

Abstract
Introduction:
Incidence of diabetes mellitus has increased over the past few years, mainly due to our eating habits and physical inactivity. This also includes the use of artificial sweetening agents which have broadly replaced other forms of sugars and have shown a paradoxical, negative effect on blood glucose. Ingestion of these artificial sweeteners (AS) results in the release of insulin from pancreas which is mistaken for glucose (due to their sweet taste). This increases the levels of insulin in blood eventually leading to decreased receptor activity due to insulin resistance.
Methodology:
It is a crosssectional study that was conducted on patients diagnosed with type-2 diabetes mellitus of a tertiary care hospital in Central India. All the diabetics that presented in the OPD were divided into 2 groups based on whether they use AS (group A) or not (group B). Insulin resistance was calculated for each group using HOMA-IR and graphs were plotted.
Results:
The HOMAIR values for Group A and B ranged from 0.9–24.33 and 0.12–10.83 with mean values 7.39 and 2.6, respectively, showing that the ones who used AS had a higher insulin resistance. The study also showed that the duration of use of artificial sweeteners had a direct impact on insulin resistance.
Keywords: Artificial sweeteners, diabetes mellitus, glucose metabolism, HOMA-IR, insulin resistance
Introduction
Diabetes mellitus is a long-term metabolic disorder that is characterized by high blood sugar, insulin resistance, and relative lack of insulin. Common symptoms include increased thirst, frequent urination, and unexplained weight loss. Insulin, a pancreatic hormone, helps glucose from food get into the cells to be used for energy.[1]
Diabetes mellitus type-2 is defined as a metabolic disorder that results in hyperglycemia (high blood glucose levels) due to the body:
Developing insulin resistance
Being unable to produce enough insulin.
The American Heart Association (AHA) and American Diabetes Association (ADA) have given a cautious nod to the use of artificial sweeteners in place of sugar to combat obesity, metabolic syndrome, and diabetes, all risk factors for heart disease.
”While they are not magic bullets, smart use of non-nutritive sweeteners could help you reduce added sugars in your diet, therefore lowering the number of calories you eat. Reducing calories could help you attain and maintain a healthy body weight, and thereby lower your risk of heart disease and diabetes,” said Dr. Christopher Gardner, an associate professor of medicine at Stanford University in California, in a press release accompanying the scientific statement.[2,3]
Over a past few decades, diabetes mellitus has become the most common endocrine disorder and the most important comorbidity in the world. Its main cause is believed to be the development of resistance to insulin by the body. An important factor nowadays thought to be involved is faulty or inappropriate food habits—junk food, high-fat and high-carbohydrate diet with low fiber content.[4]
According to some studies, the prime reason for development of diabetes mellitus is believed to be artificial sweeteners. In one study, people were given either sucralose or water and then subjected to glucose tolerance test. Those given sucralose had higher blood insulin levels.[5,6] Another study compared a dose-dependent relationship between artificially sweetened soft drinks and risk of type-2 diabetes mellitus.[7]
This study aims to correlate insulin resistance with consumption of artificial sweeteners.
Aims and Objectives
This study is designed to find any correlation between ingestion of artificial sweetening agents and their effect on insulin resistance. The blood glucose and serum insulin levels of the patients were recorded and insulin resistance was calculated using the HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) calculator and scale, developed by Matthew et al.[8]
Methodology
Study Type:
It is a cross-sectional observational study.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| 1) Patients who have given a written consent. | 1) Patients suffering from any other endocrinological illness. |
| 2) Patients diagnosed with type-2 DM. | 2) Patients suffering from gestational diabetes mellitus |
| 3) Patients consuming artificial sweetening agents. | 3) Patients with type-2 DM, receiving insulin therapy. |
Study Design:
The study will be conducted on patients diagnosed with type-2 diabetes mellitus of a tertiary care hospital in Central India.
Sample Size:
Patients with type-2 diabetes mellitus irrespective of their age and gender, presenting in the hospital OPD will be a part of this study.
