

Abstract
There are well-established associations between sexual assault victimization and deleterious psychological and physical health outcomes. The present study contributes to the emerging health disparities literature by examining similarities and differences in relationships between the severity of the sexual assault and health in a community sample of African American and Caucasian survivors. Although the overall pattern of relationships was expected to be comparable for all survivors, some associations were hypothesized to be stronger for African American survivors as compared to Caucasian survivors based on theories of chronic stress. Single, African American and Caucasian women were recruited for a study of dating experiences through random digit dialing in one large metropolitan area. Participants who experienced a sexual assault since age 14 were included in this study (121 African American and 100 Caucasian women). Multi-group path analyses indicated that for both African American and Caucasian survivors, sexual assault severity was significantly positively associated with PTSD symptoms and depressive symptoms were significantly positively associated with physical health symptoms. Among African American survivors, sexual assault severity affected physical health symptoms indirectly through its impact on depressive symptoms, and assault severity indirectly affected drinking problems through its impact on PTSD symptoms; these relationships were not found for Caucasian survivors. These findings highlight the need for additional research that focuses on health disparities in sexual assault survivors’ recovery process, so that treatment programs address culturally relevant issues.
Sexual assault is a pervasive problem, with a myriad of short and long-term deleterious health consequences for survivors. Based on the findings from the Center for Disease Control and Prevention’s nationally representative survey of the English and Spanish speaking U.S. population age 18 and older, 19.3% of adult American women have been raped during their lifetime; 43.9% of these women reported other forms of sexual violence victimization (Breiding et al., 2014). Survivors of sexual assault experience many negative psychological and physical health outcomes, including posttraumatic stress disorder (PTSD) symptoms, depressive symptoms, suicidal ideation, anxiety, self-reported health complaints, greater healthcare utilization, chronic health conditions, and problematic drinking (Campbell, Dworkin, & Cabral, 2009; Golding, Cooper, & George, 1997; Koss, Figueredo, & Prince, 2002; Littleton, Grills-Taquechel, Buck, Rosman, & Dodd, 2013; Ullman, Filipas, Townsend, & Starzynski, 2005; Wadsworth & Records, 2013; World Health Organization, 2013).
The long-term impact of sexual assault varies based on many factors including the amount of formal and informal support received, coping resources, and other stressors in survivors’ lives (Campbell et al., 2009; Ullman & Fillipas, 2001). All survivors are harmed by societal stereotypes that encourage victim blame; however, these stereotypes tend to be more harshly applied to ethnic minority women (Abbey, Jacques-Tiura, & Parkhill, 2010; George & Martinez, 2002). African American women’s experiences with racial discrimination, political marginalization, and social adversity affect how they conceptualize and respond to sexual assault (Abbey et al., 2010; Bryant-Davis, Chung, & Tillman, 2009; Neville & Heppner, 1999; Wadsworth & Records, 2013). Geronimus (1992) argued that health disparities are partially explained by the greater levels of chronic stress typically experienced by African Americans as compared to Caucasians because of their frequent experiences with social, political, and economic discrimination. The cumulative impact of these stressors is hypothesized to impair physiological mechanisms associated with health (Geronimus, Hicken, Keene, & Bound, 2006). In support of this hypothesis, African Americans have higher physiological indicators of chronic stress than do Caucasians, even after controlling for socioeconomic status (Chyu & Upchurch, 2011; Geronimus et al., 2006). The weathering hypothesis suggests that sexual assault may result in greater health deterioration for African American survivors as compared to Caucasian survivors because of the greater overall chronic stress burden.
The present study contributes to the emerging health disparities literature by examining similarities and differences in psychological and physical health outcomes in a community sample of African American and Caucasian survivors. In the following sections, we review the relevant literature and the study’s hypotheses.
PTSD and Depressive Symptoms
PTSD symptoms are extremely common after sexual assault (Clum, Calhoun, & Kimberling, 2000; Zoellner, Goodwin, & Foa, 2000). Although PTSD symptoms often peak soon after the assault, many survivors have symptoms that continue for years (Najdowski & Ullman, 2009; Rothbaum, Foam Murdock, Riggs, & Walsh, 1992; Steenkamp, Dickstein, Salters-Pedneault, Hofmann, & Litz, 2012). Lifetime prevalence rates for PTSD among sexual assault victims range from 30 to 65% (Clum et al., 2000; Kilpatrick, Saunders, Veronen, Best, & Von, 1987; Resnick, Kilpatrick, Dansky, Saunders, & Best, 1993; Rothbaum et al., 1992; Zoellner et al., 2000), and rates of current PTSD are around 12 to 16% (Kilpatrick et al., 1987; Resnick et al., 1993).
Sexual assault survivors are also at heightened risk for experiencing depressive symptoms and meeting clinical criteria for depression (Acierno et al., 2002; Campbell et al., 2009; Clum et al., 2000). In a national random sample of women, sexual assault victimization was significantly associated with meeting diagnostic criteria for major depressive disorder (Acierno et al., 2002). Further, depressive symptoms can persist for years after the assault. In one study, 60% of rape survivors reported depressive symptoms approximately 8 years post-assault (Mackey et al., 1992).
Only a few studies have examined ethnic differences in PTSD symptom severity or depressive symptoms among sexual assault survivors and most of these studies have reported no differences (Kaukinen & DeMaris, 2005; Littleton et al., 2013; McFarlane et al., 2005; Plichta & Falik, 2001; Ullman & Brecklin, 2002). In contrast, Littleton and Ullman (2013) found greater PTSD symptom severity among African American survivors as compared to Caucasian survivors. These studies differ in sampling procedures and measures, making it difficult to draw any general conclusions.
Physical Health Symptoms
The relationship between sexual assault victimization and physical health outcomes is well documented (World Health Organization, 2013). Women with a history of sexual assault victimization have poorer perceptions of health, more self-reported health complaints, more gastrointestinal and gynecological problems, more chronic health conditions (including fibromyalgia, diabetes, and arthritis), greater utilization of primary and emergency medical services, higher median medical bill costs, and higher mortality rates (Golding, 1999; Golding et al., 1997; Kimberling & Calhoun, 1994; Plichta & Falik, 2001).
