

Abstract
Objective:
A new coding system for classifying the roots, main and accessory canals as well as developmental anomalies has been introduced recently. This paper discusses the advantages and potential application of the new system in research and clinical practice.
Methods:
A comprehensive analysis was undertaken on the most common, existing classification for root canal morphology. The advantages and potential applications of a new system for classifying roots and canal systems in research and clinical practice are discussed.
Results:
The analysis demonstrates deficiencies of the existing classification including lack of information on the number of roots, pulp chamber outline, lack of clarity in multi-rooted teeth, inability to define complex root canal configurations. The new coding system addresses the root and canal morphology in an accurate and systematic manner to provide detailed information of the tooth, root and canal anatomical features.
Conclusion:
With current advances in endodontic research and practice and the increasing body of knowledge on root and canal morphology, the deficiencies of the existing system used for classifying root canal morphology have become more apparent. The new system for classifying root, main and accessory canal morphology as well as teeth with anomalies has the potential to be used in research, clinical practice and education to accurately reflect the real anatomy of a tooth.
Keywords: Anatomy, canal configuration, classification, morphology, root, root canal
HIGHLIGHTS.
With current advances in endodontics and increasing body of knowledge, the deficiencies of the existing system used for classifying root canal morphology have become more apparent.
The new coding system provides detailed information on the tooth, root, main and accessory canal morphology as well as teeth with anomalies.
The new coding system has the potential to be used in research, clinical practice and education.
INTRODUCTION
Effective root canal treatment requires thorough knowledge of root and canal morphology (1). Tooth anatomy is complex and several systems are available for classifying the variations that occur (2-4). The system proposed by Vertucci et al. (3) together with supplemental configuration types (5-8) has been the most commonly used classification.
With an increasing range of anatomical complexities being reported and the deficiencies of the existing systems becoming more apparent, new systems for classifying root, root canal and accessory canal morphology have been proposed, which provide detailed information on tooth notation, number of roots, root canal configuration and accessory canal morphology including teeth with anomalies (9-11). The purpose of this paper is to discuss the advantages and potential applications of these new systems in research and clinical practice.
Shortcomings of the present system to categorise canal anatomy and advantages of the new system
Defining the number of roots
Maxillary premolars: Vertucci (12) categorized the root canal systems of human teeth into eight types (Fig. 1). However, for maxillary premolars, whether the canals were within one, two or more roots was not defined (Table 1 - yellow highlight). Therefore, maxillary premolars with similar canal configuration types but involving different numbers of roots have in the past been classified under the same type (Fig. 2) (12). This means that a one rooted maxillary premolar with two separate canals and a double-rooted premolar with one canal in each root are both classified as Vertucci type IV (Fig. 2) (12). Similarly, this explains why, in most reports, single/double/three-rooted maxillary premolars with a total of three canals are referred to as Type VIII configurations (3, 12-14) (Fig. 3). On the contrary, root canal configurations were defined separately in each of the mesiobuccal, distobuccal and palatal roots of maxillary molar teeth (12) (Table 1 - blue highlight). Clearly, in terms of endodontic management, it is critical to define the number of roots and not just canals, as this will have clinical implications when interpreting radiographs, during access cavity preparation and when searching for the location of canal orifices (9, 15). Notably, three-rooted maxillary premolars can exist in two forms - two buccal roots and one palatal root, or one buccal root and two palatal roots (16, 17). In summary, it is unclear why buccal and palatal roots were not defined separately in maxillary premolars in the Vertucci classification, while mesiobuccal, distobuccal and palatal roots were considered separately in maxillary molars.
Figure 1.
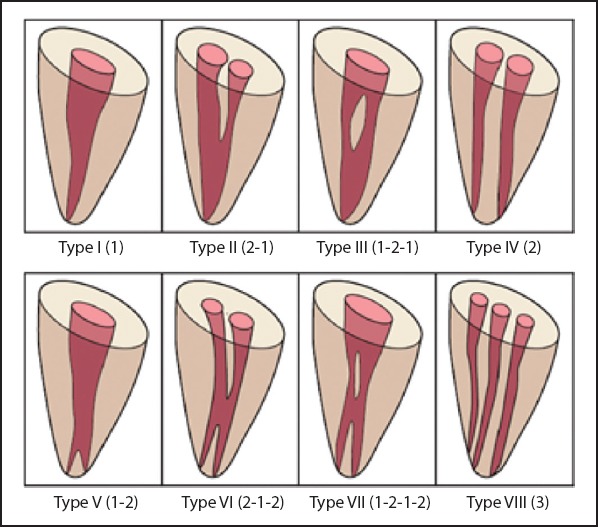
Diagrammatic representations of Vertucci’s classification for root canal morphology. (reproduced from Cleghorn et al. (29) with permission from PMPH-USA)
TABLE 1.
