

Abstract
Background
This study aims to evaluate our results of resection and reconstruction of the superior vena cava invaded by mediastinal tumors and benign diseases.
Methods
Seventeen patients (8 males, 9 females; mean age 46±17 years; range 9 to 74 years) undergoing superior vena cava resection and reconstruction due to mediastinal pathologies between September 2006 and September 2016 were retrospectively reviewed. Patients who had angioplasty with primary suturing or partial resection with stapler were excluded. Mortality and morbidity rates were analyzed based on the demographic, and intra- and postoperative measures.
Results
Majority of patients (94%) had mediastinal tumors. Twelve patients (71%) had thymic epithelial tumors. Tubular graft interposition was performed using ringed polytetrafluoroethylene prosthesis in nine patients (53%), while patch plasty using autologous pericardium, polytetrafluoroethylene or Dacron grafts was performed in eight patients (47%). Eleven patients (65%) necessitated concomitant resections of neighboring structures. Mean length of hospital stay was 11±6 days. There was no intraoperative death. Mortality occurred in three patients (18%). Five patients (29%) developed complications. Mortality occurred commonly in elderly patients (p<0.0001). Postoperative complications were more common in patients with concomitant resections (p=0.05). Neither acute nor chronic thrombosis developed in any patients. Median survival in patients with malignant diseases was 57 months, with a oneyear and three-year probability of survival of 83% and 74%, respectively.
Conclusion
Replacement of superior vena cava should be included in the therapeutic algorithm of selected patients with mediastinal tumors and benign diseases. Mortality rates may be higher in older patients, while the need for concomitant resections may increase morbidity rates.
Keywords: Grafting, mediastinum, outcomes, superior vena cava
Introduction
Superior vena cava (SVC) is vulnerable to the invasion of benign and malignant mediastinal diseases. The surgical indication and the efficacy for SVC resection and reconstruction have been debated for years.[1,2] Major invasion of the SVC by malignant tumors has long been considered as a formal contraindication, but in the 1970s and 1980s, animal research and clinical trials confirmed the feasibility of the operative replacement of the SVC.[2] The main indications for surgical resection and reconstruction of the SVC are the invasion of lung cancers or mediastinal diseases. Several series investigated the results of SVC resection and reconstruction in lung cancers.[1,3,4] The outcomes of these studies demonstrated that the resection of SVC is reasonable when a tumor directly invades the vein, not by the metastatic lymph node. There are also several reports consisting of more than 10 patients undergoing SVC resection and reconstruction due to mediastinal diseases with acceptable outcomes in early postoperative period and long-term outcomes.[2,5-12]
The resection of the SVC is a surgically challenging procedure. The requirement of a prosthetic conduit depends on the extent of the infiltration and of the vascular portion to be resected. The reconstruction can be performed basically in two ways; with partial resection and patch plasty, or complete resection and a conduit replacement.[13] Therefore, in this study, we aimed to evaluate our results of resection and reconstruction of the SVC invaded by mediastinal tumors and benign diseases.
Patients and Methods
Twenty-three patients underwent resection of the SVC and reconstruction by prosthetic or autologous grafts for treatment of benign or malignant mediastinal diseases at two different institutions (Group Florence Nightingale Hospitals and Istanbul Faculty of Medicine) between September 2006 and September 2016, and their results were presented before as oral presentation during the 19th Annual Congress of Turkish Thoracic Society in 2016.[14] Out of 23 patients, 17 patients ( 8 males, 9 females; mean age 46±17 years; range 9 to 74 years) were operated by the same surgeon, and these cases were enrolled into the study to decrease the surgical technical dependent factors and outcomes. Patients who had undergone primary repair with angioplasty or who had partial resection with stapler were excluded. The study protocol was approved by the Istanbul Bilim University, Faculty of Medicine Ethics Committee. A written informed consent was obtained from each patient. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Medical records of the patients were retrospectively reviewed. Database of the study group included demographic (age, gender, presence of SVC syndrome signs), pathologic (type of diseases, type and duration of induction treatment), intraoperative (access, duration of surgery, duration of SVC clamping, associated resections, intraoperative adverse events), postoperative (mortality, morbidity, hospital stay), and follow-up (status of the patient at last follow-up, status of the disease) measures.
Median sternotomy was the preferred approach, except for one patient with thymoma who underwent thoracotomy due to the need for additional lung resection, total pleurectomy, and diaphragmatic resection and reconstruction. We preferred the SVC reconstruction technique (patch plasty repair or graft interposition), depending on the degree of SVC infiltration, as previously described.[15] Polytetrafluoroethylene (PTFE) tubular prosthetic replacement was used in nine patients (53%), when the vascular infiltration by the disease could not be reconstructed with a patch plasty safely with negative surgical margins. The remaining eight patients (47%) had SVC infiltration safely reconstructable with negative surgical margins, and underwent patch plasty using autologous pericardium, PTFE, or Dacron.
