

Abstract
Background
Lateral ankle sprain is one of the most common musculoskeletal injuries, particularly among the sporting population. Due to such prevalence, many interventions have been tried to prevent initial, or further, ankle sprains. Current research shows that the use of traditional athletic tape can reduce the incidence of sprain recurrence, but this may be at a cost to athletic performance through restriction of motion. Kinesiology tape, which has become increasingly popular, is elastic in nature, and it is proposed by the manufacturers that it can correct ligament damage. Kinesiology tape, therefore, may be able to improve stability and reduce ankle sprain occurrence while overcoming the problems of traditional tape.
Aim
To assess the effect of kinesiology tape on ankle stability.
Methods
27 healthy individuals were recruited, and electromyography (EMG) measurements were recorded from the peroneus longus and tibialis anterior muscles. Recordings were taken from the muscles of the dominant leg during induced sudden ankle inversion perturbations using a custom-made tilting platform system. This was performed with and without using kinesiology tape and shoes, creating four different test conditions: barefoot(without tape), shoe(without tape), barefoot(with tape) and shoe(with tape). For each test condition, the peak muscle activity, average muscle activity and the muscle latency were calculated.
Results
No significant difference (p>0.05) was found by using the kinesiology tape on any of the measured variables while the wearing of shoes significantly increased all the variables.
Conclusion
Kinesiology tape has no effect on ankle stability and is unable to nullify the detrimental effects that shoes appear to have.
Keywords: taping and bracing, ankle, sprain
Key messages.
Kinesiology tape had no effect on the peak muscle activity, the average muscle activity or the muscle latency for the peroneus longus or tibialis anterior during a sudden ankle inversion.
Shoes increased all the mentioned variables during a sudden ankle inversion. Results of note are an increased activity of the tibialis anterior, a prolonged peroneus longus latency and a shortened latency from peroneus longus activation to tibialis anterior activation.
Therefore, kinesiology tape appears to have no effect on ankle stability while shoes appear to be detrimental.
It is hoped that the results of this study can be used by athletes, patients, clinicians and researchers alike to make informed decisions.
Introduction
Lateral ankle sprains (LAS) plague numerous individuals in the sporting community.1 Although regarded as a trivial injury, LAS causes distress, lost time from sport or work and most importantly can lead to instability with recurrent sprains.2 For these reasons, an effective method for protecting the ankle from sprains must be sought.
Existing research accepts that a large inversion moment about the subtalar joint axis leads to damage of the lateral ankle ligaments.3 However, one area of much controversy in the literature is the role of the peroneal muscles, the primary evertors of the ankle, and whether they can realistically protect the ankle during a sprain scenario. It has been concluded by many studies that there is a delayed peroneal reaction to sudden inversion in those with unstable ankles compared with stable.4
The other stabilising muscle of the ankle, which opposes the action of the peroneus longus, is the tibialis anterior, which is greatly under reported with regard to LAS. However, Willems et al 5 suggested that there is some implication of the tibialis anterior in LAS. In a normal reaction to a sudden ankle inversion the peroneal muscles react first, followed by the tibialis anterior. However, in those with recurrent LAS this sequence is lost, with the tibialis anterior contracting almost instantaneously with the peroneus longus. Furthermore, an increased activation of tibialis anterior during gait has been demonstrated in those with ankle instability.6 Therefore, the dysfunction of the tibialis anterior, as well as the peroneus longus, must be associated with LAS.
To reduce the incidence of ankle sprains and provide ankle support, ankle tape and braces have become increasingly popular, with promising results.7 8 While mechanical support is likely to be a part of the mechanism of offering stability, it has been suggested that the primary function of taping is to improve the deficient proprioception of unstable ankles.9 However, one issue that has been highlighted with regard to the use of ankle supports is the negative effects they may cause to athletic performance on account of their rigidity.10
A different design of tape has recently become popular on the market; kinesiology tape. It is easily recognisable with its bright colours and is commonly seen on high profile athletes. It is proposed by the manufacturers that the tape can correct ligament damage and improve proprioception.11 Given the elastic nature of the tape, it may also be able to overcome the issues of rigid traditional tape. However, despite the popularity of kinesiology tape, the literature is limited and research that has been published is very inconclusive, with any clear benefits yet to be seen, particularly in regard to ankle stability.12
Very few studies have been conducted with kinesiology tape applied to the ankle, and none to date have included shoes or made observations regarding the tibialis anterior during a sudden inversion. Therefore, the aim of this study was to assess the effect of kinesiology tape on ankle stability through its effects on the stabilising muscles of the ankle: the peroneus longus and the tibialis anterior.