Application of the Vertucci classification on maxillary teeth
| Teeth | Type I 1 canal | Type II 2-1 canal | Type III 1-2-1 canal | Type IV 2 canals | Type V 1-2 canal | Type VI 2-1-2 canal | Type VII 1-2-1-2 canal | Type VIII 3 canals |
|---|---|---|---|---|---|---|---|---|
| Maxillary central incisor | ||||||||
| Maxillary lateral incisor | ||||||||
| Maxillary canine | ||||||||
| Maxillary first premolar | ||||||||
| Maxillary second premolar | ||||||||
| Maxillary first molar | ||||||||
| Mesiobuccal | ||||||||
| Distobuccal | ||||||||
| Palatal | ||||||||
| Maxillary second molar | ||||||||
| Mesiobuccal | ||||||||
| Distobuccal | ||||||||
| Palatal | ||||||||
Figure 2.
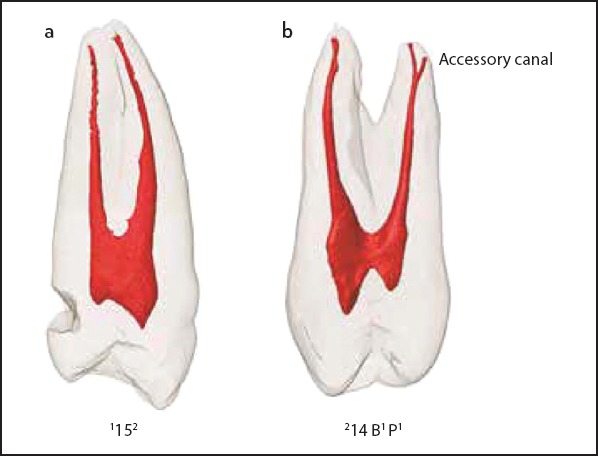
(a, b) Both maxillary premolar teeth are classified as having a configuration type IV canal. The new system describes a) as a single rooted maxillary right second premolar having 2 separate canals with the code 1152, (b) as a double rooted maxillary right first premolar having one canal in each of the buccal and palatal roots with the code 214B1P1 (modified from Ahmed et al. (9), reproduced with permission from Wiley)
Figure 3.
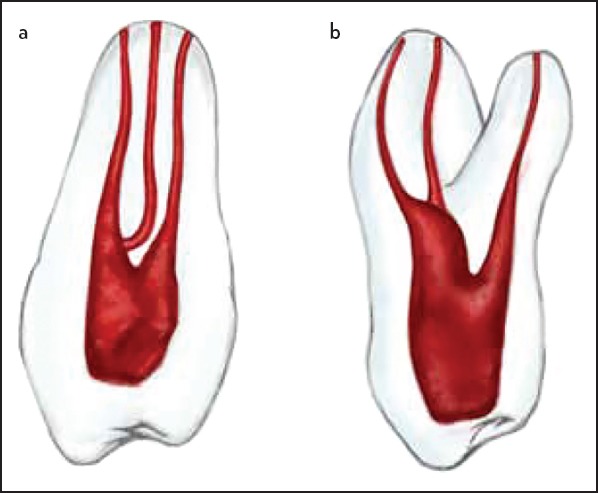
(a, b) Drawings of samples presented in Vertucci (12). (a) Single rooted maxillary second premolar with three canals. (b) Double rooted maxillary second premolar with three canals. Both maxillary premolar teeth were classified as having a configuration type VIII canal
Mandibular premolars: As with maxillary premolars, mandibular premolars with similar canal configuration types but involving different numbers of roots were classified under the same type in the Vertucci classification (Table 2 - yellow high-light) whereas they were presented separately in each of the mesial and distal roots in mandibular molar teeth (12) (Table 2 - blue highlight). Again, it is unclear why the individual roots in double-rooted mandibular premolars were not considered separately, whilst individual mesial and distal roots were considered separately in mandibular molars.
TABLE 2.
Application of the Vertucci classification on mandibular teeth
| Teeth | Type I 1 canal | Type II 2-1 canal | Type III 1-2-1 canal | Type IV 2 canals | Type V 1-2 canal | Type VI 2-1-2 canal | Type VII 1-2-1-2 canal | Type VIII 3 canals |
|---|---|---|---|---|---|---|---|---|
| Mandibular central incisor | ||||||||
| Mandibular lateral incisor | ||||||||
| Mandibular canine | ||||||||
| Mandibular first premolar | ||||||||
| Mandibular second premolar | ||||||||
| Mandibular first molar | ||||||||
| Mesial | ||||||||
| Distal | ||||||||
| Mandibular second molar | ||||||||
| Mesial | ||||||||
| Distal | ||||||||
The new system for classifying root and canal morphology provides detailed information on the tooth number, number of roots (any division of the root is considered as two or more roots) and root canal configuration in a single code, thus presenting an accurate and logical classification (9). Thus, one benefit of the new system is that teeth with similar canal configurations in separate roots are described in a way that will accurately reflect their anatomy in a single code. As examples, single-rooted maxillary right second premolars with type IV canals are categorized as 1152 (Fig. 2a), whilst double-rooted maxillary right first premolars with single canals in each of buccal (B) and palatal (P) roots are categorised as 214B1P1 (Fig. 2b), clearly identifying the difference.
Defining the outline of pulp chambers
Vertucci (12) categorized root canals into eight types as they progressed from the floor of the pulp chamber via the canal orifice to the apical foramen. However, the outline and thus the apical extent (floor) of the pulp chamber was not defined, and no mention was made of where the canal orifice(s) began.
