

Abstract
Background
Globally, fire‐related burns and smoke inhalation accounted for 238,000 deaths in 2000, a rate of 3.9 deaths/100,000, with children and young persons aged less than 44 years accounting for the highest proportion of deaths. Smoke alarm ownership has been associated with a reduced risk of residential fire death.
Objectives
We evaluated interventions to promote residential smoke alarms, to assess their effect on the prevalence of owned and working smoke alarms, and the incidence of fires and burns and other fire‐related injuries.
Search methods
We searched the Cochrane Injuries Group's specialised register, CENTRAL, MEDLINE, EMBASE, PsycINFO, CINAHL, ERIC, Dissertation Abstracts, IBSS, ISTP, FIREDOC, LRC, conference proceedings, published case studies, and bibliographies, and contacted investigators and relevant organisations to identify trials. Most of the searches were last updated in September 2007.
Selection criteria
Randomised or non‐randomised controlled trials completed or published after 1969 evaluating interventions to promote residential smoke alarms.
Data collection and analysis
Two authors independently extracted data and assessed trial quality. We performed meta‐analysis of randomised controlled trials to combine odds ratios (OR) between intervention and control groups, using a random effects model. A chi‐square test for heterogeneity used a significance level of 10%. Non‐randomised trial results are described narratively.
Main results
We identified 26 completed trials, of which 17 were randomised. Overall, counselling and educational interventions, with or without provision of free or discounted smoke alarms, modestly increased the likelihood of owning an alarm (OR = 1.21; 95% CI 0.89 to 1.64) and having an installed, functional alarm (OR = 1.33; 95% CI 0.98 to 1.80). Whether or not the intervention programme provided free or discounted smoke alarms in addition to education did not influence these results. The results were sensitive to trial quality, however. Counselling as part of primary care child health surveillance had somewhat greater effects on alarm ownership (OR = 1.96; 95% CI 1.03 to 3.72) and function (OR = 1.46; 95% CI 1.15 to 1.85), results that were generally supported by non‐randomised trials evaluating similar interventions. Injury outcomes were reported in only one randomised controlled trial, which found no effect of a smoke alarm give‐away programme on total injuries (rate ratio 1.3; 95% CI 0.9 to 1.9) or on hospitalizations and deaths (rate ratio 1.3; 95% CI 0.7 to 2.3), in contrast to the substantial reduction in serious injuries reported in a non‐randomised trial that evaluated a similar give‐away programme. Neither trial showed a beneficial effect on fires. Mass media and community education showed little benefit in multiple non‐randomised trials. Two trials, one of which was randomised, showed that smoke alarm installation programmes increase the likelihood of having a working smoke alarm, and the non‐randomised trial reported reductions in fire‐related injuries.
Authors' conclusions
This review found that programmes to promote smoke alarms have at most modest beneficial effects on smoke alarm ownership and function, and no demonstrated beneficial effect on fires or fire‐related injuries. Counselling as part of child health surveillance has a somewhat greater effect on smoke alarm ownership and function, but its effects on injuries are unevaluated. Community smoke alarm give‐away programmes have not been demonstrated to increase smoke alarm prevalence or to reduce fires or fire‐related injuries. Community‐based education programmes have not been shown to reduce burns or fire‐related injuries. Community smoke alarm installation programmes may increase the prevalence of working alarms and reduce fire‐related injuries, but these results require confirmation, and the cost‐effectiveness of such programmes has not been evaluated. Efforts to promote smoke alarms through installation programmes should be evaluated by adequately designed randomised controlled trials measuring injury outcomes and cost‐effectiveness.
Plain language summary
Interventions for promoting smoke alarm ownership and function
Many people are killed or injured by house fires each year. Fires detected with smoke alarms are associated with lower death rates. This review found that programmes to promote smoke alarms increased smoke alarm ownership and function modestly, if at all, and have not demonstrated a beneficial effect on fires or fire‐related injuries. Counselling by health care workers, as part of child health care, may increase ownership and use of smoke alarms in homes but effects on injuries have not been examined. There is little evidence to support community‐wide mass media or educational programmes or programmes to give away free smoke alarms as effective methods to promote smoke alarms or reduce injuries from fire. More research is needed to examine community‐wide smoke alarm installation programmes.
Background
Globally, fire‐related burns and smoke inhalation accounted for 238,000 deaths in 2000, a rate of 3.9 deaths/100,000, with children and young persons aged less than 44 years accounting for the highest proportion of deaths (Peden 2002). Residential fires caused 491 deaths and 14,100 non‐fatal injuries in the United Kingdom in 2005 (Fire Statistics UK). In the United States in 2005, fires caused 3,675 deaths and 17,925 non‐fatal injuries (NFPA 2006).
Fires detected by smoke alarms are associated with more rapid discovery, lower casualty rates and less property damage (Watson 1999). Smoke alarm ownership is associated with a reduced risk of fire death (DiGuiseppi 1998a; Marshall 1998; Runyan 1992) and appears particularly effective in households with young children (DiGuiseppi 1998a; Runyan 1992). We systematically reviewed trials evaluating interventions to promote residential smoke alarms, to assess their effect on smoke alarm ownership and function, fires and fire‐related injuries.
Objectives
To evaluate interventions to promote residential smoke alarms in order to assess their effect on smoke alarm ownership and function, fires, and fire‐related injuries.
Methods
Criteria for considering studies for this review
Types of studies
Controlled trials (randomised, quasi‐randomised or non‐randomised), where participants were prospectively assigned to study groups and where control group outcomes are measured concurrently with intervention group outcomes. Only studies completed or published after 1969 were included, as residential smoke alarms did not become widely available and affordable until the mid‐1970s.
Types of participants
People who were not institutionalised (that is, community‐dwelling individuals).
Types of interventions
Any interventions designed (either wholly or in part) to increase the prevalence of owned or properly functioning smoke alarms ‐ for example, mass media, education, home visits or inspections, clinician counselling, give‐away programmes, discount coupons, legislation. Interventions included programmes to increase ownership, maintenance, proper use, testing, battery changing, etc.
Types of outcome measures
Fire‐related injuries or burns (self‐reported injuries, GP visits, Accident & Emergency visits, hospitalisations, disabilities or deaths); fires; owned or installed and functioning smoke alarms (self‐reported or observed).
Search methods for identification of studies
Searches were not restricted by language, date or publication status.
Electronic searches
We searched the following electronic databases:
Cochrane Injuries Group's specialised register (September 2007),
Cochrane Controlled Trials Register (The Cochrane Library issue 3, 2007),
MEDLINE (1970 to week 1, September 2007),
EMBASE (1970 to 2007 week 37),
PsycLIT (1974 to January 1998),
PsycINFO (1998 to week 3, September 2007),
Cumulative Index to Nursing and Allied Health (CINAHL) (1982 to week 2, September 2007),
Educational Resource Information Center (ERIC) (1989 through September 2007),
Dissertation Abstracts (1970 to September 2007),
International Bibliography of the Social Sciences (IBSS) (1970 to August 2007),
Index of Scientific and Technical Proceedings (ISTP) (1970 to May 2003),
FIREDOC (Fire Research Information Service, http://firedoc.cfr.nist.gov/) (1970 to May 2003),
LRC, the US Fire Administration's online database (http://www.usfa.fema.gov/lrc/) (1970 to March 1998),
Science Citation Index Expanded (2003 to September 2007).
Details of the search strategies can be found in Appendix 1.
Searching other resources
We examined reference lists of reviews (Bass 1993; Ciliska 1996; Harborview MC 1997; Munro 1995; Towner 1996; US Task Force 1996, Towner 2001a, Towner 2001b, Warda 1999), conference proceedings (First World Cf 1989, Second World Cf 1993, Third I Cf 1996, Fourth World Cf 1998), case study collections (Kulenkamp 1994; National Center 1996; Schaenman 1990; US Fire 1993), and included trials. To find internal or unpublished documents, we contacted national and international organisations involved in fire and injury prevention, such as the Home Office (United Kingdom), National Fire Protection Association (United States), Centers for Disease Control and Prevention (United States), Centre d'Information et de Rencontre pour la Prévention des Accidents d'Enfants (France), and International Society for Child and Adolescent Injury Prevention. We contacted the investigators of eligible trials and asked them to identify additional relevant trials. We searched the Internet by author to find completed versions of previously ongoing trials.
Data collection and analysis
Selection of studies
Title, abstract and keywords of all citations were examined and studies that were ineligible based on type of study, participants, intervention, or date of completion, were excluded. The full texts of remaining citations were reviewed and those that failed to meet these same inclusion criteria were excluded. We contacted corresponding authors of all remaining studies to determine eligibility, request outcome data or other details, and identify additional trials. When the corresponding author was deceased or untraceable, we contacted additional authors.
Data extraction and management
Two investigators (CD and CG or CD and Dr. Ian Roberts) independently extracted data on participants, interventions, outcomes, loss to follow‐up, and methods of allocation concealment and outcomes assessment (as quality indicators (Schulz 1995)).
Assessment of risk of bias in included studies
Allocation concealment was rated as adequate if methods convincing of concealment were used (for example, sequentially numbered, sealed, opaque, envelopes) and otherwise as inadequate (for example, alternation) (Schulz 1995). Outcomes assessment was rated as (single) blinded if data were collected either by researchers blinded to intervention status or by postal survey. Subjects were not blinded in any trial. Differences were resolved by discussion.
Assessment of heterogeneity
A chi‐square test for heterogeneity, that is, whether observed differences among the results of included trials are greater than could be expected by chance, used a significance level of 10%. Except where specifically noted, there was no significant heterogeneity for smoke alarm outcomes. To explore heterogeneity, we planned the following subgroup analyses:
safety advice implemented as part of routine child health surveillance ('well child care')
providing discounted / free smoke alarms to participants
adequate allocation concealment
blinded outcomes assessment.
Data synthesis
Primary outcome measures included post‐intervention proportions with owned, functional (that is, installed and working based on button or smoke test), newly acquired, and newly functional smoke alarms, and incidences of fires and fire‐related injuries. When data on acquisition of alarms or of functional alarms were unavailable, we estimated these data by subtracting pre‐ from post‐intervention prevalence for each group, if possible.
We performed meta‐analysis to combine odds ratios (OR) between intervention and control groups, using a random effects model (DerSimonian 1986) because of the substantial variability in populations and interventions. For cluster randomised trials, we reduced subject numbers to 'effective sample sizes' (Hauck 1991) using published estimates for the intraclass correlation coefficient: 0.017 for medical practices (Kendrick 1999), 0.02 for school classes (Murray 1994), and 0.0003 for geographic areas (DiGuiseppi 2002). As sensitivity analyses we alternatively (i) ignored clusters and (ii) used intraclass correlation coefficients five times larger than the above. Neither alternative materially affected the results (data not shown). For DiGuiseppi 2002, which accounted for cluster randomization in its analysis, we entered numerical data into RevMan to produce the same OR and 95% CI as published. Harvey 2004 did not specify the number of clusters in two of the states. For Maryland, we counted 26 census tracts within Baltimore City. For Arkansas, for which no information was provided, we conservatively assumed one intervention and one control area.
Results from non‐randomised trials were not quantitatively combined.
Results
Description of studies
In the initial searches, we found 4,486 unduplicated citations in electronic databases. From these, we identified 118 potentially relevant citations. We found an additional 28 potentially relevant citations from other sources. We could not retrieve the full text of two studies (Botruff 1992; Linyear 1982) and nine were available only in abstract. Of 135 studies reviewed in full, 15 trials met all inclusion criteria (Barone 1988; Clamp 1998; Davis 1987; Kelly 1987; Kendrick 1999; Mallonee 1996; Mathews 1988; McConnell 1996; Miller 1982; Ozanne‐Smith 2002; Project Burn 1979; Schwarz 1993; SCIPP 1989; Thomas 1984; Williams 1988), the eligibility of 16 could not be determined, and the remainder were excluded. To determine the eligibility of the nine abstracts and remaining 16 trials, we contacted all 24 authors. From 22 (92%) responses, we identified six additional eligible trials (Gielen 2001; Jenkins 1996; King 2001; LeBailly 1990; Ploeg 1994; Smithson 1998). We also found one multi‐site trial in progress through organisational contacts (written communication, P Harvey, Centers for Disease Control and Prevention, 2 July 1998). Thus, our initial review included 22 trials, of which three were ongoing (Smithson 1998; Gielen 2001; Harvey 2004).
From our updated electronic searches, we identified 33 potentially relevant citations which were retrieved in full‐text. From these reports and from investigator contacts, we identified four new randomised controlled trials (DiGuiseppi 2002; Gielen 2002; Hendrickson 2000; Watson 2005), one new non‐randomised controlled trial (Johnston 2000), reports from two randomised controlled trials that had been ongoing in our initial review (Harvey 2004; Gielen 2001), and the final reports from two completed trials already included in the initial review (King 2001; Ozanne‐Smith 2002).
The characteristics of each included trial are listed in the table 'characteristics of included studies'.
Studies identified after August 2007 are listed as 'studies awaiting assessment'.
Randomised controlled trials
We identified a total of 18 randomised controlled trials, of which 17 are known to have been completed. The status of one trial (Smithson 1998) previously identified as ongoing could not be determined.
All 17 completed trials targeted populations at high risk for fire injury and death, that is, young children, elderly adults, or low‐income households. Nine were cluster randomised trials, which enrolled prenatal, parenting, or school classes, general clinical practices, high‐risk or deprived communities, or physicians in training. Seven individual randomised controlled trials enrolled parents of young children, while one enrolled elderly public health clients.
Ten interventions were delivered in the clinical context (Barone 1988, Clamp 1998, Gielen 2001, Gielen 2002, Jenkins 1996, Kelly 1987, Kendrick 1999, Thomas 1984, Watson 2005, Williams 1988), six interventions were delivered in the home (DiGuiseppi 2002, Harvey 2004; Hendrickson 2000, King 2001, Mathews 1988, Ploeg 1994), and one was delivered in primary school classes (Davis 1987). All of the trials included an educational component, ranging from delivery of a single fire safety brochure to multiple educational sessions including hazard assessment and behavioral change techniques. Seven trial interventions combined discounted or free smoke alarms with education (Clamp 1998; DiGuiseppi 2002; Hendrickson 2000; Kendrick 1999; King 2001; Thomas 1984; Watson 2005).
Non‐randomised controlled trials
We identified nine completed non‐randomised controlled trials. The study populations included cities or areas within cities (for example, census tracts), parents with children enrolled in clinical practices or government‐funded preschool enrichment centers, and residents in government owned housing.
