

Abstract
Prosthodontic management of palatal defect is fundamental to close patient's oronasal communication and improve masticatory function, phonetics, esthetics, and comfort. Maxillary defects are the direct consequence of the surgical treatment of malformations, neoplasms, or trauma. The primary goal of an obturator is to close palatal defects after maxillectomy and to improve speech and masticatory function. This clinical report describes the use of a flexible silicone obturator for the treatment of a 34-year-old patient with partial maxillectomy due to osteosarcoma of the maxilla. A conventional cast partial denture with a hollow bulb made in acrylic was given as a definitive obturator initially, which was not comfortable for the patient. Alternatively, a new technique of fabrication of obturator with silicone to close palatal defect was decided to establish an acceptable phonetics, comfort, speech, and function for the patient. This silicone obturator gets retention by “snug fit” from the defect site.
Keywords: Flexi-denture, hemi maxillectomy, sectional definitive prosthesis, silicone bulb
INTRODUCTION
Defects in the maxilla may result from congenital malformations or acquired defects resulting from trauma or surgery for oral neoplasms.[1] The resultant maxillary or soft palate defect will impair speech and functions of mastication and deglutition.[2] A maxillofacial prosthesis intends to replace the missing oral or facial structures and its associated functions.[3] The prosthesis constructed to rehabilitate the maxillary defect is termed as an obturator.[1] The goals of prosthetic rehabilitation for maxillectomy patients include separation of the oral and nasal cavities to allow adequate deglutition and articulation, possible support of the orbital contents to prevent enophthalmos and diplopia, support of the soft tissues to restore the midfacial contour, and an acceptable esthetic result.[4] A definitive obturator is indicated when the surgical site has healed completely and is dimensionally stable.[5] A conventional obturator is typically fabricated using acrylic resin and a cobalt–chromium palatal framework, along with an acrylic hollow bulb, to decrease the weight of the prosthesis.[6] This type has inherent disadvantages attributed to its rigid body such as difficulty in insertion and removal of one-piece obturator in large maxillary defects and in patients who do not adapt well to the prosthesis. This is overcome by using flexible materials and/or two-piece obturator. In addition, the use of flexible materials also provides excellent esthetics and comfort, adapts to the constant movement in patients, and improves speech and deglutition. Thus, flexible denture and silicone bulb are an excellent alternative to conventionally used dentures and bulb prosthesis. In this case, an innovative technique of sectional silicone bulb obturator which overcomes the trauma of insertion and removal and gives a snug fit due to its intimate contact[7] and a flexible denture was considered, as the conventional cast partial denture with obturator was not well accepted by the patient.
CASE REPORT
A female patient aged 34 years reported to the Department of Prosthodontics, Sri Ramakrishna Dental College and Hospital, with the chief complaint of poor esthetics and difficulty in speech and mastication and drooping of the lower eyelids. The past dental history revealed that the patient had osteosarcoma of the maxilla. She had undergone partial maxillectomy on the left side, extending to the floor of the orbit up to the midline. The patient was given an acrylic plate immediately after the surgery which acted as a temporary obturator. It was replaced by a removable partial denture (RPD) 1½ months after the surgery.
Intraoral examination showed Aramany Class II maxillary defect on the left maxilla, the defect not exceeding the midline, and the resection involved the hard palate, alveolar bone, teeth, and soft tissue. The missing teeth were 23, 24, 25, 26, 27, and 28 [Figure 1].
Figure 1.

