

Abstract
Purpose
Gel pad is an aqueous, flexible, easy available, disposable spacer used for the ultrasound (US) scan of superficial or difficult-to-visualize areas. In clinical practice, it is widely used in B-mode US approach of superficial lesions but, to date, no data have been provided as to its efficacy in the Doppler detection of superficial flows. The aim of our study was to demonstrate the role of stand-off gel pad in the detection of the otherwise-missed peri- or intra-lesional flow signals on Doppler imaging.
Materials and Methods
A total of 100 superficial lesions undergone to an US evaluation using a 7.5–12-MHz linear probe were evaluated prospectively with and without interposition of a gel stand-off pad to detect the presence or absence of vascularization and to classify the vascular pattern.
Results
Peri- or intra-lesional flow was demonstrated in 56% of cases without and in 84% of cases with interposition of a gel stand-off pad; moreover, a statistically significant difference (p value < 0.001) was observed at Chi-square test in the identification of the flow pattern between the use and no use of the pad.
Conclusions
The use of a gel stand-off pad allows the detection of otherwise-missed peri- or intra-lesional flow signals on Doppler imaging, increasing the diagnostic role of this technique in differential diagnosis of superficial lesions.
Keywords: Skin ultrasound, Doppler techniques, Gel stand-off pad, Skin lesions, Melanoma
Introduction
Sonography (US) of the skin is rapidly gaining importance as a non-invasive, accurate, and reproducible method to detect focal lesions and describe their morphologic appearance. However, despite many accurate descriptions of skin tumors with US, the vast majority of benign and malignant lesions seem to share the same well-defined hypoechoic pattern. Thus, although being highly sensitive in tumor detection, US can be considered poorly specific in tumor characterization [1–4].
Color Doppler US, being able to produce an accurate map of tumoral vessels, is now considered as one of the most sensitive methods to detect signs of malignant neovascularity [5]. However, despite the use of high-frequency transducers and low-flow scanner settings (high transmission frequency, low pulse repetition frequency, minimum wall filter, color gain increased up to the artifacts threshold), it is sometimes difficult or impossible to detect flow signals of the superficial lesions at color- and power-Doppler (CD and PD) US [6].
Gel pad is an aqueous, flexible, easy available, disposable spacer used for the US scan of superficial and difficult-to-visualize areas; improving the transmission of acoustic energy by shifting the focus more superficially; it is a useful tool to achieve a better B-mode US definition of skin lesions with superior probe stability and contact [7], particularly to scan uneven surfaces [8].
In our study, a commercial gel pad was used as a coupling agent for dermatologic US. The purpose was to outline the technical aspects of gel pad application and to evaluate the role of gel stand-off pad in the detection of the otherwise-missed peri- or intra-lesional flow signals on Doppler imaging. We believe that using a spacer, or a huge amount of free gel when no spacer is not available, may be particularly helpful in US laboratories where high-frequency transducers are not available. Despite an extensive literature research, no data have been provided as to the efficacy of the gel pad in the Doppler detection of superficial flows; to the best of our knowledge, this is the first study about this topic.
Materials and methods
Our single-center, prospective study was conducted over a 5-month period. We evaluated 100 superficial lesions using a multifrequency linear probe with and without interposition of a gel stand-off pad. The criterion for the inclusion in the study group was the detection of a superficial nodule as assessed at B-mode US. Also, patients with a suspected or certain clinical and US diagnosis of vascular anomaly (haemangiomas and artero-venous malformations) or aneurysm/pseudoaneurysm were excluded.
Each patient was subjected to a general clinical and dermatological examination and, subsequently, addressed to the US laboratory of our department to undergo a pre-operative skin US examination. Ethics approval was obtained from the local Institutional Research Ethics Board and informed consent was obtained from every patient.
US examination was performed with a MyLab 70 Twice scanner (Esaote, Genoa, Italy) using a multifrequency (7.5–12 MHz) linear probe. A gel pad (Aquaflex®, Parker Laboratories Inc., USA) approximately 2 cm in thickness was applied between the skin and the probe (Fig. 1).
Fig. 1.

Parker Laboratories, Inc (Fairfield, NJ) produces Aquaflex, an aqueous, flexible, easy available disposable, ultrasound gel pad that measures 9 cm in diameter and 2 cm in thickness for the US scan of superficial and difficult-to-visualize areas, which we used in our study
The focal zone position was adapted according to the position of the lesion in the superficial tissues and the magnification was adjusted as needed to enable better visualization and measurement of the lesion. The transducer was oriented so that the maximum axial diameter of the lesion was parallel to the longitudinal axis of the probe; the maximum axial diameter and the antero-posterior diameter were measured for each lesion. The lesional shape (round, ovoid, irregular), margins (well-defined, ill-defined, irregular), echogenicity (compared with the adjacent dermis, classified as anechoic, hypoechoic, isoechoic, and hyperechoic), echostructure (homogeneous, heterogeneous) and localization were evaluated. Calcifications were considered present in case of focal hyperechoic deposits of any size, with or without back-shadowing. Among the changes in the soft tissues located deeply to the lesion, we considered dorsal enhancement in case of posterior acoustic reinforcement artifact (hyperechogenicity) and back-shadowing in case of any degree of dorsal beam attenuation (hypoechogenicity).