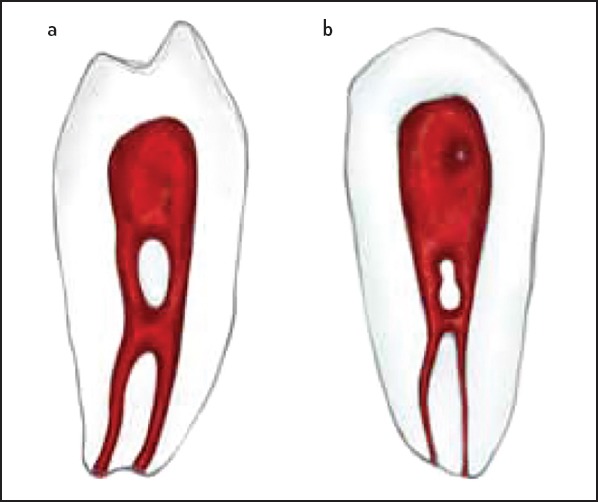
The maxillary first premolar in Figure 4a is classified as Vertucci type VIII, which means three separate, distinct canals from the pulp chamber to the canal terminus (3). However, it is clear that the canal in the buccal root is a type 1-2 canal with one canal leaving the chamber that then divides into two along the root length; this indicates that the apical extent of the pulp chamber lacked definite identification landmarks. Similar findings can be observed with other tooth types (Fig. 4b). This lack of definition of the pulp chamber outline could also lead to potential confusion where a tooth can have two possible configuration types using the Vertucci system.
Figure 4.
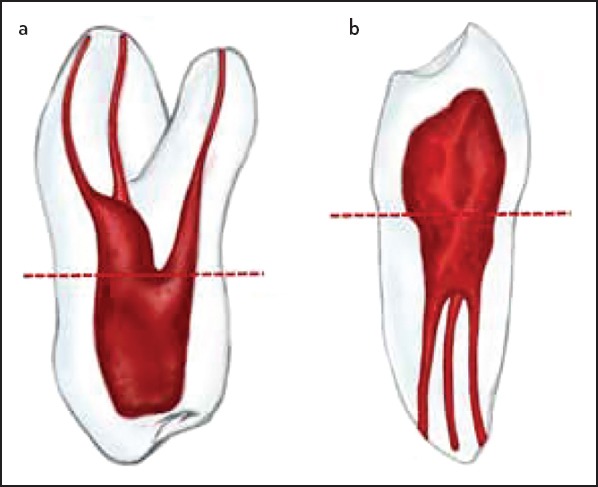
Drawings of samples presented in Vertucci et al. (3) and Vertucci (12). (a) This double rooted maxillary second premolar was classified by Vertucci as type VIII. Notably, the buccal canals have a common canal configuration in the coronal region of the root. (b) The same applies for this mandibular first premolar tooth with Type VIII canal
The new system defines the pulp chamber in single and multi-rooted teeth. In single-rooted teeth and double/multi-rooted teeth with middle or apical root bifurcations with a single canal coronally, it extends to the most apical portion of the cervical margin of the crown, whereas in double/multi-rooted teeth with coronal root and/or canal bifurcations (no single canal coronally), it extends to the floor of pulp chamber located in the coronal third of the root (9, 10). The root canal orifice is defined as the opening of the canal system at the base of the chamber where the root canal begins (9, 10). This means that the maxillary first premolar (MxFP) in Figure 4a is classified as 2MxFP B1-2P1, in which the two buccal canals have a common canal initially, and the mandibular premolar in Figure 4b is classified as 1MnP1-3, again because there is a single canal initially that divides into three. Figure 5 shows codes for single and double-rooted mandibular canines with different canal morphology (with and without a single canal coronally).
Figure 5.
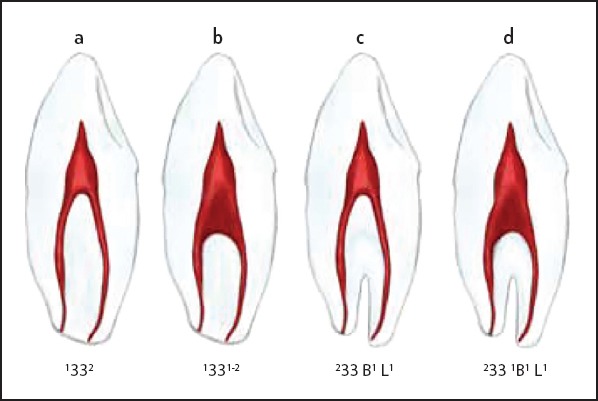
Application of the new system in single and double rooted canines with and without single coronal canal. (a) Single rooted canine with two separate canals. (b) Single rooted canine with a canal configuration type 1-2. (c) Double rooted canine with two separate canals. (d) Double rooted canine with two canals having a single coronal canal
Lack of clarity in multi-rooted teeth
Reporting the canal configuration in each root of a double or multi-rooted tooth separately is another concern of the Vertucci system (Tables 1, 2). This does not allow the reporting of the anatomical variations by “tooth” as it merely reports the configuration in the roots separately, i.e. at canal-level and not at tooth-level, which is more relevant. This flaw could lead to potential confusion because there is no correlation between the canal configurations that can occur in the individual roots of a multi-rooted tooth. In other words, it is more appropriate and more clinically relevant to report holistically the percentage of three rooted maxillary first molars with a Vertucci type 2-1 in the mesiobuccal root and type 1 canals in the distal and palatal roots, respectively, than presenting only the percentage of type 2-1 canals in the mesiobuccal root separately from the other roots (Table 1).
