

Abstract
Background
Breakdown of the developmentally immature epidermal barrier may permit entry for micro‐organisms leading to invasive infection in preterm infants. Topical emollients may improve skin integrity and barrier function and thereby prevent invasive infection, a major cause of mortality and morbidity in preterm infants.
Objectives
To assess the effect of topical application of emollients (ointments, creams, or oils) on the incidence of invasive infection, other morbidity, and mortality in preterm infants.
Search methods
We used the standard search strategy of the Cochrane Neonatal Review group to search the Cochrane Central Register of Controlled Trials (CENTRAL 2015, Issue 7), MEDLINE via PubMed (1966 to August 2015), EMBASE (1980 to August 2015), and CINAHL (1982 to August 2015). We also searched clinical trials databases, conference proceedings, previous reviews and the reference lists of retrieved articles for randomised controlled trials and quasi‐randomised trials.
Selection criteria
Randomised or quasi‐randomised controlled trials that assessed the effect of prophylactic application of topical emollient (ointments, creams, or oils) on the incidence of invasive infection, mortality, other morbidity, and growth and development in preterm infants.
Data collection and analysis
Two review authors assessed trial eligibility and risk of bias and undertook data extraction independently. We analysed the treatment effects in the individual trials and reported the risk ratio and risk difference for dichotomous data and mean difference for continuous data, with respective 95% confidence intervals. We used a fixed‐effect model in meta‐analyses and explored the potential causes of heterogeneity in subgroup analyses.
Main results
We identified 18 eligible primary publications (21 trial reports). A total of 3089 infants participated in the trials. The risk of bias varied with lack of clarity on methods to conceal allocation in half of the trials and lack of blinding of caregivers or investigators in all of the trials being the main potential sources of bias.
Eight trials (2086 infants) examined the effect of topical ointments or creams. Most participants were very preterm infants cared for in health‐care facilities in high‐income countries. Meta‐analyses did not show evidence of a difference in the incidence of invasive infection (typical risk ratio (RR) 1.13, 95% confidence interval (CI) 0.97 to 1.31; low quality evidence) or mortality (typical RR 0.87, 95% CI 0.75 to 1.03; low quality evidence).
Eleven trials (1184 infants) assessed the effect of plant or vegetable oils. Nine of these trials were undertaken in low‐ or middle‐income countries and all were based in health‐care facilities rather than home or community settings. Meta‐analyses did not show evidence of a difference in the incidence of invasive infection (typical RR 0.71, 95% CI 0.51 to 1.01; low quality evidence) or mortality (typical RR 0.94, 95% CI 0.81 to 1.08; moderate quality evidence). Infants massaged with vegetable oil had a higher rate of weight gain (about 2.55 g/kg/day; 95% CI 1.76 to 3.34), linear growth (about 1.22 mm/week; 95% CI 1.01 to 1.44), and head growth (about 0.45 mm/week; 95% CI 0.19 to 0.70). These meta‐analyses contained substantial heterogeneity.
Authors' conclusions
The available data do not provide evidence that the use of emollient therapy prevents invasive infection or death in preterm infants in high‐, middle‐ or low‐income settings. Some evidence of an effect of topical vegetable oils on neonatal growth exists but this should be interpreted with caution because lack of blinding may have introduced caregiver or assessment biases. Since these interventions are low cost, readily accessible, and generally acceptable, further randomised controlled trials, particularly in both community‐ and health care facility‐based settings in low‐income countries, may be justified.
Plain language summary
Topical emollient for preventing infection in preterm infants
Review question: Does the topical application of emollients reduce the incidence of invasive infection in preterm infants?
Background: Preterm infants (born before 37 weeks' gestation) are susceptible to bloodstream and other serious infections partly because their immature skin is not a fully effective barrier to micro‐organisms. Applying emollient (ointment, cream, or oil) may protect against skin breakdown and thereby prevent micro‐organisms from spreading into the bloodstream and causing serious infection.
Study characteristics: Our search (August 2015) identified 21 eligible trial reports (in 18 primary publications). In total, 3089 infants participated. Eight trials (2086 infants) examined the effect of topical ointments or creams. Most participants were very preterm infants cared for in health‐care facilities in high‐income countries. Eleven trials (1184 infants) assessed the effect of sunflower, sunflower seed, and other vegetable oils. Nine of these trials were undertaken in low‐ or middle‐income countries and all were based in health‐care facilities rather than home or community settings.
Results: Analyses of these trial data provided low quality evidence and did not show that emollients prevent infection or death in preterm infants.
Conclusions: These analyses do not provide evidence that the use of emollient therapy prevents invasive infection or death in preterm infants in high‐, middle‐ or low‐income countries. Since these interventions are low cost, readily accessible and generally acceptable, further randomised controlled trials, particularly in both community‐ and health care facility‐based settings in low‐income countries, may be justified.
Summary of findings
Background
Description of the condition
Invasive infection is the most common serious complication associated with intensive care for preterm infants. In high‐income countries, the incidence of invasive infection in very preterm (< 32 weeks) infants is about 20%, reflecting the duration of exposure to invasive procedures (Samanta 2011; Vergnano 2011; Berrington 2012). Coagulase‐negative staphylococci cause about half of all late‐onset invasive infections (Isaacs 2003). Other pathogens include Gram‐negative bacilli (mainly enteric bacilli), Staphylococcus aureus, enterococci, and fungi (predominantly Candida spp.) (Stoll 2002; Isaacs 2004; Gordon 2006; Camacho‐Gonzalez 2013).
Very preterm infants with late‐onset invasive infection have a higher risk of mortality and a range of important morbidities including necrotising enterocolitis (NEC), retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD), and the need for intensive care and mechanical ventilation (Adams‐Chapman 2006; Berrington 2012). These higher rates of mortality and serious morbidity are usually associated with Gram‐negative bacilli, Staphylococcus aureus, enterococcal, or fungal infection. Coagulase‐negative staphylococcal infection, although more common, is generally associated with a more benign clinical course. However, even 'low grade' coagulase‐negative staphylococcal bloodstream infection may generate inflammatory cascades associated with both acute morbidity (metabolic, respiratory or thermal instability) and long‐term white matter and other brain damage that may result in neuro‐developmental disability (Stoll 2004). As a consequence of these associated morbidities, very preterm infants with invasive infection spend about 20 more days in hospital than their peers without infection (Stoll 2002). Late‐onset invasive infection therefore has major consequences for perinatal health care and service management, delivery and costs.
Low and middle‐income countries
The epidemiology of invasive infection in preterm or low birth weight infants in low‐ or middle‐income countries differs from that in high‐income countries (Zaidi 2005). The overall incidence is much higher but infections are less likely to be directly associated with intensive care or invasive procedures. Most infections are due to Gram‐negative bacilli and the attributable mortality and morbidity is greater than in high‐income settings.
Description of the intervention
Skin barrier function in preterm infants
Maturation of the epidermis in utero does not occur until about 34 weeks gestational age. Although skin maturation is accelerated ex utero, the stratum corneum, eccrine glands, and acid mantle of preterm infants remain physically and functionally immature for several weeks after birth (Harpin 1983). Compared with term infants, preterm infants have few dermal elastic fibres and a weak dermal‐epidermal junction prone to disruption. Additionally, very preterm infants lack a vernix caseosa, a mixture of proteins, lipids and water with anti‐inflammatory and antimicrobial properties (Marchini 2002). As well as increasing the rate of transepidermal evaporative heat loss, immaturity of the epidermal barrier predisposes preterm infants to microbial colonisation and infection (Evans 1986; Rutter 1988; Cartlidge 2000; Rutter 2000). The risk of infection is increased further because preterm infants' fragile skin is susceptible to damage through several mechanisms including thermal, chemical, adhesive, friction and pressure injuries, as well as iatrogenic skin breaks from blood sampling, cannula placement, or extravasation of intravenously‐administered fluids or medicines (Dyer 2013; Ness 2013).
Emollients
Topical emollients are moisturising treatments applied directly to the skin to protect the stratum corneum, enhance epidermal barrier function and reduce evaporative water losses (Pickens 2000). Most proprietary or commercially‐available emollients are creams (oil‐in‐water suspensions) or ointments (oily creams/water‐in‐oil) (BNF for Children 2014). Some preparations contain antimicrobial or hydrating agents. Natural vegetable or plant oils (for example, mustard, safflower, sesame, coconut, olive, and soybean oils) have emollient properties and in many low‐ and middle‐income countries application of these to the newborn infant's whole body surface is a widespread traditional practice (Darmstadt 2002a; Darmstadt 2002b).
How the intervention might work
As well as providing a physical barrier to skin disruption, emollient oils, creams, or ointments provide lipids that are integrated into the epidermis to further enhance skin barrier function. Topical oils may also be a transcutaneous nutritional source of essential fatty acids for preterm or low birth weight infants (Lee 1993).
Potential adverse effects of emollients
Although emollients may plausibly improve skin barrier function, the process of application, which may include massage, could disrupt skin integrity in preterm infants. Emollients may also reduce the antimicrobial function of the acid mantle which could potentially increase the risk of colonisation and infection. Many emollients contain excipients which have the potential to be absorbed through the immature epidermal barrier resulting in contact sensitivity, epidermal injury, cutaneous haemorrhagic necrosis, and uraemia (Ness 2013).
Another concern is that emollient preparations may become contaminated and colonised with potential pathogens, particularly preparations stored in non‐sealed containers (BNF for Children 2014). A further practical limitation is that emollients may reduce the effectiveness of adhesives needed to secure intravenous catheters or endotracheal tubes.
Why it is important to do this review
Given the potential for topical emollient therapy to improve skin barrier function and prevent infection in preterm infants, we have assessed the available evidence to inform practice and research.
Objectives
To assess the effect of topical application of emollients (ointments, creams, or oils) on the incidence of invasive infection, other morbidity, and mortality in preterm infants.
Methods
Criteria for considering studies for this review
Types of studies
Controlled trials using random or quasi‐random participant allocation. Cluster randomised trials where the unit of randomisation was a group of infants (for example, all infants cared for in a participating neonatal unit) were also eligible for inclusion. Cross‐over studies that assessed the use of emollient therapy in the same infant were not eligible for inclusion as this design would not permit a meaningful assessment of the effect of the intervention on the primary outcome for this review.
Types of participants
Preterm infants (< 37 weeks gestation)
Types of interventions
We planned the following comparisons: 1. Topical ointment or cream versus routine skin care. 2. Topical oil versus routine skin care. 3. Topical ointment or cream versus topical oil. 4. One topical oil (or a combination of oils) versus another oil (or a combination of oils).
Types of outcome measures
Primary outcomes
-
Invasive infection diagnosed more than 48 hours after birth as determined by culture from a normally sterile site: cerebrospinal fluid; blood (from peripheral sites, not from indwelling catheters); urine (obtained by sterile urethral catheterization or suprapubic bladder tap); bone or joint, peritoneum, pleural space, or central venous line tip; or findings on autopsy examination consistent with invasive microbial infection. If sufficient data were available, we planned to examine specific effects on infection with these organisms:
Coagulase‐negative staphylococci (CoNS)
Other bacteria (Gram‐negative bacilli, S. aureus, enterococci)
Fungi
Secondary outcomes
Death (all cause) before hospital discharge.
Growth: Weight gain (grams/day, or grams/kg/day); linear growth (mm/week); head circumference (mm/week); skinfold thickness (mm/week) during the trial period.
Neurodevelopmental outcomes assessed at more than 12 months post‐term (measured using validated assessment tools) and classifications of disability, including auditory and visual disability. A composite outcome "severe neurodevelopmental disability" was defined as any one or combination of the following: non‐ambulant cerebral palsy, severe developmental delay, auditory impairment and visual impairment.
BPD (oxygen supplementation at 36 weeks postmenstrual age)
NEC (Bell stage 2 or 3) (Bell 1978)
ROP requiring treatment (medical or surgical) (ICCROP 2005)
Search methods for identification of studies
We used the standard search strategy of the Cochrane Neonatal Review Group.
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, Issue 7, 2015), MEDLINE (1966 to August 2015), EMBASE (1980 to August 2015, CINAHL (1982 to August 2015), and LILACS (1982 to August 2014) using the following text words and MeSH terms:
[exp Infant, Newborn/ OR Premature Birth/ OR (neonat$ or neo nat$).ti,ab. OR (newborn$ or new born$ or newly born$).ti,ab. OR (preterm or preterms or pre term or pre terms).ti,ab. OR (preemie$ or premie or premies).ti,ab. OR (prematur$ adj3 (birth$ or born or deliver$)).ti,ab. OR (low adj3 (birthweight$ or birth weight$)).ti,ab. OR (lbw or vlbw or elbw).ti,ab. OR infan$.ti,ab. OR (baby or babies).ti,ab.] AND [emollients/ OR Skin cream/ OR Ointments/ OR Dermatological agents/ OR Plant oils/ OR emollient$.ti,ab. (skin adj6 (cream$ or oil$ or unguent$ or gel$ or moisturi$ or honey or humectant$ or ointment$ or foam$ or lotion$ or conditioner$)).ti,ab. OR (topical adj2 (agent$ or treatment$ or therap$)).ti,ab. OR skin care product$.ti,ab.]
The search outputs were limited with the relevant search filters for clinical trials. We did not apply any language restriction.
We searched the World Health Organization (WHO) International Clinical Trials Registry Platform (www.who.int/ictrp/en/) and ClinicalTrials.gov (www.clinicaltrials.gov/) for completed or ongoing trials.
Searching other resources
We examined reference lists in previous reviews and included studies. We searched the proceedings of the annual meetings of the Pediatric Academic Societies (1993 to present), the European Society for Paediatric Research (1995 to 2014), the Royal College of Paediatrics and Child Health (2000 to 2015), the Perinatal Society of Australia and New Zealand (2000 to 2015), the European Society for Paediatric Infectious Diseases (2005 to 2014), and the Infectious Diseases Society of America (2003 to 2014). Trials reported only as abstracts were eligible if sufficient information was available from the report, or from contact with the authors, to fulfil the inclusion criteria.
Data collection and analysis
We used the standard methods of the Cochrane Neonatal Review Group.
Selection of studies
Two review authors screened the title and abstract of all studies identified by the above search strategy. We reassessed the full text of any potentially eligible reports and excluded those studies that did not meet all of the inclusion criteria. We discussed any disagreements until consensus was achieved.
Data extraction and management
We used a data collection form to aid extraction of relevant information from each included study. Two review authors extracted the data separately. We discussed any disagreements until consensus was achieved. We asked the investigators for further information if data from the trial reports were insufficient.
Assessment of risk of bias in included studies
We used the criteria and standard methods of the Cochrane Collaboration and the Cochrane Neonatal Group to assess the methodological quality of any included trials (Higgins 2011). We requested additional information from the trial authors to clarify methodology and results as necessary. We evaluated and reported the following issues in the 'Risk of bias' tables:
Sequence generation (the method used to generate the allocation sequence):
low risk ‐ any truly random process, e.g. random number table; computer random number generator;
high risk ‐ any non‐random process, e.g. odd or even date of birth; hospital or clinic record number;
unclear risk ‐ no or unclear information provided.
Allocation concealment (the method used to conceal the allocation sequence):
low risk: e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes;
high risk: open random allocation, e.g. unsealed or non‐opaque envelopes, alternation; date of birth;
unclear ‐ no or unclear information provided.
Blinding (the methods used to ensure blinding of participants, clinicians and caregivers, and outcome assessors):
low risk;
high risk;
unclear.
Incomplete outcome data (completeness of data including attrition and exclusions from the analysis for each outcome and any reasons for attrition or exclusion where reported): We categorised completeness as:
low risk ‐ adequate (< 10% missing data);
high risk ‐ inadequate (> 10% missing data);
unclear risk ‐ no or unclear information provided.
Quality of evidence
We assessed the quality of evidence for the main comparisons at the outcome level using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach (Guyatt 2011a). This methodological approach considers evidence from randomised controlled trials as high quality that may be downgraded based on consideration of any of five areas: design (risk of bias), consistency across studies, directness of the evidence, precision of estimates, and presence of publication bias (Guyatt 2011a). The GRADE approach results in an assessment of the quality of a body of evidence in one of four grades: 1) High: We are very confident that the true effect lies close to that of the estimate of the effect; 2) Moderate: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different; 3) Low: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect; 4) Very Low: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect (Schünemann 2013).
Two review authors independently assessed the quality of the evidence found for outcomes identified as critical or important for clinical decision making: mortality and invasive infection.
In cases where we considered the risk of bias arising from inadequate concealment of allocation, randomised assignment, complete follow‐up or blinded outcome assessment to reduce our confidence in the effect estimates, we downgraded the quality of evidence accordingly (Guyatt 2011b). Consistency was evaluated by similarity of point estimates, extent of overlap of confidence intervals (CI) and statistical criteria including measurement of heterogeneity (I²). The quality of evidence was downgraded when inconsistency across studies' results was present being large and unexplained (some studies suggest important benefit and others no effect or harm without a clinical explanation) (Guyatt 2011d). Precision was assessed according with the 95% CI around the pooled estimation (Guyatt 2011c). When trials were conducted in populations other than the target population, we downgraded the quality of evidence because of indirectness (Guyatt 2011e).
The pooled estimates of the effects and 95% CI with explicit judgements for each of the above aspects assessed were entered into the Guideline Development Tool, the software used to create 'Summary of findings' (SoF) tables (GRADEpro 2008). All judgements involving the assessment of the study characteristics described above were explained in footnotes or comments in the SoF table.
Measures of treatment effect
We analysed the treatment effects in the individual trials using Review Manager 5 and reported risk ratio (RR) and risk difference (RD) for dichotomous data and mean difference (MD) for continuous data, with respective 95% CI. We determined the number needed to treat for an additional beneficial outcome (NNTB) or for an additional harmful outcome (NNTH) for analyses with a statistically significant difference in the RD.
Unit of analysis issues
The unit of analysis was the participating infant in individually randomised trials. The participating neonatal unit or section of a neonatal unit was the intended unit of analysis in cluster randomised trials.
Dealing with missing data
We requested additional data from the investigators if data on important outcomes were missing or reported unclearly.
Assessment of heterogeneity
We examined the treatment effects of individual trials and heterogeneity between trial results by inspecting the forest plots. We calculated the I² statistic for each RR analysis to quantify inconsistency across studies and describe the percentage of variability in effect estimates that may be due to heterogeneity rather than to sampling error. If we detected substantial or considerable heterogeneity (I² > 50%), we explored the possible causes (for example, differences in study design, setting, participants, or interventions).
Assessment of reporting biases
If more than 10 trials were included in a meta‐analysis, we examined a funnel plot for asymmetry.
Data synthesis
We used the fixed‐effect model in Review Manager 5 for meta‐analyses.
Subgroup analysis and investigation of heterogeneity
We planned the following subgroup comparisons:
Very preterm (< 32 weeks) infants (versus infants born ≥ 32 weeks)
Low‐ and middle‐income versus high‐income countries: (see: http://data.worldbank.org/about/country‐and‐lending‐groups#High_income for classification (accessed 18th August 2014))
Results
Description of studies
Results of the search
We screened 2696 articles but 2658 records did not meet eligibility criteria (see: Figure 1).
1.

