

Abstract
Background:
Although evidence from animal and observational studies has supported the beneficial effects of green tea intake for lowering blood pressure (BP), randomized placebo-controlled trials (RCTs) have yielded conflicting results. In this meta-analysis of RCTs, we aimed to assess the effects of green tea supplementation on measures of BP control.
Methods:
The PubMed, Embase, and Cochrane Library databases were electronically searched from inception to August 2019 for all relevant studies. The results were pooled using the generic inverse-variance method with random-effects weighting and expressed as mean differences (MDs) with 95% confidence intervals (CIs). The quality of studies was assessed using the Jadad score. Publication bias was evaluated using funnel plots, Egger test, and Begg test.
Results:
Twenty-four trials with 1697 subjects were included in the meta-analysis. The pooled results showed that green tea significantly lowered systolic BP (SBP; MD: −1.17 mm Hg; 95%CI: −2.18 to −0.16mm Hg; P = .02) and diastolic BP (DBP; MD: −1.24 mm Hg; 95%CI:−2.07 to −0.40mm Hg; P = .004). Significant heterogeneity was found for both SBP (I2 = 43%) and DBP (I2 = 57%). In addition, no evidence of significant publication bias was found from funnel plots or Egger test (P = .674 and P = .270 for SBP and DBP, respectively).
Conclusion:
Overall, green tea significantly reduced SBP and DBP over the duration of the short-term trials. Larger and longer-term trials are needed to further investigate the effects of green tea supplementation on BP control and clinical events.
Keywords: blood pressure, catechin, green tea, meta-analysis
1. Introduction
Cardiovascular disease (CVD) is the leading cause of morbidity, mortality, and disability worldwide.[1] Hypertension is 1 of the leading causes of cardiovascular events[2,3] and the main contributor to 7 million deaths annually worldwide.[4] The risk of CVD doubles for each increment of 20/10 mm Hg in blood pressure (BP)from as low as 115/75 mm Hg.[5] Almost 50% of ischemic heart disease cases and 60% of stroke cases are attributed to elevated BP.[6] Studies have shown that even a modest reduction in BP is clinically relevant in reducing the risk of coronary heart diseases and stroke.[7]
Lifestyle modifications have been shown to be effective in regulating BP.[8] In particular, nutrition therapies have shown beneficial effects for the prevention and control of hypertension. Green tea, obtained from the plant Camellia sinensis, is a widely consumed beverage worldwide and is traditionally used in Asian countries as a medication. The mechanisms underlying the beneficial effects of green tea are mainly attributed to its flavonoid-like polyphenol contents such as catechins. Catechins mainly include epigallocatechin gallate (EGCG), epicatechin gallate, epigallocatechin, and epicatechin, which are the most common green tea extracts and have been shown to be beneficial to human health.[9] In vitro studies have shown that green tea catechins exert a cardioprotective effect through multiple mechanisms, including the inhibition of oxidation, vascular inflammation, and thrombogenesis, as well as the improvement of endothelial dysfunction.[10,11] Animal studies have also revealed that green tea catechins influence nitric oxide production and vasodilation, thereby improving endothelial dysfunction and hypertension in rodents.[10]
To date, many longitudinal observational studies and intervention trials have investigated the association between tea consumption and BP reduction; however, the results were controversial. Some studies reported that tea intake decreased BP,[12,13] whereas others reported no significant change in BP control with tea intake.[14] Thus, we conducted a meta-analysis of all published randomized placebo-controlled trials (RCTs) to quantitatively assess the effect of green tea on measures of BP reduction in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines.
2. Methods
2.1. Search strategy and eligibility criteria
This systematic review and meta-analysis was conducted in accordance with the PRISMA statement guidelines.[15]We searched PubMed, Embase, and the Cochrane Library from the index date of each database through August 2019 by using the following terms: “green tea”,“green tea extract”,“tea component(s)”, “tea solid(s)”, “catechin”, “catechins”, “EGCG”, “Camellia sinensis”, “tea polyphenols”, “blood pressure”, “hypertension”, “hypertensive”,“hypotension”,“hypotensive”,“endothelium”,“endothelial function”, and “endothelial dysfunction.” The search was limited to RCTs in adults (age > 18 years). Language was restricted to English. The reference sections of all articles selected for inclusion and those of previous meta-analysis were hand-searched for additional articles.
2.2. Study selection
The prespecified inclusion criteria were as follows:
-
(1)
Adult subjects who ingested green tea beverages or extract for ≥2 weeks.
-
(2)
RCTs with either a parallel or crossover design.
-
(3)
The baseline and endpoint values of systolic BP (SBP) or diastolic BP (DBP), or both, with standard deviations (SDs), standard errors (SEs), or 95% confidence intervals (CIs) were available for each group in the study.
-
(4)
Green tea extract was not administered as part of a multicomponent supplement in either the experimental or control group.
-
(5)
The food intake control regimens of the experimental groups were consistent with those of the control groups, and the only difference between the control and treatment groups was green tea or green tea extract supplementation; and
-
(6)
Each group had > 10 subjects.
The exclusion criteria were as follows:
-
(1)
Trials that enrolled children or pregnant women.
