

Abstract
Context
Researchers analyzing data from the National Collegiate Athletic Association Injury Surveillance Program have not considered the differences in foot injuries across specific sports and between males and females.
Objective
To describe the epidemiologic differences in rates of overall foot injuries and common injuries among sports and between sexes.
Design
Descriptive epidemiology study.
Setting
Online injury-surveillance data from 15 unique sports involving males and females that demonstrated 1967 injuries over 4 821 985 athlete-exposures.
Patients or Other Participants
Male and female athletes competing in National Collegiate Athletic Association sports from the 2009–2010 through 2014–2015 seasons.
Main Outcome Measure(s)
Foot injury rates (per 10 000 athlete-exposures) and the proportion of foot injuries were calculated for each sport. The effect of sex was calculated using Poisson-derived confidence intervals for 8 paired sports. A risk analysis was performed using a 3 × 3 quantitative injury risk-assessment matrix based on both injury rate and mean days of time loss.
Results
Foot injury rates differed between sports, with the highest rates in female gymnastics, male and female cross-country, and male and female soccer athletes. Cross-country and track and field had the highest proportions of foot injuries for both female and male sports. The 5 most common injuries were foot/toe contusions, midfoot injuries, plantar fascia injuries, turf toe, and metatarsal fractures. Only track and field athletes demonstrated a significant sex difference in injury rates, with female athletes having the higher rate. The quantitative injury risk-assessment matrix identified the 4 highest-risk injuries, considering both rate and severity, as metatarsal fractures, plantar fascia and midfoot injuries, and foot/toe contusions.
Conclusions
Important differences were present among sports in terms of injury rates, the most common foot injuries, and the risk (combination of frequency and severity) of injury. These differences warrant further study to determine the mechanisms of injury and target intervention efforts.
Keywords: injury rates, lower extremity, collegiate athletes
Key Points
Foot injury rates were highest in gymnastics, cross-country, and soccer athletes.
Cross-country and track and field athletes had the highest proportions of foot injuries compared with other anatomic regions.
The 5 most common injuries were foot/toe contusions, midfoot injuries, plantar fascia injuries, turf toe, and metatarsal fractures.
The highest-risk injuries, defined as the combination of both injury rate and severity, were metatarsal fractures, plantar fascia injuries, midfoot injuries, and foot/toe contusions.
Running, jumping, cutting, pushing off, and kicking are fundamental requirements for athletic performance, and completing these tasks requires healthy, functional feet. Unfortunately, because of the foot's complex anatomy and biomechanics, these diverse demands also represent a large number of opportunities for injury. Various estimates1–5 suggested that the foot accounted for up to 20% of all injuries, depending on the sport, competition level, and study methods. Of course, a broad category such as “foot injuries” obscures important differences in individual injuries. A contusion of the foot or toe, for example, is not equivalent to a calcaneal fracture in either frequency or severity. Given the importance of this anatomic region, a better understanding of the epidemiology of foot injuries in sport is crucial for identification, treatment, and prevention.
Because specific tasks place unique biomechanical demands on the foot,6 and individual sports emphasize particular tasks, important intersport differences are expected in both the overall rate of injuries and the dominant injuries. These differences may provide useful insights into the biomechanics of injury. For example, the observation that midfoot injuries are common in American football but not in ice hockey7 players would support the hypothesis that the limited range of motion in a hockey skate has a protective effect.
In addition to intersport differences, it is also necessary to consider sex differences within individual sports. For example, women are at a much higher risk of anterior cruciate ligament tears compared with men.8,9 Greater ligament laxity in women has been identified as a potential cause for this higher susceptibility. The rates of ankle sprain10 and plantar fasciitis11 are also higher in women. These sex-based differences not only provide further insight into injury mechanisms but also highlight that customized prevention efforts may be required for particular populations.
The goal of our research was to perform an intersport study of foot injuries in collegiate-level athletes. We used Injury Surveillance Program (ISP) data from the National Collegiate Athletic Association (NCAA) for the 2009–2010 through the 2014–2015 seasons. Differences in overall foot injury rates as well as the rates of common injuries among sports were considered. Sex differences in the injury rates were also studied when both men's and women's data were available. A better understanding of these differences in foot injuries will offer insight into their injury mechanisms, will help prioritize prevention and reduction efforts, and can direct research into equipment or rule changes that could reduce the occurrence of these injuries.
METHODS
Details regarding the collection and nature of the ISP data will not be reviewed, as they are documented in detail elsewhere.12 It is worth noting, however, that some changes have occurred since the ISP began collecting data in 1982. For example, although an injury was initially defined as requiring restricted athletic participation for at least 1 day before it could be included in the database, injuries with no time loss have been included since the 2009–2010 season. These and other changes make it difficult to compare current data with data collected before that time.
