

ABSTRACT
Background:
Bicuspid aortic valve (BAV) disease is considered the most common congenital heart disease and the main etiology of aortic valve stenosis (AS) in young adults. Although transcatheter aortic valve replacement (TAVR) is routinely used in high- and intermediate-risk patients with AS, BAV patients with AS were excluded from all pivotal trials that led to TAVR approval. We sought, therefore, to examine in-hospital outcomes of patients with BAV who underwent TAVR in comparison with surgical aortic valve replacement (SAVR).
Methods:
Using the National Inpatient Sample from 2011 to 2014, we identified patients with BAV with International Classification of Diseases-Ninth Revision-CM code 746.4. Patients who underwent TAVR were identified using ICD-9 codes 35.05 and 35.06 and those who underwent SAVR were identified using codes 35.21 and 35.22 during the same period.
Results:
A total of 37,052 patients were found to have BAV stenosis. Among them, 36,629 patients (98.8%) underwent SAVR, whereas 423 patients (1.14%) underwent TAVR. One-third of enrolled patients were female, and the majority of the patients were White with a mean age of 65.9 ± 15.1 years. TAVR use for BAV stenosis significantly increased from 0.39% in 2011 to 4.16% in 2014 (P < 0.001), which represents a 3.77% overall growth in procedure rate. The median length of stay decreased significantly throughout the study period (mean 12.2 ± 8.2 days to 7.1 ± 5.9 days, P < 0.001). There was no statistically significant difference between SAVR and TAVR groups in the in-hospital mortality (0% vs. 5.9%; adjusted P = 0.119).
Conclusion:
There is a steady increase in TAVR use for BAV stenosis patients along with a significant decrease in length of stay.
Key words: Bicuspid aortic valve stenosis, surgical aortic valve replacement, transcatheter aortic valve replacement
INTRODUCTION
Bicuspid aortic valve (BAV) disease is considered the most common congenital heart disease and the most common cause of aortic valve stenosis (AS) in young adults. Up to 50% of patients with BAV require aortic valve replacement in their lifetime.[1] This is because of the flow hemodynamics of the aortic valve which expedites the degeneration of the valve leaflets prematurely. The current guidelines recommend routine echocardiogram follow-up of patients with BAV to evaluate the valve hemodynamics, severity of the valve stenosis, and the left ventricular function.
Although transcatheter aortic valve replacement (TAVR) has been used routinely in high- and extreme-risk AS patients, BAV patients with AS were excluded from many pivotal trials that led to approval of TAVR in the United States.[2,3,4,5] This is mainly due to the concomitant aortopathy, which requires aortic root repair with a potential increased risk of aortic dissection and numerous technical challenges related to bicuspid anatomy.[6,7,8] Therefore, the treatment of choice for symptomatic bicuspid stenosis has been surgical aortic valve replacement (SAVR).[9]
With the advances in device technology, and with the accumulated experience, there has been an increased off-label use of TAVR for bicuspid stenosis in the absence of aortopathy.[10] Majority of the evidence for safety and feasibility of TAVR in patients with BAV is based on registry data and single-center experiences. There are limited data regarding the use and outcome of TAVR in BAV stenosis in the United States. We sought, therefore, to assess the trend of TAVR use in patients with BAV stenosis over the past few years and examine the subsequent in-hospital and procedural outcomes.
MATERIALS AND METHODS
Data were obtained from the Agency for Healthcare and Research, and Quality Healthcare Cost and Utilization Project National Inpatient Sample (NIS) files from January 1, 2011 through December 31, 2014. The NIS is the largest, publicly available, all-payer administrative claims database in the United States. It contains de-identified patient and clinical data from approximately 1,000 nonfederal hospitals in 45 states, including approximately 5–8 million discharges annually.[11]
We identified patients with BAV with International Classification of Diseases-Ninth Revision-CM (ICD-9) code 746.4. Patients undergoing TAVR were identified using ICD-9 codes 35.05 and 35.06. We also obtained the data of those who underwent SAVR were identified using ICD-9 codes 35.21 and 35.22 during the same period. To maintain a homogenous study population and to limit confounding, those with concomitant aortic valve disease were excluded from the analysis in addition to patients undergoing concomitant procedures. Procedure-related complications were identified using appropriate ICD-9-CM codes in any secondary diagnosis field. All measures for comorbidities, except coronary artery disease and anticoagulation history, were created from definitions in the Elixhauser Co-morbidity Index, which assigns variables that identify comorbidities in hospital discharge records using the diagnosis coding of ICD-9-CM.[12]
Major complications were recorded using established Valve Academic Research Consortium (VARC II) definitions for death, major bleeding, myocardial infarction, stroke, vascular complications, valve-related dysfunction, and acute kidney injury.[13] Hospital length of stay (LOS) was defined as the number of days from the date of the procedure to the date of being discharged home or to a rehabilitation facility.
