

Abstract
Objective:
Emergency air medical services (EAMS) share a common helicopter system for prehospital care and transfer in several countries. In Penghu, two systems are involved in EAMS: the helicopter and C130 systems. Given their features and limitations, patients using the two systems have significantly different characteristics.
Materials and Methods:
To clearly understand the disease patterns and dynamic changes in transferred patients, we studied 1228 patients transported from Penghu to Taiwan between January 2009 and December 2017.
Results:
Our findings show that the helicopter group had more acute diseases, while the C130 system group had more chronic diseases. Cardiovascular disease was the most common diagnosis (328 patients, 26.71%), followed by cerebrovascular disease (263 patients, 21.41%) and gastrointestinal disease (221 patients, 17.99%). Following interventions to support local medicine by Tri-Service General Hospital and the establishment of a cardiac catheterization laboratory, the annual number of transported patients decreased, especially those with cardiovascular diseases. The disease pattern also shifted from acute to chronic disease.
Conclusion:
Current data indicate that the local medical system is developing the ability to manage chronic diseases and care problems. This article analyzes dynamic changes in the disease patterns of transferred patients in both EAMS groups, providing a strong foundation for developing local medical systems.
KEYWORDS: Acute coronary syndrome, C-130, Emergency air medical transport, Helicopter, Penghu
INTRODUCTION
Penghu, which covers 126.864 km2 and has a population of 102,304, is a large archipelago of 90 islands between China and Taiwan. Ma-kung is the largest island in Penghu country, with a population of 60,924. It is located off the south coast of Taiwan, near Tainan and Kaohsiung. Geographic barriers have limited the development of local medical services. Penghu has only one teaching hospital and one district hospital to support the local medical service. The teaching hospital, Tri-Service General Hospital, Penghu Branch, has several medical limitations in the areas of critical care, cardiac and cerebrovascular intervention, and chemotherapy and radiotherapy. The geographic barriers and local medical limitations have necessitated the development of emergency air medical services (EAMS). Several previous studies have shown that emergency air medical transport is an effective and safe tool with several benefits, including reduced rescue times and increased cost efficacy, for patients suffering from multiple trauma, acute myocardial infarctions (AMIs), and strokes [1,2,3]. In a rural area without specialized critical care resources, the EAMS is the only choice for acute injury or time-sensitive diseases. In Penghu, the EAMS were established in 1998 and are supported by two systems: helicopters and the C-130 system. The latter consists of Lockheed C-Hercules (C-130) aircraft which belonged to the Republic of China Air Force and operate on fixed flight schedules, requiring long preparation times for patients. The helicopter system is supported by civil aviation, rescue companies, and the National Airborne Service Corps. The two systems have different characteristics; the dynamic change in transfers within the two systems reflects different patient groups. These patient characteristics have rarely been discussed in the literature.
The present descriptive study is based on the researchers' 9-year experience using the emergency air medical transport for critically ill patients; it analyzes 1228 cases transported by the C130 and helicopter systems between 2009 and 2017. The purpose of the study is to investigate the characteristics of patients transferred annually through the two systems. Our findings offer a strong foundation for developing local medical services and upgrading the EAMS.
MATERIALS AND METHODS
Patients
This study was carried out in Taipei Tzu Chi Hospital and the Tri-Service General Hospital, Penghu Branch, between January 2009 and December 2017 by the Department of Emergency Medicine, Taipei Tzu Chi Hospital, and the Buddhist Tzu Chi Medical Foundation. It was approved by the Institutional Review Board of Taipei Tzu Chi Hospital (IRB number: 07-X-069). This is a retrospective analysis of 1228 consecutive patients who were transported by emergency air medical transport from Tri-Service General Hospital and the National Defense Medical Center from Penghu to Taiwan. Cases were excluded if a patient died before the aircraft arrived, discharged himself or herself against medical advice, was receiving hospice care, or was transported by his or her family. The clinical data, including personal data, clinical data, season of the year, and diseases, were all recorded. After data collection, the patients were divided into the C130 group and the helicopter group. The groups were analyzed using the emergency air medical transport database. Our research team studied 1228 cases that met the inclusion and exclusion criteria. There were 739 patients in the C130 group and 489 patients in the helicopter group. Personal and clinical data are shown in Table 1.