Two of the studies evaluated safety advice during routine child health surveillance visits (LeBailly 1990; Miller 1982), one evaluated education during mandatory tenants' meetings (McConnell 1996), and one evaluated home safety interventions for parents of children enrolled in preschool enrichment programs. The other five evaluated community programs involving mass media, school or community education, clinical counselling, free smoke alarms, and / or alarm installation (Mallonee 1996, Ozanne‐Smith 2002, Project Burn 1979; Schwarz 1993; SCIPP 1989).
Further information on the non‐randomised studies is presented in Table 12.
1. Data from non‐randomised controlled trials.
| Study | Participants (I/C) | Intervention | Assessment | Smoke alarms | Other outcomes | Notes |
| Project Burn Prevention (McLoughlin 1979, MacKay 1982, McLoughlin 1982) | I: 3 cities in east of state C: 2 cities in west of state (with lower baseline burn incidence) | I1: Mass media I2: I1 + school program I3: I1+ community outreach C: No intervention | Population surveillance for ER injury visits, 4 years before to 12 months after; telephone surveys | Not reported for both groups | Adjusted burn incidence rate ratio, during vs before: Intervention: I1) 1.4 (1.1, 1.6) I2) 0.8 (0.5, 1.1) I3) 1.2 (0.8, 1.7) Control: 1.0 (0.6, 1.5) | |
| Miller 1982 | I: 120 consecutive parents of children seen for well child care in middle class suburban practice C: Preceding 120 consecutive, similar parents | I: Pamphlet, brief education, discount alarms in office; usual well child care C: Usual well child care | Home inspection 4‐6 weeks after intervention. Response rate: I: 108/120 (90%) C: 105/120 (88%) | Intervention: Owned: 79/108 (73%) Installed: 72/108 (67%) Functioning: 61/108 (56%) Control: Owned: 64/105 (61%) Installed: 64/105 (61%) Functioning: 46/105 (44%) | Not reported | |
| LeBailly 1990 | 407 families with children <5 yrs seen for well child care in suburban practice or urban clinic, allocated sequentially in groups of ˜100 (differed on home ownership, socio‐economic status) | I1: Free alarm and other safety devices, usual well child care I2: Free alarm and other safety devices, injury prevention counselling, usual well child care I3: Injury prevention counselling, usual well child care C: Usual well child care | Non‐blinded home interviews and inspections 9 months after intervention. Response rate: ˜75% | Intervention: Owned: I1: 100% I2: 99% I3: 92% (numerators, denominators not reported) Control: Owned: 96% (numerators, denominators not reported) | Not collected | |
| SCIPP (Guyer 1989, Bass 1991) | I: 9 communities (total pop. 139,807) C: 5 demographically similar communities (total pop. 146,866) | I: Injury prevention program in communities, schools, homes, and clinical settings C: No intervention | Population injury surveillance 1 yr before to 2 mos after. Phone survey response: pre‐ 59%, post‐ 85% (similar in 2 groups) | Intervention: Owned: 418/508 (82.3%) Change: +9.4% Control: Owned: 339/409 (83.9%) Change: +14.9% | Adjusted odds ratio for burns (during vs before), in intervention vs control communities: OR=0.8 (0.5, 1.2) | Unpublished data provided by investigators |
| Schwarz 1993 | I: 5 contiguous census tracts [3004 households (51%) participated] C: 4 bordering, contiguous census tracts (similar socio‐demographics, baseline injury rates) | I: Free alarms and installation; home inspection, education, modification; community education C: No intervention | Population injury surveillance 2 yrs before to 1 yr after program. 1‐yr post‐intervention inspection of randomly selected households. Response rate: I: 902/1250 (72%) C: 1060/1472 (72%) | Intervention: Functioning: 866/902 (96%) Control: Functioning: 816/1060 (77%) Adjusted odds ratio: 7.14 (5.0 to 10.0) | Intervention: Fire‐related injuries/1,000: Before: 1.83 During: 1.14 After: 0.86 Incidence change (after vs before): 0.5 (0.4, 0.6) Control: Fire‐related injuries/1,000: Before: 1.34 During: 2.68 After: 1.11 Incidence change (after vs before): 0.8 (0.6, 1.1) | Unpublished data provided by investigators |
| Mallonee 1996 | I: City area with highest risk of fire‐related hospitalisations and deaths C: Rest of city | I: Door‐to‐door alarm give‐away, fire prevention brochures, limited alarm installation C: No intervention | Population fire and fire‐related injury surveillance 2.5 years before to 4 years after program | Intervention: Functioning at 4 years: 45% Control: Not collected | Intervention: After vs before: Fire‐related injuries/100k: 0.2 (0.1, 0.4) Fire‐related injuries/100 fires: 0.3 (0.1, 0.6) Fires/1000 homes: 0.75 (0.5, 1.1) Control: After vs before: Fire‐related injuries/100k: 1.1 (0.7, 1.7) Fire‐related injuries/100 fires: 1.3 (0.9, 2.0) Fires/1000 homes: 0.8 (0.5, 1.3) | |
| McConell 1996 | I: All 2350 new residents of subsidised housing C: All existing residents (lower baseline fire risk, similar socio‐demographics) | I: 35‐minute mandatory lecture and video on fire safety and prevention; reminder card C: No intervention | Population fire surveillance during 15 month study period | Not collected for either group | Intervention: 278 fires/100k person years Control: 1538 fires/100k person years Relative risk (Intervention vs. Control) 0.18 (0.16, 0.21) | |
| Johnston 2000 | I: 6 preschool enrichment centers C: 3 preschool enrichment centers (213 families) C: 3 preschool enrichment centers (149 families) | I: Written safety information and free alarms or batteries if needed C: Written safety information only | Home inspection 3 months after intervention | Functioning alarms: Intervention: 211/211 (100%) Control: 136/143 (95%) Adjusted RR: 1.06 (95% CI: 1.00, 1.12); Fisher Exact 2‐tailed: P=0.018; Functioning alarms acquired: Intervention: 13/211 (6.0%) Control: 3/143 (2.1%) Adjusted RR: 2.37 (95% CI: 0.52, 10.86); Fisher Exact 2‐tailed: P=0.33 | Not collected | |
| Ozanne‐Smith 2002 | I: Municipality C: Demographically similar municipality (with higher baseline injury hospitalisation rate) | I: 6‐year community injury prevention program: mass media, education, training, promotion and action for hazard reduction and environmental change C: No intervention | Population injury surveillance; telephone survey post‐intervention of 250 randomly selected households each group | Intervention: Installed: 166/248 (67%) Installed since program began: 158/248 (64%) Control: Installed: 166/250 (66%) Installed since program began: 156/248 (63%) | Fire‐related injury data not reported. |
Risk of bias in included studies
Randomised controlled trials
Allocation concealment was judged to be adequate in nine trials (53%), including eight trials that used random numbers tables read by an independent person or computerised randomisation by an independent person (Clamp 1998; DiGuiseppi 2002; Gielen 2001; Jenkins 1996; Kendrick 1999; Ploeg 1994; Watson 2005; Williams 1988), and one that used sequentially numbered, sealed opaque envelopes (King 2001). Allocation concealment was either inadequate or unspecified in the remaining eight completed trials (Barone 1988; Davis 1987; Gielen 2002; Harvey 2004; Hendrickson 2000; Kelly 1987; Mathews 1988; Thomas 1984).
Blinded outcome assessment was reported in eight (47%) of the trials (DiGuiseppi 2002; Gielen 2001; Jenkins 1996; Kelly 1987; Kendrick 1999; King 2001; Ploeg 1994; Watson 2005).
The majority of trials (n = 10; 59%) reported loss to follow‐up or survey non‐response rates of less than 25% (Clamp 1998; Davis 1987; DiGuiseppi 2002; Hendrickson 2000; Jenkins 1996; King 2001; Mathews 1988; Ploeg 1994; Thomas 1984; Watson 2005). Loss to follow‐up is not applicable to population‐based surveillance of fires or injuries.
Non‐randomised controlled trials
Allocation concealment was rated inadequate for all non‐randomised trials. None of the trials reported blinded outcome assessment. Studies that collected smoke alarm data reported loss to follow‐up or survey non‐response rates of 28% or less, although one study did not report this information (Ozanne‐Smith 2002). Loss to follow‐up is not applicable to population‐based surveillance of fires or injuries.
Effects of interventions
Smoke alarms
Randomised controlled trials
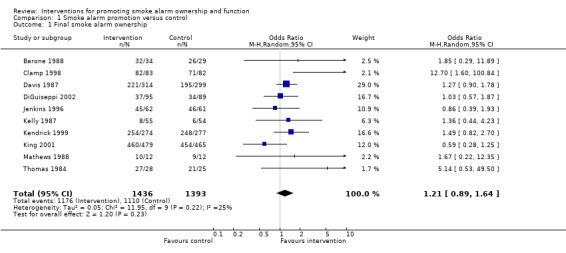
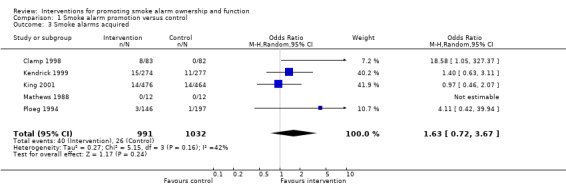
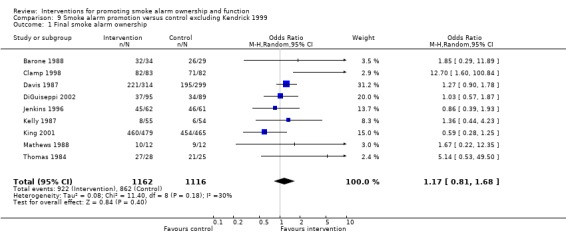
Eleven completed trials collected data on smoke alarm ownership. We were unable to obtain these data from one trial (Williams 1988), which reported "no significant difference" in alarm ownership between study groups. Combining the other ten trials, smoke alarm ownership at follow‐up appeared slightly more likely with intervention, a difference that may have been due to chance (OR = 1.21; 95% CI 0.89 to 1.64). A somewhat larger positive effect on new acquisitions of smoke alarms, with a wide confidence interval, was found among the five trials reporting this outcome (OR = 1.63; 95% CI 0.72 to 3.67).
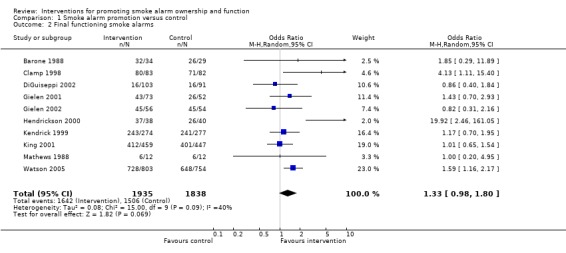
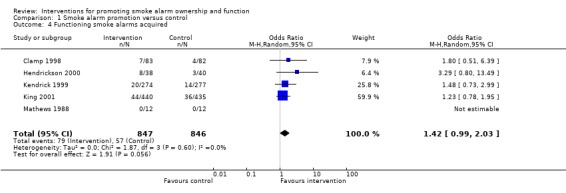
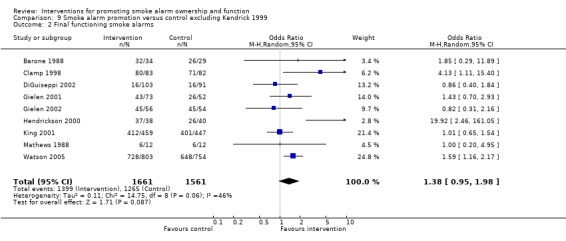
Eleven trials collected data on prevalence of working smoke alarms, and information on whether working alarms were acquired during the trial was available for five of these. Among the ten trials comparing intervention subjects to no intervention controls, there was evidence of a modestly increased likelihood of having installed, functioning alarms with intervention (OR = 1.33; 0.98 to 1.80), possibly due to chance. There was significant heterogeneity (P = 0.09; I2 = 40%), with several trials reporting no benefit or a reduction in ownership with intervention. Similar results were reported for acquisition of functioning alarms, an effect which may have been due to chance (OR = 1.42; 95% CI 0.99 to 2.03).
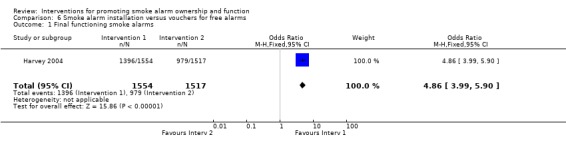
The randomised trial by Harvey 2004 compared installation of free smoke alarms to provision of vouchers for free alarms. This study reported a significantly greater likelihood of having an installed, functioning smoke alarm when the intervention included installation (OR = 4.82; 95% CI 3.97 to 5.85) compared to provision of vouchers. Re‐analysis of these data accounting for cluster randomisation did not substantially change these results.
Subgroup analysis of randomised controlled trials
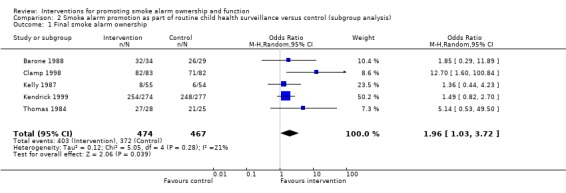
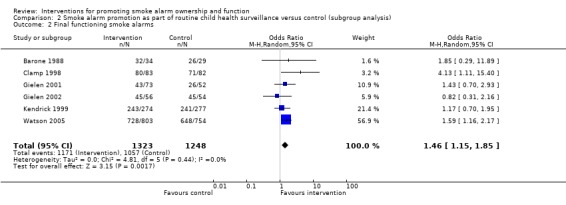
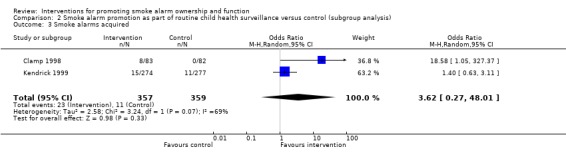
Seven of eight completed trials that evaluated provision of advice promoting smoke alarms as part of routine child health surveillance showed positive effects on smoke alarm ownership, function and acquisition (Barone 1988; Clamp 1998; Gielen 2001; Kelly 1987; Kendrick 1999; Thomas 1984; Watson 2005). Overall, intervention families were significantly more likely than control families to own an alarm (OR = 1.96; 1.03 to 3.72) and to have a functioning alarm (OR = 1.46; 1.15 to 1.85). There were also positive effects on acquiring an alarm (with significant heterogeneity) and acquiring a functioning alarm, but these results were based on only two trials.