A value of P < 0.05 was considered statistically significant. We used the Statistical Package for the Social Sciences software version 25.0 software (IBM, Armonk, NY) for all statistical analyses.
To account for potential confounding factors and reduce the effect of selection bias, a propensity-score-matching model was developed to derive two matched groups for comparative outcomes analysis. Propensity score was calculated using multivariable logistic regression models derived from hospital level, clinical, and demographic covariates, including the Elixhauser comorbidities. For calculation of the propensity score, the dependent variable was the TAVR vs. SAVR procedure use. We performed matching on the propensity score implementing a greedy algorithm to construct a balanced match of TAVR cases to SAVR cases in a 1:1 ratio using a caliper of 0.1. As we used publicly accessible, de-identified administrative level aggregate data, rather than patient-specific data, approval from the institutional review board was not required to conduct the study.
RESULTS
A total of 37,052 patients were found to have BAV stenosis. Among them, 36,629 patients (98.8%) underwent SAVR, whereas 423 patients (1.14%) underwent TAVR between January 1, 2011, and December 31, 2014. Compared with SAVR counterparts, patients with BAV who underwent TAVR were older (65.9 years ± 15.1 vs. 56.7 years ± 14.7), had more Caucasian women (34.3% vs. 26.3%), but had more co-morbidities, particularly CAD, hyperlipidemia, prior stroke, and complicated diabetes [Table 1]. The vast majority of TAVR procedures were performed in large teaching hospitals. Baseline differences existed between the groups after the propensity-adjusted analysis [Table 2].
Table 1:
Baseline characteristics and comorbidities in bicuspid aortic valve stenosis patients who underwent either surgical or transcatheter aortic valve replacement
| Variable | SAVR (N = 36,629) | TAVR (N = 423) | P value |
|---|---|---|---|
| Age | 56.7 ± 14.7 | 65.9 ± 15.1 | <0.001 |
| Sex | |||
| Female | 26.3 | 34.3 | <0.001 |
| Race | 0.027 | ||
| White | 85.3 | 89.2 | |
| Black | 2.1 | 2.4 | |
| Hispanic | 5.9 | 4.8 | |
| Asian or Pacific Islander | 1.4 | 2.4 | |
| Native American | 0.4 | 0.0 | |
| Other | 3.6 | 1.2 | |
| Elective hospitalization | 78.8 | 79.6 | 0.112 |
| Primary expected payer | <0.001 | ||
| Medicare | 31.1 | 31.4 | |
| Medicaid | 6.8 | 6.8 | |
| Private insurance | 55.6 | 55.4 | |
| Self-pay | 2.9 | 2.9 | |
| No charge | 0.4 | 0.4 | |
| Other | 3.2 | 3.1 | |
| Median household income (percentile) | <0.001 | ||
| 0–25 | 19.0 | 19.1 | |
| 26–50 | 24.6 | 24.5 | |
| 51–75 | 27.3 | 27.3 | |
| 76–100 | 29.1 | 29.1 | |