The ISP data are administered by the Datalys Center for Sports Injury Research and Prevention, Inc (Indianapolis, IN), on behalf of the NCAA. Data for all foot injuries were requested for 6 seasons (2009–2010 to 2014–2015) along with the athlete-exposure (AE) data for each sport. The latter are used to calculate injury rates, as each AE represents 1 athlete's participation in an official practice or game. We also requested the total number of injuries per sport in order to calculate the proportion represented by the foot. Because these data are fully anonymized, this study was deemed by our institution's research ethics board as exempt from oversight. The final data set contained 1967 injuries and 4 821 985 AEs. The decision was made to merge the data for indoor and outdoor track and field athletes because we expected that any biomechanical differences between the 2 would be much smaller than any differences between them and other sports. Therefore, the data set consisted of 23 groups spanning 15 unique sports.
The proportion of foot injuries per sport was calculated by dividing the number of foot injuries by the total number of injuries sustained over the same period. Foot injury rates were calculated by dividing the number of foot injuries by the total number of AEs for that sport, with the results expressed as a rate per 10 000 AEs. The effect of sex on injury rates was evaluated using Poisson-derived confidence intervals13 for paired sports: that is, those sports for which both men's and women's data were available. A value of P < .05 was deemed as significant.
More than 57 unique injury codes were represented in the data. To reduce this number, we grouped 2 or more injury codes when they represented different severities of the same injury.14 For example, midfoot sprains, dislocations, and fractures were combined as midfoot injury, plantar fasciitis and plantar fascia tears (partial or complete) were merged into plantar fascia injury, and fractures and stress fractures were grouped together. Injuries to the metatarsals were also grouped together.
A 3 × 3 quantitative injury risk-assessment matrix (QIRAM) was created so that we could assess the most frequent injuries.14 Although not common in the sport realm,15,16 risk-assessment matrices (RAMs) are routinely used in industry to prioritize prevention and mitigation efforts.17–19 Possible events are evaluated based on their likelihood of occurrence, as well as the harm they would represent should they occur, and then they are categorized in a 2-D matrix with frequency and severity as the 2 axes. Events with the highest risk (highest likelihood and highest severity) are found in the top right corner of the RAM, and those with the lowest risk (lowest likelihood and lowest severity) appear in the bottom left corner, with moderate-risk events along the diagonal from the top left to the bottom right. As recently introduced, a QIRAM addresses 2 of the criticisms of a traditional RAM in that it uses quantitative epidemiologic data (rather than subjective evaluations) to determine frequency and severity and calculates the binning sizes based on K-means clustering to improve the resolution provided by the discrete bins.
Because time-loss data are missing for some injuries, because of either omission or withdrawal from the sport, only injuries with a minimum of 15 time-loss values were included in the 3 × 3 QIRAM analysis. Injuries were pooled across sex and sport. K-means clustering was used to group each injury in terms of rate (injuries per 10 000 AEs) and severity (mean time loss in days). Although the time-loss data were not normally distributed, we chose the mean because the presence of injury events with no time loss in the data gave median values of zero for many injuries. To understand the effect that their inclusion might have on the analysis, we constructed the QIRAM with and without zero–time-loss injuries.
RESULTS
A summary of the data provided by the Datalys Center for 23 groups across 15 sports is shown in Table 1. The total number of foot injuries varied dramatically, from 8 (men's swimming and diving) to 525 (men's football). Mean time loss and the range of values were calculated for each sport. The median might be a more appropriate measure because the data were not normally distributed, but the large number of injuries with no time loss resulted in median values of 0 for all sports save football (median = 1) and wrestling (2).
Table 1.
