

Abstract
Aims:
Identification and establishment of the occlusal plane in patients with impaired occlusal plane, presents a major hurdle for the execution of natural esthetics, speech, and function. The aim of this study was to minimize such errors while occlusal rehabilitation, and employ hamular notchincisive papilla (H.I.P) plane as landmark and scribe it on the cast using H. I. P evaluator and utilise for occlusal corrections.
Settings and Design:
HIP plane being parallel to the occlusal plane could ease the operator when it could be scribed on cast to analyze and restore the compromised occlusal plane.
Materials and Methods:
Dentulous casts of two hundred participants were mounted on the Hanau Wide–Vue articulator. Reference points were marked on the maxillary right central incisor and maxillary molars on casts for attaining different occlusal planes, the incisive papilla and hamular notch region were also marked for HIP plane. A plane parallel HIP was scribed on cast using HIP Evaluator. The casts were then scanned using a three-dimensional coordinate measuring machine attached to perception V5 laser scanner and measurements were made using Geomagic X design software. The most parallel occlusal plane to HIP plane was evaluated, and the reliability of HIP evaluator was verified.
Statistical Analysis Used:
ANOVA test, Post hoc-Bonferroni test, and independent sample “t”-test were carried out for the comparison between occlusal planes, among the genders and for the analysis of the angle of deviation of scribed plane on the cast to HIP plane on the right and left sides.
Results:
Occlusal plane III (Mesio-labial incisal edge of upper right central incisor to Mesio-buccal cusp tips of upper second molars) showed least angle of deviation with 1.316° ± 1.158° to HIP plane among tested subjects. There is no significant difference between the genders. The plane scribed on the cast with H. I. P evaluator showed relative parallelism to H. I. P plane with minimum deviation of 0.010° ± 0.363°.
Conclusion:
Occlusal plane III is more parallel to H. I. P plane. Scribed plane on the cast using H. I. P evaluator is parallel to H. I. P plane. H. I. P evaluator can be used as an alternative tool to establish the occlusal plane to rehabilitate patient with deficient dentition or disordered occlusal plane.
Keywords: Hamular notch-incisive papilla evaluator, hamular notch-incisive papilla plane, hamular notch, incisive papilla, occlusal plane and perception V5 laser scanner
INTRODUCTION
Prosthodontic rehabilitation for a patient with deficient dentition or deranged occlusal plane is compelled to establishment the plane of occlusion. This plane must be as close as possible to the position, which was previously occupied by the natural dentition. Thus, a normal function of the stomatognathic system can be assured.
The precise location of the occlusal plane is rather a controversial issue.[1] Various anatomical landmarks and devices have been advocated for the orientation of the occlusal plane.[1,2,3,4,5,6,7,8,9,10,11] Arbitrary use of the reference planes may affect the three-dimensional (3D) orientation of the maxillary cast.[12] The accuracy of most areas on the skin as reference points can be adversely affected by the irregularity and asymmetry of the face and its features.[13] Hence, the functional and esthetic result of intended prosthetic rehabilitation may be compromised.
Hamular notch is an anatomical landmark which is not affected by degenerative process or surgical interference, and the incisive papilla is a significant landmark in dentulous subjects but only its posterior border is relatively stable after the loss of anterior teeth. Hamular notch-incisive papilla (H. I. P) plane is one such plane which minimizes the error and can be recorded easily on the dentulous cast. In previous studies, a simple instrument, anthropometric study, 3D analyzing machine, and computed tomography were used to evaluate the significance of H. I. P plane of occlusion.[13,14,15,16,17]
Occlusal plane rather represents the average curvature of the occlusal surface; studies were done with varying results on different occlusal planes to evaluate the occlusal plane with the least included angle so that it is more parallel to H. I. P plane.[15,16,17] Thus, the primary objective in this study was to evaluate the angle of deviation (included angle) of different occlusal planes from H. I. P plane in Indian dentate subjects and the secondary objective was to assess the reliability of the device H. I. P Evaluator for the orientation of the occlusal plane in dentate individuals.
The null hypotheses was that there will be no statistically significant difference in the angle of deviation of occlusal plane I (Mesio-labial incisal edge of the upper right central incisor to Mesio-buccal cusp tips of upper first molars) to H. I. P plane as compared to other occlusal planes.
The research hypothesis for this study was that the device H. I. P evaluator speculated for the orientation of the occlusal plane by marking scribed plane on the maxillary cast will be parallel to H. I. P plane.
MATERIALS AND METHODS
Two hundred dentulous participants (73 males and 127 females) between the age group of 20 and 50 years with informed consent were randomly selected from students and the outpatients of A. M. E's Dental College and Hospital, Raichur, Karnataka, India.