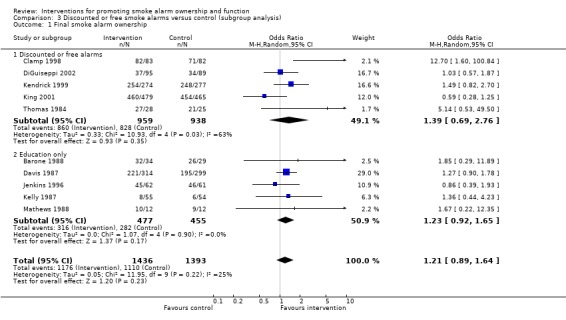
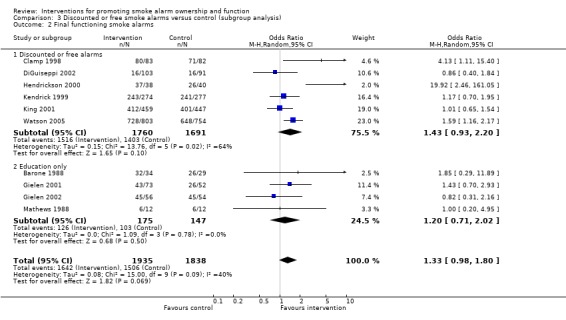
Seven trial interventions combined discounted or free smoke alarms with education (Clamp 1998; DiGuiseppi 2002; Hendrickson 2000; Kendrick 1999; King 2001; Thomas 1984; Watson 2005). For all four outcomes, offering discounted/free alarms and education resulted in modest, beneficial effects compared to no intervention, results possibly due to chance alone. There was significant heterogeneity among the trials reporting smoke alarm ownership (P = 0.03; I2 = 63.4%) and functioning smoke alarms (P = 0.02; I2 = 63.7%), however, with several of these trials reporting little or no benefit from intervention (DiGuiseppi 2002; Kendrick 1999; King 2001). Compared to providing education alone, offering discounted/free alarms showed slightly greater positive effects on smoke alarm acquisition and ownership, although all confidence intervals overlapped. For ownership and acquisition of functioning alarms, results for trials education alone were based on data from only one trial, with wide confidence intervals, making comparisons between the two types of interventions for these outcomes problematic.
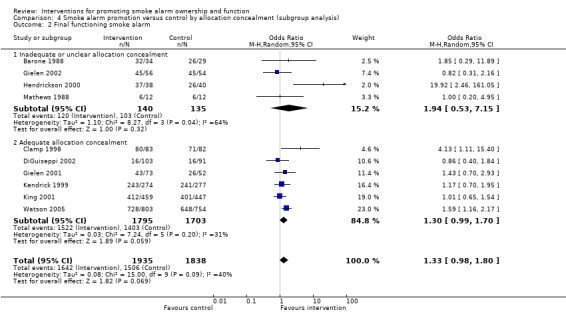
Among five trials with inadequate or unspecified allocation concealment (Barone 1988; Davis 1987; Kelly 1987; Mathews 1988; Thomas 1984), the combined effect of intervention on smoke alarm ownership (OR = 1.33; 95% CI 0.97 to 1.82) was somewhat higher than that in the five trials with adequate concealment (Clamp 1998; DiGuiseppi 2002; Jenkins 1996; Kendrick 1999; King 2001) (OR = 1.12; 95% CI 0.65 to 1.94, with significant heterogeneity, P = 0.05). For functioning smoke alarms, four studies with inadequate or unclear concealment (Barone 1988; Gielen 2002; Hendrickson 2000; Mathews 1988) showed a larger positive effect on functioning smoke alarms than did six studies with adequate concealment (Clamp 1998; DiGuiseppi 2002; Gielen 2001; Kendrick 1999; King 2001; Watson 2005) but the number of trials was small and all differences may have been due to chance.
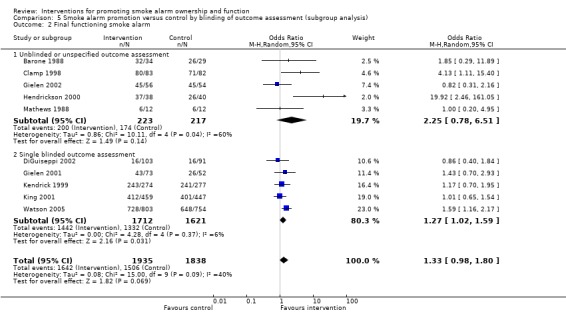
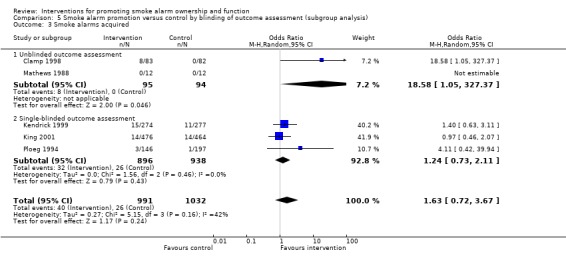
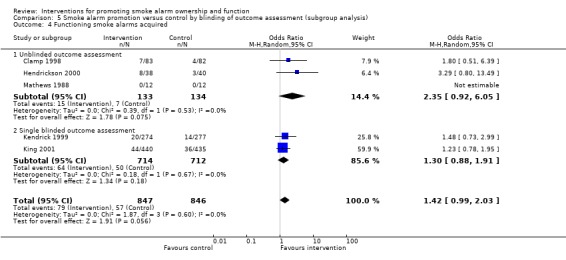
There were seven trials with unblinded (or unspecified) outcomes assessment that compared intervention and control groups and reported outcomes. Effects of intervention were substantially stronger for all outcomes among these trials than were the effects seen among eight trials with blinded outcomes assessment. For example, for smoke alarm ownership, OR = 2.13 (95% CI 0.94 to 4.82) among trials with unblinded outcomes assessment, versus OR = 1.03 (95% CI 0.75 to 1.42) for trials with blinded outcomes assessment. Trials with unblinded assessment showed a much larger positive effect on functioning smoke alarms (OR = 2.25; 95% CI 0.78 to 6.51) than did trials with blinded assessment (OR = 1.27; 95% CI 1.02 to 1.59). For both smoke alarm ownership and functioning smoke alarms, there was more heterogeneity among trials with unblinded (or unspecified) outcomes assessment than among trials with blinded outcomes assessment.
Non‐randomised controlled trials
Six completed non‐randomised trials reported smoke alarm outcomes (Johnston 2000; LeBailly 1990; Miller 1982; Ozanne‐Smith 2002; Schwarz 1993; SCIPP 1989), see Table 12.
Two involved safety advice during routine child health surveillance (LeBailly 1990; Miller 1982), and included free or discounted smoke alarms. Both showed modest beneficial effects of intervention consistent with randomised trials in similar settings. LeBailly 1990 did not see any effect in the group offered injury prevention counselling alone, but the study did not control for significant differences among groups in home ownership, education, and income, all of which are associated with alarm ownership (Roberts 1996). In addition, ownership was greater than 90% in all groups after intervention.
A trial offering education and free smoke alarms in the home (Johnston 2000) showed a modest increase in functioning alarms with intervention (100% versus 95%; adjusted RR = 1.06; 95% CI 1.00 to 1.12). A greater effect was seen on acquisition of functioning alarms (6.0% versus 2.1%; RR = 2.37; 95% CI 0.52 to 10.86) although this effect may have been due to chance. Results were not inconsistent with the widely varying results of home interventions reported among randomised trials.
Two trials of community‐wide injury prevention education reported no effects on alarm ownership (SCIPP 1989) or installation (Ozanne‐Smith 2002). In contrast, installation of free smoke alarms by study staff increased the prevalence of functioning smoke alarms by 19% in one trial (adjusted OR = 7.14; 95% CI 5.0 to 10.0) (Schwarz 1993). In the latter trial, efforts were made to match intervention and control areas on injury rates, socio‐demographic characteristics, and geographic location, to reduce the likelihood of selection bias.
Fires
Two trials that evaluated door‐to‐door smoke alarm give‐away programs found no evidence of a reduction in fire incidence with intervention (DiGuiseppi 2002; Mallonee 1996). Harvey 2004, which compared smoke alarm installation with distribution of vouchers for free alarms, collected data on self‐reported fires but did not report these data.
In a non‐randomised trial comparing a mandatory lecture and video targeting fire safety and prevention to no intervention, fire incidence in intervention (new tenant) households was one fifth that in control (existing tenant) homes, even though, before intervention, fire incidence was higher in new tenancies than in existing ones (McConnell 1996).
Fire‐related injuries
Five randomised trials collected injury outcomes (DiGuiseppi 2002; Kelly 1987; Kendrick 1999; King 2001; Watson 2005) but only DiGuiseppi 2002, a community‐based trial, reported effects of intervention on fire‐related injuries. In addition, five non‐randomised community trials measured injury outcomes (Mallonee 1996, Ozanne‐Smith 2002, Project Burn 1979, Schwarz 1993, SCIPP 1989), of which all but Ozanne‐Smith 2002 reported effects of intervention on burns or fire‐related injuries.
After direct provision (with or without installation) of free alarms, fire‐related injury rates fell significantly in intervention communities but not in control communities in two non‐randomised trials (Mallonee 1996; Schwarz 1993). In one of these trials, however, the intervention area was selected because it had the highest baseline injury rate, hence regression to the mean may explain some of the decline (Mallonee 1996). In contrast, a randomised controlled trial that evaluated a door‐to‐door smoke alarm give‐away programme found no evidence of a reduction in fire‐related injuries, either total injuries (rate ratio 1.3; 95% CI 0.9 to 1.9) or serious injuries (that is, hospitalization or death) alone (rate ratio 1.3; 95% CI 0.7 to 2.3) (DiGuiseppi 2002).
Community injury prevention education produced a modest, non‐significant effect on burn injuries (SCIPP 1989) and there was no apparent benefit from community burn prevention education (Project Burn 1979). Because these trials assessed all types of burns, but excluded smoke inhalation, results are not directly comparable to those from the trials of alarm give‐away programmes, which specifically assessed fire‐related injuries, including smoke inhalation.
Discussion
Principal findings
Evidence from randomised and non‐randomised controlled trials indicates that existing interventions to promote smoke alarms are likely to have at most a modest effect, if any, on smoke alarm ownership, function, or acquisition. The results were sensitive to type of intervention and study quality. In particular, trials with blinded outcome assessment showed little or no apparent effect from such interventions, suggesting that lack of blinding may have positively biased results in some studies. Few trials have evaluated the effect of interventions promoting smoke alarms on fires or fire‐related injuries, and these have yielded inconsistent results.
Clinical counselling and education in the context of routine child health surveillance
Modest, statistically significant beneficial effects on smoke alarm outcomes were seen among trials evaluating counselling and education in the context of routine child health surveillance. Based on our results, the estimated number of families that clinicians would have to counsel to influence one additional family to have an installed, working smoke alarm varies with baseline prevalence in the clinical practice: 14 families if 20% have working alarms, 10 families if 50% have working alarms, and 32 families if 90% own alarms. It should be noted that about half of the trials involving smoke alarm promotion in the context of child health surveillance did not report blinded outcomes assessment, which may have positively biased their results. Although observational studies support a substantial beneficial effect of smoke alarm ownership on fire‐related injuries (DiGuiseppi 1998a; Marshall 1998; Runyan 1992), there were no data from randomised controlled trials on the effects of counselling or education in the clinical setting on fire‐related injuries. Because fire‐related injuries are a leading cause of injury death in childhood, the net benefit of educational or counselling interventions in the clinical setting may be important. However, its effectiveness and cost‐effectiveness in relation to fire injuries prevented has not been adequately evaluated.
Home, school, and community‐based education
Results from randomised controlled trials do not support a strong beneficial effect of home‐ or school‐based education on smoke alarm outcomes, and there were no data from these trials on the effects of education at home or in school on fire‐related injuries. One non‐randomised trial found a beneficial effect on fires of mandatory tenant education on fire safety (McConnell 1996), but this result has not been confirmed in other studies.
No randomised trials have evaluated the effect of mass media and community‐based injury prevention education programmes on smoke alarms or fire‐related injuries, and non‐randomised trials do not support a beneficial effect of such programmes on either smoke alarm ownership or burn incidence. One study author attributed this to attenuation in the numbers who hear, then understand, then act on such information (Project Burn 1979).
Distribution of free or discounted smoke alarms
Providing free or discounted smoke alarms did appear to have a modestly greater effect on smoke alarm ownership and functioning alarms than did education alone, but differences were small and may have been due to chance. Although one might expect that giving an alarm to the family would increase owned and functioning alarms, the lack of an effect might be expected if families or households who are given an alarm lacked interest in or awareness of the value of having a working alarm, or lacked the skills, capacity or tools required to install and maintain it.
Effects of the door‐to‐door distribution of free smoke alarms on fire‐related injuries were examined in two community trials (DiGuiseppi 2002; Mallonee 1996). The trial by Mallonee 1996, which showed a strong beneficial effect on injuries, was not randomised, so selection bias or regression to the mean may have exaggerated its effects. In contrast, in a randomised controlled trial, DiGuiseppi 2002 found no evidence of a beneficial effect on fire‐related injuries. In addition, neither trial demonstrated a reduction in fires. Mallonee 1996 did not evaluate smoke alarm outcomes in the control population, and DiGuiseppi 2002 found no increase in installed and working alarms after intervention.
Installation of free smoke alarms
Harvey 2004 demonstrated a substantially greater beneficial effect on having a working smoke alarm when free alarms were installed compared to providing vouchers for free alarms, suggesting this may be a more effective intervention. Schwarz 1993 also demonstrated a strong beneficial effect on the prevalence of working smoke alarms when free alarms were installed in the homes. This study reported significant reductions in the incidence of fire‐related injuries in the intervention areas. However, Schwarz 1993 was not a randomised trial, hence selection bias or regression to the mean may have exaggerated its effects. In addition, the cost‐effectiveness of installation programmes has not been evaluated.
Exploring heterogeneity
There was statistically significant heterogeneity in the main analysis regarding smoke alarm ownership. Subgroup analyses suggest that some of this heterogeneity may be accounted for by differences in setting, intervention, and study quality. For example, there was no heterogeneity when analyses were restricted to smoke alarm promotion as part of routine child health surveillance, programmes involving education alone, or trials with blinded outcomes assessment. There was little evidence of heterogeneity in analyses involving other outcomes, in particular prevalence of working smoke alarms, suggesting such outcomes may be more consistently measured or more consistently affected by alarm promotion programmes.