Methodology
Patient and public involvement
Patients were not involved in this study. Participants, who were members of the general public, were not involved in the design of the study. They first became involved in the research process during the recruitment via email or seeing a volunteer recruitment poster. They were not asked to assess the burden of intervention or time required, nor were they involved in result dissemination. All participation was entirely voluntary and without remuneration or incentive. Volunteers were able to withdraw from the study at any time and without having to give reason.
Sampling
Twenty-seven volunteers were recruited to take part in the research study. Volunteers had to be over 18 years of age and in good health with no physical deformities or injuries to the lower limbs during the past 6 months. Participants were required to read a participant information sheet and sign consent forms before the study commenced.
Experimental apparatus
A custom-made software program designed to control tilting platforms while simultaneously recording measurements from a portable electromyography (EMG) system was used. This setup was also used in a similar study by Kerr et al 13 and is depicted in figure 1.
Figure 1.

Schematic representation of experimental setup.
The tilting platforms composed of two aluminium footplates on bars propped off the ground by a supporting block at each end and about which the bar could rotate. Tilting of the platforms was pneumatically driven, rotating at an angular velocity of 100°/s. The degree of rotation was computer controlled and could be measured via a feedback loop from the platforms. From a safety aspect and to avoid potential injuries, the plates were coated with an adhesive layer to prevent foot slippage, handrails were fitted in front of the platforms to support subjects further and only 20° of varus foot tilt was allowed which was less than that used in other studies but more than adequate to evoke a peroneal response.14 Reinforcement blocks were also placed under the platforms to ensure there was maximum of 20° inversion.
The portable EMG system used was the Mobi8 (TMS International Netherland). The activities of the two muscles, the peroneus longus and tibialis anterior, were measured during the plate inversions. In the interest of time and conservation of tape, only the dominant leg was assessed and chosen due to its higher incidence of ankle sprain.2 To prepare the skin for electrode placement and reduce interference, any hair present was removed using a razor, and the skin was cleaned with alcohol gel and wipes to eradicate any presence of dead skin and oils. Each muscle belly was located through voluntary muscle contraction and two silver/silver chloride surface EMG electrodes were placed on the skin for each muscle as per the Surface EMG for Non-Invasive Assessment of Muscles (SENIAM) recommendations. Electrodes were disc shaped with a diameter of 10 mm and an interelectrode distance of 20 mm was kept. A reference electrode was also placed on the clavicle. The electrodes were attached to an amplifier and the recorded signals were amplified and filtered before being transmitted to the computer.
Procedure
Four test conditions were used as shown in figure 2. To ensure randomisation, the order of test condition for each subject was assigned using a random number generator. Subjects were first allocated to either tape or no tape and then within each of these conditions, shoes or no shoes. This was for practicality, as applying and removing the tape twice would be time consuming and costly in the use of tape. Standard running shoes were used for the shod conditions in each subject (Nike Dart 7) and each subject acted as their own control.
Figure 2.

The four different test conditions: (A) barefoot (B) shoes (C) tape with bare feet (D) tape with shoes.
The tape used was Kinesio Tex tape (Kinesio USA, Albuquerque, New Mexico, USA) and the taping technique was that proposed by the manufacturer for a postacute LAS correction,11 this is shown in figure 3. Two strips were used, the first (dark blue in figure 3), applied at 50% tension, was for functional correction to assist dorsiflexion and eversion. This was applied from insertion to origin. The second (light blue in figure 3), applied at 75%–100% tension, was intended for the correction of the anterior talofibular ligament, the most commonly damaged during an LAS.2 All tape was applied by the same lead investigator.
Figure 3.

Taping technique.
Subjects were asked to stand on the tilting platforms with each foot at the centre so that their weight was evenly distributed across each plate. The software program used allowed different test sequences to be generated, saved and repeated. Therefore, for each of the four test conditions, a different sequence of inversions between the left and right leg was used to create simulated unexpected inversion scenarios that the volunteers do not get accustomed to.
