

Abstract
OBJECTIVE
To evaluate the translation of a paper high-risk checklist for pediatric intensive care unit (PICU) patients at risk of clinical deterioration to an automated clinical decision support tool.
DESIGN
Retrospective, observational cohort study of an automated clinical decision support tool, the PICU Warning Tool, adapted from a paper checklist to predict clinical deterioration events in PICU patients within 24-hours.
SETTING
Two quaternary care medical-surgical PICUs—The Children’s Hospital of Philadelphia and Cincinnati Children’s Hospital Medical Center.
PATIENTS
The study included all patients admitted from July 1, 2014 through June 30, 2015, the year prior to the initiation of any focused situational awareness work at either institution.
INTERVENTIONS
We replicated the predictions of the real-time PICU Warning Tool by retrospectively querying the institutional data warehouse to identify all patients that would have flagged as high-risk by the PICU Warning Tool for their index deterioration.
MEASUREMENTS
The primary exposure of interest was determination of high-risk status during PICU admission via the PICU Warning Tool. The primary outcome of interest was clinical deterioration event within 24 hours of a positive screen. The date and time of the deterioration event was used as the index time point. We evaluated the sensitivity, specificity, positive and negative predictive value of the performance of the PICU Warning Tool.
MAIN RESULTS
There were 6233 patients evaluated with 233 clinical deterioration events experienced by 154 individual patients. The positive predictive value of the PICU Warning Tool was 7.1% with a number needed to screen of 14 patients for each index clinical deterioration event. The most predictive of the individual criteria were elevated lactic acidosis, high mean airway pressure, and profound acidosis.
CONCLUSIONS
Performance of a clinical decision support translation of a paper-based tool showed inferior test characteristics. Improved feasibility of identification of high-risk patients using automated tools must be balanced with performance.
Keywords: Clinical decision support systems, cardiopulmonary resuscitation, clinical deterioration, pediatric intensive care units
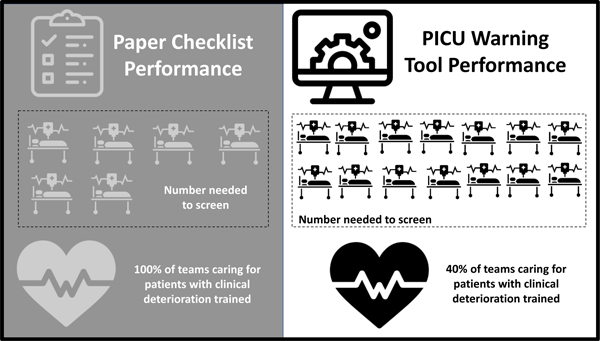
Graphical Abstract
INTRODUCTION
In children’s hospitals, most cardiopulmonary resuscitation (CPR) events occur in pediatric intensive care units (PICUs).1 Many children who require CPR die during or shortly after the event, and those who survive are often left with new disabilities.2–6 Identifying the children most likely to require CPR is important because evidence based interventions currently exist to improve their outcomes. Examples include “just in time” CPR training, team based simulation, and bundles for tracheal intubation.7–14
Our conceptual framework for identifying and improving outcomes for the PICU patients most likely to require CPR is based on the principles of risk mitigation through situational awareness.15 Situational awareness is the ability to monitor and recognize cues that increase the awareness of what is happening around you, integrate information to develop a comprehensive picture of the current state, and extrapolate forward to determine if the knowledge obtained will adversely influence the situation immediately or in the near future.16,17 The improvement of situational awareness within the PICU and development of mitigation plans to prevent CPR events is predicated on the accurate early identification of high-risk patients.
The baseline method used to identify PICU patients most likely to require CPR at the study hospitals was based on clinician intuition alone; patients that were of concern to attending physicians were identified followed by discussion of these patients twice daily at situational awareness huddles. This approach had a poor positive predictive value and a problematic number needed to screen of 37–45 patients for each clinical deterioration event, defined as a cardiac arrest or a code bell activation with response of the unit code team. Number needed to screen (NNS) is analogous to number needed to treat. This number signifies the number of patients labeled as high-risk (potentially leading providers to institute mitigation plans or receive just in time training) for each patient who experienced a clinical deterioration event. As a first step to improve the identification of high-risk PICU patients, we developed a paper checklist of factors with excellent sensitivity and specificity and a NNS of 6 patients for each clinical deterioration event.18 Despite the accuracy of the paper checklist, we found that a major barrier to implementation was the time needed to manually screen the criteria for each patient.