-
(2)
Review, meta-analysis, or abstract only; and
-
(3)
Trials without details of the EGCG or polyphenol content of the green tea. The data of multiple published reports from the same study population were included only once.
2.3. Quality assessment
The quality of studies was assessed using the Jadad score with the following criteria:
-
(1)
Randomization,
-
(2)
Double blinding (participant and researcher masking),
-
(3)
Reporting the number of and reasons for withdrawal,
-
(4)
Allocation concealment, and
-
(5)
Generation of random numbers.
The trials were scored 1 point for each area addressed in the study design, with a possible score of between 0 and 5 (highest quality).[16] The trials were categorized as high quality (Jadad score ≥4) or low quality (Jadad score <4).
2.4. Data extraction
Two authors (CGZ and XRF) independently extracted the data, and discrepancies were adjudicated by a third author (YK). The following information was abstracted:
-
(1)
Study characteristics (authors, publication year, sample size, study duration, study design, intervention dose, and type of intervention), participant characteristics (location, mean age or age range, sex, preexisting disease or condition, and
-
(2)
Treatment with antihypertensive medications), and details of the baseline and final SBP and DBP measurements. For multi-arm studies, only intervention groups that met the inclusion criteria were used in the analysis. If BP was reported several times in different stages of the trials, only the final BP records at the end of the trials were extracted for the meta-analysis.
2.5. Statistical analysis
Statistical analysis was performed with RevMan version 5 software (Cochrane Collaboration). The main outcome of the meta-analysis was the mean difference (MD) in BP (SBP and DBP, mm Hg) between the intervention and control groups from baseline to the end of the intervention period. When SDs were not directly available, they were calculated from SEs, 95% CIs, P values, or t values.[17] In addition, the change-from-baseline SD values were imputed as suggested by Follmann et al, assuming a correlation coefficient of 0.5.[18] In trials that reported more than 1 BP measure, such as nighttime and daytime ambulatory BP, we used the mean BP calculated from the greatest number of measurements.
Heterogeneity was assessed using the Cochran Q statistic, in which a P value of < .10 was considered significant; and measured inconsistency (I2) statistics, with I2> 50% considered indicative of substantial heterogeneity.[19] We presented the results on the basis of a random-effects model when the test for heterogeneity of the total population was significant. Otherwise, the results of a fixed-effects model are presented.[20] To identify the possible source of heterogeneity within the studies, subgroup and sensitivity analyses were performed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. The following information was abstracted in the subgroup analyses: consumption of catechins, divided into high (≥615 mg/d, high median) and low (<615 mg/d, low median) doses; duration of the green tea intervention, divided into long term (≥12 weeks) and short term (<12weeks); type of intervention, divided into green tea beverage and capsule; ethnicity, divided into Asian and Western; study design, divided into parallel and crossover; health status, divided into healthy and with cardiovascular risks; and baseline BP status, divided into high-normal/hypertensive and normotensive. Trials were considered to be of high quality when the score was ≥4 and low-quality when the score was < 4. Funnel plots and Egger regression test were used to assess publication bias.[21] A P value of < .05 was considered statistically significant, unless otherwise specified.
2.6. Ethics
This is a systematic review and meta-analysis and ethical approval was not necessary.
3. Results
3.1. Results of the literature search
A total of 1132 articles were initially identified after electronic searching. Of them, 1047 articles were excluded because they were not clinical trials, the interventions were irrelevant to the current meta-analysis, or they were duplicated articles. Eighty-five articles remained for a more detailed full-text inspection. An additional 61 articles were excluded for various reasons: 26 articles were excluded because no relevant outcomes were reported; 10 articles were excluded because green tea extract was administered as part of a multicomponent supplement; 4 articles were excluded because only the abstract was available; 18 articles were excluded because they did not meet the inclusion criteria; and 3 articles were excluded because the experiment duration was < 2 weeks. Finally, 24 eligible articles were considered to have met the inclusion criteria and were included in the meta-analysis (Fig. 1).
Figure 1.
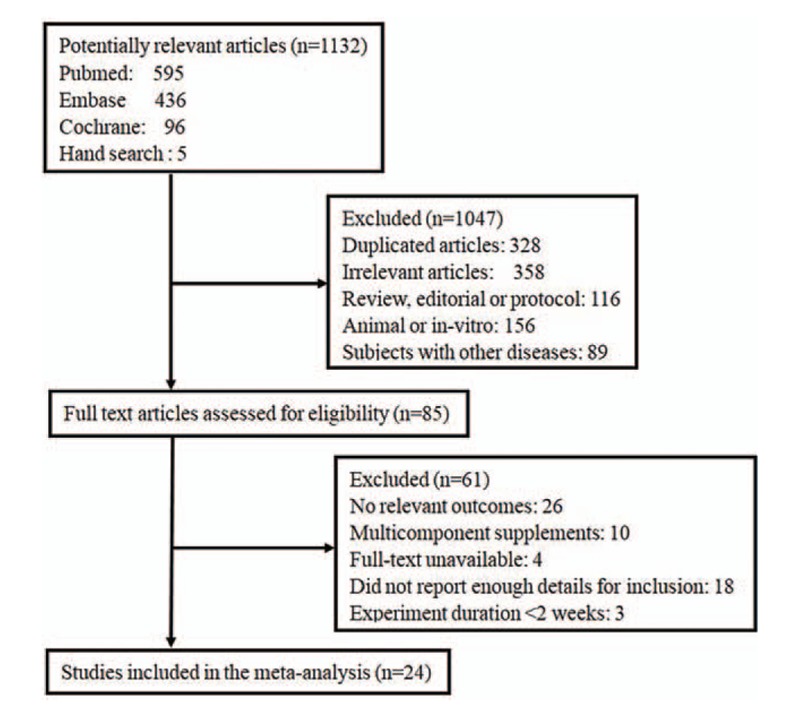
Flow diagram of the study selection process. From a total of 1132 potentially relevant studies, 24 randomized controlled trials that met the predefined inclusion and exclusion criteria were included in the meta-analysis.