Table 1.
Characteristics of patients transported by emergency air medical transport
| Variables | Total (n=1228) | C130 (n=739) | Helicopter (n=489) | P |
|---|---|---|---|---|
| Age (years), mean±SD | 58.89±22.20 | 62.41±20.17 | 53.57±24.03 | <0.001 |
| Age distribution, n (%) | ||||
| ≤20 | 84 (6.84) | 29 (3.92) | 55 (11.24) | <0.001 |
| 21-40 | 160 (13.02) | 88 (11.90) | 72 (14.72) | |
| 41-60 | 319 (25.97) | 174 (23.54) | 145 (29.65) | |
| 61-80 | 446 (36.31) | 291 (39.37) | 155 (31.69) | |
| ≥81 | 219 (17.83) | 157 (21.24) | 62 (12.67) | |
| Gender, n (%) | ||||
| Male | 824 (67.11) | 473 (64.00) | 351 (71.77) | 0.005 |
| Female | 404 (32.89) | 266 (35.99) | 138 (28.22) | |
| Season, n (%) | ||||
| Spring | 332 (27.03) | 185 (25.03) | 147 (30.06) | 0.086 |
| Summer | 345 (28.09) | 204 (27.60) | 141 (28.83) | |
| Autumn | 274 (22.31) | 180 (24.35) | 94 (19.22) | |
| Winter | 277 (22.55) | 170 (23.00) | 107 (21.88) | |
| Disease, n (%) | ||||
| Cardiovascular disease | 328 (26.71) | 128 (17.32) | 200 (40.89) | <0.001 |
| Respiratory disease | 168 (13.68) | 127 (17.18) | 41 (8.38) | <0.001 |
| Cerebrovascular disease | 263 (21.41) | 170 (23.00) | 93 (19.01) | 0.102 |
| Gastrointestinal disease | 221 (17.99) | 150 (20.29) | 71 (14.51) | 0.010 |
| Orthopedic disease | 120 (9.77) | 86 (11.63) | 34 (6.95) | 0.008 |
| Cancer | 110 (8.95) | 93 (12.58) | 17 (3.47) | <0.001 |
| Pediatric disease | 42 (3.42) | 8 (1.08) | 34 (6.95) | <0.001 |
| Obstetrics and gynecology | 21 (1.71) | 2 (0.27) | 19 (3.88) | <0.001 |
| Other | 76 (6.18) | 51 (6.90) | 25 (5.11) | 0.227 |
| Traumatic injury, n (%) | 210 (17.10) | 144 (19.48) | 66 (13.49) | 0.007 |
| Sepsis, n (%) | 144 (11.72) | 112 (15.15) | 32 (6.54) | 0.001 |
| Location of receivng hospital, n (%) | ||||
| Taipei | 324 (26.38) | 314 (42.48) | 10 (2.04) | <0.001 |
| Taoyuan | 24 (1.95) | 23 (3.11) | 1 (0.20) | <0.001 |
| Taichung | 77 (6.27) | 28 (3.78) | 49 (10.02) | <0.001 |
| Tainan | 46 (3.74) | 35 (4.73) | 11 (2.24) | 0.031 |
| Kaohsiung | 714 (58.14) | 297 (40.18) | 417 (85.27) | <0.001 |
| Other | 42 (3.42) | 41 (5.54) | 1 (0.20) | <0.001 |
SD: Standard deviation
Emergency air medical transport system in Penghu
When EAMS are requested, the standard operating procedures begin as follows [Figure 1] (1) EAMS are requested, and a form is sent to the National Aeromedical Approval Center (NAAC). If the patient is relatively stable but cannot transport him or herself, a Lockheed C-130 Hercules (C-130) plane is a possible choice. (2) After NAAC assessment, the civil aviation or rescue company will be assigned during the daytime (from 4 am to 4 pm) and the National Airborne Service Corps will provide support at night (from 4 pm to 4 am). Helicopters and fixed-wing aircraft are provided by the civil aviation or rescue companies. Take off is possible within approximately 2 h and the National Airborne Service Corps can mobilize within 25 min in the daytime and within 40 minutes at night. If the environment does not allow for transport by helicopter or fixed-wing aircraft, the Coast Guard Administration is assigned. (3) Before the aircraft arrives, the transferring hospital coordinates with accompanying medical personnel deploys medical equipment and communicates with the receiving hospital.
