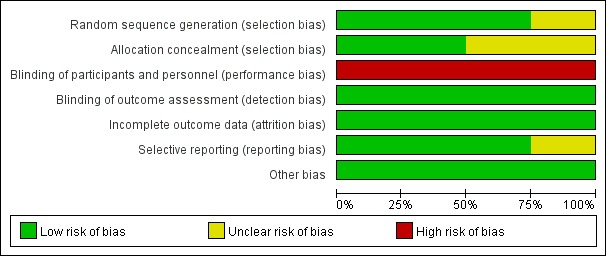
Bias risk map from the Cochrane systematic evaluation method to evaluate the quality of the included randomized control trials.
Meta-Analysis
Pain Relief Rating
A random-effects analysis model was used for the meta-analysis of the RCTs. The pain scores of the intervention group were lower than those of the control group (mean difference [MD]=–0.50, 95% CI –0.94 to –0.07, I2=62%, P=.02). Subgroup analysis was performed for apps with instant messaging modules. Instant messaging modules are a channel for real-time communication between patients and medical staff. Patients who used apps with instant messaging modules had lower pain scores (MD=–0.67, 95% CI –1.06 to –0.28, I2=57%, P<.01) than patients who used apps without an instant messaging module (MD=0.30, 95% CI –1.31 to 1.92, I2=70%, P=.71; Figure 3).
Figure 3.
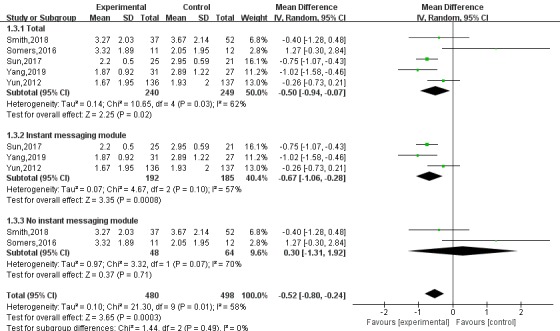
Subgroup analysis of the effects of apps with instant messaging modules on pain in patients with cancer.
Sensitivity Analysis Results
The data were analyzed with the fixed- and random-effects model, and the consistency of these results reflects the reliability of the combined results to some extent. The two effect models were used to analyze the combined effect of each risk factor and calculate 95% CIs. The results were similar, indicating that the results of this study are stable.
Impact of Apps on Other Outcomes
Two studies reported that the number of side effects in patients using apps is statistically significantly lower than in the control group, whereas Bae et al reported no reduction in the number of adverse reactions [16,26]. All studies evaluating changes in quality of life and anxiety showed significant improvement in groups using apps [16,17,20,25,28]. In addition, in 3 studies, pain catastrophizing was lower, and pain self-efficacy was higher in the intervention group when compared to the control group [18,23]. However, Smith et al [28] reported no significant difference in pain catastrophizing or self-efficacy between the intervention and control groups, only a significant improvement in fatigue. Seven studies reported high levels of satisfaction with the ease of use of the app [16,18,20,21,25,28], and 5 studies showed that patients using apps had a higher intervention completion rate [18-20,25,28]. We created a forest plot to show the effects of apps on other outcomes (Figure 4). Most of the studies had no significant differences in results, apart from those for fatigue, emotional functioning, and social functioning.
Figure 4.
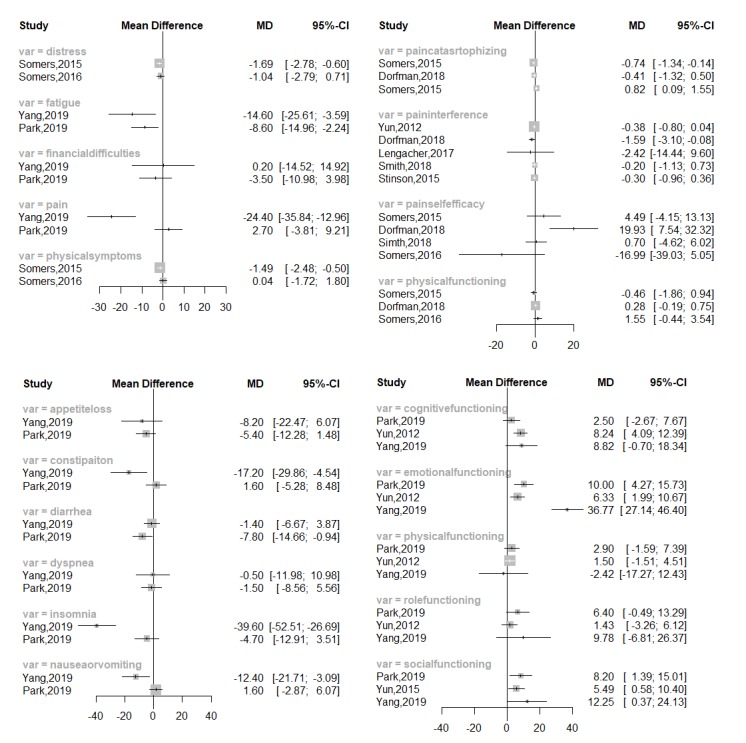
Forest plot of the effect of app use on other cancer-related outcomes.