Temporary interruption of flow during prosthetic or autologous replacement with proximal and distal caval clamps was managed with intravascular fluid expansion, lower extremity venous access, hyperventilation to reduce vasogenic cerebral edema, reverse Trendelenburg position, and vasoactive agents to increase cerebral perfusion. In some patients, a shunt to the right atrium from either of innominate veins was performed.
Once the initial dissection of the tumor or benign surrounding tissue was performed, SVC, both brachiocephalic veins (BCVs), and the proximal portion of the SVC-right atrial junction were isolated. After the SVC and/or BCV were resected, graft interposition was performed in a variety of ways. These included graft interposition from the distal SVC to the proximal SVC (n=9), from the left BCV to the right atrial appendage (n=4), from the right BCV to the right atrial appendage (n=1), from the SVC to the right atrial appendage (n=1), from the right BCV to the proximal SVC (n=1), and bilateral BCVs reconstruction with separate grafts (n=1).
In cavo-caval reconstruction, if the anastomosis was going to be performed under the level of junction, the azygos vein was ligated first. For SVC interposition, the extrapericardial portion of the SVC was prepared and intrapericardial SVC portion was exposed. When the disease involved one or both BCVs, the graft was placed between one of the BCV and the SVC, or between one of the BCV and the right atrial appendage. The cross-clamping technique was the approach of choice for vascular reconstruction. The distal anastomosis was performed first using 5-0 or 6-0 polypropylene sutures. This anastomosis was then tested for any leak. The proximal anastomosis was subsequently performed, and air was removed from the conduit before tying down the last anastomotic suture.
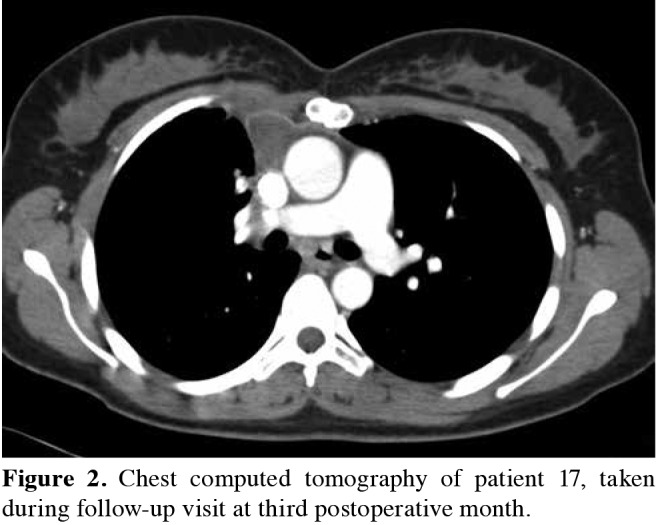
Anticoagulation therapy was routinely administered. Intravenous heparin sodium (0.5 mg/kg) was started three minutes before clamping. After intraoperative heparinization, the partial thromboplastin time was allowed to normalize without pharmacologic reversal. Patients were selectively transitioned to Coumadin® (Bristol-Myers Squibb, Princeton, NJ) on postoperative day two, which continued lifelong in patients undergoing a PTFE vascular reconstruction. Patients undergoing patch plasty were switched to Coraspin® ( Bayer T ürk K im San. Ltd. Şti, İstanbul, Turkey). Graft assessment was performed clinically in the early period. The graft patency in the late period was controlled by contrastenhanced computed-tomography scan taken at the third, sixth, and 12th p ostoperative m onths, t hen o ne per year (Figures 1 and 2).
Figure 1. Postoperative chest computed tomography of patient 16, taken at first postoperative year.
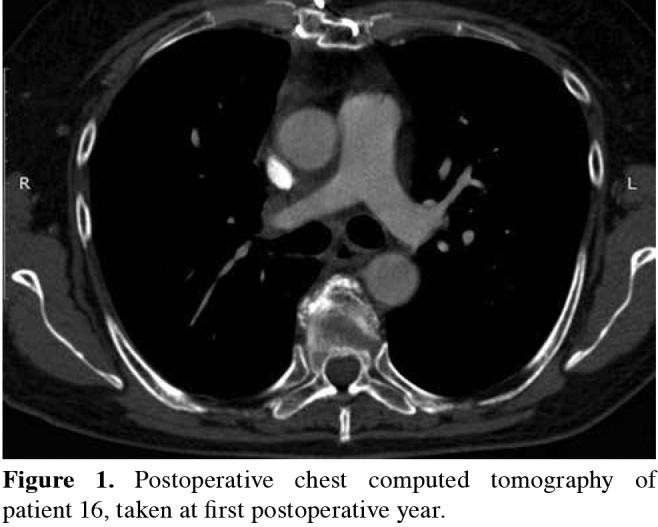
Figure 2. Chest computed tomography of patient 17, taken during follow-up visit at third postoperative month.