Summary of Sports Data
| Sport |
Sex |
Injuries, No. |
Athlete- Exposures, No. |
Time Loss, Mean (Range), d |
Underwent Surgery, % |
| Baseball | Men | 38 | 224 421 | 2.2 (0–31) | 0 |
| Basketball | Men | 165 | 283 233 | 6.7 (0–142) | 4.4 |
| Women | 126 | 239 980 | 7.7 (0–103) | 2.5 | |
| Cross-country | Men | 41 | 57 772 | 3.8 (0–64) | 0 |
| Women | 44 | 54 678 | 12.2 (0–77) | 0 | |
| Field hockey | Women | 16 | 47 455 | 5.5 (0–41) | 0 |
| Football | Men | 525 | 1 122 669 | 7.2 (0–335) | 6.4 |
| Gymnastics | Women | 60 | 56 471 | 8.1 (0–67) | 3.5 |
| Ice hockey | Men | 120 | 404 430 | 4.6 (0–91) | 2.5 |
| Women | 30 | 148 004 | 2.4 (0–48) | 0 | |
| Lacrosse | Men | 52 | 199 303 | 7.6 (0–103) | 5.8 |
| Women | 34 | 143 023 | 13.7 (0–135) | 3 | |
| Soccer | Men | 125 | 190 657 | 3.7 (0–45) | 3.4 |
| Women | 171 | 267 653 | 5.2 (0–58) | 2.4 | |
| Softball | Women | 47 | 209 396 | 3.5 (0–66) | 4.3 |
| Swimming and diving | Men | 8 | 131 745 | 1.9 (0–15) | 0 |
| Women | 11 | 156 114 | 4.6 (0–40) | 9.1 | |
| Tennis | Men | 11 | 31 785 | 3.3 (0–13) | 0 |
| Women | 21 | 45 326 | 22.8 (0–139) | 0 | |
| Track and field | Men | 86 | 261 676 | 11.3 (0–146) | 1.3 |
| Women | 122 | 247 968 | 11.5 (0–106) | 2.7 | |
| Volleyball | Women | 84 | 198 441 | 2.2 (0–41) | 3.6 |
| Wrestling | Men | 30 | 99 785 | 7.2 (0–92) | 0 |
The percentages of foot injuries per sport for female and male athletes are presented in Figure 1A. Values ranged from 15.1% for men's cross-country running to 2.5% for men's wrestling. The foot-injury rates by sport and sex, expressed in foot injuries per 10 000 AEs, are shown in Figure 1B. The highest injury rate was in women's gymnastics (10.62), and the lowest injury rates were in women's (0.70) and men's (0.61) swimming and diving.
Figure 1.

Comparisons of A, the proportion of foot injuries per sport (percentage of total injuries), and B, rates of foot injuries by sport (per 10 000 athlete-exposures).
For the 8 sports that had both women's and men's team data, we calculated Poisson-derived confidence intervals to assess whether the differences in injury rates were statistically significant (Table 2). Only track and field showed a difference (P = .0039), with women having a higher rate of injures. Because these groups represented the merging of indoor and outdoor events, the rates were analyzed separately to determine whether the decision made because of biomechanical similarity was justified based on statistics. The difference in the rates for men's indoor (3.2/10 000 AEs) and outdoor (3.4) track and field were not significant (P = .8049); the difference in women's injury rates was much larger (indoor = 4.3, outdoor = 6.0) but failed to reach significance (P = .0606). These results supported the decision to merge the 2.
Table 2.
Odds Ratios (Males:Females) for Paired Sportsa
| Sport |
Odds Ratio (95% Confidence Interval) |
P Value |
| Basketball | 1.11 (0.87, 1.41) | .3794 |
| Cross-country | 0.88 (0.56, 1.38) | .5624 |
| Ice hockey | 1.46 (0.97, 2.26) | .0604 |
| Lacrosse | 1.10 (0.70, 1.74) | .6729 |
| Soccer | 1.03 (0.81, 1.30) | .8260 |
| Swimming and diving | 0.87 (0.30, 2.35) | .7487 |
| Tennis | 0.75 (0.33, 1.62) | .4315 |
| Track and field | 0.67 (0.50, 0.89) | .0039 |
Bold type indicates significant difference between men and women.
Summary data for each injury that had a minimum of 15 entries with time-loss data, when pooled for all sports, are given in Table 3. It should be noted that the Other foot injury category is a unique code within the ISP, albeit not a particularly descriptive one. The All other injuries category consists of the pooled data for all individual injuries with fewer than the minimum 15 occurrences.
Table 3.