Maxillary defect with missing teeth
The ill-fitting RPD was replaced by an interim obturator without bulb until a definitive treatment plan was devised. A cast partial denture with obturator was planned as a definitive treatment [Figure 2].
Figure 2.
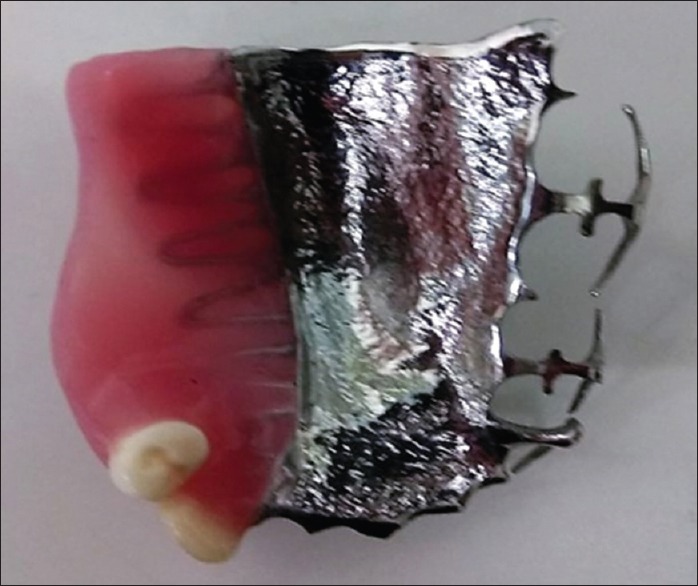
Cast partial denture with obturator
After wearing the prosthesis for 1 week, the patient complained of discomfort and had difficulty in phonetics. On examination, we found that the patient had not adapted to the insertion and removal of the denture even after multiple trials. This could be attributed to the rigid metal body of the denture and the bulb. Phonetics was affected due to poor adaptation of the rigid acrylic bulb prosthesis. Hence, an alternative technique with two-piece flexible denture (Sunflex, Sun Dental Labs, Florida, USA) and silicone obturator was planned to restore the patient's phonetics and ease of use and other functions such as esthetics and comfort.
Impression was made and the flexible denture was arranged with the canine, premolar, and molar. To ensure the maximum retention of this removable prosthesis, a labial flange was extended till the canine of the opposite side [Figure 3].
Figure 3.

Flexible denture
Obtaining Mold Space: A sectional special tray was made on the previous cast and was used to record the defective region using green stick compound (DPI Pinnacle Tracing Sticks, Mumbai) and light-body elastomers (3M ESPE Soft putty, Bengaluru).
The special tray was placed in a plastic cup filled with the dental stone [Figure 4]. After the final set of stone, the special tray was removed from the cup and was subjected to open dewaxing in a hot water bath for 10 min to form mold space.
Figure 4.

Special tray in a cup of stone
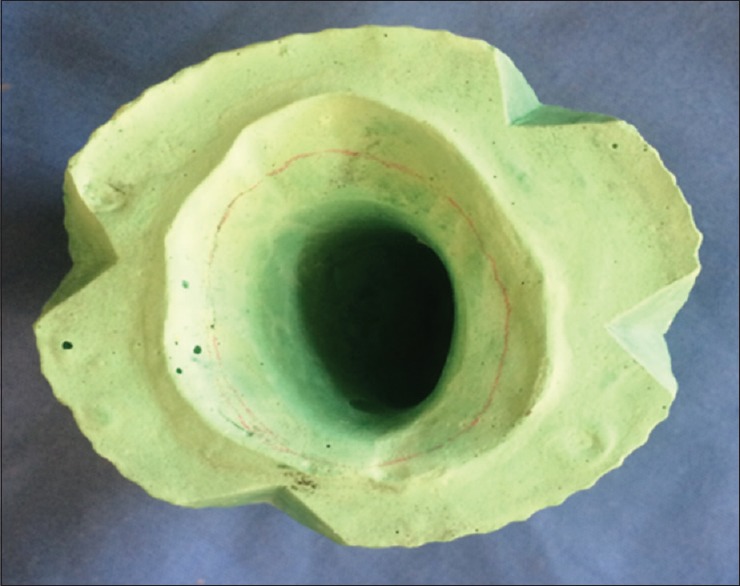
To fabricate the silicone bulb, all the undercuts were blocked out in the master cast. This facilitated easy insertion and removal of the silicone bulb. A 1–1.5 mm of the master cast was scrapped all around at the orifice to have a “snug fit” of the silicone bulb and an intimate contact with soft tissue.
Obtaining counterpart of the mold space:
A four-indexing notch was crafted encircling the orifice of the mold space
To eliminate the area occupied by the borders of the special tray, an outline was made with hematoxylin pencil approximately 2–4 mm from the top of the mold space [Figure 5]
Modeling wax (Hindustan modeling wax) was heated and formed on mold space up to the outline marked with hematoxylin pencil [Figure 6]. This border functions as a vertical stop and facilitates the insertion and removal of the silicone cap
This modified mold space with wax was again placed in the plastic cup. The cup with modified mold space was filled with the dental stone
After the final set of stone, the cup was removed and the two counterparts were obtained [Figure 7].
Figure 5.
Mold space with notches and hematoxylin stain
Figure 6.