The new system defines tooth, root(s) and canal(s) anatomy in a single code (9). This provides a more logical and accurate description of the complexity of root and canal anatomy for any tooth, regardless of its complexity (Table 3-5). This has an important clinical impact since operators must treat all canals in all roots, and not only canals in certain roots, within a tooth. In addition, it could help to compare and contrast the complexity of a canal system in one root with other roots within the same tooth. As an example, it is more relevant to report that complex canal morphology in the distobuccal root of a maxillary first molar corresponds to complex canal morphology in the mesiobuccal root than reporting the complexity of both in a separate code as with the Vertucci classification.
TABLE 3.
An example of a template for summarizing the root and canal morphology of all teeth
| RTN/O-C-F | 1 | 1-2 | 2 | 2-1 | B1 L1 | M1 D1 | MB1 DB1 P1 | etc | Total (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1Max1 | 100 | ||||||||
| 1Max2 | 100 | ||||||||
| 1Max3 | 100 | ||||||||
| 2Max4 | 100 | ||||||||
| 2Max5 | 100 | ||||||||
| 3Max6 | 100 | ||||||||
| 3Max7 | 100 | ||||||||
| 3Max8 | 100 | ||||||||
| 1Man1 | 100 | ||||||||
| 1Man2 | 100 | ||||||||
| 1Man3 | 100 | ||||||||
| 1Man4 | 100 | ||||||||
| 1Man5 | 100 | ||||||||
| 3Man6 | 100 | ||||||||
| 3Man7 | 100 | ||||||||
| 3Man8 | 100 |
Such as Max for Maxillary, Man for Mandibular can be used if teeth from both right and left sides of the arch are pooled in a given study. O-C-F: Orifice-Canal-Foramen
TABLE 5.
An example of a template for categorising canal configurations in a specific root in one type of tooth can also be categorized, e.g. the mesial roots (M) of mandibular right first molars
| Code | M2 | M2-1 | M3 | M3-1 | etc |
|---|---|---|---|---|---|
| Percentage |
Those reporting the results of research projects are able to present their data using the new system in several ways based on the unique study objectives. The root and canal morphology of a single tooth type or two or even more tooth types could be reported in a single table (Table 3). Alternatively, abbreviations (such as Max for Maxillary, Man for Mandibular) can be used if teeth from both right and left sides of the arch are pooled in a given study. If the pooled data shows a wide range of root numbers and root canal configuration types or teeth from right and left sides need to be included, then the data can be presented in more than one table (Table 4). The new system can also be applied if researchers would like to present the canal morphology of a single root of a given tooth type (Table 5).
TABLE 4.
An example of a template for summarizing the root and canal morphology in right and left single, double and three-rooted maxillary first and second premolars
| RTN/O-C-F | 1 | 1-2 | 2 | 2-1 | 3 | B1 P1 | MB1 DB1 P1 | etc | Total (%) |
|---|---|---|---|---|---|---|---|---|---|
| 114 | 100 | ||||||||
| 214 | 100 | ||||||||
| 314 | 100 | ||||||||
| 124 | 100 | ||||||||
| 224 | 100 | ||||||||
| 324 | 100 | ||||||||
| 115 | 100 | ||||||||
| 215 | 100 | ||||||||
| 315 | 100 | ||||||||
| 125 | 100 | ||||||||
| 225 | 100 | ||||||||
| 325 | 100 |
A similar approach can be used for other tooth types O-C-F: Orifice-Canal-Foramen
Complexity of canal systems
Transverse canal anastomosis: Vertucci (12) presented the percentage and location of a transverse canal anastomosis (a thin communication between two or more canals in the same root) between canals as a separate entity from root canal configurations; however, the criteria of defining such anatomy was not mentioned, and the landmarks for differentiating it from a common canal configuration were unclear (Fig. 6).
Figure 6.
Drawings of samples presented in Vertucci (12). These mandibular first premolar samples were classified as Vertucci type IV. The criteria for defining transverse anastomosis were not clear, and this anatomical feature was not included in the canal classification system. The specimen can also be classified as Vertucci type.VI (2-1-2)
The identification of a transverse canal anastomosis separately from the canal configuration is a concern since they are an integral part of the root canal configuration and because they have clinical implications during chemo-mechanical instrumentation, canal filling and root-end cavity preparation and filling (18-20). Therefore, the new system does not define a transverse canal anastomosis as a separate entity as it considers such anatomy as an integral part of the root canal configuration. However, if individuals would like to define transverse canals as a separate entity based on certain criteria, then the new system can still be used alongside.
Supplementary and non-classifiable configurations: Sert & Bayirli (8) added 14 supplementary configuration types to Vertucci’s classification to categorize more complex root canals not included in the original system (Fig. 7). However, categorizing root canal configuration by ‘type’ using simple Roman numerals becomes unworkable, inconvenient and potentially misleading. Recent reports using advanced 3D imaging technology have revealed that many canal configurations have been described as “non-classifiable” using the Vertucci system (21-24). One study reported that as many as 13% of specimens did not fit into the classification of Vertucci (25). In fact, up to 37 root canal configuration types have been identified (4).