Most Common Injuries Across All Sports
| Injury |
No. |
Injury Rate per 10 000 Athlete-Exposures (95% Confidence Interval) |
Time Loss, Mean (Range), d |
| Foot/toe contusion | 430 | 0.89 (0.81, 0.98) | 2.6 (0–70) |
| Midfoot injury | 230 | 0.48 (0.42, 0.54) | 8.4 (0–121) |
| Plantar fascia injury | 196 | 0.41 (0.35, 0.47) | 6.7 (0–135) |
| Turf toe | 192 | 0.40 (0.34, 0.46) | 3.3 (0–72) |
| Metatarsal fracture | 174 | 0.36 (0.31, 0.42) | 33.5 (0–150) |
| Other foot injury | 119 | 0.25 (0.20, 0.30) | 6.7 (0–146) |
| Forefoot extensor/flexor tear | 106 | 0.22 (0.18, 0.27) | 4.4 (0–50) |
| Medial arch sprain—partial or complete | 57 | 0.12 (0.09, 0.15) | 4.0 (0–55) |
| Stress reaction | 49 | 0.10 (0.08, 0.13) | 5.1 (0–66) |
| Sesamoiditis | 43 | 0.09 (0.06, 0.12) | 3.7 (0–74) |
| Spring ligament sprain—partial or complete | 40 | 0.08 (0.06, 0.11) | 1.5 (0–22) |
| Foot tendinitis | 33 | 0.07 (0.05, 0.10) | 0.6 (0–7) |
| Inflammation | 28 | 0.06 (0.04, 0.08) | 9.5 (0–139) |
| Subungual hematoma (toenail) | 21 | 0.04 (0.03, 0.07) | 0.9 (0–7) |
| Metatarsal arch sprain—partial or complete | 21 | 0.04 (0.03, 0.07) | 6.1 (0–42) |
| Foot/toe infection | 18 | 0.04 (0.02, 0.06) | 1.5 (0–8) |
| Foot/toe blisters | 16 | 0.03 (0.02, 0.05) | 0.8 (0–7) |
| All other injuries | 194 | 0.40 (0.35, 0.46) | 9.3 (0–335) |
The top 6 injuries (excluding Other foot injury), each of which had more than 100 occurrences in the data set, were examined across different sports. To avoid the bias possible with small numbers, we limited the sports to those with at least 75 total foot injuries. Some sport-by-sport differences in injury prevalence are described in Table 4. Contusions of the foot and toes were the most common injuries overall; however, midfoot and plantar fascia injuries were the most frequent injuries in more than half of this smaller subset of sports. The intersport differences in the prominence of individual injuries warrant further consideration.
Table 4.
Injury Numbers and Rates per 10 000 Athlete-Exposures (AEs) and 95% Confidence Interval (CIs) for the Most Common Foot Injuries (Minimum of 75) in Sportsa
| Sport |
Sex |
No. (Rate per 10 000 AEs) [95% CI] |
|||||
| Foot/Toe Contusion |
Midfoot Injury |
Plantar Fascia Injury |
Turf Toe |
Metatarsal Fracture |
Forefoot Extensor/ Flexor Tear |
||
| Basketball | Men | 23 (0.81) | 32 (1.13) | 19 (0.67) | 17 (0.60) | 21 (0.74) | 7 (0.25) |
| [0.51, 1.22] | [0.77, 1.60] | [0.40, 1.05] | [0.35, 0.96] | [0.46, 1.13] | [0.10, 0.51] | ||
| Women | 14 (0.58) | 11 (0.46) | 18 (0.75) | 6 (0.25) | 12 (0.50) | 13 (0.54) | |
| [0.32, 0.98] | [0.23, 0.82] | [0.44, 1.19] | [0.09, 0.54] | [0.26, 0.87] | [0.29, 0.93] | ||
| Football | Men | 87 (0.77) | 98 (0.87) | 25 (0.22) | 92 (0.82) | 57 (0.51) | 22 (0.20) |
| [0.62, 0.96] | [0.71, 1.06] | [0.14, 0.33] | [0.66, 1.01] | [0.38, 0.66] | [0.12, 0.30] | ||
| Ice hockey | Men | 89 (2.20) | 1 (0.02) | 0 (0.00) | 2 (0.05) | 8 (0.20) | 3 (0.07) |
| [1.77, 2.71] | [0.01, 0.14] | [0.00, 0.00] | [0.01, 0.18] | [0.09, 0.39] | [0.02, 0.22] | ||
| Soccer | Men | 45 (2.36) | 13 (0.68) | 8 (0.42) | 15 (0.79) | 7 (0.37) | 7 (0.37) |
| [1.72, 3.16] | [0.36, 1.17] | [0.18, 0.83] | [0.44, 1.30] | [0.15, 0.76] | [0.15, 0.76] | ||
| Women | 51 (1.91) | 14 (0.52) | 16 (0.60) | 17 (0.64) | 8 (0.30) | 8 (0.30) | |
| [1.42, 2.51] | [0.29, 0.88] | [0.34, 0.97] | [0.37, 1.02] | [0.13, 0.69] | [0.13, 0.69] | ||
| Track and field | Men | 13 (0.50) | 7 (0.27) | 10 (0.38) | 1 (0.04) | 6 (0.23) | 10 (0.38) |
| [0.26, 0.85] | [0.11, 0.55] | [0.18, 0.70] | [0.01, 2.13] | [0.08, 0.50] | [0.18, 0.70] | ||
| Women | 14 (0.56) | 11 (0.44) | 15 (0.60) | 6 (0.24) | 13 (0.52) | 10 (0.40) | |
| [0.31, 0.95] | [0.22, 0.79] | [0.34, 1.00] | [0.09, 0.53] | [0.28, 0.90] | [0.19, 0.74] | ||
| Volleyball | Women | 5 (0.25) | 12 (0.60) | 12 (0.60) | 4 (0.20) | 6 (0.30) | 2 (0.10) |
| [0.08, 0.58] | [0.31, 1.06] | [0.31, 1.06] | [0.05, 0.52] | [0.11, 0.66] | [0.01, 0.36] | ||
Bold type indicates the most common injury per sport.
