

Abstract
The population of Hawai‘i has traditionally been high in average fish consumption when compared to the national average. However, information is lacking on patterns of fish consumption among subpopulations. Data on fish consumption in the last 30 days from 11,293 adults was collected with the use of the Hawai‘i Health Survey (an annual telephone survey of households and household members) during the years 2007 and 2008 and weighted to represent the adult population of Hawai‘i. The US Department of Agriculture's, Environmental Protection Agency, and the United States Food and Drug Administration, recommend 8–12 ounces of fish per week for associated health benefits. Present estimates of fish consumption were skewed to the right (mean 10.5 and median 7.9 ounces) with some adults eating large amounts of fish per day and frequently. It may be of concern, given high amounts of methylmercury in select fish, that 13.7% of adults were eating fish 20 or more times per month. In addition, the serving size increased with increasing number of times per week fish was eaten.
The subpopulation variables examined included age, sex, marital status, education, ethnicity, poverty, and demographics representing the adults of Hawai‘i. The prevalence of adults consuming 8 or more ounces was highest for other than Honolulu counties, men, ages 18–74, married, with at least one year of college, Filipino and Native Hawaiian ethnicities (White, Japanese, Chinese, and All Others were also examined), employed, and adults living with higher income levels (lower poverty). However, only an estimated 46.9% of adults in Hawai‘i were eating the eight or more ounces of fish weekly. Prevalence was lowest for women, Chinese, age >74 years, and the City and County of Honolulu.
Adults who rated their general health better (excellent/good compared to fair/poor) were more likely to consume 8 or more ounces of fish per week, significantly for men. Men who rated their physical health higher and their mental health higher (via Optum SF™ Health Surveys) were associated with higher prevalence of consuming 8 or more ounces of fish per week. Higher consumption of the beneficial omega-3 fatty acids associated with fish low in methylmercury needs to be encouraged for those not meeting the recommended ounces of fish per week, particularly women, Chinese, older age groups, and adults living below the poverty level.
Keywords: fish consumption, per capita, canned tuna, methylmercury
Introduction
High Average Fish Consumption in Hawai‘i
Hawai‘i, with its multicultural population and location in the Pacific Ocean, is an ideal environment for assessing fish consumption patterns and associated health variables. Historically, average annual fish consumption estimates for the population of Hawai‘i (production plus imports minus exports of seafood) have been higher than the national average. The estimate for total per capita seafood consumption (excluding non-commercial catch; including resident civilian, military, and visitors) in Hawai‘i from 1970–1977 was 20.9 lbs/year (1.7 times higher than the national average).1 In 1983 consumption for Hawai‘i's population was 24 lbs/year (2 times higher the national average).2 And from 2000–2009 consumption in Hawai‘i was 28.5 lbs/year (1.8 times higher than the national average of commercial fish and shellfish).3,4 Two factors may have contributed to higher consumption in Hawai‘i: increasing visitors, and increasing number of immigrants from countries with higher fish consumption.4
Benefits of Eating Fish
Why eat fish or seafood? Seafood is a dietary source of omega-3 polyunsaturated fatty acids.5 Numerous health benefits have been associated with intake of omega-3 fatty acids by consuming fish, including decreased incidence of ischemic stroke, coronary heart disease (and related mortality), and dementia.6–8 Additionally, omega-3 fatty acids possess anti-inflammatory properties and may confer therapeutic benefits for individuals with chronic inflammatory health conditions such as rheumatoid arthritis.9
The omega-3 polyunsaturated fatty acids include alpha-linolenic acid (ALA) derived from plant oils, and eicosapentaenoic acid (EPA-acid) and docosahexaenoic acid (DHA) both originally derived from fish consuming phytoplankton that synthetize EPAacid and DHA. Even though reviews on fish oil and omega-3 fatty acids supplements that include EPA-acid and DHA have reported inconsistent findings on health benefits, the National Institute of Health's Office of Dietary Supplements has approved a ‘qualified’ health claim that fish and dietary supplements that contain omega-3 fatty acids, EPA-acid, and DHA, may reduce the risk of coronary heart disease.10
Amount of Fish
How much, how often, and what fish are best for consumption? Recommendations have evolved from the 2004 Environmental Protection Agency (EPA) and the FDA guidelines, which encouraged fish consumption and listed four types of fish to avoid to limit exposure to methymercury (tilefish, shark, swordfish, and king mackerel).11 Then in 2017, the EPA and the FDA updated guidelines and continued recommendations of 8–12 ounces of fish and grouped fish into consumption categories: “Best Choices” (2–3 servings per week, 8–12 oz/week), “Good Choices” (1 serving per week), and “Choices to Avoid”.12,13 However, recently, after a peer review, the recommendations are being revised. Recently, recommendations have been revised in 2019.14 Present advice recommends that women and children eat two to three servings of 8–12 ounces for adults and children >10, with smaller amounts for younger children. The advice includes eating a variety of fish and shellfish each week. A PDF chart showing how often to eat more than 60 types of fish and shellfish, can be downloaded.
The 2015–2020 Dietary Guidelines for Americans also recommend consumption of about 8 ounces per week of a variety of seafood, and for women 8–12 ounces per week from fish lower in methylmercury. Seafood that are higher in EPA-acid and DHA and lower in methylmercury are salmon, anchovies, herring, shad, sardines, Pacific oysters, trout, and Atlantic and Pacific mackerel (not King mackerel).5 Methylmercury is a neurotoxic compound that has been shown to have deleterious neurological health effects especially among children.15 The Hawai‘i Department of Health (DOH) has developed detailed fish consumption guidelines for pregnant women, nursing mothers and children based on mercury testing of locally caught fish.16,17
Table 1 summarizes advice for type of fish consumed in Hawai‘i, given the concerns of methylmercury, taken from information published by the DOH Women, Infants, and Children program (WIC).15 Advice includes eating 8–12 ounces of fish low in methylmercury every week for adults and children >10 years with children ≤10 eating smaller portions.
Table 1.
Hawai‘i Department of Health. A Local Guide to Eating Fish Safely. WIC Services Branch. 2012.15 https://health.Hawai‘i.gov/wic/files/2013/05/mercury.pdf
| Amount to Eat | |||
|---|---|---|---|
| Do Not Eat | No More Than Once Every Two Weeks |
No More Than Once a Week |
Anytime |
|
|
|
|
Goals
Given the health benefits of consuming fish, it is relevant to study patterns of fish consumption among Hawai‘i adults by demographics, ethnicity, and socio-economic variables. Previous measures of import and exports of seafood do not give estimates for segments of the population and provide only an overall measure. The Hawai‘i Health Survey (HHS) was used to provide information on the following questions;
What is the average fish consumption among adults in Hawai‘i and how does it compare to averages calculated for the nation as a whole?
