

1. Introduction
Injuries kill more than 180 000 people each year in the USA—that’s 1 death every 3 minutes. Regardless of sex, race, or economic status, violence and injuries affect everyone. From ages 1~44, more Americans die from violence and injuries—such as motor vehicle crashes, falls or homicides—than from any other cause, including infectious and non-communicable diseases[1] (Fig 1). And injury deaths are only part of the picture. Millions of Americans are injured each year and survive. Many of them are faced with life-long health, social and financial problems.
Fig 1.
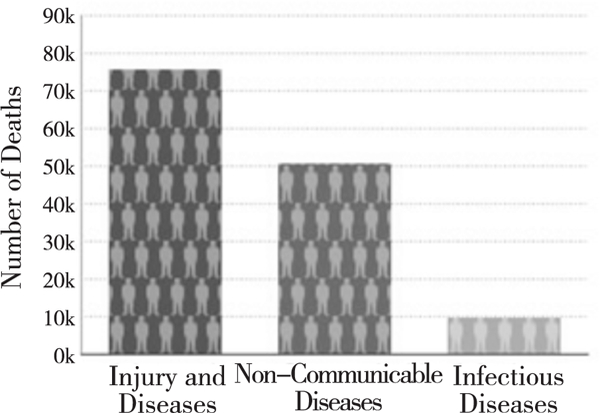
Injury Deaths Compared to Other Leading Causes of Death for Persons Ages 1~44, United States, 2010
In 1985, the US National Research Council and the Institute of Medicine (IOM) recognized the need for a coordinated effort to prevent injuries in the United States[2]. They identified CDC as the federal agency best suited to lead injury research. CDC had a strong history of interdisciplinary research, data collection and analysis, information sharing, and relationships with states-elements the Research Council and IOM deemed important. And unlike other federal agencies involved in injury prevention, CDC had no regulatory or enforcement role. In 1997, the IOM Committee on Injury Prevention and Control recommended that no one agency could effectively serve as the sole leader for injury. Rather, agencies should collaborate in injury prevention and control activities, with each agency leading in its area of expertise. CDC’s Injury Center now functions as the focal point and lead agency within the US Department of Health and Human Services for preventing injuries.
2. Key Focusing Areas of National Center for Injury Prevention and Control
The mission of the National Center for Injury Prevention and Control is to prevent injuries and violence and reduce their consequences.
For more than 20 years, CDC’s Injury Center has helped protect Americans from injury and violence and the threat injuries pose to communities [3]. CDC’s Injury Center is the nation’s leading authority on injury and violence. The Center studies unintentional injuries and violence and researches the best ways to prevent them, applying science for real-world solutions to keep people safe, healthy, and productive[4]. Scientific and program staff of the center conduct research and manage programs in the States and communities. An extramural program funds researchers and practitioners outside CDC to conduct programs that help prevent injuries at the State and community level.
2.1. Identifying and Monitoring the Injury Problem
The Injury Center develops and uses cutting-edge data systems to track injuries and deaths by age, race, and a host of other factors. These powerful tools ensure that prevention initiatives are guided by the best available science and research. By studying patterns in data, we can better understand the nature and scope of an injury or violence problem, measure how well prevention efforts are working, and identify emerging issues. Through the national violent death reporting system, for instance, the center gathers, shares, and links comprehensive state data on violent deaths.
2.2. Conducting Research to Guide Decision Making
The Injury Center conducts and funds a wide range of research that provides vital knowledge about what works in violence and injury prevention. This knowledge informs decision making about programs and policies to reduce violence and injuries, facilitating wise investments of prevention resources. For example, Injury Center research showed that lowering the illegal Blood Alcohol Level (BAC) from 0.10% to 0.08% would be effective in reducing alcohol-related traffic deaths [5]. This finding[6] served as a foundation for decision making that led to all US States adopting the 0.08 % BAC standard.
2.3. Empowering US States through Technical Assistance
The Injury Center provides critical funding and technical assistance to states through its Core Violence and Injury Prevention Program (VIPP). The program strengthens states’ capacity to collect and use data to better understand the local injury environment and challenges, plan injury prevention and control efforts, and carry out and evaluate potentially life-saving interventions for their residents. Additionally, through the Rape Prevention and Education program, the center provides funding to strengthen efforts in all 50 states, the District of Columbia, Puerto Rico, and six US territories.
2.4. Building Effective Partnerships for Prevention
Injury and violence prevention takes coordinated efforts across agencies, organizations and sectors. The Injury Center works with a variety of partners—from local health departments to national corporations—to make people safer in their homes, cars and communities. For example, a successful partnership with coaches and athletic trainers will help raise awareness of concussions and improve prevention and treatment of traumatic brain injuries in sports.