Formula for sample size in present study considered the study of K Singh et al., for calculation of sample size the formula used was[15]:
Ethical clearance certificate was provided by the Institutional Ethical clearance committee of A.M.E's Dental College and Hospital with IRB approval number is: AME/DC/456/2016-17.
This study included (inclusive criteria) maxillary casts of dentulous individuals aged between 20 and 50 years with ideal arch form and alignment having angle's Class I relationship for standardization. The exclusive criteria were with no history of orthodontic treatment without any extensive restorations, no extractions, and no temporomandibular joint disorders.
Diagnostic casts were evaluated for accurate recording of H. I. P and occluding surfaces of the teeth and mounting was carried out on Hanau Wide–Vue (Whipmix, Louisville, KY, USA) articulator after orientation using Hanau Springbow (Whipmix, Louisville, KY, USA). Articulation was needed so that a plane parallel to the occlusal plane could be scribed on the cast using H.I. P evaluator. Reference points were marked on casts and were prepared to be used by H. I. P evaluator.
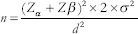
Description of H.I. P Evaluator: H.I. P evaluator is a device designed in the Department of Prosthodontics, AME's Dental College Raichur. It mainly has two parts H.I. P Jig [Figure 1] and H.I. P relocator [Figure 2].
Figure 1.
Hamular notch-incisive papilla evaluator fixed to the lower member of the Hanautm Wide-Vue II articulator. (1) Posterior reference point, (2) anterior reference point, (3) flat platform, (4) thumb screw to adjust the height of platform, (5) Jig to hold the platform
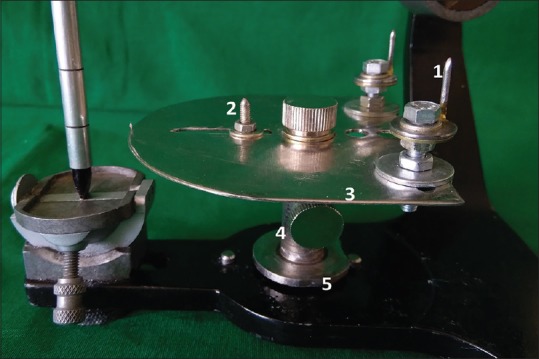
Figure 2.
Hamular notch-incisive papilla re-locator
H.I. P Jig: It consists of a stainless steel horizontal table with adjustable H.I. P pointers. The horizontal table can be adjusted by means of a fixed vertical rod, which has a flat base and can be fixed to the lower member of the articulator
H. I. P relocator: It is a “U” shaped Acrylonitrile Butadiene Styrene plastic framework with a flat base. The base rests on the H.I. P pointers; the “U” shaped frame consists of horizontal slots (at various places) at a fixed height. The lines are scribed on the base of the maxillary cast through these slots using No. 15 Bard-Parker (BP) blade. These scribed lines are joined together to obtain a horizontal plane which will be parallel to the H.I. P plane, thus parallel to occlusal plane.
The procedure of scribing plane parallel to the occlusal plane using H.I. P evaluator:
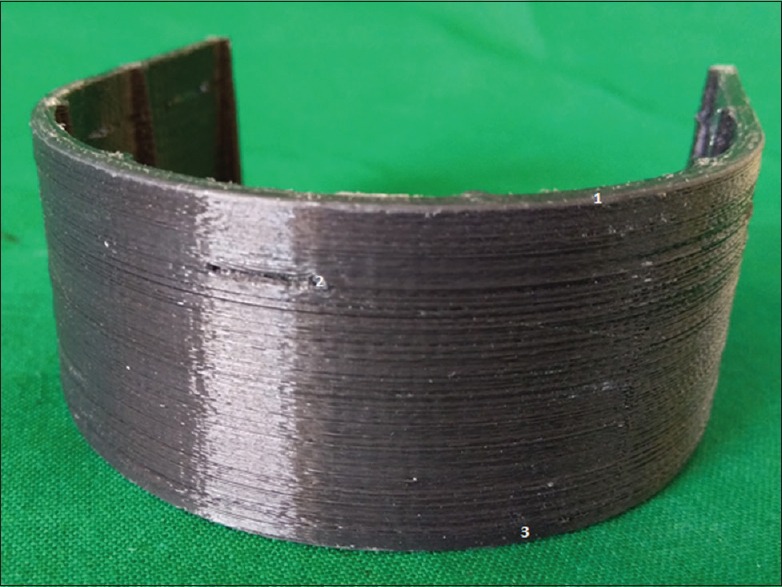
In the present study, reference points were made on middle of incisive papilla of dentulous subjects (as its position alters as the result of resorption only after the loss of anterior teeth) and at posterior deepest point of the Hamular notches of maxillary cast by creating a small pit using small straight fissure bur of 0.5-mm diameter [Figure 3]. They were so prepared to be detected by the scanner.