Are all adults eating the recommended amount of fish or does consumption vary?
Is there an association between fish consumption and self-rated health?
Methods
Hawai‘i Health Survey (HHS)
The HHS is an annual survey of households and adults that are living in Hawai‘i that became a telephone survey in 1996 and, as an anonymous survey, is exempt from the Internal Review Board process (IRB, B. Woods, PhD, DOH IRB Administrator, Hawai‘i Department of Health, Email October 2018). In each household, a knowledgeable adult (≥ 18 years) was interviewed on their fish consumption for the last 30 days. The sample frame for the two study years (2007 and 2008) was all households with landline telephone service in the State of Hawai‘i. The Office of Health Status Monitoring (OHSM) contracted with SMS Research & Marketing Services, Inc. of Hawai‘i to conduct the survey using Computer-Assisted Telephone Interviewing (CATI) software. The sample totaled 11,293 adult respondents. Missing values for age (0.7%) and income (25%) were imputed using a hot-deck method.18 Other missing values were not imputed (fish consumption questions < 2.8% missing responses). Response rates to telephone-based surveys have been declining.19 The estimated response rates (Council of American Survey Research Organizations — CASRO) for landline telephones was 36% for the years measured.
Fish Consumption Questions
Respondents were questioned on the number of times fish was consumed in the last 30 days. Consumption was not significantly different by year and 2007 and 2008 data were combined. Both years included a question on the size of an average serving in ounces. Three ounces were compared to a deck of cards.20 Questions were also asked on concerns of eating fish from Hawai‘i and type of fish consumed (Appendix A Survey Questions).
Independent variables assessed included county, age, sex, education, marital status, employment, poverty, ethnicity/race, health insurance status, a general health question (part of the SF12 Survey®, Optum SF™ Health Surveys), and mental and physical component summary scores, calculated from the 12 questions on physical and emotional well-being (SF12 Survey ®).21 A higher score indicates a healthier score. Ethnicity was determined by questions on both parent ethnicities. Any Native Hawaiian was coded first, and if none the next ethnicity (other than White) for the father, and if none the next ethnicity (other than White) for the mother, and if none and White was present the respondent was coded White. The groups included Native Hawaiian, Chinese, Filipino, White, Japanese, and Other.
Percent poverty was calculated using the US Department of Health and Human Services poverty guidelines for Hawai‘i, household income, and household size. A higher value of percent poverty indicates higher income and/or lower household size. 22
Weighting Survey Data and Statistical Analysis
Sample data were weighted and adjusted for oversampling of islands other than O‘ahu, survey nonresponse, and age and sex strata to represent the adult population of Hawai‘i. SMS research used its population growth model to adjust Census population 2010 data for 2007 and 2008 estimates.23
The amount of fish consumed in an average week was calculated from the number of times fish was eaten in the last 30 days (divided by 30 and multiplied by 7) times the serving size. Results are presented as age-adjusted predicted marginal prevalence (%) and odds ratios of adults that consumed at least 8 or more ounces of fish per week (8orMFW). The cutoff for inclusion was a sample size of 50 respondents for the denominator and < 0.30 relative standard error for estimates.
Univariate age-adjusted logistic regression models for the binary outcome yes/no consumed 8orMFW were constructed for each independent variable with a logit- transformed probability. All statistical analyses were done with SAS/STAT® software 9.4 (SAS Institute, Inc., Cary, NC) and SUDAAN (version 11.0, Research Triangle Park, NC) software with significance set at α<.05 for a two-tailed test on weighted data.24,25
Results
Average Fish Consumption
The sample size was 11,293 adult respondents representing 947,521 adult residents in Hawai‘i in 2007 and 2008. An estimated 89.9% adults consumed at least some fish in the past 30 days. The average adult fish consumption was skewed to the right with many adults eating larger amounts of fish and frequently (mean 10.5 oz/week, 10.1–10.8 95% CI; median 7.9 oz/week, 7.3–8.6 95% CI). The average serving size increased with the number of times fish was eaten (Figure 1). Fish consumption for adults was converted from oz/week to lbs/year for comparison to historical estimates (mean 34.1 lbs/year, 33.0–35.3 95% CI).
Figure 1.
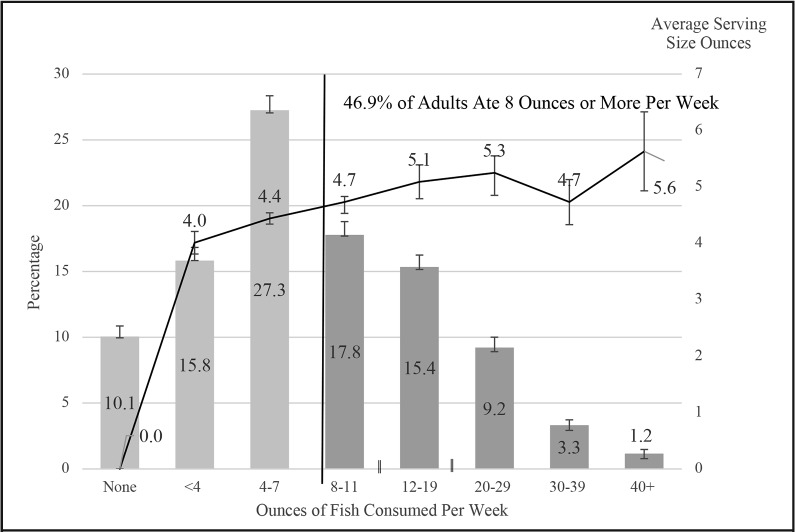
The Number of Times per Week in the Last 30 days Adults in Hawai‘i Ate Fish and Their Average Serving Size in Ounces (95% CI), Hawai‘i Health Survey 2007 and 2008 Weighted Average. DOH, OHSM
Patterns of Fish Consumption
Men's fish consumption was significantly higher than women's at P <.001 (Table 2). Consumption decreased significantly at and above 75 years for both men and women for both the mean and median. The highest prevalence for 8orMFW occurred for those who were living in counties other than Honolulu for both men and women (men P =.002, women P <.001), ages 18–74 years (both sexes significant at P <.001), adults that were employed (men P <.001, women P=.023), and women who were married (P=.013). Native Hawaiian and Filipino men (53.6% and 52.2%) had the highest prevalence of consuming 8orMFW (P=.030 for men's ethnicity) with the pattern reversed for women, Filipino 37.2%, Native Hawaiian 36.4% (P <.001 for women's ethnicity) (Table 3).