2.5. Building Awareness through Communication and Education
The Injury Center uses innovative communication campaigns, trainings, and program materials to educate about injury to advance prevention initiatives and promote policies that save lives. CDC educates health care providers, policy makers, public health practitioners, and the public about what works to prevent injuries. For example, through CDC’s Vital Signs program, we spotlight issues such as prescription painkiller overdoses, alcohol-impaired driving, and seat belt use to raise awareness about the problem and promote proven solutions [7].
2.6. Preventing Injuries and Violence around the Globe
Injuries and violence threaten people in the US and globally. CDC’s Injury Center collaborates with partners and Ministries of Health around the world, sharing vital lessons learned that can be put to work abroad. The Injury Center is committed to saving lives, protecting people, lowering the health and societal costs of injuries and violence. Our goal is to offer individuals, communities, states and countries around the world with timely, accurate information and useful tools and resources to keep people safe where they live, work, play and learn.
2.7. US-CDC and Chinese CDC Collaboration
Injuries are a major source of preventable deaths and disability in China. Road traffic crashes alone in China kill approximately 250 000 people annually, more than any other country in the world. The US CDC and Chinese CDC are working together on projects with a focus on road traffic injury epidemiology and prevention. China has a mature injury surveillance system to capture major causes of injury, and US-CDC is providing funding support for projects related to road traffic injury surveillance and evaluation, including projects on economic costs of road traffic injuries, electronic bicycles (E-bikes), child safety seat use, and behavioral risk factors for traffic injuries. These projects should provide data that will contribute to the evidence-base for prevention, and facilitate development of prevention policy and capacity building. According to the 2014 US-Chinese CDC Directors’ meeting, this collaboration will be expanded to other injury areas in the future.
3. The Public Health Approach to Injury Prevention
To solve public health problems—including injuries—CDC uses a systematic process called the public health approach. This approach has four steps: define the problem, identify risk and protective causes, develop and test interventions, and ensure widespread adoption of effective injury prevention principles and strategies (Fig 2).
Figure 2.
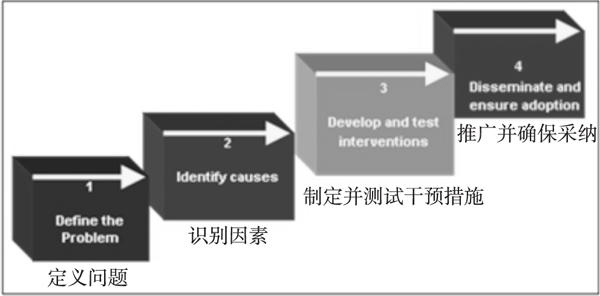
The Public Health Model Applied to Injury and Violence Prevention
3.1. Define the Problem
Before we can address an injury problem, we need to know how big the problem is, where the problem is, and whom it affects. CDC accomplishes this by gathering and analyzing data through surveillance. These data can show us how an injury problem changes over time, alert us to troubling trends in a particular type of injury, and let us know what impact prevention programs are having. Decision makers use these critical data in allocating programs and resources to the areas of most in need.
3.2. Identify Causes (Understanding Risk and Protective Factors)
It is not enough to know that a certain type of injury is affecting a certain group of people in a certain area. We also need to know why. What factors put people at risk for that injury? And conversely, what factors protect people from it? CDC conducts and supports research to answer these important questions. Once we have that information, we can develop and implement programs to eliminate or reduce risk factors for injuries and to capitalize on or increase factors that protect people from being injured.
3.3. Develop and Test Interventions
In this step, we put knowledge into action. Using information gathered in our research, CDC develops strategies to prevent particular injury problems. We implement these strategies in communities that are experiencing the problem. And we study the effects of these strategies to determine whether and how well they’re working. We use this information to identify any elements we need to change to eliminate difficulties or increase effectiveness.
3.4. Disseminate and Ensure Widespread Adoption
What we learn in developing and testing interventions has little benefit to public health unless we disseminate it widely and increase adoption of evidence-based practices. In this final step of the public health approach, CDC shares its knowledge and may provide funding or expert consultation for communities to replicate and translate these successful strategies into community programs.
4. Funded Programs and Activities
Through its funded programs and activities, the Injury Center works with national organizations, state health agencies, and other key groups to develop, implement, and promote effective injury and violence prevention practices. The following are some of the National programs and initiatives of the US-CDC.