3.2. Study characteristics
Twenty-four eligible RCTs with 1697 subjects were enrolled in the meta-analysis.[22–45] The baseline characteristics of the studies included in the meta-analysis are described in Table 1. The trial size ranged from 22 to 240 subjects. The duration of the green tea intervention varied from 3 to 16 weeks. The mean age of the trial participants ranged from 22 to 74 years. The doses of green tea catechins in the treatment group ranged from 208 to 1344 mg/d. The mean pretreatment SBP ranged from 111 to 147 mm Hg, and the mean DBP ranged from 68 to 93 mm Hg.
Table 1.
Characteristics of 24 included randomized controlled trials.
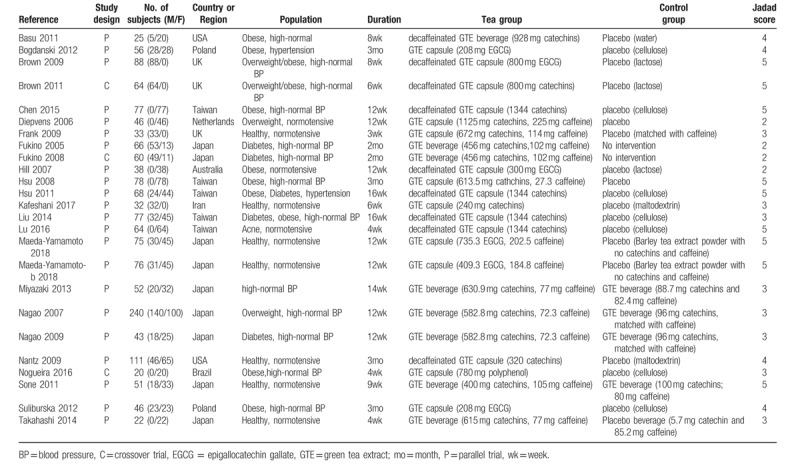
Of the 24 trials with 25 comparisons included in the current meta-analysis, 10 comparisons focused on adults with normotension[27,28,31,34,36,37,41,43,45] and 15 comparisons investigated adults with high-normal or hypertensive BPs.[22–26,29,30,32,33,35,38–40,42,44] Eight comparisons were performed in healthy subjects,[28,34,36,37,41,43,45] and 17 comparisons were conducted in patients with cardiovascular risks.[22–27,29–33,35,38–40,42,44] Most of the comparisons (22/25) used a parallel study design,[22–24,26–29,31–41,43–45] whereas 3 comparisons adopted a crossover design.[25,30,42] Eight comparisons selected green tea beverage,[22,29,30,38–40,43,45] and 17 comparisons used green tea extract capsules.[23–28,31–37,41,42,44] Of the included studies, 10 comparisons were performed in Western countries[22–25,27,28,31,41,42,44] and the remaining 15 were conducted in Asian countries.[26,29,30,32–40,43,45] Nine comparisons used decaffeinated green tea extract as supplement,[22,24–26,31,33,35,36,41] 12 comparisons used caffeinated green tea as supplement,[27–30,32,37–40,43,45] and 4 did not report the use of caffeinated supplements[23,34,42,44] (Table 1).
3.3. Data quality
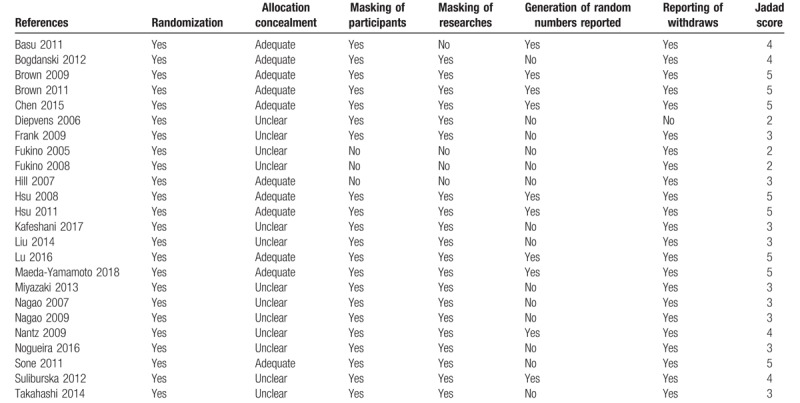
The results on the validity of the included trials are presented in Table 2. Twelve trials were classified as high quality (Jadad score of 4),[23–26,32,33,36,37,41,43,44] and 12 trials were classified as low quality (Jadad score of 2 or 3).[22,27–31,34,35,38–40,42,45] Allocation concealment was adequate in 11 trials and unclear in 13 trials. Twenty trials had a double-blinded RCT design, 1 trial had a single-blinded design, and 3 trials had an open-label design. Ten trials reported the generation of random numbers, but the other 14 trials did not. All trials except for 1 reported dropouts and the reasons for the dropouts (Table 2).