Table 3.
Age Adjusted Prevalence of Adults in Hawai–i by Sex that Ate 8 or More Ounces of Fish Per Week in the Last 30 Days by Demographic and Socio–economic Variables, Hawai–i Health Survey 2007 and 2008 Weighted Average
| Demographic Variables |
Men | Women | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Adj. Prevalence* |
95% CI | Odds Ratio | 95% CI | Wald F P–value |
Adj. Prevalence* |
95% CI | Odds Ratio | 95% CI | Wald F P–value |
|
| All Adults | 47.3% | (45.1–49.2) | 1.86 | (1.67–2.07) | <.001 33% | (31.2–34.2) | ||||
| County | ||||||||||
| Honolulu | 45.7% | (42.9–48.4) | referent | .002 | 30.5% | (28.6–32.5) | referent | <.001 | ||
| Hawai–i | 49.7% | (46.0–53.4) | 1.18 | (0.98–1.42) | 36.7% | (34.2–39.2) | 1.32 | (1.46–1.53) | ||
| Kaua–i | 55.1% | (50.0–60.1) | 1.47 | (1.16–1.86) | 37.4% | (33.9–40.9) | 1.36 | (1.42–1.63) | ||
| Maui | 52.4% | (48.7–56.1) | 1.32 | (1.09–1.59) | 37.1% | (34.5–39.8) | 1.35 | (1.16–1.56) | ||
| Age | ||||||||||
| 18–34 | 46.3% | (41.1–51.6) | 1.95 | (1.41–2.7) | <.001 | 30.5% | (26.6–34.6) | 1.56 | (1.19–2.04) | <.001 |
| 35–44 | 54.4% | (49.0–59.6) | 2.69 | (1.94–3.7) | 32.3% | (29.0–35.9) | 1.70 | (1.33–2.18) | ||
| 45–54 | 48.6% | (44.6–52.6) | 2.13 | (1.59–2.9) | 38.4% | (35.4–41.5) | 2.22 | (1.76–2.79) | ||
| 55–64 | 49.8% | (46.1–53.6) | 2.24 | (1.68–3.0) | 36.4% | (33.6–39.3) | 2.04 | (1.63–2.55) | ||
| 65–74 | 44.9% | (40.1–49.7) | 1.84 | (1.34–2.5) | 29.3% | (26.1–32.7) | 1.48 | (1.15–1.89) | ||
| ≥ 75 | 30.7% | (25.8–36.1) | referent | 21.9% | (18.9–25.3) | referent | ||||
| Marital Status | ||||||||||
| Married | 49.3% | (46.6–52.0) | 1.19 | (0.99–1.41) | .057 | 34.1% | (32.2–36.0) | 1.21 | (1.04–1.40) | .013 |
| All Other | 45.1% | (41.9–48.5) | referent | 30.0% | (27.6–32.6) | referent | ||||
| Education | ||||||||||
| None–11th Grade | 46.2% | (35.3–57.4) | referent | .340 | 28.6% | (22.6–35.4) | referent | .110 | ||
| HS Grad/GED | 47.7% | (43.5–51.9) | 1.06 | (0.65–1.73) | 31.1% | (28.3–34.2) | 1.13 | (0.81–1.59) | ||
| College 1–>4 Years | 49.0% | (46.3–51.8) | 1.12 | (0.70–1.79) | 33.9% | (32.1–35.8) | 1.29 | (0.93–1.78) | ||
| <25 Years | 39.4% | (30.6–49.0) | 0.76 | (0.41–1.41) | 27.5% | (20.3–36.1) | 0.94 | (0.56–1.60) | ||
| Ethnicity/Race | ||||||||||
| Native Hawaiian/Part | 53.6% | (48.5–58.7) | 1.55 | (1.02–2.36) | .030 | 36.4% | (33.0–39.9) | 1.51 | (1.05–2.18) | <.001 |
| Filipino | 52.2% | (45.8–58.4) | 1.46 | (0.94–2.29) | 37.2% | (33.0–41.6) | 1.56 | (1.07–2.29) | ||
| Japanese | 48.6% | (43.9–53.4) | 1.27 | (0.85–1.90) | 26.3% | (23.5–29.4) | 0.94 | (0.65–1.35) | ||
| White | 44.4% | (41.0–47.9) | 1.07 | (0.73–1.57) | 32.2% | (29.7–34.8) | 1.25 | (0.88–1.77) | ||
| Chinese | 42.8% | (34.4–51.7) | referent | 27.6% | (21.5–34.6) | referent | ||||
| Other | 44.4% | (37.9–51.1) | 1.07 | (0.68–1.68) | 34.7% | (29.4–40.3) | 1.40 | (0.92–2.12) | ||
| Employment | ||||||||||
| Employed | 51.1% | (48.4–53.9) | 1.56 | (1.26–1.92) | <.001 | 34.1% | (32.0–36.3) | 1.21 | (1.03–1.42) | .023 |
| Not Employed | 40.3% | (36.4–44.3) | referent | 30.0% | (27.6–32.6) | referent | ||||
| Poverty | ||||||||||
| Below Poverty – Poor <100% |
39.0% | (30.4–48.4) | referent | .051 | 29.1% | (24.1–34.6) | referent | .140 | ||
| Near Poor 100–199% | 43.5% | (37.9–49.2) | 1.20 | (0.76–1.90) | 29.7% | (26.0–33.7) | 1.03 | (0.75–1.42) | ||
| Middle and High Income >199% |
48.6% | (46.3–50.9) | 1.49 | (1.00–2.22) | 33.2% | (31.5–34.9) | 1.21 | (0.93–1.59) | ||
| Health Insurance Plan | ||||||||||
| Private Insurance Plan/ Military Tricare |
49.3% | (46.8–51.8) | 1.32 | (1.01–1.73) | .046 | 32.8% | (31.1–34.5) | 1.01 | (1.01–1.30) | .828 |
| Quest, Medicaid | 40.2% | (32.9–47.9) | 0.91 | (0.61–1.36) | 30.2% | (24.7–36.4) | 0.90 | (0.62–1.31) | ||
| Medicare | 47.7% | (40.9–54.5) | 1.24 | (0.85–1.80) | 31.3% | (26.7–36.2) | 0.95 | (0.68–1.30) | ||
| Uninsured/ Other | 42.4% | (36.7–48.3) | referent | 32.5% | (27.6–37.9) | referent | ||||
Adjusted for age. Hawai–i Health Survey, DOH, OHSM
Adults who ranked their general health as excellent/very good/good compared to fair/poor had higher prevalence of consuming 8orMFW at P =.015 for men and P=.023 for women (Table 4). A higher mental health score was associated with consuming higher 8orMFW for men (P=.047).