Due to this implementation barrier, we shifted our focus to adapting the paper checklist into an automated electronic health record (EHR)-based clinical decision support tool, the PICU Warning Tool. Our aim was to examine the retrospective test characteristics of the PICU Warning Tool with a pragmatic approach to the tradeoffs between predictive accuracy and the effort required to implement.
MATERIALS AND METHODS
Study Design
We performed a retrospective observational cohort study to evaluate the performance of a replicated version of the PICU Warning Tool to predict clinical deterioration events in PICU patients within a 24-hour window following a positive high-risk screen. The Institutional Review Boards of CCHMC and CHOP approved this study.
Setting
The study PICUs are tertiary care pediatric medical/surgical ICUs with 55 and 35 beds respectively and combined yearly admissions of over 6000 patients/year with a baseline clinical deterioration rate of 2–3% of all PICU patients. The cardiac surgical ICU and neonatal ICU were excluded.
Selection of the Cohort
The study included all patients admitted to the PICU at The Children’s Hospital of Philadelphia (CHOP) and Cincinnati Children’s Hospital Medical Center (CCHMC) from July 1, 2014 through June 30, 2015, the year prior to the initiation of any focused situational awareness work at either institution. No patients were excluded.
The primary exposure of interest was determination of high-risk status during PICU admission via the PICU Warning Tool. The primary outcome of interest was clinical deterioration event within 24 hours of a positive screen. The date and time of the deterioration event was used as the index time point. Only the initial deterioration event was included for each patient as the goal of the PICU Warning Tool was to establish initial situational awareness for high-risk patients. This also accounted for multiple sampling.
Identification of High-Risk Patients
The primary exposure of interest was high-risk patient status as determined by the automated PICU Warning Tool. The original paper-based checklist, on which the PICU Warning Tool is based, included 15 equally weighted single parameter high-risk patient factors that predicted clinical deterioration events.18 We began the process with a review of the paper checklist to determine if the items were computable and translatable into an automated clinical decision support tool. Some criteria were excluded because the data were not reliably recorded as discrete elements, or were not documented at all, such as “provider intuition.” While documentation fields could be added to the EHR to capture these missing elements, we chose to build a system without requiring any additional clinical documentation in order to meet the clinical decision support best practice of integration into existing workflows.19 Due to these limitations, we excluded five of the original criteria and modified others (Table 1). We added a criterion for severe cardiac dysfunction in an attempt to capture an additional high-risk population that was lost due to the excluded criteria; we have further described this process and its adherence to clinical decision support best practices in a prior manuscript.20
Table 1:
Review of original paper checklist criteria and translation to PICU Warning Tool
| Criterion | Definition or adaptation* in PICU Warning Tool, or reason for exclusion | |
|---|---|---|
| Unchanged | High Mean Airway Pressure | Mean airway pressure sustained greater than 20 cm H20 for at least 2 hours |
| Extracorporeal Membrane Oxygenation (ECMO) | Any patient receiving veno-venous or veno-arterial ECMO (up to 24 hours post decannulation) | |
| Adapted | Pulmonary Hypertension | Most recent nitric oxide gas value > 5 parts per million AND • Active pulmonary hypertension on problem list OR • Received medication indicating pulmonary hypertension in prior 24 hours |
| Use of two vasoactive medications OR high dose single drug | Medication Administration Record within the last 6 hours of: • Any dose of phenylephrine, dobutamine, or vasopressin • Any two of the following: dopamine, epinephrine, or norepinephrine • Epinephrine or norepinephrine with dose>0.1 mcg/kg/min • Dopamine with dose >5 mcg/kg/min |
|
| Traumatic Brain Injury | • Sustained elevated intracranial pressure > 20 for most recent 2 hours • 3% saline or mannitol bolus in prior 6 hours for high ICP |
|
| PICU Initiated Renal Replacement Therapy | First 5 hours on CRRT and first 5 hours off of CRRT | |
| Potassium >7.0 | Two consecutive potassium laboratory values >7 mmol/L (resulted with the last 24 hours) | |
| pH<7.1 | Most recent pH laboratory value (resulted within the past 24 hours)<7.1 | |
| Lactate>10 | Most recent lactate laboratory result >10 mmol/L | |
| Added | Severe Cardiac Dysfunction | • Mixed venous saturation<60% without 2 consecutive values >70% within the last 24 hours OR • Milrinone infusion within the previous 6 hours |
| Excluded | Stage 1 Hypoplastic Left Heart Repair in Past 24 hours | HLH patients not cared for in the study PICUs |
| Recent life-threatening event requiring code team activation or cardiac arrest | No standardized EHR documentation of events | |
| Intubation/Extubation of known difficult or critical airway | Difficult or critical airway is reliably captured at both institutions, intubation not documented until post procedure. | |
| Provider Intuition | Concern on the part of an attending physician that a patient is high-risk regardless of criteria met cannot be captured in an automated fashion. | |
| Anticipated tracheal intubation of known diagnosis of myocarditis | Tracheal intubations are only documented post procedure. |
Adaptations noted in italics
We replicated the predictions of the real-time PICU Warning Tool by retrospectively querying the institutional data warehouse to identify all patients that would have flagged as high-risk by the PICU Warning Tool, as well as the specific criteria that caused the patient to be identified as high-risk. The EHR was screened hourly for patients meeting high-risk criteria per the established definitions. Patients who met any single criteria were considered high-risk patients.