Figure 3.
Reference points on the cast
To scribe the plane parallel to H.I. P plane on cast the H.I. P jig was fixed on to the lower member of articulator and then, its height was adjusted to align the H.I. P pointers in close approximation with reference points [Figure 4]. The tips of the pointers would now represent the points of H.I. P plane. After the approximation of pointers, the jig was lowered to facilitate the placement of H.I. P relocator [Figure 5]. The base of the relocator was placed over the undisturbed pointers and a No. 15 BP blade was placed in horizontal slots of “U” shaped frame of the H.I. P relocator and the lines were scribed approximately 0.5 mm–1 mm deep to make it visible to naked eyes and to be detected by laser scanner [Figure 6]. These lines were joined to represent the plane parallel to the occlusal plane and also to H. I. P plane [Figure 7]. The casts were then scanned by the laser scanner for the analysis [Figure 8].
Figure 4.
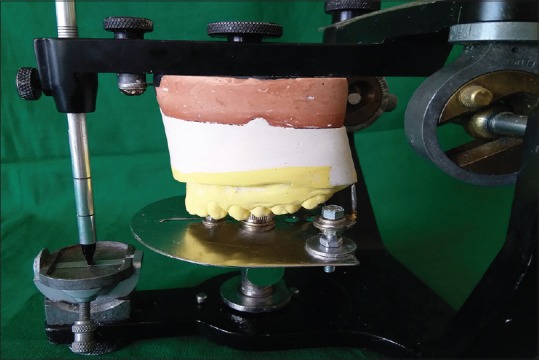
Hamular notch-incisive papilla Pointers coinciding with reference points
Figure 5.
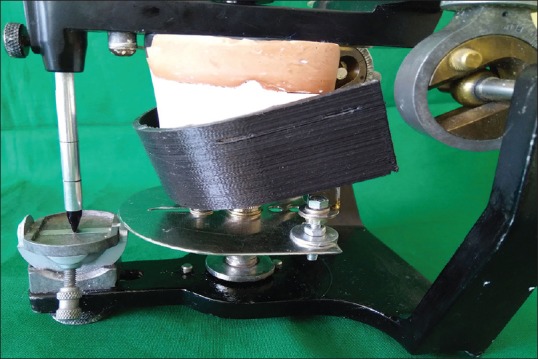
Hamular notch-incisive papilla relocator placed on hamular notch-incisive papilla pointers
Figure 6.
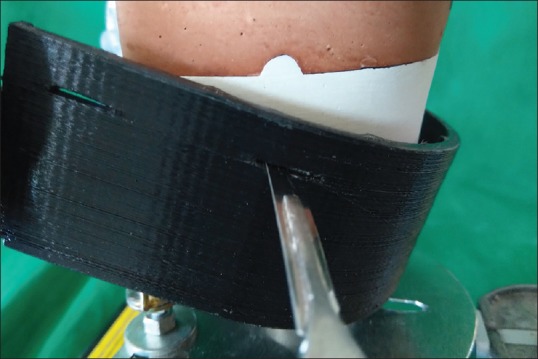
Scribing lines with BP blade in slots of hamular notch-incisive papilla re-locator
Figure 7.
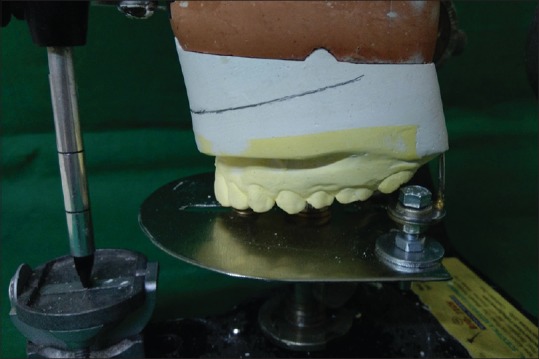
Scribed hamular notch-incisive papilla plane on cast
Figure 8.