Psychological distress, such as PTSD symptoms and depressive symptoms, may mediate the relationship between sexual assault and physical health symptoms (Campbell, Greeson, Raja, & Raja, 2008; Koss et al., 2002; Zinzow et al., 2011; Zoellner, Goodwin, & Foa, 2000). A prolonged stress response can adversely affect the HPA axis, subsequently compromising immune and inflammatory responses. Chronic inflammation, in particular, can manifest itself in pain-related health problems (Campbell et al., 2008). The weathering hypothesis (Geronimus, 1992) suggests that sexual assault may result in greater physical health problems among African American survivors as compared to Caucasian survivors because of higher pre-existing chronic stress levels.
Drinking Problems
The relationship between sexual assault victimization and drinking problems has been demonstrated in community-based and nationally representative cross-sectional studies, as well as prospective studies (Kilpatrick, Acierno, Resnick, Saunders, & Best, 1997; Lown, Nayak, Korcha, & Greenfield, 2011; Ullman et al., 2005). These studies suggest that 13 to 49% of sexual assault survivors have serious alcohol problems. In their two-year longitudinal study, Kilpatrick et al. (1997) found that women who were sexually and/or physically assaulted during the course of the study were almost three times more likely to meet diagnostic criteria for alcohol abuse after the incident than were women who did not experience an assault. Theoretical explanations for the relationship between sexual assault victimization and drinking problems include the tension reduction model, the motivation model of alcohol use, and the self-medication hypothesis (Cappell & Greeley, 1987; Cooper, Frone, Russell, & Mudar, 1995). These models posit that some traumatized individuals use alcohol to cope with negative affect.
In the general population, Caucasians have higher rates of alcohol consumption than African Americans (Delker, Brown, & Hasin, 2016; Grant et al., 2015). Moreover, Caucasian victims of sexual assault are more likely to have consumed alcohol prior to the incident (Abbey, Ross, McDuffie, & McAuslan, 1996; Littleton et al., 2013). However, findings on ethnic differences in problem drinking among sexual assault survivors are mixed. Some research suggests that African American women may be more likely to engage in heavy drinking following sexual violence (Bryant-Davis et al., 2009; Kaukinen & DeMaris, 2005). Conversely, other studies have found that African American sexual assault survivors are at a lower risk of engaging in heavy drinking than Caucasian survivors (Kaukinen & DeMaris, 2005; Littleton et al., 2013). These contradictory findings suggest there may be complex ethnic differences in risk pathways to problematic alcohol use. For instance, in Littleton and Ullman’s (2013) sample of sexual assault survivors, there were no significant ethnic differences in hazardous drinking. However, ethnicity moderated the relationship between PTSD symptoms and hazardous drinking such that PTSD symptoms predicted hazardous drinking for African Americans, but not for Caucasians.
Severity of the Assault
Although many survivors experience psychological distress for years after their assault, there is great variability. For example, Kilpatrick, Resick, and Veronen (1981) reported that a quarter of the rape victims who were recruited from a local hospital had virtually no psychological symptoms on a wide range of distress measures one year after their assault. Severity of the assault has been examined to understand why some victims experience more distress than others. Severity has been operationalized in many different ways that include objective and subjective components. In their meta-analysis, Weaver and Clum (1995) reported that objective aspects of the assault, such as the perpetrators’ degree of force, the presence of a weapon, and physical injuries, have small to moderate effect sizes in predicting psychological distress. They found that subjective aspects of severity (e.g., general appraisal, perceived life threat, self-blame, perceived controllability, and perceived safety) contributed twice as much to the prediction of distress than did objective factors. Thus, both objective and subjective components of severity were included in this study.
The Present Study: Goals and Hypotheses
The first goal of the present study was to examine psychological and physical health outcomes associated with sexual assault victimization. Figure 1 presents the conceptual model that we developed based on the literature reviewed in the previous sections. We hypothesized that survivors’ perceptions of the severity of the sexual assault would be positively associated with the amount of PTSD symptoms and depressive symptoms they experienced, which in turn were expected to be positively associated with their drinking problems and physical health symptoms. Assault severity’s impact on drinking problems and physical health were hypothesized to be indirect and mediated by PTSD symptoms and depressive symptoms.
Figure 1.
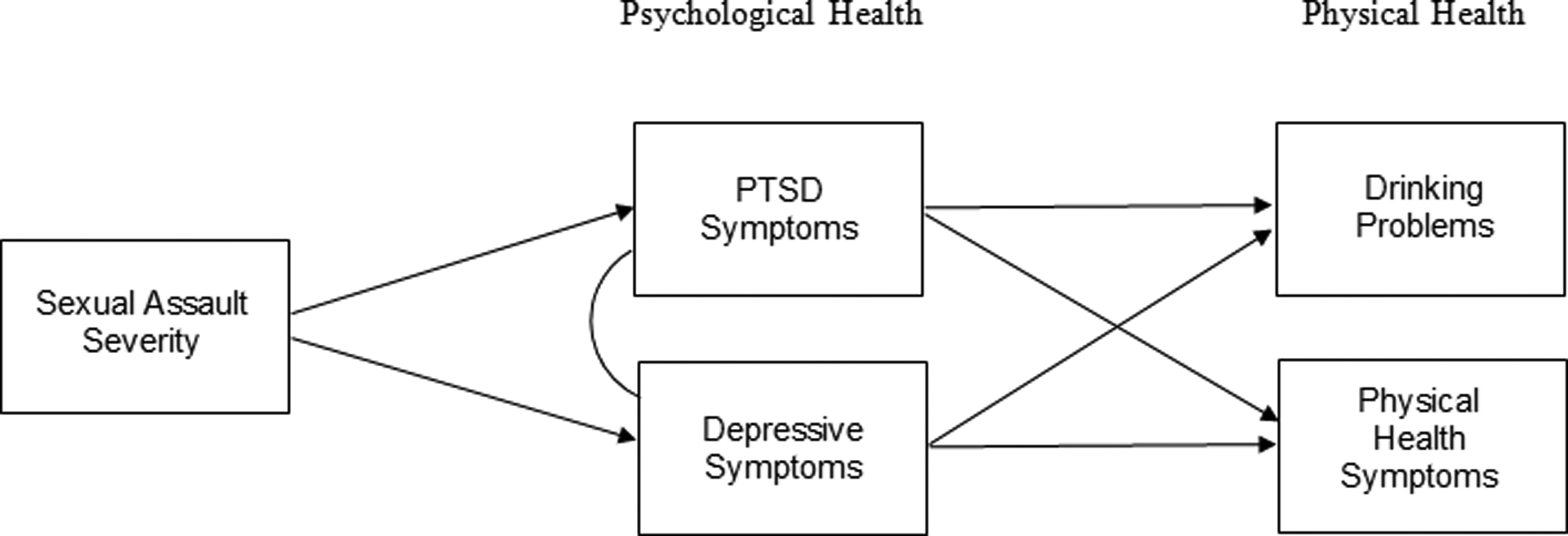
Hypothesized Model of Sexual Assault Severity as it Relates to PTSD Symptoms, Depressive Symptoms, Physical Health Symptoms, and Drinking Problems (N = 221)
The second goal of this study was to examine similarities and differences in the relationships between sexual assault severity and health for African American and Caucasian survivors. The relationships between severity, psychological health, and physical health depicted in Figure 1 were expected to be significant for both African American and Caucasian survivors. Based on general theories of chronic stress and the weathering hypothesis (Geronimus, 1992), we hypothesized that the magnitude of these relationships would be stronger for African American survivors as compared to Caucasian survivors. Based on past research, we also hypothesized that mean levels of depressive symptoms and drinking problems would be higher for Caucasian women as compared to African American women (Delker et al., 2016; Grant et al., 2015; Hasin, Goodwin, Stinson, & Grant, 2005).