A 3 × 3 QIRAM of those injuries with a minimum of 15 entries with time-loss data is shown in Figure 2. We used K-means clustering to determine the bin sizes for grouping the injuries by both frequency (injury rate per 10 000 AEs) and severity (median time loss). The term risk in this scenario was defined as the combined effect of those 2 variables. Therefore, injuries in the top right corner of the matrix represent those with the highest risk, as they have the largest combination of rate and severity, and injuries in the bottom left represent those with the lowest risk. Metatarsal fractures were the highest-risk foot injury in this data set, followed by plantar fascia and midfoot injuries and foot/toe contusions. These injury rankings were not affected by the exclusion of zero–time-loss injuries (Figure 3).
Figure 2.
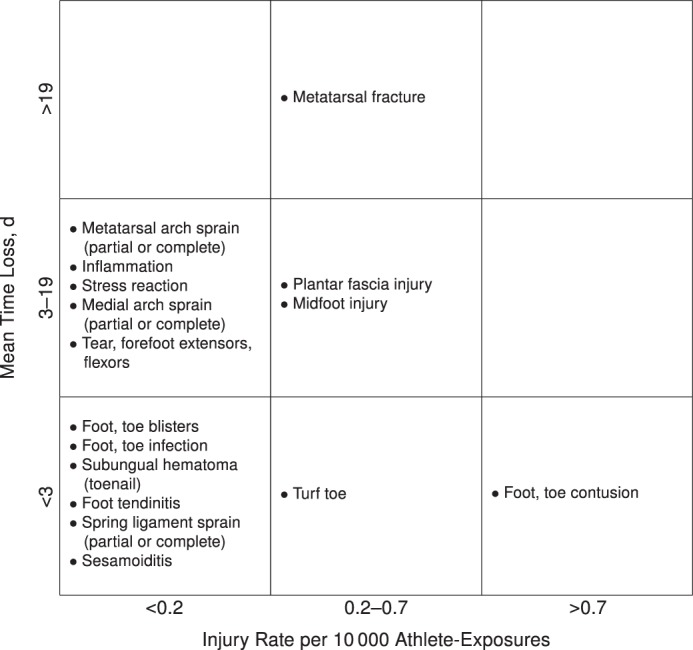
A 3 × 3 quantitative injury risk-assessment matrix of injuries with at least 15 occurrences (zero–time-loss injuries included).
Figure 3.
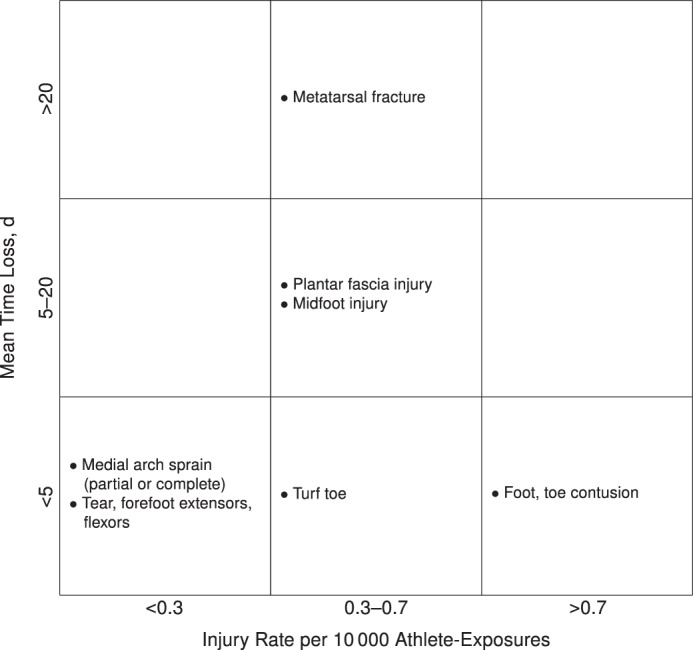
A 3 × 3 quantitative injury risk-assessment matrix of injuries with at least 15 occurrences (zero–time-loss injuries excluded).