Figure 1.

Flowchart of emergency air medical transport services at Tri-Service General Hospital, Penghu Branch
Statistical analysis
We collected and analyzed patient and clinical characteristics, receiving hospital distribution and divisions, seasonal differences, and clinical symptoms and signs. Continuous variables are presented as mean ± standard deviation and categorical variables are shown as percentages. A Chi-square test for independence was used to determine the statistical significance of differences between the two groups; an independent samples t-test was used to analyze continuous variables through SPSS software (Version 13.0 SPSS Inc., Chicago, IL, USA). P < 0.05 indicated statistical significance.
RESULTS
Patient characteristics
Between January 2009 and December 2017, a total of 1228 patients were entered into the emergency air medical transport database at Tri-Service General Hospital, Penghu Branch. These included 739 patients (60.17%) in the C130 group and 489 patients (39.82%) in the helicopter group. The mean age was 58.89 ± 22.20 (62.41 ± 20.17 in the C130 group and 53.57 ± 24.03 in the helicopter group. The patients in the C-130 group were significantly older than those in the helicopter group. Interestingly, the helicopter group had significantly more patients under 20 years old [Table 1]. Helicopters were generally used to transfer infants [Figure 2]. Both groups had higher proportions of males (473 [64.00%] in the C130 group and 351 [71.77%] in the helicopter group) than females, and older people in the 61–80 age group than other age groups. The age distribution of all patients transported from offshore islands in Penghu to Taiwan in the C130 and helicopter groups is shown in Figure 2. The most common diagnosis was cardiovascular disease, followed by cerebrovascular disease (263 patients, 21.41%) and gastrointestinal disease (221 patients, 17.99%). Patients with cardiovascular disease (40.89%) significantly dominated the helicopter group. Patients with pediatric, obstetric, and gynecological conditions were mainly transferred by helicopter. C-130 planes were generally used to transport patients with chronic diseases, including respiratory disease (17.18%), gastrointestinal disease (20.29%), orthopedic disease (11.63%), and cancer (12.58%). More patients were transported in spring and summer than in autumn and winter (677 vs. 551 patients). Subgroup analysis showed no significant differences by season (P = 0.086). Detailed seasonal events are shown in Table 2. The seasonal analysis showed that tourists did not account for a large group of transferred patients because the patient number did not increase in the summer, when most tourists visit Penghu. Most C-130 group patients were transferred to Taipei. For the helicopter group, Kaohsiung Hospital was the main destination for the helicopter group, due to the pattern of transferred diseases and other features of the helicopter system.
Figure 2.
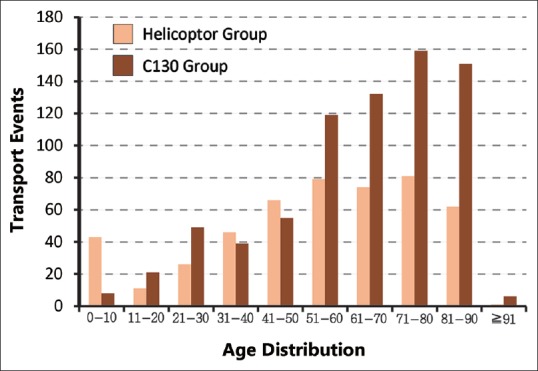
Age distribution of patients transported from Penghu to Taiwan in the C130 and helicopter groups
Table 2.
