

ABSTRACT
Purpose
This study determined associations between diet quality measured by the Healthy Eating Index (HEI)-2015, physical performance, and successful selection following a U.S. Army Special Forces Assessment and Selection course characterized by arduous cognitive and physical demands.
Methods
The HEI-2015 scores were calculated from usual diet assessed with a Block food frequency questionnaire among 782 soldiers attending Special Forces Assessment and Selection. Differences in HEI-2015 scores according to demographics and physical performance were determined with analysis of variance. Differences in likelihood of selection according to HEI-2015 scores were determined with logistic regression. Models were adjusted for potential confounders: age, education, body mass index (BMI), duration and type of resistance training, and smoking.
Results
The HEI-2015 total score was higher among older soldiers (≥25 yr), those with more education (≥some college), higher body mass index (≥25), longer duration of resistance training (≥400 min·wk−1), those that reported use of free weights, suspension training, Olympic lifting, and nonsmokers (P < 0.05). The HEI-2015 total score was higher among those with higher Army Physical Fitness Test (APFT) total scores, APFT sit-up score, APFT run score, and faster loaded road march times (P < 0.05). Those with higher HEI-2015 total scores were 75% (quartile 3 vs quartile 1: odds ratio, 1.75; 95% confidence interval, 1.09–2.81) and 65% (quartile 4 vs quartile 1: odds ratio, 1.65, 95% confidence interval, 1.03–2.65) more likely to be selected. Higher scores for total vegetables, greens and beans, seafood and plant protein, and refined grains, but lower sodium scores (indicating more sodium consumed), were associated with better physical performance (P < 0.05).
Conclusions
Dietary patterns that conform to federal dietary guidelines (except sodium) are associated with physical performance and Special Forces selection.
Key Words: MILITARY, HEALTHY EATING INDEX, EXERCISE, SODIUM, PROTEIN, FRUITS AND VEGETABLES
Diet and nutrition may optimize physical performance in athletic activities (1). Sports nutrition recommendations on the timing and amount of fluids and macronutrients to optimize performance and recovery are well established (1). However, the relationship between overall diet quality and physical performance remains largely unexplored. The Healthy Eating Index (HEI)-2015 is a measure of diet quality that assesses conformance with the 2015 to 2020 federal Dietary Guidelines for Americans (2,3). Nine of its components assess recommended adequate intakes: total vegetables, greens and beans, total fruit, whole fruit, whole grains, dairy, total protein foods, seafood and plant protein, and fatty acid ratio. Four of its components assess moderation: sodium, refined grains, added sugars, and saturated fats.
Several HEI-2015 individual components are comprised of foods or nutrients associated with measures of physical performance or physical functioning in observational studies, including fruits and vegetables (4,5), protein (6–8), and whole grains (9). Fruits, vegetables, and whole grains may contribute to meeting carbohydrate and antioxidant intake recommendations, whereas animal, seafood, and plant protein may contribute to meeting protein and iron intake recommendations (1). Consuming fewer empty calories is also associated with reduced risk of classification of overweight and obesity in men (10), and body composition is an important factor for physical performance (1,11). Higher total score from the 2005 version of the HEI is associated with faster gait speed and greater knee extensor power among older adults (12), but whether diet quality is associated with measures of physical performance in athletes or younger, physically active populations has not been explored.
Similar to athletes, U.S. military Special Forces personnel must demonstrate their ability to perform particular physical activities assessed by objective criteria. Special Forces Assessment and Selection (SFAS) is an arduous 19- to 20-d assessment course designed to select individuals with attributes for success as an elite U.S. Army Special Forces Soldier, known as a “Green Beret.” Candidate soldiers must complete extensive cognitive and physical challenges during SFAS to be selected to receive the additional training required for qualification as a Special Forces Soldier. In addition to intelligence and aptitude testing, team events, and peer evaluations, the difficult course is well known for its strenuous physical demands which contribute to a high failure rate, as the majority of candidates (>50%) are unable to successfully complete SFAS (13).
Prior reports indicate that candidates who voluntarily withdraw from SFAS often cite insufficient physical fitness as the reason (13). Physical performance is evaluated with several events, including the Army Physical Fitness Test (APFT) (14), pull-ups, multiple timed runs and timed loaded road marches, an obstacle course, and timed land navigation tasks. In addition, dietary intake among candidates during SFAS is restricted to military rations which, to a certain extent, standardizes diet during the course. Since dietary intake during the course is largely controlled, variation in the quality of the usual diet consumed before SFAS may influence candidates’ physical performance by affecting nutritional status during training and recovery, body composition, and contributing to adequate micronutrient and macronutrient status upon arrival at SFAS.
Therefore, SFAS provides a unique opportunity to evaluate associations between diet quality, physical performance, and successful selection among candidates attending the selection course. We hypothesized that higher HEI-2015 scores on entry to SFAS would be associated with better performance on physical events and increased likelihood of being selected after SFAS. Associations between HEI-2015 scores, demographics, and health characteristics were also examined.
METHODS
Participants
Participants were active duty, male, U.S. Army Soldiers, enrolled as candidates in SFAS.
