

Abstract
Background:
The Health and Family Welfare Department of Gujarat implemented a mHealth Programme called TeCHO+ (Technology for Community Health Operations) in 2018. TeCHO+ is aimed at making progress across all dimensions of the comprehensive primary healthcare services.
Objective:
The objective of this study is to record the document rollout and early implementation experience of TeCHO+ programme in Gujarat.
Methods:
The present participatory process documentation exercise was undertaken in Gujarat. The various steps for process documentation were decided after participation in multiple task force meetings and state/district- and taluka-level action seminars and reviewing the TeCHO+ programme data and progress reports. The perceptions of the health officials and field staff were gathered using key informant interviews from five districts of Gujarat: Bharuch, Narmada, Gandhinagar, Mahisagar, and The Dangs. In addition, stakeholders involved with TeCHO+ Programme were interviewed to understand the process of rollout, implementation challenges, and success.
Results:
In the initial phase, the TeCHO+ application focussed only on updating the Family Health Survey to improve the quality of data captured in the system. FHWs log-in the mobile application daily to access their daily work plan for which SMS alerts were are also generated. Most FHWs were in their 50s and were first-time smartphone users. Although, they were enthusiastic and open to the new technology, initially they faced certain difficulties in operating the application. The programme had a strong troubleshooting mechanism in terms of the use of WhatsApp group, helpline numbers, and voice calls in addition to supportive supervision.
Discussion:
TeCHO+ showed the potential to enhance the quality of the collected data and also service coverage. However, poor technology literacy of old FHWs, the launch of multiple programme memes at the same time, and target-driven task assignments pose major challenges.
Keywords: Gujarat, mHealth intervention, process documentation, TeCHO+ programme
Introduction
India has the highest burden of maternal, newborn, and child mortality and undernutrition.[1] Although there are proven community-based services available to improve mortality, undernutrition, and noncommunicable conditions, the challenge is to implement them with highest possible coverage and quality.[2,3,4] The state government of Gujarat has considered name-based tracking of individual beneficiaries to ensure the provision of due services through a web-based mother and child tracking system–known as e-Mamta.[5] The e-Mamta web-based portal tracks individual mother and child health services and their data is input by a data entry operator at the PHC level. However, this tracking system witnesses gaps. Although the frontline health workers such as female health workers (FHW) and Accredited Social Health Activists (ASHA) provide due services to eligible beneficiaries in the community, data of these services is entered in the e-Mamta portal by a data entry operator at the primary health care (PHC) centres, thereby creating a unavoidable gap between the time of service delivery and time of data entry. These factors have raised concerns over the quality of the existing data in the e-Mamta system,[6,7] such as duplications, lack of data linked with services, and filling the 93 data columns in manual register, thereby over-burdening the frontline workers and data entry operators.
In 2013, in partnership with the Health and Family Welfare Department, Gujarat, a voluntary organization tested the mHealth project–Innovative Mobile Phone Technology for Community Health Operation (ImTeCHO) in selected tribal and rural communities of Gujarat. ImTeCHO application was developed as a job-aid for staffs of PHCs and ASHA to increase coverage of maternal, neonatal, and child health (MNCH) care.[8] The trial findings showed statistically significant and meaningful improvement in the coverage of key MNCH services by ASHA.[7,8] The mHealth clinical decision support system applications are being increasingly relied upon in resource-limited settings of low- and middle-income countries mainly for efficient delivery of MNCH care.[9,10,11]
TeCHO+ Programme in Gujarat
Based on the findings from the ImTeCHO trial, the Health and Family Welfare Department scaled-up ImTeCHO as TeCHO+ (Technology for Community Health Operation) by covering 11 priority health areas across the state. The priority health areas included (1) maternal mortality, (2) infant mortality, (3) low-birth weight babies, (4) immunization, (5) maternal, child, and adolescent nutrition, (6) anemia in pregnancy, (7) epidemics, (8) communicable disease, (9) mental health, (10) family planning, spacing methods, and sex ratio at birth, and (11) noncommunicable diseases (NCDs).