Table 2.
Validity of included studies.
3.4. Effect of green tea on BP
Twenty-five comparisons from 24 studies including 859 subjects in the green tea group and 838 subjects in the placebo group reported the SBPs and DBPs at baseline and follow-up. Compared with the control, green tea significantly lowered both SBP (−1.17mm Hg; 95%CI: −2.18 to−0.16; P = .02) (Fig. 2) and DBP (−1.24mm Hg, 95%CI: −2.07 to−0.40; P = .004) (Fig. 3). The pooled effects on both SBP and DBP were heterogeneous (I2 = 43% and P = .01 for SBP, I2 = 57% and P = .0002 for DBP); thus, we reported the results from the random-effects models.
Figure 2.
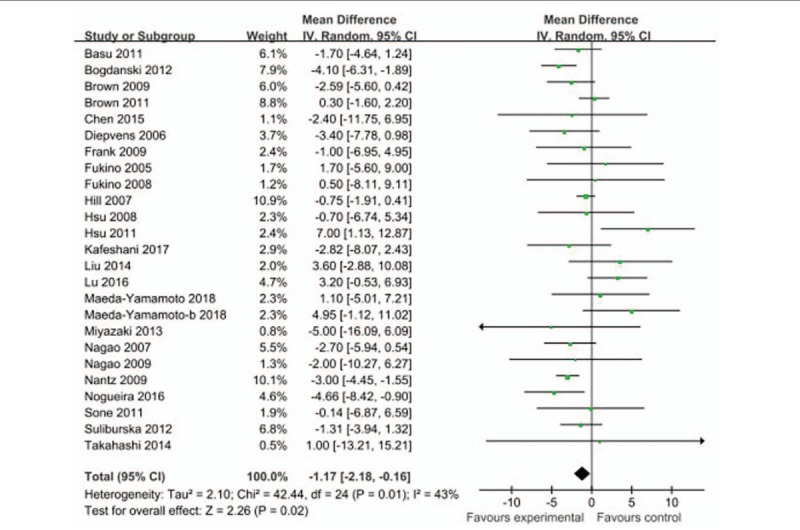
Net changes in systolic blood pressure in randomized trials of green tea supplementation.
Figure 3.
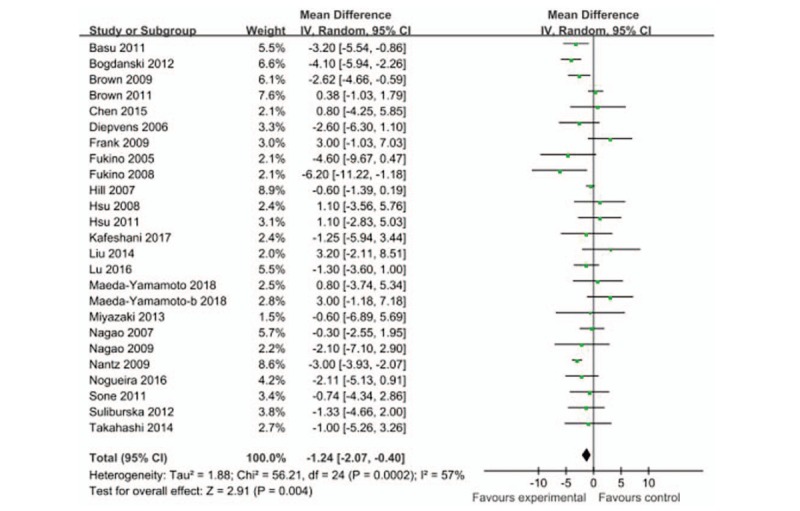
Net changes in diastolic blood pressure in randomized trials of green tea supplementation.