Statistical analysis Postoperative mortality was defined as any death occurring during the hospitalization of the patients or within 30 days after the operation. Morbidity was defined using the Society of Thoracic Surgery database's definitions.[16] The mortality and morbidity rates were analyzed based on the demographic, intraoperative, and postoperative measures. Statistical analysis was performed by using MedCalc demo version statistical software 16.4.3. Descriptive statistics were used to report the means and standard deviations of the continuous variables and number and percent of categorical variables. Student's t-test was used for the comparison of continuous variables, and Fischer's exact test for the comparison of categorical variables. Ap value of less than or equal to 0.05 was considered a statistically significant difference. Survival data for patients with malignant diseases were calculated by the Kaplan-Meier method from the day of operation until death or the day of the most recent follow-up.
Results
Table 1 outlines the preoperative, intraoperative, and postoperative characteristics of the 17 patients. Thirteen patients (76%) had previous tissue diagnosis, and three patients (18%) had mysthenia gravis and a mediastinal mass. In 16 patients (94%), SVC resection was performed for mediastinal malignant tumors. Of them, 12 patients (75%) had malignant thymic tumors (thymoma in 9 and thymic carcinoma in 3). The other four patients (25%) presented with other malignancies secondary to Hodgkin disease, thyroid medullary carcinoma, indifferentiated mediastinal sarcoma, and mediastinal germ cell tumor. Preoperative chemotherapy or radiation therapy was administered to eight patients (50%). The only patient (6%) with benign disease in this cohort had SVC resection due to benign mediastinal fibrosis with SVC stenosis resulting in SVC syndrome. Despite the three invasive interventions (mediastinoscopy, mediastinotomy, and endobronchial ultrasound), the pathology was unidentified. After the evaluation by interventional radiologists, this patient was found to be unsuitable for stent placement.
Table 1. Characteristics of patients.
| Case | Age/Gender | Symptoms | Associated conditions | Preoperative biopsy | Postoperative diagnosis | Preoperative treatment | Postoperative treatment | Reconstructed vessels | Adjacent structures resected | Interposition | Graft material | Mortality | Morbidity | Length of stay (days) | Follow-up (months) | Status |
| 1 | 74/M | - | Good syndrome | + | Thymoma | Chemotherapy | - | Right BCV-SVC |
Pulmonary wedge (bilateral) | Patch | Pericard | + (sepsis) | Chylothorax | 15 | 0 | IHD |
| 2 | 65/F | Weakness | Myasthenia gravis | - | Thymoma | - | - | Right BCV-RAA and left BCV-RAA |
Pulmonary wedge (right) | Tubular | PTFE | + (cardiac arrest) | - | 1 | 0 | IHD |
| 3 | 44/F | SVC syndrome |
- | + | Thymic carcinoma | Chemotherapy | Chemotherapy, radiotherapy |
SVC-SVC | - | Patch | PTFE | - | - | 8 | 108 | AWD |
| 4 | 74/F | - | - | + | Thymic carcinoma | Chemotherapy, radiotherapy |
- | SVC-SVC | - | Tubular | PTFE | + (Sepsis) | - | 25 | 0 | IHD |
| 5 | 53/F | SVC syndrome |
- | - | Thymoma | - | Chemotherapy | SVC-RAA | Partial right atrium | Tubular | PTFE | - | Arrhythmia (perioperative) | 9 | 95 | NED |
| 6 | 52/F | Chest pain | - | - | Lymphoma | - | Chemotherapy, radiotherapy |
SVC-SVC | Pulmonary wedge (right) | Tubular | PTFE | - | - | 9 | 28 | DOD |
| 7 | 9/M | - | - | + | Thymoma | Radiotherapy | - | SVC-SVC | - | Patch | Pericard | - | - | 7 | 59 | NED |
| 8 | 63/M | Weakness | Myasthenia gravis | - | Thymoma | - | Chemotherapy | Left BCV-RAA |
- | Tubular | PTFE | - | - | 11 | 51 | NED |
| 9 | 30/M | - | - | + | Germ cell tumor | Chemotherapy | Chemotherapy | SVC-SVC | Pulmonary wedge (right) | Patch | PTFE | - | - | 6 | 48 | NED |
| 10 | 30/M | - | - | - | Thymoma | - | Chemotherapy | SVC-SVC | - | Patch | Pericard | - | - | 7 | 47 | NED |
| 11 | 40/M | Dyspnea | - | - | Thyroid medullary carcinoma | - | Chemotherapy | Left BCV-RAA |
Thyroidectomy | Tubular | PTFE | - | - | 9 | 45 | NED |
| 12 | 45/F | Weakness, dyspnea | Myasthenia gravis | + | Thymoma | Chemotherapy | Radiotherapy | SVC-SVC | Pulmonary wedge (right) | Patch | Dacron | - | - | 8 | 35 | NED |
| 13 | 46/F | SVC syndrome |
- | + | Sarcoma | - | Chemotherapy | SVC-SVC | - | Patch | PTFE | - | - | 12 | 12 | DOD |
| 14 | 40/M | SVC syndrome |
- | + | Thymic carcinoma | Chemotherapy, radiotherapy |
Chemotherapy | Left BCV-RAA |
Pulmonary wedge (right) | Tubular | PTFE | - | Respiratory failure | 20 | 11 | DOD |