After a written consent has been achieved, the sample will be divided into two groups:
Group A - The patients who regularly consume artificial sweetening agents
Group B - The patients who do not consume artificial sweeteners in any form.
Patients from both the groups will be tested for fasting blood sugar levels and serum insulin, individually. Insulin resistance will be calculated by applying the values of both the parameters in the HOMA-IR calculator.
The information will be kept confidential and under quality control.
HOMA-IR provides us with the scales of insulin resistance using a basic mathematical algorithm, given as:[7]
Substituting the values for serum insulin and FBS in the above formula, insulin resistance can be easily calculated.
To assess insulin resistance, HOMA-IR also provides a scale or classification as:[7]
| Normal Insulin Resistance | Less than 3 |
| Moderate Insulin Resistance | 3-5 |
| Severe Insulin Resistance | Above 5 |
For an individual with no history of type-2 diabetes mellitus, the HOMA-IR reading should fall below 3.
For example, for a person with FSL of 100 (Normal = 70-110 mg/dl) and serum insulin of 10 (normal = 5-20 mU/L), the HOMA-IR reading will be = 2.46 (below 3) which is normal.
Moreover, if a patient currently is under the “Moderate” class, the patient has the probability to develop type-2 diabetes mellitus in future.
The data from groups A and B were compared for analysis of insulin resistance.
Observations and Result
Volunteers from both the groups were well informed and after obtaining their consent, blood was drawn and tested for fasting serum insulin levels and fasting serum glucose levels which were recorded.
Using the above data, the volunteers had their HOMA-IR value calculated and individually noted and charted as follows:
Group A:
The HOMA-IR values for Group A and B ranged from 0.9–24.33 and 0.12–10.83 with mean values 7.39 and 2.6, respectively [Figures 1 and 2]. Both the charts were matched, checked with the data, and the findings were noted.
Figure 1.
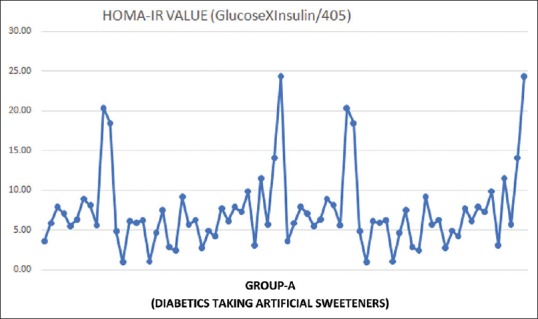
Graphical representation of patients receiving artificial sweeteners
Figure 2.
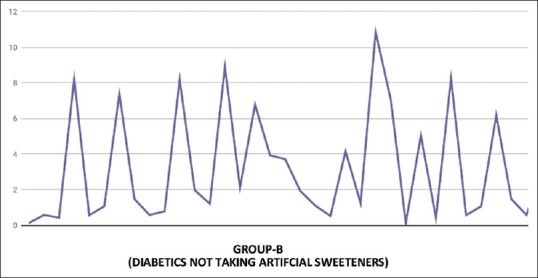
Graphical representation of patients not taking artificial sweeteners
Discussion
A similar study carried out by de Koning et al. in 2011 compared the development of diabetes mellitus type-2 with the consumption of artificially sweetened beverages and sugar-sweetened beverages (SSB) [Figure 3].[9] Increased intake of artificial sweetened beverages increased the incidence of type-2 diabetes, suggesting possible mechanism of insulin resistance over time.
Figure 3.