TeCHO+ is a mobile (android-based) and web-based application that provides name-based tracking of beneficiaries using mobile phones along with Aadhar authentication. Data entry in TeCHO+ is done at the point of service by the FHW to enable more accurate and real-time data entry. The programme is implemented in partnership with a voluntary organization that has substantial experience in implementing the mHealth intervention with a predominantly tribal population of Gujarat, a Gandhinagar-based software service company, and an Emergency Management Institute in Gujarat. TeCHO+ Programme aims to enhance the quality of primary care through real-time data entry and improve service delivery by generating alerts for high-risk cases, supportive supervision, and report automation at multiple levels.
Features of the TeCHO+ Programme
TeCHO+ has features such as providing daily work-plan which capacitates the community-based health workers in tracking the beneficiaries for primary healthcare services. It also stratifies the beneficiaries based on the risk and generates alerts for high-risk cases thus enabling the health workers for timely and appropriate service delivery. Thus, this programme assists the health workers in providing efficient delivery of primary care services. Figure 1 provides a glimpse of TeCHO+ application features.
Figure 1.

Key features of TeCHO+ mobile application
This study was conducted with the purpose of documenting the rollout of the TeCHO+ programme in Gujarat and retrospectively assesses the early implementation experience between April 2018 and February 2019.
Material and Methods
The various steps identified for process documentation were decided after reviewing the TeCHO+ programme data and progress reports and participation in multiple task force meetings and state/district and taluka-level action seminars. A Key Informant Interview was used to gather the responses of the health officials and field-level staffs responsible for implementing TeCHO+ programme in five districts of Gujarat: Bharuch, Narmada, Gandhinagar, Mahisagar, and The Dangs. In addition, stakeholders involved with the programme including officials from technical partners were also interviewed to understand the process of rollout, implementation challenges, and success. The interview guide had questions on logistics required for the rollout of the programme, software development, and issues faced in using the same, troubleshooting, and the roles and responsibilities of human resource hired for TeCHO+. We interviewed the TeCHO+ programme officials—District TeCHO+ Coordinators (DTCs) of the selected districts and Taluka TeCHO+ Co-ordinators (TTCs) of two talukas of each selected district. In addition, selected ANMs from each taluka were interviewed to know the issues and challenges faced by them during service delivery. Ethic approval has been received from Institutional Ethics Committee on date 19-03-2019 and the study focused on documentation of early implementation experience retrospectively from April 2018 to February 2019.
Enrolment of the study participants was voluntary and they could withdraw at any time. Written informed consent was obtained from all the participants after the study objectives, research methods, and data collection techniques were explained to and understood by them.
Results
The State government has rolled out reproductive and child health (RCH) module. Currently, the NCD and Nutrition module (from January 2019 onwards) is piloted in selected districts of the state for which the referral mechanism of positively identified cases of NCDs and malnutrition is also set up by the State.
Programme Structure of TeCHO+
TeCHO+ programme has a structure to facilitate effective implementation. At the state level, a TeCHO+ task force has been formed to review and facilitate prompt decision-making to aid uninterrupted implementation. At the district-level, the chief district health officer (CDHO) and reproductive and child health officers (RCHO) look after the overall coordination and supportive supervision. Recently, a new cadre of territory TeCHO+ coordinators, 1 per 75 FHWs (roughly FHWs of two-three blocks), have been deployed by the Emergency Management Institute to monitor the login rate of the FHWs, troubleshooting, and escalating software-related issues to the software development partner as well as the taluka and district TeCHO coordinators. Figure 2 shows the role of human resource towards streamlining the implementation of TeCHO+. Over and above the dedicated cadre of health workers for TeCHO+ programme, PHC-MOs have been assigned the task to verify the families in case of death of a family member or immigration or emigration of a family or a particular member of the family. Only after the verification, the changes made by the FHW were accepted.
Figure 2.
