

Abstract
Background
Plasma lactate concentrations and their trends over time are used for clinical prognosis, and to guide treatment, in critically ill patients. Although heavily relied upon for clinical decision-making, lactate kinetics of these patients is sparsely studied.
Aim
To establish and validate a feasible method to study lactate kinetics in critically ill patients.
Methods
Healthy volunteers (n = 6) received a bolus dose of 13C-labeled lactate (20 μmol/kg body weight), and 43 blood samples were drawn over 2 h to determine the decay in labeled lactate. Data was analyzed using non-compartmental modeling calculating rates of appearance (Ra) and clearance of lactate. The area under the curve (AUC) was calculated using a linear-up log-down trapezoidal approach with extrapolation beyond 120 min using the terminal slope to obtain the whole AUC. After evaluation, the same protocol was used in an unselected group of critically ill patients (n = 10).
Results
Ra for healthy volunteers and ICU patients were 12.8 ± 3.9 vs 22.7 ± 11.1 μmol/kg/min and metabolic clearance 1.56 ± 0.39 vs 1.12 ± 0.43 L/min, respectively. ICU patients with normal lactate concentrations showed kinetics very similar to healthy volunteers. Simulations showed that reducing the number of samples from 43 to 14 gave the same results. Our protocol yielded results on lactate kinetics very similar to previously published data using other techniques.
Conclusion
This simple and user-friendly protocol using an isotopically labeled bolus dose of lactate was accurate and feasible for studying lactate kinetics in critically ill ICU patients.
Trial registration
ANZCTR, ACTRN12617000626369, registered 8 March 2017. https://anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372507&isReview=true
Keywords: Lactate, Lactate kinetics, Labeled lactate, Stable isotope, ICU, Method validation
Background
The correlation between elevated plasma lactate concentrations and in-hospital mortality is firmly established in both intensive care and emergency department settings. A failure to normalize an initially elevated lactate concentration is an even stronger predictor of an unfavorable outcome [1–5]. Lactate is therefore used as a triage tool [6–8] and is recommended to be measured within 1 h in suspected sepsis [9]. These relationships are most thoroughly studied in septic patients, but similar correlations are shown in other conditions as well [10].
Although heavily relied upon for clinical decision-making, most knowledge on lactate in critical illness comes from retrospective and prospective observational clinical data. Reports on lactate metabolism and kinetics in ICU patients are sparse. This may be because of a common misconception that lactate is simply the end product of anaerobic metabolism during hypoxia. However, lactate metabolism is far more complex, and plasma lactate concentrations may be altered by e.g. metabolic stress through β-stimulation [11–13] or pharmacological substances [14, 15]. Lactate can also serve as an energy substrate in various organs, such as the heart and the brain, and is a precursor for gluconeogenesis in the liver and kidney [16–19]. Lactate plays a vital role as an energy substrate in septic rats, as animals depleted from endogenous lactate production quickly die, but show improved survival when substitution with exogenous lactate is given [20]. An elevated lactate could potentially arise from either an increase in lactate production or an impairment in lactate utilization (or clearance). Although most data suggest that an increase in lactate production is present [21], there are also reports of an additional impairment in utilization in some subjects from both animal models [22] and septic patients [23] and that this impairment correlates with worsened outcome [22, 24].
To deepen the understanding of lactate metabolism, which could help to improve treatment and avoid potential pitfalls, it is important to investigate lactate kinetics, production as well as clearance, in a variety of patient populations. However, the most frequently used method, with a primed continuous infusion of labeled lactate, will be problematic to use in acutely ill unstable patients. Also, performing extensive sampling in severely ill patients comes with practical and ethical considerations. To facilitate future clinical scientific studies of lactate kinetics, methods with high accuracy, and minimal risk of harm and interference of ongoing care, are needed. We therefore performed a study aiming to develop a relatively simple and feasible protocol for the ICU setting, using a bolus dose of 13C-labeled lactate to study lactate kinetics. To achieve this, we initially studied healthy volunteers and subsequently applied the same protocol to ten critically ill patients.
Methods
Patient population and ethical considerations
Six healthy volunteers were recruited after oral and written informed consent and screened for past and present illness. ICU patients were screened for eligibility and recruited after informed consent (or from next of kin when appropriate). The study was approved by the regional ethics committee (Stockholm, Sweden, no. 2016/722-31/1), and amendments were approved after the first part (volunteers) was completed. The study was registered at ANZCTR (ACTRN12617000626369).
Experimental setup
In part I, volunteers were studied after an overnight fast. A peripheral venous catheter and an arterial catheter were inserted after the application of local anesthesia. In part II, all ICU patients had both venous and arterial catheters, as part of ongoing care, prior to enrollment. ICU patients were studied with ongoing nutrition according to the local protocol. For the ICU patients, their ideal weight was assessed as:
The body weight used for each ICU subject was:
Measured weight was used for the healthy volunteers.