Discussion
Principal Findings
The purpose of our study was to assess the effectiveness of apps for pain management in patients with cancer and to explore which modules influence pain relief ratings. A total of 13 studies were included in this study, and most of the studies reported that pain apps are effective. Patients who use the apps have less pain than patients who do not use the apps. Other results, such as quality of life, pain catastrophizing, and pain self-efficacy, significantly improved in patients using apps. Due to the lack of reported data and heterogeneity, a synthesis of the other results using statistical methods was not performed.
The apps used to manage cancer pain typically have multiple modules, including common records, training, and real-time feedback. These types of apps can be installed on a computer or mobile phone or accessed directly from a website. They can effectively teach patients about pain and provide the ability to record pain and provide feedback. To determine which modules have the greatest impact, we further conducted a subgroup analysis of the RCTs, which showed that, the use of an app that has instant messaging modules significantly improves pain relief ratings. Furthermore, the use of an app without instant messaging modules had no significant effect on the pain relief ratings of patients with cancer. Therefore, instant messaging modules in apps may be a key factor for pain relief. This may be because the patient can report their condition to the medical staff in a timely manner.
When using an app with an instant messaging module, patients with cancer can notify doctors or pharmacists of a pain outbreak or persistent pain, allowing pharmacists or doctors to intervene in real time. Additionally, a physician can give advice on the dosage of prescribed medication, manage the patient's pain and adverse drug reactions in real time, or recommend that the patient see a doctor immediately, thereby improving compliance with pain treatment and pain relief ratings [27,29]. A pharmacist can relieve stress by discussing how the patient is feeling or suggesting suitable alternative pain management methods. Studies have shown that yoga, proper exercise, or listening to soothing music can relieve pain [30,31]. These activities effectively allow patients to control their pain outside the hospital setting without panic or confusion [32]. Therefore, an instant messaging module could provide patients with both technical support and a sense of security when outside the hospital, which is an important part of pain management apps.
Limitations
There are some limitations to our study. The included literature had relatively small sample sizes and varying follow-up times, some as short as 14 days. Despite these limitations, this study is the first to comprehensively analyze the effect of app modules on the ability of the app to effectively intervene. Therefore, larger samples and longer clinical RCTs are needed to further evaluate the impact of app intervention on pain relief ratings.
Comparison With Prior Work
To the best of our knowledge, this is the first systematic review of the effectiveness of mobile apps for pain management in cancer patients. In published systematic reviews, the evaluation of the effects of apps focus on other chronic pain [6,13,33,34] or explore the impact of an app on quality of life and other symptoms for a single cancer type. They generally provide qualitative descriptions without an assessment of the overall effectiveness of the app as a tool for managing pain. These studies have also not identified which app modules are critical for the effectiveness of the app-based intervention [2,35].
The authors of 3 previous reviews reported that apps were not effective for the following reasons: The participation of health care workers was too low, the apps could not find resources in the online store, and the apps that could be downloaded did not pass scientific verification [14,36,37]. Rincon et al [2] pointed out that strict clinical trials are lacking for most apps. Three other reviews assessed multiple app types, which cannot quantitatively analyze the overall effectiveness of the apps on pain [35,38,39]. Martorella et al [38] and Fridriksdottir et al [39] studied the effects of multiple intervention types on pain, with a variety of intervention models, mainly based on the network that includes the app. Thurnheer et al [12] studied the benefits of an app for chronic pain. Of the 15 studies, 4 included in-hospital management, and 11 involved out-of-hospital management. Most preliminary reports suggest that an app is beneficial for relieving pain in patients, but all require additional scientific verification and analysis to determine which module is key for improving usability [12]. Silva et al [33] studied the effectiveness of self-management via an app for improving pain, psychological distress, fatigue, and sleep in cancer survivors. Only 6 studies were included, and the quality of the included literature was poor. Only 2 studies reported that the intervention group had a lower mean pain score at follow-up, but neither result reached statistical significance [33].