| 15 | 40/M | Chest pain | - | + | Thymoma | Chemotherapy | Chemotherapy | SVC-SVC | Pulmonary wedge (right), partial pleura, and diaphragm | Patch | PTFE | - | Respiratory failure | 20 | 17 | NED |
| 16 | 52/F | SVC syndrome |
- | - | Fibrosis | - | - | Left BCV-RAA |
Pulmonary wedge (right) | Tubular | PTFE | - | Arrhythmia (perioperative) | 7 | 12 | NED |
| 17 | 30/F | SVC syndrome |
- | + | Thymoma | - | - | Right BCV-RAA |
Pulmonary wedge | Tubular | PTFE | - | - | 7 | 3 | NED |
| BCV: Brachiocephalic vein; SVC: Superior vena cava; IHD: In-hospital death; RAA: Right atrial appendage; PTFE: Polytetrafluoroethylene; AWD: Alive with disease; NED: No evidence of disease; DOD: dead of disease. | ||||||||||||||||
Six patients (35%) presented with the following clinical signs of SVC syndrome in various combinations: face, neck or arm swelling, dry cough, collateral venous circulation, jugular distention, or erythrosis; but none of these patients underwent urgent surgery. Six patients (35%) had other complains (chest pain, cough, dyspnea, or muscle weakness). Five patients (30%) were asymptomatic. Of patients with thymic malignancies, three had myasthenia gravis whose symptoms were controlled by oral pyridostigmine, and one patient had Good syndrome.
Except for one patient, median sternotomy was the preferred approach in all patients. Patient 15 had a thymoma. This patient underwent thymomectomy, partial pericardiectomy, pulmonary wedge resection, and diaphragmatic resection and patch reconstruction via a right thoracotomy following the neoadjuvant chemotherapy.
Patient 6 underwent mediastinotomy for a mediastinal mass, and the frozen section analysis revealed a Hodgkin disease. On the next morning, sudden onset of massive hemorrhage induced by a sudden cough was noticed from the chest drain. Since she became unconscious, and tachycardia and h ypotension d eveloped w ithin m inutes, s he was immediately taken to the operating room. An emergency median sternotomy demonstrated a massive bleeding from the torn SVC which had been partially invaded by the tumor. This case had been presented before.[17]
Patient 7 was a nine-year-old child who had underwent incomplete resection for thymoma two years before in another institution, and received radiation therapy. A resternotomy was performed for the resection of the recurrent thymoma, and SVC resection and reconstruction.
Most of the resections were performed with SVC reconstruction with graft interposition. Tubular graft interposition was performed using ringed PTFE prosthesis in nine patients (53%). The remaining eight patients (47%) underwent patch plasty using PTFE (n=4), autologous pericardium (n=3), and Dacron (n=1) grafts. Median cross-clamping time was no longer than 30 minutes in all patients except for patient 6 (range 15-40 minutes).
Concomitant resections were performed in 11 patients (65%), and mostly included pulmonary wedge resections (9 patients, 82%). Details of the additional procedures were given in Table 1. Additionally, eight patients (47%) underwent diaphragmatic plication. No patient required extracorporeal bypass. Three patients required shunt to achieve resection. All 17 patients were assessed as complete resections by the pathology department.
The mean length of hospital stay was 11±6 days (range 1-25 days). There were no intraoperative deaths. Postoperative mortality occurred in three patients (18%). Patient 1 with Good syndrome had received neoadjuvant chemotherapy for type B3 thymoma. He developed postoperative chylothorax. He underwent reoperation for the stenosis of the SVC and a larger patch plasty was performed using pericardium. The patient deceased due to sepsis on postoperative day 15 despite treatment. Patient 2 died on postoperative day one due to sudden cardiac arrest. She had bilateral graft from both BCVs, and this is the only patient with two grafts. Patient 4 had a previous history of chemotherapy and radiation therapy for thymic carcinoma. She died due to sepsis on postoperative day 25 despite treatment.
Five patients (29%) experienced complications. The abovementioned patient 1 developed postoperative chylothorax. Patients 5 and 16 -both with SVC syndrome- developed intraoperative arrhythmia. The first patient required perioperative cardiac pacemaker implantation, while the second one returned to the normal sinus rhythm following perioperative cardioversion. Two other patients (14 and 15) required respiratory support with non-invasive mechanical support ventilation for respiratory insufficiency. They both recovered and were discharged without further home support.