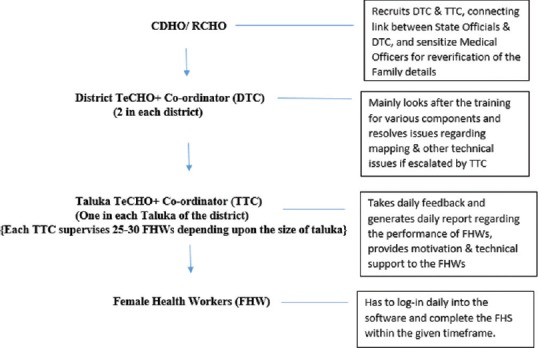
Roles of human resource for implementation of TeCHO+ programme
The programme has robust supervision, monitoring, and support mechanism at each level. At the state level, the State TeCHO+ team includes an allopathic medical officer, state data manager, IT technician, programme officer and programme assistant (both deputed from the e-Mamta division). The state data manager and medical officer are primarily responsible for supervising and monitoring TeCHO+ and the supporting software service company is responsible for the development of the software. Although coordinators are deputed for technical support at the district and taluka levels, the CDHOs and RCHOs are entrusted with the critical role of training, supervising, and monitoring the programme. The programme has utilized SATCOM (Satellite communication facilitated by Bhaskaracharya Institute for Space Applications and Geo-Informatics – BISAG, Gandhinagar) as a medium for imparting continuous capacity strengthening of the programme staff.
Role of key stakeholders
The TeCHO+ programme has three major stakeholders—a voluntary organization with experience of mhealth programme in a tribal belt of Gujarat, a software support partner, and an Emergency Management agency.
The TeCHO+ application was developed free of cost by a local software firm for perpetual use by the Health and Family Welfare Department. It was developed in a phased manner. In the initial phase, a mobile application was developed for updating the Family Health Survey (FHS). This application was enabled to fetch FHS data from e-Mamta which was verified by FHWs for incorporating in the RCH module of TeCHO+ application.
The FHW were capacitated through standardized training by the voluntary organization. Standard training videos were developed to ensure uniformity of training pedagogy and reduce communication barriers.
The emergency management agency has a crucial role in providing the necessary support on the field to health workers through the helpline. The entire field force of territory TeCHO+ coordinators was recruited through the emergency management agency. The agency also validated 3% of the data collected by the FHWs. If errors were found, respective health workers were informed to correct the family details immediately.
Early implementation experience
In the initial phase, the TeCHO+ application was focussed only for updating the Family Health Survey details. This was done to improve the quality of data captured in the system. Training was delivered using a cascade model wherein district and taluka TeCHO+ coordinators were trained as master trainers who subsequently trained FHWs in respective districts and taluka. The training primarily included components like TeCHO+ programme, use of mobile and web-interface, referral mechanism, and the roles and responsibilities of each team member.
The programme has facilitated 1,869 training sessions. During the first phase, a total 10,674 FHWs were trained and 10,688 FHWs were trained in the second phase. In the third phase, the rollout of NCD was piloted in five districts. In this phase, 288 FHWs and 1207 ASHAs were trained. In addition to FHWs and ASHAs, health officials from taluka to state level were also oriented on the TeCHO+ programme. These include data entry operators to facility managers including CDHOs, PHC-MO, RCHOs, DPCs, and allied staffs. To assess the quality of the comprehensive training, the FHWs and ASHAs were assessed for the knowledge they gained during the training through telephonic audits. The passing rates for the participating FHWs were 96% and 90% for training related to FHS and RCH module, respectively, and that for FHWs and ASHAs together was 90% for the nutrition module.
Milestones of TeCHO+ programme
The TeCHO+ Programme implementation was planned in phases: (1) zero phase in which the programme was conceptualized and received buy-in from all stakeholders; (2) the first phase included updating of Family Health Survey information in TeCHO+ application; (3) second phase primarily catered towards adding Reproductive and Child Health components in TeCHO+, and (4) the third phase comprise of adding remaining components in TeCHO+. Figure 3 provides a glimpse of the milestones of the TeCHO+ programme.
Figure 3.