In addition, the lesions were studied with CD and PD Doppler to detect the presence or absence of vascularization and to classify the vascular pattern.
Doppler sonographic parameters were adjusted for detection of low velocities. Specifically, the lowest pulse repetition frequency (PRF) and Doppler gain settings that did not cause aliasing were used; the PRF used was 500–800 Hz with 70–80% color gain, the wall filter was set at 25–50 Hz. With a restricted field of view, the color box was maintained in the area of interest and as small as possible to keep the frame rate high.
The Doppler examination was divided into two steps. First, for each lesion, a CD and PD study was performed to detect absence or presence of flow signal with and without gel pad application, to obtain two sets of sonograms. Specifically, a vessel was defined as a linear or punctuate colored signal not associated with adjacent color noise (optimized setting of color gain is important to reduce artifacts). Then, the lesions were classified by assessment of the vascular pattern according to Giovagnorio [5] as avascular (type I), hypovascular with a single vascular pole (type II), hypervascular with multiple peripheral poles (type III), and hypervascular with internal vessels (type IV) (Fig. 2). For evaluation of image quality, two experienced radiologists reviewed all images together, with results determined by consensus.
Fig. 2.

The four vascular patterns observed in tumours lesions: avascular (type I), hypovascular with a single vascular pole (type II), hypervascular with multiple peripheral poles (type III), and hypervascular with internal vessels (type IV)
The diagnostic confirmation was obtained by pathologic examination of specimens obtained from a surgical resection (n = 67) and US-guided percutaneous fine-needle aspiration cytology/biopsy (n = 33). A pathologist with expertise in skin pathology examined the specimens according to standard criteria based on the World Health Organization (WHO) classification system.
Correlation coefficients and statistical significance were calculated by Pearson correlation coefficient analysis, Student t test, and Chi-square test. All tests were performed with a statistical software package (Statistical Package for the Social Sciences, SPSS, Version 20, SPSS Inc, Chicago, IL) and by an independent statistics analyst.
Results
A total of 100 lesions were gathered from 91 patients. There were 50 males and 41 females aged from 13 to 82 years (mean, 45 years old). Each patient had a single lesion type, except one case of multiple primary malignancy. The lesions were located in the face in 4 cases, neck in 3, thigh in 28 cases, leg in 15, arm in 25, elbow in 3, forearm in 18 and hand in 4.