Study flow diagram.
Included studies
We included 21 eligible trial reports in 18 primary publications (Characteristics of included studies). Most reports were of two‐arm trials, but four were of three‐arm trials (Arora 2005; Darmstadt 2005; Sankaranarayanan 2005; Kiechl‐Kohlendorfer 2008).
Participants and setting
The included trials were conducted since the late 1990s in neonatal care centres in high‐income countries (USA, Saudi Arabia, Germany, Austria, and France), middle‐income countries (Turkey, India, Egypt, Iran, and Brazil), and a low‐income country (Bangladesh).
In total, 3089 infants participated. Most participants were born before 37 weeks' gestation or of birth weight less than 2500 g.
Birth weight or gestational age inclusion criteria:
Lane 1993: 29 to 36 weeks
Nopper 1996: < 33 weeks
Pabst 1999: 26 to 30 weeks
Soriano 2000: < 1700 g
Edwards 2004: < 31 weeks and 501 to 1000 g
Darmstadt 2004: < 34 weeks
Arora 2005: < 1500 g
Darmstadt 2005: < 33 weeks
Sankaranarayanan 2005: 1500 to 2000 g
Kiechl‐Kohlendorfer 2008: 25 to 36 weeks
Vaivre‐Douret 2008: 31 to 34 weeks
Farhat 2010: < 2000 g and < 37 weeks
Kumar 2013: < 1800 g and < 35 weeks
Fallah 2013: 1500 to 1999 g and 33 to 37 weeks
Alkharfy 2014: < 1250 g and < 33 weeks
Erdemir 2014: < 34 weeks
Kanti 2014: 1500 to 2500 g
Salam 2015: 26 to 36 weeks and > 750 g
Interventions
The intervention was generally commenced within three to seven days after birth, and continued until about two to four weeks postnatally, or until hospital discharge. The ointments or oils were usually massaged between two and six times each day into the whole skin surface (except the face or head) by either the infant's mother or nurse or other caregiver.
Comparison 1.
Eight trials compared treatment with emollient ointment (mainly proprietary preparations: Aquaphor®, Bepanthen®, Eucerin Creme®, petroleum jelly, olive oil/lanolin cream) versus routine skin care (Lane 1993; Nopper 1996; Pabst 1999; Edwards 2004; Darmstadt 2005; Kiechl‐Kohlendorfer 2008; Alkharfy 2014; Erdemir 2014).
Comparison 2.
Eleven trials compared treatment with a natural vegetable or plant oil versus routine skin care:
sunflower oil (Darmstadt 2004; Arora 2005; Darmstadt 2005; Farhat 2010; Kumar 2013; Fallah 2013; Kanti 2014)
coconut or mineral oil (Sankaranarayanan 2005; Salam 2015)
soybean oil (Soriano 2000)
almond oil or vegetable oil (Vaivre‐Douret 2008)
Comparison 3.
One trial compared ointment (Aquaphor®) versus sunflower seed oil (Darmstadt 2005).
Comparison 4.
One trial compared topical coconut oil versus mineral oil (Sankaranarayanan 2005).
Outcomes
Most trials reported data on the incidence of infection and mortality. Several trials of topical oil versus standard care in low‐ or middle‐income settings primarily assessed growth parameters but unpublished data on the rate of infection and death were available from the study investigators (Soriano 2000; Arora 2005; Sankaranarayanan 2005; Kumar 2013). None of the studies assessed any long‐term growth or neurodevelopmental outcomes.
Excluded studies
We screened the full‐text of 20 articles of studies which did not meet inclusion criteria (see Characteristics of excluded studies). Two potentially eligible studies will be re‐assessed when further information is available from the authors or via publication of the full report (Hu 2014; Nangia 2015).
Risk of bias in included studies
See Figure 2
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Methods to achieve adequate allocation concealment were reported in 10 trials. In the other trials where the methods have not been reported, we sought (but have not yet received) clarification.
Darmstadt 2005: It is unclear from the published report why there is a difference in the number of infants in the control group versus intervention groups given that allocation was blocked in groups of six infants (two infants in each of the three groups). The principal investigator has provided these possible explanations for the skewed distribution of participants:
1. The trial originally had a fourth arm (emollient therapy with safflower oil) which was deemed unacceptable to families and caregivers and removed from the trial when 24 infants had been randomised to the arms. These infants were not included in the final analyses.
2. The original allocation sequence generation method was changed from the original manual process (selecting from a block of six envelopes) to a computer‐generated sequence that did not maintain the balance of assignments within blocks.
Blinding
The caregivers and investigators were not blinded to the intervention in any of the trials.
Incomplete outcome data
All trials achieved complete or near‐complete (> 90%) evaluation of primary outcomes.
Effects of interventions
Summary of findings for the main comparison. Topical ointment or cream versus routine skin care for preventing infection in preterm infants.
| Topical ointment or cream versus routine skin care for preventing infection in preterm infants | ||||||
|
Patient or population: Preterm (< 37 weeks') and low birth weight (< 2500 g) infants
Settings: High‐income countries, and low‐ and middle‐income countries
Intervention: Topical ointment or cream ¶ Comaparison: Routine skin care | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Routine skin care | Topical ointment or cream | |||||
| Invasive infection (any organism) Follow‐up: until hospital discharge | 228 per 1000 | 257 per 1000 (221 to 298) | RR 1.13 (0.97 to 1.31) | 2098 (8) | ⊕⊕⊝⊝ low1,2 | Six trials were conducted in high‐income countries, one in a middle‐income country (Turkey), and one in a low‐income country (Bangladesh). |
| Mortality Follow‐up: until hospital discharge | 203 per 1000 | 176 per 1000 (152 to 209) | RR 0.87 (0.75 to 1.03) | 2067 (7) | ⊕⊕⊝⊝ low1,3 | Five trials were conducted in high‐income countries, one in a middle‐income country (Turkey) and one in a low‐income country (Bangladesh). |
¶ Most trials used proprietary emollient, most commonly Aquaphor® (a water free petrolatum‐based ointment) and Bepanthen® (a water‐containing lanolin and petroleum‐based ointment)
1Downgraded one level due to serious risk of bias (unclear random sequence generation in most trials; caregivers and investigators not blinded in all trials). In one trial (Darmstadt 2005), there was a disruption in the method of the randomisation process, which may have contributed to an unequal distribution of infants between groups.
2 Downgraded one level due to inconsistency: I² = 36%. Moderate heterogeneity not explained by pre‐specified sub‐group analysis.
3 Downgraded one level due to inconsistency: I² = 39%. Moderate heterogeneity not explained by pre‐specified sub‐group analysis.
Summary of findings 2. Topical oil versus routine skin care for preterm and low birth weight infants.
| Topical oil versus routine skin care for preventing infection in preterm infants | ||||||
|
Patient or population: Preterm (< 37 weeks) and low birth weight (< 2500 g) infants
Settings: High‐income countries, and low‐ and middle‐income countries
Intervention: Topical oil¶ Comaparison: Routine skin care | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Routine skin care | Topical oil | |||||
| Invasive infection (any organism) Follow‐up: until hospital discharge | 142 per 1000 | 139 per 1000 (92 to 207) | RR 0.71 (0.51 to 1.01 | 844 (6) | ⊕⊕⊝⊝ low1,2 | Five trials were conducted in low‐ or middle‐income countries, and one in a high income country (Germany). |
| Mortality Follow‐up: until hospital discharge | 357 per 1000 | 336 per 1000 (293 to 389) | RR 0.94 (0.81 to 1.08) | 1002 (9) | ⊕⊕⊕⊝ moderate1 | Seven trials were conducted in low‐ or middle‐income countries, and two in a high income country (France, Germany). |
¶ Sunflower, sunflower seed, other vegetable oils.
1 Downgraded one level due to serious risk of bias (unclear random sequence generation for Soriano 2000; no blinding in any trial). 2 Downgraded one level due to inconsistency. There was evidence of considerable heterogeneity in this meta‐analysis (I² = 80%).
Comparison 1. Topical ointment or cream versus routine skin care
Confirmed invasive infection (outcome 1.1–1.5):
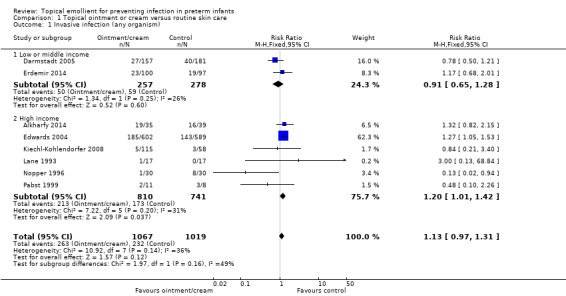
Meta‐analysis did not show a statistically significant difference (typical RR 1.13, 95% CI 0.97 to 1.31; typical RD 0.03, 95% CI −0.01 to 0.07; 8 trials, 2086 infants) (Figure 3). There was evidence of moderate heterogeneity (I² = 36%) that was not explained by pre‐specified subgroup analyses:
3.