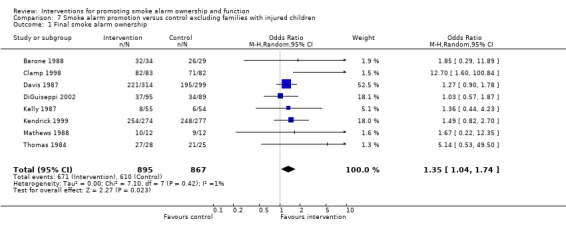
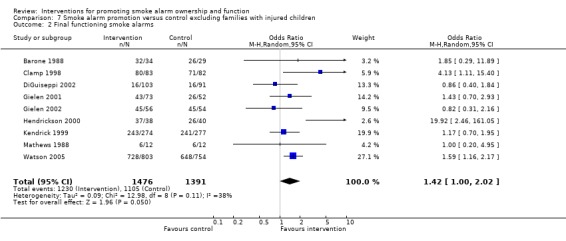
Post hoc examination of results suggests that variations in other factors may also influence results. In the only two trials (Jenkins 1996; King 2001) involving families of injured children, ownership and acquisition were equally high in control and intervention families, so there was no apparent effect of intervention. Having an injured child may lead to safety behaviour changes so large that they obscure any safety education effects. Exclusion of these two trials results in stronger intervention effects on alarm ownership (OR = 1.35; 95% CI 1.04 to 1.74), functioning smoke alarms (OR = 1.42; 95% CI 1.00 to 2.02), and other alarm outcomes, with reduced heterogeneity.
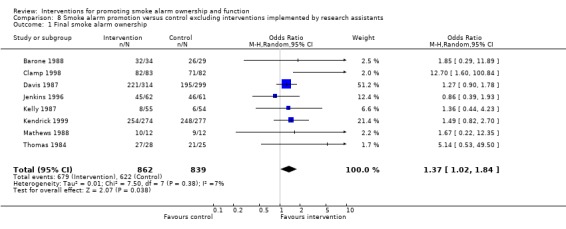
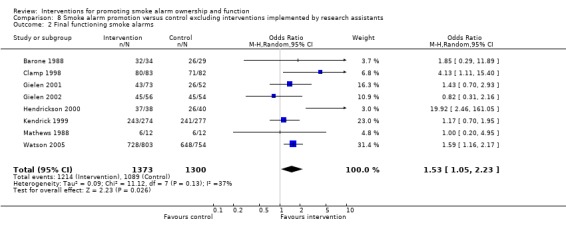
King 2001 and DiGuiseppi 2002 were the only randomised trials in which the intervention was delivered by research assistants rather than a health professional, teacher, community worker, or other trained professional. When these trials are excluded, there is a stronger positive effect of intervention on smoke alarm ownership (OR = 1.37; 95% CI 1.02 to 1.84), functioning smoke alarms (OR=1.53; 95% CI 1.05 to 2.23), and other alarm outcomes, with reduced heterogeneity. The relationship established between the family and their doctor, nurse, teacher or community worker may be an important aspect of effective intervention, a hypothesis supported by the subgroup analysis of routine child health surveillance.
Finally, in one trial (Kendrick 1999) the response rate was notably poor and there was systematic response bias, in that control responders were more likely than intervention responders to live in rental accommodation, have lower socioeconomic status and live in deprived areas (written communication, D Kendrick, University of Nottingham, 2 September 1999). Because these factors are associated with reduced smoke alarm ownership (Roberts 1996), the estimate of the effect of the intervention might have been biased upward. However, results were not materially affected by exclusion of this trial, except that a stronger effect was seen on acquisition of alarms, which may have been due to chance.
Limitations
Publication bias, which threatens the validity of systematic reviews, may arise if research is unpublished or if outcome data are selectively omitted from published reports, which often occurs because the results fail to reach statistical significance (Dickersin 1993; Easterbrook 1991). To minimise this, we searched for unpublished trials and wrote to the authors of any trials in which the methods and intervention were eligible to ask if relevant outcomes were measured. Eight trials were identified after author and organisational contacts, including seven completed trials (Gielen 2001; Harvey 2004; Jenkins 1996; Kendrick 1999; King 2001; LeBailly 1990, Ploeg 1994). Many investigators also provided unpublished data on smoke alarm or injury outcomes (Clamp 1998; Hendrickson 2000; Jenkins 1996; Kendrick 1999; King 2001; Ploeg 1994; Schwarz 1993, SCIPP 1989; Smithson 1998; Watson 2005).
The authors of three potentially eligible trials did not respond, so we were unable to determine their eligibility. We could not locate the text or authors for two further citations. Four of these were known to be non‐randomised, and the fifth (Botruff 1992), as a community intervention, was probably not randomised. Hence, their omission is unlikely to have biased our meta‐analyses.
Authors' conclusions
Implications for practice.
Our review suggests that at best, only modest increases in the prevalence of working smoke alarms result from educational interventions promoting smoke alarms, whether or not free or discounted smoke alarms are also provided. Smoke alarm promotion delivered as part of child health surveillance appears to be effective in increasing the prevalence of owned and functioning smoke alarms, although several studies on which these conclusions are based suffered from methodological weaknesses, and injury outcomes have not been evaluated in these settings. Nevertheless, such interventions may be considered, particularly among high risk populations with a low prevalence of smoke alarms. Existing evidence does not support the implementation of community‐based programmes, including smoke alarm give‐away programmes, mass media, or injury prevention education, to increase the prevalence of installed and functioning smoke alarms or reduce the incidence of fires or fire‐related injuries.
Implications for research.
While community programmes that provide and install smoke alarms appear to increase the prevalence of working alarms and reduce fire‐related injuries, the quality of that evidence is limited and such interventions are likely to be costly. The evidence in support of smoke alarm promotion delivered as part of routine child health surveillance has methodological limitations, and injury outcomes have not been evaluated in these settings. Further trials to evaluate community smoke alarm installation programmes or smoke alarm promotion as part of child health surveillance in primary care should assess their impact on fire‐related injuries, using randomisation, adequate allocation concealment and blinded outcomes assessment, and should incorporate cost‐effectiveness analyses.
What's new
| Date | Event | Description |
|---|---|---|
| 14 December 2009 | Amended | The odds ratios and confidence intervals in the abstract have been corrected, and are now consistent with the analyses. |
History
Protocol first published: Issue 3, 2000 Review first published: Issue 2, 2001
| Date | Event | Description |
|---|---|---|
| 11 July 2008 | Amended | Converted to new review format. |
| 19 September 2007 | New search has been performed | Updated searches for new trials were completed in September 2007. Studies identified after August 2007 are listed as 'studies awaiting assessment'. Five completed randomised controlled trials (four new and one that was previously ongoing) (DiGuiseppi 2002; Gielen 2002; Hendrickson 2000; Watson 2005; Gielen 2001), two non‐randomised controlled trials (one new and one now completed) (Johnston 2000; Harvey 2004), and final reports from two trials already in the review (King 2001; Ozanne‐Smith 2002) are included. The analyses, the results and discussion sections, and the conclusions, have been revised accordingly. |
Acknowledgements
We thank the investigators who responded to our queries, Ian Roberts for advice and for initial review data extraction, Irene Kwan and Frances Bunn for assistance in preparation of the initial review, and Karen Blackhall and Katharine Ker for assistance in the preparation of the updated review.
C DiGuiseppi and C Goss were funded in part by Grant Number R49/CCR811509 from the Centers for Disease Control and Prevention. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.
Appendices
Appendix 1. Search strategy
Injuries Specialised Register; searched 20th September 2007 (((detector* or alarm*) and (fire* or smoke)) or ((fire or fires or burn or burns) and (prevent* or control* or avoid* or stop*))) and (home* or house or resident* or domestic)
MEDLINE 1966 to Sept (week 1) 2007 1. burns/pc [Prevention & Control] 2. fires/pc [Prevention & Control] 3. exp Accident Prevention/ 4. (fire or fires or burn or burns or smoke).ab,ti. 5. 3 and 4 6. ((detector$ or alarm$) adj5 (fire$ or smoke)).ab,ti. 7. ((fire or fires or burn or burns) adj3 (prevent$ or control$ or avoid$ or stop$)).ab,ti. 8. ((home$ or house) adj3 (safety or accident$ or fire or fires)).ab,ti. 9. 1 or 2 or 5 or 6 or 7 or 8 10. exp Protective Devices/ 11. exp Burns/ 12. exp Fires/ 13. (fire or fires or burn or burns).ab,ti. 14. or/11‐13 15. 10 and 14 16. 9 or 15 17. exp "Wounds and Injuries"/ 18. 14 and 17 19. exp Smoke Inhalation Injury/ 20. 18 or 19 21. 16 and 20 22. clinical trial.pt. 23. randomized.ti,ab. 24. randomised.ti,ab. 25. placebo.ti,ab. 26. program$.ti,ab. 27. randomly.ti,ab. 28. (trial or study).ti,ab. 29. groups.ti,ab. 30. or/22‐29 31. exp animals/ 32. exp humans/ 33. 31 not (31 and 32) 34. 30 not 33 35. 16 and 20 and 34 CENTRAL 2007, issue 3 #1 MeSH descriptor Burns explode all trees with qualifier: PC #2 MeSH descriptor Fires explode all trees with qualifier: PC #3 MeSH descriptor Accident Prevention explode all trees #4 fire or fires or burn or burns or smoke #5 (#3 AND #4) #6 (detector* or alarm*) near5 (fire* or smoke) #7 (fire or fires or burn or burns) near3 (prevent* or control* or avoid* or stop*) #8 (home* or house) near3 (safety or accident* or fire or fires) #9 (#1 OR #2 OR #5 OR #6 OR #7 OR #8) #10 MeSH descriptor Protective Devices explode all trees #11 MeSH descriptor Burns explode all trees #12 MeSH descriptor Fires explode all trees #13 fire or fires or burn or burns #14 (#11 OR #12 OR #13) #15 (#10 AND #14) #16 (#9 OR #15) #17 MeSH descriptor Wounds and Injuries explode all trees #18 (#14 AND #17) #19 MeSH descriptor Smoke Inhalation Injury explode all trees #20 (#18 OR #19) #21 #6 OR (#16 AND #20), from 2003 to 2007
EMBASE 1980 to Sept (week 37) 2007 1. exp Burn/pc [Prevention] 2. exp Fire protection/ 3. exp Accident Prevention/ 4. (fire or fires or burn or burns or smoke).ab,ti. 5. 3 and 4 6. ((detector$ or alarm$) adj5 (fire$ or smoke)).ab,ti. 7. ((fire or fires or burn or burns) adj3 (prevent$ or control$ or avoid$ or stop$)).ab,ti. 8. ((home$ or house) adj3 (safety or accident$ or fire or fires)).ab,ti. 9. 1 or 2 or 5 or 6 or 7 or 8 10. exp Protective Devices/ 11. exp Burn/ 12. exp Fire/ 13. (fire or fires or burn or burns).ab,ti. 14. or/11‐13 15. 10 and 14 16. 9 or 15 17. exp "Wounds and Injuries"/ 18. 14 and 17 19. exp Smoke Inhalation Injury/ 20. 18 or 19 21. 16 and 20 22. exp clinical study/ 23. exp Clinical Trial/ 24. randomized.ab,ti. 25. randomised.ab,ti. 26. placebo.ti,ab. 27. randomly.ab,ti. 28. (trial or study or program$).ab,ti. 29. groups.ti,ab. 30. or/22‐29 31. exp animal/ 32. exp human/ 33. 31 not (31 and 32) 34. 30 not 33 35. (6 or 21) and 34
National Research Register 2007, issue 3 #1 (detector* or alarm*) and (fire* or smoke) #2 (fire or fires or burn or burns) and (prevent* or control* or avoid* or stop*) #3 home* or house or resident* or domestic #4 #1 or #2 #5 #3 and #4
Zetoc; (searched 24th Sept 2007) Fire alarm* trial* OR Fire alarm* program* OR Smoke alarm* trial* OR Smoke alarm* program* OR Fire detector* trial* OR Fire detector* program* OR Smoke detector* trial* OR Smoke detector* program*
IBSS to 2007/08; searched 24th September 2007 #1 (fire or fires or burn or burns) near (prevent* or control* or avoid* or stop*) #2 (detector* or alarm*) near (fire* or smoke) #3 #1 or #2
All other searches were carried out using terms included in these strategies and adapted as appropriate to the specifications of each database.
Data and analyses
Comparison 1. Smoke alarm promotion versus control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 10 | 2829 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.89, 1.64] |
| 2 Final functioning smoke alarms | 10 | 3773 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [0.98, 1.80] |
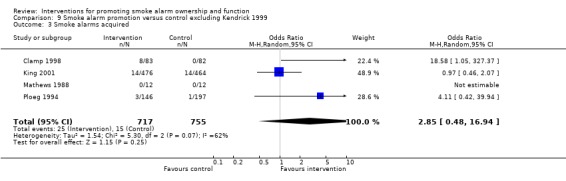
| 3 Smoke alarms acquired | 5 | 2023 | Odds Ratio (M‐H, Random, 95% CI) | 1.63 [0.72, 3.67] |
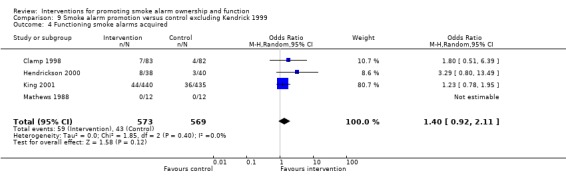
| 4 Functioning smoke alarms acquired | 5 | 1693 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.99, 2.03] |
1.1. Analysis.
Comparison 1 Smoke alarm promotion versus control, Outcome 1 Final smoke alarm ownership.
1.2. Analysis.
Comparison 1 Smoke alarm promotion versus control, Outcome 2 Final functioning smoke alarms.
1.3. Analysis.
Comparison 1 Smoke alarm promotion versus control, Outcome 3 Smoke alarms acquired.
1.4. Analysis.
Comparison 1 Smoke alarm promotion versus control, Outcome 4 Functioning smoke alarms acquired.
Comparison 2. Smoke alarm promotion as part of routine child health surveillance versus control (subgroup analysis).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 5 | 941 | Odds Ratio (M‐H, Random, 95% CI) | 1.96 [1.03, 3.72] |
| 2 Final functioning smoke alarms | 6 | 2571 | Odds Ratio (M‐H, Random, 95% CI) | 1.46 [1.15, 1.85] |
| 3 Smoke alarms acquired | 2 | 716 | Odds Ratio (M‐H, Random, 95% CI) | 3.62 [0.27, 48.01] |
| 4 Functioning smoke alarms acquired | 2 | 716 | Odds Ratio (M‐H, Random, 95% CI) | 1.55 [0.84, 2.87] |
2.1. Analysis.
Comparison 2 Smoke alarm promotion as part of routine child health surveillance versus control (subgroup analysis), Outcome 1 Final smoke alarm ownership.