Milestones of TeCHO+ programme
Routine tasks of female health workers (FHWs)
FHWs log-in the mobile application daily and receive their daily work plan which helps them schedule household visits. During the household visit, the patients' details are recorded in the application and the triaging mechanism in the software identify high-risk cases. The application automatically displays the videos for health promotion according to the risk assessment. This ensures providing standardized messages to the end users. In case of failure to make a visit, the system generates alert to the FHW. Also, the respective PHC-MO gets an alert in case of identification of high-risk cases and can also supervise the work carried out by the FHWs of their PHCs.
Piloting NCD and nutrition modules
During January 2019, a pilot of NCD module was launched in five districts of the state viz. Gandhinagar, Narmada, Porbandar, Dahod, and Mehsana. In this module, ASHA workers were trained and equipped with a mobile phone. Their role includes surveying all family members aged more than 30 years to assess the presence of NCDs or their risk to develop the disease mainly diabetes mellitus, hypertension, oral cancer, cervical cancer (in women), and breast cancer (in women). High-risk cases to be referred to ANM for the next level of screening. Positive cases were further referred to the respective PHCs. Parallel to this, the nutrition module was also piloted in one district, i.e., Gandhinagar. The mechanism of referral of identified moderately acute and severely acute malnourished children requiring facility-based treatment was planned in such a way that the alert is generated on the dashboard of Rashtriya Bal Swasthya Karyakram (RBSK) coordinator and the respective Child Malnutrition Treatment Centre (CMTC) or Nutrition Rehabilitation Centre (NRC). On admission of such a child, services are provided to them and on their discharge, the ANM and ASHA get notification and reminder for their follow-up at an interval of 15 days until they complete three visits.
Problem addressal mechanism
The programme has strong troubleshooting mechanisms in terms of the use of WhatsApp group, helpline, and supervisors. A WhatsApp group of FHWs and taluka and district TeCHO+ coordinators was created for continuously communicating field-level operational problems and solutions. Urgent issues were sorted out using voice calls. In addition to this mechanism, FHWs were also provided with the Helpline number (operated by the Emergency Management Institute) for any field-level problems. Flexible and prompt solution-focused decisions from the state programme team prevented hindrances in implementation. Furthermore, the programme has decentralized actions at the district level to address field-level challenges locally.
Change management
Successful scale-up of the health programme requires effective change management without reducing the quality of service delivery as well as the data.[7] mHealth solutions are not merely “add-ons” to existing service delivery and ways of working, but for managing and adapting the “change” effectively. The TeCHO+ programme was prepared for change management. The programme has imbibed hierarchical bureaucracy[8] and collaborative breakthrough method[12] to implement a new better way of working, to comply with new standards, and encourage FHWs to adopt new technology and workstyle. The government has formed a task force to ensure collective planning, coordinated implementation and periodic review of the TeCHO+ programme.
Procurement and management of mobile handsets
The mobile phones that support TeCHO+ application, VLC media player (to show videos to the beneficiaries), and basic camera (to capture field photos) were procured. All the districts have been given at least 5% buffer stock of mobile phones as a replacement to faulty or lost phones. A buffer stock of mobile phones were made available at the level of talukas that were situated away from the district headquarters or in case of larger districts. Mobile handsets were replaced immediately in case of any mishaps to help them carry their daily work. In case of loss of mobile handset or the damage due to carelessness, recovery amount equal to the cost of the handset is charged in the first year whereas year-wise depreciation is considered from the second year.
Implementation challenges
The state-wide rollout of TeCHO+ programme was accompanied by various challenges. Engaging the cadre of FHWs and training them, fast scaling-up, sequencing the technical human resource for monitoring the progress were the key challenges. The programme was approved and started in the middle of the financial year 2017–2018. Due to mid-year approval, the budget was not allocated for the TeCHO+ programme. This constraint prevented timely procurement of needed quantities of mobile phone and staff recruitment. This had repercussions in terms of delay in training FHWs and commencing Family Health Survey across the state. Most FHWs were in their 50s and were first-time smartphone users. They were enthusiastic and readily accepted the new technology but reported to face difficulties in operating the application.
