

Introduction
Cardiac rhabdomyomas are commonly found in children with tuberous sclerosis and may cause electrocardiogram (ECG) abnormalities such as ST-segment elevation,1, 2, 3 pseudo-preexcitation,4 ventricular hypertrophy,5 and atrioventricular block,6 as well as atrial and ventricular arrhythmias.7 We present the case of a newborn with large ventricular rhabdomyomas causing PR depression and significant ST-segment elevation on ECG.
Case report
A newborn girl with a fetal diagnosis of intracardiac tumors and occasional premature ventricular contractions was born at 40 weeks gestation via an uncomplicated spontaneous vaginal delivery. Her Apgar scores were 8 and 9 at 1 and 5 minutes, respectively. Her vital signs were normal for age and she was in no distress. Postnatal echocardiogram confirmed the fetal diagnosis, revealing a large intracardiac mass on the right ventricular side of the interventricular septum and another large mass originating from the apical aspect of the left ventricular lateral wall and wrapping around the apex of both ventricles (Figure 1). The masses did not cause significant inflow or outflow tract obstruction. There was a tiny pericardial effusion, a patent foramen ovale, and mild tricuspid regurgitation. The right coronary artery was noted to originate from the left sinus of Valsalva. There was otherwise normal structural anatomy and biventricular systolic function, and no atrial masses were seen.
Figure 1.
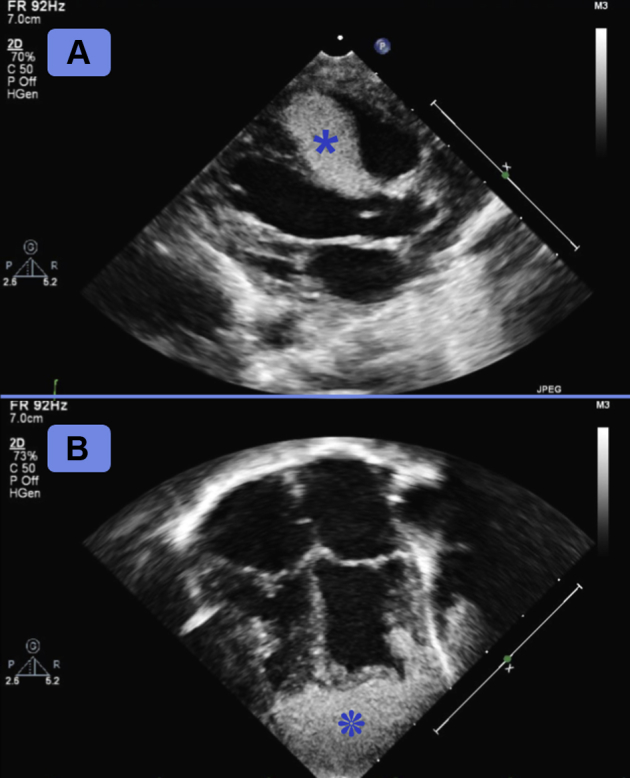
Postnatal echocardiogram. A: Large intracardiac mass on right ventricular side of interventricular septum, extending from level of pulmonic valve down to the apex. B: Additional large mass originating from apical aspect of lateral left ventricular wall, wrapping around the apex of both ventricles. Each mass is indicated by an asterisk.
An ECG performed on the first day of life (Figure 2) demonstrated normal sinus rhythm with right ventricular hypertrophy, PR-segment depression, and massive J-point and ST-segment elevations (maximum: ∼8 mm) in the mid and lateral precordial leads. Brain magnetic resonance imaging was significant for cortical dysplasia, and ash leaf spots were noted on the chest and back. Genetic testing revealed a mutation in TSC1, confirming the suspected diagnosis of tuberous sclerosis. The infant remained clinically well on no medications and was discharged home on the third day of life. During the postnatal admission, there was no evidence of ventricular ectopy or tachyarrhythmias.
Figure 2.