Method
Participants
To meet the goals of the original study, participants were required to be women who self-identified as African American or Caucasian between the ages of 18–49, who were currently single, but had dated a man in the last 2 years and who had lived in the United States for at least 10 years (Abbey, BeShears, Clinton-Sherrod, & McAuslan, 2004). This study was restricted to the 221 women who reported during the course of the interview that they experienced some form of sexual assault since the age 14. Of these women, 54.8% (n = 121) identified as African American and 45.2% (n = 100) identified as Caucasian. The mean age of participants was 31.84 years at the time of the study (SD = 9.64). Ninety-three percent of participants had at least a high school degree. Participants’ median annual household income, measured in $5,000 increments, was in the $30,000 to $35,000 range.
Procedure
Random digit dialing was used by Wayne State University’s Center for Urban Studies to identify eligible participants in the metropolitan Detroit area. This region of approximately 4 million residents includes a broad range of suburban and semi-rural communities in southeastern Michigan, as well as the city of Detroit. African Americans were oversampled to achieve a sample that was approximately half African American and half Caucasian participants. The sample was restricted to the two largest ethnic groups in the area so that subgroup sample sizes would be large enough for multivariate data analyses.
Participants were screened by telephone to insure they met the eligibility criteria described above. During the screening call, participants were told about the study’s general focus on women’s positive and negative dating experiences. Eligible participants were scheduled for an in person interview at a location of their choosing, with a female interviewer of the same ethnicity. Interviews were conducted in participants’ homes, restaurants, coffee shops, and in a private office on Wayne State University’s campus. Computer-assisted self-interviews were conducted to increase participants’ comfort disclosing sensitive information. Interviewers reviewed the consent form, explained how to use the computer, and were available to answer questions. The consent form described the scope of the measures, including questions on unwanted sexual activity. Participants were provided with contact information for several counseling centers and told they could stop the study at any time if it was too stressful (none did). It took participants approximately 90 minutes to complete the survey. After the interview, participants were compensated $50 for their time.
Measures
Demographic information.
Demographic information was collected regarding participants’ age, education, and income.
Sexual assault victimization.
All participants included in this paper experienced at least one type of sexual victimization as assessed by a modified version of the Sexual Experiences Survey (SES; Koss, Gidycz, & Wisniewski, 1987). The modified SES (Abbey et al., 1996; Abbey et al., 2004) contains 17 behaviorally-specific items and measures an array of sexual assault experiences since age 14, including: forced sexual contact and penetrative sex (i.e., vaginal, anal, and/or oral sex) via various tactics (i.e., verbal coercion, physical force, use of alcohol/substances). The SES is the most frequently used measure of sexual assault; the measure has demonstrated good validity and reliability (Koss et al., 1987). Because all participants in this study experienced at least one sexual assault, for each item, participants indicated the number of times they experienced the event ranging from (0) never to (5) five or more times. Participants also reported their age at the time.
Sexual assault severity.
Participants answered a detailed list of questions about one sexual assault incident. If more than one occurred, a computer algorithm selected one incident based on the assault type (ascending order of severity: forced sexual contact, verbally coerced intercourse, attempted rape, completed rape) and recency of the assault. Severity of the incident was assessed using a combination of seven different indicators which are described below. These questions were developed by the researchers based on past research (Abbey et al., 1996; Muehlenhard & Linton, 1987; Weaver & Clum, 1995).
A checklist of 14 tactics was used to assess force. Participants were asked to identify types of pressure or force the perpetrator used, such as “pressure or coercion with words,” and “use of a weapon or object to hurt you.” Responses were summed.
A checklist of 8 items was used to assess injuries. Sample injuries include: bruises, black eye(s), vaginal tearing or bleeding, and broken bones. Responses were summed.
A checklist of 5 threatening actions was used to assess post-assault threat. Sample items include: “Did he threaten you after the unwanted sexual activity occurred?” and “Did he continue to physically hurt you after the unwanted sexual activity occurred, for example, hitting you, pulling your hair, throwing you down?” Responses were summed.
A checklist of 20 items was used to assess immediate negative affect. Sample feelings include: ashamed, disgusted, dirty, embarrassed, and degraded. Responses were summed.
To assess the extent to which the assault was considered a sexual offense, participants were asked, “Which number best describes the extent to which you consider what happened to be rape?” and “Which number best describes the extent to which you consider what happened to be a sexual offense?” The highest value from either item was used. Response options ranged from (1) definitely not rape (sexual offense) to (7) definitely rape (sexual offense).
To assess perceived seriousness at the time and seriousness now, participants were asked, “Which number best describes how serious this experience was to you at the time?” and “Which number best describes how serious this experience is for you now?” Response options ranged from (1) not very serious to (7) very serious.
To assess the extent to which the incident disrupted their relationships with men, participants were asked, “To what extent did this experience disrupt your relationships with men?” Response options ranged from (1) not at all to (5) very much.