Identification of Patients who Experienced Clinical Deterioration
The outcome of interest was clinical deterioration event within 24 hours of a positive high-risk screen by the PICU Warning Tool. Clinical deterioration was defined as a cardiac arrest or a code bell activation with response of the unit code team. These events were identified through multiple means including the use of a quality improvement database in place at the time of the study that tracked CPR and respiratory emergency events (CHOP), an electronic log of code button presses with manual chart review (CCHMC), and a review of all code sheets documented during that time period (CHOP, CCHMC).
Data Analysis
We evaluated the sensitivity, specificity, positive and negative predictive value of the overall performance of the PICU Warning Tool to retrospectively identify patients who would experience clinical deterioration within 24 hours of a positive screen. A second sensitivity analysis evaluated the test characteristics of the PICU Warning Tool to predict a clinical deterioration event at any point during a patient’s PICU admission following a positive high-risk flag. Secondary analysis included standard diagnostic test characteristics of individual components of the EHR-based PICU Warning Tool including likelihood ratios, sensitivity, specificity, positive predictive value, and negative predictive value of each component within the combined data set from both institutions and evaluated separately. Categorical variables between institutions were compared using the chi-square test or Fisher’s exact test.
RESULTS
A total of 6233 patients were evaluated between the two centers. There was a total of 233 clinical deterioration events experienced by 154 individual patients (2.5%). At CCHMC, 3.7% of patients (83 out of 2241 total patients) experienced a clinical deterioration event and 21.6% (485 out of 2241 total patients) met high-risk criteria during their PICU stay. At CHOP, 1.8% of patients (71 out of 3992 total patients) experienced clinical deterioration and 9.6% (385 out of 3992 total patients) met high-risk criteria during their PICU stay (Figure 1). Both the number of clinical deterioration events and the percent of patients meeting high-risk criteria were significantly different at the two institutions (p<0.0001 for both).
Figure 1:
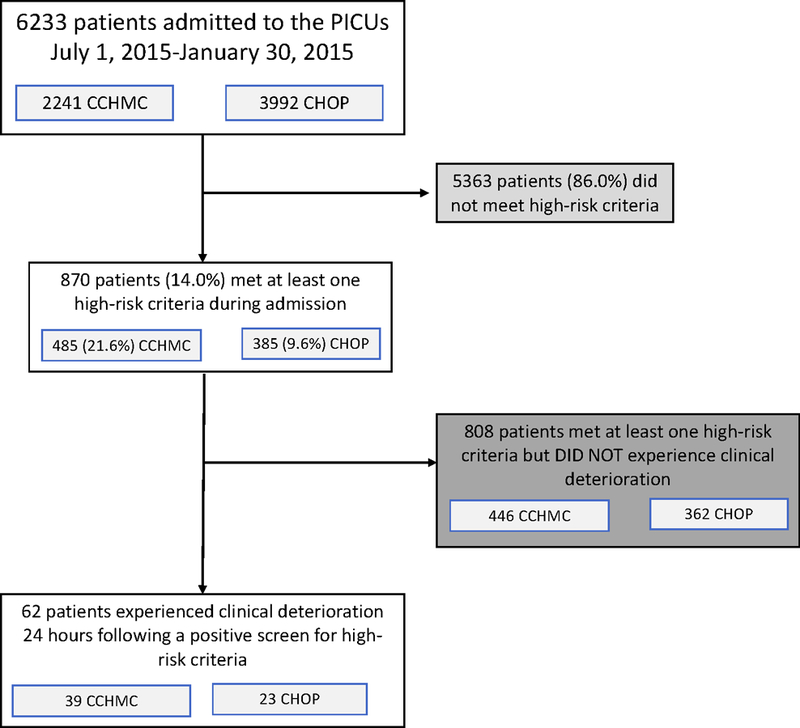
Cohort Identification
The percent of patients meeting individual high-risk criteria was also different between centers for three of the criteria—pulmonary hypertension, high mean airway pressure, and profound acidosis (Table 2). The highest frequency criteria was vasoactive shock at both centers followed by profound acidosis and high mean airway pressure.