2.2. Analysis.
Comparison 2 Smoke alarm promotion as part of routine child health surveillance versus control (subgroup analysis), Outcome 2 Final functioning smoke alarms.
2.3. Analysis.
Comparison 2 Smoke alarm promotion as part of routine child health surveillance versus control (subgroup analysis), Outcome 3 Smoke alarms acquired.
2.4. Analysis.

Comparison 2 Smoke alarm promotion as part of routine child health surveillance versus control (subgroup analysis), Outcome 4 Functioning smoke alarms acquired.
Comparison 3. Discounted or free smoke alarms versus control (subgroup analysis).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 10 | 2829 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.89, 1.64] |
| 1.1 Discounted or free alarms | 5 | 1897 | Odds Ratio (M‐H, Random, 95% CI) | 1.39 [0.69, 2.76] |
| 1.2 Education only | 5 | 932 | Odds Ratio (M‐H, Random, 95% CI) | 1.23 [0.92, 1.65] |
| 2 Final functioning smoke alarms | 10 | 3773 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [0.98, 1.80] |
| 2.1 Discounted or free alarms | 6 | 3451 | Odds Ratio (M‐H, Random, 95% CI) | 1.43 [0.93, 2.20] |
| 2.2 Education only | 4 | 322 | Odds Ratio (M‐H, Random, 95% CI) | 1.20 [0.71, 2.02] |
| 3 Smoke alarms acquired | 5 | 2023 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.56 [0.95, 2.57] |
| 3.1 Discounted or free alarms | 3 | 1656 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.48 [0.89, 2.46] |
| 3.2 Education only | 2 | 367 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.11 [0.42, 39.94] |
| 4 Functioning smoke alarms acquired | 5 | 1693 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.99, 2.03] |
| 4.1 Discounted or free alarms | 4 | 1669 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.99, 2.03] |
| 4.2 Education only | 1 | 24 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
3.1. Analysis.
Comparison 3 Discounted or free smoke alarms versus control (subgroup analysis), Outcome 1 Final smoke alarm ownership.
3.2. Analysis.
Comparison 3 Discounted or free smoke alarms versus control (subgroup analysis), Outcome 2 Final functioning smoke alarms.
3.3. Analysis.

Comparison 3 Discounted or free smoke alarms versus control (subgroup analysis), Outcome 3 Smoke alarms acquired.
3.4. Analysis.

Comparison 3 Discounted or free smoke alarms versus control (subgroup analysis), Outcome 4 Functioning smoke alarms acquired.
Comparison 4. Smoke alarm promotion versus control by allocation concealment (subgroup analysis).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 10 | 2829 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.89, 1.64] |
| 1.1 Inadequate or unclear allocation concealment | 5 | 862 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [0.97, 1.82] |
| 1.2 Adequate allocation concealment | 5 | 1967 | Odds Ratio (M‐H, Random, 95% CI) | 1.12 [0.65, 1.94] |
| 2 Final functioning smoke alarm | 10 | 3773 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [0.98, 1.80] |
| 2.1 Inadequate or unclear allocation concealment | 4 | 275 | Odds Ratio (M‐H, Random, 95% CI) | 1.94 [0.53, 7.15] |
| 2.2 Adequate allocation concealment | 6 | 3498 | Odds Ratio (M‐H, Random, 95% CI) | 1.30 [0.99, 1.70] |
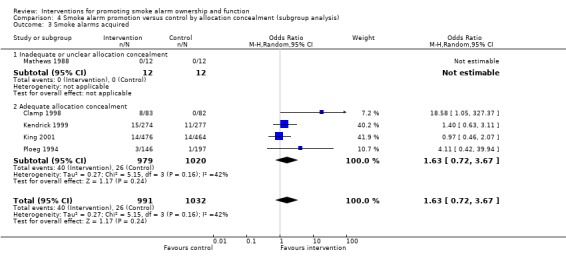
| 3 Smoke alarms acquired | 5 | 2023 | Odds Ratio (M‐H, Random, 95% CI) | 1.63 [0.72, 3.67] |
| 3.1 Inadequate or unclear allocation concealment | 1 | 24 | Odds Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 3.2 Adequate allocation concealment | 4 | 1999 | Odds Ratio (M‐H, Random, 95% CI) | 1.63 [0.72, 3.67] |
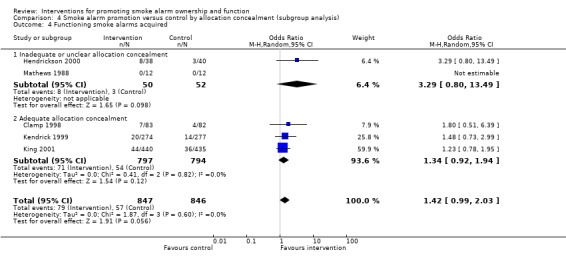
| 4 Functioning smoke alarms acquired | 5 | 1693 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.99, 2.03] |
| 4.1 Inadequate or unclear allocation concealment | 2 | 102 | Odds Ratio (M‐H, Random, 95% CI) | 3.29 [0.80, 13.49] |
| 4.2 Adequate allocation concealment | 3 | 1591 | Odds Ratio (M‐H, Random, 95% CI) | 1.34 [0.92, 1.94] |
4.1. Analysis.

Comparison 4 Smoke alarm promotion versus control by allocation concealment (subgroup analysis), Outcome 1 Final smoke alarm ownership.
4.2. Analysis.
Comparison 4 Smoke alarm promotion versus control by allocation concealment (subgroup analysis), Outcome 2 Final functioning smoke alarm.
4.3. Analysis.
Comparison 4 Smoke alarm promotion versus control by allocation concealment (subgroup analysis), Outcome 3 Smoke alarms acquired.
4.4. Analysis.
Comparison 4 Smoke alarm promotion versus control by allocation concealment (subgroup analysis), Outcome 4 Functioning smoke alarms acquired.
Comparison 5. Smoke alarm promotion versus control by blinding of outcome assessment (subgroup analysis).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 10 | 2829 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.89, 1.64] |
| 1.1 Unblinded outcome assessment | 5 | 918 | Odds Ratio (M‐H, Random, 95% CI) | 2.13 [0.94, 4.82] |
| 1.2 Single blinded outcome assessment | 5 | 1911 | Odds Ratio (M‐H, Random, 95% CI) | 1.03 [0.75, 1.42] |
| 2 Final functioning smoke alarm | 10 | 3773 | Odds Ratio (M‐H, Random, 95% CI) | 1.33 [0.98, 1.80] |
| 2.1 Unblinded or unspecified outcome assessment | 5 | 440 | Odds Ratio (M‐H, Random, 95% CI) | 2.25 [0.78, 6.51] |
| 2.2 Single blinded outcome assessment | 5 | 3333 | Odds Ratio (M‐H, Random, 95% CI) | 1.27 [1.02, 1.59] |
| 3 Smoke alarms acquired | 5 | 2023 | Odds Ratio (M‐H, Random, 95% CI) | 1.63 [0.72, 3.67] |
| 3.1 Unblinded outcome assessment | 2 | 189 | Odds Ratio (M‐H, Random, 95% CI) | 18.58 [1.05, 327.37] |
| 3.2 Single‐blinded outcome assessment | 3 | 1834 | Odds Ratio (M‐H, Random, 95% CI) | 1.24 [0.73, 2.11] |
| 4 Functioning smoke alarms acquired | 5 | 1693 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.99, 2.03] |
| 4.1 Unblinded outcome assessment | 3 | 267 | Odds Ratio (M‐H, Random, 95% CI) | 2.35 [0.92, 6.05] |
| 4.2 Single blinded outcome assessment | 2 | 1426 | Odds Ratio (M‐H, Random, 95% CI) | 1.30 [0.88, 1.91] |
5.1. Analysis.

Comparison 5 Smoke alarm promotion versus control by blinding of outcome assessment (subgroup analysis), Outcome 1 Final smoke alarm ownership.
5.2. Analysis.
Comparison 5 Smoke alarm promotion versus control by blinding of outcome assessment (subgroup analysis), Outcome 2 Final functioning smoke alarm.
5.3. Analysis.
Comparison 5 Smoke alarm promotion versus control by blinding of outcome assessment (subgroup analysis), Outcome 3 Smoke alarms acquired.
5.4. Analysis.
Comparison 5 Smoke alarm promotion versus control by blinding of outcome assessment (subgroup analysis), Outcome 4 Functioning smoke alarms acquired.
Comparison 6. Smoke alarm installation versus vouchers for free alarms.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final functioning smoke alarms | 1 | 3071 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.86 [3.99, 5.90] |
6.1. Analysis.
Comparison 6 Smoke alarm installation versus vouchers for free alarms, Outcome 1 Final functioning smoke alarms.
Comparison 7. Smoke alarm promotion versus control excluding families with injured children.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 8 | 1762 | Odds Ratio (M‐H, Random, 95% CI) | 1.35 [1.04, 1.74] |
| 2 Final functioning smoke alarms | 9 | 2867 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [1.00, 2.02] |
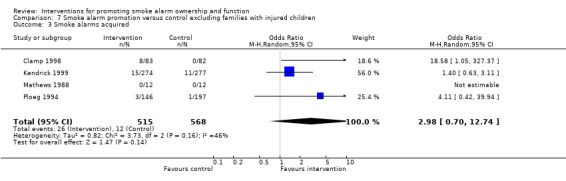
| 3 Smoke alarms acquired | 4 | 1083 | Odds Ratio (M‐H, Random, 95% CI) | 2.98 [0.70, 12.74] |
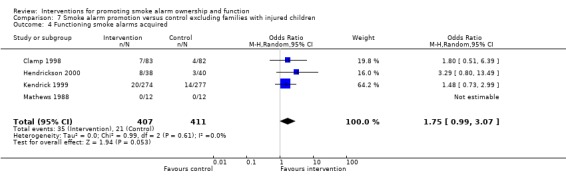
| 4 Functioning smoke alarms acquired | 4 | 818 | Odds Ratio (M‐H, Random, 95% CI) | 1.75 [0.99, 3.07] |
7.1. Analysis.
Comparison 7 Smoke alarm promotion versus control excluding families with injured children, Outcome 1 Final smoke alarm ownership.
7.2. Analysis.
Comparison 7 Smoke alarm promotion versus control excluding families with injured children, Outcome 2 Final functioning smoke alarms.
7.3. Analysis.
Comparison 7 Smoke alarm promotion versus control excluding families with injured children, Outcome 3 Smoke alarms acquired.
7.4. Analysis.
Comparison 7 Smoke alarm promotion versus control excluding families with injured children, Outcome 4 Functioning smoke alarms acquired.
Comparison 8. Smoke alarm promotion versus control excluding interventions implemented by research assistants.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 8 | 1701 | Odds Ratio (M‐H, Random, 95% CI) | 1.37 [1.02, 1.84] |
| 2 Final functioning smoke alarms | 8 | 2673 | Odds Ratio (M‐H, Random, 95% CI) | 1.53 [1.05, 2.23] |
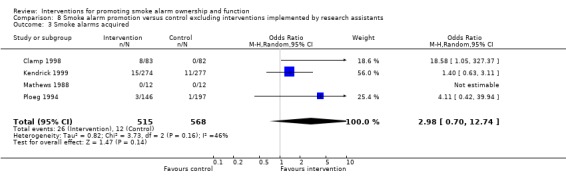
| 3 Smoke alarms acquired | 4 | 1083 | Odds Ratio (M‐H, Random, 95% CI) | 2.98 [0.70, 12.74] |
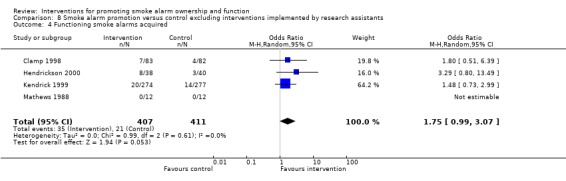
| 4 Functioning smoke alarms acquired | 4 | 818 | Odds Ratio (M‐H, Random, 95% CI) | 1.75 [0.99, 3.07] |
8.1. Analysis.
Comparison 8 Smoke alarm promotion versus control excluding interventions implemented by research assistants, Outcome 1 Final smoke alarm ownership.
8.2. Analysis.
Comparison 8 Smoke alarm promotion versus control excluding interventions implemented by research assistants, Outcome 2 Final functioning smoke alarms.
8.3. Analysis.
Comparison 8 Smoke alarm promotion versus control excluding interventions implemented by research assistants, Outcome 3 Smoke alarms acquired.
8.4. Analysis.
Comparison 8 Smoke alarm promotion versus control excluding interventions implemented by research assistants, Outcome 4 Functioning smoke alarms acquired.
Comparison 9. Smoke alarm promotion versus control excluding Kendrick 1999.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 9 | 2278 | Odds Ratio (M‐H, Random, 95% CI) | 1.17 [0.81, 1.68] |
| 2 Final functioning smoke alarms | 9 | 3222 | Odds Ratio (M‐H, Random, 95% CI) | 1.38 [0.95, 1.98] |
| 3 Smoke alarms acquired | 4 | 1472 | Odds Ratio (M‐H, Random, 95% CI) | 2.85 [0.48, 16.94] |
| 4 Functioning smoke alarms acquired | 4 | 1142 | Odds Ratio (M‐H, Random, 95% CI) | 1.40 [0.92, 2.11] |
9.1. Analysis.
Comparison 9 Smoke alarm promotion versus control excluding Kendrick 1999, Outcome 1 Final smoke alarm ownership.
9.2. Analysis.
Comparison 9 Smoke alarm promotion versus control excluding Kendrick 1999, Outcome 2 Final functioning smoke alarms.
9.3. Analysis.
Comparison 9 Smoke alarm promotion versus control excluding Kendrick 1999, Outcome 3 Smoke alarms acquired.
9.4. Analysis.
Comparison 9 Smoke alarm promotion versus control excluding Kendrick 1999, Outcome 4 Functioning smoke alarms acquired.