4.1. National Centers of Excellence in Youth Violence Prevention
(http://www.cdc.gov/ViolencePrevention/ACE/)
CDC created the National Centers of Excellence in Youth Violence Prevention to connect academic and community resources to study and create lasting ways to prevent youth violence. Currently there are 6 centers funded to implement and evaluate comprehensive youth violence prevention strategies in high-risk communities. Each center is working to enhance collaboration among researchers and local partners, including the health department, within a defined community.
4.2. Core Violence and Injury Prevention Program (Core VIPP)
(http://www.cdc.gov/injury/stateprograms)
The Injury Center provides funds and technical assistance to states through its Core Violence and Injury Prevention Program (Core VIPP). The program supports 20 state health departments to strengthen capacity to collect and use data and implement evidence-based strategies to reduce morbidity and mortality at the state level.
4.3. DELTA FOCUS (Domestic Violence Prevention Enhancements and Leadership through Alliances, Focusing on Outcomes for Communities United with States)
(http://www.cdc.gov/violenceprevention/deltafocus/in
DELTA FOCUS is proving five years of funding to 10 state domestic violence coalition grantees to engage in primary prevention of intimate partner violence (IPV). Primary prevention means stopping IPV before it occurs. DELTA FOCUS grantees support IPV prevention at the national, state and local level. In addition to addressing individual and relationship factors associated with IPV outcomes, grantees support work to change the environments and conditions in which people live, work and play.
4.4. Web-based Injury Statistics Query and Reporting System (WISQARS)
(http://www.cdc.gov/injury/wisqars/)
CDC’s WISQARS™ (Web-based Injury Statistics Query and Reporting System) is an interactive, online database that provides fatal and nonfatal injury, violent death, and cost of injury data from a variety of trusted sources. Researchers, the media, public health professionals, and the public can use WISQARS™ data to learn more about the public health and economic burden associated with unintentional and violence-related injury in the United States [8]. Users can search, sort, and view the injury data and create reports, charts, and maps based on the following:
Intent of injury (unintentional injury, violence-related, homicide/assault, legal intervention, suicide/ intentional self-harm)
Mechanism (cause) of injury (e.g., fall, fire, firearm, motor vehicle crash, poisoning, suffocation)
Body region (e.g., traumatic brain injury, torso, upper and lower extremities)
Nature (type) of injury (e.g., fracture, dislocation, internal injury, open wound, amputation, and bum)
Geographic location (national, regional and state) where the injury occurred
Sex, race/ethnicity and age of the injured person
4.5. Injury Control Research Centers (ICRCs)
(http://www.cdc.gov/injury/erpo/icrc/index.html)
In 1987 the CDC began funding Injury Control Research Centers (ICRCs) throughout the United States to study ways to prevent injuries and disabilities, educate of injury researchers and practitioners, and provide outreach to the community. CDC funds 12 Injury Control Research Centers (with two cycling off in 2015) to conduct research in injury control and serve as training centers as well as information centers for the public. Research design in these centers is interdisciplinary and incorporates the fields of medicine, engineering, epidemiology, law and criminal justice, behavioral and social sciences, biostatistics and public health management. Currently funded (August, 2014) CRCs include:
Columbia University
Emory University
Johns Hopkins School of Public Health
Washington University
University of Iowa
University of Michigan
Mount Sinai School of Medicine
The Research Institute at Nationwide Children’s Hospital
University of North Carolina at Chapel Hill
University of Rochester Medical Center
West Virginia University
4.6. National Violent Death Reporting System (NVDRS)
(http://www.cdc.gov/violencePrevention/NVDRS/index.html)
NVDRS is a state-based surveillance system that links data from law enforcement, coroners and medical examiners, death certificate and crime laboratories to assist each participating state in tracking and understanding violence. By providing a clearer understanding of violent deaths, NVDRS is helping to guide decisions about prevention. NVDRS provides data on violent deaths and their circumstances to help state and local violence prevention practitioners to develop, implement and evaluate violence prevention strategies.
4.7. Rape Prevention and Education (RPE) Program
(http://www.cdc.gov/violencePrevention/RPE/index.html)
Sexual violence, including rape, is preventable. Recognizing this, Congress passed the Violence against Women Act in 1994. This landmark legislation established the Rape Prevention and Education (RPE) program at the Centers for Disease Control and Prevention (CDC). The RPE program seeks to develop and strengthen sexual violence prevention efforts at the local, state, and national level. RPE funding is awarded to health departments, there are programs in all 50 states, the District of Columbia, Puerto Rico, Guam and the Commonwealth of Northern Mariana Islands.