Monthly distribution of patients transported by C130 and helicopter from 2009 to 2017
| Years | Total | C130 (n=739) | Helicopter (n=489) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Spring | Summer | Autumn | Winter | Spring | Summer | Autumn | Winter | ||
| 2009 | 148 | 18 | 6 | 7 | 7 | 39 | 15 | 19 | 37 |
| 2010 | 161 | 18 | 13 | 19 | 12 | 39 | 32 | 8 | 20 |
| 2011 | 113 | 13 | 15 | 12 | 17 | 17 | 18 | 9 | 12 |
| 2012 | 134 | 17 | 29 | 25 | 20 | 5 | 15 | 14 | 9 |
| 2013 | 127 | 21 | 20 | 33 | 22 | 6 | 9 | 6 | 10 |
| 2014 | 149 | 25 | 41 | 23 | 27 | 3 | 18 | 7 | 5 |
| 2015 | 139 | 31 | 16 | 27 | 25 | 11 | 11 | 11 | 7 |
| 2016 | 89 | 20 | 20 | 17 | 16 | 8 | 6 | 6 | 1 |
| 2017 | 163 | 22 | 44 | 17 | 24 | 19 | 17 | 13 | 7 |
Cardiovascular disease patients
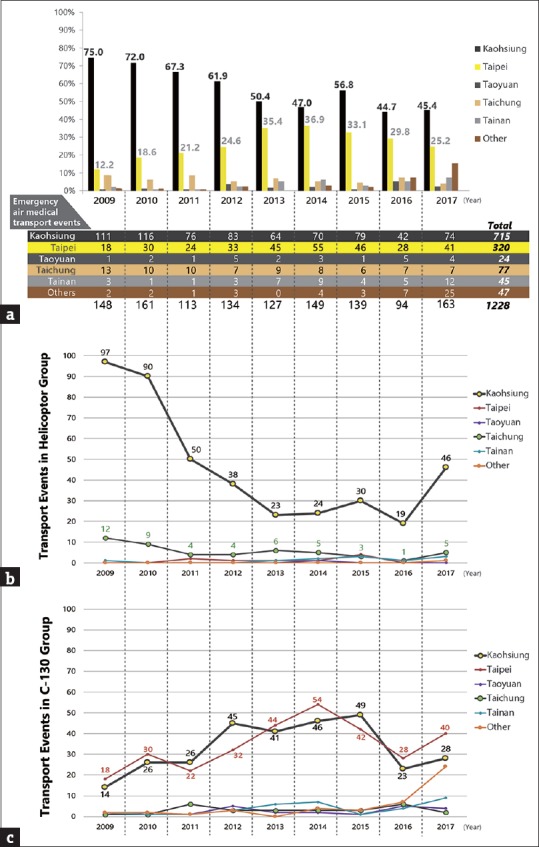
Over the 9 years of the study, the annual proportion of patients transported by C130 increased from 26% in 2009 to 66% in 2017, while that in the helicopter group decreased from 74% in 2009 to 34% in 2017 [Figure 3a]. The increase in C130 transfers was associated with an annual increase in chronic diseases and care problems, such as chemotherapy and radiotherapy for malignancy. Acute coronary syndrome is one of the main acute diseases in Penghu. The largest population of transported patients had cardiovascular disease. However, the number of cardiovascular disease patients transported decreased significantly from 62 patients in 2009 to 14 patients in 2017 [Figure 3b]. The proportion of cardiovascular disease patients transported by C130 increased from 13% in 2009 to 71% in 2017, while that in the helicopter group decreased from 87% in 2009 to 29% in 2017 [Figure 3c].
Figure 3.

(a) Annual distribution of patients transported from Penghu to Taiwan by C130 plane and helicopter from 2009 to 2017. (b) Annual number of cardiovascular disease patients. (c) Annual distribution of cardiovascular disease patients
Receiving hospital location
The location of receiving hospitals was classified into five main city areas, Taipei, Taoyuan, Taichung, Tainan, and Kaohsiung, and “Other.” Taipei and Kaohsiung received the most transported patients. The annual distribution of transported patients by area is shown in Figure 4a. Those received in Kaohsiung decreased between 2009 and 2017. This change reflected a decrease in the helicopter group as only the helicopter system was used to transfer patients to Kaohsiung. It also suggested a decrease in the number of patients with acute diseases and a shift toward chronic care problems. This change is compatible with a decrease in cardiovascular diseases [Figure 4b]. Kaohsiung and Taipei received the most transported patients in the C130 group [Figure 4c].