Candidates were recruited for the study from 12 SFAS courses between May 2015 and March 2017 by an informational briefing. Of the 1750 candidates briefed, 821 provided written consent to participate in the study (47%). Seven participants, after not being selected on their first SFAS attempt, enrolled in the study a second time. After excluding data from the first enrollment of the participants that enrolled twice (n = 7), in addition to those that voluntarily withdrew after providing consent (n = 14), and were missing dietary intake (n = 13) or demographic data (n = 5), 782 participants had complete dietary intake, demographic, and selection status data (Fig. 1). The sample size of models assessing physical performance measures varied from 468 to 770, depending on whether the candidate progressed far enough in the course to perform the physical performance event. This research was conducted under a Memorandum of Agreement between the U.S. Army Special Operations Command (USASOC) and the U.S. Army Research Institute of Environmental Medicine (USARIEM). The USARIEM Institutional Review Board approved this study. The investigators adhered to the policies for protection of human subjects as prescribed by Department of Defense Instruction 3216.02, and the research was conducted in adherence with the provisions of 32 CFR Part 219.
FIGURE 1.
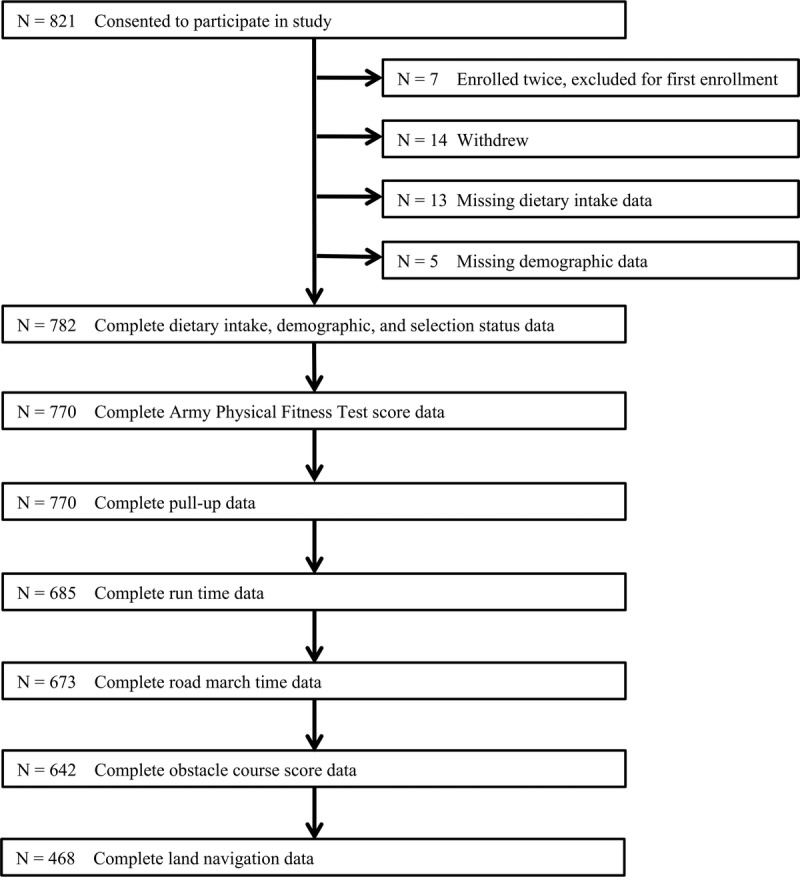
Participant sample size.
Demographics and health characteristics
Information on demographics and health characteristics were obtained before the start of the course. A standardized self-report questionnaire was used to determine age, education, duration of resistance training and aerobic exercise, participation in types of resistance training exercises, cigarette smoking, and smokeless tobacco use. Duration of resistance training and aerobic exercise was calculated by multiplying the midpoint of self-reported exercise duration categories (minutes) by frequency (days per week). Duration categories included 1 to 15 min, 16 to 30 min, 31 to 60 min, 61 to 75 min, 76 to 90 min, 91 to 120 min, or >120 min. Midpoint of the >120-min category was set to 135.5 (midpoint of 121–150). Frequency categories included never, 1, 2, 3, 4, 5, 6, 7 d·wk−1. Multiple daily sessions could also be selected and were recoded as daily frequency (7 d·wk−1). Participants were also asked to select categories for types of resistance training activities performed: free weights, machine weights, body weight exercises (such as pull-ups and push-ups), suspension training, Olympic lifting, and high-intensity training. Participants could also write-in activities or resistance training exercise programs not listed. Trademarked or named exercise programs considered high-intensity training were combined with the high-intensity training category, whereas other named exercise programs were grouped as a separate category (other exercise program). U.S. Army John F. Kennedy Special Warfare Center and School (USAJFKSWCS) personnel provided officer/enlisted status designation as 18X enlisted, active duty enlisted, or commissioned officer. Enlisted personnel were categorized as 18X or active duty because they were derived from either the active duty population or the 18X enlistment option. The 18X enlistment option is a direct enlistment option which provides recruits the opportunity to attend SFAS after their initial Basic Combat Training and Airborne training. By contrast, enlisted personnel attending SFAS that are derived from the active duty population first serve initial duty in the U.S. Army before attending SFAS. Body mass index (BMI) was calculated from body mass measured in kilograms with a calibrated electronic scale (Befour, Staukville, WI) and vertical height measured in centimeters with stadiometer (Hopkins Medical Products, Caledonia, MI).