4.8. Violence against Children Surveys (VACS)
(http://www.cdc.gov/violenceprevention/vacs/index.html)
The VACS systematically measure physical, emotional and sexual violence against girls and boys and identify risk and protective factors and health consequences, as well as use of services and barriers to seeking help. Children who experience violence are at greater risk for common and destructive yet preventable consequences, including HIV, chronic diseases, crime and drug abuse, as well as serious mental health problems. Findings from VACS enable countries to better allocate limited resources to develop, launch, evaluate violence prevention programs and child protection systems.
5. Conclusions
The National Center for Injury Prevention and Control at US-CDC was created in 1991 and celebrated its 20th anniversary in 2012, documenting the development and advances in the field of injury and violence prevention during that time[ 3 ]. The vision and scientific leadership of staff and key partners, including states, community groups, advocates and other federal agencies, have contributed to this progress. Increased resources at CDC have helped state health department programs to flourish, enabling the delivery of life-saving interventions to communities and families. CDC’s declaration of motor vehicle injury prevention as a ‘winnable battle’ has enabled CDC to reach across its borders and provide technical assistance in surveillance and evaluation to countries in need. Competitive Centers of Excellence or Injury Control Research Centers have been funded to enrich the research base for injury prevention, and to train a continuing cadre of new young professionals. Foundations and philanthropies have stepped up to fund specific initiatives, and evidence-based practices, guidelines and recommendations have been developed and implemented by non—governmental organizations. Keys to US-CDC’s success in growing the Federal program have been credible science, strong leadership, training, and committed partners.
Despite this progress, the magnitude of the injury problem remains a problem around the world, and the resources, in China and elsewhere, do not yet coincide with the burden. But there is more interest and support than ever before for preventing injury and violence, worldwide. Progress in advancing global injury prevention will depend on how Governments, NGOs leading researchers and community practitioners are supported, how they and their agencies use existing resources and limited human capital, and how successful they will be in training and attracting young talent. These factors will determine whether preventing injuries and violence will remain a public health priority for future generations.
Acknowledgements
We acknowledge the assistance of Arlene Greenspan, Associate Director for Science at the National Center for Injury Prevention and Control (NCIPC), Tamara M Haegerich, Angela Marr, Tom Simon and Rod McClure (Director of the Division of Analysis, Research and Program Integration) at the NCIPC for helpful comments and to Duan Leilei from the National Center For NCD Control and Prevention, Chinese CDC, for her leadership in the US-China collaboration. Material included in this article was adapted from NCIPC website (http://www.cdc.gov/ncipc/) and from other written material in the public domain. It may be freely reproduced without permission.
Footnotes
Disclaimer: Reference herein to any specific commercial products, programs or services by trade name, trademark, manufacturer. Otherwise, does not necessarily constitute or imply its endorsement, recommendation or favoring by the United States Government. The views and opinions of authors expressed herein do not necessarily state or reflect the official position of the US-CDC and shall not be used for advertising or product endorsement purposes.
References
- [1].Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Injury: The Leading Cause of Death Among Persons Ages 1–44 [ EB/OL ].(2014. –9–4). http://www.cdc.gov/injury/.
- [2].Institute of Medicine (IOM). Injury in America: A continuing public health problem [ M ].Wahington DC:National Academy Press, 1985:164. [PubMed] [Google Scholar]
- [3].Sleet DA, Baldwin G, Man A,et al. History of Injury and Violence as Public Health Problems and Emergence of the National Center for Injury Prevention and Control at CDC [ J ]. Journal of Safety Research,2012,43(4):233–248. [DOI] [PubMed] [Google Scholar]
- [4].Sleet DA, Dahlberg LL, Basavaraju SV, et al. Injury prevention, violence prevention, and trauma care: building the scientific base [J]. MMWR Surveill Summ,2011,60(Suppl 4):78–85. [PubMed] [Google Scholar]
- [5].Shults RA, Elder RW, Sleet DA,et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving [ J ]. Am J Prev Med,2001,21 (4):66–88. [DOI] [PubMed] [Google Scholar]
- [6].Sleet DA, Mercer SL, Cole KH,et al. Scientific evidence and policy change: lowering the legal blood alcohol limit for drivers to 0.08% in the USA [ J]. Global Health Promotion,2011,18 (1):23–26. [DOI] [PubMed] [Google Scholar]
- [7].Centers for Disease Control and Prevention. Vitalsigns. Teen Drinking and Driving: A dangerous mix [ EB/OL ]. [ 2015-5– 14 ]. http://www.cdc.gov/vitalsigns.
- [8].Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS) [ EB/OL ].(2014-3–4). http://www.cdc.gov/injury/wisqars/.