Baseline samples were drawn, and a 13C-labeled lactate containing solution was administered intravenously over 20 s (20 μmol of sodium-lactate/kg body weight, diluted with isotonic NaCl, to a final volume of 20 mL). The amount of lactate given was based on the rate of appearance (Ra) for lactate from our previous study [25], the lactate pool size, and our experience from a bolus approach with labeled glutamine [26]. After baseline samples were drawn, administration of lactate started at t = 0 and a total of 42 arterial blood samples were drawn in the following 2 h. Sampling was performed at t = 2 min and then every 2 min for the first hour and every 5 min in the following hour. At each sampling, blood was drawn in an EDTA tube, centrifuged at 2000g for 10 min, plasma extracted, and immediately frozen and kept at − 80 °C until analysis. During the first 16 min, a total of five additional arterial blood samples were taken and immediately analyzed on a point-of-care blood gas analyzer for plasma lactate concentration. In total, approximately 100 mL of blood was sampled from each subject.
Laboratory analysis and specifications
1-13C-labeled sodium-lactate (Cambridge Isotope Laboratory, Tewksbury, MA, USA) for i.v. administrations was prepared by a licensed pharmacy (APL, Stockholm, Sweden) before use. Arterial blood samples were analyzed for plasma lactate concentrations on a blood gas analyzer (ABL 800 flex, Radiometer Medical Aps, Copenhagen, Denmark). Frozen plasma samples were defrosted and analyzed by gas chromatography-mass spectroscopy (GS-MS) (Inert XL MSD. 5975C, Agilent Technologies, Santa Clara, CA, USA) as previously described [25] for the 13C-lactate enrichment and expressed as molar percent excess (MPE).
Statistics and mathematical modeling
Data was analyzed using Excel (2016, Microsoft Software, Redmond, WA, USA) and Prism (7.02, GraphPad Software, La Jolla, CA, USA).
For each test subject, a decay curve was obtained by plotting enrichment data against time. Non-compartmental analysis was used, where linear elimination from the central compartment was assumed (for details, see Additional file 1). As enrichment did not reach base line within the 2 h, data were transformed to the logarithmic domain and the terminal slope (λz) was determined by extrapolation (from t = 70 min). As the first sample was drawn after 2 min and the bolus given over 20 s, we extrapolated the “early” phase (points 2, 4, 6 min) back to t = 0.5 min in the log domain, and the corresponding MPE was calculated. A straight line was drawn from zero to this point. These boundaries were then used to calculate the area under the curve (AUC) using a linear-up log-down trapezoidal method according to:
Rate of appearance (Ra; μmol/kg/min) was calculated as:
where Dose [13CLactate] refers to the amount of tracer given per kg body weight. Ra is the amount or lactate that appears into the plasma, and when no exogenous lactate is given, this represents de novo tissue synthesized lactate that is released into the plasma. Clearance (L/min) was calculated as:
Three patients had ongoing continuous renal replacement treatment (CRRT) during the study period. Loss of lactate through this route was assessed by collecting dialysate during the study period and measure volume and lactate concentration of the dialysate. CRRT clearance of lactate was calculated as the excreted amount per time divided by plasma concentration. Finally, CRRT clearance was subtracted from total clearance (given by the above formula) to get a metabolic clearance comparable to the other subjects.
The non-compartmental pharmacokinetic analysis was performed in accordance with reference text books [27]. Further details and equations are presented in Additional file 1.
Simulations to determine the accuracy with a lower number of samples were performed, using the following time points: baseline, 2, 4, 6, 8, 16, 30, 60, 70, 80, 90, 100, 110, and 120 min.
The healthy volunteers and the ICU patients were compared using an unpaired two-sided t test with Welch’s correction (not assuming the same standard deviation in both groups) or Mann-Whitney test, respectively, for normal and non-normal distributed data according to Shapiro-Wilks normality test. Results are expressed as mean ± SD or median (range).
Results
Baseline characteristics for the volunteers and ICU patients are presented in Tables 1 and 2. The volunteers were younger, had a similar body weight (83 vs 79 kg), and had a smaller male predominance (67% vs 90%).
Table 1.
Baseline characteristics of healthy volunteers
| Age (years) | Sex | Weight (kg) | Height (cm) | Plasma lactate (mmol/L) |
|---|---|---|---|---|
| 23 | M | 84 | 187 | 0.9 |
| 23 | M | 77 | 187 | 0.6 |
| 47 | F | 74 | 165 | 0.6 |
| 54 | F | 66 | 165 | 0.4 |
| 32 | M | 109 | 182 | 0.8 |
| 23 | M | 88 | 185 | 0.8 |
Table 2.