Overall, of the 100 lesions examined, 32 were histologically benign and 68 malignant. Specifically, the lesions examined were 33 melanomas (33%) (Fig. 3), 12 basocellular carcinomas (12%), 10 spinocellular carcinomas (10%), 8 cutaneous lymphomas (8%), 5 merkel cell carcinomas (5%) (Fig. 4), 15 complicated cysts (15%) (Fig. 5), 8 granulomas (8%), 5 abscesses/cellulitis (5%) and 4 melanocytic nevi (4%) (Table 1). Also, our patient with multiple primary malignancies presented with the simultaneous occurrence of a malignant melanoma and a pigmented basal cell carcinoma at two different sites (face and neck).
Fig. 3.
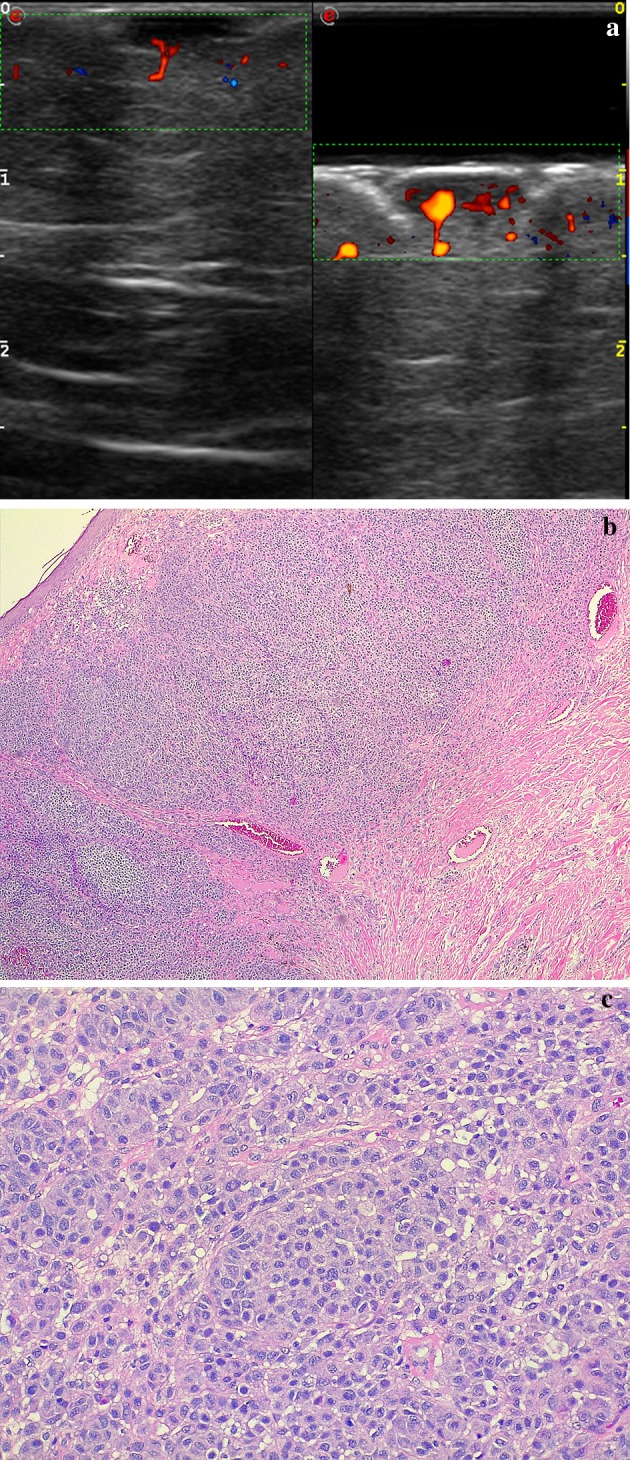
Post-surgical back cutaneous melanoma recurrence. a Directional PD technique, split-screen mode (left without spacer, right with spacer). More flow signals can be detected around and within the cutaneous nodule by using a spacer, which allows to better focus the beam superficially. b, c Photomicrographs—hematoxylin-eosin stain, magnification 4x (b) and 20x (c): proliferation of atypical melanocytes arising from the epidermis and infiltrating the dermis and characterized by nests and sheets of cells epithelioid and spindle-shaped with a high nuclear-cytoplasmic ratio, nuclear grooves and pseudoinclusions, large eosinophilic nucleoli and abundant mitotic figures. The immunehistochemistry cytoplasmic positivity for HMB-45 and MART-1 confirmed the diagnosis of melanoma
Fig. 4.
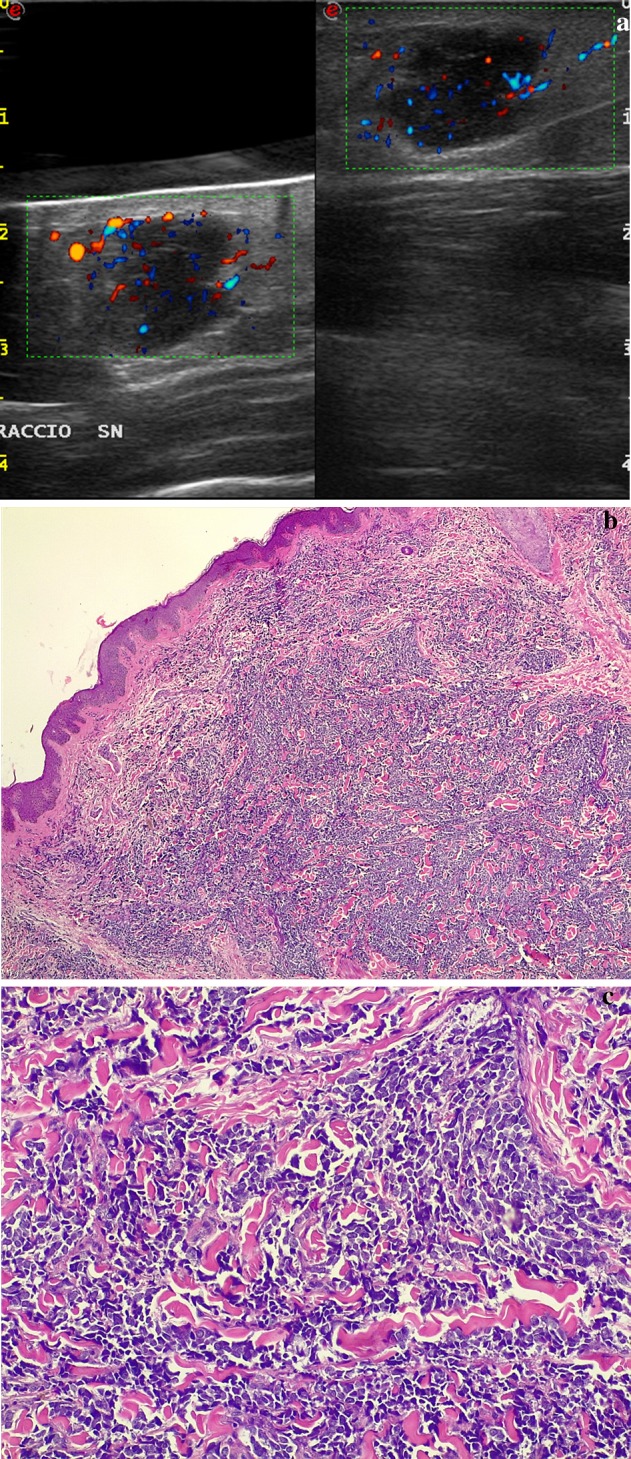
Arm merkel cell carcinoma. a Directional power-Doppler technique. Use of a gel pad to adequately depict the hypoechoic, bulging nodule at US and PD: more peri- and intranodular flow signals are seen using the spacer (left) than without any spacing (right), especially in the uppermost aspect of the nodule. b, c Photomicrographs—hematoxylin-eosin stain, magnification 4x (b) and 20x (c): overgrowth of cells uniform in size arranged in solid sheets and compact nests, which replaced the dermis and subcutaneous tissue without affecting the epidermis. The cytoplasm was scanty but visible as a thin acidophilic rim; the nuclei were round and vesicular with a fine granular chromatin and multiple nucleoli. Mitotic figures and fragmented nuclei were plentiful. The immunohistochemistry cytoplasmic positivity for CK20, NSE, chromogranin and synaptophysin confirmed the diagnosis of Merkel cell carcinoma
Fig. 5.