Forest plot of comparison: 1 Topical ointment or cream versus routine skin care, outcome: 1.1 Invasive infection (any organism).
1. Very preterm (< 32 weeks) infants (versus infants born ≥ 32 weeks): Only two trials restricted participation to very preterm infants (Pabst 1999; Edwards 2004). Meta‐analysis showed a statistically significant higher incidence of invasive infection (typical RR 1.25, 95% CI 1.04 to 1.50; typical RD 0.06, 95% CI 0.01 to 0.11; NNTH 17, 95% CI 9 to 100; 2 trials, 1210 infants; Figure 4). The other trials did not report subgroup data for infants born at 32 weeks or more.
4.

Forest plot of comparison: 1 Topical ointment or cream versus routine skin care, outcome: 1.2 Invasive infection (trials with only very preterm infants participating).
2. Low‐ and middle‐income versus high‐income countries: Meta‐analysis did not show a statistically significant difference in the subgroup of trials conducted in low‐ and middle‐income countries (typical RR 0.91, 95% CI 0.65 to 1.28; typical RD −0.02, 95% CI −0.09 to 0.05; 2 trials, 535 infants) but did show a borderline statistically significant higher incidence in trials conducted in high‐income countries (typical RR 1.20, 95% CI 1.01 to 1.42; typical RD 0.05, 95% CI 0.00 to 0.09; 6 trials, 1551 infants). The test for subgroup difference was not statistically significant (Chi² = 1.97, df = 1 (P = 0.16), I² = 49%) (Figure 3).
Infection with specific organisms
Six reports provided data on the type of infecting organism (Lane 1993; Nopper 1996; Pabst 1999; Edwards 2004; Darmstadt 2005; Erdemir 2014). The meta‐analyses showed a borderline statistically significant higher risk of infection with coagulase‐negative staphylococci but no statistically significant effects on infection with other bacteria or fungi:
Coagulase‐negative staphylococci (outcome 1.3): typical RR 1.30, 95% CI 1.03 to 1.65; typical RD 0.03, 95% CI 0.00 to 0.07; 6 trials, 1839 infants.
Other bacteria (Gram‐negative bacilli, S. aureus, enterococci) (outcome 1.4): typical RR 0.84, 95% CI 0.63 to 1.12; typical RD −0.02, 95% CI −0.04 to 0.01.
Fungi (outcome 1.5): typical RR 1.27, 95% CI 0.78 to 2.06; typical RD 0.01, 95% CI −0.01 to 0.03.
Mortality (outcome 1.6–1.7):
Meta‐analysis did not show a statistically significant difference (typical RR 0.87, 95% CI 0.75 to 1.03: typical RD −0.02, 95% CI −0.05 to 0.00; 6 trials, 2067 infants) (Figure 5). There was evidence of moderate heterogeneity (I² = 39%) that was not explained by pre‐specified subgroup analyses:
5.

Forest plot of comparison: 1 Topical ointment or cream versus routine skin care, outcome: 1.6 Mortality.
1. Very preterm (< 32 weeks) infants (versus infants born ≥ 32 weeks): Only one trial restricted participation to very preterm infants (Edwards 2004). Analysis of this trial did not show a statistically significant difference (RR 0.90, 95% CI 0.65 to 1.23; RD −0.01, 95% CI −0.05 to 0.02; 1 trial, 1191 infants; Figure 6). The other trials did not report subgroup data for infants born at 32 weeks or more.
6.

Forest plot of comparison: 1 Topical ointment or cream versus routine skin care, outcome: 1.7 Mortality (trials with only very preterm infants participating).
2. Low‐ and middle‐income versus high‐income countries: Meta‐analysis showed a borderline significant lower incidence in the subgroup of trials conducted in low‐ and middle‐income countries (typical RR 0.82, 95% CI 0.69 to 0.98: typical RD −0.08, 95% CI −0.15 to −0.01; NNTB 12, 95% CI 7 to 100; 2 trials, 535 infants), but did not show a statistically significant difference in trials conducted in high‐income countries (typical RR 0.96, 95% CI 0.71 to 1.31; typical RD 0.00, 95% CI −0.03 to 0.03; 5 trials, 1532 infants). The test for subgroup difference was not statistically significant (Chi² = 0.80, df = 1 (P = 0.37), I² = 0%) (Figure 5).
Growth: Not reported.
Neurodevelopmental outcomes: Not reported.
BPD (outcome 1.8):
Meta‐analysis did not detect a statistically significant difference (typical RR 1.00, 95% CI 0.88 to 1.14; typical RD 0.00, 95% CI −0.06 to 0.06; 2 trials, 1009 infants).
NEC (outcome 1.9):
Meta‐analysis did not detect a statistically significant difference (typical RR 1.25, 95% CI 0.89 to 1.76; typical RD 0.02, 95% CI −0.01 to 0.05; 4 trials, 1472 infants). There was no evidence of heterogeneity in this meta‐analysis (I² = 0%).
ROP requiring treatment (outcome 1.10):
Only Edwards 2004 reported the incidence of ROP. This trial did not find a statistically significant difference (RR 0.99, 95% CI 0.77 to 1.28; RD −0.00, 95% CI −0.05 to 0.05; 1 trial, 952 infants).
Comparison 2. Topical oil versus routine skin care
Confirmed invasive infection (outcome 2.1–2.4):
Meta‐analysis did not detect a statistically significant difference in confirmed invasive infection (typical RR 0.71, 95% CI 0.51 to 1.01; typical RD −0.04, 95% CI −0.09 to 0.0; 6 trials, 844 infants) (Figure 7). There was evidence of considerable heterogeneity in this meta‐analysis (I² = 69%) that was not explained by pre‐specified subgroup analyses:
7.
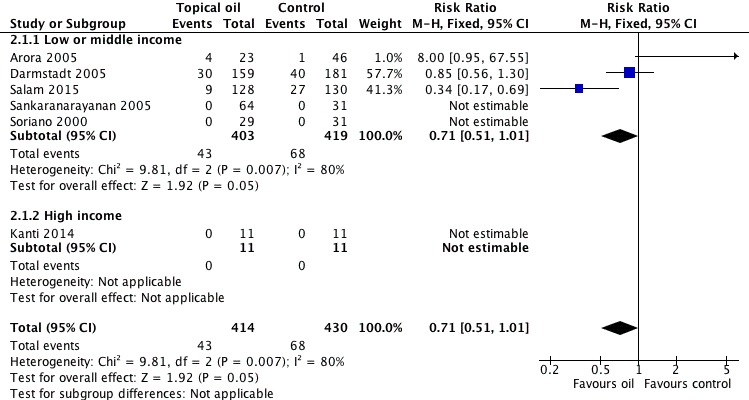
Forest plot of comparison: 2 Topical oil versus routine skin care, outcome: 2.1 Invasive infection (any organism).
1. Very preterm (< 32 weeks) infants (versus infants born ≥ 32 weeks): The included trials did not report subgroup data for infants born at less than 32 weeks versus those born at 32 weeks or more.
2. Low‐ and middle‐income versus high‐income countries: typical RR 0.71, 95% CI 0.51 to 1.01; typical RD −0.05, 95% CI −0.09 to 0.0; 5 trials, 822 infants.
Darmstadt 2004 stated that the incidence of invasive infection was statistically significantly lower in the intervention (sunflower seed oil) group but did not report the number of infants in each group who had (at least one) episode of invasive infection. We contacted the principal investigator but these data are not available for inclusion in this review.
Infection with specific organisms
Two reports provided data on the type of infecting organism (Darmstadt 2005; Salam 2015). None of the participants in three of the trials had an episode of invasive infection (Soriano 2000; Sankaranarayanan 2005; Kanti 2014). None of the meta‐analyses showed a statistically significant difference:
Coagulase‐negative staphylococci (outcome 2.2): typical RR 0.15, 95% CI 0.02 to 1.16; typical RD −0.02, 95% CI −0.03, 0.0; 5 trials, 775 infants.
Other bacteria (Gram‐negative bacilli, Staphylococcus aureus, enterococci) (outcome 2.3): typical RR 0.70, 95% CI 0.47 to 1.05; typical RD −0.04, 95% CI −0.08 to 0.01; 5 trials, 775 infants.
Fungi (outcome 2.4): typical RR 1.93, 95% CI 0.42 to 8.78; typical RD 0.01, 95% CI −0.01 to 0.02; 5 trials, 775 infants.
Mortality (outcome 2.5):
Meta‐analysis did not detect a statistically significant difference: typical RR 0.94, 95% CI 0.81 to 1.08; typical RD 0.00, 95% CI −0.03 to 0.02; 9 trials, 1002 infants (Figure 8). There was no evidence of heterogeneity in this meta‐analysis (I² = 0%). Pre‐specified subgroup analyses did not detect any subgroup effects:
8.

Forest plot of comparison: 2 Topical oil versus routine skin care, outcome: 2.5 Mortality.
1. Very preterm (< 32 weeks) infants (versus infants born ≥ 32 weeks): The included trials did not report subgroup data for infants born at less than 32 weeks versus those born at 32 weeks or more.
2. Low‐ and middle‐income versus high‐income countries:
Low‐ or middle‐income countries: typical RR 0.94, 95% CI 0.81 to 1.08; typical RD 0.0, 95% CI −0.03 to 0.02; 7 trials, 931 infants.
High‐income countries: typical RR not estimable (no events): typical RD 0.00, 95% CI −0.07 to 0.07; 2 trials, 71 infants.
Darmstadt 2004 reported infection‐attributed mortality but not all‐cause mortality data. We contacted the principal investigator but this information is not available for inclusion.
Growth during the trial period (outcome 2.6):
Meta‐analyses found a statistically significant higher rate of weight gain (WMD 2.55 (95% CI 1.76 to 3.34) g/kg/day), linear growth (WMD 1.22 (95% CI 1.01 to 1.44) mm/week), and head circumference growth (WMD 0.45 (95% CI 0.19 to 0.70) mm/week). Triceps skinfold thickness was not statistically significantly different (Figure 9).
9.