Diet quality
Usual dietary intake over the previous year was assessed with a 127-item 2014 Block food frequency questionnaire (NutritionQuest, Berkeley, CA) (15,16). Daily consumption of foods and total energy intake derived from the frequency and quantity of food items reported on the FFQ were used to calculate HEI-2015 scores. The HEI-2015 scores were calculated according to minimum and maximum score standards, described in detail elsewhere (2,3,17). Briefly, the nine components that assess compliance with adequate intakes have maximum scores ranging from 5 to 10 that correspond to the following standards: ≥1.1 cup equivalents per 1000 kcal for total vegetables, ≥0.2 cup equivalents per 1000 kcal for greens and beans, ≥0.8 cup equivalents per 1000 kcal for total fruit, ≥0.4 cup equivalents per 1000 kcal for whole fruit, ≥1.5 oz equivalents per 1000 kcal for whole grains, 1.3 cup equivalents per 1000 kcal for dairy, ≥2.5 oz equivalents per 1000 kcal for total protein foods, ≥0.8 oz equivalents per 1000 kcal for seafood and plant protein, and (polyunsaturated fatty acids + monounsaturated fatty acids)/saturated fatty acids ≥2.5 for fatty acid ratio. The minimum score of zero corresponds to a standard of no intake of foods in aforementioned components, or a ratio of ≤1.2 for the fatty acid ratio component. The four components that assess compliance with moderation each have a maximum score of 10 that corresponds to the following standards: ≤1.1 g per 1000 kcal for sodium, ≤1.8 oz equivalents per 1000 kcal for refined grains, ≤6.5% of energy for added sugars, and ≤8% of energy for saturated fats. The minimum score of zero corresponds to ≥2.0 g per 1000 kcal for sodium, ≥4.3 oz equivalents per 1000 kcal for refined grains, ≥26% of energy for added sugars, and ≥16% of energy for saturated fats. The total HEI-2015 score ranges from 0 to 100 and is calculated from the sum of individual component scores, with higher scores indicating greater compliance with federal guidelines (17).
Physical performance and selection outcome
Candidates performed several physical events as routine requirements during SFAS, including the APFT, pull-ups, timed runs, timed loaded road marches, an obstacle course, and land navigation assessment. The APFT is comprised of push-ups, sit-ups, and a 2-mile run, scored from 0 to 100 for each event with a maximum score totaling 300 (14). Scores were calculated from standards for males, age 17 to 21 yr. After the APFT, the number of pull-ups completed was also recorded (14). Candidates performed multiple timed runs and timed loaded road marches over wooded terrain of distances that are not disclosed to candidates (recorded in minutes). Runs and road marches were required to be completed within unknown time limits. To maximize sample size, only the first run and road march times were used in analyses. Candidates completed an obstacle course consisting of approximately 20 obstacles that required climbing ropes and nets, crawling through dark enclosed tunnels, and navigating apparatuses at elevated heights. The obstacle course score was calculated as the sum of the points received for each obstacle successfully completed. Land navigation required the candidates to locate grid coordinates with only a paper map and compass in unfamiliar wooded terrain within time limits. The total number of coordinates successfully located was recorded. After successfully completing physical events and other course procedures, including intelligence and aptitude testing, team challenges, and peer evaluations, a board of USAJFKSWCS personnel made a final determination whether to select a candidate. Candidates’ selection outcome (selected or not selected) was provided by USAJFKSWCS personnel.
Statistical analyses
The SAS statistical software package (version 9.4; SAS Institute, Cary, NC), was used to perform all analyses. Categorized demographics and health characteristic variables were summarized with descriptive statistics (frequencies and percentages). Differences in least square mean HEI-2015 total score according to categorized demographics, health characteristics, physical performance, and selection status variables were determined with analysis of variance using the general linear model procedure in SAS. Differences in the probability (percentage selected) and likelihood of selection (odds ratio [OR] and 95% confidence interval [CI]) according to quartile of HEI-2015 total score were determined with χ2 and logistic regression. In post hoc analyses, differences in least square mean HEI-2015 individual component scores according to categorized total APFT score and road march time were determined with analysis of variance, as these physical performance measures were associated with HEI-2015 total score (P < 0.05). Physical performance and selection status models were adjusted for potential confounders of age, education, BMI, duration of resistance training, use of free weights, suspension training, Olympic lifting, and cigarette smoking, as these variables were independently associated with HEI-2015 total score (Table 1, P < 0.05) and may be associated with the outcomes of interest. The least square means (physical performance models) and odds ratios (selection status models) presented in adjusted models represent the association between HEI-2015 score and physical performance or selection status while holding potential confounders constant (unchanged). All physical performance variables were categorized as quartiles because raw data for physical performance events were not permitted by USAJFKSWCS to be released. To maintain consistency, quartiles of run and road march times were displayed in reverse order since lower quartiles corresponded to faster times and better physical performance. To limit the number of comparisons, differences in quartiles and levels of categorized variables were compared with a referent group and were considered statistically significant where P < 0.05 or where the 95% CI for the OR excluded 1.00. The Open Source Epidemiologic Statistics for Public Health calculator was used for power calculations (18). At α = 0.05 and β = 0.20, the total sample size of 770 (APFT), 770 (pull-ups), 685 (run time), road march time (673), obstacle course (642), and 468 (land navigation) was sufficient to detect mean differences of 3.28, 3.46, 3.69, 3.73, 3.86, and 4.60, respectively, in HEI-2015 score between quartile 1 and quartile 4 of physical performance variables in adjusted models.