Axillary inflammed epidermal cyst (sebaceous cyst) with partial rupture. a Directional PD technique, split-screen mode (left without spacer, right with spacer). Doppler US demonstrates a lobulated hypoechoic lesion in the superficial tissues of axillary region. The adjunct of a pad spacer allows obtaining a better display of the vascularity of the lesion, increased under inflammation-rupure phase. b, c Photomicrographs—hematoxylin-eosin stain, magnification 4x (b) and 20x (c): cyst lined by stratified squamous epithelium containing lamellar keratin without calcification
Table 1.
Pathologic confirmation of skin lesions in our study
| Histological examination | |
|---|---|
| Skin lesions | |
| Benign lesions | (32) |
| Complicated Cysts | 15 |
| Granulomas | 8 |
| Abscesses/Cellulitis | 5 |
| Melanocytic Nevi | 4 |
| Malignant lesions | (68) |
| Melanomas | 33 |
| Non-Melanoma Skin Cancer | |
| Basal Cell Carcinoma | 12 |
| Squamous Cell Carcinoma | 10 |
| Other Malignant Skin Tumors | |
| Cutaneous Lymphoma | 8 |
| Merkel Cell Carcinoma | 5 |
The size of the lesions at US ranged from 6 to 21 mm (mean, 10 mm). The shape was round in 32 cases (32%), oval in 49 (49%), and irregular in 19 (19%). The margins, straight or polylobulated, were well defined in 78 cases (78%), ill-defined in 15 (15%) and irregular in 7 (7%). The echogenicity was hypoechoic in 81 lesions (81%), isoechoic in 12 (12%) and hyperechoic in 7 (7%). Thirty-six lesions were homogeneous (36%), forty-three slightly heterogeneous (43%) and twenty-one overtly heterogeneous (21%). Calcifications were present in a single case. Dorsal enhancement was present in 12 cases (12%).
Among the 100 lesions examined with CD and PD, peri- or intra-lesional flow was demonstrated in 56% of cases without and in 84% of cases with interposition of a gel stand-off pad; a statistically significant difference (p value < 0.001) was observed at Chi-square test in the identification of flow signal between the use and no use of the pad (Fig. 6). Moreover, statistical analysis revealed a strong correlation between the flow pattern, and the use or no use of the gel pad; in particular, vascular pattern type II was found in 26 lesions with and in 10 lesions without application of a gel pad (p < 0.005). A minor correlation was found also for types III and IV vascular patterns and the use of gel pad (Table 2).
Fig. 6.
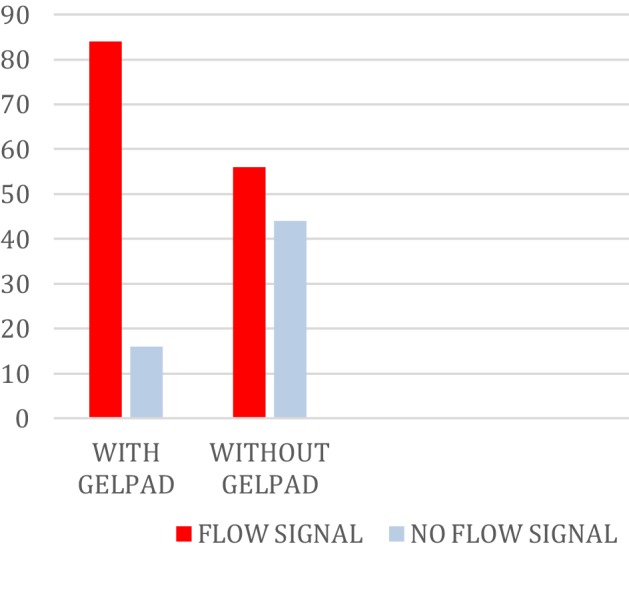
Among the 100 lesions examined with CD and PD, intra- or peri-lesional flow was demonstrated in 56% of cases without and in 84% of cases with interposition of a gel stand-off pad; a statistically significant difference (p value < 0.001) was observed at Chi-square test in the identification of flow signal between the use and no use of the pad
Table 2.