ICU patients
| Age (years) | Sex | Weight (kg) | Height (cm) | ICU diagnosis | Plasma lactate (mmol/L) | Alive at 30 days | CRRT | SAPS 3 | SOFA |
|---|---|---|---|---|---|---|---|---|---|
| 42 | M | 87 | 181 | Liver transplantation | 2.1 | Y | Y | 27 | 9 |
| 70 | M | 78 | 187 | Respiratory insufficiency | 1.3 | Y | N | 56 | 2 |
| 75 | M | 75 | 184 | Respiratory insufficiency | 0.7 | Y | N | 51 | 7 |
| 35 | F | 38 | 167 | Intoxication | 0.6 | Y | N | 29 | 2 |
| 61 | M | 80 | 185 | Bowel ischemia | 0.6 | Y | N | 45 | 6 |
| 50 | M | 77 | 176 | Liver failure | 4.9 | N | Y | 55 | 5 |
| 73 | M | 90 | 178 | Sepsis | 1.5 | Y | N | 56 | 4 |
| 75 | M | 88 | 175 | Fluid overload | 0.8 | Y | N | 66 | 5 |
| 63 | M | 99 | 198 | Pneumonia | 3.5 | N | Y | 55 | 9 |
| 60 | M | 76 | 178 | Respiratory insufficiency | 4.0 | N | N | 50 | 12 |
LOS length of stay, CRRT continuous renal replacement therapy during the study period, SAPS Simplified Acute Physiology Score (at admission), SOFA Sequential Organ Failure Assessment score (at the day of investigation)
In the healthy volunteers, 2 samples (0.8%) were lost due to mishandling; in ICU patients, a total of 13 samples (3%) were lost in two patients due to arterial line malfunction. Missing data were not replaced but handled by the log-down trapezoidal method.
The 13C-lactate bolus resulted in decay curves that allowed for calculations of the AUC (Fig. 1 and Additional file 2). Since 13C-lactate levels had not returned to baseline at 120 min, the terminal slope was estimated and the whole extrapolated AUC used for kinetic calculations. The extrapolated AUC for the volunteers and the ICU patients were 6.7 and 9.7% of the total AUC, respectively (Table 3). In healthy volunteers, the administration of labeled lactate increased plasma lactate slightly (0.1–0.2 mmol/L), after 2–4 min, but concentrations had returned to baseline at after 8 min in all subjects. In ICU patients, this effect was even less pronounced and all subjects returned to baseline lactate concentrations at t = 4 min (Additional file 3: Fig. S1).
Fig. 1.

Plasma enrichment of labeled lactate over time in all subjects. Decay curves of plasma lactate enrichments after a bolus dose of 13C-labeled lactate in healthy volunteers (filled black lines, n = 6) and ICU patients (red dotted lines n = 10). The left panel includes all values, 43 samples per subject, and the right panel shows a reduced number, 14 samples per subject
Table 3.
Comparison for lactate kinetic parameters between volunteers and ICU patients by non-compartmental analysis
| Volunteers (n = 6) | ICU patients (n = 10) | p | |
|---|---|---|---|
| AUC total [% × min] | 172 ± 50 | 105 ± 43 | 0.021 |
| AUCextrap [% × min] | 11.6 ± 7.8 | 9.0 ± 4.9 | 0.474 |
| AUCextrap [% of AUC total] | 6.7 ± 4.2 | 9.7 ± 7.0 | 0.300 |
| Ra [μmol/kg/min] | 12.8 ± 3.9 | 22.7 ± 11.1 | 0.025 |
| Ra [mmol/min] | 1.1 ± 0.5 | 1.8 ± 0.9 | 0.067 |
| Metabolic clearance [L/min] | 1.56 ± 0.39 | 1.12 ± 0.43 | 0.058 |
| Plasma lactate [mmol/L] | 0.7 (0.4–0.9) | 1.4 (0.6–4.9) | 0.065 |
| AUMC total [% × min2] | 5138 ± 2350 | 3899 ± 1358 | 0.263 |
| MRT [min] | 25.8 (21.6–51.2) | 33.3 (22.8–82.2) | 0.076 |
| Vss [L] | 45.4 ± 14.0 | 42.0 ± 14.7 | 0.649 |
| Vc [L] | 9.6 ± 2.5 | 9.7 ± 3.0 | 0.937 |
Values are presented as means ± standard deviation or medians (range) as appropriate according to Shapiro Wilk’s normality test. p values refer to unpaired two-sided t test with Welch’s correction (not assuming the same standard deviation in both groups) or Mann-Whitney test for nonparametric data. AUC area under the curve, AUCextrap the part of AUC that is beyond the last measurement point, Ra rate of appearance, AUMC area under the first moment curve, MRT mean residence time, Vss volume of distribution at steady state, Vc central volume of distribution. Details of the pharmacokinetic non-compartmental modeling are presented in Additional file 1
The main findings are presented in Table 3. Plasma lactate concentration and Ra for healthy volunteers and ICU patients were 0.7 (0.4–0.9) vs 1.4 (0.6–4.9) mmol/L, p = 0.065, and 12.8 ± 3.9 vs 22.7 ± 11.1 μmol/kg body weight/min, p = 0.025, respectively. Metabolic clearances were 1.56 ± 0.39 vs 1.12 ± 0.43 L/min, p = 0.058. For the 3 patients on CRRT, the CRRT clearance contributed with 2.4 to 4.7% of the total lactate clearance. Central volume of distribution and volume of distribution at steady state for labeled lactate were 9.6 ± 2.6 vs 9.7 ± 3.0 L, p = 0.9 and 45.4 ± 14.0 vs 42.0 ± 14.7 L, p = 0.65. Absolute Ra was 1.1 ± 0.5 vs 1.8 ± 0.9, mmol/min, p = 0.07, for healthy volunteers and ICU patients, respectively. For measurements in the ICU patients, there were statistically significant correlations between plasma concentration and Ra of lactate, r2 = 0.84 (p < 0.0002), and lactate metabolic clearance, r2 = 0.48 (p = 0.025) (Fig. 2).