Table 4.
Logistic Regression of Adults in Hawai‘i by Sex that Ate 8 or More Ounces of Fish Per Week in the Last 30 Days by Health Variables, Hawai‘i Health Survey 2007 and 2008 Weighted Average
| Health Variable |
Men | Women | ||||||||
| Adj. Prevalence* |
95% CI | Odds Ratio | 95% CI | Wald F P-value |
Adj. Prevalence* |
95% CI | Odds Ratio | 95% CI | Wald F P-value |
|
| General Health | ||||||||||
| Excellent | 49.4% | (44.9–53.9) | 1.51 | (1.14–2.01) | .015 | 34.0% | (30.7–37.5) | 1.26 | (0.99–1.59) | .023 |
| Very Good | 48.7% | (44.8–52.5) | 1.47 | (1.22–1.93) | 35.3% | (32.5–38.1) | 1.33 | (1.07–1.65) | ||
| Good | 48.5% | (45.0–51.9) | 1.46 | (1.13–1.89) | 30.8% | (28.4–33.3) | 1.08 | (0.88–1.34) | ||
| Fair/Poor | 39.3% | (34.2–44.7) | referent | 29.1% | (25.6–32.9) | referent | ||||
| Mental Health | ||||||||||
| > 1 SD above mean | 46.9% | (42.7–51.1) | 1.32 | (0.91–1.92) | .047 | 32.8% | (29.5–36.3) | 0.96 | (0.71–1.30) | .983 |
| Mean +1 SD | 50.0% | (47.1–52.8) | 1.50 | (1.05–2.13) | 32.6% | (30.6–34.6) | 0.95 | (0.72–1.25) | ||
| Mean − 1 SD | 43.6% | (38.2–49.1) | 1.15 | (0.77–1.73) | 33.0% | (29.5–36.8) | 0.97 | (0.71–1.320 | ||
| > 1 SD below mean | 40.1% | (32.5–48.3) | referent | 33.7% | (28.2–39.7) | referent | ||||
| Physical Health | ||||||||||
| > 1 SD above mean | 51.5% | (40.1–62.6) | 1.38 | (0.82–2.33) | .104 | 33.1% | (25.1–42.2) | 1.11 | (0.71–1.71) | .689 |
| Mean +1 SD | 49.2% | (46.6–51.7) | 1.26 | (0.97–1.63) | 33.4% | (31.5–35.3) | 1.12 | (0.91–1.39) | ||
| Mean – 1 SD | 43.9% | (39.4–48.5) | 1.02 | (0.76–1.37) | 31.9% | (28.8–35.2) | 1.05 | (0.82–1.33) | ||
| > 1 SD below mean | 43.5% | (37.7–49.4) | referent | 30.9% | (27.0–35.2) | referent | ||||
Concerns of Eating Fish and Type of Fish Consumed
Among adults surveyed, 22% listed concerns about consuming fish with the most common concerns mercury (11.4%), ciguatera poisoning (9.3%), pollution (6.8%), and parasites (0.9%). In contrast, higher fish consumption was associated with adults listing concerns (age and gender adjusted, P=.002). Estimates of type of fish consumed indicated 25% was canned tuna, 66% from fresh ocean fish, and 9% fish from freshwater lakes and streams.
Discussion
Total Consumption
Fish are an important part of the diet throughout the Asia-Pacific region and Hawai‘i is no exception with self-reported adult mean fish consumption estimated at 34.1 lbs/year (33.0–35.3 95% CI) comparable (although methods differ) to the 2000–2009 estimate for Hawai‘i of average per capita live weight pounds of seafood consumption at 36.9 lbs/year (commercial and non-commercial).4
These data support that adults in Hawai‘i on average consume more fish than adults on the mainland. The island heritage and cultural heritage of Asian and Pacific Islanders may play a part in the higher total consumption compared to the national average. The mean ounces of fish consumption per day for the adult population of Hawai‘i for age ≥21 years is approximately 3.2 times higher and the median 2.6 times higher in comparison to the 2003–2010 National Health and Nutrition Examination Survey (NHANES- survey data using total usual prepared weight finfish consumption for adults ≥21 years and a complex statistical methodology).26
The Native Hawaiian raw fish dish, poke, may play a part in increased consumption of fish. Also, consumption of canned tuna may account for part of the increased consumption in Hawai‘i as canned tuna was 25% of the total consumption for Hawai‘i compared to the national average at 17% for the same years (2007 and 2008).27 Greater consumption of canned tuna is concerning as canned tuna (canned and fresh) was one of the dominant seafood contributing to the edible supply of seafood and associated methylmercury intake in the nation.28
Hawai‘i's adults in comparison to other Pacific Islands, as measured by the Food and Agriculture Organization (FAO) household survey study, are low in average fish consumption compared to islands such as Tuvalu (with the highest consumption per capita at 244 lbs/year) and Samoa (the next highest at 142 lbs/year). The adult consumption in Hawai‘i measured by the HHS was comparable to Papua New Guinea with an average of 28.7 lbs/year per capita.29 Consumption may be lower in Hawai‘i due to influence of ethnicities other than Pacific Islanders and Asian and the high cost of living.