DISCUSSION
We used NCAA-ISP data to study intersport differences in the prevalence and severity of athletic foot injuries for the 2009–2010 through the 2014–2015 seasons. Although ISP data collection began in 1982, changes were made to the collection criteria as of 2009–2010 (eg, zero–time-loss injuries began to be recorded) that may hinder comparisons with older data.
A total of 1967 injuries—gathered from 23 groups, 15 unique sports, and more than 4.8 million AEs—were analyzed. Sex differences in injury patterns were also investigated when data from the same sport were available for both men and women.
Cross-country (13.8% and 15.1%) and track and field (12.5% and 9.5%) had the highest proportions of foot injuries for both women's and men's sports (Figure 1A). These figures are higher than the 9.1% reported by Margherita et al20 for high school cross-country runners, but the differences may reflect the higher intensity and greater competition at the collegiate level, as well as the greater distances run by college athletes.21 Women's gymnastics had both a very high proportion (11.9%) and the highest rate (10.6/10 000AEs) of foot injuries among the sports included in the ISP data. The proportion of 11.9% was consistent with the range of 4.7% to 18.5% reported by the 7 previous studies summarized by Caine.22 Dismounts are recognized as a major source of injury in gymnastics,23,24 which likely explains the high rate of injury seen at the foot and ankle. It should be noted that the ordering of sports by injury rate in our study (gymnastics, cross-country, soccer) is identical to the results for foot and ankle injuries reported at a single Division I school by Hunt et al.25
The 5 most frequent injuries across the entire data set were foot/toe contusions, midfoot injuries, plantar fascia injuries, turf toe, and metatarsal fractures (Table 4). However, when the combination of both frequency and severity was considered, contusions represented a lower overall risk (Figure 2). The probability of a metatarsal fracture was less than half that of a contusion, but the injury was more than 12 times as severe in terms of mean time loss because treatment typically involves a cast or, in extreme cases, surgery.26 Therefore, to improve the safety of athletes, the highest-risk injuries—metatarsal fractures, plantar fascia injuries, and midfoot injuries—should be the priorities for prevention and mitigation strategies.
Although contusions were the most frequent injuries when all information was pooled, important sport-by-sport differences were observed (Table 4). Midfoot injuries were most common in men's basketball and football and tied for first place with plantar fascia injuries in women's volleyball. This result was consistent with our experimental understanding of the mechanism of midfoot injuries involving a combination of loading and twisting of the foot.14,27,28 That midfoot injuries were much less common in soccer, relatively speaking, is noteworthy because one would expect the biomechanical demands to be similar to those in basketball and football. The disparity in prevalences may be due to the differences in playing surface or a reduced risk of player contact in soccer. Similarly, the fact that turf toe is the second most common injury in football but proportionally less frequent in other sports should prompt additional study. Comparisons and contrasts among sports should be investigated so that we can better understand injury mechanisms.
In terms of sex effects, only track and field demonstrated a difference in the injury rates between men's and women's teams. Larger sample sizes will be needed to provide sufficient power to confirm whether no differences exist, yet pooling all foot injuries for specific sports may obscure important sex-based patterns in individual injuries. For example, we found that plantar fascia injuries were most frequent in 3 sports: women's basketball, women's track and field, and women's volleyball. This result is consistent with earlier research11 showing a higher incidence of plantar fascia injuries in women. These and other sex differences in injury rates not only highlight important anatomic and physiologic indicators of injury but also underscore that prevention efforts need to be targeted at specific groups.
One challenge when pooling data from different sports is that bias may be introduced. The total number of injuries and AEs varied dramatically, which means some sports were overrepresented and others underrepresented. In any given year, the ISP data sample only a portion of the entire population of each sport; also, that proportion can change year by year. The reason for this annual variation is that the ISP relies on the voluntary reporting of injury and exposure data by athletic trainers. Although we made no attempts to weight the data received from the Datalys Center, this would affect only the rankings of the most common injuries (Table 4) and the QIRAM (Figure 2). These 2 analyses are expected to overrepresent the “larger” sports in the data, particularly men's football. All of our other analyses relied on comparing rates and were not affected.