Fig. 2.
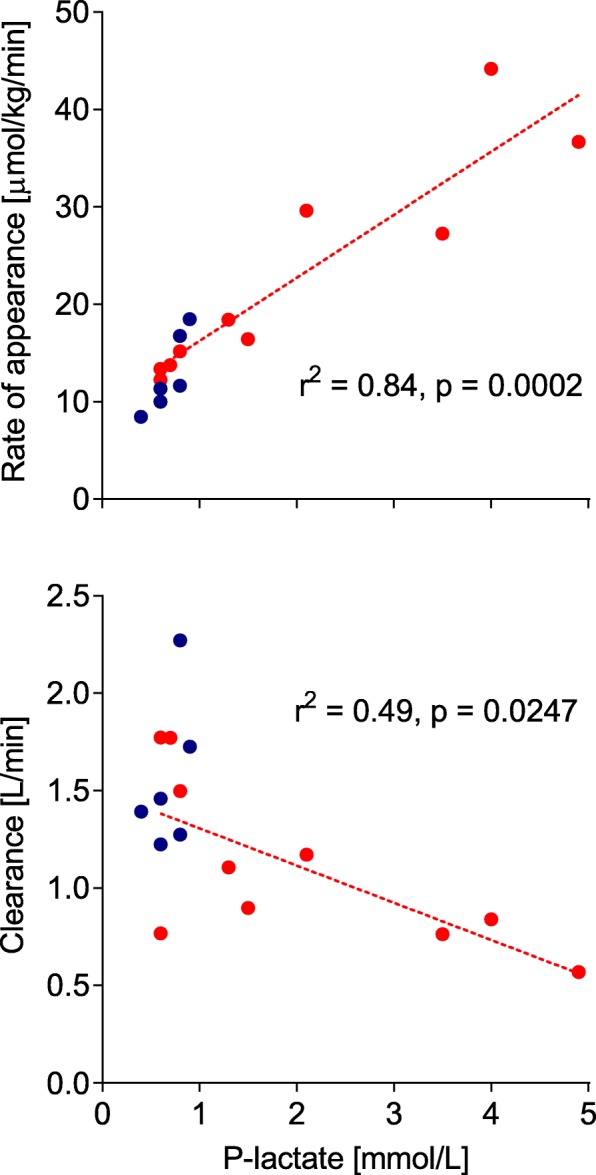
Relationship between plasma concentration and rate of appearance and clearance of lactate. Relation between plasma lactate concentrations and rate of appearance of lactate (upper panel) and metabolic clearance of lactate (bottom panel) as calculated from a bolus dose of 13C-labeled lactate in healthy volunteers (blue circles, n = 6) and ICU patients (red circles, n = 10). The lines of regression and associated statistics apply to the group of ICU patients only
When the number of blood samples was reduced to 14, the decay curves were similar to the full protocol using 43 samples (Fig. 1) and the impact on the results of the non-compartmental analysis was negligible (Table 4).
Table 4.
Comparison between 43 and 14 sample protocols
| N = 43 | N = 14 | p | |
|---|---|---|---|
| AUCtot [% × min] | 130 ± 55 | 132 ± 57 | 0.054 |
| AUCextrap [% × min] | 10.0 ± 6.0 | 10.3 ± 7.2 | 0.538 |
| λz 70 [min−1] | − 0.015 ± 0.006 | − 0.015 ± 0.006 | 0.748 |
| Ra [μmol/kg/min] | 15.8 (8.5–44.2) | 15.8 (8.3–44.2) | 0.404 |
Mean ± SD or median (range) for all subjects (healthy volunteers and ICU patients). Differences between protocols are analyzed by paired t test or Wilcoxon test for nonparametric data. AUCtot area under the curve, AUCextrap the part of AUC that is beyond the last measurement point, λz 70 terminal slope as calculated from t = 70 min, Ra rate of appearance of lactate. Details of the pharmacokinetic non-compartmental modeling are presented in Additional file 1
When ICU patients were dichotomized into groups with normal plasma lactate (≤ 2 mmol/L, n = 6, median lactate 0.9 mmol/L) and elevated plasma lactate (> 2 mmol/L, n = 4, median lactate 3.8 mmol/L), those with normal plasma concentrations had lactate kinetics more similar to the healthy volunteers as Ra (both absolute and per body weight) and plasma clearance was almost identical (Table 5).
Table 5.