Subpopulation Fish Consumption
Information on fish consumption by ethnicity in the nation is limited especially among Asian and Pacific Islander groups that are often grouped into ‘other’ or not included as a separate category for analysis.30 When Asians and Pacific Islanders have been included in surveys they have had high rates of consumption compared to other groups.31,32 In the present study, Native Hawaiians, with the unique history of herding fish and cultivating baby fish in Hawaiian fish ponds had the highest prevalence for men consuming 8orMFW and the second highest for women (53.6% and 36.4%). Filipino men had the second highest prevalence for men and for women the highest prevalence of consuming 8orMFW (52.2% and 37.2%). Chinese and Other ethnicities had the lowest consumption of 8orMFW for men, (42.8% and 44.4%), Japanese, and Chinese for women (26.3% and 27.6%). That Chinese consume less fish than Filipinos has also been found in the FAO household survey study for the Asia-Pacific region where Filipinos consumed more than four times the amount of fish than the Chinese per capita.29 However, using fish consumption calculations from capture and aquaculture, fish utilization, and international trade to calculate apparent fish consumption the pattern was reversed with Chinese consuming more than Filipinos.33
Numbers from the 2003–2008 National Health and Nutrition Examination Survey (NHANES) on fish consumption also indicated an average fish consumption below recommended levels (and lower in women than men).34 The mean usual intake of total fish was 0.61 ± 0.03 oz/day and the median was 0.43 oz/day (equivalent to a mean of 4.3 oz/week and a median of 3.0 oz per week), both below the recommended amount. Data indicated people from older age groups ate more fish, however, ages ≥51 were combined and it is impossible to tell fish consumption by smaller age groups. The 2003–2010 NHANES study found, as in the present study, lower fish consumption for ages ≥65.25 Of particular concern is the low fish intake among women of reproductive age.
It is possible that pregnant and nursing women avoided eating fish due to local and national public health advisories regarding mercury and other contaminants.35 Advisories on fish risks usually outweigh the information presented for the benefits.36 Data from the HHS indicated over 20% of adults in Hawai‘i were concerned about eating fish, and the top concern was mercury. The concerns are warranted given two studies in Hawai‘i found that higher mercury levels in humans were associated with higher fish consumption.37,38 Although, research has suggested that contaminants in fish (especially among long-lived predatory species) are a legitimate concern for women of child-bearing age, the benefits of regular fish consumption likely outweigh the potential health risks.39 DHA is important for normal brain development during the fetal and infantile stages, as well as supporting brain function throughout life.40 It has been suggested that it is especially important for adults with children or grandchildren to understand the importance of omega-3 fatty acid intake because CVD risk factors may develop in childhood and can be reversible.41
The NHANES 2003–2010 study revealed lower income and education levels were associated with lower fish consumption. The decreased consumption with lower income and lower education was attributed to the correlation of income and education. It was hypothesized that cost, perceived, or real, may be a barrier to consumption of seafood.25
The present study also supports the contention that adults with a higher economic status (education above a high school degree, lower level of poverty, and employed) are associated with higher consumption of fish comparable to other studies.25,42 Purchased fish may be out of the price range of many adults in Hawai‘i. Fish portion sizes increased with the frequency of eating fish. Because seafood is an important staple in most Polynesian and Asian cultures, larger fish portions, in addition to higher frequency of fish consumption may be of concern. Many adults were consuming large quantities of fish; 13.7% of adults ate ≥20 ounces of fish per week. Eating higher amounts than recommended levels may have dangerous health effects given that select fish have potentially high methylmercury levels.
A healthier ranking in self-reported general health for both sexes and a higher MCS-12 score for men were associated with higher prevalence of eating the recommended 8orMFW per week. An association of mental health and higher consumption of fish has also been noted in other studies.43 It is difficult to conclude the benefits are from the omega-3 content of the fish or seafood, other components of the seafood, substitution of fish for less healthful foods, a healthier lifestyle, or a combination of factors.11 The association of healthier self-rated health with fish consumption does not imply causation and may be more associated with a healthier life style and higher economic status.
Increasing Fish Consumption
Boosting fish consumption is complicated and may involve factors other than promoting health-related beliefs and consumer knowledge.44 Will there be enough fish to supply our population if everyone ate the recommended amount of fish? There has been a history of overexploitation of fish populations, however, efforts to restore marine fisheries ecosystems and promote aquaculture have been increasing. There have been advances in managing and sustaining fish populations worldwide that provide hope for ensuring sustainability.45 In addition, detailed information on the complicated subject of which fish to eat can be considered from many points of view including toxicological, nutritional, ecological, and economic and advice is offered on multiple sites.11–13,46,47 Increasing omega-3 fatty acids by supplementation, food additives, or other alternate food sources may provide an alternative to fish consumption but the data are mixed on benefits. The American Heart Association's advisory concluded that physicians should consider prescribing fish oil to patients with recent coronary heart disease, a heart attack, or with prevalent heart failure with reduced left ventricular function.48 However, a recent meta-analysis of 10 clinical trials concluded omega-3 fatty acid supplements do little to protect patients from cardiovascular or heart disease.49 Improved diets with greater fish consumption and previous treatment may have reduced the effect of subsequently adding fish oil supplements.50 Notably, clinical trials have been underway to further study Vitamin D and/or Omega-3 supplements.51,52 The ASCEND trial reports no significant risk of serious vascular events between those participants (with diabetes but without evidence of cardiovascular disease) who received n-3 fatty acid supplementation and a placebo.53 The VITAL and other Vitamin D trials showed a significant reduction in cancer mortality but not for incidence of cancer or cardiovascular endpoints. Additional research is needed to determine who would benefit from vitamin D supplementation.54
It is recommended that all adults, especially the elderly and women, eat the recommended amount of fish, (at least 8orMFW) but also limit fish consumption to recommended levels and types of fish to reduce intake of methylmercury.14
Limitations
The survey is a point-in-time collection of data. Reporting and recall errors in the frequency and serving size of fish consumed were likely present during the collection of the data. Bias may be introduced as households without landlines or adults with cell phones only were not included and the bias may be different for different communities or subpopulations. Given that in 2008 adults ≥65 years had the highest percentage of landline only phones55 and in the HHS data lower fish consumption estimates, present estimates may be biased toward lower estimates of fish consumption. Also, rounding the estimates of fish consumption per week and the number of ounces may introduce error. The present report does not include types of fish and thus does not have information on mercury exposure. Native Hawaiians and other ethnicities in Hawai‘i consume poke, raw fish mixed with other ingredients. However, whether the fish was raw or cooked was not asked. Because raw fish is cubed, it may be difficult to accurately estimate serving size.
Conclusion
Average fish intake among adults in Hawai‘i was higher than for adults nationally. Consuming the recommended 8orMFW was higher for counties other than Honolulu, men, ages <75 years, married, Native Hawaiian, Filipino, and employed adults. Importantly, the present study found an association of higher self-rated health and higher prevalence of 8orMFW for both men and women. Fish consumption was associated with economic status (higher prevalence for married, college educated, employed, and low poverty — higher income adults). Thus, commercial sources of fish may be beyond the price range of lower income families.
Although the benefits and potential risks of fish consumption are well known and recommended consumption suggestions have been well established, fish consumption for many adults in Hawai‘i remains well below the recommended intakes. It is an important health concern that 53.1% of adults in Hawai‘i are not consuming the recommended amount of fish per week. Increased consumption of fish (species low in methylmercury) is recommended especially for women of childbearing age, elderly, and lower income adults.