Forest plot of comparison: 2 Topical oil versus routine skin care, outcome: 2.6 Growth.
Neurodevelopmental outcomes: Not reported.
BPD: Not reported.
NEC: Not reported.
ROP: Not reported.
Comparison 3. Topical ointment or cream versus oil
Invasive infection (outcome 3.1):
Darmstadt 2005 did not detect a statistically significant difference in the number of infants with invasive infection (RR 0.91, 95% CI 0.57 to 1.46; RD −0.02, 95% CI −0.10 to 0.07).
Infection with specific organisms
(i) Coagulase‐negative staphylococci (outcome 3.2): No events.
(ii) Other bacteria (Gram‐negative bacilli, Staphylococcus aureus, enterococci) (outcome 3.3): No statistically significant difference (RR 0.90, 95% CI 0.53 to 1.50; RD −0.02, 95% CI −0.10 to 0.06; 1 trial, 316 infants).
(iii) fungi (outcome 3.4): No statistically significant difference (RR 1.35, 95% CI 0.31 to 5.94; RD 0.01, 95% CI −0.03 to 0.04; 1 trials, 316 infants).
Mortality (outcome 3.5):
Darmstadt 2005 found a statistically significant reduction in mortality in the ointment/cream (Aquaphor) group (RR 0.82, 95% CI 0.68 to 0.98; RD −0.12, 95% CI −0.23 to −0.01; NNTB 8, 95% CI 4 to 100).
Growth outcomes: Not reported.
Neurodevelopmental outcomes: Not reported.
BPD: Not reported.
NEC: Not reported.
ROP: Not reported.
Comparison 4. Topical oil versus another oil
Invasive infection and mortality:Sankaranarayanan 2005 did not detect any episodes of invasive infection or mortality in either group.
Growth during the trial period (outcome 4.3.1):Sankaranarayanan 2005 found a statistically significant higher rate of weight gain (WMD 2.00 (95% CI 0.84, 3.16) g/kg/day) in the coconut oil group compared to the mineral oil group. Rates of change in length and head circumference were not statistically significantly different.
Neurodevelopmental outcomes: Not reported.
BPD: Not reported.
NEC: Not reported.
ROP: Not reported.
Discussion
Summary of main results
Topical ointment or cream versus routine skin care
We found eight randomised controlled trials in which a total of 2086 preterm infants participated. The trials were undertaken during the past 20 years. Six were conducted in high‐income countries, one in a middle‐income country (Turkey) and one in a low‐income country (Bangladesh). Most trials used proprietary emollient, most commonly Aquaphor® (a water‐free petrolatum‐based ointment) and Bepanthen® (a water‐containing lanolin and petroleum‐based ointment). Most participants were preterm infants born before 32 weeks gestation and in the largest trial all participants were extremely low birth weight infants (N = 1191) (Edwards 2004).
Meta‐analyses did not show differences in the incidence of invasive infection, mortality or morbidity (BPD, ROP, NEC) before discharge from hospital. These meta‐analyses contained moderate heterogeneity. We did not find evidence of a subgroup effect in a pre‐specified analysis of trials set in high‐income versus low‐ or middle‐income countries; the test for subgroup differences was not statistically significant and the 95% CIs for the RR estimates overlapped (Figure 5; Figure 7).
Topical oil versus routine skin care
We found 11 randomised controlled trials in which a total of 904 preterm infants participated. The trials were undertaken within the past 20 years. Nine were conducted in low‐ or middle‐income countries, and two in high‐income countries (Vaivre‐Douret 2008; Kanti 2014). All of the trials were based in health‐care facilities rather than home or community settings. The most commonly used emollients were sunflower and other plant or vegetable oils. All of the trials had some methodological imitations, particularly lack of blinding of caregivers and clinicians, and uncertainty about the mechanics of the randomisation procedure.
Meta‐analyses did not show differences in the incidence of invasive infection or neonatal mortality. Infants massaged with vegetable oil had a higher rate of weight gain (about 2 g/kg/day), linear growth (about 0.8 mm/week), and head growth (about 0.8 mm/week) but these meta‐analysis contained considerable heterogeneity. There are not yet any data at all on long‐term growth and developmental outcomes.
Topical ointment or cream versus topical oil
One trial that compared ointment (Aquaphor®) versus sunflower seed oil found a statistically significant reduction in mortality in the ointment group but no evidence of an effect on the invasive infection rate (Darmstadt 2005).
Different oils
One small trial that compared coconut oil versus mineral oil did not detect any episodes of invasive infection or mortality in either group (Sankaranarayanan 2005).
Overall completeness and applicability of evidence
Topical ointment or cream versus routine skin care
The available data do not provide any evidence that routine use of emollient ointments or creams reduces the incidence of invasive infection in preterm infants. In fact, the subgroup analysis of trials set in high‐income countries suggests that routine topical application of ointments might increase the risk of infection. These trials recruited predominantly very preterm infants and most participants in the largest trial were of extremely low birth weight. The commonest organisms causing bloodstream infection in these trials were coagulase‐negative staphylococci. Although some care practices, including infection control measures, feeding policies, and exposure to invasive procedures, may have changed since the larger trials that were conducted more than about 15 years ago, these findings are likely to remain applicable to the modern context of neonatal intensive care in high‐income countries.
One plausible mechanism for the increased risk of infection with coagulase‐negative staphylococci is that application of the ointment causes skin trauma and epidermal micro‐abrasion which permits transcutaneous migration of skin commensals. However, this is not consistent with the reported finding in these trials that topical emollient improves skin condition as measured by skin score and evaporative water loss. Another possibility is that contamination may have occurred during the application process and that the ointment provided an environment conducive to the proliferation of bacteria. Our analyses did not demonstrate an effect on infection due to other, more pathogenic, bacteria (Gram negative bacilli, enterococci, S. aureus) or fungi but these infections occurred infrequently compared with coagulase‐negative staphylococcal infection and the 95% CI for these estimates are broad. It remains possible and plausible that emollient application may also increase the risk of infection with Gram‐negative bacilli, enterococci, S. aureus or fungi as these organisms preferentially colonise moist environments (Chiller 2001). Larger trials would be needed to obtain more precise estimates of the specific effect on these less common, though much more virulent, infections.
The finding from one trial that treatment with a topical ointment (Aquaphor®) compared to routine skin care or application of vegetable oil results in a statistically significant and substantial reduction in neonatal mortality should be interpreted and applied cautiously (Darmstadt 2005). Uncertainty exists concerning the method used to randomly allocate participants (discussed below).
Topical oil versus routine skin care
Although the meta‐analyses did not show statistically significant differences in the incidence of invasive infection or mortality in infants treated with vegetable oils versus standard skin care, the 95% CI for these estimates are broad. More precise estimates of effect sizes may be obtained when further data from a trial that has not yet reported the number of infants who developed invasive infection or died are available (Darmstadt 2004). Further data may also be available for inclusion when the on‐going or incompletely repeated trials are completed and their findings published (Mullany 2010; Hu 2014; Nangia 2015).
The mechanism by which massage with vegetable oils increases the rates of weight and length gain is not clear. Transcutaneously absorbed lipids may be an additional source of calories or essential fatty acids. Reducing evaporative heat loss is another plausible mechanism. Applying topical oils by massage may have a calming effect that reduces energy expenditure or promotes more effective enteral feeding behaviours. Given the high risk of nutritional compromise that exists for preterm infants, particularly in low‐ and middle‐income countries, it may be appropriate to undertake further trials to assess whether topical vegetable oils may have clinically important benefits during this potentially critical phase of growth and growth‐programming (Mullany 2005).
Quality of the evidence
We assessed the quality of evidence for the main outcomes (risk of infection and death) to be low or moderate quality. Most of the meta‐analyses contained heterogeneity that was not explained by subgroup analyses. Many of the trials contained methodological weakness, specifically uncertainty about adequate allocation concealment methods in about half of the trials and lack of blinding in all of the trials. Parents, caregivers, clinicians and investigators were likely to have been aware of the treatment group to which infants had been allocated and this knowledge may have affected some care‐giving practices or investigation strategies, including thresholds for screening for invasive infection, that may have affected the outcomes assessed.
A further specific concern exists with regard to the random allocation process used in one of the largest of the included trials (Darmstadt 2005). The report states that infants were randomised within "blocks of six with two assignments per block for all three of the groups". In theory, this form of block randomisation would be expected to generate roughly equal numbers of participants in each of the three study arms. However, the report indicates unequal distribution of infants. The principal investigator has provided further information (post hoc withdrawal of a fourth arm and change in the sequence generation and allocation methods) that may have contributed to this discrepancy. Given the potential for this to have disrupted the integrity of the randomisation process, it may be most appropriate to interpret and apply the findings of this trial with caution.
Potential biases in the review process
The main concern with the review process is the possibility that the findings are subject to publication and other reporting biases. We attempted to minimise this threat by screening the reference lists of included trials and related reviews and searching the proceedings of the major international perinatal conferences to identify trial reports that are not (or not yet) published in full form in academic journals. The meta‐analyses that we performed did not contain sufficient trials to explore symmetry of funnel plots as a means of identifying possible publication or reporting bias.
We have not been able to obtain data from two trials for inclusion in meta‐analyses. Darmstadt 2004 did not report the number of infants in each group who acquired an infection (only the total number of infections which includes multiple infections in individual infants) or all‐cause mortality (only infection‐attributed mortality). These data have not yet been available from the investigators. Another trial has been completed but has yet to report methodological details and numerical data (Hu 2014). When available, we will include these data in an updated version of this review.
Authors' conclusions
Implications for practice.
Prophylactic topical application of emollient ointment, particularly for very preterm infants in high‐income countries, has not been shown to reduce the risk of infection or its associated morbidity or mortality, and may increase the risk of infection with coagulase‐negative staphylococci.
In low‐ and middle‐income countries, the available data do not provide strong evidence that topical emollients (either proprietary ointments or low cost vegetable oils) prevent infection or reduce mortality. Some evidence exists that massage with vegetable oil results in higher rates of weight gain and linear growth but the effect on long‐term growth and development is unknown.
Implications for research.
Given the potential for this simple, low‐cost, and readily available intervention to reduce the huge burden of infectious morbidity and mortality in preterm infants, particularly in low‐ and middle‐income countries, further pragmatic randomised controlled trials are justified in order to improve the precision of the estimates of effect sizes.
What's new
| Date | Event | Description |
|---|---|---|
| 27 January 2016 | New citation required and conclusions have changed | Conclusions changed |
| 30 November 2015 | Amended | Expanded and revised protocol and review, with pre‐specified analyses of trials conducted in low‐ and middle‐income versus high‐income countries. |
History
Protocol first published: Issue 3, 1998 Review first published: Issue 3, 1998
| Date | Event | Description |
|---|---|---|
| 24 July 2003 | New search has been performed | This review updates the previously published review titled "Emollient ointment for preventing infection in preterm infants", The Cochrane Library, Issue 3, 1998 (Soll 1998). The updated review includes data from two additional randomized trials (Pabst 1999, Edwards 2001). Additional outcomes are noted including fungal infection, patent ductus arteriosus, bronchopulmonary dysplasia, and chronic lung disease. Results and conclusions have changed with inclusion of two more randomized trials. |
| 24 July 2003 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
We are grateful to Drs Darmstadt, Martinez, Soll, Sankaranarayanan, and Kumar, the principal investigators of the included trials, for providing unpublished data for inclusion in this systematic review.
We thank Newton Opiyo and Toby Lasserson of the Cochrane Central Editorial Unit for editorial advice and guidance.
Data and analyses
Comparison 1. Topical ointment or cream versus routine skin care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Invasive infection (any organism) | 8 | 2086 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.13 [0.97, 1.31] |
| 1.1 Low or middle income | 2 | 535 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.65, 1.28] |
| 1.2 High income | 6 | 1551 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [1.01, 1.42] |
| 2 Invasive infection (trials with only very preterm infants participating) | 2 | 1210 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [1.04, 1.50] |
| 3 Invasive infection (coagulase negative staphylococci) | 6 | 1839 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.30 [1.03, 1.65] |
| 3.1 Low or middle income | 2 | 535 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.26 [0.71, 2.22] |
| 3.2 High income | 4 | 1304 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.31 [1.02, 1.70] |
| 4 Invasive infection (other bacteria) | 6 | 1839 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.84 [0.63, 1.12] |
| 4.1 Low or middle income | 2 | 535 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.74 [0.46, 1.18] |
| 4.2 High income | 4 | 1304 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.63, 1.29] |
| 5 Invasive infection (fungi) | 6 | 1839 | Risk Difference (M‐H, Fixed, 95% CI) | 0.01 [‐0.01, 0.03] |
| 5.1 Low or middle income | 2 | 535 | Risk Difference (M‐H, Fixed, 95% CI) | 0.01 [‐0.01, 0.03] |
| 5.2 High income | 4 | 1304 | Risk Difference (M‐H, Fixed, 95% CI) | 0.01 [‐0.01, 0.03] |
| 6 Mortality | 7 | 2067 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.75, 1.03] |
| 6.1 Low or middle income | 2 | 535 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.69, 0.98] |
| 6.2 High income | 5 | 1532 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.71, 1.31] |
| 7 Mortality (trials with only very preterm infants participating) | 1 | 1191 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.65, 1.23] |
| 8 BPD | 2 | 1009 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.88, 1.14] |
| 9 NEC | 4 | 1472 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.89, 1.76] |
| 10 ROP (severe) | 1 | 952 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.77, 1.28] |
1.1. Analysis.
Comparison 1 Topical ointment or cream versus routine skin care, Outcome 1 Invasive infection (any organism).
1.2. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 2 Invasive infection (trials with only very preterm infants participating).
1.3. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 3 Invasive infection (coagulase negative staphylococci).
1.4. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 4 Invasive infection (other bacteria).
1.5. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 5 Invasive infection (fungi).
1.6. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 6 Mortality.
1.7. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 7 Mortality (trials with only very preterm infants participating).
1.8. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 8 BPD.
1.9. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 9 NEC.
1.10. Analysis.