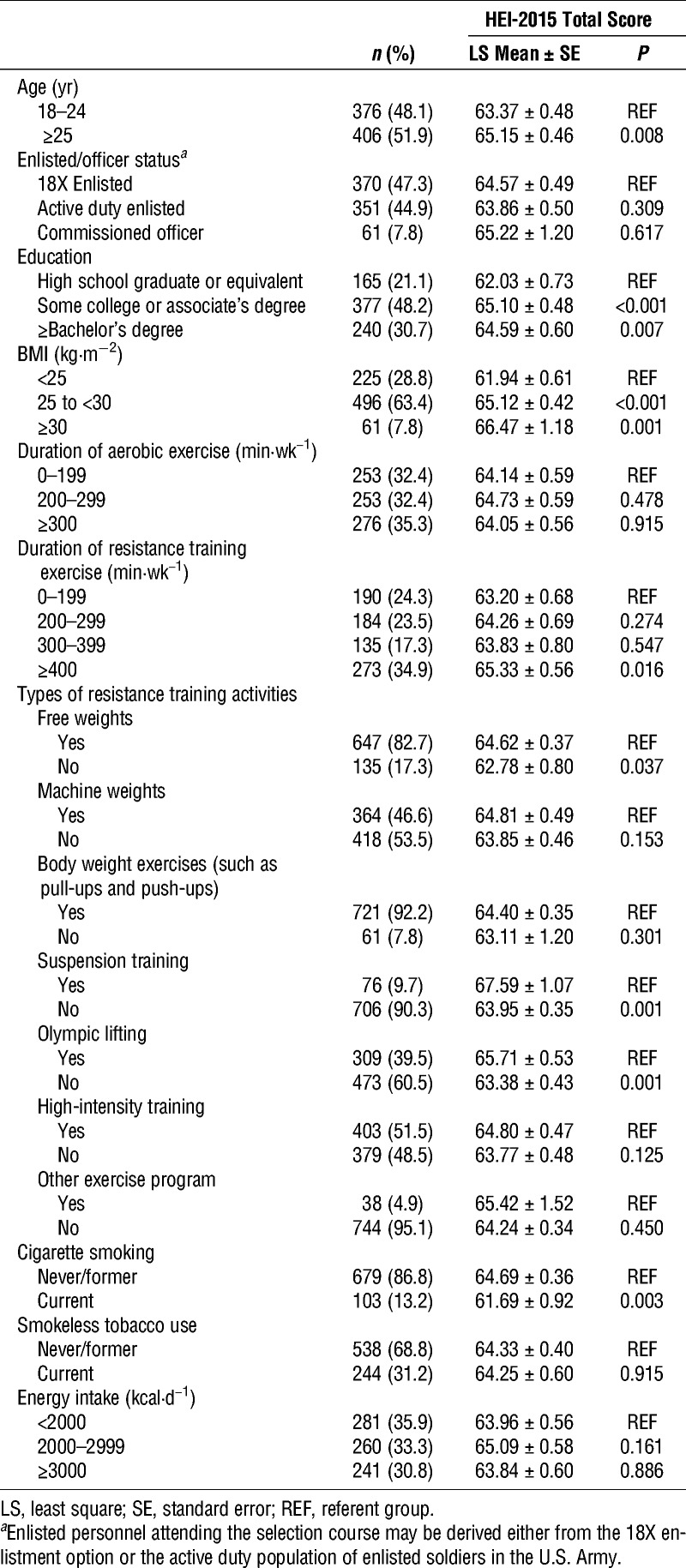
TABLE 1.
Association between HEI-2015 total score, demographic characteristics, and health behaviors among candidates in the U.S. Army SFAS course (N = 782).
RESULTS
The HEI-2015 total score was significantly higher among older soldiers (≥25 yr), those with more education (some college or a bachelor’s degree), higher BMI (≥25), those engaged in longer duration of resistance training exercise (≥400 min·wk−1), those that used free weights or suspension training, those engaged in Olympic lifting, and nonsmokers (Table 1). There were no significant associations between HEI-2015 total score and enlisted/officer status, duration of aerobic exercise, use of machine weights, body weight exercises, high-intensity training, other exercise programs, smokeless tobacco use, or energy intake.