Figure 7.

Illustrative diagram showing the supplemental configuration types to Vertucci’s classification of root canal systems (Types IX-Type XXIII) as suggested by Sert & Bayirli (8). (reproduced from Cleghorn et al. (29) with permission from PMPH-USA)
The new coding system describes what the clinician or researcher can see in a simple yet accurate manner. It can also define previously “non-classifiable” canal configurations since only a simple code is required with no requirement to use several Latin numerals for the canals in each root of a multi-rooted tooth. Figure 8 provides examples of codes of Vertucci non-classifiable root canal configuration types. It is worth noting that non-classifiable canal systems have also been reported within in vivo research studies on population groups using cone beam computed tomography (26). In addition, clinical reports have shown that the application of contemporary diagnostic modalities (including the dental operating microscope) demonstrate that some complex anatomical variations do not fit into the eight categories of the Vertucci classification, e.g. mandibular molars with various configurations in the mesial root, maxillary molars with similar anatomical variations in the mesiobuccal root, and mandibular premolars with complex canal morphology (27-29). This confirms the relevance and utility of the new system as it can help clinicians define and appreciate complex variations of the root canal system.
Figure 8.
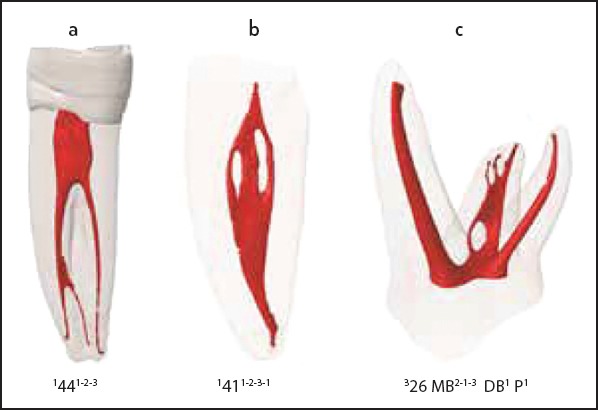
Examples for the application of the new coding system to present non-classifiable Vertucci root canal configuration types
Accessory canal morphology and developmental anomalies
Vertucci (12) categorized lateral canals according to their location (coronal, middle, apical or furcation), but no information on the accessory canal configuration and type (patent, blind or loop) was provided. In addition, the percentages of lateral canals in maxillary premolars were reported without referring to the number of roots. Tooth, root and canal anomalies were not addressed in the various reports by Vertucci.
The new classification provides a coding system for accessory canals (Tables 6, 7), and developmental anomalies (Tables 8, 9). Notably, these coding systems are complementary and provide a single integrated system that adds more detailed information on the morphological features of teeth that are essential for proper diagnostic, training and research. The ability to combine codes for main root canals together with accessory canals (9, 10), and developmental anomalies has not been achieved in previous classifications (Fig. 9) (11).
TABLE 6.
An example of a template for summarizing the accessory canal morphology in single-rooted anterior teeth (central, lateral and canine)
| RTN | (C1) | (M1) | (A1) | (C1, M1) | (C1, A1) | (C1, M1) | (D) | etc | Total (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1Max1 | 100 | ||||||||
| 1Max2 | 100 | ||||||||
| 1Max3 | 100 |
C: Coronal third, M: Middle third, A: Apical third
TABLE 7.
An example of a template for summarizing the accessory canal morphology in double rooted maxillary (Max) first and second premolar teeth
| RTN | B(C1) P | B(M1) P | B(A1) P | B P(C1) | B P(M1) | B P(A1) | etc | Total (%) |
|---|---|---|---|---|---|---|---|---|
| 2Max4 | 100 | |||||||
| 2Max5 | 100 |
C: Coronal third, M: Middle third, A: Apical third
TABLE 8.
An example of a template for summarizing a developmental anomaly (C-shaped canals)
| RTN | (CsCI) | (CsCII) | (CsCIII) | Total (%) |
|---|---|---|---|---|
| 2Man1 | 100 | |||
| 2Man2 | 100 | |||
| 2Man3 | 100 |
CsC: C-shaped Canal
TABLE 9.
An example of a template for summarizing a developmental anomaly (Root Dilaceration) in double rooted mandibular molars
| RTN | M(RD) D | M D(RD) | (RD)M D | Total (%) |
|---|---|---|---|---|
| 2Man1 | 100 | |||
| 2Man2 | 100 | |||
| 2Man3 | 100 |
RD: Root dilaceration; M: Mesial; D: Distal
Figure 9.