Comparison 10. Smoke alarm promotion versus control without cluster adjustment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Final smoke alarm ownership | 10 | 3316 | Odds Ratio (M‐H, Random, 95% CI) | 1.22 [0.91, 1.63] |
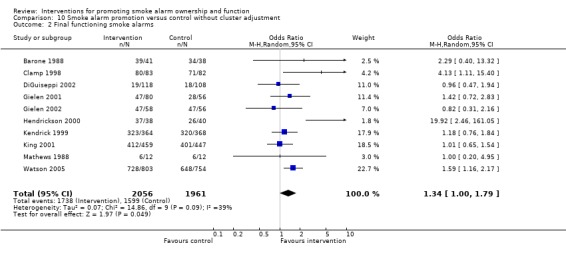
| 2 Final functioning smoke alarms | 10 | 4017 | Odds Ratio (M‐H, Random, 95% CI) | 1.34 [1.00, 1.79] |
| 3 Smoke alarms acquired | 5 | 2204 | Odds Ratio (M‐H, Random, 95% CI) | 1.57 [0.73, 3.38] |
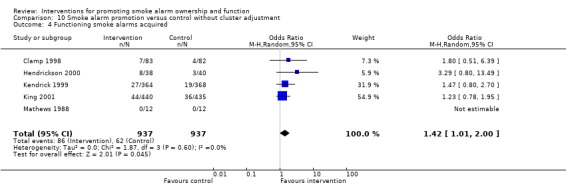
| 4 Functioning smoke alarms acquired | 5 | 1874 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [1.01, 2.00] |
10.1. Analysis.

Comparison 10 Smoke alarm promotion versus control without cluster adjustment, Outcome 1 Final smoke alarm ownership.
10.2. Analysis.
Comparison 10 Smoke alarm promotion versus control without cluster adjustment, Outcome 2 Final functioning smoke alarms.
10.3. Analysis.

Comparison 10 Smoke alarm promotion versus control without cluster adjustment, Outcome 3 Smoke alarms acquired.
10.4. Analysis.
Comparison 10 Smoke alarm promotion versus control without cluster adjustment, Outcome 4 Functioning smoke alarms acquired.
Comparison 11. Smoke alarm promotion versus control using greater ICC for cluster adjustment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
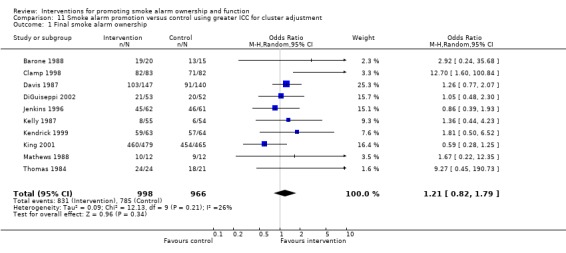
| 1 Final smoke alarm ownership | 10 | 1964 | Odds Ratio (M‐H, Random, 95% CI) | 1.21 [0.82, 1.79] |
| 2 Final functioning smoke alarms | 10 | 3217 | Odds Ratio (M‐H, Random, 95% CI) | 1.38 [0.97, 1.95] |
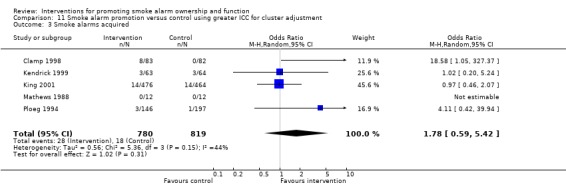
| 3 Smoke alarms acquired | 5 | 1599 | Odds Ratio (M‐H, Random, 95% CI) | 1.78 [0.59, 5.42] |
| 4 Functioning smoke alarms acquired | 5 | 1269 | Odds Ratio (M‐H, Random, 95% CI) | 1.42 [0.95, 2.12] |
11.1. Analysis.
Comparison 11 Smoke alarm promotion versus control using greater ICC for cluster adjustment, Outcome 1 Final smoke alarm ownership.
11.2. Analysis.

Comparison 11 Smoke alarm promotion versus control using greater ICC for cluster adjustment, Outcome 2 Final functioning smoke alarms.
11.3. Analysis.
Comparison 11 Smoke alarm promotion versus control using greater ICC for cluster adjustment, Outcome 3 Smoke alarms acquired.
11.4. Analysis.

Comparison 11 Smoke alarm promotion versus control using greater ICC for cluster adjustment, Outcome 4 Functioning smoke alarms acquired.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Barone 1988.
| Methods | Cluster randomised controlled trial. Allocation by coin toss within paired classes. Outcomes assessment not blinded. | |
| Participants | 5 parenting classes (108 parents of toddlers). | |
| Interventions | I: Slides, handouts on burn prevention; motor vehicle safety education and video; bath water thermometer; hot water gauge. C: Usual safety education. | |
| Outcomes | Home inspection 6 months after class: 1) Final alarm ownership. 2) Final functioning alarms. | |
| Notes | 27% of parents attending randomly allocated classes did not enrol in trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Clamp 1998.
| Methods | Randomised controlled trial. Allocation by random numbers table numbered 1‐165, the first 83 numbers on the list were allocated to the intervention group; allocation by researcher blinded to number given to each family at time of allocation. Outcome assessment not blinded. | |
| Participants | 165 families of children <5 years on GP list. | |
| Interventions | I: Safety advice by health visitors and practice nurses, leaflets, discount safety devices for low income families. C: Usual care. | |
| Outcomes | Telephone / mail survey 6 weeks after visit: 1) Final alarm ownership. 2) Final functioning alarms. 3) Alarms acquired. 4) Functioning alarms acquired. | |
| Notes | Unpublished data provided by investigators. No loss to follow‐up. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Davis 1987.
| Methods | Cluster randomised controlled trial. Allocation methods not stated. Outcomes assessment not blinded. | |
| Participants | 41 Grade 4‐6 classes (861 children). | |
| Interventions | I: Six 1‐hour fire safety lessons with workbook, demonstrations, teacher training, materials, take‐home materials for parents. C: Usual lessons. | |
| Outcomes | In‐school survey immediately after last class: Final alarm ownership. | |
| Notes | Loss to follow‐up: I: 1% of children; C: 0% of children. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
DiGuiseppi 2002.
| Methods | Cluster randomised controlled trial. Allocation by independent statistician using computer‐generated random numbers. Blinded outcome assessment. | |
| Participants | 40 socio‐economically deprived electoral wards in central London (˜147,444 households). | |
| Interventions | I: Door‐to‐door alarm give‐away, fire prevention brochures, limited alarm installation; reminder postcards to change battery at 1 year. C: No intervention. | |
| Outcomes | Population fire & fire‐related injury surveillance 13 months before to 24 months after program. Home inspection 12‐18 months after program in sample of council homes: 1) Final alarm ownership. 2) Final functioning alarms. | |
| Notes | No loss to follow‐up. Response rate for home inspection: I: 75%; C: 70%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Gielen 2001.
| Methods | Cluster randomised controlled trial. Allocation by random numbers table by independent person (per investigator). Blinded outcomes assessment (per investigator). | |
| Participants | 31 doctors in training (196 parents of children aged 0‐6 mo). | |
| Interventions | I: 5 hours of special training in injury prevention counseling. C: Usual training. | |
| Outcomes | Home inspection, interview after 12 months, health surveillance visit: Final functioning alarms. | |
| Notes | Loss to follow‐up: I: 33% of families; C: 26% of families. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Gielen 2002.
| Methods | Cluster randomised controlled trial. Allocation by project director using random numbers table. Blinding not specified. | |
| Participants | 39 doctors in training (187 parents of children aged 0‐6 months). | |
| Interventions | I: Offer to parents of home safety visit by community health worker for hazard assessment and safety education, and referral to safety center; 5 hours of special training for doctors in injury prevention counseling. C: Referral of parents to safety center; 5 hours of special training for doctors in injury prevention counseling. | |
| Outcomes | Home inspection, interview after 12 months health surveillance visit: Final functioning alarms. | |
| Notes | Loss to follow‐up: I: 34% of families; C: 35% of families. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Harvey 2004.
| Methods | Cluster randomised controlled trial. Allocation method & blinding of outcome assessment not specified. | |
| Participants | Areas, counties or census tracts in 5 US states (4455 households with resident <5 or >64, without any working smoke alarms, located in high‐risk area [based on high prevalence of fire deaths, non functioning alarms, low income, or rental units]). | |
| Interventions | I1: Installation of smoke alarm(s) by study staff, fire safety education. I2: Voucher for free smoke alarm(s), fire safety education. | |
| Outcomes | Home visit & inspection 6‐12 months after visit: 1) Self‐reported fires. 2) Final functioning alarms. | |
| Notes | Loss to follow‐up: I1: 28%; I2: 31%. Fire rates not reported by investigator. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Hendrickson 2000.
| Methods | Randomised controlled trial. Allocation by coin toss. Unblinded outcomes assessment. | |
| Participants | 82 low‐income mothers (87% Hispanic) with children aged 10‐47 months. | |
| Interventions | I: Home visit, with safety teaching, brochure, free smoke alarms, involving mother in installation and maintenance of alarms. C: No intervention. | |
| Outcomes | Home inspection 1 month after intervention: 1) Final functioning alarms. 2) Functioning alarms acquired. | |
| Notes | Loss to follow‐up: I: 7.3%; C: 2.0%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Jenkins 1996.
| Methods | Randomised controlled trial. Allocation by random numbers table read by independent person. Outcomes assessment blinded. | |
| Participants | 141 families of children <17 years in burn unit. | |
| Interventions | I: Discharge teaching book about burn care and prevention; routine discharge teaching. C: Routine discharge teaching. | |
| Outcomes | Interview in clinic at first follow‐up visit: Final alarm ownership. | |
| Notes | Unpublished data provided by investigators. Loss to follow‐up 13%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Johnston 2000.
| Methods | Non randomised controlled trial. Two groups assigned by coin toss. Unblinded outcome assessment. | |
| Participants | 418 families of children aged 4‐5 yrs enrolled in 9 government funded preschool enrichment centers for high‐risk children. | |
| Interventions | I: Written safety information at home visit; alarms or batteries if needed, other safety devices. C: Written safety information at home visit. | |
| Outcomes | Home inspection 3 months after visit: 1) Final functioning alarms. 2) Functioning alarms acquired. | |
| Notes | Loss to follow‐up: I: 17.5%; C: 6.9%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Kelly 1987.
| Methods | Randomised controlled trial. Allocation methods not stated. Outcomes assessment blinded. | |
| Participants | 171 parents of children aged 6 months seen for child health surveillance. | |
| Interventions | I: Developmentally oriented child safety education, hazard assessment, and handout, at 6, 9, 12 month visits. C: Usual well child care. | |
| Outcomes | Home inspection, medical chart review 1 month after 12‐month visit: 1) Final smoke alarm ownership. 2) Total injuries. | |
| Notes | Loss to follow‐up: I: 35%; C: 37%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Kendrick 1999.
| Methods | Cluster randomised controlled trial. Allocation by random numbers table by investigator blind to identity of practices. Outcomes assessment blinded. | |
| Participants | 36 general practices (2052 registered children aged 3‐13 months). | |
| Interventions | I: Safety advice by health visitors and practice nurses, safety literature, discount safety devices for low income families, home safety checks and first aid training by health visitors. C: Usual care. | |
| Outcomes | Medical record review; postal survey at 25 month follow‐up: 1) Smoke alarms acquired. 2) Functioning smoke alarms acquired. 3) Final smoke alarm ownership. 4) Final functioning smoke alarms. 5) Medically attended injuries. | |
| Notes | Unpublished data provided by investigators. Loss to follow‐up: For record review: 0%; for survey of safety practices, I: 67%; C: 64%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
King 2001.
| Methods | Randomised controlled trial. Allocation by opening sealed, serially numbered, opaque envelopes. Outcomes assessment blinded. | |
| Participants | 1172 families of children aged <8 yrs presenting to ED with a targeted injury. | |
| Interventions | I: Home safety inspection, education, safety device coupons; telephone reinforcement at 4 and 8 months; follow‐up letter. C: Home safety inspection and safety pamphlet only. | |
| Outcomes | Survey and home inspection at 1 year follow‐up: 1) Final alarm ownership. 2) Final functioning alarms. 3) Smoke alarms acquired. 4) Functioning smoke alarms acquired. 5) Self‐reported injury visits to physician. | |
| Notes | Unpublished data provided by investigators. Loss to follow‐up: I: 20%; C: 18%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
LeBailly 1990.
| Methods | Non‐randomised controlled trial. Allocation sequentially in groups of ˜100. Unblinded outcomes assessment. | |
| Participants | 407 families with children aged <5 years seen for routine health surveillance (groups differed on socio‐ economic status, home ownership). | |
| Interventions | I1: Free alarm and other safety devices. I2: Free alarm and other safety devices, injury prevention counseling. I3: Injury prevention counseling. C: No intervention. | |
| Outcomes | Home interviews and inspections 9 months after intervention: Final alarm ownership. | |
| Notes | Response rate: ˜75%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Mallonee 1996.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: City area with highest risk of fire‐related hospitalisations and deaths. C: Rest of city (lower risk of fire injury, death). | |
| Interventions | I: Door‐to‐door alarm give‐away, fire prevention brochures, limited alarm installation. C: No intervention. | |
| Outcomes | Population injury surveillance 2.5 years before to 4 years after program, 1) Fires. 2) Fire‐related injuries. 3) Final functioning alarms in intervention group only. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Mathews 1988.
| Methods | Quasi‐randomised controlled trial. First eight participants allocated by odd‐even, rest assigned using open random numbers table. Blinding not stated. | |
| Participants | 26 mothers of toddlers recruited from clinics, day care centres. | |
| Interventions | I: Home safety inspection, video, handouts, modelling re: safety and managing dangerous child behaviour; hot water thermometers; choke tube. C: Home visit with video, hand‐outs, modelling on language stimulation. | |
| Outcomes | Home inspection 2 weeks after home visit: 1) Final alarm ownership. 2) Final functioning alarms. 3) Smoke alarms acquired. 4) Functioning alarms acquired. | |
| Notes | Loss to follow‐up: 8%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
McConnell 1996.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: All 2350 new residents of subsidised housing. C: All existing residents (lower baseline fire risk, similar socio‐demo‐graphics). | |
| Interventions | I: 35‐minute mandatory lecture and video on fire safety and prevention; reminder card. C: No intervention. | |
| Outcomes | Population surveillance during 15 month study period: Fires. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Miller 1982.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: 120 consecutive parents of children seen for routine health surveillance in middle class suburban practice. C: Preceding 120 consecutive, similar parents. | |
| Interventions | I: Pamphlet, brief education, discount alarms, usual care. C: Usual care. | |
| Outcomes | Home inspection 4‐6 weeks after intervention: 1) Final alarm ownership. 2) Final functioning alarms. | |
| Notes | Response rate to inspection: I: 90%, C: 88%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Ozanne‐Smith 2002.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: Municipality. C: Demographically similar municipality (with higher baseline injury hospitalisation rate). | |
| Interventions | I: 6‐year community injury prevention program: mass media, education, training, promotion and action for hazard reduction and environmental change. C: No intervention. | |
| Outcomes | Population injury surveillance; telephone survey pre‐, interim, and post‐intervention of 250 randomly selected households in each group: 1) Injuries. 2) Final alarm ownership. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Ploeg 1994.