Table 2:
Percent of patients meeting individual high-risk criteria by center
| Criteria | % of High Risk Patients who Met Criteria (N)*) | % of CCHMC High Risk Patients who Met Criteria (N)*) | % of CHOP High Risk Patients who Met Criteria (N)*) | P-Value |
|---|---|---|---|---|
| ECMO | 1.1% (10) | 0.6% (3) | 1.8% (7) | 0.10 |
| Hyperkalemia | 2.6% (23) | 1.9% (9) | 3.6% (14) | 0.12 |
| Renal Replacement Therapy | 4.4% (38) | 3.9% (19) | 4.9% (19) | 0.47 |
| Pulmonary Hypertension | 4.7% (41) | 3.3% (16) | 6.5% (25) | 0.03 |
| Lactic Acidosis | 5.3% (46) | 4.1% (20) | 6.8% (26) | 0.08 |
| Intracranial Hypertension | 12.6% (110) | 12.0% (58) | 14.5% (56) | 0.28 |
| Severe Cardiac Dysfunction | 25.7% (224) | 26.4% (128) | 24.9% (96) | 0.62 |
| High Mean Airway Pressure | 26.6% (231) | 21.0% (102) | 33.5% (129) | <0.01 |
| Profound Acidosis | 30.0% (261) | 34.0% (165) | 24.9% (96) | 0.004 |
| Vasoactive Shock | 48.2% (419) | 50.3% (244) | 45.5% (175) | 0.16 |
Total number of high risk patients=870, CCHMC high risk patients=485, CHOP high risk patients=385
The overall positive predictive value of the EHR-based tool was 7.1% (95% CI: 5.9–8.6%) with a NNS of 14 patients (95% CI: 12–17) for each index clinical deterioration event. The tool performed with a PPV of 8.0% and a NNS of 13 at CCHMC as compared to CHOP with a PPV of 6.0% and a NNS of 17. All of these test characteristics were inferior to the original paper-based tool with a positive predictive value of 17.3% and an NNS of 6 (Table 3).
Table 3:
Test Characteristics of the electronic PICU Warning Tool at each center and overall as compared with the original paper based tool.
| Test Characteristics | CHOP | CCHMC | Overall | Paper Checklist |
|---|---|---|---|---|
| Sensitivity (95% CI) | 32.4% (21.8–44.6%) | 47.0% (35.6–58.3%) | 40.3% (32.5–48.5%) | 100.0% |
| Specificity (95% CI) | 90.8% (89.8–91.6%) | 79.3% (77.6–81.0%) | 86.7% (85.8–87.6%) | 97.7% |
| PPV (95% CI) | 6.0% (4.3–8.3%) | 8.0% (6.4–10.0%) | 7.1% (5.9–8.6%) | 17.3% |
| NPV (95% CI) | 98.7% (98.4–98.9%) | 97.5% (97.0–98.0%) | 98.3% (98.1–98.5%) | 100% |
| NNS (95% CI) | 17 (12–23) | 13 (10–16) | 14 (12–17) | 6 |
The predictive value of the individual criteria varied. The most predictive of the individual criteria was elevated lactic acidosis with a positive likelihood ratio (LR) of 6 (95% CI: 2.6–13.9), high mean airway pressure had a positive LR of 4.8 (95% CI: 3.3–7.0) and profound acidosis had a positive LR of 3.6 (95% CI: 2.4–5.5) (Figure 2). The least predictive were ECMO and hyperkalemia which did not accurately predict any clinical deterioration events followed by intracranial hypertension with a positive LR of 1 (95% CI: 0.2–2.9). Pulmonary hypertension only predicted clinical deterioration at CHOP and renal replacement therapy only predicted clinical deterioration events at CCHMC.