Comparison 1 Topical ointment or cream versus routine skin care, Outcome 10 ROP (severe).
Comparison 2. Topical oil versus routine skin care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Invasive infection (any organism) | 6 | 844 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.51, 1.01] |
| 1.1 Low or middle income | 5 | 822 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.51, 1.01] |
| 1.2 High income | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Invasive infection (coagulase negative staphylococci) | 5 | 775 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.15 [0.02, 1.16] |
| 2.1 Low or middle income | 4 | 753 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.15 [0.02, 1.16] |
| 2.2 High income | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Invasive infection (other bacteria) | 5 | 775 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.47, 1.05] |
| 3.1 Low or middle income | 4 | 753 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.47, 1.05] |
| 3.2 High income | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Invasive infection (fungi) | 5 | 775 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.93 [0.42, 8.78] |
| 4.1 Low or middle income | 4 | 753 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.93 [0.42, 8.78] |
| 4.2 High income | 1 | 22 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Mortality | 9 | 1002 | Risk Ratio (IV, Fixed, 95% CI) | 0.94 [0.81, 1.08] |
| 5.1 Low or middle income | 7 | 931 | Risk Ratio (IV, Fixed, 95% CI) | 0.94 [0.81, 1.08] |
| 5.2 High income | 2 | 71 | Risk Ratio (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Growth | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Rate of weight gain (g/kg/day) | 6 | 379 | Mean Difference (IV, Fixed, 95% CI) | 2.55 [1.76, 3.34] |
| 6.2 Change in crown‐heel length (mm/week) | 5 | 320 | Mean Difference (IV, Fixed, 95% CI) | 1.22 [1.01, 1.44] |
| 6.3 Change in head circumference (mm/week) | 5 | 320 | Mean Difference (IV, Fixed, 95% CI) | 0.45 [0.19, 0.70] |
| 6.4 Change in triceps skinfold thickness (mm/week) | 2 | 99 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.00, 0.05] |
2.1. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 1 Invasive infection (any organism).
2.2. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 2 Invasive infection (coagulase negative staphylococci).
2.3. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 3 Invasive infection (other bacteria).
2.4. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 4 Invasive infection (fungi).
2.5. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 5 Mortality.
2.6. Analysis.

Comparison 2 Topical oil versus routine skin care, Outcome 6 Growth.
Comparison 3. Topical ointment or cream vs. topical oil.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Invasive infection (any organism) | 1 | 316 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.57, 1.46] |
| 2 Invasive infection (coagulase negative staphylococci) | 1 | 316 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Invasive infection (other bacteria) | 1 | 316 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.53, 1.50] |
| 4 Invasive infection (fungi) | 1 | 316 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.31, 5.94] |
| 5 Mortality | 1 | 316 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.68, 0.98] |
3.1. Analysis.

Comparison 3 Topical ointment or cream vs. topical oil., Outcome 1 Invasive infection (any organism).
3.2. Analysis.

Comparison 3 Topical ointment or cream vs. topical oil., Outcome 2 Invasive infection (coagulase negative staphylococci).
3.3. Analysis.

Comparison 3 Topical ointment or cream vs. topical oil., Outcome 3 Invasive infection (other bacteria).
3.4. Analysis.

Comparison 3 Topical ointment or cream vs. topical oil., Outcome 4 Invasive infection (fungi).
3.5. Analysis.

Comparison 3 Topical ointment or cream vs. topical oil., Outcome 5 Mortality.
Comparison 4. One topical oil (or combination) vs. another oil (or combination).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Invasive infection | 1 | 64 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Mortality | 1 | 64 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Growth | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Rate of weight gain (g/kg/day) | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | 2.0 [0.84, 3.16] |
| 3.2 Change in crown‐heel length (mm/week) | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐0.29, 1.09] |
| 3.3 Change in head circumference (mm/week) | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐0.17, 0.37] |
4.1. Analysis.

Comparison 4 One topical oil (or combination) vs. another oil (or combination), Outcome 1 Invasive infection.
4.2. Analysis.

Comparison 4 One topical oil (or combination) vs. another oil (or combination), Outcome 2 Mortality.
4.3. Analysis.