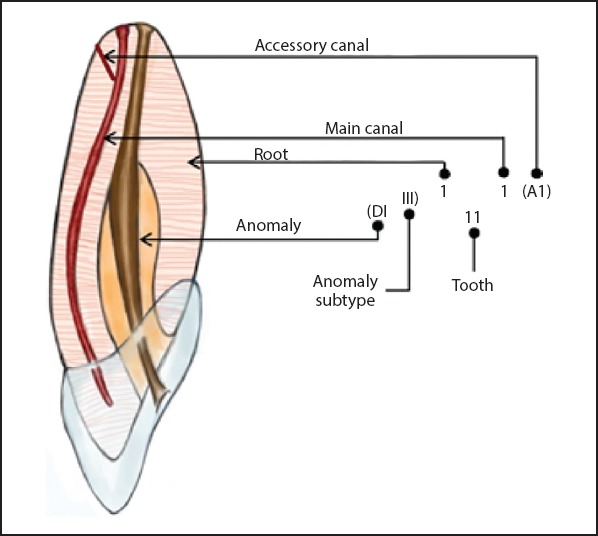
An illustrative drawing showing an integrated formula for the coding system for root, main canal, accessory canals and anomalies (modified from Ahmed et al. (11), reproduced with permission from Wiley)
DI: Dens Invaginatus
Application of the new system in daily clinical practice
The new system can be applied using any diagnostic tool applied in clinical practice (periapical radiography, dental operating microscope, CBCT) (Figs. 10, 11). The operator simply needs to identify the tooth type, number of roots and root canal configuration, and the presence of accessory canals and anomalies (Fig. 9). Usually the tooth number and number of roots can be identified during clinical examination and from preoperative radiographs. However, in some instances, root canal treatment is performed on a tooth that has migrated from its position in the arch following extraction of neighbouring teeth or it may have been restored and the shape of the crown not visible. Thus, on some occasions, the operator is not able to identify precisely the tooth type; in such cases, a suitable abbreviation can be used (such as MCI for mandibular central incisor, etc.) in place of the normal tooth code.
Figure 10.

Periapical radiographs showing various root, main and accessory canal morphology as well as developmental anomalies. (a) 1111 - a single rooted maxillary right central incisor having a root canal configuration type 1. (b) 1421-2-1 - a single rooted mandibular right lateral incisor having a root canal configuration type 1-2-1. (c) 1442 - a single rooted mandibular right first premolar having a root canal configuration type 2. (d) 1252-1 - a single rooted maxillary left second premolar having a root canal configuration type 2-1. (reproduced from Ahmed (32) with permission from Medknow). (e) 215 B1 P1 - a double rooted maxillary right second premolar in which the buccal and palatal roots having a root canal configuration type 1. (f) 236 M2-1(A1) D1(A1) - a double rooted mandibular left first molar in which the mesial root has a root canal configuration type 2-1 and the distal root has a root canal configuration type 1. Each of the mesial and distal roots has an accessory canal in the apical third configuration type 1. (reproduced from Ahmed (32) with permission from Medknow). (g) (RE)336 M2 D1 DL1 - a three rooted mandibular left first molar in which the mesial root has a canal configuration type 2, whilst each of the distal and distolingual roots (radix entomolaris) encase a root canal configuration type 1
Figure 11.

Postoperative CBCT image of a mandibular left first molar with 6 separate canals with the code - 236M3D3. (a) Postoperative CBCT scan (coronal and sagittal sections - mesial root) (b) Postoperative CBCT scan (coronal and sagittal sections - distal root) (c) Postoperative CBCT image [axial section - coronal] (d) Postoperative CBCT image [axial section - middle] (e) Postoperative CBCT image [axial section - apical] (reproduced from Hashem & Ahmed (33) with permission from Aves)
The number of roots, as well as some developmental anomalies, is usually identified on periapical radiographs (perhaps using different angulations). The root canal configuration is identified usually during the treatment procedure and more easily done following root filling when the post-operative radiograph highlights the anatomy more clearly than on pre- or intra-operative films. This means that the operator will only be able to define the full code after completion of treatment. However, information on tooth number, roots and anomalies (without root canal configurations) can be used in referrals between clinicians and/or students (an example: a referral of (DIIII)111 describes a single-rooted maxillary right incisor (tooth 11) with a dens invaginatus (DI) type III). This kind of detailed, consistent documentation will be of benefit for case reports in which the reader can easily follow the anatomical landmarks of a given tooth in a systematic manner. When CBCT images are used pre-operatively, it may be possible to define the canal configuration from the outset.
Consistent categorisation
As a general rule, the introduction of new systems is challenging because clinicians and researchers will find difficulty when comparing their results with previous studies that used existing classification systems. However, it is worth noting that even when using the same system a precise comparison between results of different studies is not always possible because if similar root canal configurations (such as Vertucci type IV) have been identified with similar percentages in two studies, this does not mean that both have the same number of roots as discussed above. Moreover, the Vertucci classification does not provide a clear definition of the pulp chamber outline and the location of the root canal orifice, which could lead to different identification parameters among different studies.
The assessment of canal configuration in the apical region may vary depending on the method used for identification, which can be subjective amongst observers. For example, based on certain experimental measurements of canal dimensions or clinical negotiability, some apical bifurcations could either be classified as an apical delta/ramification or a division from the main canal (type 1-2). Similar arguments do exist with regards to complex canal irregularities such as the canal isthmus, which has been classified by a number of researchers (30, 31). It is obvious that a standard consistent view of such anatomy cannot be achieved, and therefore, such anatomical landmarks should be classified based on the method and criteria used for identification (9).
