

To the Editor,
A 68-year-old female postmenopausal woman presented with bleeding per vagina and pelvic pain of 2-week duration. Gynecological examination revealed a fleshy mass of size approximately 4 cm × 3 cm seen arising from the anterior lip of the cervix, which bled on touch. Magnetic resonance imaging (MRI) of the pelvis with contrast revealed an enlarged uterus with a well-marginated mass of size 3.6 cm × 4.1 cm × 4.3 cm within the anterior cervix predominantly hyperintense on T1 and T2 and hypointense on T2 fat-suppression sequences consistent with a diagnosis of lipoleiomyoma. The endometrial cavity of the uterus revealed T1 hyperintense collection consistent with hematometra [Figures 1 and 2]. Complementary computed tomography (CT) examination revealed macroscopic fat content within the lesion [Figure 3]. Uterine lipoleiomyoma is composed of mature adipose tissue and smooth muscle cells. Scattered adipocytes in typical leiomyoma are a relatively common finding; a leiomyoma that contains a striking number of adipocytes is called a lipoleiomyoma. Lipoleiomyomas account for approximately 0.03%–0.2% of all uterine leiomyomas and are comprised of a mixture of variable amounts of mature adipocytes and smooth muscle cells.[1] Lipoleiomyomas typically occur in older postmenopausal women, whereas leiomyomas occur mostly in women of reproductive age and usually regress after menopause. The most common location of a lipoleiomyoma is the uterus, whereas other reported sites include the cervix, ovaries, and, on occasion, the retroperitoneum.[2] Occasionally, a cervical fibroid may become pedunculated and prolapse through the external os.[3] The differential diagnosis of a lipomatous tumor in the pelvic region includes benign cystic teratoma of ovary, uterine lipomas, spindle cell lipoma, angiolipoma, angiomyolipoma, and well-differentiated liposarcoma.[4] Ultrasonography has been thought to be specific enough to allow for tissue description, and to establish a precise preoperative diagnosis, MRI or CT can exclusively show the fat content within the tumor. Therefore, in combination with sonography, CT and MRI may assist in the preoperative diagnosis of lipoleiomyomas. Chemical shift imaging, based on the innate differences in the inherent magnetic field experienced by the protons in fat molecules compared with those in water molecules, can also be used for the confirmation of fat. Using Dixon method of chemical shift imaging, fat-only image is acquired showing hyperintense fatty component.[5] Patients with lipoleiomyomas have many estrogen-related conditions including endometriosis, adenomyosis, endometrial hyperplasia, polyps, and gynecologic malignancies. Imaging appearance of endometrial carcinoma, endometrial polyps, and endometrial hyperplasia may be similar. Obstruction of the endometrial canal by endometrial carcinoma is the most common cause of hematometra. However, our case demonstrates hematometra secondary to obstruction by a cervical lipoleiomyoma. In conclusion, diagnosis of a cervical lipoleiomyoma can be challenging as its appearance on imaging resembles that of a liposarcoma. Due to their solid nature, lipoleiomyomas of the cervix may necessitate surgical intervention to relieve associated symptoms and to rule out cervical malignancy.
Figure 1.
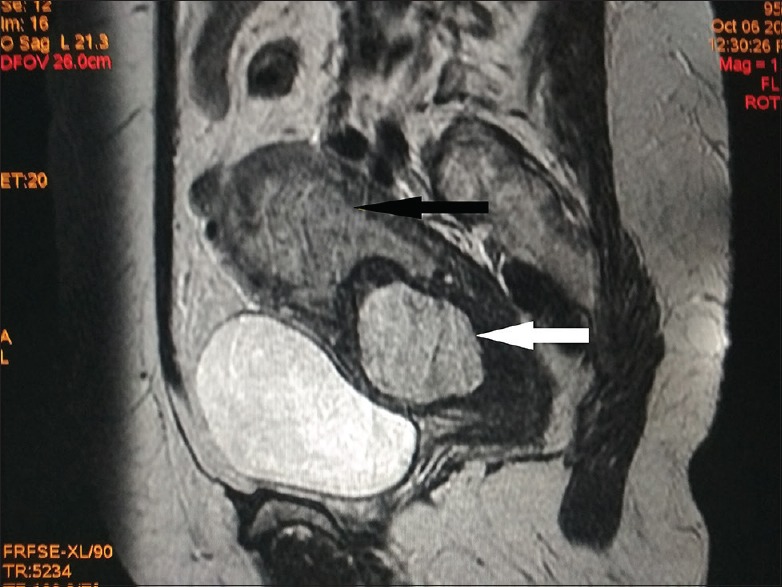
Sagittal T2-weighted magnetic resonance image of the pelvis demonstrating an enlarged uterus with hematometra in the endometrial cavity (black arrow) and a well-defined hyperintense lesion involving the anterior cervix (white arrow)
Figure 2.