Comparison 4 One topical oil (or combination) vs. another oil (or combination), Outcome 3 Growth.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Alkharfy 2014.
| Methods | Randomised controlled trial. | |
| Participants | Infants weighing 501 to 1250 grams at birth and with a gestational age of < 33 weeks. | |
| Interventions | 1. Twice‐daily topical therapy of 2 grams/kg pure, preservative‐free topical petroleum jelly until 34 weeks postmenstrual age (N = 35) 2. Standard skin care (N = 39) |
|
| Outcomes | Invasive infection. NEC. BPD. Mortality. |
|
| Notes | Setting: Department of Pediatrics, King Khalid University Hospital, King Saud University, Riyadh, Saudi Arabia (January 2008 to December 2009). Petroleum jelly is a semi‐solid mixture of hydrocarbons. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes kept in closed closet, managed by study co‐ordinator |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up |
Arora 2005.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants of birth weight < 1500 grams, and < 10 days old, who were receiving enteral feeds. | |
| Interventions | 1. Massage with sunflower oil: N = 23 2. Massage without oil: N = 23 3. No massage (or oil): N = 23 Intervention applied for at least 10 days after enrolment. We combined groups 2 and 3 as a single control group for meta‐analyses. |
|
| Outcomes | Growth parameters. Invasive infection. Mortality. | |
| Notes | Setting: Regional Neonatal Unit, Associated Lok Nayak Hospital, New Dehli, India (Mar to Dec 2001). Infection and mortality data courtesy of Professor Kumar. SD for change in length and head circumference imputed from Soriano 2000. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated sequence |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded parents, caregivers, clinicians and investigators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Near‐complete follow‐up assessment |
Darmstadt 2004.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants of gestational age < 34 weeks and postnatal age < 72 hours. Exclusions: Infants considered likely to die within 48 hours, infants with major congenital anomalies, infants requiring major surgery, infants with immunodeficiency. |
|
| Interventions | 1. Cutaneous application of sunflower seed oil to whole body apart from face and head (4 grams/kg/dose): N = 51. Infants received emollient thrice daily for 14 days, then twice daily until 28 days or discharge from hospital. 2. No emollient: N = 52. Control infants received standard skin care for preterm infants, which included minimal to no use of topical emollients. |
|
| Outcomes | Mortality attributed to sepsis (all‐cause mortality not reported or available from investigators). Invasive infection diagnosed more than 2 days after birth: The report did not state the number of infants in each group who had (at least one) episode of invasive infection. We contacted the principal investigator to seek these data but these have not yet been provided. |
|
| Notes | Setting: Kasr El‐Aini NICU, Cairo University (dates not stated but trial likely to have been undertaken during late 1990s or early 2000s). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete outcome assessment |
Darmstadt 2005.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants of gestational age at birth < 33 weeks and aged < 72 hours. Exclusions: Infants considered likely to die within 48 hours, infants with major congenital anomalies, infants requiring major surgery, infants with established skin infections. |
|
| Interventions | Cutaneous massage (whole body apart from face and head) with: 1. Sunflower seed oil: N = 159 2. Aquaphor®: N = 157 3. No emollient (control): N = 181 Infants were massaged thrice daily for 14 days, then twice daily until discharge from hospital. Control infants received standard skin care for preterm infants, which included minimal to no use of topical emollients. |
|
| Outcomes | Invasive infection. Mortality. | |
| Notes | Setting: Special Care Nursery, Dhaka Shishu Hospital, Bangladesh (1998 to 2003). Aquaphor is a water‐free petrolatum‐based ointment manufactured by Beiersdorf. The report states that infants were randomised within "blocks of six with two assignments per block for all three of the groups". However, this process appears to be inconsistent with the allocated distribution of infants: 1. sunflower seed oil (N = 159), or 2. Aquaphor (N = 157), or 3. no emollient (control) (N = 181). The principal investigator of the trial has explained that this inconsistency may be due to two possible factors: 1. The trial originally had a fourth arm (emollient therapy with safflower oil) which was deemed unacceptable to parents and caregivers and removed from the trial when 24 infants had been randomised to the arms. These infants were not included in the final analyses. 2. The allocation sequence generation method was changed from the original manual process (selecting from a block of six envelopes) to a computer‐generated sequence that did not maintain the balance of assignments within blocks. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Manual generation of blocks of six with two assignments per block for all three of the groups, then computer‐generated sequence |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded parents, caregivers, clinicians and investigators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Near‐complete follow‐up assessment |
Edwards 2004.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants, < 31 weeks gestation and birth weight 501 to 1000 grams, aged < 48 hours without evidence of skin disease and expected to survive beyond 48 hours. | |
| Interventions | 1. Prophylactic application of preservative free ointment (Aquaphor®, Beiersdorf Inc.) twice daily for 14 days: N = 602 2. Routine skin care: N = 589 (could include local application of Aquaphor to area of dermatitis if required) |
|
| Outcomes | Invasive infection
Mortality BPD NEC ROP |
|
| Notes | 53 centres across Vermont Oxford Network in USA (trial performed during late 1990s to early 2000s). Dr Soll kindly provided data on fungal infections. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Near complete outcome assessment |
Erdemir 2014.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants (< 34 weeks) and < 24 hours old. Exclusions: Admitted after 24 hours, major congential abnormalities, infection (skin or systemic). |
|
| Interventions | 1. Aquaphor® once daily to entire body surface except head for 14 days: N = 100 2. Routine skin care without emollient: N = 97 |
|
| Outcomes | Infection Mortality NEC |
|
| Notes | Setting: Tepecik Hospital, Turkey (2010 to 2012). Aquaphor® is a water‐free petrolatum‐based ointment manufactured by Beiersdorf. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not reported |
| Allocation concealment (selection bias) | Low risk | Sealed, opaque envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow‐up |
Fallah 2013.
| Methods | Randomised controlled trial. | |
| Participants | Newborn infants (< 10 days old) of gestational age 33 to 37 weeks, and birth weight 1500 to 1999 grams. Exclusions: multiple pregnancy, birth asphyxia, sepsis, major congenital malformation, small for gestational age. |
|
| Interventions | 1. Massage with sunflower oil, three times daily for 14 days (N = 30) 2. Massage without oil (N = 30) |
|
| Outcomes | Growth parameters Mortaity Infection data sought from investigators (May 2014) |
|
| Notes | Setting: Shahid Saddoughi Hospital, Yazd, Iran (2011). Growth reported as mean (SD) at baseline and one month. We calculated mean change, but had to impute the associated SD for weight gain from Kumar 2013 and SD for change in length and head circumference from Soriano 2000 (similar population, and same timescale of measurement, as per Cochrane Handbook for Systematic Reviews of Interventions 16.1.3.2). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Near‐complete follow up: 5 infants (2 in intervention group, and 3 controls) were lost to follow up (and growth parameter data not available). |
Farhat 2010.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (< 37 weeks) or birth weight < 2000 grams and receiving 150 mL/kg/day of breast milk | |
| Interventions | 1. Daily massage with sunflower oil for 7 days: N = 30 2. Routine skin care (no massage): N = 29 |
|
| Outcomes | Weight change [mean estimated from graph, SD imputed from Kumar 2013] | |
| Notes | Setting: Emamreza Hospital, Mashhad, Iran (2007‐9). Further data on infection and mortality not available from investigators (May 2014). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete assessment of weight change outcome |
Kanti 2014.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (< 48 hours after birth) with birth weight 1500 to 2500 grams | |
| Interventions | 1. Sunflower seed oil daily applied to whole body every 3 to 4 hours for 10 days: N = 11 2. Control (no oil): N = 11 |
|
| Outcomes | Transepidermal water loss, stratum corneum hydration, skin pH and sebum level | |
| Notes | Setting: Department of Neonatology, Charité Universitätsmedizin Berlin, Germany (2009 to 2011). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up assessment |
Kiechl‐Kohlendorfer 2008.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (25 to 36 weeks) admitted to NICU | |
| Interventions | 1. Water‐in‐oil emollient cream (Bepanthen®): N = 57 2. Olive oil cream (70% lanolin, 30% olive oil): N = 58 3. Routine skin care (control group): N = 58 Emolients applied twice daily to body surface except head for 4 weeks |
|
| Outcomes | Invasive infection Mortality |
|
| Notes | Setting: Department of Pediatrics, Innsbruck Medical University, Innsbruck, Austria (2004 to 2006). Bepanthen® is a water‐containing lanolin and petroleum‐based ointment manufactured by Bayer. We combined groups 1 and 2 as a single intervention (ointment) group for meta‐analyses. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. |
| Allocation concealment (selection bias) | Unclear risk | Not described. |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up assessment. |
Kumar 2013.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants of birth weight < 1800 grams and < 35 weeks' gestation, who were receiving ≥ 100 ml/kg/day enteral feeds. Exclusions: Infants receiving supplemental oxygen > 48 hours after birth, infants with major congenital anomalies, intracranial haemorrhage, meningitis or encephalopathy. |
|
| Interventions | 1. Massage with sunflower oil four times daily: N = 27 2. Standard care (no massage): N = 25 Intervention applied for up to 28 days. |
|
| Outcomes | Growth parameters Mortality |
|
| Notes | Setting: Neonatal Intensive Care Unit (NICU), LLRM Medical College, Meerut, India (2009 to 2010). Cross‐over contamination was limited by "segregating the two groups in separate NICU rooms". SD for change in length and head circumference imputed from Soriano 2000. We contacted the principal investigator to seek data on invasive infection (May 2014). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Low risk | Opaque, sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Near‐complete growth data assessment (3 randomised infants not included because of protocol violation or loss to follow up) |
Lane 1993.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (gestational age 29 to 36 weeks), aged < 24 hours. | |
| Interventions | 1. Prophylactic application of water‐in‐oil emollient (Eucerin Creme®, Beiersdorf, Inc) twice daily for 16 days: N = 17 2. No emollient (standard skin care): N = 17 | |
| Outcomes | Invasive infection. Mortality (no deaths). |
|
| Notes | Setting: Departments of Dermatology and Pediatrics, Stanford University, California, early 1990s (single centre). Clarification of methods and outcomes courtesy of Professor Alfred Lane (May 2014). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comlete follow up |
Nopper 1996.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (gestational age < 33 weeks), aged < 96 hours, without evidence of skin disease. | |
| Interventions | 1. Prophylactic application of preservative‐free ointment (Aquaphor®, Beiersdorf, Inc.) applied twice daily for 14 days: N = 30 2. Standard skin care (which could include a water‐in‐oil emollient if required (Eucerin®, Beiersdorf, Inc.): N = 30 | |
| Outcomes | Invasive infection Mortality Weight change Time to regain birth weight |
|
| Notes | Setting: Departments of Dermatology and Pediatrics, Stanford University, California, early‐mid 1990s (single centre). Clarification of methods and outcomes courtesy of Professor Alfred Lane (May 2014). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | High risk |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up |
Pabst 1999.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (gestational age 26 to 30 weeks), aged < 24 hours. | |
| Interventions | 1. Prophylactic application of preservative‐free ointment (Aquaphor Ointment, Beiersdorf, Inc.) applied twice daily for 14 days: N = 11 2. Standard skin care (no emollients): N = 8 | |
| Outcomes | Weight change. Invasive infection. [Mortality not reported] |
|
| Notes | Setting: Department of Pediatrics, University of Maryland, Baltimore, US (mid‐1990s). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete outcome assessment |
Salam 2015.
| Methods | Randomised controlled trial | |
| Participants | Hospital‐born preterm infants (gestational age > 26 weeks). | |
| Interventions | 1. Coconut oil massage twice daily: N = 128 2. Routine skin care: N = 130 Twice daily topical application of coconut oil by nurses from birth until discharge and continued thereafter by mothers at home until completion of the 28th day of life. |
|
| Outcomes | Invasive infection. Neonatal mortality. |
|
| Notes | Setting: Nursery and neonatal intensive care unit at Aga Khan University Hospital, Pakistan. ClinicalTrials.gov Identifier: NCT01396642 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Low risk | Staff "blinded to randomisation" |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up assessment |
Sankaranarayanan 2005.
| Methods | Randomised controlled trial. | |
| Participants | Appropriate for gestational age preterm infants with birth weight 1500 to 2000 grams. | |
| Interventions | 1. Coconut oil massage: N = 38 2. Mineral oil massage: N = 37 3. Massage with baby powder: N = 37 Intervention applied from day 2 until day 31 after birth (4 times daily for 5 minutes). |
|
| Outcomes | Growth parameters. | |
| Notes | Setting: Department of Neonatology, LTM Medical College and General Hospital, Mumbai, India. Infection and mortality data courtesy of Dr Sankaranarayanan. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Low risk | Sealed opaque envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete follow up assessment |