Comparison between volunteers and ICU patients with normal and elevated plasma lactate
| Volunteers (n = 6) | ICU, normal lactate (n = 6) | ICU, elevated lactate (n = 4) | |
|---|---|---|---|
| P-lactate [mmol/L] | 0.7 (0.4–0.9) | 0.8 (0.6–1.5) | 3.8 (2.1–4.9) |
| Ra [μmol/kg/min] | 11.5 (8.5–18.5) | 14.5 (12.3–18.4) | 33.2 (27.3–44.2) |
| Metabolic clearance [L/min] | 1.43 (1.22–2.27) | 1.30 (0.77–1.77) | 0.80 (0.57–1.17) |
| Vc [L] | 9.0 (7.0–14.2) | 8.4 (5.3–13.5) | 10.3 (7.6–14.7) |
Normal lactate ≤ 2 mmol/L, elevated lactate > 2 mmol/L. Data are presented as median (range). Ra rate of appearance of lactate, Vc central distribution volume
Discussion
In this study, we examined a tracer bolus approach to study lactate kinetics in critically ill ICU patients. The feasibility was first demonstrated in healthy volunteers with normal plasma lactate concentrations. The protocol was then repeated in an unselected group of critically ill ICU patients, with normal or elevated plasma lactate concentrations, with comparable feasibility. Simulations showed that the accuracy of the method was unchanged when sampling was decreased from 43 to 14 samples. Therefore, we advocate the use of this technique in clinical studies of lactate kinetics.
The 13C-lactate bolus initially increased the lactate concentrations slightly, but the levels returned to baseline within 8 min and are unlikely to affect the measured lactate kinetics over the 120 min. This was expected, as the bolus we gave (20 μmol/kg) was equivalent to roughly twice the rate of appearance per minute in the healthy volunteers. Lowering the bolus would compromise the accuracy of the MPE measurements and the calculation of the AUC. About 10% of the total AUC of the decay curve is after the 120 min sampling period, suggesting that it is important to include the terminal slope in the kinetic calculations. We corrected the clearance for the clearance via loss with CRRT. Although the contribution of the CRRT clearance was less than 5% of the total clearance, it is important to measure this and correct for it. This number may seem small as lactate is a small molecule that is easily dialyzed. However, lactate has a high turnover with high production and clearance (rate of disappearance from plasma) throughout the body and therefore the percentage of the turnover that is removed by dialysis is low.
Continuous infusions of labeled lactate have been used to study lactate metabolism in different populations. We wanted to validate a bolus approach in the ICU settings to stay independent of the underlying assumptions of the continuous infusion approach, such as the appropriate size of the priming dose, and the assumption of a tracer steady state. Both assumptions are problematic in ICU patients, especially in the acute unstable clinical situation when lactate metabolism is most interesting to study. To determine the usefulness and validity of our protocol, the results should be similar to the results obtained with other methods. In resting healthy volunteers (all male and younger), lactate Ra is 11 ± 2 μmol/kg body weight/min [25], similar to the present group of volunteers. This is also close to the Ra of 15 and 12 μmol/kg/min that are reported in lean and obese healthy humans [28] and in the healthy volunteers used as controls by Revelly et al. (11.2 ± 2.7 μmol/kg/min) [29], all using different protocols for continuous infusion of labeled lactate. During rest, elite cross-country skiers produce roughly the same amount of lactate, approximately 1.5 mmol/min [30], as volunteers in the present study (1.1 mmol/min). In conclusion, our results agree with previously published results using different methodology in healthy human subjects, supporting the validity of our protocol.
In one of the few studies on lactate metabolism in ICU patients, Revelly et al. [29] used a complex protocol infusing labeled lactate at a rate of 10 μmol/kg/min, which after 2 h was increased to 20 μmol/kg/min for another 2 h. Unfortunately, this protocol may affect lactate metabolism as the infused amount almost matches the endogenous lactate production. This is acknowledged by the authors, whom only report production during the lower infusion rate. They report a Ra of 26 ± 11 μmol/kg/min in severe sepsis (n = 7) and 26 ± 5 μmol/kg/min in cardiogenic shock (n = 7).
Levraut et al. assessed lactate kinetics without the use of labeled substrates but by administering 1 mmol/kg sodium-lactate and measuring the subsequent decrease in plasma lactate in hemodynamically stable, normolactemic, and slightly hyperlactemic septic patients (total n = 34) [23]. Both the normal and slightly hyperlactemic patients showed similar lactate production rates (20 ± 5 vs 20 ± 4 μmol/kg/min) but differed in clearance (1.0 ± 0.28 vs 0.47 ± 0.10 L/kg/h, p < 0.0001). In their subsequent trial, they included septic ICU patients with lactate concentration < 3 mmol/L (n = 56) [24]. In this trial, survivors, in comparison to non-survivors, have a higher lactate clearance (0.86 ± 0.32 vs 0.58 ± 0.18 L/kg/h, p = 0.016) and a tendency towards a higher lactate production (20 ± 10 vs 15 ± 4 μmol/kg/min, p = 0.055), but no difference in plasma lactate concentration. Both of these studies, using the unlabeled lactate, show similar Ra and clearance rates as the ICU patients in the present study. However, this methodology has limitations as the subject’s lactate concentration actually increases by approximately 1.5 mmol/L, which makes it more difficult to assume that the measurement itself does not affect lactate metabolism.