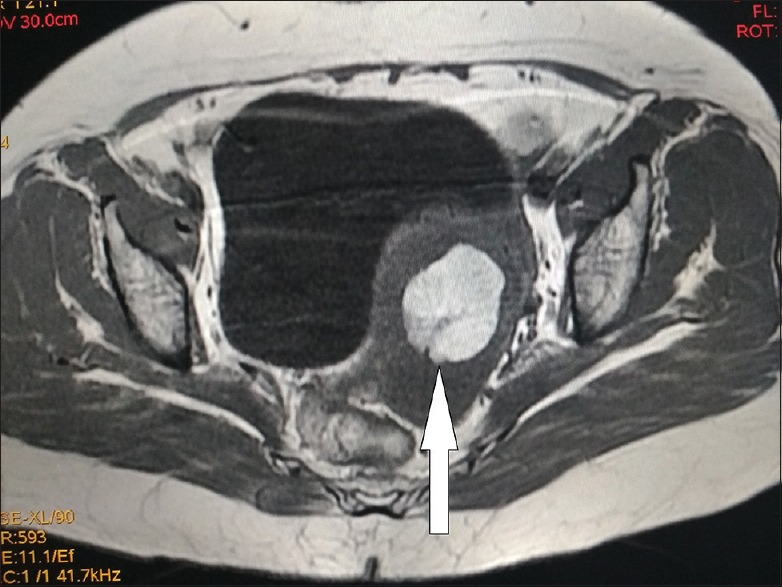
Axial T1-weighted magnetic resonance image of the pelvis demonstrating hyperintense lesion in the cervix representing macroscopic fat-containing lesion proved to be lipoleiomyoma
Figure 3.
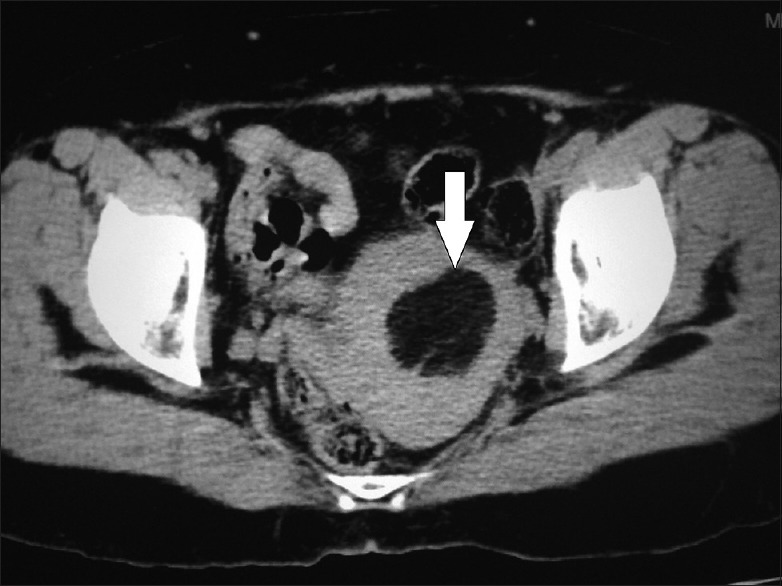
Axial computed tomography image of the pelvis demonstrating well-defined fat density lesion in the cervix suggestive of a lipoleiomyoma
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Prieto A, Crespo C, Pardo A, Docal I, Calzada J, Alonso P. Uterine lipoleiomyomas: US and CT findings. Abdom Imaging. 2000;25:655–7. doi: 10.1007/s002610000052. [DOI] [PubMed] [Google Scholar]
- 2.Su WH, Wang PH, Chang SP, Su MC. Preoperational diagnosis of a uterine lipoleiomyoma using ultrasound and computed tomography images: A case report. Eur J Gynaecol Oncol. 2001;22:439–40. [PubMed] [Google Scholar]
- 3.Wang X, Kumar D, Seidman JD. Uterine lipoleiomyomas: A clinicopathologic study of 50 cases. Int J Gynecol Pathol. 2006;25:239–42. doi: 10.1097/01.pgp.0000192273.66931.29. [DOI] [PubMed] [Google Scholar]
- 4.Aung T, Goto M, Nomoto M, Kitajima S, Douchi T, Yoshinaga M, et al. Uterine lipoleiomyoma: A histopathological review of 17 cases. Pathol Int. 2004;54:751–8. doi: 10.1111/j.1440-1827.2004.01748.x. [DOI] [PubMed] [Google Scholar]
- 5.Avritscher R, Iyer RB, Ro J, Whitman G. Lipoleiomyoma of the uterus. AJR Am J Roentgenol. 2001;177:856. doi: 10.2214/ajr.177.4.1770856. [DOI] [PubMed] [Google Scholar]