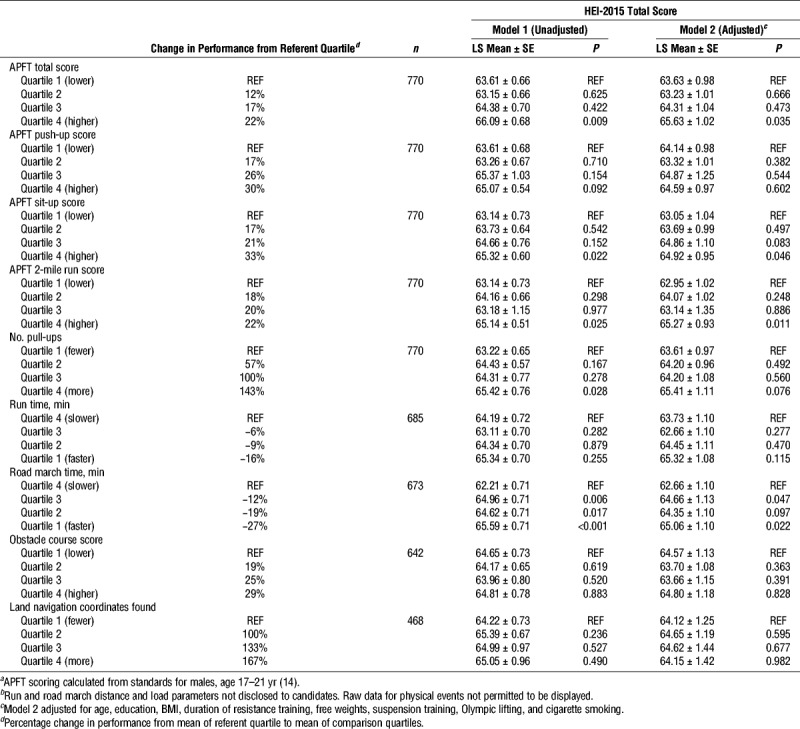
Associations between HEI-2015 total score and physical performance measures are shown in Table 2. Before adjustment for potential confounders (age, education, BMI, duration of resistance training, use of free weights, suspension training, Olympic lifting, and cigarette smoking), HEI-2015 total score was significantly higher among those with higher APFT total scores (quartile 4 vs quartile 1), APFT sit-up scores (quartile 4 vs quartile 1), APFT run scores (quartile 4 vs quartile 1), greater number of pull-ups (quartile 4 vs quartile 1), and faster road march times (quartiles 1, 2, and 3 vs quartile 4). After adjustment, HEI-2015 total score was significantly higher among those with higher APFT total scores (quartile 4 vs quartile 1), APFT sit-up scores (quartile 4 vs quartile 1), APFT run scores (quartile 4 vs quartile 1), and faster road march times (quartiles 1 vs quartile 4). After adjustment, the association between HEI-2015 total score and number of pull-ups was no longer significant (P = 0.076). There were no significant associations between HEI-2015 total score and run time, obstacle course score, or number of land navigation coordinates found.
TABLE 2.
Association between HEI-2015 total score and physical performance in the U.S. Army SFAS course.a,b
The probability of selection was significantly higher among those with higher HEI-2015 total scores (quartile 1 vs quartiles 3 and 4) (Table 3). After adjustment, those with HEI-2015 total score in quartiles 3 and 4 were 75% and 65% more likely, respectively, to be selected compared with those with scores in quartile 1.
TABLE 3.
Association between quartile of HEI-2015 total score and likelihood of successful selection in the U.S. Army SFAS course (N = 782).

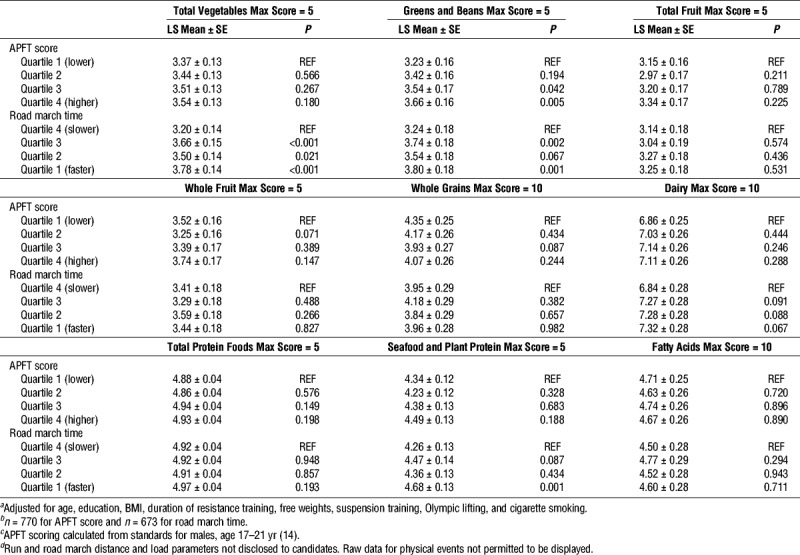
Associations between HEI-2015 individual component scores assessing adequate intakes and physical performance are shown in Table 4. After adjustment, total vegetable score was significantly higher among those with faster road march times (quartiles 1, 2, and 3 vs quartile 4). Greens and beans score was significantly higher among those with higher APFT scores (quartiles 4 and 3 vs quartile 1) and faster road march times (quartiles 1 and 3 vs quartile 4). Seafood and plant protein score was significantly higher among those with faster road march times (quartile 1 vs quartile 4). There were no significant associations between total fruit, whole fruit, whole grains, dairy, total protein foods, or fatty acid ratio score and any physical performance measures.
TABLE 4.
Association between HEI-2015 individual component scores assessing adequate intakes and physical performance in the U.S. Army SFAS course.a,b,c,d
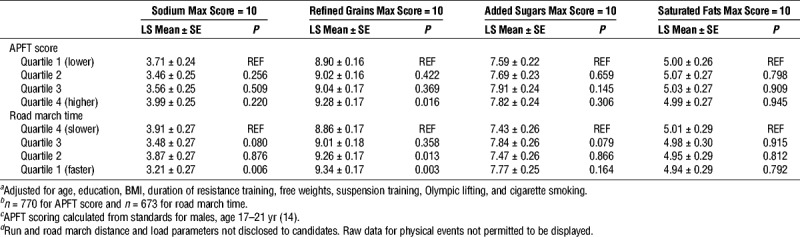
Associations between HEI-2015 individual component scores assessing moderation and physical performance are shown in Table 5. After adjustment, sodium score was significantly lower (indicating more sodium consumed) among those with faster road march times (quartile 1 vs quartile 4). Refined grains score was significantly higher (indicating fewer refined grains consumed) among those with higher APFT scores (quartile 4 vs quartile 1) and faster road march times (quartiles 1 and 2 vs quartile 4). There were no significant associations between added sugars or saturated fats individual component scores and physical performance.