Figure 2:
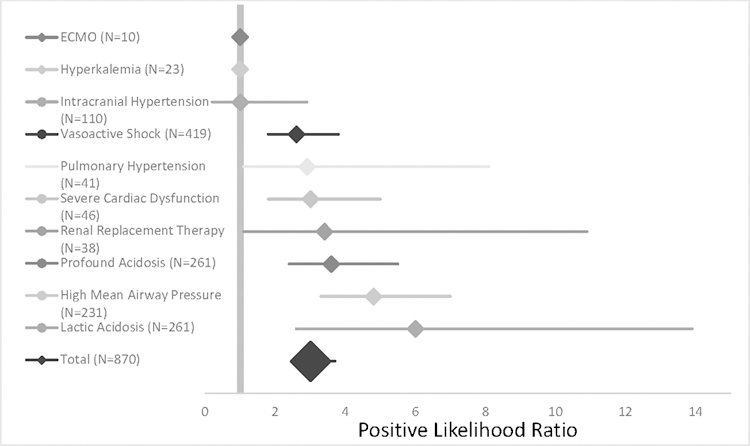
Positive likelihood ratios with confidence limits for individual criteria and overall for prediction.
Sensitivity Analysis
To predict clinical deterioration at any point following a positive screen during the patient’s PICU admission, the PICU Warning Tool had improved test characteristics with a sensitivity of 60.4% (95% CI: 52.2% to 68.2%), specificity of 87.2% (95% CI: 86.3–88.0%), positive predictive value 10.7% (9.4%−12.1%), negative predictive value of 98.9% (95% CI:98.6–99.1%), and a number needed to screen of 10 (95% CI: 9–11).
DISCUSSION
Using data from two institutions, we evaluated the performance of an automated clinical decision support tool, the PICU Warning Tool, derived from a previously published single center paper checklist. The key findings of this study were that, with adaptation from paper to automated to ease screening, the sensitivity decreased from 100% to 40% to predict clinical deterioration within 24 hours of a positive high-risk screen, and the NNS increased from 6 to 14. As a practical example, using the PICU Warning Tool rather than the paper checklist, a 30-bed PICU with yearly admissions of 2000 patients would have on average five high-risk patients per week requiring mitigation planning and just in time training. However, this would only train the teams of 40% of patients who would experience clinical deterioration within 24 hours and 60% of patients who would experience clinical deterioration during their PICU admission. Using the paper checklist, this same PICU would have on average one high-risk patient per week requiring just in time training and would train 100% of the teams caring for patients who experience clinical deterioration. While this example may overestimate the performance of the paper checklist in a real-life setting, as it was only studied over a three-month period at a single center, it does raise important concerns about the often unstudied conversion from a paper based clinical decision support tool to an automated one.
To summarize, in adapting the tool from paper to electronic, we eliminated the workload burden of manual screening but markedly reduced the tool’s sensitivity and more than doubled the NNS. Depending on the recommended action associated with screening positive, this could increase providers’ workload burden of developing mitigation plans or delivering just in time training, limiting its feasibility and acceptability. More standard situational awareness improvements around structured communication tools21, standardized handoffs22, and huddles16,23 are likely feasible for most centers with a NNS of 14 patients for each clinical deterioration event. However, more intensive training centered around individual at-risk patients5,8,24 and team based simulations12–14 may not be feasible at this NNS. It is important to note that although we have focused on individual level patient identification and mitigation, prior work demonstrates that with improved situational awareness and a proactive approach to identify high-risk patients, improvements can be seen in prevention of high-risk events at a systems level.23,25–27
This difference in test characteristics identified here demonstrates the importance of evaluating the translation from paper to automated clinical decision support tools. Optimizing the human-automation interaction may lead to improved outcomes in this context. Prior literature demonstrates that automation does not replace the human activity but changes it in planned and unplanned ways.28 To the extent to which the clinical decision support automation provides the right information at the right time, it can decrease the team workload and improve the team situational awareness.29 While the performance of the automated tool may be inferior to that of the paper tool, our use of clinical decision support best practices19,30,31 and our implementation plan for effective automation design32, may lead to improved patient outcomes despite the higher NNS.
We speculate that the decrease in sensitivity and increase in NNS is likely related to the removal of components that are known to be predictive including high-risk intubations33 and prior clinical deterioration events.34 In addition, provider intuition (i.e. identification of high-risk patients by physician judgement) has been shown to be more predictive than early warning scores alone when completed by attendings.35 As the original evaluation of the paper checklist did not include evaluation of the individual criteria, it was not possible for us to know a priori the impact of removing these elements. It is reasonable to study the addition of these criteria to the future prospective implementation of this tool to see if we are able to improve the sensitivity of the PICU Warning Tool using a combined automated screening component and a manual entry component from those criteria identified during huddle.