To create an index of sexual assault severity, principal components analysis (PCA) with varimax rotation was performed. The PCA revealed 2 factors: subjective assault characteristics (immediate negative affect, extent to which assault was considered a sexual offense, perceived serious now/ at the time, and the extent to which the assault disrupted their relationships with men) and objective assault characteristics (perpetrator’s force, sum of injuries, and post-assault threat) loading on a second factor. However, all of the variables and the two factors were strongly correlated with one another. Thus, a second factor analysis was conducted that restricted extraction of factors to 1. All of the subjective and objective assault characteristics had factor loadings of at least .35. Therefore, the single factor solution was used to create a single indicator of assault severity. Z-scores were computed so that all variables were on the same scale. The index has good reliability with a Cronbach’s alpha of .84.
PTSD symptoms.
Frequency of posttraumatic stress symptoms was assessed using Davidson’s Trauma Scale (Davidson et al., 1997). This measure contains 17 items based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; American Psychiatric Association, 1994). Participants were instructed to answer the questions regarding the sexual assault that they described in detail. A sample item is: “How frequently have you had painful images, memories, or thoughts of the event?” Response options ranged from (1) not at all to (5) all of the time. Participants’ mean score was computed. This scale demonstrated a high Cronbach’s alpha of .99 in Davidson et al. (1997), and has a Cronbach’s alpha of .95 in the current study.
Depressive symptoms.
An abbreviated version of Beck’s Depression Inventory was used to assess depressive symptoms (Beck, 1967). Only 14 of the measure’s original 20 items were used because the focus was not on determining clinical diagnoses in this community sample. The measure maintained a high Cronbach’s alpha of .96 in the current study. Participants were instructed to choose one statement in each group which best describes how they have been feeling during the past week, including that day. For example, in one group options are: (0) I do not feel sad, (1) I feel sad, (2) I am sad all the time and I can’t snap out of it, and (3) I am so sad or unhappy that I can’t stand it. A composite score was computed by summing all of their responses.
Physical health symptoms.
The research team developed a list of 21 general somatic and gynecological symptoms based on the Somatization subscale of the Hopkins Symptom Checklist (Lipman, Covi, & Shapiro, 1979), as well as symptoms commonly reported by sexual assault survivors (Golding et al., 1997; Plichta & Falik, 2001). Participants were instructed to indicate how much they have been bothered by each symptom during the past week. Examples of symptoms include indigestion or stomach discomfort, headaches, back pain, painful menstrual periods, and pain or discomfort when having sex. Response options were: (0) not at all, (1) mildly, it did not bother me much, (2) moderately, it was very unpleasant but I could stand it, and (3) severely, I could barely stand it. Participants’ mean score was computed. This scale has excellent reliability with a Cronbach’s alpha of .90 in the current study.
Drinking problems.
Drinking problems were assessed using Hilton’s (1987) 13-item Problematic Drinking subscale. This measure was selected because it was developed for use in a general sample of adults by the National Institute on Alcohol Abuse and Alcoholism. Participants are asked whether or not they experienced each drinking-related problems in the past 12 months. Sample items include: “I need more alcohol than I used to, to get the same effect as before.” and “Once I started drinking it was difficult for me to stop (before I became completely intoxicated).” Response options were (0) no or (1) yes, and responses were summed. This scale has a Cronbach’s alpha of .77 in the current study.
Results
Descriptive Analyses and Comparison of Means
The types of sexual assault described by African American and Caucasian women were comparable with 23% of African Americans and 26% of Caucasians describing a completed rape, 7% of African Americans and 7% of Caucasians describing an attempted rape, 32% of African Americans and 35% of Caucasians describing verbally coerced penetrative sex, and 37% of African Americans and 32% of Caucasians describing forced sexual contact, (χ2 = .75, p = .86).
A series of one-way ANOVAs were conducted to determine if there were significant differences in African American and Caucasian women’s income, education, age, or number of years since the assault. The only significant difference was for income. Caucasian survivors (M = $17,922.41; SD = $13,530.00) had significantly higher incomes than did African American survivors (M = $11,513.32; SD = $11,396.97; F (1,219) = 14.61, p < .001). Thus, income was included as a covariate in all subsequent analyses.
Next, a series of one-way ANCOVAs were conducted to determine if there were any differences in the levels of sexual assault severity, PTSD symptoms, depressive symptoms, drinking problems, and physical health symptoms reported by African American and Caucasian survivors. There was only one significant difference. Controlling for income, Caucasians reported more depressive symptoms (M = 7.34, SD = 8.41) than did African Americans (M = 3.93, SD = 6.09; F 1,219) = 12.14, p = .001).
Bivariate Analyses
Table 1 is a partial correlation matrix (controlling for income) that displays the relationships between the study variables separately for African American and Caucasian survivors. Among African Americans, severity was significantly positively correlated with PTSD symptoms, depressive symptoms, and physical health. However, among Caucasians, severity was only significantly correlated with PTSD symptoms. For both groups of survivors, PTSD symptoms, depressive symptoms, and physical health symptoms were significantly correlated with each other. Both PTSD symptoms and depressive symptoms were significantly positively correlated with drinking problems among African Americans, whereas those relationships were not statistically significant among Caucasians. Further, drinking problems was significantly positively correlated with physical health symptoms for African Americans, however there was not a statistically significant relationship for Caucasians.
Table 1.
Partial Correlations among Study variables for African American (n = 121) and Caucasian (n = 100) Survivors
| Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Sexual assault severity | ---- | .57*** | .34*** | .14 | .23* |
| 2. PTSD symptoms | .59*** | ---- | .62*** | .25** | .43*** |
| 3. Depressive symptoms | .01 | .29** | ---- | .19* | .49*** |
| 4. Drinking problems | −.02 | .01 | .13 | ---- | .31** |
| 5. Physical health symptoms | −.01 | .26*** | .37*** | .07 | ---- |
Note: Matrix is controlling for income.
p < .05.
p < .01.
p < .001.
Correlations for African Americans are located on the top half of the matrix. Correlations for Caucasians are located on the bottom half of the matrix.
Multi-group Comparison Analysis
It was hypothesized that the relationships between sexual assault severity and health outcomes would be mediated by psychological health outcomes, and that ethnicity would moderate these relationships (see Figure 1). To examine the hypothesized model, path analyses were conducted using LISREL 8.80 with maximum likelihood method of estimation. Partial correlations, controlling for income and assault recency, and standard deviations were entered into LISREL to perform analyses. Latent constructs were formed using total aggregation with reliability correction (Williams & O’Boyle, 2008). Specifically, the sum or average of each measure was used as a single indicator of the latent variable. In the path model, theta-epsilon values were computed using the formula (1-rels)σs2, and lambda values were set to 1.