| Bed size | <0.001 | ||
| Small | 7.4 | 2.4 | |
| Medium | 19.0 | 14.2 | |
| Large | 73.6 | 83.5 | |
| Location/teaching status | 0.001 | ||
| Rural | 1.7 | 0.0 | |
| Urban nonteaching | 18.7 | 10.4 | |
| Urban teaching | 79.6 | 89.6 | |
| Hospital region | 0.114 | ||
| Northeast | 21.8 | 22.2 | |
| Midwest | 26.2 | 23.1 | |
| South | 31.5 | 33.1 | |
| West | 20.5 | 23.4 | |
| Carotid artery disease | 2.4 | 3.5 | 0.153 |
| Coronary artery disease | 32.6 | 42.3 | <0.001 |
| Smoking | 12.9 | 7.1 | <0.001 |
| Hyperlipidemia | 48.9 | 55.5 | 0.008 |
| Prior stroke | 4.9 | 8.1 | 0.003 |
| Atrial fibrillation | 33.5 | 35.3 | 0.469 |
| Alcohol abuse | 3.6 | 3.5 | 1.000 |
| Deficiency anemia | 13 | 15.4 | 0.165 |
| RA/collagen vascular disease | 1.9 | 5.9 | <0.001 |
| Chronic blood loss anemia | 0.9 | 2.4 | 0.008 |
| Congestive heart failure | 0.9 | 15.4 | <0.001 |
| Chronic lung disease | 16.7 | 16.7 | <0.001 |
| Coagulopathy | 28.1 | 23.6 | 0.045 |
| Depression | 7.9 | 10.6 | 0.043 |
| Obesity | 17.5 | 9.5 | <0.001 |
| Weight loss | 2.8 | 8.3 | <0.001 |
| Uncomplicated DM | 14.9 | 17.7 | 0.112 |
| Complicated DM | 2.4 | 7.1 | <0.001 |
| Drug abuse | 0.0 | 2.1 | <0.001 |
| Hypertension | 61.3 | 70.7 | <0.001 |
| Hypothyroidism | 8.5 | 8.5 | 0.111 |
| Liver disease | 1.8 | 1.8 | <0.001 |
| Lymphoma | 0.4 | 0.0 | 0.417 |
| Fluid and Electrolyte disorders | 33.9 | 33.8 | 0.003 |
| Other neurological disorders | 3.9 | 3.9 | 0.377 |
| Paralysis | 0.9 | 1.0 | 0.008 |
| PVD | 30.4 | 30.3 | <0.001 |
| Renal failure | 6.6 | 6.8 | <0.001 |
| Pulmonary circulation disorders | 0.4 | 0.4 | <0.001 |
| Psychosis | 2.1 | 2.1 | 0.056 |
PCI = percutaneous coronary intervention;
CABG = coronary artery bypass graft; RA = Rheumatoid arthritis; DM = diabetes; PVD = peripheral vascular disease.
Table 2:
Baseline characteristics and comorbidities in a matched cohort of bicuspid aortic valve stenosis patients who underwent either surgical or transcatheter aortic valve replacement
| Variable | SAVR (N = 68) | TAVR (N = 68) | P value |
|---|---|---|---|
| Age | 64.6 ± 12.4 | 65.0 ± 14.8 | 0.871 |
| Sex | |||
| Female | 27.9 | 32.4 | 0.709 |
| Race | 0.126 | ||
| White | 85.3 | 88.2 | |
| Black | 10.3 | 1.2 | |
| Hispanic | 2.9 | 5.9 | |
| Asian or Pacific Islander | 0.0 | 2.9 | |
| Other | 1.5 | 1.5 | |
| Elective hospitalization | 80.9 | 77.9 | 0.832 |
| Primary expected payer | 0.676 | ||
| Medicare | 45.6 | 52.9 | |
| Medicaid | 5.9 | 5.9 | |
| Private insurance | 48.5 | 41.2 | |
| Median household income (percentile) | 0.618 | ||
| 0–25 | 23.5 | 29.4 | |
| 26–50 | 25.0 | 16.2 | |
| 51–75 | 25.0 | 26.5 | |
| 76–100 | 26.5 | 27.9 | |
| Bed size | 0.603 | ||