In both healthy volunteers and ICU patients, the initial volume of distribution (Vc) was 10 L, which may correspond to the body’s visceral high flow compartment. The total volume of distribution (Vss) was approximately 43 L, which is in the same range as total body water. We find these results plausible since lactate, a small, water-soluble, charged molecule, is likely to behave in the same way as other similar molecules such as ethanol [31].
As one of the aims of this study was to establish a user-friendly protocol, we examined whether reducing the number of blood samples was possible without affecting the results. Simulations showed that decreasing sampling from 43 to 14 samples did not alter kinetic rates (Table 4). This indicates that a reliable protocol is possible with approximately 30 mL of blood sampling.
Within our approach, we made some assumptions. As we did not sample before t = 2 min, we have no means of knowing the exact enrichment of labeled lactate before that time point. We chose to extrapolate back to 0.5 min (rather than 0 min) which will give a short time for the substance to mix evenly throughout the blood, since we gave the bolus over the first 20 s. Previously, Avram et al. have shown that concentrations of administered substances show great variability in the first minute, especially in conditions with affected cardiac output [32], which could pose a problem in hemodynamically affected patients. We therefore assume that our approach will give a reasonable average of the levels of enrichment during the first 2 min.
In this study, we made statistical comparisons between the results from the healthy volunteers and the unselected ICU patients (Table 3). We are aware that these two groups do not belong to the same cohort, regarding e.g. background physiology, and are therefore in a strict sense not comparable. The statistical comparison should therefore be seen just as a comparison of the numerical values and be interpreted with care. On the other hand, the correlations of the Ra and clearance with lactate concentrations in the ICU patients showed a strong correlation between lactate levels and lactate metabolism. Also, when the hyperlactemic ICU patients were excluded, the normolactemic ICU patients and the healthy volunteers had very similar lactate kinetics.
The patients with elevated plasma lactate had a higher Ra and possibly a lower clearance as compared to normolactemic ICU patients (Table 5). From the correlations (Fig. 2) between lactate concentrations and Ra and clearance, we can hypothesize that critically ill patients with elevated lactate have high lactate production rates as well as low clearance. Since the study was not designed to investigate these differences, no statistical analysis is presented and we consider the results as hypothesis generating. The main aim of this study was to design a protocol that can be used to study lactate kinetics in various, larger, ICU cohorts. Hopefully, these future studies will allow us to differentiate between patients with different lactate kinetics and thereby improve the care of critically ill patients.
Conclusion
In conclusion, we present a feasible, reliable, and user-friendly protocol that yields similar results as more complex protocols to elucidate lactate kinetics in healthy volunteers as well as ICU patients. This may be useful for larger studies on lactate metabolism in septic and other patient groups, with the aim to study to what degree high production rates or low clearance rates contribute to hyperlactatemia.
Supplementary information
Additional file 1. Complete documentation of formulas used for mathematical modelling of data.
Additional file 2. Plasma lactate enrichment of labeled lactate for healthy volunteers and ICU patients
Additional file 3. Individual values for lactate concentrations in plasma for healthy volunteers and ICU patients during experiment.
Acknowledgements
Towe Jakobsson for laboratory analysis and Kristina Kilsand for screening and recruitment of the patients.
Authors’ contributions
JG co-designed the study, wrote CRF, recruited and characterized the ICU patients, performed the statistical analysis for ICU patients, and wrote the manuscript and specific funding applications. TF performed the experiments on healthy volunteers and performed the statistical analysis on healthy volunteers. PP recruited the ICU patients and performed the laboratory analysis. JW co-designed the study, co-wrote the manuscript, and wrote the ethical application. ÅN co-designed the study, performed the kinetic modeling, interpreted the model, and co-wrote the manuscript. OR designed the study, co-performed the kinetic modeling and interpretation, and co-wrote the manuscript. All authors read and approved the final manuscript.
Funding
The study received funding through the European Society of Intensive Care Medicine (ESICM) Clinical Research Award (Paris, 2018) and Lars Bindslevs Memorial Fund (Stockholm 2018), as well as researchers’ personal grants from Stockholm County Council. None of the funding sources have had any impact on the study design, sample collection, analysis, or interpretation of data.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study was approved by the regional ethics committee in Stockholm (Stockholm, Sweden, no. 2016/722-31/1). All participants gave informed consent after written and oral information. In some cases, the consent was given by the next of kin after information as specified in the ethical permit.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s13054-020-2753-6.