| Methods | Randomised controlled trial. Allocation by random numbers table read by independent person. Outcome assessment blinded. | |
| Participants | 359 public health clients aged 65+ years. | |
| Interventions | I: Home safety inspection, safety promotion. C: Home visit for influenza vaccine promotion. | |
| Outcomes | Telephone survey 2‐3 months after home visit: Smoke alarms acquired. | |
| Notes | Unpublished data provided by investigators. Loss to follow‐up: I: 1%; C: 7%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Project Burn 1979.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: 3 cities in east of state. C: 2 cities in west of state (with lower baseline burn incidence). | |
| Interventions | I1: Mass media. I2: I1 + school program. I3: I1+ community outreach. C: No intervention. | |
| Outcomes | Population injury surveillance 4 years before to 12 months after. Telephone surveys. Incidence of burns seen in emergency dept. | |
| Notes | Smoke alarm ownership not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Schwarz 1993.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: 5 contiguous census tracts [3004 households (51%) participated]. C: 4 bordering, contiguous census tracts (similar socio‐demographics, baseline injury rates). | |
| Interventions | I: Free alarms installed; home safety inspection, education, modification; community education. C: No intervention. | |
| Outcomes | Population injury surveillance 2 years before to 1 year after program; inspection of random sample of homes at 1‐year follow‐up: 1) Fire‐related injuries. 2) Final functioning alarms. | |
| Notes | Unpublished data provided by investigators. Inspection response rate: I: 72%; C: 72%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
SCIPP 1989.
| Methods | Non‐randomised controlled trial. | |
| Participants | I: 9 communities (total pop. 139,807). C: 5 demographically similar communities (total pop. 146,866). | |
| Interventions | I: Injury prevention program in communities, schools, homes, and clinical settings. C: No intervention. | |
| Outcomes | Population injury surveillance 1 year before to 2 months after; telephone survey pre‐ and post‐intervention. 1) Burn incidence. 2) Final alarm ownership. 3) Smoke alarms acquired. | |
| Notes | Unpublished data provided by investigators. Phone survey response rate: pre 59%, post 85% ("similar in the two groups"). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Thomas 1984.
| Methods | Cluster randomised controlled trial. Allocation by coin toss. Blinding of outcomes assessment not stated. | |
| Participants | 16 well‐baby classes (55 parents). | |
| Interventions | I: Burn prevention lecture, pamphlets, handouts, coupon for alarm; usual safety education. C: Usual safety education. | |
| Outcomes | Home inspection 4‐6 weeks after class. Final alarm ownership. | |
| Notes | No loss to follow‐up. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
Watson 2005.
| Methods | Randomised controlled trial. Allocation by independent researcher using computer generated random numbers, in blocks of 8. Blinded outcomes assessment. | |
| Participants | 3428 families with children aged <5 years, recruited from caseloads of 62 health visitors. | |
| Interventions | I: Structured, individualized 20‐minute safety consultation; free or discounted alarms; alarm installation for low income families. C: Usual care. | |
| Outcomes | Medical record review; postal questionnaire to 1000 subjects per group at 12 & 24 months: 1) Medically attended injuries. 2) Injury hospitalization. 3) Final functioning alarms. | |
| Notes | No loss to follow‐up for injury outcomes. Response rates at 12 months: I=78%; C=76%. Response rates at 24 months: I=82%; C=76%. Fire‐related injury rates not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Williams 1988.
| Methods | Cluster randomised controlled trial. Classes allocated by random numbers table by independent statistician. Unblinded outcomes assessment. | |
| Participants | 12 prenatal classes (165 pregnant women). | |
| Interventions | I: 1‐hour lecture, handouts on burn prevention; motor vehicle safety education and video; usual safety education. C: 1‐hour lecture, handouts & video on infant stimulation, feeding; usual safety education. | |
| Outcomes | Home inspection 2‐4 weeks after live birth: Final alarm ownership. | |
| Notes | 55% of women attending randomly allocated classes did not enrol in trial. Outcome data not available. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
I = Intervention C = Control I1 = Intervention Group 1 I2 = Intervention Group 2
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Botruff 1992 | Unable to obtain full paper or contact author, so unable to assess if met the inclusion criteria. |
| Culp 1999 | Not an intervention trial. |
| Kendrick 2001 | Not designed to increase smoke alarms. |
| Linyear 1982 | Unable to obtain full paper or contact author, so unable to assess if met the inclusion criteria. |
| Nunn 1998 | Not designed to increase smoke alarms. |
| Petridou 1997 | Not designed to increase smoke alarms. |
| Rowland 2002 | Not designed to increase smoke alarms; compared different types of smoke alarms to assess function over time. |
| Shults 1998 | Not a controlled trial. |
| Sundelin 1996 | Not designed to increase smoke alarms. |
| Treadwell 2000 | Not a controlled trial. |
| Ytterstad 1998 | Not designed to increase smoke alarms. |
Characteristics of ongoing studies [ordered by study ID]
Smithson 1998.
| Trial name or title | Smithson et al. |
| Methods | |
| Participants | 8 paired areas in 4 deprived communities (˜240 families of children aged 2 yrs or less in each area). |
| Interventions | I: Home visits every 2 months for 2 years by trained lay worker, teaching child development, safety, first aid; low cost safety devices; home safety inspection. C: Home safety inspection. |
| Outcomes | In progress. Home inspection, survey at 2 years. |
| Starting date | 1997 |
| Contact information | Dr. R. Smithson Consultant in Communicable Disease Western Health and Social Services Board 15 Gransha Park Clooney Road Londonderry, N. Ireland BT47 1TG UK |
| Notes | Preliminary results available from 1 pair: Alarm ownership I: 287/312 (92%) C: 271/302 (90%) |
Contributions of authors
CD designed the protocol, designed and ran searches, examined search results, applied inclusion criteria, extracted data, analysed data, interpreted results, and wrote the review. JH performed data analyses and interpreted results for, and assisted with writing of, the original review. CG collected data, examined search results, applied inclusion criteria, extracted data, interpreted results, and critically reviewed the manuscript.
Sources of support
Internal sources
Institute of Child Health, University College London, UK.
External sources
Colorado Injury Control Research Center, Colorado State University, USA.
National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (CDC), USA.
Camden & Islington Health Authority, UK.
National Health Service Research & Development Directorate, UK.
Declarations of interest
None known.
Edited (no change to conclusions)
References
References to studies included in this review
Barone 1988 {published data only}
- Barone VJ. An analysis of well‐child parenting classes: the extent of parent compliance with health‐care recommendations to decrease potential injury of their toddlers. [Dissertation]. Kansas City, KS: University of Kansas 1988.
Clamp 1998 {published and unpublished data}
- Clamp M, Kendrick D. A randomised controlled trial of general practitioner safety advice for families with children under 5 years. BMJ 1998;316:1576‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Davis 1987 {published data only}
- Davis JW. Get Fired Up: a model for developing inschool Four‐H programs (safety) [dissertation]. Clemson, SC: Clemson University, 1987. [Google Scholar]
DiGuiseppi 2002 {published data only}
- DiGuiseppi C, Roberts I, Wade A, Sculpher M, Edwards P, Godward C, et al. Incidence of fires and related injuries after giving out free smoke alarms: cluster randomised controlled trial. BMJ 2002;325(7371):995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiGuiseppi C, Roberts I, Wade A, Sculpher M, Edwards P, Godward C, et al. The 'Let's Get Alarmed!' initiative: a smoke alarm giveaway programme. Injury Prevention 1999;5(3):177‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiGuiseppi C, Slater S, Roberts I. Increasing the prevalence of smoke alarms: a community give‐away programme targeted to low income households. 4th World Conference on Injury Prevention and Control, Amsterdam. 1998.
Gielen 2001 {published data only}
- Chen LH, Gielen AC, MacDonald EM. Validity of self reported home safety practices. Injury Prevention 2003;9(1):73‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gielen AC, Wilson MEH, McDonald EM, Serwint JR, Andrews JS, Hwang W, et al. Randomized trial of enhanced anticipatory guidance for injury prevention. Archives of Pediatrics & Adolescent Medicine 2001;155:42‐9. [DOI] [PubMed] [Google Scholar]
Gielen 2002 {published data only}
- Gielen AC, McDonald EM, Wilson ME, Hwang WT, Serwint JR, Andrews JS, et al. Effects of improved access to safety counseling, products, and home visits on parents' safety practices: results of a randomised controlled trial. Archives of Pediatrics & Adolescent Medicine 2002;156(1):33‐40. [DOI] [PubMed] [Google Scholar]
Harvey 2004 {published data only}
- Harvey PA, Aitkin M, Ryan GW, Demeter LA, Givens J, Sundararaman R, Goulette S. Strategies to increase smoke alarm use in high‐risk households. Journal of Community Health 2004;29(5):375‐85. [DOI] [PubMed] [Google Scholar]
Hendrickson 2000 {published and unpublished data}
- Hendrickson SL. Effects of a nursing intervention on home safety in a low‐income community. Doctoral Dissertation, The University of Texas at Austin 2000.
Jenkins 1996 {published and unpublished data}
- Jenkins HML, Blank V, Miller K, Turner J, Stanwick RS. A randomized single‐blind evaluation of a discharge teaching book for pediatric patients with burns. Journal of Burn Care Rehabilitation 1996;17:49‐61. [PubMed] [Google Scholar]
Johnston 2000 {published data only}
- Johnston BD, Britt J, D'Ambrosio L, Mueller BA, Rivara FP. A preschool program for safety and injury prevention delivered by home visitors. Injury Prevention 2000;6:305‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelly 1987 {published data only}
- Kelly B, Sein C, McCarthy PL. Safety education in a pediatric primary care setting. Pediatrics 1987;79:818‐24. [PubMed] [Google Scholar]
Kendrick 1999 {published and unpublished data}
- Kendrick D, Hapgood R, Marsh P. Is it only 'safe' families who request home safety checks?. International Journal of Health Promotion and Education 2000;38(4):134‐7. [Google Scholar]
- Kendrick D, Marsh P. Inequalities in receipt of injury prevention in primary care. Health Education Journal 2000;59(2):50‐6. [Google Scholar]
- Kendrick D, Marsh P, Fielding K, Miller P. Preventing injuries in children: cluster randomised controlled trial in primary care. BMJ 1999;318:980‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
King 2001 {published and unpublished data}
- King WJ, Klassen TP, LeBlanc J, Bernard‐Bonnin AC, Robitaille Y, Pham B, et al. The effectiveness of a home visit to prevent childhood injury. Pediatrics 2001;108(2):382‐8. [DOI] [PubMed] [Google Scholar]
- Klassen TP, King WJ, Beaulne G, et al. A randomized controlled trial of a multi‐faceted home injury intervention in children following an ED visit [abstract]. Program and Abstracts, 38th Annual Meeting of the Ambulatory Pediatric Association, New Orleans, LA, May 1‐5. 1998:40‐41.
LeBailly 1990 {published data only}
- LeBailly SA, Freel K, Hicks‐Bartlett S, Kirschenman J, Ritts‐Benally K, Sasicki J. The Children's Safety Research Project. Elk Grove Village, Illinois: American Academy of Pediatrics, 1990. [Google Scholar]
Mallonee 1996 {published data only}
- Douglas MR, Istre GR, Mallonee S. Comparison of community based smoke detector distribution methods in an urban community. Injury Prevention 1998;4(1):28‐32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Douglas MR, Mallonee S, Istre GR. Estimating the proportion of homes with functioning smoke alarms: A comparison of telephone survey and household survey results. American Journal of Public Health 1999;89(7):1112‐1114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallonee S, Istre GR, Rosenberg M, et al. Surveillance and prevention of residential‐fire injuries. New England Journal of Medicine 1996;335:27‐31. [DOI] [PubMed] [Google Scholar]
Mathews 1988 {published data only}
- Mathews JR. An analysis of dangerous behavior in toddlers [Dissertation]. Kansas City, KS: University of Kansas, 1988. [Google Scholar]
McConnell 1996 {published data only}
- McConnell CF, Dwyer WO, Leeming FC. A behavioral approach to reducing fires in public housing. Journal of Community Psychology 1996;24:201‐12. [Google Scholar]
Miller 1982 {published data only}
- Miller RE, Reisinger KS, Blatter MM, Wucher F. Pediatric counseling and subsequent use of smoke detectors. American Journal of Public Health 1982;72:392‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ozanne‐Smith 2002 {published data only}
- Ozanne‐Smith J, Day L, Cassell E, Stathakis V, Sherrard J. A controlled evaluation of a community based injury prevention program. Fourth World Conference on Injury Prevention and Control, Amsterdam, Netherlands, 17‐20 May 1998. 1998; Vol. Book of Abstracts, Vol II:856.