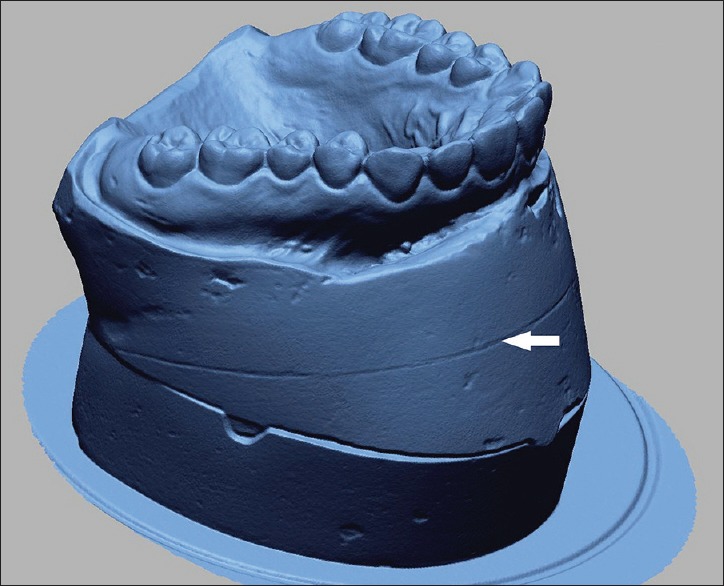
Maxillary cast scanned for the analysis
Few more reference points for analyzing different occlusal plane were marked on the same maxillary casts for analyzing different occlusal planes and for assessing the most parallel occlusal plane to the H.I. P plane. It was marked on Mesio-Labial edge of upper right central incisor, Mesio-buccal and Mesio-Palatal cusp tips of first molars and Mesio-Buccal and Mesio-palatal cusp tips of second molars.
The maxillary casts with all the reference points and a reference plane scribed were scanned using Hexagonal portable coordinate measuring machine attached with perception V5 noncontact laser scanner, which had the capability of scanning 458,400 points per second with a minimum point to point resolution of 12 μ.
The following were assessed after scanning;
Plane I-Mesio-labial incisal edge of upper right central incisor to Mesio-buccal cusp tips of upper first molars
Plane II-Mesio-labial incisal edge of upper right central incisor to Mesio-palatal cusp tips of upper first molars
Plane III-Mesio-labial incisal edge of upper right central incisor to Mesio-buccal cusp tips of upper second molars
Plane IV-Mesio-labial incisal edge of upper right central incisor to Mesio-palatal cusp tips of upper second molars.
Figure 9 shows the angle of deviation of Occlusal plane I, Occlusal plane II, Occlusal plane III Occlusal plane IV, and Occlusal plane from H. I. P plane.
Figure 9.
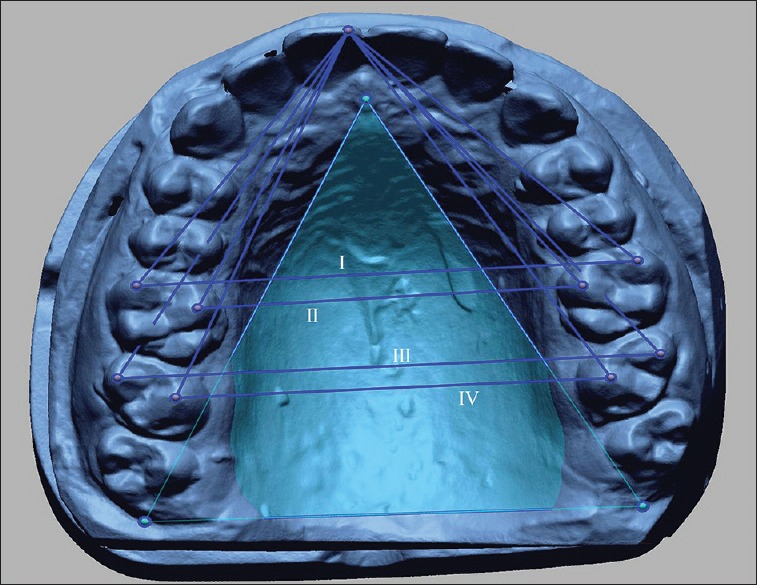
Marking the hamular notch-incisive papilla and occlusal Planes I, II, III, and IV on scanned cast
The parallelism between the scribed plane on the maxillary cast to H.I. P plane [Figure 10].
Figure 10.
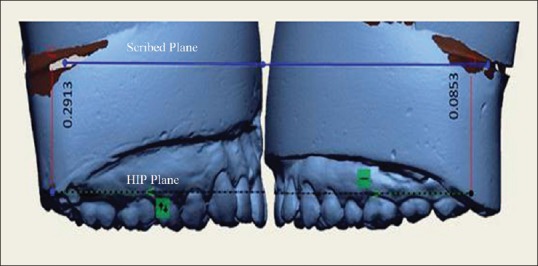
Scanned images showing the angle of deviation between the scribed plane on the cast and the hamular notch-incisive papilla plane on the right and left sides
Statistical analysis
The data obtained from the study was compiled systematically, and measurements were recorded in Microsoft Excel (Microsoft Excel™) following which statistical analysis was conducted using SPSS version 16.0 Software (SPSS Inc., Chicago, IL, USA). The total data were presented as individual tables and along with graphs. Data comparison and statistical analysis of ANOVA test were done to compare between the occlusal planes from the H. I. P plane and within each occlusal plane. Post hoc-Bonferroni test for multiple comparison between the occlusal planes from the H.I. P plane was carried out. An independent sample “t”-test was carried out for the comparison among the genders.