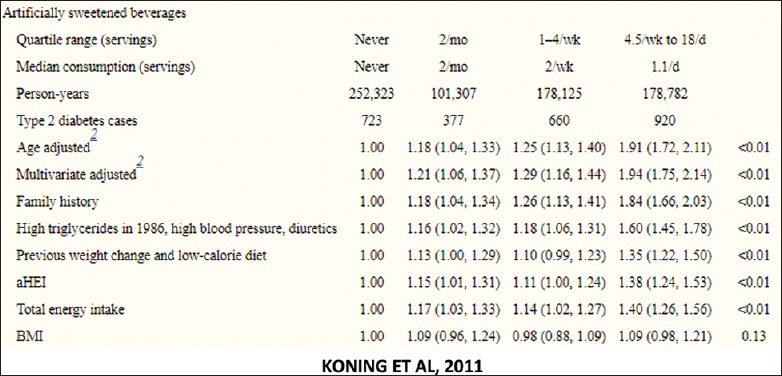
Study published by Koning et al. In 2011
Another study carried out in 2016 by Löfvenborg JE et al.[10] showed a positive correlation between sugar-sweetened beverages and development of LADA.
Recent studies have shown that sucrose or sucralose increase the T1R2 and T1R3 taste receptors that in turn stimulated the intestine and circulating levels of GIP and GLP-1 leading to hyperinsulinemia.[11]
Conclusion
Group A patients who consumed artificial sweetening agents had higher insulin resistance as compared to group B patients who had no artificial sweeteners based on HOMA-IR. However, further studies are required to conclude a direct correlation of artificial sweeteners with decreased insulin sensitivity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Barnett AH. Type 2 Diabetes. 2nd ed. Oxford University Press; 2012. p. 162. [Google Scholar]
- 2.Mehnert H. Health and Sugar Substitutes ERGOB Conference on Sugar Substitutes, Geneva, October/November 1978: Proceedings Basel, Karger, 1979. :262–5. [Google Scholar]
- 3.Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. 2004;27:1487–95. doi: 10.2337/diacare.27.6.1487. [DOI] [PubMed] [Google Scholar]
- 4.Sylvetsky AC, Welsh JA, Brown RJ, Vos MB. Low-calorie sweetener consumption is increasing in the United States. Am J Clin Nutr. 2012;96:640–6. doi: 10.3945/ajcn.112.034751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pepino MY, Yanina Pepino M, Tiemann CD, Patterson BW, Wice BM, Klein S. Sucralose affects glycemic and hormonal responses to an oral glucose load. Diabetes Care. 2013;36:2530–5. doi: 10.2337/dc12-2221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Romo-Romo A, Aguilar-Salinas CA, Brito-Córdova GX, Gómez-Díaz RA, Almeda-Valdes P. Sucralose decreases insulin sensitivity in healthy subjects: A randomized controlled trial. Am J Clin Nutr. 2018;108:485–91. doi: 10.1093/ajcn/nqy152. [DOI] [PubMed] [Google Scholar]
- 7.Greenwood D, Threapleton D, Evans C, Cleghorn C, Nykjaer C, Woodhead C, et al. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose–response meta-analysis of prospective studies. Br J Nutr. 2014;112:725–34. doi: 10.1017/S0007114514001329. [DOI] [PubMed] [Google Scholar]
- 8.Matthew DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412–9. doi: 10.1007/BF00280883. [DOI] [PubMed] [Google Scholar]
- 9.de Koning L, Malik VS, Rimm EB, Willett WC, Hu FB. Sugar-sweetened and artificially sweetened beverage consumption and risk of type 2 diabetes in men. Am J Clin Nutr. 2011;93:1321–7. doi: 10.3945/ajcn.110.007922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Löfvenborg JE, Andersson T, Carlsson PO, Dorkhan M, Groop L, Martinell M, et al. Sweetened beverage intake and risk of latent autoimmune diabetes in adults (LADA) and type 2 diabetes. Eur J Endocrinol. 2016;175:605–14. doi: 10.1530/EJE-16-0376. [DOI] [PubMed] [Google Scholar]
- 11.Sánchez-Tapia M, Martínez-Medina J, Tovar AR, Torres N. Natural and artificial sweeteners and high fat diet modify differential taste receptors, insulin, and TLR4-mediated inflammatory pathways in adipose tissues of rats. Nutrients. 2019;11:880. doi: 10.3390/nu11040880. [DOI] [PMC free article] [PubMed] [Google Scholar]