The motivation for this research was to aid injury prevention. However, we must recognize that identifying differences in injury patterns is only the first step toward that goal. Future authors should contrast individual injuries across sports to identify the biomechanical loading conditions, equipment, playing surface, training techniques, and other sport-specific details responsible for these differences. It is well known, for example, that certain training regimens can reduce the likelihood of particular injuries.29,30 Team training may specifically target prevention; nonetheless, it is also possible that certain drills or activities included to develop skills have an added prophylactic effect. For example, soccer dribbling drills intended to increase athletes' performance might also strengthen the foot and protect against midfoot sprains. A better understanding of how these variables affect the risk of injury would allow for preventive measures to be implemented.
To this end, our results suggest particular sports for specific future research directions. Gymnastics and cross-country running are ideal target sports given that they have both high proportions and high rates of foot injuries (Figure 1), whereas track and field represents the best option for looking at sex differences in injury patterns (Table 2). Metatarsal fractures were the highest-risk foot injury when accounting for both frequency and severity. Because men's and women's basketball, men's football, and women's track and field had the highest rates of metatarsal fractures (Table 4), these sports should be the focus of analysis and prevention efforts.
CONCLUSIONS
Important differences in terms of injury rates and the proportion of injuries represented by the foot were present among the 15 sports studied. The most common foot injuries across all sports were contusions, midfoot injuries, plantar fascia injuries, turf toe, and metatarsal fractures; however, meaningful intersport differences were found in their relative rankings. The highest-risk (combined frequency and severity) foot injuries were metatarsal fractures, plantar fascia injuries, midfoot injuries, and contusions. These differences warrant further study to improve our understanding of injury mechanisms and to better target intervention efforts.
ACKNOWLEDGMENTS
This publication contains materials created, compiled, or produced by the Datalys Center for Sports Injury Research and Prevention, Inc, on behalf of the NCAA. The NCAA-ISP data were provided by the Datalys Center. The ISP was funded by the NCAA. The content of this manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the Datalys Center or the NCAA. We thank the many athletic trainers who have volunteered their time and efforts to submit data to the NCAA ISP. Their efforts are greatly appreciated and have had a tremendously positive effect on the safety of collegiate athletes.
REFERENCES
- 1.Åman M, Forssblad M, Larsén K. National injury prevention measures in team sports should focus on knee, head, and severe upper limb injuries. Knee Surg Sports Traumatol Arthrosc. 2019;27(3):1000–1008. doi: 10.1007/s00167-018-5225-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beachy G, Akau CK, Martinson M, Olderr TF. High school sports injuries: a longitudinal study at Punahou School: 1988 to 1996. Am J Sports Med. 1997;25(5):675–681. doi: 10.1177/036354659702500515. [DOI] [PubMed] [Google Scholar]
- 3.Drakos MC, Domb B, Starkey C, Callahan L, Allen AA. Injury in the National Basketball Association: a 17-year overview. Sports Health. 2010;2(4):284–290. doi: 10.1177/1941738109357303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Herbenick MA, King JS, Altobelli G, Nguyen B, Podesta L. Injury patterns in professional arena football. Am J Sports Med. 2008;36(1):91–98. doi: 10.1177/0363546507308933. [DOI] [PubMed] [Google Scholar]
- 5.Walter SD, Hart LE, McIntosh JM, Sutton JR. The Ontario cohort study of running-related injuries. Arch Intern Med. 1989;149(11):2561–2564. [PubMed] [Google Scholar]
- 6.Riley PO, Kent RW, Dierks TA, Lievers WB, Frimenko RE, Crandall JR. Foot kinematics and loading of professional athletes in American football-specific tasks. Gait Posture. 2013;38(4):563–569. doi: 10.1016/j.gaitpost.2012.03.034. [DOI] [PubMed] [Google Scholar]
- 7.Lievers WB, Frimenko RE, McCullough KA, Crandall JR, Kent RW. Etiology and biomechanics of midfoot (Lisfranc) injuries in athletes. Crit Rev Biomed Eng. 2015;43(2–3):213–238. doi: 10.1615/CritRevBiomedEng.v43.i2-3.60. [DOI] [PubMed] [Google Scholar]