The inclusion of this new system in teaching and education is another challenge. It is easier for students and trainees to present their cases using a system that defines the tooth number, root and configuration of the main and accessory canal morphology without referring to Latin numerals. Postgraduate students and specialists, who usually face more complex cases, will be able to address and correlate complex canal configuration types together with anomalies (if present) using integrated codes that accurately reflect the level of complexity of their cases, thus constructing an appropriate treatment plan and help define the risks associated with specific anatomical features.
Limitations
Despite the detailed information provided when using the new coding system, it does not provide information with regards to the shape (such as round and oval), size (narrow and wide) of the root canal system, degree of root and canal curvatures and several other sophisticated anatomical landmarks of accessory canal morphology [such as dimensions and tortuosity (34)] and developmental anomalies (such as depth/dimensions of palato-gingival grooves, morphological cross sections of C-shaped canals). The inclusion of these parameters could be useful; however, they will add considerable complexity and the potential for misunderstanding. In addition, a new system must be simple so that it can be adopted universally. However, researchers and clinicians are still able to add more detailed information, if needed, using words or phrases to acompany the code to describe a particular detail related to the root or canal (such as 214B1P1 with narrow buccal canal, etc.).
CONCLUSION
With current advances in endodontic research and practice and the increasing body of knowledge on root and canal morphology, the deficiencies of the existing systems used for classifying root canal morphology have become more apparent. The new system for classifying root, main and accessory canal morphology as well as teeth with anomalies has the potential to be used in research, clinical practice and education to accurately reflect the real anatomy of a tooth.
Footnotes
Conflict of interest: No conflict of interest was declared by the authors.
Peer-review: Externally peer-reviewed.
Financial Disclosure: The authors declared that this study has received no financial support.
Authorship contributions: Concept – H.M.A.A, P.M.H.D.; Design – H.M.A.A, P.M.H.D.; Supervision – H.M.A.A, P.M.H.D.; Analysis and/or interpretation – H.M.A.A, P.M.H.D.; Literature search – H.M.A.A, P.M.H.D.; Writing – H.M.A.A, P.M.H.D.; Critical Review – H.M.A.A, P.M.H.D.
REFERENCES
- 1.Vertucci F. Root canal morphology and its relationship to endodontic procedures. Endod Top. 2005;10:3–29. [Google Scholar]
- 2.Weine FS, Healey HJ, Gerstein H, Evanson L. Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surg Oral Med Oral Pathol. 1969;28(3):419–25. doi: 10.1016/0030-4220(69)90237-0. [DOI] [PubMed] [Google Scholar]
- 3.Vertucci F, Seelig A, Gillis R. Root canal morphology of the human maxillary second premolar. Oral Surg Oral Med Oral Pathol. 1974;38(3):456–64. doi: 10.1016/0030-4220(74)90374-0. [DOI] [PubMed] [Google Scholar]
- 4.Versiani M, Ordinola-Zapata R. Root canal anatomy:implications in biofilm disinfection. In: Chavez de Paz L, Sedgley C, Kishen A., editors. Root canal biofilms. Toronto: Springer; 2015. pp. 23–52. [Google Scholar]
- 5.Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J. 2001;34(5):359–70. doi: 10.1046/j.1365-2591.2001.00399.x. [DOI] [PubMed] [Google Scholar]
- 6.Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J. 2002;35(1):56–62. doi: 10.1046/j.1365-2591.2002.00452.x. [DOI] [PubMed] [Google Scholar]
- 7.Ng YL, Aung TH, Alavi A, Gulabivala K. Root and canal morphology of Burmese maxillary molars. Int Endod J. 2001;34(8):620–30. doi: 10.1046/j.1365-2591.2001.00438.x. [DOI] [PubMed] [Google Scholar]
- 8.Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod. 2004;30(6):391–8. doi: 10.1097/00004770-200406000-00004. [DOI] [PubMed] [Google Scholar]
- 9.Ahmed HMA, Versiani MA, De-Deus G, Dummer PMH. A new system for classifying root and root canal morphology. Int Endod J. 2017;50(8):761–70. doi: 10.1111/iej.12685. [DOI] [PubMed] [Google Scholar]
- 10.Ahmed HMA, Neelakantan P, Dummer PMH. A new system for classifying accessory canal morphology. Int Endod J. 2017 doi: 10.1111/iej.12800. In Press. [DOI] [PubMed] [Google Scholar]
- 11.Ahmed HMA, Dummer PMH. A new system for classifying tooth, root and canal anomalies. Int Endod J. 2017 doi: 10.1111/iej.12867. In Press. [DOI] [PubMed] [Google Scholar]
- 12.Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589–99. doi: 10.1016/0030-4220(84)90085-9. [DOI] [PubMed] [Google Scholar]