Table 2.
Ounces of Fish Consumed Per Week in the Last 30 Days for Adults in Hawai‘i by Age and Sex, Hawai‘i Health Survey 2007 and 2008 Weighted Average
| Men | ||||||
|---|---|---|---|---|---|---|
| Age | Mean | 95% CI | P-value* | Median | 95% CI | P-value** |
| Total | 12.4 | (11.8–13.0) | 7.9 | (7.0–8.7) | <.001 | |
| 18–34 | 12.6 | (11.0–14.2) | <.001 | 7.0 | (5.8–8.3) | |
| 35–44 | 13.6 | (12.1–15.2) | <.001 | 9.5 | (8.3–11.3) | |
| 45–54 | 12.9 | (11.7–14.1) | <.001 | 8.2 | (7.1–9.3) | |
| 55–64 | 12.5 | (11.5–13.4) | <.001 | 8.2 | (7.4–9.3) | |
| 65–74 | 11.7 | (10.3–13.0) | .001 | 7.2 | (6.3–8.3) | |
| ≥ 75 | 8.5 | (7.3–9.7) | referent | 5.1 | (4.2–6.0) | |
| Women | ||||||
| Age | Mean | 95% CI | P-value* | Median | 95% CI | P-value** |
| Total | 8.6 | (8.2–9.0) | 5.2 | (4.9–5.6) | <.001 | |
| 18–34 | 8.5 | (7.3–9.6) | .007 | 3.8 | (3.4–5.2) | |
| 35–44 | 8.8 | (7.9–9.7) | <.001 | 5.2 | (4.4–5.6) | |
| 45–54 | 9.7 | (8.9–10.6) | <.001 | 5.9 | (5.5–7.0) | |
| 55–64 | 8.8 | (8.2–9.4) | <.001 | 5.4 | (5.2–6.1) | |
| 65–74 | 7.9 | (7.2–8.6) | .014 | 4.9 | (4.4–5.3) | |
| ≥ 75 | 6.6 | (5.9–7.3) | referent | 3.8 | (3.5–4.3) | |
P-value Wald F
P-value Chi-Square
P-value <.001 for mean of men compared to women for both mean and median
Abbreviations
- 8orMFW
8 or more ounces of fish per week
- CVD
Cardiovascular disease
- DHA
docosahexaenoic acid
- DOH
Hawai‘i Department of Health
- EPA
Environmental Protection Agency
- EPA-acid
eicosapentaenoic acid
- FDA
Food and Drug Administration
- HHS
Hawai‘i Health Survey
- MCS-12
Mental health, Mental Component Summary Score, Optum SF™ Health Surveys
- NHANES
National Health and Nutrition Examination Survey
- OHSM
Office of Health Status Monitoring
- PCS-12
Physical health, Physical Component Summary Score, Optum SF™ Health Surveys
Appendix A. Survey Questions
2007 and 2008 Questions on Fish Consumption
Alright, now a few questions about your diet. Whether it is breakfast, lunch, or dinner - canned, frozen, or fresh. How many times did you eat fish in the last 30 days?
-
How many times in the last 30 days did you eat large, fresh fish from the ocean?
Fish like Ahi, Mahimahi, Aku, or Swordfish.
How many times in the last 30 days did you eat small fish from Hawai‘i freshwater lakes and streams? Fish like Tilapia, Barracuda, Papio.
How many times in the last 30 days did you eat canned tuna?
When you eat fish how large a serving, in ounces do you eat? 3 ounces is about the size and thickness of a deck of playing cards or a computer mouse.
-
Have you ever been concerned about eating fish in Hawai‘i?
Yes
No
Do not know
Refused
-
What are your concerns?
Mercury
Parasites
Chemical contamination
Sewage contamination
Ciguatera
Other [SPECIFY]
Do not know
Refused
Contributor Information
Kathleen Kromer Baker, Office of Health Status Monitoring, Hawai‘i Department of Health, Honolulu HI; Office of Public Health Studies, University of Hawai‘i at Manoa, Honolulu, HI (KKB).
James E. Dannemiller, SMS Research, Honolulu HI (JED).
Barbara A. Brooks, Hazard Evaluation Emergency Response Office, Environmental Health Administration State Toxicology (BAB).
Conflict of Interest
None of the authors identify any conflict of interest.
References
- 1.Hudgins LL. Per capita annual utilization and consumption of fish and shellfish in Hawai‘i, 1970-77. Mar Fish Rev. 1980;42((2)):16–20. https://www.researchgate.net/publication/322555088_Per_capita_annual_utilization_and_consumption_of_fish_and_shellfish_in_Hawaii_1970-77_USA. Accessed May 15, 2016. [Google Scholar]
- 2.Pooley SG, Cooper JC. Seafood Consumption and Exports Are Up in Hawai‘i. NOAA/NMFS Developments. Mar Fish Rev. 1983;45((1)):18. https://spo.nmfs.noaa.gov/sites/default/files/pdf-content/mfr4513.pdf. Accessed December 20, 2016. [Google Scholar]
- 3.Geslani C, Loke M, Takenaka B, Leung PS. Hawaii's Seafood Consumption and its Supply Source. Pelagic Fisheries Research Program. SOEST 2012-01 JIMAR Contribution. :12–379. [Google Scholar]
- 4.Loke M, Geslani C, Takenaka B, Leung P. An overview of seafood consumption and supply sources: Hawai‘i versus US. UH-TAHR Economic Issues. 2012;22:1–9. https://www.researchgate.net/publication/259864527_An_Overview_of_Seafood_Consumption_and_Supply_Sources_Hawaii_versus_US. Accessed June 18, 2016. [Google Scholar]
- 5.U.S. Department of Health and Human Services and U.S. Department of Agriculture 2015%#x2013;2020 Dietary Guidelines for Americans. 2015. http://health.gov/dietaryguidelines/2015/guidelines/. Accessed December 20, 2017.