First, the model was tested for the overall sample. There was one nonsignificant path from depressive symptoms to drinking problems which was omitted (preliminary analyses indicated it was nonsignificant for both African Americans and Caucasians). This revised model was then examined using multi-group analysis so the (in)equality of parameters for African American and Caucasian survivors could be evaluated. The fully constrained model assumed no differences between the groups, whereas the unconstrained model allowed for differences. Results of a chi-square difference test indicated that the groups are different at the model level (χ2 = 23.23, df = 6, p < .05), thus providing support to retain the unconstrained model.
Because there was evidence for moderation at the path level, separate models for the two groups were compared, and Fischer z-scores were calculated to determine which paths significantly differ across groups. This information can be seen in Figure 2. The overall models for both African Americans (χ2 = 6.45, df = 4, RMSEA = 0.07, CFI = .99) and Caucasians (χ2 = 4.22, df = 4, RMSEA = 0.02, CFI = 1.00) indicated good model fit. The path from severity to PTSD symptoms was statistically significant for African Americans and Caucasians, and the path was not significantly different between groups. The path from severity to depressive symptoms was significant for African Americans, but not for Caucasians. The difference between the groups was statistically significant (Fisher’s z = 3.00, p <.01). The path from PTSD symptoms to physical health symptoms was statistically significant for the overall sample, however it was only marginally significant for both groups, and the groups were not significantly different. The path from PTSD symptoms to drinking problems was significant for African Americans, but not for Caucasians. Moreover, this path was significantly different between groups (Fisher’s z = 2.11, p <.05). Finally, the path from depressive symptoms to physical health symptoms was statistically significant for both groups, and the groups were not significantly different.
Figure 2. Revised Model of Sexual Assault Severity as it Relates to PTSD Symptoms, Depressive Symptoms, Physical Health Symptoms, and Drinking Problems (N = 221): Multi-group Comparison.
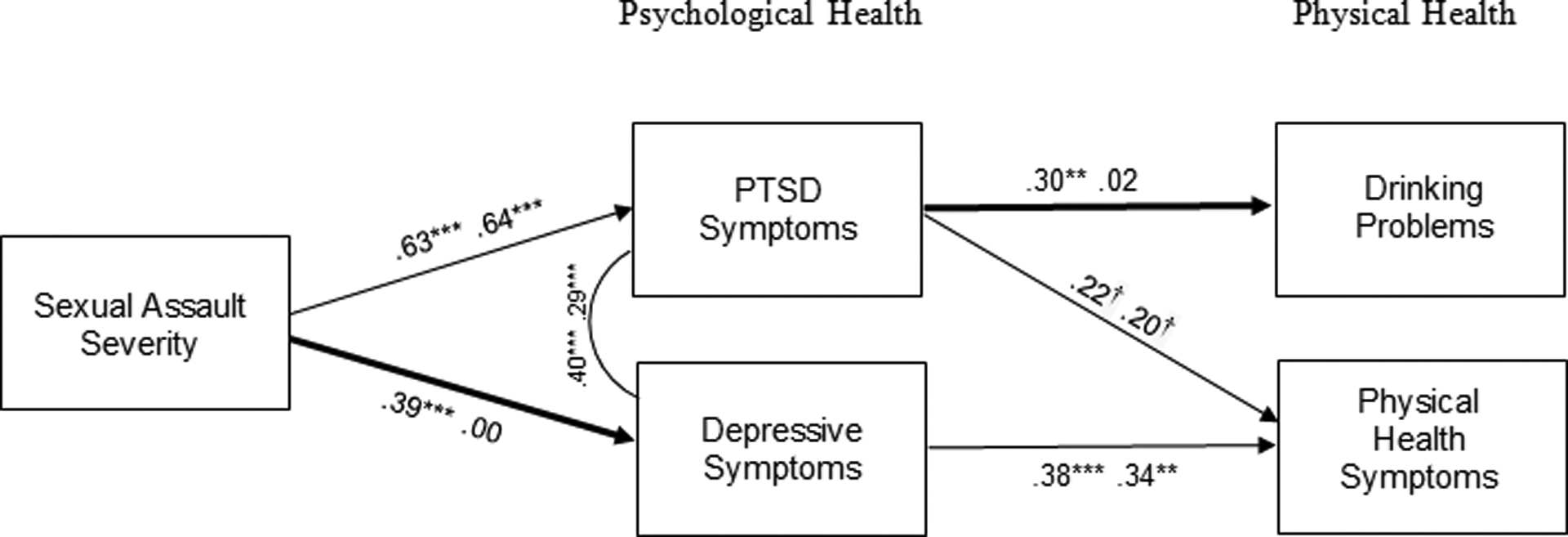
Note: Standardized loadings shown. Path coefficients for African Americans appear first; path coefficients for Caucasians appear second. Pathways that are significantly different between groups have a bolded arrow. †p = .06. *p < .05. **p < .01. ***p < .001.
Table 2 provides the direct, indirect and total effects of sexual assault severity and psychological health on drinking problems and physical health symptoms. For African American survivors, sexual assault severity had significant indirect effects on drinking problems and physical health symptoms. In contrast, these indirect effects were not significant for Caucasian survivors. The model predicted 30% of the variance for physical health symptoms among African Americans and 20% of the variance among Caucasians. However, the model did not account for much variance in drinking problems (9% for African Americans and 1% for Caucasians).
Table 2.
Standardized Direct, Indirect, and Total Effects of Study Variables on Physical Health Symptoms and Drinking Problems
| African Americans | Caucasians | ||||||
|---|---|---|---|---|---|---|---|
| Direct Effect | Indirect Effect | Total Effect | Direct Effect | Indirect Effect | Total Effect | ||
| Drinking problems | |||||||
| Severity | x | 0.19 | 0.19 | x | 0.06 | 0.06 | |
| PTSD symptoms | 0.30 | x | 0.30 | 0.02 | x | 0.02 | |
| Physical health symptoms | |||||||
| Severity | x | 0.29 | 0.29 | x | 0.13 | 0.13 | |
| PTSD symptoms | 0.22 | x | 0.22 | 0.20 | x | 0.20 | |
| Depressive symptoms | 0.38 | x | 0.38 | 0.34 | x | 0.34 | |
Note: PTSD = posttraumatic stress disorder. Values in bold are significant at p < .05. Direct, indirect, and total effects are provided for the final model, which omits the nonsignificant path from Depression to Drinking Problems.