Overall, the mortality was more common in older patients (71±5 vs. 41±13 years, p<0.0001). Postoperative complications mostly occurred in patients undergoing concomitant resections (45% vs. 0%, p=0.05). Any of the other demographic, intraoperative, and postoperative measures had no impact on mortality or morbidity.
Median follow-up was 40 months (range 3-108 months). Signs of the SVC syndrome disappeared in all six patients following the surgery. None of the discharged 14 patients developed neither acute nor chronic thrombotic event.
At the end of the follow-up period, the only patient with benign pathology was alive and disease free. Eleven (93%) out of 13 patients with malignant pathologies received adjuvant chemotherapy and/or radiation therapy. Three patients (6, 13, and 14) died due to metastasis. Patient 6 developed tracheomalacia after adjuvant chemotherapy and radiation therapy, and stayed intubated with the tracheal stent placement in another institution for two months after a vertebroplasty operation. She had a tracheoplasty for the correction of tracheomalacia. Two patients with thymic epithelial tumor developed pleural tumoral recurrences. Patient 15 underwent pleurectomy on postoperative eighth month. Patient 12 underwent surgery for repair of an aortic aneurysm which developed on postoperative 12th m onth. This patient was later detected to have recurrence on postoperative 27th month, and underwent pleurectomy. The remaining patients with malignant pathologies were alive with no evidence of disease, except for patient 3 who was alive with disease. Median survival in patients with malignant diseases was 57 months, with one-year and three-year probability of survival of 83% and 74%, respectively.
Discussion
Although resection and reconstruction of the SVC are technically challenging, it is generally accepted that SVC resection for malignant mediastinal tumors is feasible. Several series of SVC resection have been published confirming feasibility in the past 25 years. Table 2 outlines some studies consisting of more than 10 patients who underwent SVC resection and reconstruction due to mediastinal pathologies. The encouraging results suggest that if complete resection is pursued, then concomitant SVC resection can be performed.[2] However, today, most of the surgeons still have problems in decision making. Some prefer to use induction treatment, while some prefer direct surgery. Our experience demonstrates that the resection of the SVC may still be required and that we preferred an induction treatment in most of the situations.
The selection of appropriate candidates for SVC resection and reconstruction due to invasive mediastinal diseases remains challenging. Our indications for surgical resection and reconstruction of the SVC depended on two criteria as well as to the eligibility of the patient for operative intervention, as suggested by Picquet et al.[2] The first criterion was the presence of clinical symptoms of the SVC syndrome. Patients with SVC syndrome may present with face, neck or arm swelling, dry cough, collateral venous circulation, jugular distention, or erythrosis, and the severity of the SVC syndrome depends on the rate of SVC compression and the degree of development of venous drainage.[18] This is a contradictory situation for lung cancer invasion to the SVC. For lung cancer invasion to the SVC, almost every time, there should not be a sign of the obstruction unlike mediastinal disease. Compared with pulmonary neoplasms, SVC syndrome occurs more commonly in the presence of a mediastinal mass, and complete resolution of clinical signs is observed after surgery.[2] Spaggiari et al.[15] recommended that SVC resection should never be considered in the case of urgent treatment of an acute SVC syndrome. The authors mentioned that the dramatic hemodynamic changes occurring in case of an acute SVC syndrome might create instability at the patient during cross-clamping, thus causing difficulty in a radical complete resection. Six patients in our study presented with SVC syndrome (not in acute phase), and none of them underwent urgent surgery. Signs of the SVC syndrome disappeared in all patients postoperatively. Similar outcome has been reported before.[2,19]
Our second criterion was the histology of the SVC lesion presumed or confirmed by preoperative investigations. Superior vena cava may be invaded by mediastinal neoplasms such as thymomas, thymic carcinomas and germ cell tumors, and thyroid neoplasms.[20] Sixteen patients (94%) in our study had mediastinal neoplasms. All of the patients in this study had preoperative tissue diagnosis, except for three patients with myasthenia gravis and one patient with mediastinal fibrosis.
Benign diseases are rare causes of SVC reconstruction. Most patients undergoing surgical resection of the SVC have benign mediastinal fibrosis, followed by venous thrombosis. Besides surgical treatment, endovascular therapy with balloon angioplasty and stenting of the SVC have been performed with increasing frequencies.[21] Only one patient (6%) in this cohort had idiopathic mediastinal fibrosis. The patient underwent surgery, first, due to the presence of SVC syndrome, and second, because the interventional radiologist found this patient unsuitable to be stented because of heavy calcific obstruction.
We used cross-clamping technique in each SVC reconstruction. Our median cross-clamping time was less than 30 minutes in all patients, except for patient 6 (40 minutes). Dartevelle et al.[13] reported that clamping time of SVC of more than 45 minutes carried a risk for cerebral damage. Although they also described the use of SVC shunts during complete caval occlusion, we used this technique in only three patients whose surgeries were potentially difficult. In this study, in addition to SVC resection, eight patients (47%) necessitated resection of both BCVs. In this situation, we preferred unilateral reconstruction (seven out of 11) with satisfactory long-term patency, and performed bilateral reconstruction in only patient 2, which resulted in early postoperative mortality due to cardiac arrest.