TABLE 5.
Association between HEI-2015 individual component scores assessing moderation and physical performance in the U.S. Army SFAS course.a,b,c,d
DISCUSSION
This study determined associations between diet quality, physical performance, and successful selection following the U.S. Army SFAS course. The assessment course is characterized by arduous cognitive and physical demands and is designed to select individuals with attributes required to be successful in the elite U.S. Army Special Forces. Higher overall diet quality as measured by the HEI-2015 was associated with objective measures of physical performance, including faster loaded road march times and higher fitness test scores, as well as increased probability of selection. However, the individual component for sodium intake was an exception, in which lower scores (indicative of more sodium consumed) were associated with faster loaded road march times. These findings are important since the loaded road march is the physical performance measure that is most predictive of successful selection in SFAS and the fitness test is the first physical event soldiers must pass to continue in the course (13).
It is plausible that the quality of usual diet consumed before SFAS may influence performance through several mechanisms, such as supporting nutritional needs during training and recovery after physical events, facilitating ideal body composition, and contributing to adequate micronutrient and macronutrient status. Because diet quality is potentially modifiable, these findings may be used to provide nutritional guidance to soldiers preparing to attend SFAS and athletes preparing to compete in rigorous physical events, in combination with established dietary strategies known to enhance athletic performance (1).
Investigations examining relationships between diet quality and physical performance have typically been limited to observational studies among older populations that utilize various methods to characterize diet quality and performance. Higher scores indicating adherence with a Nordic diet (calculated from scores assigned to intake of fruits, vegetables, cereals, polyunsaturated fatty acid to saturated fatty acid and trans fatty acid ratio, low-fat milk, fish, red and processed meat, total fat, and alcohol) was longitudinally associated with better performance on chair stand, 6-min walk, and arm curl tests among Finnish women, but not men (19). Similarly, higher scores indicating adherence to a Mediterranean-style diet were associated with a battery of physical performance measures among Italian women and men, including 4-m walking speed, chair rises, and standing balance, before adjustment for potential confounding variables (20). Healthier dietary patterns identified by principal components analyses have also been associated with grip strength (5,21,22) and better performance on the chair rise, timed-up-and-go, or standing balance tests (9,22), with associations generally more robust before adjustment for confounding variables. Higher HEI-2005 total scores were associated with faster gait speed and greater knee extensor power (12), but adjustment for physical activity attenuated the association. In contrast to several of the aforementioned studies among older adults (5,9,20–22), the association in the present study persisted after adjustment for potential confounding variables, including measures of physical activity. One possible reason the association with diet quality persisted after adjustment may be because many of the physical performance measures examined in our study were more challenging than the measures used to assess physical performance in older adults.
Our finding of an association between diet quality and physical performance measures corroborates previous observational studies. However, to our knowledge, this is the first study to demonstrate this association with diet quality measured by the HEI-2015 in a younger, healthy, and physically active population. One prior study reported that soldiers with higher healthy eating scores measured with a brief 5-question survey were more likely to pass the APFT (23). Similarly, in the present study, diet quality scores were associated with APFT total score, in addition to individual events assessing aspects of muscular endurance (APFT sit-up score) and cardiovascular endurance (APFT run score). Some studies have described diet quality in athletes measured by various composite scores (24–29), but these have not related diet quality to objective measures of physical performance. Two studies reported that nutrition knowledge was associated with diet quality scores (28,29). Others reported the adequacy of diet quality with mixed results (24–27). More commonly, adequacy of dietary intake among athletes has been described in relation to energy and macronutrient intakes (30).
Diet quality was associated with several demographic and health characteristics. The finding that HEI-2015 total score was higher among those that reported engaging in longer duration of resistance training (≥400 min·wk−1), as well as Olympic lifting, is consistent with previous research showing that better diet quality as measured by the HEI is associated with greater frequency of physical activity among U.S. adults (31). Although the association between HEI-2015 scores and physical performance measures persisted after adjustment for duration of resistance training, use of free weights and suspension training, and participation in Olympic lifting, the possibility that higher diet quality combined with effective physical training strategies work synergistically to support optimal physical performance cannot be dismissed. For example, higher diet quality measured by the Canadian HEI combined with increases in physical activity over time, but not higher diet quality alone, were associated with less loss of elbow flexor strength among older adult men (32). In soldiers, higher healthy eating scores were associated with meeting weekly exercise recommendations (23).
HEI-2015 total score was also higher among soldiers with higher BMI (≥25). This is in contrast to a previous report in which adult men with higher HEI-2010 scores were less likely to have a BMI classified as overweight or obese (≥25) (10). Another study reported that HEI-2005 scores were inversely associated with BMI among men age 30 to 59 yr, but not those age 20 to 29 yr (33), whereas HEI scores were not associated with a BMI classified as overweight or obese (≥25) among U.S. adult men (31). In our sample of healthy, physically active men, it is possible that higher BMI is a poor indicator of overweight and obesity and may also be reflective of differences in lean mass. For example, the average BMI of elite U.S. Army Special Operations Forces (SOF) soldiers was previously reported to be 26.3 ± 2.4 (34). The average lean mass reported for these SOF soldiers is also higher than the average lean mass reported for recruits in basic combat training (77 kg vs 72 kg) (35), in which the same body composition measures were used to calculate lean mass in both studies. In agreement with previous research, higher diet quality scores were also associated with older age, more education, and being a nonsmoker (31).