Modeling wax on mold space
Figure 7.

Mold space with the counterpart
Fabrication of room-temperature-vulcanizing (RTV) silicone (MP Sai Enterprises) bulb prosthesis:
The mold space with wax was subjected to open dewaxing for 10 min to boil out the wax. Then, the RTV silicone material was packed into the mold space, and the two counterparts were repositioned and kept under room temperature. After 3 days, the solid RTV silicone bulb was retrieved from mold space [Figure 8].
Figure 8.

Room-temperature-vulcanizing silicone bulb
Thus, a sectional prosthesis with flexible denture replacing missing teeth and RTV silicone bulb to close the maxillary defect was fabricated [Figure 9]. The patient was instructed about insertion and removal of bulb prosthesis and was made to practice, as this was their major complaint. Following this, the flexible denture was inserted. After a 1-week review, the patient was comfortable with insertion and removal of the new prosthesis. The oronasal communication was closed with no passage of oral fluid and air between the oral and nasal cavities. The reduction in hypernasality in speech and the improvement in deglutition were noted.
Figure 9.

Sectional prosthesis with Sunflex denture
DISCUSSION
Obturator plays an important role in the recovery of oral functions in post maxillectomy patients. Various methods have been described in the literature on the different designs, techniques, and materials which can be used for an obturator. A maxillary defect can be closed with three different types of the obturator, namely a solid bulb obturator, hollow bulb obturator, or a two-piece obturator which is commonly prescribed for patients with reduced mouth opening, especially after radiotherapy.[8] An obturator needs to fulfill certain criteria to function well, which includes tissue compatibility, ease of insertion and removal, durability, and easy cleaning among others. However, the insertion and removal of one-piece obturator in large maxillary defects with or without trismus is difficult. In such cases, the fabrication of a two-piece obturator, which has a bulb component and a maxillary plate (with or without artificial teeth), overcomes the problem.[9] The definitive prosthesis described in this case report is a two-piece obturator that uses two different materials, a flexible denture made of nylon thermoplastic replacing the missing teeth and a silicone bulb with a snug fit for palatal defect. Flexible dentures because of its inherent flexibility and ability to engage hard- and soft-tissue undercuts for retention are more natural and comfortable in the mouth. Sunflex dentures are unbreakable, yet, lightweight and translucent which allows natural tissue to show through. Furthermore, there is no need of metal clasps – only tissue-colored clasps that blend with natural teeth are used, thereby improving esthetics.[10] The flexibility of the material provides balanced masticatory forces over the entire supporting ridge instead of individual support points.[11] In addition, flexible resin RPDs are seen to display a biocompatibility similar to that of the cast RPDs, and they do not engage the abutment teeth alone for support and retention; hence; the relative stresses on the abutment teeth are relieved.[12]
Bulbs can be made from different materials. Silicone is nontoxic, noncarcinogenic, resilient, hygienic, easy to handle; and well tolerated by intraoral tissues. The softness and resiliency of the RTV silicone materials enable it to engage undercuts within the defects, thus providing retention, support, and stability of the prosthesis. The flexibility of the material allows it to be slowly teased out from the defect site without injuring the soft tissues.[13]