Several types of conduit have been used in the reconstruction of the SVC. But there exist no evidence to confirm the superiority of any conduit over the other.[15] We p erformed p atch p lasty u sing a utologous pericardium, PTFE, or Dacron in patients with SVC infiltration of less than 50% of the diameter, not requiring circumferential resection. When a circumferential resection was performed, we used PTFE as the prosthetic conduit.
Polytetrafluoroethylene is considered to be the gold standard of SVC prosthetic replacement.[15] It has the advantage to have rings which prevent graft collapses when the central venous pressure becomes negative.[2] Polytetrafluoroethylene is also considered to be an optimal material because of its excellent antithrombogenic properties.[22]
Pericardium is also considered as an ideal material for the reconstruction of the SVC, but the availability of autologous pericardium is insufficient to construct SVC prosthesis.[15] The preservation of the human pericardium by glutaraldehyde has been proposed to improve tissue stability and reduce inflammatory response.[23] Besides autologous pericardium, stapled bovine pericardial conduit is another prosthetic material preferred in the reconstruction of the SVC.[24] We used autologous pericardium in three patients, and none of them developed graft infection.
Dacron is another material used rarely in the SVC reconstruction. Chen et al.[8] mostly preferred Dacron as the prosthetic conduit in their study. The researchers did not mention why they preferred Dacron, but reported no graft infection. In this study, we used Dacron in only one patient, and no graft infection developed.
Leo et al.[11] compared patients undergoing primary repair (direct suture, stapling, or autologous pericardium) with those undergoing prosthetic replacement of the SVC. They demonstrated no significant increased rate of morbidity between the groups. We also observed similar results. The type of conduit (PTFE, autologous pericardium, or Dacron) did not significantly affect the postoperative outcomes.
A graft reconstruction of the SVC may result in low blood flow velocity, leading to obstruction and recurrence of the SVC compression. The thrombosis rate of SVC reconstruction with PTFE varied between 0% and 56%.[2,5-7,10-12] We experienced no episode of graft occlusion in any patients undergoing tubular reconstruction with PTFE. No thrombotic event occurred in patients undergoing patch plasty in this study, although we had this complication in two of our patients undergoing SVC resection and reconstruction due to lung cancer.
As mentioned above, we mostly preferred unilateral reconstruction of the BCV, in case of the involvement by the disease. Several authors also suggested unilateral reconstruction.[15,20] In contrast, Shintani et al.[7] recommended bilateral BCV reconstruction owing to the higher thrombosis rate exceeding 50%, particularly in patients with unilateral left venous reconstruction. We did not observe thrombosis in the only patient with bilateral reconstruction in our study.
The mortality rate of SVC resection and reconstruction in mediastinal diseases is mostly reported to be ni,[5,7-9,12] but may be up to 8%.[2,10,11] The rate of mortality in this series was higher than the literature data (18%). Two of our patients died due to infection related causes, and one died due to sudden cardiac arrest. In our series, all mortalities were seen in the very early cases (Patients 1, 2, and 4). Older age was found to be a significant predictor of mortality (p<0.0001). Two of the three deceased patients received induction treatment, which was not a significant predictor of mortality. Morbidity rate has been reported to be between 6% to 33%.[2,5,7,8] In our series, 29% of the patients developed complications, commonly in those undergoing concomitant resections (p=0.05).
Spaggiari et al.[15] reported a median survival of 49 months in patients with mediastinal malignant tumors. The overall probability of survival in patients with mediastinal malignant diseases is 60% at three years,[5] and ranges between 45% to 63% at five years.[5,6,15] We obtained better results in our series and calculated a median survival of 57 months, while oneand three-year probabilities of survival were 83% and 74%, respectively.
This study has some limitations. Firstly, our study is a very recent study, thus most of our patients did not complet follow-up of five years. So, this prevented us to give five year probability of survival. Second limitation is that this study consisted of less patients, compared to studies given in Table 2. More comprehensive results can be obtained with prospectively designed future studies consisting of more patients. Therefore, this study is valuable since, as far as we know, this is first major study reflecting the results of SVC resection and reconstruction due to mediastinal diseases.