The average HEI-2015 scores among soldiers in the third and fourth quartile in the present study (68.92 ± 2.65 and 77.64 ± 4.57, respectively) approximate the average HEI-2010 score previously reported among elite U.S. Army SOF soldiers (70.3 ± 9.1) (36) and the average HEI-2005 score of U.S. Army recruits in the highest tertile of diet quality in basic training (73.1 ± 6.2) (37). Soldiers with diet quality scores in the third and fourth quartiles were also much more likely to be selected for the opportunity to receive additional training to qualify as a Special Forces Soldier after SFAS than those in the first quartile (36% vs 23%). Taken together, it may be surmised that variation in the quality of usual dietary intake exists among U.S. Army Soldiers and that higher diet quality may be characteristic of dietary patterns adopted by successful SOF personnel.
Higher HEI-2015 scores for several individual components were associated with fitness test scores or loaded road march time, including total vegetables, greens and beans, seafood and plant protein, and refined grains. The associations were independent of energy intake since HEI-2015 scores are calculated from intakes standardized to energy intake. It cannot be determined from this observational study whether the individual components are causally related. However, both vegetable (4,5) and protein (6–8) consumption has been associated with physical performance measures or physical functioning in observational studies. To minimize loss of muscle mass, protein intake of 1.5 to 2.0 g·kg−1 body mass is recommended for military personnel during periods of increased metabolic demand (38). Higher scores for the refined grains individual component (indicating fewer refined grains consumed) may be reflective of an overall healthier dietary pattern, as post hoc analyses show the HEI-2015 total score and refined grains score are correlated (r = 0.44, P < 0.001).
The individual component for sodium was the only exception, as lower scores, indicative of more sodium consumed, were associated with better performance on the loaded road march. The requirement to replace water and sodium losses from sweat among athletes to prevent dehydration and hyponatremia is well established (39). Athletes are not advised to restrict sodium after bouts of exercise (1), and soldiers are advised to replace sodium losses due to physical work by consuming food, beverages, and adding salt to foods (40). The use of carbohydrate-electrolyte beverages may be warranted under certain conditions, such as when sodium losses cannot be replaced by diet alone (40). Our finding of an association between consuming more sodium and better performance on a loaded road march test supports existing guidance for athletes and physically active soldiers for avoiding excessive restriction of sodium intake.
In agreement with our hypothesis, higher diet quality, as measured by the HEI-2015 was associated with better performance on objective measures of physical performance among soldiers in the U.S. Army SFAS course, including faster loaded road march times and higher fitness test scores. Soldiers with higher diet quality scores were more likely to be selected to receive additional training to be qualified as a Special Forces soldier. One exception was the individual component for sodium, as lower scores were associated with better performance on the loaded road march. These findings may be used to formulate guidance on overall dietary patterns for soldiers or athletes that engage in arduous physical activities.
Acknowledgments
The authors thank the volunteers for their participation in this study and the USARIEM technical staff for collecting and processing data. This research was conducted under a Memorandum of Agreement between the USASOC and the USARIEM, and was reviewed by the USASOC Public Affairs Office. For more information, please contact the USASOC Public Affairs Office at (910) 432–6005 or pao@socom.mil. This work was supported by the US Army Medical Research and Development Command (USAMRDC). The views, opinions and findings in this report are those of the authors and should not be construed as an official Department of Defense policy, or decision, unless so designated by other official documentation. Citations of commercial organizations and trade names in this report do not constitute an official Department of the Army endorsement or approval of the products or services of these organizations.