Other studies that did not meet our inclusion criteria (eg, studies that included patients with non-cancer pain and studies of different types) showed similar results to the studies included in our analysis. Schatz et al [40] used smartphone-based cognitive-behavioral therapy in children with sickle cell disease. The results suggested that smartphone-supported cognitive-behavioral therapy coping methods can reduce pain intensity in children with sickle cell disease. Sundberg et al [41] used an interactive smartphone app (Interaktor, Health Navigator, Sweden) to detect and treat symptoms during early prostate cancer radiotherapy, and the intervention group had significantly lower levels of fatigue and nausea at the end of radiotherapy. Therefore, it is an effective mobile health tool to promote supportive care during cancer treatment. Uhm et al [42] studied breast cancer patients using mobile health smartphone apps and pedometers, which resulted in greater improvements in quality of life than with traditional exercise manuals.
Conclusions
This study found that patients with cancer might benefit from the use of apps for cancer pain management, especially those with instant messaging modules, which can reduce pain scores in cancer patients. Patient acceptance of these apps is high. At the same time, the app has a palliative effect on patients’ cancer pain and other cancer-related symptoms. Pain management apps with instant messaging modules provide the ability to connect patients and medical professionals with a convenient learning channel, especially in outpatient clinics and for patients living in remote areas with less access to doctors and medical support. Therefore, the findings of this study can guide the development of cancer pain apps, help optimize app modules, and narrow the gap between doctors and patients to achieve better control of cancer-related pain.
Acknowledgments
Joint Funds for the Innovation of Science and Technology, Fujian Province (Grant number: 2018Y9045); Key Project for Youth Academic Talents (2019-ZQN-39) from Health and Family Planning Commission of Fujian Province.
Abbreviations
- BAS
before-after study
- MD
mean difference
- PHR
personal health record
- RCT
randomized controlled trial
Appendix
Search strategy to find literature on the use of apps for cancer pain management and interventions.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov 12;68(6):394–424. doi: 10.3322/caac.21492. doi: 10.3322/caac.21492. [DOI] [PubMed] [Google Scholar]
- 2.Rincon E, Monteiro-Guerra F, Rivera-Romero O, Dorronzoro-Zubiete E, Sanchez-Bocanegra CL, Gabarron E. Mobile Phone Apps for Quality of Life and Well-Being Assessment in Breast and Prostate Cancer Patients: Systematic Review. JMIR Mhealth Uhealth. 2017 Dec 04;5(12):e187. doi: 10.2196/mhealth.8741. https://mhealth.jmir.org/2017/12/e187/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Brown MR, Ramirez JD, Farquhar-Smith P. Pain in cancer survivors. Br J Pain. 2014 Nov;8(4):139–53. doi: 10.1177/2049463714542605. http://europepmc.org/abstract/MED/26516548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Magee D, Bachtold S, Brown M, Farquhar-Smith P. Cancer pain: where are we now? Pain Manag. 2019 Jan 01;9(1):63–79. doi: 10.2217/pmt-2018-0031. [DOI] [PubMed] [Google Scholar]
- 5.Grasaas E, Fegran L, Helseth S, Stinson J, Martinez S, Lalloo C, Haraldstad K. iCanCope With Pain: Cultural Adaptation and Usability Testing of a Self-Management App for Adolescents With Persistent Pain in Norway. JMIR Res Protoc. 2019 Jun 03;8(6):e12940. doi: 10.2196/12940. https://www.researchprotocols.org/2019/6/e12940/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lalloo C, Shah U, Birnie KA, Davies-Chalmers C, Rivera J, Stinson J, Campbell F. Commercially Available Smartphone Apps to Support Postoperative Pain Self-Management: Scoping Review. JMIR Mhealth Uhealth. 