Table 2. Studies consisting of more than 10 patients undergoing superior vena cava resection and reconstruction due to mediastinal pathologies.
| Authors | Year | N | n | Pathology | Mortality | Morbidity | Occlusion | |||
| n | % | n | % | n | % | |||||
| Dartevelle et al.[5] | 1991 | 22 | 16 | MMT | 0 | 0 | 1 | 6 | 1 early | 13 |
| 1 late | ||||||||||
| Bacha et al.[6] | 1998 | 21 | 21 | MMT | NS | NS | 1 early | 10 | ||
| 1 late | ||||||||||
| Shintani et al.[7] | 2005 | 18 | 18 | MMT | 0 | 0 | 6 | 33 | 10 | 56 |
| Chen et al.[8] | 2006 | 15 | 15 | MMT | 0 | 0 | 2 | 13 | NG | |
| Picquet et al.[2] | 2009 | 24 | 12 | MMT + BMD | 1 | 8 | 1 | 8 | 0 | 0 |
| Sekine et al.[9] | 2010 | 20 | 11 | MMT | 0 | 0 | 13 | 65* | NS | |
| Leo et al.[11] | 2010 | 28 | 17 | MMT | 1 | 4* | 6 | 21* | 2 in-hospital* | 18 |
| 3 early* | ||||||||||
| Okereke et al.[10] | 2010 | 38 | 29 | MMT + BMD | 3 | 8* | 8 | 21* | 2* | 5 |
| Lee et al.[12] | 2016 | 16 | 15 | MMT | 0 | 0 | NS | 7 | 47 | |
| This study | 2016 | 17 | 17 | MMT + BMD | 3 | 18 | 5 | 29 | 0 | 0 |
| N: Total number of the patients with both mediastinal and pulmonary pathologies undergoing SVC resection and reconstruction; n: Total number of the patients with only mediastinal pathologies undergoing SVC resection and reconstruction; MMT: Malignant mediastinal tumor; BMD: Benign mediastinal disease; NS: Not specific; NG: Not given; * According to N. | ||||||||||
In conclusion, our experience suggests that the need for SVC reconstruction should not be considered a contraindication for mediastinal pathologies in an otherwise curable patient, provided that a complete resection can be achieved. We believe that replacement of the SVC should be included in the therapeutic algorithm in selected patients with mediastinal diseases who have no other contraindications. Mortality rate may be increased in older patients, and the need for concomitant resections may cause a higher rate of morbidity. Patient selection and surgical experience are believed to affect the outcomes directly.
Footnotes
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Financial Disclosure: The authors received no financial support for the research and/or authorship of this article.
References
- 1.Spaggiari L, Magdeleinat P, Kondo H, Thomas P, Leon ME, Rollet G, et al. Results of superior vena cava resection for lung cancer. Analysis of prognostic factors. Lung Cancer. 2004;44:339–346. doi: 10.1016/j.lungcan.2003.11.010. [DOI] [PubMed] [Google Scholar]
- 2.Picquet J, Blin V, Dussaussoy C, Jousset Y, Papon X, Enon B. Surgical reconstruction of the superior vena cava system: indications and results. Surgery. 2009;145:93–99. doi: 10.1016/j.surg.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 3.Suzuki K, Asamura H, Watanabe S, Tsuchiya R. Combined resection of superior vena cava for lung carcinoma: prognostic significance of patterns of superior vena cava invasion. Ann Thorac Surg. 2004;78:1184–1189. doi: 10.1016/j.athoracsur.2004.04.066. [DOI] [PubMed] [Google Scholar]
- 4.Shargall Y, de Perrot M, Keshavjee S, Darling G, Ginsberg R, Johnston M, et al. 15 years single center experience with surgical resection of the superior vena cava for non-small cell lung cancer. Lung Cancer. 2004;45:357–363. doi: 10.1016/j.lungcan.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 5.Dartevelle PG, Chapelier AR, Pastorino U, Corbi P, Lenot B, Cerrina J, et al. Long-term follow-up after prosthetic replacement of the superior vena cava combined with resection of mediastinal-pulmonary malignant tumors. J Thorac Cardiovasc Surg. 1991;102:259–265. [PubMed] [Google Scholar]
- 6.Bacha EA, Chapelier AR, Macchiarini P, Fadel E, Dartevelle PG. Surgery for invasive primary mediastinal tumors. Ann Thorac Surg. 1998;66:234–239. doi: 10.1016/s0003-4975(98)00350-6. [DOI] [PubMed] [Google Scholar]
- 7.Shintani Y, Ohta M, Minami M, Shiono H, Hirabayashi H, Inoue M, et al. Long-term graft patency after replacement of the brachiocephalic veins combined with resection of mediastinal tumors. J Thorac Cardiovasc Surg. 2005;129:809–812. doi: 10.1016/j.jtcvs.2004.05.001. [DOI] [PubMed] [Google Scholar]