A statistical analysis revealed a strong correlation between the grade of flow signal and the use or not of the gel pad; in particular, vascular pattern type II was found in 26 lesions with and in 10 lesions without application of a gel pad (p < 0.005)
| Vascular pattern | With gel pad | Without gel pad | p |
|---|---|---|---|
| Type I | 16 | 44 | |
| Type II | 26 | 10 | 0.005 |
| Type III | 28 | 22 | |
| Type IV | 30 | 24 |
| p < 0.001 | With gel pad | Without gel pad |
|---|---|---|
| Vessels + | 84 | 56 |
| Vessels 0 | 16 | 44 |
A minor correlation was found also for types III and IV vascular patterns and the use of gel pad
Discussion
Since the early 1980s reports of high-frequency sonography application to skin study, the development of technologies has allowed US to become a useful tool associated with clinical examination in various indications, particularly with the development of 20-MHz probes [9, 10].
Indeed, in the study of superficial organs, particularly in the field of dermatology, the depth of the region to be investigated is about 1–2 cm. Therefore, the use of high-frequency probes, allowing high-resolution imaging, is of crucial importance. Nevertheless, currently used 7- to 17-MHz linear arrays probes, as the one by which we performed our study, also allow the visualization of deep layers up to 3.5 cm in depth with a fairly good axial resolution, thus permitting an adequate approach to the study of superficial tissues [6].
Nodular lesions of the skin are a frequent and serious clinical problem, because some of the most aggressive neoplasms originate from the skin (melanoma, lymphoma) and manifest with a nodular pattern, so to result indistinguishable from benign ones [5].
US has been employed extensively in this field but it lacks specificity, since many nodular lesions share the same sonographic appearance, suggesting that the method may be useful only when a morphologic description of an already diagnosed malignancy is needed [6].
Doppler techniques are a simple, non-invasive method able to increase the specificity of US by providing a real-time evaluation of vascularity, which is an important clue in distinguishing benign from malignant lesions; malignant tumors show an increased number of vessels, which generally appear distorted and deformed, and multiple peripheral poles [5, 6].
In previous studies, Doppler US is used to assess the vascularization of the skin tumors before surgical excision, high vascularization being correlated with an important risk of metastasis [11, 12]. Also, there are several studies concerning the relationship between the thickness of skin melanomas and the presence and aspect of vascularization. Lassau et al. [13] and Srivastava et al. [14] found a strong positive correlation between the vascularization and Breslow tumor thickness, reporting that Breslow thickness and vascularity offer information for the prognosis of these patients. Catalano et al. [15] demonstrated that the presence of intratumoral vessels is correlated with the Breslow index and with patient survival.
Therefore, knowing that vascularization is related to tumor aggressiveness, relapsing or metastatic potential and long-term survival, Doppler US evaluation is very important for dermatologic patients not only for diagnostic characterizations, but also for a good management of both pre- and post-operatively [16].
In our study, we illustrated that the use of a gel stand-off pad allows to detect flow signals within superficial skin lesions. These signals were not seen without the use of the gel pad or were seen in a lesser extent. Our observations also demonstrate that the use of gel pad is helpful in clinical practice, allowing achievement of a presumptive or definitive diagnosis of superficial lesions otherwise indeterminate, and better identifying those with hypovascular pattern (type II).
Technically, it is well known that the body area closer to the transducer, the Fresnel zone or near-field, is the area better seen during US scanning since the beam is collimated and the resolution is high. Instead, at some point distal to the transducer, the beam begins to diverge with decreased resolution: this is the far-field or Fraunhofer zone. However, the nearest region to the transducer, including the cutaneous tissues, is compressed on US image for a length that depends on the transducer quality and on the emission frequency [17, 18]. Gel stand-off pad, increasing the distance between the transducer and the target, enables that the latter falls into the best focus area, maximizing the axial resolution at the depth where the focus is manually placed by the operator. Thus, more flow signals can be detected within the small cutaneous nodules using a spacer [19].
Moreover, our study casually documented a case of coexistence of malignant melanoma and basal cell carcinoma, which we diagnosed as multiple primary malignancy according to criteria given by Warren and Gates [20] and modified later by Moertel et al. and National Cancer Institute for their surveillance, epidemiology and end results (SEER) program [20–24]. To our knowledge, there are only few reports of similar cases in literature [25].
Our study has, however, some limitations. It has a selection bias, as the patients enrolled were selected from a population of patients entering a cancer institute. It is, therefore, obvious that among these patients, there was a high prevalence of malignant lesions. Furthermore, another limit of our study was to not include superficial lesions of vascular origin. Indeed, although US and Doppler appearance of this type of lesions has been extensively documented [26–33] and they may sometimes not be easily differentiated from hypervascularized malignant ones, especially if they show high vessel density such as some hemangiomas or artero-venous malformations [26], we preferred not to include them in our case studies because of their different histopathogenesis, also considering the low case number we encountered during the study period. Finally, in our study, we have not performed an integration with the administration of contrast medium, which surely would have been beneficial to the study of the vascularity of lesions.
Contrast-enhanced ultrasound (CEUS) using second-generation contrast agents is a “new” simple, immediate, and effective tool: microbubbles circulate freely inside the body and constitute an intravascular contrast agent [34–37]; therefore, they permit analysis of tissue perfusion and regional blood flow [38–41]. To date, the value of CEUS for the examination of superficial lesions has not been studied in detail [42, 43]. CEUS previous studies of soft-tissue tumors demonstrated that microbubble-enhanced US can improve the detection of perfusion if compared with CD: in a substantial number of tumors that appear only sparsely vascularized with CD, CEUS gives a completely different impression by depicting more vessels and more intense perfusion [38–41]. Therefore, with these results, our group is planning to evaluate tumor neovasculature with CEUS.