2017 Oct 23;5(10):e162. doi: 10.2196/mhealth.8230. https://mhealth.jmir.org/2017/10/e162/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bonoto BC, de Araújo VE, Godói IP, de Lemos LLP, Godman B, Bennie M, Diniz LM, Junior AAG. Efficacy of Mobile Apps to Support the Care of Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR Mhealth Uhealth. 2017 Mar 01;5(3):e4. doi: 10.2196/mhealth.6309. https://mhealth.jmir.org/2017/3/e4/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wu X, Guo X, Zhang Z. The Efficacy of Mobile Phone Apps for Lifestyle Modification in Diabetes: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth. 2019 Jan 15;7(1):e12297. doi: 10.2196/12297. https://mhealth.jmir.org/2019/1/e12297/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Luo D, Wang P, Lu F, Elias J, Sparks JA, Lee YC. Mobile Apps for Individuals With Rheumatoid Arthritis: A Systematic Review. J Clin Rheumatol. 2019 Apr;25(3):133–141. doi: 10.1097/RHU.0000000000000800. [DOI] [PubMed] [Google Scholar]
- 10.Vollmer Dahlke Deborah, Fair K, Hong YA, Beaudoin CE, Pulczinski J, Ory MG. Apps seeking theories: results of a study on the use of health behavior change theories in cancer survivorship mobile apps. JMIR Mhealth Uhealth. 2015 Mar 27;3(1):e31. doi: 10.2196/mhealth.3861. https://mhealth.jmir.org/2015/1/e31/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stinson JN, Jibb LA, Nguyen C, Nathan PC, Maloney AM, Dupuis LL, Gerstle JT, Alman B, Hopyan S, Strahlendorf C, Portwine C, Johnston DL, Orr M. Development and testing of a multidimensional iPhone pain assessment application for adolescents with cancer. J Med Internet Res. 2013 Mar 08;15(3):e51. doi: 10.2196/jmir.2350. https://www.jmir.org/2013/3/e51/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thurnheer SE, Gravestock I, Pichierri G, Steurer J, Burgstaller JM. Benefits of Mobile Apps in Pain Management: Systematic Review. JMIR Mhealth Uhealth. 2018 Oct 22;6(10):e11231. doi: 10.2196/11231. https://mhealth.jmir.org/2018/10/e11231/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lalloo C, Jibb LA, Rivera J, Agarwal A, Stinson JN. "There's a Pain App for That": Review of Patient-targeted Smartphone Applications for Pain Management. Clin J Pain. 2015 Jun;31(6):557–63. doi: 10.1097/AJP.0000000000000171. [DOI] [PubMed] [Google Scholar]
- 14.de la Vega R, Miró J. mHealth: a strategic field without a solid scientific soul. a systematic review of pain-related apps. PLoS One. 2014;9(7):e101312. doi: 10.1371/journal.pone.0101312. http://dx.plos.org/10.1371/journal.pone.0101312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jin YZ, Yan S, Yuan WX. Effect of isometric handgrip training on resting blood pressure in adults: a meta-analysis of randomized controlled trials. J Sports Med Phys Fitness. 2017;57(1-2):154–160. doi: 10.23736/S0022-4707.16.05887-4. [DOI] [PubMed] [Google Scholar]
- 16.Yang J, Weng L, Chen Z, Cai H, Lin X, Hu Z, Li N, Lin B, Zheng B, Zhuang Q, Du B, Zheng Z, Liu M. Development and Testing of a Mobile App for Pain Management Among Cancer Patients Discharged From Hospital Treatment: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2019 May 29;7(5):e12542. doi: 10.2196/12542. https://mhealth.jmir.org/2019/5/e12542/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yun YH, Lee KS, Kim Y, Park SY, Lee ES, Noh D, Kim S, Oh JH, Jung SY, Chung K, Lee YJ, Jeong S, Park KJ, Shim YM, Zo JI, Park JW, Kim YA, Shon EJ, Park S. Web-based tailored education program for disease-free cancer survivors with cancer-related fatigue: a randomized controlled trial. J Clin Oncol. 2012 Apr 20;30(12):1296–303. doi: 10.1200/JCO.2011.37.2979. http://jco.ascopubs.org/cgi/pmidlookup?view=long&pmid=22412149. [DOI] [PubMed] [Google Scholar]