This work has several limitations. First, the retrospective evaluation of this automated clinical decision support tool was completed at only two centers, and the frequency of deterioration events at these centers was low. External validation in a larger number of pediatric centers is important prior to widespread adoption. Second, this data was collected retrospectively. Although designed to mimic the real-time queries of the prospective tool, there may have been missed indications due to documentation errors such as incorrect documentation of a patient’s mean airway pressure or diagnosis in the problem list. Lastly, we only evaluate the first clinical deterioration event of each patient. It is possible the predictability of the tool changes with subsequent events.
We will next implement and study the PICU Warning Tool as a prospective high-risk patient identifier on its impact on clinical deterioration rate. To improve the performance of the tool, we plan to add the missing criteria through manual identification to investigate if the sensitivity of the PICU Warning Tool increases using combined automated screening and manual entry of criteria identified twice daily during safety huddle. As we decrease the prevalence of clinical deterioration events, the positive predictive value will fall and the NNS of the tool will rise. It will therefore be imperative that we track additional outcomes including situational awareness among team members, use of mitigation plans, and quality of resuscitation response in addition to predictive ability.
Conclusions
An automated clinical decision support translation of a paper checklist for PICU patients at risk for clinical deterioration demonstrates reduced accuracy in prediction with a NNS of 14 rather than 6 despite improved feasibility. We speculate that improved feasibility of identification of high-risk patients using automated EHR warning tools may allow for risk mitigation and just in time preparation and that test characteristics may improve with incorporation of more provider and procedural concerns.
Supplementary Material
ACKNOWLEDGMENTS:
This work was supported in part by an American Academy of Pediatrics Section of Critical Care Small Project Award and the Cincinnati Children’s Hospital Medical Center Place Outcomes Research Award. The study sponsors had no role in the study design, collection, analysis, and interpretation of data, in the writing of the manuscript, nor in the decision to submit the manuscript for publication.
Copyright form disclosure: Dr. Dewan’s institution received funding from American Academy of Pediatrics Section of Critical Care Small Project Award and Cincinnati Children’s Hospital Medical Center Place Outcomes Research Award, and she received support for article research from the National Institutes of Health (NIH). Dr. Muthu’s institution received funding from Agency for Healthcare Research and Quality (AHRQ) and Pew Charitable Trusts, and he received funding from Phrase Health. Dr. Brady’s institution received funding from AHRQ and NIH. Dr. Kirkendall received funding from American Academy of Pediatrics, Council on Clinical Information Technology (reimbursed for travel costs/hotels for executive meetings); Goodis, Thompson and Miller, PA (expert legal case review); and VigiLanz (licensing royalties for software). Dr. Wolfe received funding from Zoll Medical (speaking honoraria).
Footnotes
The remaining authors have disclosed that they do not have any potential conflicts of interest.