Figure 4.
(a) Distribution of transported patients by location of receiving hospital (%); (b) annual number of patient transfers in the helicopter group; (c) annual number of patient transfers in the C-130 group
DISCUSSION
The C130 system is only used to transport patients when their medical needs match its scheduled flights. Patients are transported to Magong Airport by ambulance about two hours before the C130 arrives. There is one nurse in the ambulance from the local hospital responsible for transporting the patient to the airport. A flight nurse cares for the patient in the C-130 until he or she arrives at the receiving hospital. The interior of the C130 is not designed specifically for emergency air medical transport. Transferred patients must lie on stretchers instead of beds; they are exposed to engine noise that exceeds permitted levels. Due to the fixed flight schedule and long preparation times, patients transported in this way must be carefully selected by doctors. The C-130s are used to transport relatively stable patients with no life-threatening or chronic diseases, including disabled patients needing rehabilitation and cancer patients needing chemotherapy or radiotherapy. The types of patients transferred by C-130 planes reflect Penghu's general chronic disease care and treatment problems. The helicopter system is more flexible than the C130 system, as is requires shorter takeoff times and less landing space. Although preparation times are shorter, the process still takes approximately two hours, due to a lack of helicopter stations across the Penghu islands. Helicopters transport more emergency and time-dependent patients than C130 planes. Patients in the helicopter group tend to have acute diseases and injuries. Our study showed that patients in the C130 group had more types of diseases than those in the helicopter group. In the helicopter group, acute diseases were the main reason for transfer, in particular, cardiovascular disease, which was also the main diagnosis and accounted for up to 27.74% of the total group and 44.11% of the helicopter group. Before 2014, the EAMS was the only choice for AMI patients. It shortened transport times and significantly improved outcomes [4]. However, it was difficult to deliver patients within the golden time, even when the distance was short, such as to Kaohsiung. To resolve the dilemma, the authorities assessed the possibility of having helicopters on standby in Penghu; however, the cost was very high. Choi et al. [5] analyzed the data between January 2004 and December 2007 and indicated that each mission would cost more than NT$ 300,000, taking into account the cost of transporting staff and services. To improve the outcome of acute disease patients, early diagnosis and timely intervention are necessary. After estimating the cost and benefits of EAMS, it was concluded that an independent medical system in Penghu might be more beneficial than EAMS.
In 2006, Tri-Service General Hospital intervened to support local medicine. The number of patients transported per year from Penghu to Taiwan decreased from 2009 to 2016. According to Su et al. [6], the mortality rate for acute cardiovascular disease significantly decreased after intervention by Tri-Service General Hospital in Penghu. The data in our study are compatible with the forecasts provided by previous studies, as shown in Figure 2. Unfortunately, Tri-Service General Hospital, Penghu Branch, had several medical limitations in the areas of critical care, cardiac and cerebrovascular interventions, chemotherapy, and radiotherapy. There was a shortage of critical care physicians and facilities for managing patients with time-sensitive diseases. After 2014, the first cardiac catheterization laboratory was set up in Penghu Hospital by the Ministry of Health and Welfare. The number of transported patients with cardiovascular diseases significantly decreased in 2014, especially in the helicopter group. Patients with AMI could receive reperfusion with primary percutaneous coronary intervention within the guideline-recommended timeframe.