The time gap between RCH pilot and implementation at the state level was also very short which constrained the software developers to take corrective actions for the issues raised during the pilot of the RCH module. This ultimately has made the system vulnerable for many field-level issues which would not have been the case if the pilot had been given enough time.
Successful scale-up requires equitable access to a skilled and motivated health worker within a performing health system.[13] The government mobilized existing human resource for the programme. The Ayush medical officers were assigned responsibilities as district and taluka TeCHO+ coordinators. However, in PHCs wherein medical officer positions were vacant, Ayush medical officers were given the additional charge of PHC-MO. As a result, they were not able to spare time for the supervision of the TeCHO+ programme which resulted in a lack of coordination between FHWs and TTCs.
Discussion
Mobile health (mHealth) has the ability to transform the delivery of health services and bring about a paradigm shift in healthcare delivery processes.[14] Improvements in technological innovations can also help improve healthcare services.[15] The TeCHO+ programme has many strengths like innovative use of technology for knowledge management, prompt referral, and supportive supervision; active participation of stakeholders, proactive programme as well as field staff. The regular feedback taken by the state officials from various cadres of health workers and stakeholders enabled the government to take timely corrective actions to improve the TeCHO+ application and implement the TeCHO+ programme. This importance to communication within and between stakeholders and decision-making enabled effective implementation of the programme.
However, implementation of mHealth solutions does not occur smoothly, and many impending challenges reduced the effectiveness of health service delivery. The barriers include resistance to change in general and lack of end-user education.[16] The TeCHO+ programme implementation encountered several challenges. The delay in commencing TeCHO+ implementation left the field workers with limited time for FHS. In addition, the time gap between FHS and RCH module was very short. Further, the age of FHWs and limited practice during the training are the reasons for the errors made by FHWs and their inability to acclimatize with the programme as expected. Also, they were asked to maintain the register in addition to data entry in the TeCHO+ application which predisposed them to perform more work than usual which could have impacted the data quality. The government provided additional responsibilities to existing staff, which constrained the implementation. This approach may prevent motivated staff from contributing to the success of the programme.
mHealth interventions have thrived across the globe, but few have reached scale-up and shown public health impact.[16,17] The scale-up of the mHealth pilots is a difficult, context-specific process that is significantly influenced by organizational culture, continuous technological upgradations as per users' perspective, and supportive supervision and responsive health system. Although TeCHO+ faced implementation challenges, the special features of TeCHO+ programme such as well-planned schedule of FHWs visits, real-time data entry of the services, risk-stratification, vigilant tracking, management of high-risk cases, prompt and effective supportive supervision and monitoring systems demonstrate TeCHO+ as a potentially successful scale-up which has the fair prospect of showing public health impact upon incorporation of the lessons learnt from the rollout phase of the programme.
Financial support and sponsorship
This study was made possible through a Health Technology Assessment Regional Resource Centre at the Indian Institute of Public Health Gandhinagar, Gujarat supported by the Department of Health Research, Government of India.
Conflict of Interest
There is no conflict of interest.
Acknowledgements
Three major stakeholders of the programme include: Argusoft India Ltd., responsible for software development and maintenance, SEWA Rural technical partner for capacity building and supporting state-level team for roll out, and UNICEF provided technical support at state-level and GVK EMRI for managing a helpline, first-level troubleshooting, and service validation.
References
- 1.Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, et al. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet. 2008;371:243–60. doi: 10.1016/S0140-6736(07)61690-0. [DOI] [PubMed] [Google Scholar]
- 2.India: Reducing Undernutrition through Community-Based Interventions | Innovations, lessons learned and good practices | UNICEF [Internet] [Last cited on 2019 Aug 07]. Available from: https://www.unicef.org/innovations/index_49150.html .