REFERENCES
- 1.Berg RA, Sutton RM, Holubkov R, et al. Ratio of PICU versus ward cardiopulmonary resuscitation events is increasing. Crit Care Med 2013;41(10):2292–2297. doi: 10.1097/CCM.0b013e31828cf0c0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sutton RM, French B, Niles DE, et al. 2010 American Heart Association recommended compression depths during pediatric in-hospital resuscitations are associated with survival. Resuscitation 2014;85(9):1179–1184. doi: 10.1016/j.resuscitation.2014.05.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cheng A, Lin Y, Nadkarni V, et al. The effect of step stool use and provider height on CPR quality during pediatric cardiac arrest: A simulation-based multicentre study. CJEM April 2017:1–9. doi: 10.1017/cem.2017.12 [DOI] [PubMed] [Google Scholar]
- 4.Abella BS, Edelson DP, Kim S, et al. CPR quality improvement during in-hospital cardiac arrest using a real-time audiovisual feedback system. Resuscitation 2007;73(1):54–61. doi: 10.1016/j.resuscitation.2006.10.027 [DOI] [PubMed] [Google Scholar]
- 5.Niles DE, Nishisaki A, Sutton RM, et al. Improved Retention of Chest Compression Psychomotor Skills With Brief “Rolling Refresher” Training. Simul Healthc 2017;12(4):213–219. doi: 10.1097/SIH.0000000000000228 [DOI] [PubMed] [Google Scholar]
- 6.Lin Y, Wan B, Belanger C, et al. Reducing the impact of intensive care unit mattress compressibility during CPR: a simulation-based study. Adv Simul 2017;2(1):22. doi: 10.1186/s41077-017-0057-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sutton RM, Niles D, Meaney PA, et al. Low-dose, high-frequency CPR training improves skill retention of in-hospital pediatric providers. Pediatrics 2011;128(1):e145–51. doi: 10.1542/peds.2010-2105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Niles D, Sutton RM, Donoghue A, et al. “Rolling Refreshers”: a novel approach to maintain CPR psychomotor skill competence. Resuscitation 2009;80(8):909–912. doi: 10.1016/j.resuscitation.2009.04.021 [DOI] [PubMed] [Google Scholar]
- 9.Sutton RM, Niles D, Meaney PA, et al. “Booster” training: evaluation of instructor-led bedside cardiopulmonary resuscitation skill training and automated corrective feedback to improve cardiopulmonary resuscitation compliance of Pediatric Basic Life Support providers during simulated cardiac . Pediatr Crit Care Med 2011;12(3):e116–21. doi: 10.1097/PCC.0b013e3181e91271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wolfe H, Zebuhr C, Topjian AA, et al. Interdisciplinary ICU cardiac arrest debriefing improves survival outcomes*. Crit Care Med 2014;42(7):1688–1695. doi: 10.1097/CCM.0000000000000327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Parker MM, Nuthall G, Brown C 3rd, et al. Relationship Between Adverse Tracheal Intubation Associated Events and PICU Outcomes. Pediatr Crit Care Med 2017;18(4):310–318. doi: 10.1097/PCC.0000000000001074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Knight LJ, Gabhart JM, Earnest KS, Leong KM, Anglemyer A, Franzon D. Improving code team performance and survival outcomes: implementation of pediatric resuscitation team training. Crit Care Med 2014;42(2):243–251. doi: 10.1097/CCM.0b013e3182a6439d [DOI] [PubMed] [Google Scholar]
- 13.Stewart C, Shoemaker J, Keller-Smith R, Edmunds K, Davis A, Tegtmeyer K. Code Team Training: Demonstrating Adherence to AHA Guidelines During Pediatric Code Blue Activations. Pediatr Emerg Care October 2017. doi: 10.1097/PEC.0000000000001307 [DOI] [PubMed] [Google Scholar]
- 14.Gilfoyle E, Koot DA, Annear JC, et al. Improved Clinical Performance and Teamwork of Pediatric Interprofessional Resuscitation Teams With a Simulation-Based Educational Intervention. Pediatr Crit Care Med 2017;18(2):e62–e69. doi: 10.1097/PCC.0000000000001025 [DOI] [PubMed] [Google Scholar]
- 15.Brady PW, Wheeler DS, Muething SE, Kotagal UR. Situation awareness: A new model for predicting and preventing patient deterioration. Hosp Pediatr 2014. doi: 10.1542/hpeds.2013-0119 [DOI] [PubMed] [Google Scholar]
- 16.Goldenhar LM, Brady PW, Sutcliffe KM, Muething SE, Anderson JM. Huddling for high reliability and situation awareness. BMJ Qual Saf 2013;22:899–906. doi: 10.1136/bmjqs-2012-001467 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Endsley MR. Measurement of Situation Awareness in Dynamic Systems. Hum Factors J Hum Factors Ergon Soc 1995;37(1):65–84. doi: 10.1518/001872095779049499 [DOI] [Google Scholar]