RESULTS
This study included evaluating various parameters like the angle of deviation of four occlusal planes (occlusal Plane I, II, III, and IV) from the H.I. P plane and parallelism of the scribed plane on cast using HIP evaluator to the H.I. P plane.
The relationship of H.I. P plane to occlusal Plane III showed the least deviation of 1.316° ± 1.158° and maximum angle of deviation with the mean value of 2.492° ± 1.370° for occlusal Plane IV. Thus indicating that occlusal Plane III is the most parallel to H.I. P plane [Graph 1]
Graph 1.
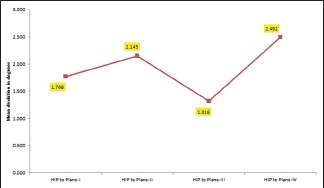
Mean angle of deviation of occlusal Plane I, II, III, and IV to the hamular notch-incisive papilla plane
Statistical analysis of the ANOVA test revealed that there is a statistical significance (P < 0.05) between the occlusal planes and within the occlusal plane though not clinically evident [Table 1]. Post hoc-Bonferroni test for multiple comparison also showed statistical significance between different occlusal planes with H.I. P plane [Table 2].
Table 1.
ANOVA test between and within the occlusal planes
| Angle of deviation between the HIP plane and occlusal planes | Sum of squares | Df | Mean square | F | Significance |
|---|---|---|---|---|---|
| Between the OP | 153.04 | 3 | 51.013 | 32.28 | 0.000* |
| Within the OP | 1257.942 | 796 | 1.58 | ||
| Total | 1410.982 | 799 |
*Statistically significant. HIP: hamular notch-incisive papilla, OP: Occlusal Plane
Table 2.
Post-hoc- Bonferroni test for comparison of angle of deviation between the occlusal planes
| Comparision of angle of deviation between the occlusal planes | Mean difference | SE | Significant | 95% CI | |
|---|---|---|---|---|---|
| Lower bound | Upper bound | ||||
| Plane-I | |||||
| Plane-II | −0.377° | 0.126° | 0.017* | −0.709° | −0.045° |
| Plane-III | 0.452° | 0.126° | 0.002* | 0.119° | 0.784° |
| Plane-IV | −0.724° | 0.126° | 0.000* | −1.057° | −0.392° |
| Plane-II | |||||
| Plane-III | 0.829° | 0.126° | 0.000* | 0.496° | 1.161° |
| Plane-IV | −0.347° | 0.126° | 0.035* | −0.680° | −0.015° |
| Plane-III | |||||
| Plane-IV | −1.176° | 0.126° | 0.000* | −1.508° | −0.843° |
*Statistically significant. SE: Standard error, CI: Confidence interval
An independent sample “t”-test was carried out for the comparison among the genders. In the analysis, the occlusal plane III has the least deviation of 1.411° ± 1.205° in females and 1.151° ± 1.060° in males. The occlusal Plane IV has maximum angle of deviation of 2.524° ± 1.430° in females and 1.267° ± 1.267° in males, but there was no statistical significance between the genders [Tables 2a and b].
Table 2a.
Comparison of angle of deviation of occlusal planes among the genders
| Angle of deviation of occlusal planes between male and female population | Sex | n | Mean±SD | SEM |
|---|---|---|---|---|
| Plane-I | Female | 127 | 1.886°±1.298° | 0.115° |
| Male | 73 | 1.561°±1.136° | 0.133° | |
| Plane-II | Female | 127 | 2.197°±1.287° | 0.114° |
| Male | 73 | 2.054°±1.165° | 0.136° | |
| Plane-III | Female | 127 | 1.411°±1.205° | 0.107° |
| Male | 73 | 1.151°±1.060° | 0.124° | |
| Plane-IV | Female | 127 | 2.524°±1.430° | 0.127° |
| Male | 73 | 2.437°±1.267° | 0.148° |
SD: Standard deviation, SEM: Standard error of the mean
Table 2b.
Independent sample t-test for the comparison among the genders
| Angle of deviation comparison among the genders | t | df | Significant | Mean difference | SE difference | 95% CI of the difference | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Plane-I | 1.782° | 198 | 0.076* | 0.324° | 0.182° | −0.034° | 0.684° |
| Plane-II | 0.781° | 198 | 0.436* | 0.142° | 0.182° | −0.210° | 0.503° |
| Plane-III | 1.534° | 198 | 0.127* | 0.260° | 0.169° | −0.074° | 0.594° |
| Plane-IV | 0.432° | 198 | 0.666* | 0.087° | 0.201° | −0.310° | 0.484° |
*Not significant. SE: Standard error, CI: Confidence interval
The angle of deviation was calculated for the scribed plane on the cast on the right and left sides. The average angle of deviation of 0.0088° ± 0.0467° from the H.I. P plane, on right was 0.0279° ± 0.0321° and left was 0.0367° ± 0.0399°. The obtained values are statistically significant (P < 0.05), though clinically not statistically significant [Table 3].