- 3.Nimmagadda S, Gopalakrishnan L, Avula R, Dhar D, Diamond-Smith N, Fernald L, et al. Effects of an mHealth intervention for community health workers on maternal and child nutrition and health service delivery in India: Protocol for quasi-experimental mixed-methods evaluation. BMJ Open. 2019;9:e025774. doi: 10.1136/bmjopen-2018-025774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lutz B, Coleman S, Bushnell C, Duncan P, Gesell S. Challenges and Strategies for Implementing Interventions in a Statewide System-Based Pragmatic Trial (P5015) Neurology. 2018;90(15 Supplement) [Google Scholar]
- 5.NHM Gujarat. E-Mamta initiatives. [Last cited on 2019 Apr 04]. Available from: https://nhm.gujarat.gov.in/e-Mamta1.htm .
- 6.Nagarajan P, Tripathy J, Goel S. Is a mother and child tracking system (MCTS) on the right track? Experience from a northern state of India. Indian J Public Health. 2016;60:34–9. doi: 10.4103/0019-557X.177298. [DOI] [PubMed] [Google Scholar]
- 7.Gera R, Muthusamy N, Bahulekar A, Sharma A, Singh P, Sekhar A, et al. An in-depth assessment of India's Mother and Child Tracking System (MCTS) in Rajasthan and Uttar Pradesh. BMC Health Serv Res. 2015;15:315. doi: 10.1186/s12913-015-0920-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Modi D, Desai S, Dave K, Shah S, Desai G, Dholakia N, et al. Cluster randomized trial of a mHealth intervention “ImTeCHO” to improve delivery of proven maternal, neonatal, and child care interventions through community-based Accredited Social Health Activists (ASHAs) by enhancing their motivation and strengthening. Trials. 2017;18:270. doi: 10.1186/s13063-017-1998-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Amoakoh HB, Klipstein-Grobusch K, Agyepong IA, Zuithoff NPA, Amoakoh-Coleman M, Kayode GA, et al. The effect of an mHealth clinical decision-making support system on neonatal mortality in a low resource setting: A cluster-randomized controlled trial. EClinicalMedicine. 2019;12:31–42. doi: 10.1016/j.eclinm.2019.05.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Amoakoh HB, Klipstein-Grobusch K, Ansah EK, Grobbee DE, Yveoo L, Agyepong I. How and why front-line health workers (did not) use a multifaceted mHealth intervention to support maternal and neonatal healthcare decision-making in Ghana. BMJ Glob Health. 2019;4:e001153. doi: 10.1136/bmjgh-2018-001153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shiferaw S, Workneh A, Yirgu R, Dinant GJ, Spigt M. Designing mHealth for maternity services in primary health facilities in a low-income setting-lessons from a partially successful implementation. BMC Med Inform Decis Mak. 2018;18:96. doi: 10.1186/s12911-018-0704-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Yamey G. What are the barriers to scaling up health interventions in low and middle income countries? A qualitative study of academic leaders in implementation science. Global Health. 2012;8:11. doi: 10.1186/1744-8603-8-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lassi ZS, Musavi NB, Maliqi B, Mansoor N, de Francisco A, Toure K, et al. Systematic review on human resources for health interventions to improve maternal health outcomes: Evidence from low-and middle-income countries. Hum Resour Health. 2016;14:10. doi: 10.1186/s12960-016-0106-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.World Health Organization. mHealth: New horizons for health through mobile technologies. [Last cited on 2019 Aug 07]. Available from: http://wwwwhoint/goe/publications/goe_mhealth_webpdf .
- 15.Malvey D, Slovensky DJ. mHealth: Transforming Healthcare. New York, NY: Springer; 2014. [Google Scholar]
- 16.Gurupur VP, Wan TTH. Challenges in implementing mHealth interventions: A technical perspective. Mhealth. 2017;3:32. doi: 10.21037/mhealth.2017.07.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bardosh KL, Murray M, Khaemba AM, Smillie K, Lester R. Operationalizing mHealth to improve patient care: A qualitative implementation science evaluation of the WelTel texting intervention in Canada and Kenya. Global Health. 2017;13:87. doi: 10.1186/s12992-017-0311-z. [DOI] [PMC free article] [PubMed] [Google Scholar]