Silicone is commonly used as a cap or liner over the bulb obturator. In patients with trismus and those who do not get adapted to the insertion and removal, the use of full silicone bulb, as a part of twopiece obturator, can be an alternative. Few cases of silicone bulb have been reported in the literature, and further study is needed. The disadvantage of silicone bulb is that it cannot be used in larger sized defects, as it increases the weight of the silicone bulb compromising retention. Silicone needs to be replaced once every 6 months as the prosthesis loses its physical properties, such as color, flexibility, and also dimensional changes are observed.[14] Therefore, long-term follow-up is needed to evaluate for deterioration.[15]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to b`e reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Singh M, Bhushan A, Kumar N, Chand S. Obturator prosthesis for hemimaxillectomy patients. Natl J Maxillofac Surg. 2013;4:117–20. doi: 10.4103/0975-5950.117814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brown JS, Rogers SN, McNally DN, Boyle M. A modified classification for the maxillectomy defect. Head Neck. 2000;22:17–26. doi: 10.1002/(sici)1097-0347(200001)22:1<17::aid-hed4>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 3.Venugopalan S, Kiran Kumar KS. Silicone obturator: As an aid for retention of interim prosthesis in edentulous maxillary defect. SRM J Res Dent Sci. 2013;4:39–42. [Google Scholar]
- 4.Wang RR. Sectional prosthesis for total maxillectomy patients: A clinical report. J Prosthet Dent. 1997;78:241–4. doi: 10.1016/s0022-3913(97)70020-9. [DOI] [PubMed] [Google Scholar]
- 5.Qoran AH, Aminifar S, Adli AR, Abachizadeh H. Using a silicone core to reduce the weight of maxillary obturator prosthesis. J Dent Sch. 2012;30:136–42. [Google Scholar]
- 6.Patil PG, Nimbalkar-Patil S. Lost wax-bolus technique to process closed hollow obturator with uniform wall thickness using single flasking procedure. J Indian Prosthodont Soc. 2017;17:84–8. doi: 10.4103/0972-4052.176538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Batra P. An obturator with a soft touch: A case report. Int J Sci Technol Res. 2013;2:13–8. [Google Scholar]
- 8.Prema S, Felon MR. Two piece obturator using “lock-and-key” mechanism. J Indian Prosthodont Soc. 2017;2:207–11. doi: 10.4103/0972-4052.203194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dholam KP, Sadashiva KM, Bhirangi PP. Rehabilitation of large maxillary defect with two-piece maxillary obturators. J Cancer Res Ther. 2015;11:664. doi: 10.4103/0973-1482.140801. [DOI] [PubMed] [Google Scholar]
- 10.Prashanti E, Jain N, Shenoy VK. Flexible denture – A flexible option to treat edentulous patient. J Nepal Dent Assoc. 2010;11:85–7. [Google Scholar]
- 11.Phoenix RD, Mansueto MA, Ackerman NA, Jones RE. Evaluation of mechanical and thermal properties of commonly used denture base resins. J Prosthodont. 2004;13:17–27. doi: 10.1111/j.1532-849X.2004.04002.x. [DOI] [PubMed] [Google Scholar]
- 12.Hundal M, Madan R. Comparative clinical evaluation of removable partial dentures made of two different materials in Kennedy Applegate class II partially edentulous situation. Med J Armed Forces India. 2015;71:S306–12. doi: 10.1016/j.mjafi.2012.08.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mitra A, Choudhary S, Garg H, Jagadheesh HG. Maxillofacial prosthetic materials- an inclination towards silicones. J Clin Diagn Res. 2014;8:ZE08–13. doi: 10.7860/JCDR/2014/9229.5244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tomar BS, Chandu GS, Singh S, Goutam M. Panacea to lost gingival tissue architecture and spacing: Silicone gingival prosthesis. J Indian Prosthodont Soc. 2016;16:400–4. doi: 10.4103/0972-4052.176524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ohno T, Hojo K, Fujishima I. Soft obturator prosthesis for postoperative soft palate carcinoma: A clinical report. J Prosthet Dent. 2018;119:845–7. doi: 10.1016/j.prosdent.2017.06.024. [DOI] [PubMed] [Google Scholar]