The platforms began in the neutral position, parallel to the ground (0°), then underwent a random sequence of three left and three right (six in total) inversions to 20°. After each inversion, the platform would remain in inversion for 5 s to produce an average muscle activity. The plates would then return to the neutral position and the sequence would continue. There was a period of 2 min between each condition to allow for rest and preparation for the next sequence. The synchronised EMG system recorded muscle activity in situ and the recordings were collected at a sampling rate of 2000 Hz.13
Data processing
Following the amplification, filtering and rectifying of the recorded EMG signals a custom-made extraction programme allowed the three variables of interest to be calculated for each inversion. Those variables were the peak activity (greatest muscle activity following inversion), average activity (average muscle activity in the 5 s following inversion) and muscle latency (time from beginning of tilt to first muscle reaction).
Statistical analysis
The results for the peak, average and latency were then collated from each subject under the four different test conditions for statistical analysis, which was conducted using IBM SPSS SENIAM V.22.0 Statistics software. For each muscle and variable (ie, the peak peroneus longus muscle activity), SPSS was used with the general linear model, repeated measures function. This gave an estimate of mean, SE of mean and 95% CI for each variable, as well as a pairwise comparison between each of the four test conditions for each variable and in each muscle.
Results
Of the 27 participants recruited, 16 were male and 11 females. The participants had a mean age of 21.1 (±1.45) years, height of 174 (±7.94) cm and weight of 74.0 (±10.8) kg.
Peroneus longus results
The mean peak activity, average activity and latency period for the peroneus longus are shown in table 1. For the peak and average activity, the shod conditions caused a significant increase compared with the non-shod conditions. For the latency, shoe caused a significant increase compared with barefoot and, while not significantly, tape and shoe also increased the latency. The contrary is true for the tape, with no significant differences observed between the taped and non-taped conditions, therefore, these pairwise comparisons are not included in the tables.
Table 1.
Peroneus longus muscle activity
| Variable | Condition | Mean (SE) | P value |
| Peak activity (µV) | Barefoot | 247 (±19.1) | – |
| Tape (barefoot) | 249 (±16.1) | 0.891 | |
| Shoe | 367 (±21.6) | 0.000* | |
| Tape and shoe | 337 (±19.0) | 0.000* | |
| Average activity (µV) | Barefoot | 70.0 (±5.89) | – |
| Tape (barefoot) | 77.6 (±5.79) | 0.059 | |
| Shoe | 109 (±7.27) | 0.000* | |
| Tape and shoe | 109 (±6.83) | 0.000* | |
| Latency (ms) | Barefoot | 183 (±8.59) | – |
| Tape (barefoot) | 200 (±6.43) | 0.074 | |
| Shoe | 205 (±6.53) | 0.026* | |
| Tape and shoe | 197 (±6.16) | 0.082 |
*Indicates a significant difference (p<0.05) compared with the barefoot condition.
Tibialis anterior results
Table 2 shows the results for the tibialis anterior. For the peak activity, the shod conditions caused a significant increase compared with barefoot and this was also the case for shoe in the average activity. Tape and shoe did cause an increase in average activity, however, not of statistical significance. There were no significant differences between the taped and non-taped conditions and similarly to the table for the peroneus longus results these have not been included. There were also no significant differences between any conditions in the latency for the tibialis anterior.
Table 2.
Tibialis anterior muscle activity
| Variable | Condition | Mean (SE) | P value |
| Peak activity (µV) | Barefoot | 125 (±14.8) | – |
| Tape (barefoot) | 125 (±11.5) | 0.976 | |
| Shoe | 167 (±15.8) | 0.010* | |
| Tape and shoe | 163 (±15.8) | 0.027* | |
| Average activity (µV) | Barefoot | 31.5 (±4.41) | – |
| Tape (barefoot) | 33.9 (±3.86) | 0.527 | |
| Shoe | 39.9 (±3.64) | 0.012* | |
| Tape and shoe | 37.5 (±2.81) | 0.069 | |
| Latency (ms) | Barefoot | 214 (±6.11) | – |
| Tape (barefoot) | 221 (±4.78) | 0.383 | |
| Shoe | 221 (±3.98) | 0.353 | |
| Tape and Shoe | 215 (±3.97) | 0.917 |
*Indicates a significant difference (p<0.05) compared with the barefoot condition.