Table 3.
Parallelism of scribed line on the cast to HIP plane
| Angle of deviation of scribed line to HIP plane | n | Mean | SD | SEM | P |
|---|---|---|---|---|---|
| Angle on left | 200 | 0.0367° | 0.0399° | 0.003° | <0.05* |
| Angle on right | 200 | 0.0279° | 0.0321° | 0.002° | <0.05* |
| Difference of mean and SD | 0.0088° | 0.0467° |
*Statistically significant. SEM: Standard error of the mean, SD: Standard deviation
An independent sample “t”-test was carried out for analyzing the angle of deviation between scribed plane on the cast and the H.I. P plane. On left side, the included angle was 0.0378° ± 0.039° in females, 0.0347° ± 0.0286° in males and the included angle right side was 0.0275° ± 0.03522° in females and 0.0286° ± 0.02608° in males. There was no statistical significance between the genders [Table 4a and b].
Table 4a.
Gender comparison of parallelism between the scribed plane on the cast to its hamular notch-incisive papilla plane
| Gender comparison for scribed plane on the cast to HIP plane | n | Mean | SD | SEM |
|---|---|---|---|---|
| Left | ||||
| Female | 127 | 0.0378° | 0.03939° | 0.00350° |
| Male | 73 | 0.0347° | 0.04096° | 0.00479° |
| Right | ||||
| Female | 127 | 0.0275° | 0.03522° | 0.00312° |
| Male | 73 | 0.0286° | 0.02608° | 0.00305° |
SEM: Standard error of the mean, SD: Standard deviation
Table 4b.
Independent sample t-test for the comparison among the genders
| Scribed plane on the cast to HIP plane comparison among the genders | T-test for equality of means | ||||||
|---|---|---|---|---|---|---|---|
| t | df | Significant | Mean difference | SEM | 95% CI of the difference | ||
| Lower bound | Upper bound | ||||||
| Left | 0.532° | 198 | 0.595* | 0.0031° | 0.0058° | −0.0084° | 0.0147° |
| Right | −0.244° | 198 | 0.807* | −0.0011° | 0.0047° | −0.0104° | 0.0081° |
*Not significant. SEM: Standard error of the mean, CI: Confidence interval
DISCUSSION
A plane although it refers to a flat surface, the occlusal plane is not a straight line; rather, it is a curve, representing the average curvature of the occlusal surfaces. The curvatures of the occlusal plane are due to a large extent to the varying degrees of inclinations of natural teeth. There is a significant correlation between the inclination of the occlusal plane and the direction of the closing path during mastication.[18] Thus determining the occlusal plane becomes challenging though various soft tissue, hard tissue, intra- and extra-oral landmarks are recommended. The most common anatomical landmarks that have been suggested clinically are the upper lip, corners of the mouth, lateral margins of the tongue, buccinator grooves, two-third of the height of the retromolar pad, parallel to the Camper's plane or ala tragus line (a plane established by the inferior border of the ala of the nose and the superior border of the tragus of ear), 3.3 mm below the parotid papilla, etc.[1,2,3,4,5,6,7,8] However, their reliability and accuracy have always been questioned. The arbitrary use of the reference planes may affect the spatial orientation of the maxillary cast.[3] The inappropriate orientation of the occlusal plane jeopardizes the coordination between the components of the orofacial articulatory complex and also affects the esthetics and function.[19,20] Hence, the outcome of planned prosthetic rehabilitation may be compromised.
Various studies were conducted to find landmarks which are more precise, reliable, and can guide the clinician in a better way to reestablish the occlusal plane and identify the reference landmarks that can be recorded on the cast, H.I. P plane is one such plane that is parallel to occlusal plane and can be registered.[3,13,14,15,16,17,21]
H.I. P plane was evaluated and registered by a simple instrument but on worn dentition.[13] Cephalometrics also proved to be of limited value for the prediction of the occlusal plane.[22] Three-dimensional measuring machine used to analyze various reference points in the dental casts proved to be have an accurate method for determining the occlusal plane, but the apparent limitation could have been matching the reference points and fabrication of bite blocks.[15]
Computed tomography (CT) scans of restricted heterogeneous patients were used by Pittschieler et al. evaluating that H.I. P plane is closest to the occlusal plane and when used for articulator mounting could achieve better technical results.[17]
In the present study, the Hexagonal portable 3D coordinate measuring machine attached with PerceptionV5 noncontact laser scanner was used to scan the dental casts. Measurements were done using Geomagic X design Software (Geomagic Inc.morrisville, North Carolina, USA) to check the angle of deviation (included angle) between the H.I. P plane and four occlusal planes and also the angle of deviation on the left and right sides of casts with that of H.I. P plane was verified. Further in this study, drilling small pits near the reference points of casts eased the process of matching them on H.I. P evaluator as well as on the scanner.