Discussion
Many sexual assault survivors experience psychological and physical health problems for years after the incident. The study described in this paper had two primary goals. The first goal was to determine if sexual assault severity was associated with the strength of survivors’ psychological health problems, which in turn were expected to be associated with the strength of their physical health concerns. The second goal was to examine the extent to which the interrelationships between assault severity, psychological health, and physical health were similar for African American and Caucasian survivors. Although we had expected the magnitude of these relationships to be stronger for African American survivors as compared to Caucasian survivors, instead we found in path analyses that some relationships were comparable (i.e., links between sexual assault severity and PTSD symptoms; PTSD symptoms and physical health symptoms; depressive symptoms and physical health symptoms). Other relationships only existed in path analyses for African American survivors (i.e., links between sexual assault severity and depressive symptoms; PTSD symptoms and drinking problems). Contrary to hypothesis, no relationship was found between depressive symptoms and drinking problems for African American or Caucasian survivors. Overall, the proposed model explained more variance in the health outcomes of African American survivors than Caucasian survivors. These differences cannot be primarily explained by differences in mean levels of experienced distress because the mean levels of perceived assault severity, PTSD symptoms, drinking problems, and physical health symptoms were comparable for African American and Caucasian survivors. Caucasian survivors’ experienced higher levels of depressive symptoms than did African American survivors and African American survivors had lower household incomes than did Caucasian survivors.
These findings might be explained by differences in the coping resources available to African American and Caucasian survivors in this sample. Income is associated with access to a variety of coping resources that might have mitigated the impact of sexual assault severity on participants’ psychological and physical health (Habarth, Graham-Bermann, & Bermann, 2009). Although many survivors report that they are treated poorly by providers when they seek psychological and/or physical health care services after the sexual assault, low income minority women are particularly likely to receive inadequate care, thus exacerbating the relationships between assault severity and negative health outcomes (Dovidio et al., 2008; Penner et al., 2009). Because this study relied on an existing dataset that did not measure coping resources and health care providers’ responses, these post hoc explanations cannot be evaluated in this article. Given the paucity of research examining ethnic similarities and differences in response to sexual assault, additional mixed method research is needed that assesses a wide range of coping resources and includes open ended questions that help researchers better understand the challenges faced by survivors from varied ethnic and cultural backgrounds.
Strengths and Limitations
A strength of the present study is the sampling methodology. In this study, a community sample of women was recruited for a study of dating relationships. Many researchers post advertisements for women who want to be in a study of sexual assault survivors. Women who volunteer to discuss a past sexual assault self-identify as survivors, which may be a sign of good adjustment (because they feel able to discuss it with a stranger) or poor adjustment (because they are hoping the interview might be therapeutic). Another strength was the inclusion of a sufficiently large sample of African American and Caucasian survivors to conduct complex multivariate analyses.
One novel aspect of the present study was the use of an index of sexual assault severity, which included a variety of subjective and objective components of severity. Although they fit together well in a single index, it would be valuable in future research to determine if different components of severity have a differential impact on recovery sequelae. Future research is needed to determine if there are individual differences in the impact of objective and subjective aspects of severity. For some survivors, physical harm may have the greatest impact on recovery; whereas for other survivors, long-term disruption in relationships with men may have the greatest impact on recovery.
The present study also has some limitations. Although participants were assured their data would be confidential, it is possible that some participants underreported unwanted sexual experiences and post-assault experiences due to embarrassment, perceived stigma, or discomfort. In addition, participants were approximately 9 years post-assault on average at the time of the study, which could have affected recall. Although this is fairly typical of other studies of sexual assault victimization (e.g, 13 years post-assault in Najdowski & Ullman, 2009), assessment closer to the time of victimization would reduce the potential for recall bias. In addition, the current study did not assess culturally specific factors that might contribute to assault recovery, for instance: ethnic identity, race-based stress, and adherence to cultural schemas and attributions. Neville, Heppner, Oh, Spanierman, and Clark (2004) found that African American women who endorsed more cultural blame beliefs (e.g., “People think Black women are sexually loose”), blamed themselves more for the assault, which in turn was associated with lower self-esteem. Few studies have investigated ethnicity-related constructs and processes related to sexual assault recovery, thus, this is an important direction for future research.
Implications for Treatment and Policy
Although these findings need to be replicated and extended to other ethnic and cultural groups, they highlight the need for researchers, clinicians, advocates, policy makers, and community agencies to collaborate to establish comprehensive, culturally-inclusive intervention programs. These efforts should be grounded in a theoretical framework, such as the culturally inclusive ecological model of sexual assault recovery (Neville & Heppner, 1999). This model attempts to contextualize sexual assault recovery by examining how cultural variables affect women prior to the assault (e.g., socio-economic resources, psychological and physical health status, and general coping strategies), assault characteristics (e.g., relationship to the perpetrator and assault severity), and after the assault (e.g., treatment received from providers, availability of services). Health disparities are implicitly addressed by this model; however, it is important to explicitly consider how the overall burden of chronic stress can disproportionately affect African American and other ethnic minority survivors’ capacity to cope with sexual assault.
Acknowledgments
This research was supported by a grant from the National Institute on Alcohol Abuse and Alcoholism awarded to the second author (R01 AA11346).