References
- 1.Zhou X, Liu D, Su L. Lactate and stepwise lactate kinetics can be used to guide resuscitation. Crit Care. 2017;21(1):267. doi: 10.1186/s13054-017-1859-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Varis E, Pettila V, Poukkanen M, Jakob SM, Karlsson S, Perner A, Takala J, Wilkman E. Evolution of blood lactate and 90-day mortality in septic shock. A post hoc analysis of the FINNAKI study. Shock. 2017;47(5):574–581. doi: 10.1097/SHK.0000000000000772. [DOI] [PubMed] [Google Scholar]
- 3.Howell MD, Davis AM. Management of sepsis and septic shock. JAMA. 2017;317(8):847–848. doi: 10.1001/jama.2017.0131. [DOI] [PubMed] [Google Scholar]
- 4.Gu WJ, Zhang Z, Bakker J. Early lactate clearance-guided therapy in patients with sepsis: a meta-analysis with trial sequential analysis of randomized controlled trials. Intensive Care Med. 2015;41(10):1862–1863. doi: 10.1007/s00134-015-3955-2. [DOI] [PubMed] [Google Scholar]
- 5.Suistomaa M, Ruokonen E, Kari A, Takala J. Time-pattern of lactate and lactate to pyruvate ratio in the first 24 hours of intensive care emergency admissions. Shock. 2000;14(1):8–12. doi: 10.1097/00024382-200014010-00002. [DOI] [PubMed] [Google Scholar]
- 6.Park YJ, Kim DH, Kim SC, Kim TY, Kang C, Lee SH, Jeong JH, Lee SB, Lim D. Serum lactate upon emergency department arrival as a predictor of 30-day in-hospital mortality in an unselected population. PLoS One. 2018;13(1):e0190519. doi: 10.1371/journal.pone.0190519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Junhasavasdikul D, Theerawit P, Ingsathit A, Kiatboonsri S. Lactate and combined parameters for triaging sepsis patients into intensive care facilities. J Crit Care. 2016;33:71–77. doi: 10.1016/j.jcrc.2016.01.019. [DOI] [PubMed] [Google Scholar]
- 8.Ward MJ, Self WH, Singer A, Lazar D, Pines JM. Cost-effectiveness analysis of early point-of-care lactate testing in the emergency department. J Crit Care. 2016;36:69–75. doi: 10.1016/j.jcrc.2016.06.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med. 2018;46(6):997–1000. doi: 10.1097/CCM.0000000000003119. [DOI] [PubMed] [Google Scholar]
- 10.Hajjar LA, Almeida JP, Fukushima JT, Rhodes A, Vincent JL, Osawa EA, Galas FR. High lactate levels are predictors of major complications after cardiac surgery. J Thorac Cardiovasc Surg. 2013;146(2):455–460. doi: 10.1016/j.jtcvs.2013.02.003. [DOI] [PubMed] [Google Scholar]
- 11.Bundgaard H, Kjeldsen K, Suarez Krabbe K, van Hall G, Simonsen L, Qvist J, Hansen CM, Moller K, Fonsmark L, Lav Madsen P, et al. Endotoxemia stimulates skeletal muscle Na+-K+-ATPase and raises blood lactate under aerobic conditions in humans. Am J Physiol Heart Circ Physiol. 2003;284(3):H1028–H1034. doi: 10.1152/ajpheart.00639.2002. [DOI] [PubMed] [Google Scholar]
- 12.Levy B, Desebbe O, Montemont C, Gibot S. Increased aerobic glycolysis through beta2 stimulation is a common mechanism involved in lactate formation during shock states. Shock. 2008;30(4):417–421. doi: 10.1097/SHK.0b013e318167378f. [DOI] [PubMed] [Google Scholar]
- 13.Levy B. Lactate and shock state: the metabolic view. Curr Opin Crit Care. 2006;12(4):315–321. doi: 10.1097/01.ccx.0000235208.77450.15. [DOI] [PubMed] [Google Scholar]
- 14.Green JP, Berger T, Garg N, Suarez A, Hagar Y, Radeos MS, Panacek EA. Impact of metformin use on the prognostic value of lactate in sepsis. Am J Emerg Med. 2012;30(9):1667–1673. doi: 10.1016/j.ajem.2012.01.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Park J, Hwang SY, Jo IJ, Jeon K, Suh GY, Lee TR, Yoon H, Cha WC, Sim MS, Carriere KC, et al. Impact of metformin use on lactate kinetics in patients with severe sepsis and septic shock. Shock. 2017;47(5):582–587. doi: 10.1097/SHK.0000000000000782. [DOI] [PubMed] [Google Scholar]
- 16.van Hall G. Lactate kinetics in human tissues at rest and during exercise. Acta Physiol. 2010;199:499–508. doi: 10.1111/j.1748-1716.2010.02122.x. [DOI] [PubMed] [Google Scholar]
- 17.van Hall G, Stromstad M, Rasmussen P, Jans O, Zaar M, Gam C, Quistorff B, Secher NH, Nielsen HB. Blood lactate is an important energy source for the human brain. J Cereb Blood Flow Metab. 2009;29(6):1121–1129. doi: 10.1038/jcbfm.2009.35. [DOI] [PubMed] [Google Scholar]