Kaohsiung received the most patients in both groups, for several reasons. First, the distance is shorter; helicopters can land on the rooftops at Kaohsiung Veterans General Hospital and Kaohsiung International Airport. Second, Penghu is located south of Taiwan, near Tainan and Kaohsiung. Many residents can live with their families in Tainan and Kaohsiung and may prefer to be transferred to southern Taiwan. Third, helicopters are always allowed to land in southern Taiwan; they are restricted from transferring patients to northern Taiwan. After the Tri-Service General Hospital intervention and cardiac catheterization laboratory was established, the proportion of patients in the Kaohsiung group decreased from 75% in 2009 to 45.4% in 2017. This phenomenon was more pronounced in the helicopter group than into C130 group. Annual data revealed that the disease pattern shifted toward chronic diseases and care problems because patients were being transported to hospitals other than the nearest hospital in Kaohsiung. The role of C130 planes in transporting patients from Penghu became increasingly important. However, the treatment plans for chronic diseases were limited by a lack of medical equipment and shortage of hospital doctors. Oncology patients were diagnosed in Penghu but had to go to mainland Taiwan for chemotherapy and radiotherapy. To address this issue, a chemotherapy preparation room was set up in 2015. It will be important to evaluate the effects and benefits of this resource for oncology patients. In addition, tourists make up some of the patients, and they may ask to be transferred to their own cities for further care. Although a seasonal analysis revealed that the number of patients did significantly increase in spring and summer, tourists did not account for a large proportion of the transferred patients.
In conclusion, the dynamic change in the disease pattern corresponds with the annual number of transferred patients in the C130 and helicopter groups, indicating that patients with acute diseases were receiving timely intervention in Penghu. This study reveals that the disease pattern of transferred patients has shifted from acute to chronic diseases. This suggests that local medical systems can provide early management of time-sensitive diseases, such as AMI. The primary role in transporting patients has shifted from the helicopter system to the C-130 system. The interventions of Tri-Service General Hospital and a cardiac catheterization laboratory have played an important role in providing timely treatment and improving clinical outcomes. In addition, the upgrade of local capacity for improving healthcare services can potentially decrease the cost of emergency air medical transport. The treatment of chronic diseases and care problems by local medical systems and EAMS will become a new medical issue for Penghu.
This study has several limitations. First, the particular geographic location and disease pattern in Taiwan resulted in lower external validation. Second, details of confounding factors associated with changing demographic patterns were not included in our database. Finally, the clinical outcomes in this database were not recorded in detail, due to difficulties with long-term follow-up. Therefore, we were unable to analyze or include these data. We aim to investigate this issue in a future study.
Financial support and sponsorship
Nil.
Conflicts of interest
There is no conflict of interest.
Acknowledgments
We are grateful to Chieh-Min Liu, Tzu-Chien Lin, Kai-Hao Lin, and Yi-Min Chu for sharing their experiences with emergency air medical transport in Taiwan and visiting Tri-Service General Hospital, Penghu Branch with us between November 01, 2016 and December 31, 2016.
REFERENCES
- 1.Abe T, Takahashi O, Saitoh D, Tokuda Y. Association between helicopter with physician versus ground emergency medical services and survival of adults with major trauma in Japan. Crit Care. 2014;18:R146. doi: 10.1186/cc13981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grines CL, Westerhausen DR, Jr, Grines LL, Hanlon JT, Logemann TL, Niemela M, et al. A randomized trial of transfer for primary angioplasty versus on-site thrombolysis in patients with high-risk myocardial infarction: The air primary angioplasty in myocardial infarction study. J Am Coll Cardiol. 2002;39:1713–9. doi: 10.1016/s0735-1097(02)01870-3. [DOI] [PubMed] [Google Scholar]
- 3.Silliman SL, Quinn B, Huggett V, Merino JG. Use of a field-to-stroke center helicopter transport program to extend thrombolytic therapy to rural residents. Stroke. 2003;34:729–33. doi: 10.1161/01.STR.0000056529.29515.B2. [DOI] [PubMed] [Google Scholar]
- 4.Chen WL, Ma HP, Wu CH, Chiou HY, Yen Y, Chiu WT, et al. Clinical research of mortality in emergency air medical transport. Biomed Res Int. 2014;2014:767402. doi: 10.1155/2014/767402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choi WM, Tsai SH, Chang WH, Chang KS, Kao CJ. Preliminary study on emergency aeromedical transport of elderly patients from offshore islands in Taiwan. Int J Gerontol. 2009;3:114–21. [Google Scholar]
- 6.Su CH, Wu CP, Tsai SH, Pai L, Tu CM, Chang FC, et al. Outcome of patients with cardiovascular disease transferred by emergency air medical transportation from Penghu Islands to Taiwan: 5 years study. Taiwan Crit Care Med. 2009;10:283–98. [Google Scholar]