Latency between peroneus longus activation to tibialis anterior activation
The time taken for the tibialis anterior to activate following the peroneus longus under each of the conditions was calculated by subtracting the peroneus longus latency time from the tibialis anterior time in each trial and finding the mean. This is demonstrated in figure 4. Although not statistically significant, barefoot had the longest time while shoe had the shortest. There was no significant difference between the conditions.
Figure 4.
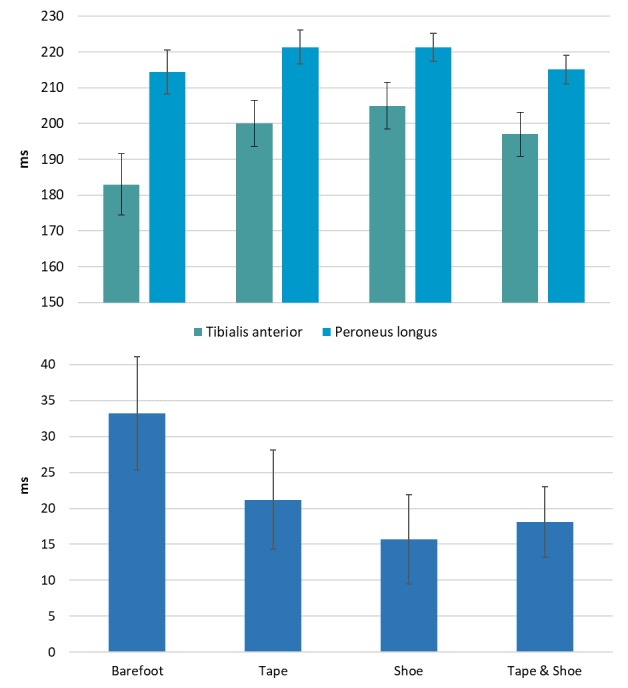
Graph shows the comparison of mean (SE) difference in latency between the peroneus longus and tibialis anterior between test conditions.
Discussion
The aim of this study was to assess the effect of kinesiology tape on ankle stability, in particular, its effects on the primary stabilising muscles of the ankle: the peroneus longus and the tibialis anterior. In order to make this assessment, EMG measurements of the peroneus longus and tibialis anterior were recorded during the sudden ankle inversion perturbations, with and without the use of kinesiology tape and shoes. From the EMG recordings, the peak muscle activity, the average muscle activity and the muscle latency were analysed.
Peak and average activity
The results of the study showed a significant increase in activity of the peroneus longus and tibialis anterior when shoes were worn. This was expected for the peroneus longus following studies by Kerr et al 13 and Ramanathan et al. 15 16 The mechanism likely to be most accountable is due to the greater inversion moment arm that is created by the sole of the shoe raising the foot off the ground. This in turn increases the overall inversion moment. Therefore, in attempting to restore equilibrium about the ankle, the internal eversion moment must increase, and as the moment arm cannot be lengthened, it is the eversion force from the peroneal muscles that needs to increase.
The results for the tibialis anterior show that wearing shoes also increase its activity, similar to the peroneus longus, which is counterintuitive given their antagonistic actions. However, as established by Hopkins et al,6 the tibialis anterior has an increased activity during the gait of those with functional instability. Therefore, increased tibialis anterior activity caused by the shoes may be due to their impairment to proprioception, creating a state of functional instability in the ankle. Another possible reason for this increased activity, which may also explain the increased peroneus longus activity, is again related to the diminished sensory input when wearing shoes.9 17 If there is reduced proprioceptive feedback to the foot and ankle, the ankle musculature, including the peroneus longus and tibialis anterior, will contract to a greater extent in order to reinforce and stabilise the ankle. Thus, producing the observed results.
The lack of significant difference between the activities for the taped and non-taped conditions indicates that the tape offered no mechanical support or proprioceptive improvement, contrary to that proposed by the manufacturers. This mirrors the findings of Briem et al 18 who despite using a different taping method, also found that kinesiology tape had no effect on peroneus longus activity.