- 18.Hui S, Ghergurovich JM, Morscher RJ, Jang C, Teng X, Lu W, Esparza LA, Reya T, Le Z, Yanxiang Guo J, et al. Glucose feeds the TCA cycle via circulating lactate. Nature. 2017;551(7678):115–118. doi: 10.1038/nature24057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Leverve XM, Mustafa I. Lactate: a key metabolite in the intercellular metabolic interplay. Crit Care. 2002;6(4):284–285. doi: 10.1186/cc1509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Levy B, Mansart A, Montemont C, Gibot S, Mallie JP, Regnault V, Lecompte T, Lacolley P. Myocardial lactate deprivation is associated with decreased cardiovascular performance, decreased myocardial energetics, and early death in endotoxic shock. Intensive Care Med. 2007;33(3):495–502. doi: 10.1007/s00134-006-0523-9. [DOI] [PubMed] [Google Scholar]
- 21.Tappy L, Chiolero R. Substrate utilization in sepsis and multiple organ failure. Crit Care Med. 2007;35(9 Suppl):S531–S534. doi: 10.1097/01.CCM.0000278062.28122.A4. [DOI] [PubMed] [Google Scholar]
- 22.Correa TD, Pereira AJ, Brandt S, Vuda M, Djafarzadeh S, Takala J, Jakob SM. Time course of blood lactate levels, inflammation, and mitochondrial function in experimental sepsis. Crit Care. 2017;21(1):105. doi: 10.1186/s13054-017-1691-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Levraut J, Ciebiera JP, Chave S, Rabary O, Jambou P, Carles M, Grimaud D. Mild hyperlactatemia in stable septic patients is due to impaired lactate clearance rather than overproduction. Am J Respir Crit Care Med. 1998;157(4 Pt 1):1021–1026. doi: 10.1164/ajrccm.157.4.9705037. [DOI] [PubMed] [Google Scholar]
- 24.Levraut J, Ichai C, Petit I, Ciebiera JP, Perus O, Grimaud D. Low exogenous lactate clearance as an early predictor of mortality in normolactatemic critically ill septic patients. Crit Care Med. 2003;31(3):705–710. doi: 10.1097/01.CCM.0000045561.85810.45. [DOI] [PubMed] [Google Scholar]
- 25.Grip J, Jakobsson T, Hebert C, Klaude M, Sandstrom G, Wernerman J, Rooyackers O. Lactate kinetics and mitochondrial respiration in skeletal muscle of healthy humans under influence of adrenaline. Clin Sci. 2015;129(4):375–384. doi: 10.1042/CS20140448. [DOI] [PubMed] [Google Scholar]
- 26.Mori M, Smedberg M, Klaude M, Tjader I, Norberg A, Rooyackers O, Wernerman J. A tracer bolus method for investigating glutamine kinetics in humans. PLoS One. 2014;9(5):e96601. doi: 10.1371/journal.pone.0096601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gabrielsson J, Weiner D. Pharmacokinetic and pharmacodynamic data analysis: concepts and applications, fourth edition. Oxford: Taylor & Francis; 2007.
- 28.Kreisberg RA, Pennington LF, Boshell BR. Lactate turnover and gluconeogenesis in normal and obese humans. Effect of starvation. Diabetes. 1970;19(1):53–63. doi: 10.2337/diab.19.1.53. [DOI] [PubMed] [Google Scholar]
- 29.Revelly JP, Tappy L, Martinez A, Bollmann M, Cayeux MC, Berger MM, Chiolero RL. Lactate and glucose metabolism in severe sepsis and cardiogenic shock. Crit Care Med. 2005;33(10):2235–2240. doi: 10.1097/01.CCM.0000181525.99295.8F. [DOI] [PubMed] [Google Scholar]
- 30.van Hall G, Jensen-Urstad M, Rosdahl H, Holmberg HC, Saltin B, Calbet JAL. Leg and arm lactate and substrate kinetics during exercise. Am J Physiol Endocrinol Metab. 2003;284(1):E193–E205. doi: 10.1152/ajpendo.00273.2002. [DOI] [PubMed] [Google Scholar]
- 31.Norberg A, Gabrielsson J, Jones AW, Hahn RG. Within- and between-subject variations in pharmacokinetic parameters of ethanol by analysis of breath, venous blood and urine. Br J Clin Pharmacol. 2000;49(5):399–408. doi: 10.1046/j.1365-2125.2000.00194.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Avram MJ, Krejcie TC, Henthorn TK, Niemann CU. Beta-adrenergic blockade affects initial drug distribution due to decreased cardiac output and altered blood flow distribution. J Pharmacol Exp Ther. 2004;311(2):617–624. doi: 10.1124/jpet.104.070094. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1. Complete documentation of formulas used for mathematical modelling of data.
Additional file 2. Plasma lactate enrichment of labeled lactate for healthy volunteers and ICU patients
Additional file 3. Individual values for lactate concentrations in plasma for healthy volunteers and ICU patients during experiment.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.