Soriano 2000.
| Methods | Randomised controlled trial. | |
| Participants | Preterm infants (gestational age 28 to 34 weeks and birth weight < 1700 grams). Infants were fully enterally fed before entering the trial. Exclusions: Infants receiving supplemental oxygen, ventilation, inotropic agents, corticosteroids, and infants with congenital anomalies. |
|
| Interventions | 1. Thrice daily cutaneous application of soybean oil (6 grams/kg/day of linoleic acid) for 30 days: N = 29 2. No cutaneous treatment: N = 31 |
|
| Outcomes | Growth parameters Invasive infection Mortality | |
| Notes | Setting: Newborn Nursery, Hospital das Clinicas de Ribeirao Preto, Sao Paulo, Brazil (1992 to 1993). Further data courtesy of Dr Francisco Martinez. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete outcome assessment |
Vaivre‐Douret 2008.
| Methods | Randomised controlled trial | |
| Participants | Preterm infants (31 to 34 weeks). Exclusions: Mechanical ventilation or supplemental oxygen requirement, maternal drug misuse, congenital abnormalities. |
|
| Interventions | 1. Almond oil or vegetable oil massage twice daily for ten days: N = 24 2. Saline massage or no intervention (routine care): N = 25 |
|
| Outcomes | Growth (weight and length percentage change) reported but data suitable for inclusion in meta‐analyses not available. Mortality (no deaths). Infection not reported and data not available from investigators. |
|
| Notes | Setting: Tertiary Neonatal Unit, Poitou‐Charentes, France (2002 to 2004). We have sought but have not received further clarification and data from the investigators (May 2014). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number tables. |
| Allocation concealment (selection bias) | High risk | Clinician allocation (likely to have been aware) |
| Blinding (performance bias and detection bias) All outcomes | High risk | Unblinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete growth parameters data reported |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abdallah 2013 | Quasi‐experimental design (not a randomised controlled trial or quasi‐randomised controlled trial). First cohort recruited were the control, then the subsequent cohort of infants were the intervention group. Olive oil‐based massage versus no massage. |
| Ang 2012 | No emollient in intervention |
| Beeram 2006 | Retrospective case control study of infants < 27 weeks gestation treated with topical Aquaphor, with birthweight and gestational age‐matched infants. |
| Berger 2009 | Duplicate. Article reporting same research as Kiehl‐Kohlendorfer 2008 |
| Brandon 2010 | No Sting (not an emollient) versus emollient. No routine care as control. |
| Brice 1981 | Quasi random, comparison of paraffin mixture and thermal blankets. |
| Campbell 2000 | Case control study using historical controls to evaluate risk factors associated with systemic candidiasis. Topical ointment application of white petrolatum was used for skin care during this study period. |
| Diego 2008 | No emollient in intervention |
| Ferber 2005 | No emollient in intervention. |
| Fernandez 1987 | Prospective case‐control study of preterm infants to assess the effectiveness of corn oil on fasting serum triglyceride levels and need for incubator to maintain normal core body temperature. |
| Fernandez 2005 | Not a randomised controlled trial. |
| Guzzetta 2011 | No emollient in intervention |
| Jansi 2008 | Data includes term babies. Data of preterm or low birth weight infants not subgrouped. |
| Mathai 2001 | Quasi‐randomised trial of massage using powder or mineral oil. These were removed from skin using a cotton bud 15 minutes after massage. |
| Mendes 2008 | No emollient in intervention. |
| Rutter 1981 | Non‐random, before‐and‐after evaluation of topical application of paraffin mixture. |
| Smith 2013 | No emollient in intervention. |
| Solanki 2005a | Randomised controlled trial. Safflower oil versus coconut oil versus no oil. Measured effect on fatty acid profiles and triglyceride levels in blood. No data on outcome measures of interest. |
| Wananukul 2001 | Infants as own controls, comparison of topical application of liquid paraffin 1:1 mixture to one side of the body with no application to the other side. Outcome measure was transepidermal water loss. |
| Wananukul 2002 | Effect of liquid paraffin emollient on trans‐epidermal water loss and ambient skin temperature. Outcomes measured for 5 hours only. |
Characteristics of studies awaiting assessment [ordered by study ID]
Hu 2014.
| Methods | Randomised controlled trial |
| Participants | 428 preterm infant < 34 weeks' gestational age and < 72 hours old were considered eligible for the study during September 2010 to June 2012 |
| Interventions | Infants were randomly assigned to sunflower seed oil group (153 cases) or Johnson oil group (140 cases) or control group (135 cases) |
| Outcomes | Skin condition Infection |
| Notes |
Nangia 2015.
| Methods | Randomised controlled trial |
| Participants | Very low birth weight neonates |
| Interventions | Twice‐daily coconut oil topical application without massage for seven days Control group received standard skin care. |
| Outcomes | Trans‐epidermal water loss by seven days Microbial skin colonisation at seven days |
| Notes |
Characteristics of ongoing studies [ordered by study ID]
Mullany 2010.
| Trial name or title | Impact of Sunflower Seed Oil Massage on Neonatal Mortality and Morbidity in Nepal (NOMS) |
| Methods | Randomised controlled trial (community‐based) |
| Participants | Newborn infants (N = 10,000): likely proportion of preterm infants (or whether and how preterm infants will be identified as a subgroup) is not stated |
| Interventions | Locally manufactured refined sunflower seed oil provided to pregnant women late in pregnancy. Community workers promote its daily use during massage of newborns during the first month of life. Locally manufactured mustard seed oil provided to pregnant women late in pregnancy. Community workers promote its daily use during massage of newborns during the first month of life. |
| Outcomes | All‐cause neonatal mortality |
| Starting date | November 2010 |
| Contact information | Luke C Mullany, Johns Hopkins Bloomberg School of Public Health, USA |
| Notes | ClinicalTrials.gov identifier: NCT01177111 |
Differences between protocol and review
Expanded and revised protocol and review, with pre‐specified analyses of trials conducted in low‐ and middle‐income versus high‐income countries. We planned sensitivity analyses to determine if the findings are affected by including only studies of adequate methodology (low risk of bias), defined as adequate randomisation and allocation concealment, blinding of intervention and measurement, and less than 10% loss to follow‐up.
Contributions of authors
Jemma Cleminson and William McGuire updated the search strategy, appraised the identified literature, extracted data from included studies and drafted the revised review.
Sources of support
Internal sources
Hull York Medical Schoo and Centre for Reviews and Dissemination, University of York, UK.
External sources
-
National Institute of Health Research (NIHR), UK.
This report is independent research funded by a UK NIHR Cochrane Programme Grant (13/89/12). The views expressed in this publication are those of the authors and not necessarily those of the NHS, the NIHR, or the UK Department of Health.
-
Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA.
Editorial support of the Cochrane Neonatal Review Group has been funded with Federal funds from the Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA, under Contract No. HHSN275201100016C
Declarations of interest
None.
Edited (conclusions changed)
References
References to studies included in this review
Alkharfy 2014 {published data only}
- AlKharfy T, Ba‐Abbad R, Hadi A, Alfaleh K. Use of topical petroleum jelly for prevention of sepsis in very low‐birthweight infants: a prospective, randomised controlled trial. Paediatrics and International Child Health 2014;34(3):194‐7. [PUBMED: 24593664] [DOI] [PubMed] [Google Scholar]
Arora 2005 {published data only}
- Arora J, Kumar A, Ramji S. Effect of oil massage on growth and neurobehavior in very low birth weight preterm neonates. Indian Pediatrics 2005;42(11):1092‐100. [PUBMED: 16340050] [PubMed] [Google Scholar]
Darmstadt 2004 {published data only}
- Darmstadt GL, Badrawi N, Law PA, Ahmed S, Bashir M, Iskander I, et al. Topically applied sunflower seed oil prevents invasive bacterial infections in preterm infants in Egypt: a randomized, controlled clinical trial. Pediatric Infectious Disease Journal 2004;23(8):719‐25. [PUBMED: 15295221] [DOI] [PubMed] [Google Scholar]
- Darmstadt GL, Mao‐Q. Topical therapy to improve epidermal barrier function and prevent infections in preterm infants in developing countries. Pediatric Research 2003;53:316A. [Google Scholar]
Darmstadt 2005 {published data only}
- Ahmed AS, Saha SK, Chowdhury MA, Law PA, Black RE, Santosham M, et al. Acceptability of massage with skin barrier‐enhancing emollients in young neonates in Bangladesh. Journal of Health, Population, and Nutrition 2007;25(2):236‐40. [PUBMED: 17985826] [PMC free article] [PubMed] [Google Scholar]
- Darmstadt GL, Ahmed S, Ahmed AN, Saha SK. Mechanism for prevention of infection In preterm neonates by topical emollients: a randomized, controlled clinical trial. Pediatric Infectious Disease Journal 2014;33(11):1124‐7. [PUBMED: 24853544] [DOI] [PubMed] [Google Scholar]
- Darmstadt GL, Saha SK, Ahmed AS, Choi Y, Chowdhury MA, Islam M, et al. Effect of topical emollient treatment of preterm neonates in Bangladesh on invasion of pathogens into the bloodstream. Pediatric Research 2007;61(5 Pt 1):588‐93. [PUBMED: 17413870] [DOI] [PubMed] [Google Scholar]
- Darmstadt GL, Saha SK, Ahmed AS, Chowdhury MA, Law PA, Ahmed S, et al. Effect of topical treatment with skin barrier‐enhancing emollients on nosocomial infections in preterm infants in Bangladesh: a randomised controlled trial. Lancet 2005;365(9464):1039‐45. [PUBMED: 15781099] [DOI] [PubMed] [Google Scholar]
Edwards 2004 {published data only}
- Edwards WH, Conner JM, Soll RF. The effect of Aquaphor Original Emollient Ointment on nosocomial sepsis rates and skin integrity in infants of birth weight 501 to 1000 grams. Pediatric Research 2001;49:388A. [DOI] [PubMed] [Google Scholar]
- Edwards WH, Conner JM, Soll RF, Vermont Oxford Network Neonatal Skin Care Study Group. The effect of prophylactic ointment therapy on nosocomial sepsis rates and skin integrity in infants with birth weights of 501 to 1000 g. Pediatrics 2004;113(5):1195‐203. [PUBMED: 15121929] [DOI] [PubMed] [Google Scholar]
Erdemir 2014 {published data only}
- Erdemir A, Kahramaner Z, Yuksel Y, Cosar H, Turkoglu E, Sutcuoglu S, et al. The effect of topical ointment on neonatal sepsis In preterm infants. The Journal of Maternal‐Fetal & Neonatal Medicine 2014;28(1):33‐6. [PUBMED: 24588277] [DOI] [PubMed] [Google Scholar]
Fallah 2013 {published data only}
- Fallah R, Akhavan Karbasi S, Golestan M, Fromandi M. Sunflower oil versus no oil moderate pressure massage leads to greater increases in weight in preterm neonates who are low birth weight. Early Human Development 2013;89(9):769‐72. [PUBMED: 23830725] [DOI] [PubMed] [Google Scholar]
Farhat 2010 {published data only}
- Farhat AS, Mohammadzadeh A, Amiri R, Amiri M. Effect of dermal sunflower oil on growth of low birth weight preterm infants. XXII European Congress of Perinatal Medicine; Granada, Spain; 2010 May 26‐29. Granada, 2010.
Kanti 2014 {published data only}
- Kanti V, Grande C, Stroux A, Buhrer C, Blume‐Peytavi U, Garcia Bartels N. Influence of sunflower seed oil on the skin barrier function of preterm infants: a randomized controlled trial. Dermatology 2014;229(3):230‐9. [PUBMED: 25323538] [DOI] [PubMed] [Google Scholar]
Kiechl‐Kohlendorfer 2008 {published data only}
- Kiechl‐Kohlendorfer U, Berger C, Inzinger R. The effect of daily treatment with an olive oil/lanolin emollient on skin integrity in preterm infants: a randomized controlled trial. Pediatric Dermatology 2008;25(2):174‐8. [PUBMED: 18429773] [DOI] [PubMed] [Google Scholar]
Kumar 2013 {published data only}
- Kumar J, Upadhyay A, Dwivedi AK, Gothwal S, Jaiswal V, Aggarwal S. Effect of oil massage on growth in preterm neonates less than 1800 g: A randomized control trial. Indian Journal of Pediatrics 2013;80(6):465‐9. [PUBMED: 23054851] [DOI] [PubMed] [Google Scholar]
Lane 1993 {published data only}
- Lane AT, Drost SS. Effects of repeated application of emollient cream to premature neonates' skin. Pediatrics 1993;92(3):415‐9. [PUBMED: 8361795] [PubMed] [Google Scholar]
Nopper 1996 {published data only}
- Nopper AJ, Horii KA, Sookdeo‐Drost S, Wang TH, Mancini AJ, Lane AT. Topical ointment therapy benefits premature infants. Journal of Pediatrics 1996;128(5 Pt 1):660‐9. [PUBMED: 8627439] [DOI] [PubMed] [Google Scholar]
Pabst 1999 {published data only}
- Pabst RC, Starr KP, Qaiyumi S, Schwalbe RS, Gewolb IH. The effect of application of aquaphor on skin condition, fluid requirements, and bacterial colonization in very low birth weight infants. Journal of Perinatology 1999;19(4):278‐83. [PUBMED: 10685239] [DOI] [PubMed] [Google Scholar]
Salam 2015 {published data only}
- Salam RA, Darmstadt GL, Bhutta ZA. Effect of emollient therapy on clinical outcomes in preterm neonates in Pakistan: a randomised controlled trial. Archives of Disease in Childhood. Fetal and Neonatal Edition 2015;100(3):F210‐5. [PUBMED: 25637007] [DOI] [PubMed] [Google Scholar]
- Salam RA, Das JK, Darmstadt GL, Bhutta ZA. Emollient therapy for preterm newborn infants ‐ evidence from the developing world. BMC Public Health 2013;13 Suppl 3:S31. [PUBMED: 24564550] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sankaranarayanan 2005 {published data only}
- Sankaranarayanan K, Mondkar JA, Chauhan MM, Mascarenhas BM, Mainkar AR, Salvi RY. Oil massage in neonates: an open randomized controlled study of coconut versus mineral oil. Indian Pediatrics 2005;42(9):877‐84. [PUBMED: 16208048] [PubMed] [Google Scholar]
Soriano 2000 {published data only}
- Soriano CR, Martinez FE, Jorge SM. Cutaneous application of vegetable oil as a coadjutant in the nutritional management of preterm infants. Journal of Pediatric Gastroenterology and Nutrition 2000;31(4):387‐90. [PUBMED: 11045835] [DOI] [PubMed] [Google Scholar]
Vaivre‐Douret 2008 {published data only}
- Vaivre‐Douret L, Oriot D, Blossier P, Py A, Kasolter‐Pere M, Zwang J. The effect of multimodal stimulation and cutaneous application of vegetable oils on neonatal development in preterm infants: a randomized controlled trial. Child: Care, Health and Development 2009;35(1):96‐105. [PUBMED: 18991972] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Abdallah 2013 {published data only}