References
- Abbey A, BeShears R, Clinton-Sherrod AM, & McAuslan P (2004). Similarities and differences in women’s sexual assault experiences based on tactics used by the perpetrator. Psychology of Women Quarterly, 28, 323–332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Abbey A, Jacques-Tiura AJ, & Parkhill MR (2010). Sexual assault among diverse populations of women: Common ground, distinctive features, and unanswered questions In Landrine H Russo N (Eds.), Handbook of diversity in feminist psychology (pp. 391–425). New York, NY US: Springer Publishing Co. [Google Scholar]
- Abbey A, Ross LT, McDuffie D, & McAuslan P (1996). Alcohol and dating risk factors for sexual assault among college women. Psychology of Women Quarterly, 20, 147–169. [Google Scholar]
- Acierno R, Brady K, Gray M, Kilpatrick DG, Resnick H, & Best C (2002). Psychopathology following interpersonal violence: A comparison of risk factors in older and younger adults. Journal of Clinical Geropsychology, 8(1), 13–23. [Google Scholar]
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders. Washington, DC: American Psychiatric Association. [Google Scholar]
- Beck AT (1967). Depression: Clinical, experimental, and theoretical aspects (Vol. 32). University of Pennsylvania Press. [Google Scholar]
- Breiding MJ, Smith SG, Basile KC, Walters M, Chen J, & Merrick MT (2014). Prevalence and characteristics of sexual violence, stalking, and intimate partner violence victimization - National Intimate Partner and Sexual Violence Survey, United States, 2011. Morbidity and Mortality Weekly, 63(8), 1–18. [PMC free article] [PubMed] [Google Scholar]
- Bryant-Davis T, Chung H, & Tillman S (2009). From margins to the center: Ethnic minority women and the mental health effects of sexual assault. Trauma, Violence, and Abuse, 10(4), 330–357. [DOI] [PubMed] [Google Scholar]
- Campbell R, Dworkin E, & Cabral G (2009). An ecological model of the impact of sexual assault on women’s mental health. Trauma, Violence, and Abuse, 10(3), 225–246. [DOI] [PubMed] [Google Scholar]
- Campbell R, Greeson MR, Raja Bybee, D., & Raja S (2008). The co-occurrence of childhood sexual abuse, adult sexual assault, intimate partner violence, and sexual harassment: A mediational model of posttraumatic stress disorder and physical health outcomes. Journal of Consulting and Clinical Psychology, 76(2), 194–207. [DOI] [PubMed] [Google Scholar]
- Cappell H, & Greeley J (1987). Alcohol and tension reduction: An update on research and theory In Blane HT & Leonard KE (Eds.). Psychological theories of drinking and alcoholism (pp. 15–54). New York: Guilford Press. [Google Scholar]
- Chyu L, & Upchurch DM (2011). Racial and ethnic patterns of allostatic load among adult women in the United States: Findings from the National Health and Nutrition Examination Survey 1999–2004. Journal of Women’s Health, 20(4), 575–583. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clum GA, Calhoun KS, & Kimberling R (2000). Associations among symptoms of depression and posttraumatic stress disorder and self-reported health in sexually assaulted women. Journal of Nervous and Mental Disease, 188, 671–678. [DOI] [PubMed] [Google Scholar]
- Cooper ML, Frone MR, Russell M, & Mudar P (1995). Drinking to regulate positive and negative emotions: A motivation model of alcohol use. Journal of Personality and Social Psychology, 69(5), 990–1005. [DOI] [PubMed] [Google Scholar]
- Davidson JR, Book SW, Colket JT, Tupler LA, Roth S, David D, … & Feldman ME (1997). Assessment of a new self-rating scale for post-traumatic stress disorder. Psychological Medicine, 27(1), 153–160. [DOI] [PubMed] [Google Scholar]
- Delker E, Brown Q, & Hasin DS (2016). Alcohol consumption in demographic subpopulations: An epidemiologic overview. Alcohol Research: Current Reviews, 38 (1), 1–7. [PMC free article] [PubMed] [Google Scholar]
- Dovidio JF, Penner LA, Albrecht TL, Norton WE, Gaertner SL, & Shelton JN (2008). Disparities and distrust: The implications of psychological processes for understanding racial disparities in health and health care. Social Science & Medicine, 67(3), 478–486. [DOI] [PubMed] [Google Scholar]
- George WH, & Martínez LJ (2002). Victim blaming in rape: Effects of victim and perpetrator race, type of rape, and participant racism. Psychology of Women Quarterly, 26(2), 110–119. [Google Scholar]
- Geronimus AT (1992). The weathering hypothesis and the health of African-American women and infants: Evidence and speculations. Ethnicity Disorders, 2, 207–221. [PubMed] [Google Scholar]
- Geronimus AT, Hicken M, Keene D, & Bound J (2006). “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. American Journal of Public Health, 96(5), 826–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Golding JM, Cooper ML, & George LK (1997). Sexual assault history and health perceptions: Seven general population studies. Health Psychology, 16(5), 417–425. [DOI] [PubMed] [Google Scholar]
- Golding JM (1999). Sexual-assault history and long-term physical health problems: Evidence from clinical and population epidemiology. Current Directions in Psychological Science, 8(6), 191–194. [Google Scholar]
- Grant BF, Goldstein RB, Saha TD, Chou P, Jung J, Zhang H, ... Hasin DS (2015). Epidemiology of DSM-5 alcohol use disorder results from the national epidemiolic survey on alcohol and related conditions III (2015). Journal of the American Medical Association Psychiatry, 72, 757– 766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Habarth JM, Graham-Bermann SA, & Bermann EA (2009). Coping in context: Community and natural resources in low-income women’s environments. Environment and Behavior, 41(2), 205–232. [Google Scholar]
- Hasin DS, Goodwin RD, Stinson FS, & Grant BF (2005). Epidemiology of major depressive disorder. Archives of General Psychiatry, 62, 1097– 1106. [DOI] [PubMed] [Google Scholar]
- Hilton ME (1987). Demographic characteristics and the frequency of heavy drinking as predictors of self‐reported drinking problems. British Journal of Addiction, 82(8), 913–925. [DOI] [PubMed] [Google Scholar]
- Kaukinen C, & DeMaris A (2005). Age at first sexual assault and current substance use and depression. Journal of Interpersonal Violence, 20(10), 1244–1270. [DOI] [PubMed] [Google Scholar]
- Kilpatrick DG, Acierno R, Resnick HS, Saunders BE, & Best CL (1997). A 2-year longitudinal analysis of the relationships between violent assault and substance use in women. Journal of Consulting and Clinical Psychology, 65(5), 834–847. [DOI] [PubMed] [Google Scholar]