3.5. Subgroup analyses
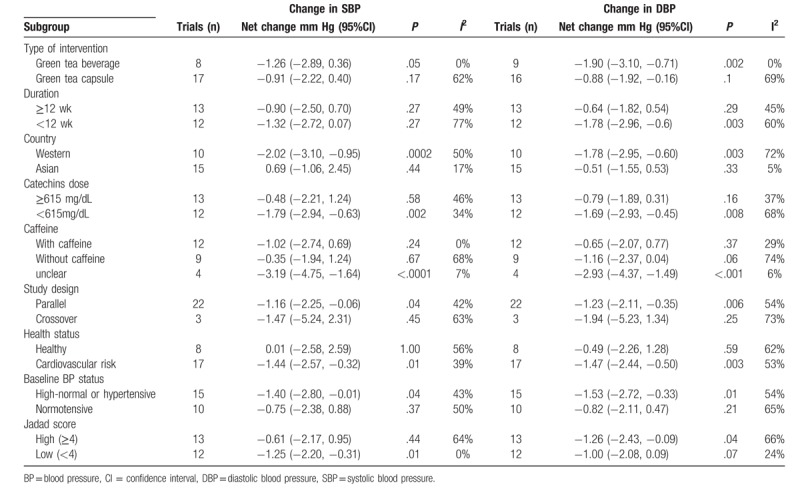
Subgroup analyses were conducted to examine heterogeneity. However, substantial heterogeneity persisted in most subgroup analyses. The subgroup analyses included study duration effects, dose-effect relationship, health status effects, ethnic group variation, coffee content variation, catechin dosage variation, study design effect, and type of intervention effect (green tea beverage or capsule). The subgroup analyses showed that the effects of green tea on both SBP and DBP were greater in subjects with any of the following characteristics: from Western countries, had low catechin dosage(<615 mg/dL), from parallel trials, had high-normal or hypertensive BP, and had cardiovascular risks. The significant reductions in both SBP and DBP were not influenced by the effect of caffeine. Finally, when the studies were stratified according to Jadad score, a significant reduction in SBP was found in low Jadad scores and a significant reduction in DBP was found in high Jadad scores (Table 3).
Table 3.
Subgroup analyses of mean change in BP.
3.6. Publication bias
The funnel plots of the studies were symmetrical for SBP and DBP. Furthermore, the results of Egger regression test suggested no significant asymmetry for the overall effect estimation of SBP (P = .674) and DBP (P = .270).
4. Discussion
Our meta-analysis of 24 observational studies with 1697 subjects showed that green tea consumption significantly lowered both SBP and DBP. In addition, the results of the subgroup analyses suggested that the beneficial effect of green tea (ie, with respect to lowering both SBP and DBP) might be more pronounced in subjects with high-normal BP/hypertension, or other CVD risks. These findings are generally consistent with the results from previous meta-analyses of RCTs in the general population or in participants with cardiovascular risks and provide additional evidence supporting the beneficial effect of green tea supplementation in reducing BP.[12,46]
Observational prospective cohort and case-control studies have been performed to determine the effect of green tea on CVD; however, the results were conflicting. A large population-based study involving 40,000 middle-aged Japanese individuals revealed that compared with non-drinking of tea, habitual green tea consumption (an average of > 2 cups [almost 17oz]/d for 10 years) was associated with a lower risk of death from CVDs.[47] Some studies have revealed that green tea intake significantly lowered BP.[23,41] By contrast, several other studies reported no positive correlations between green tea intake and BP reduction.[26,34] To clarify the precise effect of green tea on BP control, we conducted the current meta-analysis of published RCTs.
The beneficial effects of green tea on cardiovascular health may be related to the high concentration of green tea catechins. Green tea catechins have numerous biological activities that can possibly provide antihypertensive benefits, such as:
-
(1)
Increasing the plasma nitric oxide concentration, which can inhibit proinflammatory cytokines and platelet aggregation and lead to improvement of endothelial dysfunction;[48]
-
(2)
Exerting an antiinflammatory effect through the suppression of several inflammatory factors, such as cytokines, nuclear factor-kappa B, and adhesion molecules;[49,50]
-
(3)
Suppressing the contractile response by inhibiting the mRNA expression of both endothelial nitric oxide synthase and endothelin-1at the physiological concentration, which results in vasodilation and subsequent reduction in BP;[51,52]and
-
(4)
Improving calcium signals in the regulation of phosphorylation levels of inositol triphosphate, calmodulin-dependent protein kinase II, and calmodulin antibodies, particularly EGCG, which possesses a strong antihypertensive activity.[53]
In this meta-analysis, subgroup analyses were performed on the basis of our predefined variables to identify sources of heterogeneity. Our findings indicated that subjects with high-normal BP/hypertension, and CVD risks would obtain the maximum benefit from green tea with respect to SBP and DBP reduction, perhaps through the inhibition of oxidation, vascular inflammation, and thrombogenesis, and by improving endothelial dysfunction in patients with poor BP control and other CVD risks.[51–53] In addition, the subgroup analyses revealed that green tea supplementation had a more pronounced effect on both SBP and DBP in subjects from Western countries than in subjects from Asian countries, which is consistent with the findings of an earlier meta-analysis by Liu et al.[13] Our meta-analysis demonstrated that the BP reduction effect was greater in the low catechin dosage group than in the high catechin dosage group. This result was possibly due to differences in green tea composition and preparations, as well as ethnicity variations among the subjects.
We observed that the effect of caffeine was not significant for both SBP and DBP. As tea naturally contains caffeine in addition to catechins and other compounds, whether caffeine intake influences the BP-lowering effects of tea is another potential issue and is still controversial. Some studies have shown that caffeine alone could increase BP by increasing arterial stiffness and influencing arterial compliance.[54,55] However, other studies indicated that the dosage of caffeine in green tea is relatively lower than the dosage of catechins; thus, the negative effect of caffeine on BP may not overcome the positive effect of tea and catechins.[13]
This meta-analysis had several significant strengths. First, the trials included in this meta-analysis were all RCTs, which ensured relatively high quality and accurate information. Second, the results were unlikely to be influenced by publication bias. The results of Egger regression test suggested no significant asymmetry of the funnel plot for the overall effect estimation of MDs in SBP or DBP. Furthermore, subgroup analyses were performed to detect the sources of heterogeneity in outcomes.