- 18.Somers TJ, Abernethy AP, Edmond SN, Kelleher SA, Wren AA, Samsa GP, Keefe FJ. A Pilot Study of a Mobile Health Pain Coping Skills Training Protocol for Patients With Persistent Cancer Pain. J Pain Symptom Manage. 2015 Oct;50(4):553–8. doi: 10.1016/j.jpainsymman.2015.04.013. http://europepmc.org/abstract/MED/26025279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dorfman CS, Kelleher SA, Winger JG, Shelby RA, Thorn BE, Sutton LM, Keefe FJ, Gandhi V, Manohar P, Somers TJ. Development and pilot testing of an mHealth behavioral cancer pain protocol for medically underserved communities. J Psychosoc Oncol. 2019;37(3):335–349. doi: 10.1080/07347332.2018.1479327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Park S, Kim JY, Lee JC, Kim HR, Song S, Kwon H, Ji W, Choi CM. Mobile Phone App-Based Pulmonary Rehabilitation for Chemotherapy-Treated Patients With Advanced Lung Cancer: Pilot Study. JMIR Mhealth Uhealth. 2019 Feb 04;7(2):e11094. doi: 10.2196/11094. https://mhealth.jmir.org/2019/2/e11094/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sun Y, Jiang F, Gu JJ, Wang YK, Hua H, Li J, Cheng Z, Liao Z, Huang Q, Hu W, Ding G. Development and Testing of an Intelligent Pain Management System (IPMS) on Mobile Phones Through a Randomized Trial Among Chinese Cancer Patients: A New Approach in Cancer Pain Management. JMIR Mhealth Uhealth. 2017 Jul 25;5(7):e108. doi: 10.2196/mhealth.7178. https://mhealth.jmir.org/2017/7/e108/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stinson JN, Jibb LA, Nguyen C, Nathan PC, Maloney AM, Dupuis LL, Gerstle JT, Hopyan S, Alman BA, Strahlendorf C, Portwine C, Johnston DL. Construct validity and reliability of a real-time multidimensional smartphone app to assess pain in children and adolescents with cancer. Pain. 2015 Dec;156(12):2607–15. doi: 10.1097/j.pain.0000000000000385. [DOI] [PubMed] [Google Scholar]
- 23.Somers TJ, Kelleher SA, Westbrook KW, Kimmick GG, Shelby RA, Abernethy AP, Keefe FJ. A Small Randomized Controlled Pilot Trial Comparing Mobile and Traditional Pain Coping Skills Training Protocols for Cancer Patients with Pain. Pain Res Treat. 2016;2016:2473629. doi: 10.1155/2016/2473629. doi: 10.1155/2016/2473629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jibb LA, Stevens BJ, Nathan PC, Seto E, Cafazzo JA, Johnston DL, Hum V, Stinson JN. Implementation and preliminary effectiveness of a real-time pain management smartphone app for adolescents with cancer: A multicenter pilot clinical study. Pediatr Blood Cancer. 2017 Oct;64(10) doi: 10.1002/pbc.26554. [DOI] [PubMed] [Google Scholar]
- 25.Lengacher CA, Reich RR, Ramesar S, Alinat CB, Moscoso M, Cousin L, Marino VR, Elias MN, Paterson CL, Pleasant ML, Rodriguez CS, Wang H, Kip KE, Meng H, Park JY. Feasibility of the mobile mindfulness-based stress reduction for breast cancer (mMBSR(BC)) program for symptom improvement among breast cancer survivors. Psychooncology. 2018 Feb;27(2):524–531. doi: 10.1002/pon.4491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Bae WK, Kwon J, Lee HW, Lee S, Song E, Shim H, Ryu KH, Song J, Seo S, Yang Y, Park J, Lee KH, Han HS. Feasibility and accessibility of electronic patient-reported outcome measures using a smartphone during routine chemotherapy: a pilot study. Support Care Cancer. 2018 Nov;26(11):3721–3728. doi: 10.1007/s00520-018-4232-z. [DOI] [PubMed] [Google Scholar]
- 27.Oldenmenger WH, Baan MAG, van der Rijt CCD. Development and feasibility of a web application to monitor patients' cancer-related pain. Support Care Cancer. 2018 Feb;26(2):635–642. doi: 10.1007/s00520-017-3877-3. http://europepmc.org/abstract/MED/28929433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Smith SK, MacDermott K, Amarasekara S, Pan W, Mayer D, Hockenberry M. Reimagine: a randomized controlled trial of an online, symptom self-management curriculum among breast cancer survivors. Support Care Cancer. 2019 May;27(5):1775–1781. doi: 10.1007/s00520-018-4431-7. [DOI] [PubMed] [Google Scholar]