| Small | 5.9 | 2.9 | |
| Medium | 16.2 | 13.2 | |
| Large | 77.9 | 83.8 | |
| Location/teaching status | 0.325 | ||
| Urban nonteaching | 4.4 | 7.4 | |
| Urban teaching | 95.6 | 92.6 | |
| Hospital region | 0.158 | ||
| Northeast | 235 | 22.1 | |
| Midwest | 27.9 | 19.1 | |
| South | 36.8 | 32.4 | |
| West | 11.8 | 26.5 | |
| Carotid artery disease | 44.1 | 44.1 | 1.000 |
| Coronary artery disease | 4.4 | 4.4 | 1.000 |
| Smoking | 11.8 | 5.9 | 0.365 |
| Hyperlipidemia | 42.6 | 57.4 | 0.122 |
| Prior stroke | 10.3 | 10.3 | 1.000 |
| Atrial fibrillation | 33.8 | 36.8 | 0.858 |
| Alcohol abuse | 1.5 | 4.4 | 0.619 |
| Deficiency anemia | 13.2 | 14.7 | 1.000 |
| RA/collagen vascular disease | 2.9 | 4.4 | 1.000 |
| Chronic blood loss anemia | 1.5 | 1.5 | 1.000 |
| Congestive heart failure | 4.4 | 0.0 | 0.244 |
| Chronic lung disease | 23.5 | 25.0 | 1.000 |
| Coagulopathy | 29.4 | 23.5 | 0.560 |
| Depression | 13.2 | 11.8 | 1.000 |
| Obesity | 10.3 | 13.2 | 0.449 |
| Weight loss | 5.9 | 5.9 | 1.000 |
| Uncomplicated DM | 19.1 | 17.6 | 1.000 |
| Complicated DM | 4.4 | 5.9 | 1.000 |
| Drug abuse | 2.9 | 0.0 | 0.496 |
| Hypertension | 36.8 | 72.1 | 0.849 |
| Hypothyroidism | 11.8 | 11.8 | 1.000 |
| Liver disease | 5.9 | 2.9 | 0.680 |
| Fluid and electrolyte disorders | 30.9 | 25.0 | 0.567 |
| Other neurological disorders | 4.4 | 5.9 | 1.000 |
| Paralysis | 1.5 | 2.9 | 1.000 |
| PVD | 19.1 | 23.5 | 0.676 |
| Renal failure | 20.6 | 19.1 | 1.000 |
| Pulmonary circulation disorders | 1.5 | 0.0 | 1.000 |
| Psychosis | 1.5 | 4.4 | 0.619 |
PCI = percutaneous coronary intervention,
CABG = coronary artery bypass graft, RA = rheumatoid arthritis, DM = diabetes, PVD = peripheral vascular disease
The number of patients with a BAV stenosis who underwent TAVR significantly increased from 0.39% in 2011 to 4.16% in 2014 (P < 0.001), which represents a 3.77% overall growth in procedure rate [Figure 1]. The median LOS was 10.2 days and decreased significantly throughout the above period (mean [SD] 12.2 [8.2] days to 7.1 [5.9] days, P < 0.001) [Figure 2].
Figure 1.
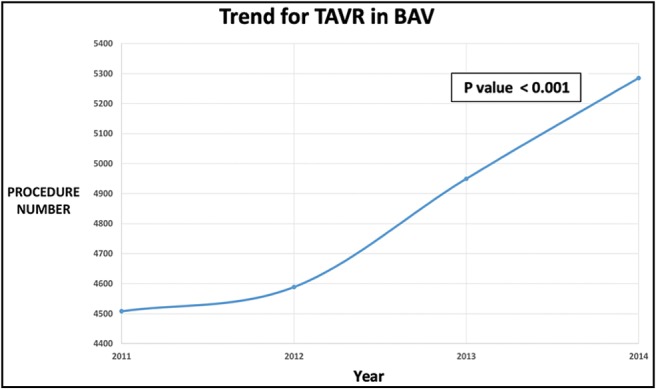
Trend of transcatheter aortic valve replacement (TAVR) in patients with bicuspid aortic valve (BAV) stenosis
Figure 2.
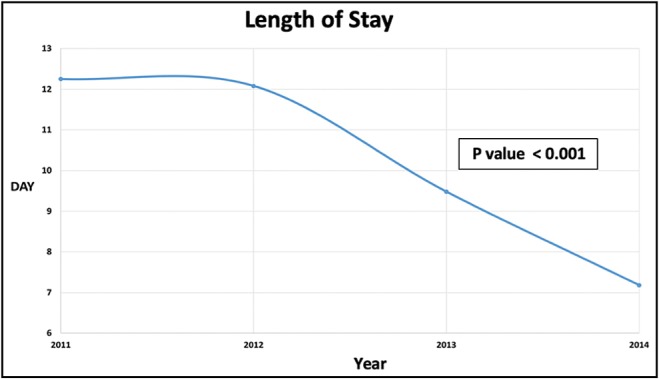
Trends in length of hospital stay
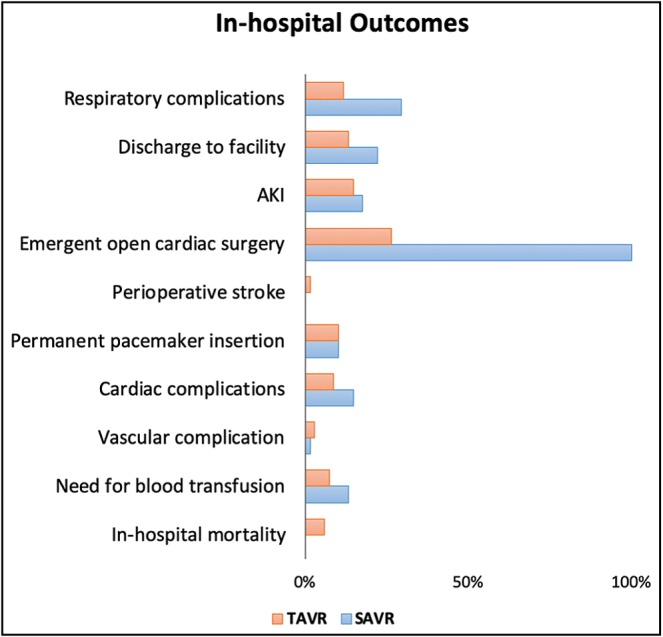
No statistically significant difference in the need for permanent pacemaker placement or the incidence postoperative aortic rupture was observed. On the contrary, the overall vascular complications, the need for blood transfusion, and the requirement for emergent open cardiac surgery have declined over the same period [Figure 3].