- 6.He K, Song Y, Daviglus ML, et al. Fish consumption and incidence of stroke: a meta-analysis of cohort studies. Stroke. 2004;35:1538–1542. doi: 10.1161/01.STR.0000130856.31468.47. [DOI] [PubMed] [Google Scholar]
- 7.Torris C, Smastuen MC, Molin M. Nutrients in Fish and Possible Associations with Cardiovascular Disease Risk Factors in Metabolic Syndrome. Nutrients. 2018 Jul;10((7)):952. doi: 10.3390/nu10070952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Raji CA, Erickson KI, Lopez OL, et al. Regular Fish Consumption and Age-Related Brain Gray Matter Loss. Am J Prev Med. 2014;47((4)):444–451. doi: 10.1016/j.amepre.2014.05.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Goldberg R, Katz J. A meta-analysis of the analgesic effects of omega-3 polyunsaturated fatty acid supplementation for inflammatory joint pain. Pain. 2007;129:210–223. doi: 10.1016/j.pain.2007.01.020. [DOI] [PubMed] [Google Scholar]
- 10.National Institutes of Health, Office of Dietary Supplements. U.S. Department of Health and Human Services Omegas-3 fatty acids, fact sheet for health professionals. https://ods.od.nih.gov/factsheets/Omega3FattyAcids-HealthProfessional/ Accessed June 18, 2018.
- 11.Food and Drug Administration – Environmental Protection Agency. Advisor (Online Advisory). What You Need to Know About Mercury in Fish and Shellfish (Brochure). March 2004. EPA-823-R-04-005. https://www.fda.gov/food/metals/what-you-need-know-about-mercury-fish-andshellfish. Accessed December 7, 2018.
- 12.Food and Drug Administration. US Department of Human Services Eating Fish: What Pregnant Women and Parents Should Know. 2017. https://www.fda.gov/Food/ResourcesForYou/Consumers/ucm393070.htm Accessed November 7, 2018.
- 13.US Environmental Protection Agency Choose Fish and Shellfish Wisely: Federal Advisory on Mercury in Fish and Shellfish. https://www.epa.gov/choose-fish-and-shellfish-wisely Accessed February 18, 2018.
- 14.US Environmental Protection Agency EPA-FDA. Advice about Eating Fish and Shellfish. https:// www.epa.gov/fish-tech/epa-fda-advice-about-eating-fish-and-shellfish Accessed November 19, 2019.
- 15.Grandjean P, Pichery C, Bellanger M, Budtz-Jørgensen E. Calculation of mercury's effect on neurodevelopment. Environ Health Perspect. 2012;120((12)):A452. doi: 10.1289/ehp.1206033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hawai‘i Department of Health A local guide to eating fish safely. WIC Services Branch. 2012. Jul, https://health.Hawai‘i.gov/wic/files/2013/05/mercury.pdf. Accessed July 18, 2016.
- 17.Kaneko JJ, Takenaka B, Bartram P. Keeping Hawai‘i seafood safe to eat. Hawai‘i Seafood Council. Hawai‘i Seafood Safety Project, March 31, 2005, Honolulu, Hawai‘i USA. https://www.Hawai‘i-seafood.org/seafood-safety/ Accessed September 2, 2016. [Google Scholar]
- 18.Andridge RR, Little RJA. A review of hot deck imputation for survey non-response. Int Stat Rev. 2010;78((1)):40–64. doi: 10.1111/j.1751-5823.2010.00103.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.The Pew Research Center for People and the Press Assessing the Representativeness of Public Opinion Surveys website. 2012. http://www.people-press.org/2012/05/15/assessingthe-representativeness-of-public-opinion-surveys/. Accessed November 20, 2016.
- 20.BreastCancer.org Portion Size. https://www.breastcancer.org/tips/nutrition/healthy_eat/portions. Accessed June 18, 2019.
- 21.Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220. doi: 10.1097/00005650-199603000-00003. https://www.ncbi.nlm.nih.gov/pubmed/8628042. Accessed September 16, 2018. [DOI] [PubMed] [Google Scholar]
- 22.US Department of Health and Human Services U.S. Federal Poverty Guidelines Used to Determine Financial Eligibility for Certain Federal Programs. https://aspe.hhs.gov/povertyguidelines. Accessed June 18, 2011.
- 23. 2008 Hawaii Health Survey Procedure Manual, Hawaii Department of Health, SMS Research and Marketing Services, Inc. August 2009.
- 24.SAS Institute Inc. SAS/ACCESS® 9.4 Cary, NC: SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc. in the USA and other countries. ® indicates USA registration. SAS Institute Inc. 2013.
- 25.Research Triangle Park, NC: Research Triangle Institute; 2014. SUDAAN User's Manual. RTI. Release 11.0. [Google Scholar]
- 26.2014. HANES 2003-2010 Estimated Fish Consumption Rates for the U.S. Population and selected Subpopulations. EPA-820-R-14-002. https://www.epa.gov/fish-tech/estimated-fish-consumption-rates-reports. Accessed September 22, 2015. [Google Scholar]
- 27. Office of Science and Technology, Fisheries Statistics Division. National Marine Fisheries Service, Fisheries of the United States 2014. https://www.st.nmfs.noaa.gov/commercial-fisheries/fus/fus14/index. Accessed September 15, 2018.