- Abdallah B, Badr LK, Hawwari M. The efficacy of massage on short and long term outcomes in preterm infants. Infant Behavior & Development 2013;36(4):662‐9. [PUBMED: 23932956] [DOI] [PubMed] [Google Scholar]
Ang 2012 {published data only}
- Ang JY, Lua JL, Mathur A, Thomas R, Asmar BI, Savasan S, et al. A randomized placebo‐controlled trial of massage therapy on the immune system of preterm infants. Pediatrics 2012;130(6):e1549‐58. [PUBMED: 23147978] [DOI] [PMC free article] [PubMed] [Google Scholar]
Beeram 2006 {published data only}
- Beeram M, Olvera R, Krauss D, Loughran C, Petty M. Effects of topical emollient therapy on infants at or less than 27 weeks' gestation. Journal of the National Medical Association 2006;98(2):261‐4. [PUBMED: 16708512] [PMC free article] [PubMed] [Google Scholar]
Berger 2009 {published data only}
- Berger C, Inzinger R. Study of skin care in premature and newborn infants [Studie zur Hautpflege bei Fruh‐ und Neugeborenen.]. Kinderkrankenschwester : Organ der Sektion Kinderkrankenpflege / Deutsche Gesellschaft fur Sozialpadiatrie und Deutsche Gesellschaft fur Kinderheilkunde 2009;28(3):116‐25. [PUBMED: 19382435] [PubMed] [Google Scholar]
Brandon 2010 {published data only}
- Brandon DH, Coe K, Hudson‐Barr D, Oliver T, Landerman LR. Effectiveness of No‐Sting skin protectant and Aquaphor on water loss and skin integrity in premature infants. Journal of Perinatology 2010;30(6):414‐9. [PUBMED: 19890343] [DOI] [PubMed] [Google Scholar]
Brice 1981 {published data only}
- Brice JEH, Rutter N, Hull D. Reduction of skin water loss in the newborn. II. Clinical trial of two methods in very low birthweight babies. Archives of Disease in Childhood 1981;56(9):673‐5. [PUBMED: 7294869] [DOI] [PMC free article] [PubMed] [Google Scholar]
Campbell 2000 {published data only}
- Campbell JR, Zaccaria, E, Baker CJ. Systemic candidiasis in extremely low birth weight infants receiving topical petrolatum ointment for skin care: a case‐control study. Pediatrics 2000;105(5):1041‐5. [PUBMED: 10790460] [DOI] [PubMed] [Google Scholar]
Diego 2008 {published data only}
- Diego MA, Field T, Hernandez‐Reif M. Temperature increases in preterm infants during massage therapy. Infant Behavior & Development 2008;31(1):149‐52. [PUBMED: 17692385] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ferber 2005 {published data only}
- Ferber SG, Feldman R, Kohelet D, Kuint J, Dollberg S, Arbel E, et al. Massage therapy facilitates mother‐infant interaction in premature infants. Infant Behavior & Development 2005;28(1):74‐81. [Google Scholar]
Fernandez 1987 {published data only}
- Fernandez A, Patkar S, Chawla C, Taskar T, Prabhu SV. Oil application in preterm babies‐‐a source of warmth and nutrition. Indian Pediatrics 1987;24(12):1111‐6. [PUBMED: 3450663] [PubMed] [Google Scholar]
Fernandez 2005 {published data only}
- Fernandez AR, Krishnamoorthy G, Patil N, Mondkar JA, Swar BD. Transcutaneous absorption of oil in preterm babies‐‐a pilot study. Indian Pediatrics 2005;42(3):255‐8. [PUBMED: 15817974] [PubMed] [Google Scholar]
Guzzetta 2011 {published data only}
- Guzzetta A, D'Acunto MG, Carotenuto M, Berardi N, Bancale A, Biagioni E, et al. The effects of preterm infant massage on brain electrical activity. Developmental Medicine and Child Neurology 2011;53 Suppl 4:46‐51. [PUBMED: 21950394] [DOI] [PubMed] [Google Scholar]
Jansi 2008 {published data only}
- Jansi LB. Effect of oil massage on changes in weight and neurobehavioural response of low birth weight babies. The Nursing Journal of India 2008;99(11):256‐8. [PUBMED: 19323348] [PubMed] [Google Scholar]
Mathai 2001 {published data only}
- Mathai S, Fernandez A, Mondkar J, Kanbur W. Effects of tactile‐kinesthetic stimulation in preterms: a controlled trial. Indian Pediatrics 2001;38(10):1091‐8. [PUBMED: 11677298] [PubMed] [Google Scholar]
Mendes 2008 {published data only}
- Mendes EW, Procianoy RS. Massage therapy reduces hospital stay and occurrence of late‐onset sepsis in very preterm neonates. Journal of Perinatology 2008;28(12):815‐20. [PUBMED: 18633421] [DOI] [PubMed] [Google Scholar]
Rutter 1981 {published data only}
- Rutter N, Hull D. Reduction of skin water loss in the newborn. I. Effect of applying topical agents. Archives of Disease in Childhood 1981;56(9):669‐72. [PUBMED: 7294868] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2013 {published data only}
- Smith SL, Lux R, Haley S, Slater H, Beachy J, Moyer‐Mileur LJ. The effect of massage on heart rate variability in preterm infants. Journal of Perinatology 2013;33(1):59‐64. [PUBMED: 22538325] [DOI] [PMC free article] [PubMed] [Google Scholar]
Solanki 2005a {published data only}
- Solanki K, Matnani M, Kale M, Joshi K, Bavdekar A, Bhave S, et al. Transcutaneous absorption of topically massaged oil in neonates. Indian Pediatrics 2005;42(10):998‐1005. [PUBMED: 16269830] [PubMed] [Google Scholar]
Wananukul 2001 {published data only}
- Wananukul S, Praisuwanna P, Kescorncam K. Effects of clear topical ointment on transepidermal water loss in jaundiced preterm infants receiving phototherapy. Journal of the Medical Association of Thailand 2001;84(6):837‐41. [PUBMED: 11556462] [PubMed] [Google Scholar]
Wananukul 2002 {published data only}
- Wananukul S, Praisuwanna P. Clear topical ointment decreases transepidermal water loss in jaundiced preterm infants receiving phototherapy. Journal of the Medical Association of Thailand 2002;85(1):102‐6. [PUBMED: 12075708] [PubMed] [Google Scholar]
References to studies awaiting assessment
Hu 2014 {published data only}
- Hu X, Zhang Y. Effect of topically applied sunflower seed oil in preterm infants. Pediatric Critical Care Medicine. Conference: 7th World Congress on Pediatric Intensive and Critical Care; 2014 May 4‐7; Istanbul, Turkey. Lippincott Williams and Wilkins, 2014; Vol. 15:144‐5.
Nangia 2015 {published data only}
- Nangia S, Paul VK, Deorari AK, Sreenivas V, Agarwal R, Chawla D. Topical oil application and trans‐epidermal water loss in preterm very low birth weight infants‐ a randomized trial. Journal of Tropical Pediatrics 2015;Sep 3:[Epub ahead of print]. [PUBMED: 26338490] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
Mullany 2010 {published data only}
- Impact of Sunflower Seed Oil Massage on Neonatal Mortality and Morbidity in Nepal (NOMS). Ongoing study November 2010.
Additional references
Adams‐Chapman 2006
- Adams‐Chapman I, Stoll BJ. Neonatal infection and long‐term neurodevelopmental outcome in the preterm infant. Current Opinion in Infectious Diseases 2006;19(3):290‐7. [PUBMED: 16645492] [DOI] [PubMed] [Google Scholar]
Bell 1978
- Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Annals of Surgery 1978;187(1):1‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berrington 2012
- Berrington JE, Hearn RI, Bythell M, Wright C, Embleton ND. Deaths in preterm infants: changing pathology over 2 decades. The Journal of Pediatrics 2012;160:49‐53.e1. [PUBMED: 21868028] [DOI] [PubMed] [Google Scholar]
BNF for Children 2014
- Paediatric Formulary Committee. BNF for Children. London: BMJ Group, Pharmaceutical Press, and RCPCH Publications, 2014. [Google Scholar]
Camacho‐Gonzalez 2013
- Camacho‐Gonzalez A, Spearman PW, Stoll BJ. Neonatal infectious diseases: evaluation of neonatal sepsis. Pediatric Clinics of North America 2013;60(2):367‐89. [PUBMED: 23481106] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cartlidge 2000
- Cartlidge P. The epidermal barrier. Seminars in Neonatology 2000;5(4):273‐80. [PUBMED: 11032710] [DOI] [PubMed] [Google Scholar]
Chiller 2001
- Chiller K, Selkin BA, Murakawa GJ. Skin microflora and bacterial infections of the skin. Journal of Investigative Dermatology 2001;6(3):170‐4. [PUBMED: 11924823] [DOI] [PubMed] [Google Scholar]
Darmstadt 2002a
- Darmstadt GL, Mao‐Qiang M, Chi E, Saha SK, Ziboh VA, Black RE, et al. Impact of topical oils on the skin barrier: possible implications for neonatal health in developing countries. Acta Paediatrica 2002;91(5):546‐54. [PUBMED: 12113324] [DOI] [PubMed] [Google Scholar]
Darmstadt 2002b
- Darmstadt GL, Saha SK. Traditional practice of oil massage of neonates in Bangladesh. Journal of Health, Population, and Nutrition 2002;20(2):184‐8. [PUBMED: 12186200] [PubMed] [Google Scholar]
Dyer 2013
- Dyer JA. Newborn skin care. Seminars in Perinatology 2013;37(1):3‐7. [PUBMED: 23419756] [DOI] [PubMed] [Google Scholar]
Evans 1986
- Evans NJ, Rutter N. Development of the epidermis in the newborn. Biology of the Neonate 1986;49(2):74‐80. [PUBMED: 3697429] [DOI] [PubMed] [Google Scholar]
Gordon 2006
- Gordon A, Isaacs D. Late onset neonatal Gram‐negative bacillary infection in Australia and New Zealand: 1992‐2002. The Pediatric Infectious Disease Journal 2006;25(1):25‐9. [PUBMED: 16395098] [DOI] [PubMed] [Google Scholar]
GRADEpro 2008 [Computer program]
- Brozek J, Oxman A, Schünemann H. GRADEpro [Version 3.2 for Windows]. The GRADE Working Group, 2008.
Guyatt 2011a
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction‐GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [PUBMED: 21195583] [DOI] [PubMed] [Google Scholar]
Guyatt 2011b
- Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso‐Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence‐‐study limitations (risk of bias). Journal of Clinical Epidemiology 2011;64(4):407‐15. [PUBMED: 21247734] [DOI] [PubMed] [Google Scholar]
Guyatt 2011c
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso‐Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence‐‐imprecision. Journal of Clinical Epidemiology 2011;64(12):1283‐93. [PUBMED: 21839614] [DOI] [PubMed] [Google Scholar]
Guyatt 2011d
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidence‐‐inconsistency. Journal of Clinical Epidemiology 2011;64(12):1294‐302. [PUBMED: 21803546] [DOI] [PubMed] [Google Scholar]
Guyatt 2011e
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence‐‐indirectness. Journal of Clinical Epidemiology 2011;64(12):1303‐10. [PUBMED: 21802903] [DOI] [PubMed] [Google Scholar]
Harpin 1983
- Harpin VA, Rutter N. Barrier properties of the newborn infant's skin. Journal of Pediatrics 1983;102(3):419‐25. [PUBMED: 6827416] [DOI] [PubMed] [Google Scholar]
ICCROP 2005
- International Committee for the Classification of Retinopathy of Prematurity. The International Classification of Retinopathy of Prematurity revisited. Archives of Ophthalmology 2005;123(7):991‐9. [DOI] [PubMed] [Google Scholar]
Isaacs 2003
- Isaacs D, Australian Study Group for Neonatal Infections. A ten year, multicentre study of coagulase negative staphylococcal infections in Australasian neonatal units. Archives of Disease in Childhood. Fetal and Neonatal Edition 2003;88(2):F89‐93. [PUBMED: 12598493] [DOI] [PMC free article] [PubMed] [Google Scholar]
Isaacs 2004
- Isaacs D, Fraser S, Hogg G, Li HY. Staphylococcus aureus infections in Australasian neonatal nurseries. Archives of Disease in Childhood. Fetal and Neonatal Edition 2004;89:F331‐5. [PUBMED: 15210669] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lee 1993
- Lee EJ, Gibson RA, Simmer K. Transcutaneous application of oil and prevention of essential fatty acid deficiency in preterm infants. Archives of Disease in Childhood 1993;68(1 Spec No):27‐8. [PUBMED: 8439192] [DOI] [PMC free article] [PubMed] [Google Scholar]
Marchini 2002
- Marchini G, Lindow S, Brismar H, Stabi B, Berggren V, Ulfgren AK, et al. The newborn infant is protected by an innate antimicrobial barrier: peptide antibiotics are present in the skin and vernix caseosa. The British Journal of Dermatology 2002;147(6):1127‐34. [PUBMED: 12452861] [DOI] [PubMed] [Google Scholar]
Mullany 2005
- Mullany LC, Darmstadt GL, Khatry SK, Tielsch JM. Traditional massage of newborns in Nepal: implications for trials of improved practice. Journal of Tropical Paediatrics 2005;51(2):82‐6. [PUBMED: 15677372] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ness 2013
- Ness MJ, Davis DM, Carey WA. Neonatal skin care: a concise review. International Journal of Dermatology 2013;52(1):14‐22. [PUBMED: 23278604] [DOI] [PubMed] [Google Scholar]
Pickens 2000
- Pickens WL, Warner RR, Boissy YL, Boissy RE, Hoath SB. Characterization of vernix caseosa: water content, morphology, and elemental analysis. Journal of Investigative Dermatology 2000;115(5):875‐81. [PUBMED: 11069626] [DOI] [PubMed] [Google Scholar]
Rutter 1988
- Rutter N. The immature skin. British Medical Bulletin 1988;44(4):957‐70. [PUBMED: 3076838] [DOI] [PubMed] [Google Scholar]
Rutter 2000
- Rutter N. Clinical consequences of an immature barrier. Seminars in Neonatology 2000;5(4):281‐7. [PUBMED: 11032711] [DOI] [PubMed] [Google Scholar]
Samanta 2011
- Samanta S, Farrer K, Breathnach A, Heath PT. Risk factors for late onset gram‐negative infections: a case‐control study. Archives of Disease in Childhood. Fetal and Neonatal Edition 2011;96(1):F15‐8. [PUBMED: 20538712] [DOI] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors. GWG. GRADE handbook for grading quality of evidence and strength of recommendations. Available from www.guidelinedevelopment.org/handbook Updated October 2013.
Stoll 2002
- Stoll BJ, Hansen N, Fanaroff AA, Wright LL, Carlo WA, Ehrenkranz RA, et al. Late‐onset sepsis in very low birth weight neonates: the experience of the NICHD Neonatal Research Network. Pediatrics 2002;110(2 Pt 1):285‐91. [PUBMED: 12165580] [DOI] [PubMed] [Google Scholar]
Stoll 2004
- Stoll BJ, Hansen NI, Adams‐Chapman I, Fanaroff AA, Hintz SR, Vohr B, et al. Neurodevelopmental and growth impairment among extremely low‐birth‐weight infants with neonatal infection. JAMA 2004;292(19):2357‐65. [PUBMED: 15547163] [DOI] [PubMed] [Google Scholar]
Vergnano 2011
- Vergnano S, Menson E, Kennea N, Embleton N, Russell AB, Watts T, et al. Neonatal infections in England: the NeonIN surveillance network. Archives of Disease in Childhood. Fetal and Neonatal Edition 2011;96(1):F9‐F14. [PUBMED: 20876594] [DOI] [PubMed] [Google Scholar]
Zaidi 2005
- Zaidi AK, Huskins WC, Thaver D, Bhutta ZA, Abbas Z, Goldmann DA. Hospital‐acquired neonatal infections in developing countries. Lancet 2005;365(9465):1175‐88. [PUBMED: 15794973] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Conner 2008
- Conner JM, Soll R, Edwards WH. Topical ointment for preventing infection in preterm infants. Cochrane Database of Systematic Reviews 2008, Issue 4. [DOI: 10.1002/14651858.CD001150.pub2] [DOI] [PubMed] [Google Scholar]
Edwards 2001
- Edwards WH, Conner JM, Soll RF, et al. The effect of Aquaphor Original Emollient Ointment on nosocomial sepsis rates and skin integrity in infants of birth weight 501 to 1000 grams. Pediatric Research 2001;49:388A. [DOI] [PubMed] [Google Scholar]
Soll 1998
- Soll RF, Edwards WH. Emollient ointment for preventing infection in preterm infants. Cochrane Database of Systematic Reviews 1998, Issue 3. [DOI: 10.1002/14651858.CD001150] [DOI] [PubMed] [Google Scholar]