Furthermore, it may be the case that the tape in fact reduces proprioception rather than improves it. This is based on the comparison between barefoot and tape for the average peroneus longus activity, which verged on being significant (p<0.059). An explanation for this difference is that the tape covering the relatively large portion of the plantar surface of the foot impedes the tactile interface with the plate and reduces sensory input. Therefore, once the plates come to rest at the 20° inversion stance (when average activity is being measured) the reduced sensory input, particularly of the shear forces between the foot and the platform plate, causes an overall larger peroneal response for the taped condition. This is in attempt to stabilise the ankle.
Latency
The results from the current study found that shoes caused a significantly longer latency period compared with the non-shod conditions for the peroneus longus. Taking into consideration that the peroneal latency is prolonged in unstable ankles, due to afferent denervation,19 it would seem reasonable that the sensory disruption caused by the shoes would also lead to this result. However, this is in contrast to the findings of Kerr et al 13 who reported no difference in the reaction time when shoes were worn. Furthermore, of the two studies by Ramanathan et al,15 16 one found that shoes caused no significant difference to the latency while the other suggested that shoes shorten the latency compared with barefoot, which is the opposite of that found in the current study. One thing noticed between these various studies was the different types of shoes used, such as boots, running shoes and typical leisure shoes which were all of various dimensions and materials. It may be the case that different types of shoes cause different reactions of the peroneus longus. This uncertainty warrants further research as it may be possible to design a shoe that is less damaging to ankle stability.
Again, there was no significant difference between the taped and non-taped conditions, with the tape unable to shorten the prolonging effect of the shoe to the reaction time. These results appear to follow the trend set by Briem et al 18 and Correia et al. 20 Moreover, the tape increased the latency when compared with barefoot, however, this was not of significance (p<0.074). This is likely to be due to the disruption of the sensory input at the plantar surface.
There were no significant differences between the results for the tibialis anterior latency for the difference test conditions. The other aspect of the tibialis anterior reaction time analysed was its period of latency after the peroneus longus contraction. This was considered pertinent following the study by Willems et al 5 who stated that a faster tibialis anterior reaction time is a risk factor for LAS. In the current study, the results showed that shod conditions had a shorter latency period from peroneus longus activation to tibialis anterior activation when compared with the non-shod. This is yet another result eluding to the increased risk of LAS that shoes cause. The tape caused no significant differences.
Limitations
It is acknowledged that for the current study only subjects with healthy ankles were recruited while from the literature it was ascertained that the greatest differences seen from interventions were in those with unstable ankles.7 However, given the instability that is conceded from wearing shoes, the shoes effectively created an ‘unstable’ group.13 15 16 Therefore, comparing shoe to tape and shoe was similar to testing an intervention in a group with unstable ankles.
Acknowledgments
The authors would like to acknowledge Ian Christie for his valuable contribution of bespoke illustrations.
Footnotes
Contributors: All coauthors are in agreement to be accountable for the work presented in this manuscript. ZMS: planning and conducting the study, analysing the data, reporting the study and generating the write up. GPA: coplanning, analysing data. WW: statistical analysis. RJA: reporting the study, revision of original manuscript, designing the footplates, submitting the study.
Funding: This study was internally funded by the department.
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: The study was approved by the University Medical School Research Ethics Committee (Ref: SMED REC 109/18).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: All data relevant to the study are included in the article or uploaded as online supplementary information. All data relevant to the study are included in the article.