- 18.Niles DE, Dewan M, Zebuhr C, et al. A pragmatic checklist to identify pediatric ICU patients at risk for cardiac arrest or code bell activation. Resuscitation 2016;99:33–37. doi: 10.1016/j.resuscitation.2015.11.017 [DOI] [PubMed] [Google Scholar]
- 19.Bates DW, Kuperman GJ, Wang S, et al. Ten Commandments for Effective Clinical Decision Support : Making the Practice of Evidence-based Medicine a Reality. J Am Med Informatics Assoc 2003;10(6):523–530. doi: 10.1197/jamia.M1370.Although [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shelov E, Muthu N, Wolfe H, et al. Design and Implementation of a Pediatric ICU Acuity Scoring Tool as Clinical Decision Support. Appl Clin Inf 2018;09(03):576–587. doi: 10.1055/s-0038-1667122 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Haig KM, Sutton S, Whittington J. SBAR: A shared mental model for improving communication between clinicians. Jt Comm J Qual Patient Saf 2006. doi: 10.1016/S1553-7250(06)32022-3 [DOI] [PubMed] [Google Scholar]
- 22.Starmer AJ, Sectish TC, Simon DW, et al. Rates of medical errors and preventable adverse events among hospitalized children following implementation of a resident handoff bundle. JAMA - J Am Med Assoc 2013. doi: 10.1001/jama.2013.281961 [DOI] [PubMed] [Google Scholar]
- 23.Brady PW, Muething S, Kotagal U, et al. Improving situation awareness to reduce unrecognized clinical deterioration and serious safety events. Pediatrics 2013;131(1):e298–308. doi: 10.1542/peds.2012-1364 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Cheng A, Brown LL, Duff JP, et al. Improving cardiopulmonary resuscitation with a CPR feedback device and refresher simulations (CPR CARES Study): a randomized clinical trial. JAMA Pediatr 2015;169(2):137–144. doi: 10.1001/jamapediatrics.2014.2616 [DOI] [PubMed] [Google Scholar]
- 25.Hueckel RM, Turi JL, Cheifetz IM, Mericle J, Meliones JN, Mistry KP. Beyond Rapid Response Teams: Instituting a “Rover Team” Improves the Management of At-Risk Patients, Facilitates Proactive Interventions, and Improves Outcomes; 2008. [PubMed] [Google Scholar]
- 26.Sandquist M, Tegtmeyer K. No more pediatric code blues on the floor: evolution of pediatric rapid response teams and situational awareness plans. Transl Pediatr 2018;7(4):291–298. doi: 10.21037/tp.2018.09.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McClain Smith M, Chumpia M, Wargo L, Nicol J, Bugnitz M. Watcher Initiative Associated With Decrease in Failure to Rescue Events in Pediatric Population. Hosp Pediatr 2017;7(12):710–715. doi: 10.1542/hpeds.2017-0042 [DOI] [PubMed] [Google Scholar]
- 28.Nickerson RS. Reviews of Human Factors and Ergonomics, Volume I. Ergon Des Q Hum Factors Appl 2011. doi: 10.1177/106480460601400208 [DOI] [Google Scholar]
- 29.Wright MC, Kaber DB. Effects of automation of information-processing functions on teamwork. Hum Factors 2005;47(1):50–66. doi: 10.1518/0018720053653776 [DOI] [PubMed] [Google Scholar]
- 30.Osheroff J, Teich J, Levick D, et al. Improving Outcomes with Clinical Decision Support: An Implementer’s Guide 2nd ed. Chicago, IL: Healthcare Information and Management Systems Society (HIMSS); 2012. [Google Scholar]
- 31.Wright A, Phansalkar S, Bloomrosen M, et al. Best Practices in Clinical Decision Support. Appl Clin Inform 2010;1(3):331–345. doi: 10.4338/ACI-2010-05-RA-0031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Klein G, Woods DD, Bradshaw JM, Hoffman RR, Feltovich PJ. Ten challenges for making automation a “team player” in joint human-agent activity. IEEE Intell Syst 2004. doi: 10.1109/MIS.2004.74 [DOI] [Google Scholar]
- 33.Graciano AL, Tamburro R, Thompson AE, Fiadjoe J, Nadkarni VM, Nishisaki A. Incidence and associated factors of difficult tracheal intubations in pediatric ICUs: a report from National Emergency Airway Registry for Children: NEAR4KIDS. Intensive Care Med 2014;40(11):1659–1669. doi: 10.1007/s00134-014-3407-4 [DOI] [PubMed] [Google Scholar]
- 34.Gupta P, Pasquali SK, Jacobs JP, et al. Outcomes Following Single and Recurrent In-Hospital Cardiac Arrests in Children With Heart Disease: A Report From American Heart Association’s Get With the Guidelines Registry-Resuscitation. Pediatr Crit Care Med 2016;17(6):531–539. doi: 10.1097/PCC.0000000000000678 [DOI] [PubMed] [Google Scholar]
- 35.Sweney JS, Poss WB, Grissom CK, Keenan HT. Comparison of severity of illness scores to physician clinical judgment for potential use in pediatric critical care triage. Disaster Med Public Health Prep 2012;6(2):126–130. doi: 10.1001/dmp.2012.17 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.