- 28.Sunderland EM, Li M, Bullard K. Decadal Changes in the Edible Supply of Seafood and Methylmercury Exposure in the United States. Environ Health Persp. 2018;126((1)):017006. doi: 10.1289/EHP2644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Needham S, Funge-Smith SJ. 2014. The consumption of fish and fish products in the Asia-Pacific region based on household surveys. FAO Regional Office for Asia and the Pacific, Bangkok, Thailand. RAP Publication. 2015;12:87. http://www.fao.org/apfic/publications/detail/en/c/396958/. Accessed June 18, 2018. [Google Scholar]
- 30.Jahns L, Raatz SK, Johnson LK, Kranz S, Silverstein JT, Picklo MJ., Sr. Intake of Seafood in the US Varies by Age, Income, and Education Level but Not by Race-Ethnicity. Nutrients. 2014;6((12)):6060–6075. doi: 10.3390/nu6126060.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mahaffey K.R., Clickner R.P., Jeffries R.A. Adult women's blood mercury concentrations vary regionally in the United States: Association with patterns of fish consumption (NHANES 1999–2004) Environ Health Persp. 2009;117:47–53. doi: 10.1289/ehp.11674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sechena R, Liao S, Lorenzana R, Nakano C, Polissar N, Fenske R. Asian American and Pacific Islander seafood consumption – a community-based study in King County, Washington. J Expo Sci Env Epid. 2003;13:256–266. doi: 10.1038/sj.jea.7500274. [DOI] [PubMed] [Google Scholar]
- 33.Food and Agriculture Association FAO. 2016. The State of World Fisheries and Aquaculture 2016. Contributing to food security and nutrition for all. Rome. 2016:1–200. [Google Scholar]
- 34.Papanikolaou Y, Brooks J, Reider C, Fulgoni VL III. U.S. adults are not meeting recommended levels for fish and omega-3 fatty acid intake. Results of an analysis using observational data from NHANES 2003–2008. Nutr J. 2014;13:31. doi: 10.1186/1475-2891-13-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Oken E, Kleinman KP, Berland WE, Simon SR, Rich-Edwards JW, Gillman MW. Decline in Fish Consumption Among Pregnant Women After a National Mercury Advisory. Obstet Gynecol. 2003;102((2)):346–351. doi: 10.1016/S0029-7844(03)00484-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Scherer AC, Tsuchiya A, Younglove LR, Burbacher TM, Faustman EM. Comparative Analysis of State Fish Consumption Advisories Targeting Sensitive Populations. Environ Health Persp. 2008 Dec;116((12)):1598–1606. doi: 10.1289/ehp.11372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sato RL, Li GG, Shaha S. Antepartum Seafood Consumption and Mercury Levels in Newborn Cord Blood. Am J Obstet Gynecol. 2006;194((6)):1683–8. doi: 10.1016/j.ajog.2006.03.005. [DOI] [PubMed] [Google Scholar]
- 38.Soon R, Dye TD, Ralston NV, Berry MJ, Sauvage LM. Seafood consumption and umbilical cord blood mercury concentrations in a multiethnic maternal and child health cohort. BMC Pregnancy Childb. 2014;14:209. doi: 10.1186/1471-2393-14-209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mozzaffarian D, Rimm EB. Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA. 2006;296((15)):1885–1899. doi: 10.1001/jama.296.15.1885. [DOI] [PubMed] [Google Scholar]
- 40.Innis S. Dietary (n-3) fatty acids and brain development. J Nutr. 2007;137:855–859. doi: 10.1093/jn/137.4.855. [DOI] [PubMed] [Google Scholar]
- 41.Rodrigues AN, Abreu GR, Resende RS, Goncalves WLS, Alves Gouvea S. Cardiovascular risk factor investigation: a pediatric issue. Int J Gen Med. 2013;6:57–66. doi: 10.2147/IJGM.S41480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Barberger G P, Jutand MA, Letenneur L, Larrieu S, Tavernier B, Berr C, 3C Study Group Correlates of regular fish consumption in French elderly community dwellers: data from the Three-City study. Eur J Clin Nutr. 2005;59((7)):817–25. doi: 10.1038/sj.ejcn.1602145. [DOI] [PubMed] [Google Scholar]
- 43.Silvers KM, Scott KM. Fish consumption and self-reported physical and mental health status. Public Health Nutr. 2002 Jun;5((3)):427–431. doi: 10.1079/PHNPHN2001308. [DOI] [PubMed] [Google Scholar]
- 44.Pieniak Z., Verbeke W., Scholderer J. Health-related beliefs and consumer knowledge as determinants of fish consumption. J Hum Nutr Diet. 2010;23:480–488. doi: 10.1111/j.1365-277X.2010.01045.x. [DOI] [PubMed] [Google Scholar]
- 45.Gordon TAC, Harding HR, Clever FK, et al. Fishes in a changing world: learning from the past to promote sustainability of fish populations. J Fish Biol. 2018 Mar;92((3)):804–827. doi: 10.1111/jfb.13546. [DOI] [PubMed] [Google Scholar]
- 46.Hawai‘i Seafood. Seafood and Health. Hawai‘i-Seafood.org v1.7.4a. 2015. https://www.Hawai‘iseafood.org/seafood-health/
- 47.Oken E, Choi AL, Karagas MR, et al. Which Fish Should I Eat? Perspectives Influencing Fish Consumption Choices. Environ Health Persp. 2012;120((6)):790–798. doi: 10.1289/ehp.1104500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Siscovick DS, Barringer TA, Fretts AM, Wu JH, Lichtenstein AH, et al. Omega-3 Polyunsaturated Fatty Acid (Fish Oil) Supplementation and the Prevention of Clinical Cardiovascular Disease. A Science Advisory from the American Heart Association. Circulation. 2017;135:e867–e884. doi: 10.1161/CIR.0000000000000482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Aung T, Halsey J, Kromhout D, et al. Associations of Omega-3 Fatty Acid Supplement Use with Cardiovascular Disease Risks Meta-analysis of 10 Trials Involving 77 917 Individuals. JAMA Cardiol. 2018;3((3)):225–234. doi: 10.1001/jamacardio.2017.5205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Abbasi J. Another Nail in the Coffin for Fish Oil Supplements. JAMA. 2018;319((18)):1851–1852. doi: 10.1001/jama.2018.2498. [DOI] [PubMed] [Google Scholar]
- 51.US National Library of Medicine ASCEND: A Study of Cardiovascular Events In Diabetes. ClinicalTrials.gov Identifier: NCT00135226.
- 52.US National Library of Medicine Vitamin D and Omega-3 Trial (VITAL) ClinicalTrials.gov Identifier: NCT01169259.
- 53.ASCEND Study Collaborative Group. Bowman L, Mafham M, Wallendszus K, Stevens W, Buck G, Barton J, Murphy K, Aung T, Haynes R, Cox J, Murawska A, Young A, Lay M, Chen F, Sammons E, Waters E, Adler A, Bodansky J, Farmer A, McPherson R, Neil A, Simpson D, Peto R, Baigent C, Collins R, Parish S, Armitage J. Effects of n-3 Fatty Acid Supplements in Diabetes Mellitus. N Engl J Med. 2018 Oct 18;379((16)):1540–1550. doi: 10.1056/NEJMoa1804989. Epub 2018 Aug 26. [DOI] [PubMed] [Google Scholar]
- 54.Manson JE, Bassuk SS, Buring JE, VITAL Research Group Principal Results of the VITamin D and OmegA-3 TriaL (VITAL) and Updated Meta-analyses of Relevant Vitamin D Trials. J Steroid Biochem Mol Biol. 2019 Nov;13:105522. doi: 10.1016/j.jsbmb.2019.105522. [Epub ahead of print] Review. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Rosentiel T, Keeter S. Research Roundup: Latest Findings on Cell Phones and Polling. Research Roundup: Latest Findings on Cell Phones and Polling. Pew Research Center. Numbers, Facts and Trends Shaping Your World. May 22, 2008. http://www.pewresearch.org/2008/05/22/research-roundup-latest-findings-on-cell-phones-and-polling/