However, the apparent possibilities of Doppler US, even if increased by the use of the spacer as we demonstrated, are balanced by some weak points, which will probably prevent the technique from gaining a leading role in the diagnostic protocols of skin nodule. First, such a superficial and easily accessible disease can be effectively characterized with physical examination and biopsy alone; so that dermatologists are generally unwilling to perform further examinations. Second, since most of skin nodules are removed surgically, Doppler sonography cannot be proposed for follow-up.
In conclusion, gel pad is able to increase significantly the specificity of Doppler US in the evaluation of skin nodules, but the availability of well-known and affordable gold standards, such as physical examination and biopsy, will probably limit its diagnostic role to some well-defined fields.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Antonio Corvino, Email: an.cor@hotmail.it.
Fabio Sandomenico, Email: f.sandomenico@istitutotumori.na.it.
Fabio Corvino, Email: effecorvino@gmail.com.
Maria Raffaela Campanino, Email: mr.campanino@gmail.com.
Francesco Verde, Email: green.franc@gmail.com.
Francesco Giurazza, Email: francesco.giurazza@aocardarelli.it.
Domenico Tafuri, Email: domenicotaf@yahoo.it.
Orlando Catalano, Email: orlandcat@tin.it.
References
- 1.Nessi R, Betti R, Bencini PL, Crosti C, Blanc M, Uslenghi C. Ultrasonography of nodular and infiltrative lesions of the skin and subcutaneous tissues. J Clin Ultrasound. 1990;18(2):103–109. doi: 10.1002/jcu.1870180207. [DOI] [PubMed] [Google Scholar]
- 2.Nazarian LN, Alexander AA, Rawool NM, Kurtz AB, Maguire HC, Mastrangelo MJ. Malignant melanoma: impact of superficial US on management. Radiology. 1996;199(1):273–277. doi: 10.1148/radiology.199.1.8633159. [DOI] [PubMed] [Google Scholar]
- 3.Giovagnorio F. Sonography of cutaneous non-Hodgkin’s lymphomas. Clin Radiol. 1997;52(4):301–303. doi: 10.1016/S0009-9260(97)80059-1. [DOI] [PubMed] [Google Scholar]
- 4.Halani S, Foster FS, Breslavets M, Shear NH. Ultrasound and infrared-based imaging modalities for diagnosis and management of cutaneous diseases. Front Med (Lausanne) 2018;5:115. doi: 10.3389/fmed.2018.00115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Giovagnorio F, Andreoli C, De Cicco ML. Color Doppler sonography of focal lesions of the skin and subcutaneous tissue. J Ultrasound Med. 1999;18(2):89–93. doi: 10.7863/jum.1999.18.2.89. [DOI] [PubMed] [Google Scholar]
- 6.Scotto di Santolo M, Sagnelli M, Mancini M, Scalvenzi M, Delfino M, Schonauer F, Molea G, Ayala F, Salvatore M. High-resolution color-Doppler ultrasound for the study of skin growths. Arch Dermatol Res. 2015;307(7):559–566. doi: 10.1007/s00403-015-1538-2. [DOI] [PubMed] [Google Scholar]
- 7.Klucinec B. The effectiveness of the aquaflex gel pad in the transmission of acoustic energy. J Athl Train. 1996;31(4):313–317. [PMC free article] [PubMed] [Google Scholar]
- 8.Tsui BC, Tsui J. A flexible gel pad as an effective medium for scanning irregular surface anatomy. Can J Anaesth. 2012;59(2):226–227. doi: 10.1007/s12630-011-9623-2. [DOI] [PubMed] [Google Scholar]
- 9.Uematsu T, Kasami M, Kiyohara Y. B-mode ultrasound imaging, Doppler imaging, and real-time elastography in cutaneous malignant melanoma and lymph node metastases. Healthcare (Basel) 2013;1(1):84–95. doi: 10.3390/healthcare1010084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Vilana R, Puig S, Sanchez M, Squarcia M, Lopez A, Castel T, Malvehy J. Preoperative assessment of cutaneous melanoma thickness using 10-MHz sonography. AJR Am J Roentgenol. 2009;193(3):639–643. doi: 10.2214/AJR.08.1387. [DOI] [PubMed] [Google Scholar]
- 11.Doben AR, MacGillivray DC. Current concepts in cutaneous melanoma: malignant melanoma. Surg Clin North Am. 2009;89(3):713–725. doi: 10.1016/j.suc.2009.03.003. [DOI] [PubMed] [Google Scholar]
- 12.Leiter U, Buettner PG, Eigentler TK, Bröcker EB, Voit C, Gollnick H, Marsch W, Wollina U, Meier F, Garbe C. Hazard rates for recurrent and secondary cutaneous melanoma: an analysis of 33,384 patients in the German Central Malignant Melanoma Registry. J Am Acad Dermatol. 2012;66(1):37–45. doi: 10.1016/j.jaad.2010.09.772. [DOI] [PubMed] [Google Scholar]