According to a study by Fu et al.[16] in 100 Taiwanese young adults the occlusal plane defined as the incisal edge of the maxillary central incisor to mesiobuccal cusp tips of maxillary second molars had the smallest included angle with the H.I. P plane 2.61° ± 0.81°, but Pittschieler et al.[17] found that the occlusal plane defined as the contact point of the incisors (incisal edge), and the mesiobuccal tip of the first molars is more parallel to H. I. P plane with included angle of −0.6° ± 4.0°. The result of this study confirms that the occlusal plane defined as the incisal edge of the maxillary central incisor to mesiobuccal cusp tips of maxillary second molars had the smallest included angle of 1.316° ± 1.158° to the H.I. P plane, suggesting that occlusal plane III is more parallel to HIP plane. Thus rejects null hypotheses as there is statistically significant difference in the angle of deviation of occlusal Plane I (Mesio-labial incisal edge of upper right central incisor to Mesio-buccal cusp tips of upper first molars) to H.I. P plane as compared to other planes.
The reliability of H.I. P Evaluator for the orientation of the occlusal plane in dentate individuals was assessed by scribing a parallel plane on the maxillary cast and scanning it. The included angle of 0.0031 ± 0.0058 (left side) and −0.0011 ± 0.0047 (right side) with no statistical significance resulted, suggesting that the scribed plane and H.I. P plane are parallel. The research hypothesis is accepted for this study as the device H.I. P Evaluator speculated for the orientation of the occlusal plane by marking scribed plane on the maxillary cast is parallel to H.I. P plane.
When a plane parallel to H.I. P plane is scribed on the cast, it would, in turn, mean that it is parallel to occlusal Plane III. It could be justified that scribed plane on cast can be used for the orientation of the occlusal plane in subjects needing occlusal plane alteration. Thus after the reconstructive procedures, the finished appliance will have its occlusal plane close to the natural occlusal plane.
The clinical significance of H.I. P Evaluator is that it could be used as an alternative aid to re-establish the occlusal plane in patients needing full mouth rehabilitation; it is a simple device which rule outs the use of any radiographs, CT scanning, or 3D scanner. It is easy to handle, economical, and reliable. The device can be used for orienting the occusal plane, by just scribing the plane on the maxillary cast and correlating the parallelism with the three reference points unlike the use of Broadrick flag which requires repeated trial and retrial, to achieve the ideal survey center to achieve the most acceptable plane of occlusion.
The limitations of the present study could include slight error while scribing plane on the cast while using the H.I. P relocator. Only one axis was considered in the scanned models while analyzing the most parallel occlusal plane with H.I. P plane. For evaluating the reliability of H.I. P plane of occlusion and its application in edentulous conditions a study can be conducted considering the caudal point of the half-circle contour of the incisive canal in dentulous subjects, also studies must be carried on subjects needing occlusal corrections to assess actual reliability of H.I. P evaluator.