The potential limitations should also be considered. First, our meta-analysis did not identify an optimal dosage of green tea that would best improve BP. The variations in characteristics among the included trials, such as the wide range of catechin dosages (from 208 to 1344 mg/d), made it difficult to assess the true dose-response relationship between tea intake and BP-reducing effects. In addition, the safety margin has not been revealed because no serious adverse effects were reported in the included trials. However, concerns have been raised about the safety of high-dose green tea catechin supplementation. Animal trials reported that intraperitoneal injection of green tea catechins increased the plasma concentrations of alanine transaminase.[56] Clinical trials have also indicated that green tea was the major dietary source of oxalate in some patients with kidney oxalate stones.[57] Second, we identified large variations in trial duration, trial participants, green tea catechin dose, ethnic group, green tea intervention type, and baseline health status. Some of these variations may be significant sources of heterogeneity, which may limit the validity of the overall pooled results. Third, the studies included in the meta-analysis were generally conducted over a short duration, ranging from 3 to 16 weeks, and it is crucial to know the long-term effect of green tea intake on BP. Fourth, the quality of the included studies varied from low to high. Of the 24 studies, 11 were of high quality and the remaining 13 were of low quality, which may have affected the confidence level of the meta-analysis.
In conclusion, evidence from randomized controlled trials to date suggests that green tea supplementation may have a role in lowering both SBP and DBP. However, before green tea supplementation can be recommended for the prevention of hypertension or as an adjuvant antihypertensive therapy, additional trials with larger sample sizes, longer duration, various catechin dosages, and high quality are needed in the future.
Author contributions
Conceptualization: Guangzhi Chen.
Data curation: Renfan Xu.
Formal analysis: Renfan Xu.
Funding acquisition: Renfan Xu.
Methodology: Guangzhi Chen.
Investigation: Renfan Xu.
Software: Ke Yang.
Supervision: Jie Ding.
Validation: Ke Yang, Guangzhi Chen.
Writing – original draft: Renfan Xu.
Writing – review & editing: Guangzhi Chen.
Guangzhi Chen orcid: 0000-0003-2004-1486.
Footnotes
Abbreviations: BP = blood pressure, CI = confidence interval, CVD = cardiovascular disease, DBP = diastolic blood pressure, EGCG = epigallocatechin gallate, MD = mean difference, PRISMA = preferred reporting items for systematic reviews and meta-analyses, RCT = randomized placebo-controlled trial, SBP = systolic blood pressure, SD = standard deviation, SE = standard error.
How to cite this article: Xu R, Yang K, Ding J, Chen G. Effect of green tea supplementation on blood pressure: A systematic review and meta-analysis of randomized controlled trials. Medicine. 2020;99:6(e19047).
The present study was supported by the National Natural Science Foundation of China (No. 81500293).
The authors have no conflicts of interest to disclose.
References
- [1].Salehi-Abargouei A, Maghsoudi Z, Shirani F, et al. Effects of dietary approaches to stop hypertension (DASH)-style diet on fatal or nonfatal cardiovascular diseases--incidence: a systematic review and meta-analysis on observational prospective studies. Nutrition 2013;29:611–8. [DOI] [PubMed] [Google Scholar]
- [2].Jones DW, Hall JE. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure and evidence from new hypertension trials. Hypertension 2004;43:1–3. [DOI] [PubMed] [Google Scholar]
- [3].Sarrafzadegan N, Talaei M, Sadeghi M, et al. The Isfahan cohort study: rationale, methods and main findings. J Hum Hypertens 2011;25:545–53. [DOI] [PubMed] [Google Scholar]
- [4].Jones WS, Vemulapalli S, Patel MR. Interventional treatment of hypertension: a new paradigm. Curr Cardiol Rep 2013;15:356. [DOI] [PubMed] [Google Scholar]
- [5].Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903–13. [DOI] [PubMed] [Google Scholar]
- [6].Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation 2014;129:e28–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Officers A. Coordinators for the ACRGTA, Lipid-Lowering Treatment to Prevent Heart Attack T Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). JAMA 2002;288:2981–97. [DOI] [PubMed] [Google Scholar]
- [8].Kokkinos P, Panagiotakos DB, Polychronopoulos E. Dietary influences on blood pressure: the effect of the Mediterranean diet on the prevalence of hypertension. J Clin Hypertens 2005;7:165–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Sano M, Tabata M, Suzuki M, et al. Simultaneous determination of twelve tea catechins by high-performance liquid chromatography with electrochemical detection. Analyst 2001;126:816–20. [DOI] [PubMed] [Google Scholar]