Electrocardiogram (ECG) on first day of life. A: A 12-lead ECG showing right ventricular hypertrophy, PR-segment depression, J-point elevation, and ST-segment elevation in the precordial leads, consistent with a pericarditis pattern. B: Zoomed-in ECG of the most pronounced ST-segment elevation, approximately 8 mm (lead V4).
At an outpatient visit at 6 months of age, a repeat echocardiogram found slight involution of both the interventricular and apical rhabdomyomas. A 24-hour Holter monitor was unremarkable. The ECG (Figure 3) demonstrated significant improvement of the PR depression and J-point elevation, with persistent coved ST elevation. As the patient remained asymptomatic, with no inflow or outflow obstruction and no tachyarrhythmias, antiproliferative medications such as sirolimus were not initiated.
Figure 3.

Electrocardiogram (ECG) at 6 months of age. A: A 12-lead ECG showing resolution of PR-segment depression and significant improvement in J-point elevation. There is persistent doming of the ST segments in the precordial leads. B: Zoomed-in ECG of lead V4.
Discussion
Cardiac rhabdomyomas may cause a variety of electrocardiographic abnormalities, possibly owing to their intrusion into the cardiac conduction system. ST elevation mimicking myocardial ischemia has been rarely described; authors have hypothesized that this may be due to myocardial infiltration and fibrosis,2 myocyte compression,3 or superimposed repolarization of atrial masses.8 Our patient’s ECG findings of PR-segment depression, J-point elevation, and ST-segment elevation are most consistent with a pericarditis pattern, likely caused by pericardial stretch from a massive apical rhabdomyoma. The improved PR-segment depression and J-point elevation at 6 months of age suggest resolution of the acute phase of pericardial inflammation, as well as tumor involution over time; the residual ST abnormalities may reflect repolarization disturbances caused by the infiltration of the rhabdomyomas into the normal conduction system. This finding of a pericarditis pattern represents yet another ECG phenomenon that may be seen in newborns with cardiac rhabdomyomas.
Key Teaching Points.
-
•
Neonates with tuberous sclerosis and cardiac rhabdomyomas may have significant ST-segment elevation on electrocardiogram (ECG).
-
•
When a large rhabdomyoma stretches the pericardium, it may cause a pericarditis pattern on ECG.
-
•
This ECG finding may be associated with an asymptomatic newborn and a benign clinical course.
References
- 1.Aslan E., Sap F., Sert A., Odabas D. Tuberous sclerosis and cardiac tumors: new electrocardiographic finding in an infant. Tex Heart Inst J. 2014;41:530–532. doi: 10.14503/THIJ-13-3571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Iezzi F., Quarti A., Capestro A., Surace F.C., Pozzi M. Evolution of a rare ECG pattern in an aggressive case of neonatal tuberous sclerosis complex. Int J Surg Case Rep. 2018;44:197–201. doi: 10.1016/j.ijscr.2018.02.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nguyen T., Smythe J., Baranchuk A. Rhabdomyoma of the interventricular septum presenting as a Brugada phenocopy. Cardiol Young. 2011;21:591–594. doi: 10.1017/S1047951111000424. [DOI] [PubMed] [Google Scholar]
- 4.Mehta A.V. Rhabdomyoma and ventricular preexcitation syndrome. A report of two cases and review of literature. Am J Dis Child. 1993;147:669–671. doi: 10.1001/archpedi.1993.02160300075027. [DOI] [PubMed] [Google Scholar]
- 5.Shiono J., Horigome H., Yasui S. Electrocardiographic changes in patients with cardiac rhabdomyomas associated with tuberous sclerosis. Cardiol Young. 2003;13:258–263. [PubMed] [Google Scholar]
- 6.De Wilde H., Benatar A. Cardiac rhabdomyoma with long-term conduction abnormality: progression from pre-excitation to bundle branch block and finally complete heart block. Med Sci Monit. 2007;13:CS21–CS23. [PubMed] [Google Scholar]
- 7.Mühler E.G., Kienast W., Turniski-Harder V., von Bernuth G. Arrhythmias in infants and children with primary cardiac tumours. Eur Heart J. 1994;15:915–921. doi: 10.1093/oxfordjournals.eurheartj.a060610. [DOI] [PubMed] [Google Scholar]
- 8.Paech C., Gebauer R.A. ECG phenomena: pseudopreexcitation and repolarization disturbances resembling ST-elevation myocardial infarction caused by an intraatrial rhabdomyoma in a newborn. Congenit Heart Dis. 2014;9:E66–E69. doi: 10.1111/chd.12085. [DOI] [PubMed] [Google Scholar]