Figure 3.

In-hospital outcomes following TAVR in patient with BAV stenosis
After propensity matching of 68 patients [Table 3 and Figure 4], there was no statistically significant difference between SAVR and TAVR groups in the in-hospital mortality (0% vs. 5.9%; adjusted P = 0.119), vascular and cardiac complications, perioperative stroke, acute kidney injury, and permanent pacemaker placement between the two groups. On the contrary, respiratory complications were significantly lower in patients who underwent TAVR (11.8% vs. 29.4%, adjusted P = 0.011).
Table 3:
In-hospital outcomes of a matched cohort of bicuspid aortic valve stenosis patients who underwent either surgical or transcatheter aortic valve replacement
| Outcome | SAVR (N = 68) | TAVR (N = 68) | P value |
|---|---|---|---|
| In-hospital mortality | 0% | 5.9% | 0.11 |
| Need for blood transfusion | 13.2% | 7.4% | 0.39 |
| Vascular complication | 1.5% | 2.9% | 1.00 |
| Injury to blood vessels, accidental puncture, injury to retro-peritoneum, other vascular complications, vascular complications requiring surgery | |||
| Cardiac complications | 14.7% | 8.8% | 0.42 |
| Permanent pacemaker insertion | 10.3% | 10.3% | 1.00 |
| Perioperative stroke | 0% | 1.5% | 1.00 |
| Emergent open cardiac surgery | 100% | 26.5% | <0.001 |
| AKI | 17.6% | 14.7% | 0.81 |
| Discharge to facility | 22.1% | 13.2% | 0.26 |
| Including short term in other hospitals, skilled nursing facility, intermediate care facility, and another type of facility | |||
| Respiratory complications | 29.4% | 11.8% | 0.01 |
| Post-operative acute pneumothorax, postoperative pulmonary edema, pulmonary collapse, prolonged mechanical ventilation >96h, tracheostomy |
SAVR = surgical aortic valve replacement, TAVR = transcatheter aortic valve replacement, AKI = acute kidney injury
Figure 4.
In-hospital outcomes of a matched cohort of bicuspid aortic valve stenosis patients who underwent either surgical or transcatheter aortic valve replacement
DISCUSSION
The findings of our study suggest an increase in the adoption of TAVR for BAV stenosis patients in the United States with overall comparable in-hospital outcomes in those who underwent TAVR and their counterpart in the SAVR cohort.
Patients with BAV were excluded from major early TAVR trials[2,3,4,5] because of several concerns that BAV anatomy might lead to a less than optimal prosthetic valve positioning and expansion leading to significant paravalvular regurgitation or annulus rupture. In addition, the presence of concomitant aortopathy with a potential increased risk of aortic dissection or rupture as well as a questionable long-term durability of transcatheter valves in younger patients with longer life expectancy. Nevertheless, the accumulated experience and advances in device technology have led to the increased off-label use of TAVR for bicuspid AS.[10] Early report by Wijesinghe et al.[14] showed the feasibility of TAVR in 11 patients with severe BAV stenosis. Edwards SAPIEN valves (Edwards Lifesciences, Irvine, CA) were implanted successfully in all patients with significant hemodynamic improvement, but two patients (18.2%) had a moderate paravalvular leak. Although Mylotte et al.[15] showed that TAVR using the first-generation balloon-expandable valves (SAPIEN) or self-expanding valves (Medtronic CoreValve, Medtronic, Dublin, Ireland) were feasible with encouraging short- and intermediate-term clinical outcomes reporting a device success rate of 89.9% and a one-year mortality rate of 17.5% however, a high incidence of post-implantation aortic regurgitation was observed in about 28% of the cases.