- Kilpatrick DG, Saunders BE, Veronen LJ, Best CL, & Von JM (1987). Criminal victimization: Lifetime prevalence, reporting to police, and psychological impact. Crime & Delinquency, 33(4), 479–489. [Google Scholar]
- Kilpatrick DG, Resick PA, & Veronen LJ (1981). Effects of a rape-experience: A longitudinal study. Journal of Social Issues, 37(4), 105–120. [Google Scholar]
- Kimberling R & Calhoun KS (1994). Somatic symptoms, social support, and treatment seeking sexual assault victims. Journal of Consulting and Clinical Psychology, 62, 333–340. [DOI] [PubMed] [Google Scholar]
- Koss MP, Figueredo AJ, & Prince RJ (2002). Cognitive mediation of rape’s mental, physical, and social health impact: Tests of four models in cross-sectional data. Journal of Consulting and Clinical Psychology, 70(4), 926–941. [PubMed] [Google Scholar]
- Koss M, Gidycz CA, & Wisniewski N (1987). The scope of rape: Incidence and prevalence of sexual aggression and victimization in a national sample of higher education students. Journal of Consulting and Clinical Psychology, 55, 162–170. [DOI] [PubMed] [Google Scholar]
- Lipman RS, Covi L, & Shapiro AK (1979). The Hopkins Symptom Checklist (HSCL): Factors derived from the HSCL-90. Journal of Affective Disorders, 1, 9–24. [DOI] [PubMed] [Google Scholar]
- Littleton HL, Grills-Taquechel AE, Buck KS, Rosman L, & Dodd JC (2013). Health risk behavior and sexual assault among ethnically diverse women. Psychology of Women Quarterly, 37(1), 7–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Littleton HL, & Ullman SE (2013). PTSD symptomatology and hazardous drinking as risk factors for sexual assault revictimization: Examination in European American and African American women. Journal of Traumatic Stress, 26(3), 345–353. [DOI] [PubMed] [Google Scholar]
- Lown EA, Nayak MB, Korcha RA, & Greenfield TK (2011). Child physical and sexual abuse: A comprehensive look at alcohol consumption patterns, consequences, and dependence from the National Alcohol Survey. Alcoholism: Clinical and Experimental Research, 35(2), 317–325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackey T, Sereika SM, Weissfeld LA, Hacker SS, Zender JF, & Heard SL (1992). Factors associated with long-term depressive symptoms of sexual assault survivors. Archives of Psychiatric Nursing, 5(1), 10–25. [DOI] [PubMed] [Google Scholar]
- McFarlane J, Melecha A, Watson K, Gist J, Batten E, Hall I, & Smith S (2005). Intimate partner sexual assault against women: Frequently, health consequences, and treatment outcomes. Obstetrics & Gynecology, 105(1), 99–108. [DOI] [PubMed] [Google Scholar]
- Muehlenhard CL, & Linton MA (1987). Date rape and sexual aggression in dating situations: Incidence and risk factors. Journal of Counseling Psychology, 34, 186–196. [Google Scholar]
- Najdowski CJ, & Ullman SE (2009). PTSD symptoms and self-rated recovery among adult sexual assault survivors: The effects of traumatic life events and psychosocial variables. Psychology of Women Quarterly, 33, 43–53. [Google Scholar]
- Neville HA, & Heppner MJ (1999). Contextualizing rape: Reviewing sequelae and proposing a culturally inclusive ecological model of sexual assault recovery. Applied and Preventive Psychology, 8, 41–62. [Google Scholar]
- Neville HA, Heppner MJ, Oh E, Spanierman LB, & Clark M (2004). General and culturally specific factors influencing black and white rape survivors’ self-esteem. Psychology of Women Quarterly, 28, 83–94. [Google Scholar]
- Penner LA, Dovidio JF, Edmondson D, Dailey RK, Markova T, Albrecht TL, & Gaertner SL (2009). The experience of discrimination and black-white health disparities in medical care. Journal of Black Psychology, 35(2), 180–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plichta SB, & Falik M (2001). Prevalence of violence and its implications for women’s health. Women’s Health Issues, 11(3), 244–258. [DOI] [PubMed] [Google Scholar]
- Resnick HS, Kilpatrick DG, Dansky BS, Saunders BE, & Best CL (1993). Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women. Journal of Consulting and Clinical Psychology, 61(6), 984–991. [DOI] [PubMed] [Google Scholar]
- Rothbaum B, Foa E, Murdock T, Riggs D, & Walsh W (1992). A prospective examination of post-traumatic stress disorder in rape survivors. Journal of Traumatic Stress, 5, 455–475. [Google Scholar]
- Steenkamp MM, Dickstein BD, Salters-Pedneault K, Hofmann SG, & Litz BT (2012). Trajectories of PTSD symptoms following sexual assault: Is resilience the modal outcome? Journal of Traumatic Stress, 25, 469–474. [DOI] [PubMed] [Google Scholar]
- Ullman SE, & Brecklin LR (2002). Sexual assault history, PTSD, and mental health service seeking in a national sample of women. Journal of Community Psychology, 30(3), 261–279. [Google Scholar]
- Ullman SE, & Filipas HH (2001). Predictors of PTSD symptom severity and social reactions in sexual assault survivors. Journal of Traumatic Stress, 14(2), 369–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ullman SE, Filipas HH, Townsend SM, & Starzynski LL (2005). Trauma exposure, posttraumatic stress disorder and problem drinking in sexual assault survivors. Journal of Studies on Alcohol, 66(5), 610–619. [DOI] [PubMed] [Google Scholar]
- Wadsworth P, & Records K (2013). A review of the health effects of sexual assault on African American women and adolescents. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 42(3), 249–273. [DOI] [PubMed] [Google Scholar]
- Weaver TL, & Clum GA (1995). Psychological distress associated with interpersonal violence: A meta-analysis. Clinical Psychology Review, 15(2), 115–140. [Google Scholar]
- Williams LJ & O’Boyle J (2008). Measurement models for linking latent variables and indicators: A review of human resource management research using parcels. Human Resource Management Review, 18, 233–242. [Google Scholar]
- World Health Organization (2013). Global and regional estimates of violence against women: Prevalence and health effects of intimate partner violence and non-partner sexual violence. Geneva, World Health Organization. [Google Scholar]
- Zinzow HM, Amstadter AB, McCauley JL, Ruggiero KJ, Resnick HS, & Kilpatrick DG (2011). Self-rated health in relation to rape and mental health disorders in a national sample of college women. Journal of American College Health, 59(7), 588–594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zoellner LA, Goodwin ML, & Foa EB (2000). PTSD severity and health perceptions in female survivors of sexual assault. Journal of Traumatic Stress,13(4), 635–649. [DOI] [PubMed] [Google Scholar]