- 29.Devan H, Farmery D, Peebles L, Grainger R. Evaluation of Self-Management Support Functions in Apps for People With Persistent Pain: Systematic Review. JMIR Mhealth Uhealth. 2019 Feb 12;7(2):e13080. doi: 10.2196/13080. https://mhealth.jmir.org/2019/2/e13080/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Greenlee H, DuPont-Reyes MJ, Balneaves LG, Carlson LE, Cohen MR, Deng G, Johnson JA, Mumber M, Seely D, Zick SM, Boyce LM, Tripathy D. Clinical practice guidelines on the evidence-based use of integrative therapies during and after breast cancer treatment. CA Cancer J Clin. 2017 May 06;67(3):194–232. doi: 10.3322/caac.21397. doi: 10.3322/caac.21397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bradt J, Dileo C, Magill L, Teague A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst Rev. 2016 Aug 15;(8):CD006911. doi: 10.1002/14651858.CD006911.pub3. [DOI] [PubMed] [Google Scholar]
- 32.Kroenke K, Theobald D, Wu J, Norton K, Morrison G, Carpenter J, Tu W. Effect of telecare management on pain and depression in patients with cancer: a randomized trial. JAMA. 2010 Jul 14;304(2):163–71. doi: 10.1001/jama.2010.944. http://europepmc.org/abstract/MED/20628129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hernandez Silva E, Lawler S, Langbecker D. The effectiveness of mHealth for self-management in improving pain, psychological distress, fatigue, and sleep in cancer survivors: a systematic review. J Cancer Surviv. 2019 Feb;13(1):97–107. doi: 10.1007/s11764-018-0730-8. [DOI] [PubMed] [Google Scholar]
- 34.Sundararaman LV, Edwards RR, Ross EL, Jamison RN. Integration of Mobile Health Technology in the Treatment of Chronic Pain: A Critical Review. Reg Anesth Pain Med. 2017;42(4):488–498. doi: 10.1097/AAP.0000000000000621. [DOI] [PubMed] [Google Scholar]
- 35.Jongerius C, Russo S, Mazzocco K, Pravettoni G. Research-Tested Mobile Apps for Breast Cancer Care: Systematic Review. JMIR Mhealth Uhealth. 2019 Feb 11;7(2):e10930. doi: 10.2196/10930. https://mhealth.jmir.org/2019/2/e10930/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Rosser BA, Eccleston C. Smartphone applications for pain management. J Telemed Telecare. 2011;17(6):308–12. doi: 10.1258/jtt.2011.101102. [DOI] [PubMed] [Google Scholar]
- 37.Portelli P, Eldred C. A quality review of smartphone applications for the management of pain. Br J Pain. 2016 Aug;10(3):135–40. doi: 10.1177/2049463716638700. http://europepmc.org/abstract/MED/27583140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Martorella G, Boitor M, Berube M, Fredericks S, Le May S, Gélinas C. Tailored Web-Based Interventions for Pain: Systematic Review and Meta-Analysis. J Med Internet Res. 2017 Nov 10;19(11):e385. doi: 10.2196/jmir.8826. https://www.jmir.org/2017/11/e385/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Fridriksdottir N, Gunnarsdottir S, Zoëga S, Ingadottir B, Hafsteinsdottir EJG. Effects of web-based interventions on cancer patients' symptoms: review of randomized trials. Support Care Cancer. 2018 Feb;26(2):337–351. doi: 10.1007/s00520-017-3882-6. [DOI] [PubMed] [Google Scholar]
- 40.Schatz J, Schlenz AM, McClellan CB, Puffer ES, Hardy S, Pfeiffer M, Roberts CW. Changes in coping, pain, and activity after cognitive-behavioral training: a randomized clinical trial for pediatric sickle cell disease using smartphones. Clin J Pain. 2015 Jun;31(6):536–47. doi: 10.1097/AJP.0000000000000183. http://europepmc.org/abstract/MED/25503599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sundberg K, Wengström Y, Blomberg K, Hälleberg-Nyman M, Frank C, Langius-Eklöf A. Early detection and management of symptoms using an interactive smartphone application (Interaktor) during radiotherapy for prostate cancer. Support Care Cancer. 2017 Jul 24;25(7):2195–2204. doi: 10.1007/s00520-017-3625-8. http://europepmc.org/abstract/MED/28236145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Uhm KE, Yoo JS, Chung SH, Lee JD, Lee I, Kim JI, Lee SK, Nam SJ, Park YH, Lee JY, Hwang JH. Effects of exercise intervention in breast cancer patients: is mobile health (mHealth) with pedometer more effective than conventional program using brochure? Breast Cancer Res Treat. 2017 Feb;161(3):443–452. doi: 10.1007/s10549-016-4065-8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Search strategy to find literature on the use of apps for cancer pain management and interventions.