- 8.Chen KN, Xu SF, Gu ZD, Zhang WM, Pan H, Su WZ, et al. Surgical treatment of complex malignant anterior mediastinal tumors invading the superior vena cava. World J Surg. 2006;30:162–170. doi: 10.1007/s00268-005-0009-x. [DOI] [PubMed] [Google Scholar]
- 9.Sekine Y, Suzuki H, Saitoh Y, Wada H, Yoshida S. Prosthetic reconstruction of the superior vena cava for malignant disease: surgical techniques and outcomes. Ann Thorac Surg. 2010;90:223–228. doi: 10.1016/j.athoracsur.2010.03.050. [DOI] [PubMed] [Google Scholar]
- 10.Okereke IC, Kesler KA, Rieger KM, Birdas TJ, Mi D, Turrentine MW, et al. Results of superior vena cava reconstruction with externally stented-polytetrafluoroethylene vascular prostheses. Ann Thorac Surg. 2010;90:383–387. doi: 10.1016/j.athoracsur.2010.04.004. [DOI] [PubMed] [Google Scholar]
- 11.Leo F, Bellini R, Conti B, Delledonne V, Tavecchio L, Pastorino U. Superior vena cava resection in thoracic malignancies: does prosthetic replacement pose a higher risk. Eur J Cardiothorac Surg. 2010;37:764–769. doi: 10.1016/j.ejcts.2009.10.024. [DOI] [PubMed] [Google Scholar]
- 12.Lee GD, Kim HR, Choi SH, Kim YH, Kim DK, Park SI. Prosthetic graft interposition of the brachiocephalic veins or superior vena cava combined with resection of malignant tumors: graft patency and risk factors for graft occlusion. J Thorac Dis. 2016;8:61–67. doi: 10.3978/j.issn.2072-1439.2016.01.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dartevelle P, Macchiarini P, Chapelier A. Technique of superior vena cava resection and reconstruction. Chest Surg Clin N Am. 1995;5:345–358. [PubMed] [Google Scholar]
- 14.Toker A, Özkan B, Özyurtkan MO, Kaba E, Ayalp K, Tanju S, et al. Türk Toraks Derneği 19. Yıllık Kongresi 6-10 Nisan 2016, Sözlü Sunum Kitapçığı. 2016. Mediastinal kitlelerde superior vena kava rezeksiyon ve rekonstrüksiyonu; pp. 101–101. [Google Scholar]
- 15.Spaggiari L, Leo F, Veronesi G, Solli P, Galetta D, Tatani B, et al. Superior vena cava resection for lung and mediastinal malignancies: a single-center experience with 70 cases. Ann Thorac Surg. 2007;83:223–230. doi: 10.1016/j.athoracsur.2006.07.075. [DOI] [PubMed] [Google Scholar]
- 16.The Society of Thoracic Surgeons. Database. Available from: http://www.sts.org/sections/stsnationaldatabase/publications/executive/artcile.html. [Google Scholar]
- 17.Toker A, Tanju S, Erus S. Emergency reconstruction of superior vena cava following biopsy of mediastinal lymphoma. Turk Gogus Kalp Dama. 2012;20:390–392. [Google Scholar]
- 18.The superior vena cava syndrome: clinical characteristics and evolving etiology. Medicine (Baltimore) 2006;85:37-42. 2012;20:390–392. doi: 10.1097/01.md.0000198474.99876.f0. [DOI] [PubMed] [Google Scholar]
- 19.Gloviczki P, Pairolero PC, Toomey BJ, Bower TC, Rooke TW, Stanson AW, et al. Reconstruction of large veins for nonmalignant venous occlusive disease. J Vasc Surg. 1992;16:750–761. [PubMed] [Google Scholar]
- 20.Lanuti M, De Delva PE, Gaissert HA, Wright CD, Wain JC, Allan SA, et al. Review of the superior vena cava resection in the management of benign disease and pulmonary or mediastinal malignancies. Ann Thorac Surg. 2009;88:392–398. doi: 10.1016/j.athoracsur.2009.04.068. [DOI] [PubMed] [Google Scholar]
- 21.Kalra M, Gloviczki P, Andrews JC, Cherry KJ Jr, Bower TC, Panneton JM, et al. Open surgical and endovascular treatment of superior vena cava syndrome caused by nonmalignant disease. J Vasc Surg. 2003;38:215–223. doi: 10.1016/s0741-5214(03)00331-8. [DOI] [PubMed] [Google Scholar]
- 22.Nakano T, Endo S, Kanai Y, Otani S, Tsubochi H, Yamamoto S, et al. Surgical outcomes after superior vena cava reconstruction with expanded polytetrafluoroethylene grafts. Ann Thorac Cardiovasc Surg. 2014;20:310–315. doi: 10.5761/atcs.oa.13-00050. [DOI] [PubMed] [Google Scholar]
- 23.Carpentier A, Lemaigre G, Robert L, Carpentier S, Dubost C. Biological factors affecting long-term results of valvular heterografts. J Thorac Cardiovasc Surg. 1969;58:467–483. [PubMed] [Google Scholar]
- 24.Ciccone AM, Venuta F, D'Andrilli A, Andreetti C, Ibrahim M, De Giacomo T, et al. Long-term patency of the stapled bovine pericardial conduit for replacement of the superior vena cava. Eur J Cardiothorac Surg. 2011;40:1487–1491. doi: 10.1016/j.ejcts.2011.03.008. [DOI] [PubMed] [Google Scholar]