- 13.Velmurugan N, Parameswaran A, Kandaswamy D, Smitha A, Vijayalakshmi D, Sowmya N. Maxillary second premolar with three roots and three separate root canals--case reports. Aust Endod J. 2005;31(2):73–5. doi: 10.1111/j.1747-4477.2005.tb00230.x. [DOI] [PubMed] [Google Scholar]
- 14.Peiris R. Root and canal morphology of human permanent teeth in a Sri Lankan and Japanese population. Anthropol Sci. 2008;116(2):123–33. [Google Scholar]
- 15.Ahmed HM, Cheung GS. Accessory roots and root canals in maxillary premolar teeth:a review of a critical endodontic challenge. ENDO - Endod Prac Today. 2012;6(1):7–18. [Google Scholar]
- 16.Neelakantan P, Subbarao C, Ahuja R, Subbarao CV. Root and canal morphology of Indian maxillary premolars by a modified root canal staining technique. Odontology. 2011;99(1):18–21. doi: 10.1007/s10266-010-0137-0. [DOI] [PubMed] [Google Scholar]
- 17.George GK, Varghese AM, Devadathan A. Root canal treatment of a maxillary second premolar with two palatal roots:A case report. J Conserv Dent. 2014;17(3):290–2. doi: 10.4103/0972-0707.131807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.von Arx T. Frequency and type of canal isthmuses in first molars detected by endoscopic inspection during periradicular surgery. Int Endod J. 2005;38(3):160–8. doi: 10.1111/j.1365-2591.2004.00915.x. [DOI] [PubMed] [Google Scholar]
- 19.Wu MK, Dummer PM, Wesselink PR. Consequences of and strategies to deal with residual post-treatment root canal infection. Int Endod J. 2006;39(5):343–56. doi: 10.1111/j.1365-2591.2006.01092.x. [DOI] [PubMed] [Google Scholar]
- 20.Endal U, Shen Y, Knut A, Gao Y, Haapasalo M. A high-resolution computed tomographic study of changes in root canal isthmus area by instrumentation and root filling. J Endod. 2011;37(2):223–7. doi: 10.1016/j.joen.2010.10.012. [DOI] [PubMed] [Google Scholar]
- 21.Verma P, Love RM. A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J. 2011;44(3):210–7. doi: 10.1111/j.1365-2591.2010.01800.x. [DOI] [PubMed] [Google Scholar]
- 22.Kim Y, Chang SW, Lee JK, Chen IP, Kaufman B, Jiang J, et al. A micro-computed tomography study of canal configuration of multiple-canalled mesiobuccal root of maxillary first molar. Clin Oral Investig. 2013;17(6):1541–6. doi: 10.1007/s00784-012-0852-8. [DOI] [PubMed] [Google Scholar]
- 23.Lee KW, Kim Y, Perinpanayagam H, Lee JK, Yoo YJ, Lim SM, et al. Comparison of alternative image reformatting techniques in micro-computed tomography and tooth clearing for detailed canal morphology. J Endod. 2014;40(3):417–22. doi: 10.1016/j.joen.2013.09.014. [DOI] [PubMed] [Google Scholar]
- 24.Leoni GB, Versiani MA, Pecora JD, Damiao de Sousa-Neto M. Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod. 2014;40(5):710–6. doi: 10.1016/j.joen.2013.09.003. [DOI] [PubMed] [Google Scholar]
- 25.Filpo-Perez C, Bramante CM, Villas-Boas MH, Hungaro Duarte MA, Versiani MA, Ordinola-Zapata R. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J Endod. 2015;41(2):231–6. doi: 10.1016/j.joen.2014.09.024. [DOI] [PubMed] [Google Scholar]
- 26.Martins JNR, Marques D, Mata A, Carames J. Root and root canal morphology of the permanent dentition in a Caucasian population:a cone-beam computed tomography study. Int Endod J. 2017;50(11):1013–26. doi: 10.1111/iej.12724. [DOI] [PubMed] [Google Scholar]
- 27.Azim AA, Deutsch AS, Solomon CS. Prevalence of middle mesial canals in mandibular molars after guided troughing under high magnification:an in vivo investigation. J Endod. 2015;41(2):164–8. doi: 10.1016/j.joen.2014.09.013. [DOI] [PubMed] [Google Scholar]
- 28.Ahmad IA, Al-Jadaa A. Three root canals in the mesiobuccal root of maxillary molars:case reports and literature review. J Endod. 2014;40(12):2087–94. doi: 10.1016/j.joen.2014.07.034. [DOI] [PubMed] [Google Scholar]
- 29.Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular second premolar:a literature review. J Endod. 2007;33(9):1031–7. doi: 10.1016/j.joen.2007.03.020. [DOI] [PubMed] [Google Scholar]
- 30.Hsu YY, Kim S. The resected root surface. The issue of canal isthmuses. Dent Clin North Am. 1997;41(3):529–50. [PubMed] [Google Scholar]
- 31.Teixeira FB, Sano CL, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ. A preliminary in vitro study of the incidence and position of the root canal isthmus in maxillary and mandibular first molars. Int Endod J. 2003;36(4):276–80. doi: 10.1046/j.1365-2591.2003.00638.x. [DOI] [PubMed] [Google Scholar]
- 32.Ahmed HM. Guidelines to enhance the interpretation of two-dimensional periapical radiographic images in endodontics. Eur J Gen Dent. 2015;4(3):106–12. [Google Scholar]
- 33.Hashem AAR, Ahmed HMA. Endodontic management of a mandibular first molar with unusual canal morphology. Eur Endod J. 2017;2:1–4. doi: 10.5152/eej.2017.17042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Xu T, Tay FR, Gutmann JL, et al. Micro-computed tomography assessment of apical accessory canal morphologies. J Endod. 2016;42(5):798–802. doi: 10.1016/j.joen.2016.02.006. [DOI] [PubMed] [Google Scholar]