References
- 1. Garrick JG. The frequency of injury, mechanism of injury, and epidemiology of ankle sprains*. Am J Sports Med 1977;5:241–2. 10.1177/036354657700500606 [DOI] [PubMed] [Google Scholar]
- 2. Yeung MS, Chan KM, So CH, et al. An epidemiological survey on ankle sprain. Br J Sports Med 1994;28:112–6. 10.1136/bjsm.28.2.112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Fong DTP, Chan Y-Y, Mok K-M, et al. Understanding acute ankle ligamentous sprain injury in sports. BMC Sports Sci Med Rehabil 2009;1:14 10.1186/1758-2555-1-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Menacho MdeO, Pereira HM, Oliveira BIRde, et al. The peroneus reaction time during sudden inversion test: systematic review. J Electromyogr Kinesiol 2010;20:559–65. 10.1016/j.jelekin.2009.11.007 [DOI] [PubMed] [Google Scholar]
- 5. Willems TM, Witvrouw E, Delbaere K, et al. Intrinsic risk factors for inversion ankle sprains in females--a prospective study. Scand J Med Sci Sports 2005;15:336–45. 10.1111/j.1600-0838.2004.00428.x [DOI] [PubMed] [Google Scholar]
- 6. Hopkins JT, Coglianese M, Glasgow P, et al. Alterations in evertor/invertor muscle activation and center of pressure trajectory in participants with functional ankle instability. J Electromyogr Kinesiol 2012;22:280–5. 10.1016/j.jelekin.2011.11.012 [DOI] [PubMed] [Google Scholar]
- 7. Surve I, Schwellnus MP, Noakes T, et al. A Fivefold reduction in the incidence of recurrent ankle Sprains in soccer players using the Sport-Stirrup orthosis. Am J Sports Med 1994;22:601–6. 10.1177/036354659402200506 [DOI] [PubMed] [Google Scholar]
- 8. Dewar RA, Arnold GP, Wang W, et al. The effects of wearing an Ankle Stabilizing Orthosis (ASO) ankle brace on ankle joints kinetics and kinematics during a basketball rebounding task. Foot 2019;40:34–8. 10.1016/j.foot.2019.05.003 [DOI] [PubMed] [Google Scholar]
- 9. Robbins S, Waked E, Rappel R. Ankle taping improves proprioception before and after exercise in young men. Br J Sports Med 1995;29:242–7. 10.1136/bjsm.29.4.242 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Metcalfe RC, Schlabach GA, Looney MA, et al. A comparison of moleskin tape, linen tape, and lace-up brace on joint restriction and movement performance. J Athl Train 1997;32:136–40. [PMC free article] [PubMed] [Google Scholar]
- 11. Kase K, Wallis J, Kase T. Clinical Theraputic applications of the Kinesio Taping method. 3rd edn Albuquerque, NM, 2013. [Google Scholar]
- 12. Williams S, Whatman C, Hume PA, et al. Kinesio taping in treatment and prevention of sports injuries: a meta-analysis of the evidence for its effectiveness. Sports Med 2012;42:153–64. 10.2165/11594960-000000000-00000 [DOI] [PubMed] [Google Scholar]
- 13. Kerr R, Arnold GP, Drew TS, et al. Shoes influence lower limb muscle activity and may predispose the wearer to lateral ankle ligament injury. J Orthop Res 2009;27:318–24. 10.1002/jor.20744 [DOI] [PubMed] [Google Scholar]
- 14. Vaes P, Duquet W, Van Gheluwe B. Peroneal reaction times and eversion motor response in healthy and unstable ankles. J Athl Train 2002;37:475–80. [PMC free article] [PubMed] [Google Scholar]
- 15. Ramanathan AK, Parish EJ, Arnold GP, et al. The influence of shoe sole's varying thickness on lower limb muscle activity. Foot Ankle Surg 2011;17:218–23. 10.1016/j.fas.2010.07.003 [DOI] [PubMed] [Google Scholar]
- 16. Ramanathan AK, Wallace DT, Arnold GP, et al. The effect of varying footwear configurations on the peroneus longus muscle function following inversion. Foot 2011;21:31–6. 10.1016/j.foot.2010.11.001 [DOI] [PubMed] [Google Scholar]
- 17. Abboud RJ. (I) relevant foot biomechanics. Curr Orthop 2002;16:165–79. 10.1054/cuor.2002.0268 [DOI] [Google Scholar]
- 18. Briem K, Eythörsdöttir H, Magnúsdóttir RG, et al. Effects of Kinesio tape compared with nonelastic sports tape and the Untaped ankle during a sudden inversion perturbation in male athletes. J Orthop Sports Phys Ther 2011;41:328–35. 10.2519/jospt.2011.3501 [DOI] [PubMed] [Google Scholar]
- 19. Freeman MAR, Dean MRE, Hanham IWF. The etiology and prevention of functional instability of the foot. J Bone Joint Surg Br 1965;47-B:678–85. 10.1302/0301-620X.47B4.678 [DOI] [PubMed] [Google Scholar]
- 20. Correia C, Lopes S, Gonçalves R, et al. Kinesiology taping does not change fibularis longus latency time and postural sway. J Bodyw Mov Ther 2016;20:132–8. 10.1016/j.jbmt.2015.07.037 [DOI] [PubMed] [Google Scholar]