- Ozanne‐Smith J, Day L, Stathakis V, Sherrad J. Controlled evaluation of a community based injury prevention program ini Australia. Injury Prevention 2002;8:18‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozanne‐Smith J, Sherrard J, Brumen IA, Vulcan P. Community ‐based injury prevention education report: Shire of Bulla Safe Living Program. Vol. Report 66, Victoria, Australia: Monash University Accident Research Centre, 1994. [Google Scholar]
Ploeg 1994 {published and unpublished data}
- Ploeg J, Black ME, Hutchison BG, Walter SD, Scott EAF, Chambers LW. Personal, home and community safety promotion with community‐dwelling elderly persons: response to a public health nurse intervention. Canadian Journal of Public Health 1994;85:188‐91. [PubMed] [Google Scholar]
Project Burn 1979 {published data only}
- MacKay AM, Rothman KJ. The incidence and severity of burn injuries following Project Burn Prevention. American Journal of Public Health 1982;72:248‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLoughlin E, Healer C, Healer C. Burn education intervention: a controlled study. Burns 1979;6:26‐29. [Google Scholar]
- McLoughlin E, Vince CJ, Lee AM, Crawford JD. Project Burn Prevention: outcome and implications. American Journal of Public Health 1982;72:241‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schwarz 1993 {published and unpublished data}
- Schwarz DF, Grisso JA, Miles C, Holmes JH, Sutton RL. An injury prevention program in an urban African‐American community. American Journal of Public Health 1993;83:675‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
SCIPP 1989 {published and unpublished data}
- Bass JL, Mehta KA, Ostrovsky M. Childhood injury prevention in a suburban Massachusetts population. Public Health Report 1991;106:437‐42. [PMC free article] [PubMed] [Google Scholar]
- Guyer B, Gallagher SS, Chang BH, Azzara CV, Cupples LA, Colton T. Prevention of childhood injuries: evaluation of the Statewide Childhood Injury Prevention Program (SCIPP). American Journal of Public Health 1989;79:1521‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Thomas 1984 {published data only}
- Thomas KA, Hassanein RS, Christophersen ER. Evaluation of group well‐child care for improving burn prevention practices in the home. Pediatrics 1984;74:879‐82. [PubMed] [Google Scholar]
Watson 2005 {published and unpublished data}
- Kendrick D, Watson M, Dewey M, Woods AJ. Does sending a home safety questionnaire increase recruitment to an injury prevention trial? A randomised controlled trial. Journal of Epidemiology & Community Health 2001;55(11):245‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson M, Kendrick D, Coupland C. Validation of a home safety questionnaire used in a randomised controlled trial. Injury Prevention 2003;9(2):180‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson M, Kendrick D, Coupland C, Woods A, Futers D, Robinson J. Providing child safety equipment to prevent injuries: Randomised controlled trial. BMJ 2005;5:178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson M, Woods A, Kendrick D. Injury prevention: working together on an RCT. Community Practitioner 2002;75(5):172‐5. [Google Scholar]
Williams 1988 {published data only}
- Williams GE. An analysis of prenatal education classes: an early start to injury prevention [Dissertation]. Kansas City, KS: University of Kansas, 1988. [Google Scholar]
References to studies excluded from this review
Botruff 1992 {published data only}
- Botruff T. Fire and Burn Injury Prevention Project: Fort McDowell Indian Reservation. Arizona: Western Arizona District Office, 1992. [Google Scholar]
Culp 1999 {published data only}
- Culp C. Residential smoke detector program distribution priorization and effectiveness measurement. National Fire Academy 1999.
Kendrick 2001 {published and unpublished data}
- Kendrick D, Pritchard A, Cloke J, Barley M. Randomised controlled trial assessing the impact of increasing information to health visitors about children's injuries. Archives of Disease in Childhood 2001;85:366‐70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Linyear 1982 {published data only}
- Linyear AS. A systems approach to the prevention and treatment of childhood injuries ‐ third year report. Richmond, VA: Bureau of Maternal and Child Health, 1982. [Google Scholar]
Nunn 1998 {published data only}
- Nunn RJ, Alder RG, Parmenter G, Lebnan VM, Laverick J. Primary prevention in firesetting. Russell.Nunn@Med.Monash.Edu.Au 1998.
Petridou 1997 {published data only}
- Petridou E, Tolma E, Dessypris N, Trichopoulos D. A controlled evaluation of a community injury prevention project in two Greek islands. International Journal of Epidemiology 1997;26(1):173‐9. [ISSN 0300‐5771] [DOI] [PubMed] [Google Scholar]
Rowland 2002 {published data only}
- Rowland D, DiGuiseppi C, Roberts I, Curtis K, Roberts H, Ginnelly L, et al. Prevalence of working smoke alarms in local authority inner city housing: randomised controlled trial. BMJ Clinical Research Ed 2002;325(7371):998‐1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shults 1998 {published data only}
- Shults RA, Sacks JJ, Briske LA, Dickey PH, Kinde MR, Mallonee S, et al. Evaluation of three smoke detector promotion programs. American Journal of Preventive Medicine 1998;15(3):165‐71. [DOI] [PubMed] [Google Scholar]
Sundelin 1996 {published data only}
- Sundelin C, Rasmussen F, Berfenstam R, Troedsson K. Information through television: does it promote child safety?. Injury Prevention 1996;2(1):36‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Treadwell 2000 {published data only}
- Treadwell L. Effectiveness of the Lubbock Fore Department's smoke detecor program. National Fire Academy 2000.
Ytterstad 1998 {published data only}
- Ytterstad B, Smith GS, Coggan CA. Harstad injury prevention study: prevention of burns in young children by community based intervention. Injury Prevention 1998;4:176‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies awaiting assessment
Azeredo 2003 {published data only}
- Azeredo R, Stephens‐Stidham S. Design and implementation of injury prevention curricula for elementary schools: lessons learned. Injury Prevention 2003;9(3):274‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell 2001 {published data only}
- Campbell NR, Ayala GX, Litrownik AJ, Slymen DJ, Zavala F, Elder JP. Evaluation of a first aid and home safety program for Hispanic migrant adolescents. American Journal of Preventive Medicine 2001;20(4):258‐65. [DOI] [PubMed] [Google Scholar]
Duggan 2004 {published data only}
- Duggan A, Fuddy L, Burrell L, Higman SM, McFarlane E, Windham A, Sia C. Randomized trial of a statewide home visiting program to prevent child abuse: impact in reducing parental risk factors. Child Abuse & Neglect 2004;28(6):625‐45. [DOI] [PubMed] [Google Scholar]
Gong 2001 {published data only}
- Gong D. Evaluation of an unintentional injury prevention curriculum for Korean‐American students. [Dissertation]. University of Georgia. United States ‐‐ Georgia, 2001.
Hatfield 2006 {published data only}
- Hatfield PM, Staresinic AG, Sorkness CA, Peterson NM, Schirmer J, Katcher ML. Validating self reported home safety practices in a culturally diverse non‐inner city population. Injury Prevention 2006;12(1):52‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hwang 2006 {published data only}
- Hwang V, Duchossois GP, Garcia‐Espana JF, Durbin DR. Impact of a community based fire prevention intervention on fire safety knowledge and behavior in elementary school children. Injury Prevention 2006;12(5):344‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kendrick 2007 {published data only}
- Kendrick D, Groom L, Stewart J, Watson M, Mulvaney C, Casterton R. "Risk Watch'': Cluster randomised controlled trial evaluating an injury prevention program. Injury Prevention 2007;13(2):93‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
McDonald 2005 {published data only}
- McDonald EM, Solomon B, Shields W, Serwint JR, Jacobsen H, Weaver NL, et al. Evaluation of kiosk‐based tailoring to promote household safety behaviors in an urban pediatric primary care practice. Patient Education and Counseling 2005;58(2):168‐81. [DOI] [PubMed] [Google Scholar]
Nansel 2002 {published data only}
- Nansel TR, Weaver N, Donlin M, Jacobsen H, Kreuter MW, Simons‐Morton B. Baby, Be Safe: The effect of tailored communications for pediatric injury prevention provided in a primary care setting. Patient Education and Counseling 2002;46(3):175‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Peek‐Asa 2005 {published data only}
- Peek‐Asa C, Allareddy V, Yang J, Taylor C, Lundell J, Zwerling C. When one is not enough: prevalence and characteristics of homes not adequately protected by smoke alarms. Injury Prevention 2005;11(6):364‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Posner 2004 {published data only}
- Posner JC, Hawkins LA, Garcia‐Espana F, Durbin DR. A randomized, clinical trial of a home safety intervention based in an emergency department setting. Pediatrics 2004;113(6):1603‐8. [DOI] [PubMed] [Google Scholar]
Robertson 2005 {published data only}
- Robertson AS, Rivara FP, Ebel BE, Lymp JF, Christakis DA. Validation of parent self reported home safety practices. Injury Prevention 2005;11(4):209‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sangvai 2007 {published data only}
- Sangvai S, Cipriani L, Colborn DK, Wald ER. Studying injury prevention: Practices, problems, and pitfalls in implementation. Clinical Pediatrics 2007;46(3):228‐35. [DOI] [PubMed] [Google Scholar]
Svanstrom 1995 {published data only}
- Svanstrom L, Ekman R, Schelp L, Lindstrom A. The Lidkoping Accident Prevention Programme ‐ a community approach to preventing childhood injuries in Sweden. Injury Prevention 1995;1:169‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sznajder 2003 {published data only}
- Sznajder M, Leduc S, Janvrin MP, Bonnin MH, Aegerter P, Baudier F, Chevallier B. Home delivery of an injury prevention kit for children in four french cities: a controlled randomized trial. Injury Prevention 2003;9(3):261‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to ongoing studies
Smithson 1998 {published data only}
- Smithson RD, Mullan C. Community childhood accident prevention project [abstract]. Book of Abstracts. Fourth World Conference on Injury Prevention and Control, Amsterdam, 17‐20 May 1998, p 373; Vol. 1.
Additional references
Bass 1993
- Bass JL, Christoffel KK, Widome M, Boyle W, Scheidt P, Stanwick R, et al. Childhood injury prevention counseling in primary care settings: a critical review of the literature. Paediatrics 1993;92:544‐50. [PubMed] [Google Scholar]
Ciliska 1996
- Ciliska D, Hayward S, Thomas H, Mitchell A, Dobbins M, Underwood J, et al. A systematic overview of the effectiveness of home visiting as a delivery strategy for public health nursing intervention. Canadian Journal of Public Health 1996;87:193‐8. [PubMed] [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [DOI] [PubMed] [Google Scholar]
Dickersin 1993
- Dickersin K, Min YI. NIH clinical trials and publication bias. Online Journal of Current Clinical Trials 1993;Apr 28:Doc No 50. [PubMed] [Google Scholar]
Dickersin 1994
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. BMJ 1994;309:1286‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
DiGuiseppi 1998a
- DiGuiseppi C, Roberts I, Li L. Smoke alarm ownership and house fire death rates in children. Journal of Epidemiology & Community Health 1998;52:760‐1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Easterbrook 1991
- Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet 1991;337:867‐72. [DOI] [PubMed] [Google Scholar]
Fire Statistics UK
- Fire Statistics, United Kingdom, 2005. Department of Communities and Local Government. London, 2007.
First World Cf 1989
- First World Conference on Accident and Injury Prevention, Stockholm, Sweden. 17‐20 September 1989.
Fourth World Cf 1998
- Fourth World Conference on Injury Prevention and Control, Amsterdam, Netherlands. 17‐20 May 1998.
Harborview MC 1997
- Harborview Medical Center Injury Prevention and Research Center. Systematic reviews of childhood injury prevention interventions. http://depts.washington.edu/hiprc/childinjury/ Updated 20 July 1997.
Hauck 1991
- Hauck WW, Gilliss CL, Donner A, Gortner S. Randomization by cluster. Nursing Research 1991;40:356‐8. [PubMed] [Google Scholar]
Kulenkamp 1994
- Kulenkamp A, Lundquist B, Schaenman P. Reaching the hard‐to‐reach: techniques from fire prevention programs and other disciplines. Arlington, VA. TriData Corporation, 1994. [Google Scholar]
Marshall 1998
- Marshall SW, Runyan CW, Bangdiwala SI, Linzer MA, Sacks JJ, Butts JD. Fatal residential fires: who dies and who survives?. JAMA 1998;279:1633‐7. [DOI] [PubMed] [Google Scholar]
Munro 1995
- Munro J, Coleman P, Nicholl J, Harper R, Kent G, Wild D. Can we prevent accidental injury to adolescents? A systematic review of the evidence. Injury Prevention 1995;1:249‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Murray 1994
- Murray DM, Rooney BL, Hannan PJ, Peterson AV, Ary DV, Biglan A, et al. Intraclass correlation among common measures of adolescent smoking: estimates, correlates, and applications in smoking prevention studies. American Journal of Epidemiology 1994;140:1038‐50. [DOI] [PubMed] [Google Scholar]
National Center 1996
- National Center for Injury Prevention and Control. Efforts to increase smoke detector use in US households: an inventory of programs. Atlanta: Centers for Disease Control and Prevention, 1996. [Google Scholar]
NFPA 2006
- Fire Loss in the U.S. during 2005. National Fire Protection Association 2006.
Peden 2002
- Peden M, McGee K, Sharma G. The injury chart book: a graphical overview of the global burden of injuries. Geneva: World Health Organization, 2002. [Google Scholar]
Roberts 1996
- Roberts I. Smoke alarm use: prevalence and household predictors. Injury Prevention 1996;2:263‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Runyan 1992
- Runyan CW, Bangdiwala SI, Linzer MA, Sacks JJ, Butts J. Risk factors for fatal residential fires. New England Journal of Medicine 1992;327:859‐63. [DOI] [PubMed] [Google Scholar]
Schaenman 1990
- Schaenman P, Stambaugh H, Rossomando C, Jennings C, Perroni C. Proving public fire education works. Arlington, VA: TriData Corporation, 1990. [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias: dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273:408‐12. [DOI] [PubMed] [Google Scholar]
Second World Cf 1993
- Second World Conference on Injury Control, Atlanta, Georgia. 20‐23 May 1993.
Third I Cf 1996
- Third International Conference on Injury Prevention and Control, Melbourne, Australia. 18‐22 February 1996.
Towner 1996
- Towner E, Simpson G, Jarvis S, Dowswell T (ed). Health promotion in childhood and young adolescence for the prevention of unintentional injuries. London: Health Education Authority, 1996. [Google Scholar]
Towner 2001a
- Towner E, Dowswell T, Jarvis S. Updating the evidence. A systematic review of what works in preventing childhood unintentional injuries: Part 1. Injury Prevention 2001;7:161‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Towner 2001b
- Towner E, Dowswell T, Jarvis S. Updating the evidence. A systematic review of what works in preventing childhood unintentional injuries: Part 2. Injury Prevention 2001;7:249‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
US Fire 1993
- US Fire Administration. Directory of national community volunteer fire prevention program community‐based fire prevention education initiatives: 1984‐1992. Emmitsburg, MD: US Fire Administration, 1993. [Google Scholar]
US Task Force 1996
- US Prevention Task Force. Counseling to prevent household and recreational injuries. In: DiGuiseppi C, Atkins D, Woolf S, Kamerow D editor(s). Guide to clinical preventive services. 2nd Edition. Washington DC: US Government Priniting Office, 1996:659‐85. [Google Scholar]
Warda 1999
- Warda L, Tenenbein M, Moffatt MEK. House fire injury prevention update. Part II. A review of the effectiveness of preventive interventions. Injury Prevention 1999;5:217‐225. [DOI] [PMC free article] [PubMed] [Google Scholar]
Watson 1999
- Watson L, Gamble J. Fire statistics: United Kingdom 1998. Home Office Statistical Bulletin. Vol. 15/99, London UK: Government Statistical Service, 1999. [Google Scholar]
References to other published versions of this review
DiGuiseppi 2000
- DiGuiseppi C, Higgins JPT. Systematic review of controlled trials of interventions to promote smoke alarms. Arch Dis Child 2000;82:341‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]