- 8.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 9.Renstrom P, Ljungqvist A, Arendt E, et al. Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med. 2008;42(6):394–412. doi: 10.1136/bjsm.2008.048934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123–140. doi: 10.1007/s40279-013-0102-5. [DOI] [PubMed] [Google Scholar]
- 11.Scher DL, Belmont PJ, Jr, Bear R, Mountcastle SB, Orr JD, Owens BD. The incidence of plantar fasciitis in the United States military. J Bone Joint Surg Am. 2009;91(12):2867–2872. doi: 10.2106/JBJS.I.00257. [DOI] [PubMed] [Google Scholar]
- 12.Kerr ZY, Dompier TP, Snook EM, et al. National Collegiate Athletic Association Injury Surveillance System: review of methods for 2004–2005 through 2013–2014 data collection. J Athl Train. 2014;49(4):552–560. doi: 10.4085/1062-6050-49.3.58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sahai H, Khurshid A. Formulae and tables for the determination of sample sizes and power in clinical trials for testing differences in proportions for the two-sample design: a review. Stat Med. 1996;15(1):1–21. doi: 10.1002/(SICI)1097-0258(19960115)15:1<1::AID-SIM134>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 14.Lievers WB, Adamic PF. Incidence and severity of foot and ankle injuries in men's collegiate American football. Orthop J Sports Med. 2015;3(5):2325967115581593. doi: 10.1177/2325967115581593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Drawer S, Fuller CW. Evaluating the level of injury in English professional football using a risk based assessment process. Br J Sports Med. 2002;36(6):446–451. doi: 10.1136/bjsm.36.6.446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fuller CW, Ward CJ. An empirical approach for defining acceptable levels of risk: a case study in team sports. Inj Prev. 2008;14(4):256–261. doi: 10.1136/ip.2008.018739. [DOI] [PubMed] [Google Scholar]
- 17.Middleton M, Franks A. Using risk matrices. Chem Eng. 2001;723:34–37. [Google Scholar]
- 18.National Aeronautics and Space Administration. NASA Risk Management Handbook. NASA report NASA/SP-2011-3422. Washington, DC: National Aeronautics and Space Administration;; 2011. [Google Scholar]
- 19.Thun JH, Hoenig D. An empirical analysis of supply chain risk management in the German automotive industry. Int J Prod Econ. 2011;131(1):242–249. [Google Scholar]
- 20.Margherita AJ, Rice SG, Koepsell TD, Rivara FP. High school cross country running injuries: a longitudinal study. Clin J Sports Med. 2000;10(2):110–116. doi: 10.1097/00042752-200004000-00005. [DOI] [PubMed] [Google Scholar]
- 21.Rasmussen CH, Nielsen RO, Juul MS, Rasmussen S. Weekly running volume and risk of running-related injuries among marathon runners. Int J Sports Phys Ther. 2013;8(2):111–120. [PMC free article] [PubMed] [Google Scholar]
- 22.Caine DJ. Injury epidemiology. In: Sands WA, Caine DJ, Borms J, editors. Scientific Aspects of Women's Gymnastics. Medicine and Sport Science. Vol. 45 Basel, Switzerland: Karger;; 2003. pp. 72–109. vol. [Google Scholar]
- 23.Marshall SW, Covassin T, Dick R, Nassar LG, Agel J. Descriptive epidemiology of collegiate women's gymnastics injuries: National Collegiate Athletic Association injury surveillance system, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):234–240. [PMC free article] [PubMed] [Google Scholar]
- 24.Chilvers M, Donahue M, Nassar L, Manoli A., II Foot and ankle injuries in elite female gymnasts. Foot Ankle Int. 2007;28(2):214–218. doi: 10.3113/FAI.2007.0214. [DOI] [PubMed] [Google Scholar]
- 25.Hunt KJ, Hurwit D, Robell K, Gatewood C, Botser IB, Matheson G. Incidence and epidemiology of foot and ankle injuries in elite collegiate athletes. Am J Sports Med. 2017;45(2):426–433. doi: 10.1177/0363546516666815. [DOI] [PubMed] [Google Scholar]
- 26.Shuen WMV, Boulton C, Batt ME, Moran C. Metatarsal fractures and sports. Surgeon. 2009;7(2):86–88. doi: 10.1016/s1479-666x(09)80022-x. [DOI] [PubMed] [Google Scholar]
- 27.Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot Ankle. 1986;6(5):225–242. doi: 10.1177/107110078600600504. [DOI] [PubMed] [Google Scholar]
- 28.DeOrio M, Erickson M, Usuelli FG, Easley M. Lisfranc injuries in sport. Foot Ankle Clin North Am. 2009;14(2):169–186. doi: 10.1016/j.fcl.2009.03.008. [DOI] [PubMed] [Google Scholar]
- 29.Hewett TE, Myer GD, Ford KR. Reducing knee and anterior cruciate ligament injuries among female athletes: a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18(1):82–88. doi: 10.1055/s-0030-1248163. [DOI] [PubMed] [Google Scholar]
- 30.Mohammadi F. Comparison of 3 preventive methods to reduce the recurrence of ankle inversion sprains in male soccer players. Am J Sports Med. 2007;35(6):922–926. doi: 10.1177/0363546507299259. [DOI] [PubMed] [Google Scholar]