- 13.Lassau N, Lamuraglia M, Koscielny S, Spatz A, Roche A, Leclere J, Avril MF. Prognostic value of angiogenesis evaluated with high-frequency and colour Doppler sonography for preoperative assessment of primary cutaneous melanomas: correlation with recurrence after a 5 year follow-up period. Cancer Imaging. 2006;25(6):24–29. doi: 10.1102/1470-7330.2006.0009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Srivastava A, Woodcock JP, Mansel RE, Webster DJ, Laidler P, Hughes LE, Dwivedi A. Doppler ultrasound flowmetry predicts 15 year outcome in patients with skin melanoma. Indian J Surg. 2012;74(4):278–283. doi: 10.1007/s12262-011-0398-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Catalano O, Siani A. Cutaneous melanoma: role of ultrasound in the assessment of locoregional spread. Curr Probl Diagn Radiol. 2010;39(1):30–36. doi: 10.1067/j.cpradiol.2009.04.001. [DOI] [PubMed] [Google Scholar]
- 16.Botar Jid C, Bolboacă SD, Cosgarea R, Şenilă S, Rogojan L, Lenghel M, Vasilescu D, Dudea SM. Doppler ultrasound and strain elastography in the assessment of cutaneous melanoma: preliminary results. Med Ultrason. 2015;17(4):509–514. doi: 10.11152/mu.2013.2066.174.dus. [DOI] [PubMed] [Google Scholar]
- 17.Hangiandreou NJ. AAPM/RSNA physics tutorial for residents. Topics in US: B-mode US: basic concepts and new technology. Radiographics. 2003;23(4):1019–1033. doi: 10.1148/rg.234035034. [DOI] [PubMed] [Google Scholar]
- 18.Lawrence JP. Physics and instrumentation of ultrasound. Crit Care Med. 2007;35(8 Suppl):S314–S322. doi: 10.1097/01.CCM.0000270241.33075.60. [DOI] [PubMed] [Google Scholar]
- 19.Corvino A, Corvino F, Catalano O, Sandomenico F, Petrillo A. The tail and the string sign: new sonographic features of subcutaneous melanoma metastasis. Ultrasound Med Biol. 2016;43(1):370–374. doi: 10.1016/j.ultrasmedbio.2016.09.008. [DOI] [PubMed] [Google Scholar]
- 20.Warren S, Gates O. Multiple primary malignant tumors: a survey of the literature and statistical study. Am J Cancer. 1932;16:1358–1414. [Google Scholar]
- 21.Vogt A, Schmid S, Heinimann K, Frick H, Herrmann C, Cerny T, Omlin A. Multiple primary tumours: challenges and approaches, a review. ESMO Open. 2017;2(2):e000172. doi: 10.1136/esmoopen-2017-000172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Maurea S, Corvino A, Imbriaco M, Avitabile G, Mainenti P, Camera L, Galizia G, Salvatore M. Simultaneous non-functioning neuroendocrine carcinoma of the pancreas and extra-hepatic cholangiocarcinoma. A case of early diagnosis and favorable post-surgical outcome. JOP. 2011;12(3):255–258. [PubMed] [Google Scholar]
- 23.Corvino A, Corvino F, Radice L, Catalano O. Synchronous mucinous colonic adenocarcinoma and multiple small intestinal adenocarcinomas: report of a case and review of literature. Clin Imaging. 2015;39(3):538–542. doi: 10.1016/j.clinimag.2014.12.019. [DOI] [PubMed] [Google Scholar]
- 24.Campanile F, Maurea S, Mainenti P, Corvino A, Imbriaco M. Duodenal involvement by breast cancer. Breast J. 2012;18(6):615–616. doi: 10.1111/tbj.12034. [DOI] [PubMed] [Google Scholar]
- 25.Sharma S, Agrawal U, Gupta P, Bhatnagar A, Jairajpuri Z. Malignant melanoma and basal cell carcinoma of the face: a rare coexistence. Ann Saudi Med. 2013;33(3):304–306. doi: 10.5144/0256-4947.2013.304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Peer S, Wortsman X. Hemangiomas and vascular malformations. In: Wortsman X, editor. Dermatologic ultrasound with clinical and histologic correlations. New York: Springer; 2013. pp. 183–234. [Google Scholar]
- 27.Pellino G, Candilio G, De Fatico GS, Marcellinaro R, Piccione A, Cautiero R, Capozzolo A, Guerniero R, Volpicelli A, Reginelli A, Corvino A, Sciaudone G, Canonico S, Selvaggi F. Vascular anomalies of the large bowel. Int Angiol. 2015;34(6 Suppl 1):23–27. [PubMed] [Google Scholar]
- 28.Pellino G, Candilio G, De Fatico GS, Marcellinaro R, Piccione A, Cautiero R, Capozzolo A, Guerniero R, Volpicelli A, Reginelli A, Corvino A, Sciaudone G, Canonico S, Selvaggi F (2015) Vascular anomalies of the large bowel. Int Angiol. 2015 May 21. [Epub ahead of print]. PMID: 25994449 [PubMed]