- [10].Li D, Wang R, Huang J, et al. Effects and mechanisms of tea regulating blood pressure: evidences and promises. Nutrients 2019;11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Chen XQ, Hu T, Han Y, et al. Preventive effects of catechins on cardiovascular disease. Molecules 2016;21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Peng X, Zhou R, Wang B, et al. Effect of green tea consumption on blood pressure: a meta-analysis of 13 randomized controlled trials. Sci Rep 2014;4:6251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Liu G, Mi XN, Zheng XX, et al. Effects of tea intake on blood pressure: a meta-analysis of randomised controlled trials. Br J Nutr 2014;112:1043–54. [DOI] [PubMed] [Google Scholar]
- [14].Vieira Senger AE, Schwanke CH, Gomes I, et al. Effect of green tea (Camellia sinensis) consumption on the components of metabolic syndrome in elderly. J Nutr Health Aging 2012;16:738–42. [DOI] [PubMed] [Google Scholar]
- [15].Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA 2000;283:2008–12. [DOI] [PubMed] [Google Scholar]
- [16].Moher D, Pham B, Jones A, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 1998;352:609–13. [DOI] [PubMed] [Google Scholar]
- [17].Anzures-Cabrera J, Sarpatwari A, Higgins JP. Expressing findings from meta-analyses of continuous outcomes in terms of risks. Stat Med 2011;30:2967–85. [DOI] [PubMed] [Google Scholar]
- [18].Follmann D, Elliott P, Suh I, et al. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol 1992;45:769–73. [DOI] [PubMed] [Google Scholar]
- [19].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [20].DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88. [DOI] [PubMed] [Google Scholar]
- [21].Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Basu A, Du M, Sanchez K, et al. Green tea minimally affects biomarkers of inflammation in obese subjects with metabolic syndrome. Nutrition 2011;27:206–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Bogdanski P, Suliburska J, Szulinska M, et al. Green tea extract reduces blood pressure, inflammatory biomarkers, and oxidative stress and improves parameters associated with insulin resistance in obese, hypertensive patients. Nutr Res 2012;32:421–7. [DOI] [PubMed] [Google Scholar]
- [24].Brown AL, Lane J, Coverly J, et al. Effects of dietary supplementation with the green tea polyphenol epigallocatechin-3-gallate on insulin resistance and associated metabolic risk factors: randomized controlled trial. Br J Nutr 2009;101:886–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Brown AL, Lane J, Holyoak C, et al. Health effects of green tea catechins in overweight and obese men: a randomised controlled cross-over trial. Br J Nutr 2011;106:1880–9. [DOI] [PubMed] [Google Scholar]
- [26].Chen IJ, Liu CY, Chiu JP, et al. Therapeutic effect of high-dose green tea extract on weight reduction: a randomized, double-blind, placebo-controlled clinical trial. Clin Nutr 2016;35:592–9. [DOI] [PubMed] [Google Scholar]
- [27].Diepvens K, Kovacs EM, Nijs IM, et al. Effect of green tea on resting energy expenditure and substrate oxidation during weight loss in overweight females. Br J Nutr 2005;94:1026–34. [DOI] [PubMed] [Google Scholar]
- [28].Frank J, George TW, Lodge JK, et al. Daily consumption of an aqueous green tea extract supplement does not impair liver function or alter cardiovascular disease risk biomarkers in healthy men. J Nutr 2009;139:58–62. [DOI] [PubMed] [Google Scholar]
- [29].Fukino Y, Shimbo M, Aoki N, et al. Randomized controlled trial for an effect of green tea consumption on insulin resistance and inflammation markers. J Nutr Sci Vitaminol (Tokyo) 2005;51:335–42. [DOI] [PubMed] [Google Scholar]
- [30].Fukino Y, Ikeda A, Maruyama K, et al. Randomized controlled trial for an effect of green tea-extract powder supplementation on glucose abnormalities. Eur J Clin Nutr 2008;62:953–60. [DOI] [PubMed] [Google Scholar]
- [31].Hill AM, Coates AM, Buckley JD, et al. Can EGCG reduce abdominal fat in obese subjects? J Am Coll Nutr 2007;26:396S–402S. [DOI] [PubMed] [Google Scholar]
- [32].Hsu CH, Tsai TH, Kao YH, et al. Effect of green tea extract on obese women: a randomized, double-blind, placebo-controlled clinical trial. Clin Nutr 2008;27:363–70. [DOI] [PubMed] [Google Scholar]
- [33].Hsu CH, Liao YL, Lin SC, et al. Does supplementation with green tea extract improve insulin resistance in obese type 2 diabetics? Altern Med Rev 2011;16:157–63. [PubMed] [Google Scholar]
- [34].Kafeshani M, Entezari MH, Karimian J, et al. A comparative study of the effect of green tea and sour tea on blood pressure and lipid profile in healthy adult men. ARYA Atheroscler 2017;13:109–16. [PMC free article] [PubMed] [Google Scholar]
- [35].Liu CY, Huang CJ, Huang LH, et al. Effects of green tea extract on insulin resistance and glucagon-like peptide 1 in patients with type 2 diabetes and lipid abnormalities: a randomized, double-blinded, and placebo-controlled trial. PLoS One 2014;9:e91163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Lu PH, Hsu CH. Does supplementation with green tea extract improve acne in post-adolescent women? A randomized, double-blind, and placebo-controlled clinical trial. Complement Ther Med 2016;25:159–63. [DOI] [PubMed] [Google Scholar]