More recently, Perlman et al.[16] showed that TAVR in BAV stenosis using a new-generation device was feasible and effective with favorable valve performance and no cases of moderate or severe aortic regurgitation. Yoon et al.[17] provided a head-to-head comparison between the early- and new-generation devices in BAV stenosis patients undergoing TAVR and showed an all-cause mortality rate of 4.3% at 30 days and 14.4% at 1 year. The outcome was comparable to TAVR outcomes in patients with tricuspid AS. Interestingly, there were no cases of moderate or severe paravalvular regurgitation with new-generation devices, as compared with 8.5% incidence of paravalvular regurgitation with the early-generation devices, resulting in higher device success. Recent data from the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapies (STS/ACC TVT) registry from June 2015 to November 2018 compared outcomes of 2,691 matched BAV patients with an equal number who had a tricuspid valve who were considered intermediate or high risk for open-heart surgery and underwent TAVR. There were similar rates for all-cause mortality rates at 30 days (2.6% vs. 2.4%) and one-year (10.8% vs. 12.1%) post-procedure. However, patients with a BAV had a 50% higher risk of stroke at 30 days (2.4%, vs. 1.6% for tricuspid patients). Among patients with a BAV, 0.9% encountered problems during the TAVR procedure that required converting to open-heart surgery, compared with 0.4% of patients in the tricuspid group.[18]
In terms of respiratory complications, our analysis showed a significantly fewer respiratory-related complications (including post-operative pneumothorax, pulmonary edema, pulmonary collapse, prolonged mechanical ventilation, and tracheostomy) in the TAVR group. This favorable respiratory-related outcomes in TAVR is in line with previous reports and could be explained by the shorter intubation period during TAVR procedures compared to SAVR as well as the fact that open cardiac surgery would likely cause more pain and hence increased use of analgesics that can suppress the respiratory drive thus might result in respiratory failure, atelectasis, or aspiration pneumonia.[19]
Limitation
Our study has the following limitations. The analysis of the large administrative data is inherently prone to error because of potential inaccurate coding. However, the NIS database is a reliable source with broad applicability, given its large sample size. Outcome analysis was limited to in-hospital outcomes with no outcomes or complications after discharge were not recorded. Given the patients with BAV are often, younger compared with tricuspid AS, the durability of TAVR prosthesis is of interest, and this is what not captured in this database. In addition, TAVR procedures in this cohort of patients were done using old generation valves, and we were unable to delineate a change of outcome based on the prosthesis or delivery system that was used. However, we can assume that the Edwards SAPIEN Valve (Edwards Lifesciences, Irvine, CA) was dominantly used between the years 2011 and 2014 as the Medtronic CoreValve (Medtronic, Minneapolis, MN) received Food and Drug Administration approval in early 2014. Lastly, because of the small sample of matched patients’ population, this study might not be powered enough to detect a statistically significant difference in the in-hospital mortality between SAVR and TAVR groups (0% vs. 5.9%; adjusted P = 0.119).