- 29.Corvino A, Catalano O, Corvino F, Sandomenico F, Setola SV, Petrillo A. Superficial temporal artery pseudoaneurysm: what is the role of ultrasound? J Ultrasound. 2016;19(3):197–201. doi: 10.1007/s40477-016-0211-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Corvino F, Silvestre M, Cervo A, Giurazza F, Corvino A, Maglione F. Endovascular occlusion of pulmonary arteriovenous malformations with the ArtVentive Endoluminal Occlusion System™. Diagn Interv Radiol. 2016;22(5):463–465. doi: 10.5152/dir.2016.15620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cangiano G, Corvino F, Giurazza F, Silvestre M, Amodio F, Corvino A, Niola R. Endovascular treatment of simultaneous iliac and superficial femoral arterial pseudoaneurysms after stenting procedure complications. Vasc Endovasc Surg. 2019;53(2):160–164. doi: 10.1177/1538574418805588. [DOI] [PubMed] [Google Scholar]
- 32.Corvino F, Giurazza F, Cangiano G, Silvestre M, Cavaglià E, de Magistris G, Amodio F, Corvino A, Niola R. Endovascular treatment of peripheral vascular blowout syndrome in end-stage malignancies. Ann Vasc Surg. 2019 doi: 10.1016/j.avsg.2018.10.051. [DOI] [PubMed] [Google Scholar]
- 33.Corvino F, Giurazza F, Cangiano G, Cavaglià E, Amodio F, De Magistris G, Corvino A, Niola R. Safety and effectiveness of transcatheter embolization in the treatment of internal mammary artery injuries. Radiol Med. 2018;123(5):369–377. doi: 10.1007/s11547-017-0844-5. [DOI] [PubMed] [Google Scholar]
- 34.Corvino A, Catalano O, Corvino F, Sandomenico F, Petrillo A. Diagnostic performance and confidence of contrast-enhanced ultrasound in the differential diagnosis of cystic and cysticlike liver lesions. AJR Am J Roentgenol. 2017;209(3):W119–W127. doi: 10.2214/AJR.16.17062. [DOI] [PubMed] [Google Scholar]
- 35.Corvino A, Catalano O, Setola SV, Sandomenico F, Corvino F, Petrillo A. Contrast-enhanced ultrasound in the characterization of complex cystic focal liver lesions. Ultrasound Med Biol. 2014;41(5):1301–1310. doi: 10.1016/j.ultrasmedbio.2014.12.667. [DOI] [PubMed] [Google Scholar]
- 36.Corvino A, Catalano O, Corvino F, Petrillo A. Rectal melanoma presenting as a solitary complex cystic liver lesion: role of contrast-specific low-MI real-time ultrasound imaging. J Ultrasound. 2015;19(2):135–139. doi: 10.1007/s40477-015-0182-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Guarino B, Catalano O, Corvino A, Corvino F, Amore A, Petrillo A. Hepatic inflammatory pseudotumor: educational value of an incorrect diagnosis at contrast-enhanced ultrasound. J Med Ultrasonics. 2001;42(4):547–552. doi: 10.1007/s10396-015-0624-6. [DOI] [PubMed] [Google Scholar]
- 38.Gaitini D. Introduction to color Doppler ultrasound of the skin. In: Wortsman X, editor. Dermatologic ultrasound with clinical and histologic correlations. New York: Springer; 2013. pp. 3–14. [Google Scholar]
- 39.Oebisu N, Hoshi M, Ieguchi M, Takada J, Iwai T, Ohsawa M, Nakamura H. Contrast-enhanced color Doppler ultrasonography increases diagnostic accuracy for soft tissue tumors. Oncol Rep. 2014;32(4):1654–1660. doi: 10.3892/or.2014.3378. [DOI] [PubMed] [Google Scholar]
- 40.De Giorgi V, Gori A, Grazzini M, Rossari S, Marino G, D’Elia G, Crocetti E, Roselli G, Innocenti P, Dini M, Lotti T. Contrast-enhanced ultrasound: a filter role in AJCC stage I/II melanoma patients. Oncology. 2010;79(5–6):370–375. doi: 10.1159/000323494. [DOI] [PubMed] [Google Scholar]
- 41.Rubaltelli L, Beltrame V, Scagliori E, Bezzon E, Frigo AC, Rastrelli M, Stramare R. Potential use of contrast-enhanced ultrasound (CEUS) in the detection of metastatic superficial lymph nodes in melanoma patients. Ultraschall Med. 2014;35(1):67–71. doi: 10.1055/s-0033-1335857. [DOI] [PubMed] [Google Scholar]
- 42.Schröder RJ, Mäurer J, Zlowodski M, Hidajat N, Schlums D, Weber S, Felix R. Vascularization of malignant and benign skin tumours measured by D-galactose-based signal-enhanced colour Doppler sonography. Acta Radiol. 2001;42(3):294–301. doi: 10.1080/028418501127346855. [DOI] [PubMed] [Google Scholar]
- 43.Wortsman X. Sonography of the primary cutaneous melanoma: a review. Radiol Res Pract. 2012;2012:814396. doi: 10.1155/2012/814396. [DOI] [PMC free article] [PubMed] [Google Scholar]