CONCLUSION
Occlusal plane defined by mesio-labial incisal edge of upper right central incisor to mesio-buccal cusp tips of upper second molars is the most parallel plane to H.I. P plane in tested dentulous subjects, suggesting that H.I. P plane can be used as an anatomical landmark for the orientation of the occlusal plane and HIP evaluator can be used as a guide in establishing the disordered and deficient occlusal plane in prosthetic rehabilitation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ismail YH, Bowman JF. Position of the occlusal plane in natural and artificial teeth. J Prosthet Dent. 1968;20:407–11. doi: 10.1016/s0022-3913(68)80017-4. [DOI] [PubMed] [Google Scholar]
- 2.Augsburger RH. Occlusal plane relation to facial type. J Prosthet Dent. 1953;3:755–70. [Google Scholar]
- 3.Sloane RH, Cook J. A guide to orientation of the occlusal plane. J Prosthet Dent. 1953;3:53–65. [Google Scholar]
- 4.Merkeley HJ. Lower denture technic based on a proper understanding of the accessory muscles of mastication. J Am Dent Assoc. 1957;54:769–82. doi: 10.14219/jada.archive.1957.0115. [DOI] [PubMed] [Google Scholar]
- 5.Yasaki M. The height of the occlusion rim and the interocclusal distance. J Prosthet Dent. 1961;11:26–31. [Google Scholar]
- 6.Lundquist DO, Luther WW. Occlusal plane determination. J Prosthet Dent. 1970;23:489–98. doi: 10.1016/0022-3913(70)90198-8. [DOI] [PubMed] [Google Scholar]
- 7.Foley PF, Latta GH., Jr A study of the position of the parotid papilla relative to the occlusal plane. J Prosthet Dent. 1985;53:124–6. doi: 10.1016/0022-3913(85)90080-0. [DOI] [PubMed] [Google Scholar]
- 8.Shigli K, Chetal BR, Jabade J. Validity of soft tissue landmarks in determining the occlusal plane. J Indian Prosthodont Soc. 2005;5:139. [Google Scholar]
- 9.Mittal R. Comparison of the occlusal plane in dentulous and edentulous patients: A cephalometric study. J Indian Prosthodont Soc. 2008;8:195–200. [Google Scholar]
- 10.Shetty S, Shenoy KK, Ninan J, Mahaseth P. An evaluation of relation between the relative parallelism of occlusal plane to ala-tragal line and variation in the angulation of Po-Na-ANS angle in dentulous subjects: A cephalometric study. J Indian Prosthodont Soc. 2015;15:168–72. doi: 10.4103/0972-4052.159968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Inamdar AH, Dange SP, Mahale KM, Khalikar SA. A device for occlusal plane determination. J Indian Prosthodont Soc. 2019;19:93–6. doi: 10.4103/jips.jips_323_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ferrario VF, Sforza C, Serrao G, Schmitz JH. Three-dimensional assessment of the reliability of a postural face-bow transfer. J Prosthet Dent. 2002;87:210–5. doi: 10.1067/mpr.2002.121447. [DOI] [PubMed] [Google Scholar]
- 13.Rich H. Evaluation and registration of the H.I.P. plane of occlusion. Aust Dent J. 1982;27:162–8. doi: 10.1111/j.1834-7819.1982.tb04081.x. [DOI] [PubMed] [Google Scholar]
- 14.Bogatova EA, Lepakhina AA, Nikonova LG, Zhulev EN, Alexy A. Anthropometric study of HIP-plane morphology and correlation relations of its parameters with cerebral and facial cranium measurements. Sovrem Tekhnologii Med. 2013;5:84–7. [Google Scholar]
- 15.Singh K, Lakshmi N, Agnihotri Y, Suvarna SR, Sahoo S, Kumar P. Three-dimensional analysis to compare parallelism of occlusal planes to the hamular notch-incisive papilla plane in dentulous and edentulous subjects. Eur J Gen Dent. 2013;2:286. [Google Scholar]
- 16.Fu PS, Hung CC, Hong JM, Wang JC, Tsai CF, Wu YM. Three-dimensional relationship of the maxillary anterior teeth to the incisive papilla in young adults. Kaohsiung J Med Sci. 2007;23:519–25. doi: 10.1016/S1607-551X(08)70010-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pittschieler E, Foltin A, Falkensammer F, Figl M, Birkfellner W, Jonke E, et al. Comparison of skeletal and dental reference planes with the hamulus-incisive-papilla plane: A pilot study on 3D reconstructed tomographies of the skull. Int J Prosthodont. 2016;29:274–6. doi: 10.11607/ijp.4560. [DOI] [PubMed] [Google Scholar]
- 18.Ogawa T, Koyano K, Suetsugu T. Correlation between inclination of occlusal plane and masticatory movement. J Dent. 1998;26:105–12. doi: 10.1016/s0300-5712(97)00001-8. [DOI] [PubMed] [Google Scholar]
- 19.van Niekerk FW, Miller VJ, Bibby RE. The ala-tragus line in complete denture prosthodontics. J Prosthet Dent. 1985;53:67–9. doi: 10.1016/0022-3913(85)90068-x. [DOI] [PubMed] [Google Scholar]
- 20.Gupta R, Aeran H, Singh SP. Relationship of anatomic landmarks with occlusal plane. J Indian Prosthodont Soc. 2009;9:142. [Google Scholar]
- 21.Sugaya K, Suminokura S, Ohira H, Masuda T, Shinya A, Saitoh F, et al. The correlation of various planes in dental prosthetics. Nihon Hotetsu Shika Gakkai Zasshi. 1986;30:1347–58. doi: 10.2186/jjps.30.1347. [DOI] [PubMed] [Google Scholar]
- 22.Karkazis HC, Polyzois GL. Cephalometrically predicted occlusal plane: Implications in removable prosthodontics. J Prosthet Dent. 1991;65:258–64. doi: 10.1016/0022-3913(91)90172-s. [DOI] [PubMed] [Google Scholar]