CONCLUSIONS
This study shows a steadily increase in the adoption of TAVR for BAV stenosis patients in the United States along with a significant decrease in LOS. TAVR seems a safe and effective therapy in patients with BAV stenosis without aortopathy as compared with SAVR. Further research with multi-institutional studies is warranted to assess the long-term durability and complications associated with TAVR in this patient population.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Michelena HI, Prakash SK, Della Corte A, Bissell MM, Anavekar N, Mathieu P, et al. Bicuspid aortic valve: identifying knowledge gaps and rising to the challenge from the international bicuspid aortic valve consortium (BAVCon) Circulation. 2014;129:2691–704. doi: 10.1161/CIRCULATIONAHA.113.007851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. doi: 10.1056/NEJMoa1008232. [DOI] [PubMed] [Google Scholar]
- 3.Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187–98. doi: 10.1056/NEJMoa1103510. [DOI] [PubMed] [Google Scholar]
- 4.Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Søndergaard L, Mumtaz M, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2017;376:1321–31. doi: 10.1056/NEJMoa1700456. [DOI] [PubMed] [Google Scholar]
- 5.Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374:1609–20. doi: 10.1056/NEJMoa1514616. [DOI] [PubMed] [Google Scholar]
- 6.Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790–8. doi: 10.1056/NEJMoa1400590. [DOI] [PubMed] [Google Scholar]
- 7.Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597–607. doi: 10.1056/NEJMoa1008232. [DOI] [PubMed] [Google Scholar]
- 8.Popma JJ, Adams DH, Reardon MJ, Yakubov SJ, Kleiman NS, Heimansohn D, et al. Transcatheter aortic valve replacement using a self-expanding bioprosthesis in patients with severe aortic stenosis at extreme risk for surgery. J Am Coll Cardiol. 2014;63:1972–81. doi: 10.1016/j.jacc.2014.02.556. [DOI] [PubMed] [Google Scholar]
- 9.Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, III, Guyton RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease. J Thor Cardiovas Surg. 2014;148:e1–e132. doi: 10.1016/j.jtcvs.2014.05.014. [DOI] [PubMed] [Google Scholar]
- 10.Hira RS, Vemulapalli S, Li Z, McCabe JM, Rumsfeld JS, Kapadia SR, et al. Trends and outcomes of off-label use of transcatheter aortic valve replacement: insights from the NCDR STS/ACC TVT registry. JAMA Cardiol. 2017;2:846–54. doi: 10.1001/jamacardio.2017.1685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Overview of the National (Nationwide) Inpatient Sample (NIS) Available from: https://www.hcup-us.ahrq.gov/nisoverview.jsp . [Last accessed on 2018 Feb] [DOI] [PMC free article] [PubMed]
- 12.Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. doi: 10.1097/00005650-199801000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EH. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the valve academic research consortium-2 consensus document. Eur Heart J. 2012;33:2403–18. doi: 10.1093/eurheartj/ehs255. [DOI] [PubMed] [Google Scholar]
- 14.Wijesinghe N, Ye J, Rodés-Cabau J, Cheung A, Velianou JL, Natarajan MK, et al. Transcatheter aortic valve implantation in patients with bicuspid aortic valve stenosis. JACC Cardiovasc Interv. 2010;3:1122–5. doi: 10.1016/j.jcin.2010.08.016. [DOI] [PubMed] [Google Scholar]
- 15.Mylotte D, Lefevre T, Søndergaard L, Watanabe Y, Modine T, Dvir D, et al. Transcatheter aortic valve replacement in bicuspid aortic valve disease. J Am Coll Cardiol. 2014;64:2330–9. doi: 10.1016/j.jacc.2014.09.039. [DOI] [PubMed] [Google Scholar]
- 16.Perlman GY, Blanke P, Dvir D, Pache G, Modine T, Barbanti M, et al. Bicuspid aortic valve stenosis: favorable early outcomes with a next-generation transcatheter heart valve in a multicenter study. JACC Cardiovasc Interv. 2016;9:817–24. doi: 10.1016/j.jcin.2016.01.002. [DOI] [PubMed] [Google Scholar]
- 17.Yoon SH, Lefèvre T, Ahn JM, Perlman GY, Dvir D, Latib A, et al. Transcatheter aortic valve replacement with early- and new-generation devices in bicuspid aortic valve stenosis. J Am Coll Cardiol. 2016;68:1195–205. doi: 10.1016/j.jacc.2016.06.041. [DOI] [PubMed] [Google Scholar]
- 18.Makkar RR, Yoon SH, Leon MB, Chakravarty T, Rinaldi M, Shah PB, et al. Association between transcatheter aortic valve replacement for bicuspid vs tricuspid aortic stenosis and mortality or stroke. JAMA. 2019;321:2193–202. doi: 10.1001/jama.2019.7108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ando T, Adegbala O, Akintoye E, Ashraf S, Pahuja M, Briasoulis A. Is transcatheter aortic valve replacement better than surgical aortic valve replacement in patients with chronic obstructive pulmonary disease? a nationwide inpatient sample analysis. J Am Heart Assoc. 2018;7:pii, e008408. doi: 10.1161/JAHA.117.008408. [DOI] [PMC free article] [PubMed] [Google Scholar]