- [37].Maeda-Yamamoto M, Nishimura M, Kitaichi N, et al. A randomized, placebo-controlled study on the safety and efficacy of daily ingestion of green tea (Camellia sinensis L.) cv. “Yabukita” and “Sunrouge” on eyestrain and blood pressure in healthy adults. Nutrients 2018;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [38].Miyazaki R, Kotani K, Ayabe M, et al. Minor effects of green tea catechin supplementation on cardiovascular risk markers in active older people: a randomized controlled trial. Geriatr Gerontol Int 2013;13:622–9. [DOI] [PubMed] [Google Scholar]
- [39].Nagao T, Hase T, Tokimitsu I. A green tea extract high in catechins reduces body fat and cardiovascular risks in humans. Obesity (Silver Spring) 2007;15:1473–83. [DOI] [PubMed] [Google Scholar]
- [40].Nagao T, Meguro S, Hase T, et al. A catechin-rich beverage improves obesity and blood glucose control in patients with type 2 diabetes. Obesity 2009;17:310–7. [DOI] [PubMed] [Google Scholar]
- [41].Nantz MP, Rowe CA, Bukowski JF, et al. Standardized capsule of Camellia sinensis lowers cardiovascular risk factors in a randomized, double-blind, placebo-controlled study. Nutrition 2009;25:147–54. [DOI] [PubMed] [Google Scholar]
- [42].Nogueira LP, Nogueira Neto JF, Klein MR, et al. Short-term effects of green tea on blood pressure, endothelial function, and metabolic profile in obese prehypertensive women: a crossover randomized clinical trial. J Am Coll Nutr 2017;36:108–15. [DOI] [PubMed] [Google Scholar]
- [43].Sone T, Kuriyama S, Nakaya N, et al. Randomized controlled trial for an effect of catechin-enriched green tea consumption on adiponectin and cardiovascular disease risk factors. Food Nutr Res 2011;55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Suliburska J, Bogdanski P, Szulinska M, et al. Effects of green tea supplementation on elements, total antioxidants, lipids, and glucose values in the serum of obese patients. Biol Trace Elem Res 2012;149:315–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Takahashi M, Miyashita M, Suzuki K, et al. Acute ingestion of catechin-rich green tea improves postprandial glucose status and increases serum thioredoxin concentrations in postmenopausal women. Br J Nutr 2014;112:1542–50. [DOI] [PubMed] [Google Scholar]
- [46].Li G, Zhang Y, Thabane L, et al. Effect of green tea supplementation on blood pressure among overweight and obese adults: a systematic review and meta-analysis. J Hypertens 2015;33:243–54. [DOI] [PubMed] [Google Scholar]
- [47].Kuriyama S, Shimazu T, Ohmori K, et al. Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study. JAMA 2006;296:1255–65. [DOI] [PubMed] [Google Scholar]
- [48].Griendling KK, Alexander RW. Oxidative stress and cardiovascular disease. Circulation 1997;96:3264–5. [PubMed] [Google Scholar]
- [49].Rajagopalan S, Kurz S, Munzel T, et al. Angiotensin II-mediated hypertension in the rat increases vascular superoxide production via membrane NADH/NADPH oxidase activation. Contribution to alterations of vasomotor tone. J Clin Invest 1996;97:1916–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [50].Pagano PJ, Clark JK, Cifuentes-Pagano ME, et al. Localization of a constitutively active, phagocyte-like NADPH oxidase in rabbit aortic adventitia: enhancement by angiotensin II. Proc Natl Acad Sci U S A 1997;94:14483–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Antonello M, Montemurro D, Bolognesi M, et al. Prevention of hypertension, cardiovascular damage and endothelial dysfunction with green tea extracts. Am J Hypertens 2007;20:1321–8. [DOI] [PubMed] [Google Scholar]
- [52].Aird WC. Phenotypic heterogeneity of the endothelium: structure, function, and mechanisms. Circ Res 2007;100:158–73. [DOI] [PubMed] [Google Scholar]
- [53].Ohno S, Yokoi H, Mori K, et al. Ablation of the N-type calcium channel ameliorates diabetic nephropathy with improved glycemic control and reduced blood pressure. Sci Rep 2016;6:27192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [54].Giggey PP, Wendell CR, Zonderman AB, et al. Greater coffee intake in men is associated with steeper age-related increases in blood pressure. Am J Hypertens 2011;24:310–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Potter JF, Haigh RA, Harper GD, et al. Blood pressure, plasma catecholamine and renin responses to caffeine in elderly hypertensives. J Hum Hypertens 1993;7:273–8. [PubMed] [Google Scholar]
- [56].Galati G, Lin A, Sultan AM, et al. Cellular and in vivo hepatotoxicity caused by green tea phenolic acids and catechins. Free Radic Biol Med 2006;40:570–80. [DOI] [PubMed] [Google Scholar]
- [57].Gasinska A, Gajewska D. Tea and coffee as the main sources of oxalate in diets of patients with kidney oxalate stones. Rocz Panstw Zakl Hig 2007;58:61–7. [PubMed] [Google Scholar]