The authors declare no conflicts of interest. Results of the present study do not constitute endorsement by the American College of Sports Medicine. Results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
REFERENCES
- 1.Thomas DT, Erdman KA, Burke LM. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: nutrition and athletic performance. J Acad Nutr Diet. 2016;116(3):501–28. [DOI] [PubMed] [Google Scholar]
- 2.Guenther PM, Casavale KO, Kirkpatrick SI, et al. Update of the Healthy Eating Index: HEI-2010. J Acad Nutr Diet. 2013;113(4):569–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Guenther PM, Kirkpatrick SI, Reedy J, et al. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 dietary guidelines for Americans. J Nutr. 2014;144(3):399–407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Houston DK, Stevens J, Cai J, Haines PS. Dairy, fruit, and vegetable intakes and functional limitations and disability in a biracial cohort: the atherosclerosis risk in communities study. Am J Clin Nutr. 2005;81(2):515–22. [DOI] [PubMed] [Google Scholar]
- 5.Robinson SM, Jameson KA, Batelaan SF, et al. Diet and its relationship with grip strength in community-dwelling older men and women: the Hertfordshire cohort study. J Am Geriatr Soc. 2008;56(1):84–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fanelli Kuczmarski M, Pohlig RT, Stave Shupe E, Zonderman AB, Evans MK. Dietary protein intake and overall diet quality are associated with handgrip strength in African American and white adults. J Nutr Health Aging. 2018;22(6):700–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gregorio L, Brindisi J, Kleppinger A, et al. Adequate dietary protein is associated with better physical performance among post-menopausal women 60-90 years. J Nutr Health Aging. 2014;18(2):155–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Landi F, Calvani R, Tosato M, et al. Animal-derived protein consumption is associated with muscle mass and strength in community-dwellers: results from the Milan EXPO survey. J Nutr Health Aging. 2017;21(9):1050–6. [DOI] [PubMed] [Google Scholar]
- 9.Robinson SM, Westbury LD, Cooper R, et al. Adult lifetime diet quality and physical performance in older age: findings from a British birth cohort. J Gerontol A Biol Sci Med Sci. 2018;73:1532–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Drenowatz C, Shook RP, Hand GA, Hébert JR, Blair SN. The independent association between diet quality and body composition. Sci Rep. 2014;4:4928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vogel JA, Friedl KE. Body composition and physical performance: applications for the Military Services. In: Marriott BM, Grumstrup-Scott J, editors. Army Data: Body Composition and Physical Performance. Washington, DC: National Academies Press; 1992. pp. 89–103. [PubMed] [Google Scholar]
- 12.Xu B, Houston DK, Locher JL, et al. Higher Healthy Eating Index-2005 scores are associated with better physical performance. J Gerontol A Biol Sci Med Sci. 2012;67(1):93–9. [DOI] [PubMed] [Google Scholar]
- 13.Beal SA, U.S. Army Research Institute for the Behavioral and Social Sciences. In: The Roles of Perseverance, Cognitive Ability, and Physical Fitness in U.S. Army Special Forces Assessment and Selection (Report No. 1927). Arlington, VA; 2010. Available from: Defense Technical Information Center. http://www.dtic.mil/dtic/tr/fulltext/u2/a525579.pdf. [Google Scholar]
- 14.Army Physical Readiness Training, Field Manual 7–22. Washington, DC: Headquarters, Department of the Army; 2012. [Google Scholar]
- 15.Block G, Woods M, Potosky A, Clifford C. Validation of a self-administered diet history questionnaire using multiple diet records. J Clin Epidemiol. 1990;43(12):1327–35. [DOI] [PubMed] [Google Scholar]
- 16.Mares-Perlman JA, Klein BE, Klein R, Ritter LL, Fisher MR, Freudenheim JL. A diet history questionnaire ranks nutrient intakes in middle-aged and older men and women similarly to multiple food records. J Nutr. 1993;123(3):489–501. [DOI] [PubMed] [Google Scholar]
- 17.Krebs-Smith SM, Pannucci TE, Subar AF, et al. Update of the Healthy Eating Index: HEI-2015. J Acad Nutr Diet. 2018;118(9):1591–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health Website, Version 3.01. Accessed March 14, 2019. Available at: www.openepi.com.
- 19.Perälä MM, von Bonsdorff M, Männistö S, et al. A healthy Nordic diet and physical performance in old age: findings from the longitudinal Helsinki Birth Cohort Study. Br J Nutr. 2016;115(5):878–86. [DOI] [PubMed] [Google Scholar]
- 20.Milaneschi Y, Bandinelli S, Corsi AM, et al. Mediterranean diet and mobility decline in older persons. Exp Gerontol. 2011;46(4):303–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Martin H, Aihie Sayer A, Jameson K, et al. Does diet influence physical performance in community-dwelling older people? Findings from the Hertfordshire Cohort Study. Age Ageing. 2011;40(2):181–6. [DOI] [PubMed] [Google Scholar]
- 22.Granic A, Jagger C, Davies K, et al. Effect of dietary patterns on muscle strength and physical performance in the very old: findings from the Newcastle 85+ study. PLoS One. 11(3):e0149699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Purvis DL, Lentino CV, Jackson TK, Murphy KJ, Deuster PA. Nutrition as a component of the performance triad: how healthy eating behaviors contribute to soldier performance and military readiness. US Army Med Dep J. 2013;66–78. [PubMed] [Google Scholar]
- 24.Jürgensen LP, Silva Daniel NV, da Costa Padovani R, D’Avila Lourenco LC, Ridel Juzwiak C. Assessment of the diet quality of sports athletes. Rev Bras Cineantropom Desempenho Hum. 2015;17(3):280–90. [Google Scholar]
- 25.Tsoufi A, Maraki MI, Dimitrakopoulos L, Famisis K, Grammatikopoulou MG. The effect of professional dietary counseling: elite basketball players eat healthier during competition days. J Sports Med Phys Fitness. 2017;57(10):1305–10. [DOI] [PubMed] [Google Scholar]
- 26.McConnell C, McPherson A, Woolf K. Competition level not associated with diet quality in marching artists. Int J Sport Nutr Exerc Metab. 2018;28(1):66–74. [DOI] [PubMed] [Google Scholar]
- 27.Burrows T, Harries SK, Williams RL, Lum C, Callister R. The diet quality of competitive adolescent male Rugby union players with energy balance estimated using different physical activity coefficients. Nutrients. 2016;8(9):E548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Citarella R, Itani L, Intini V, et al. Nutritional knowledge and dietary practice in elite 24-hour ultramarathon runners: a brief report. Sports (Basel). 2019;7(2):E44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Spronk I, Heaney SE, Prvan T, O’Connor HT. Relationship between general nutrition knowledge and dietary quality in elite athletes. Int J Sport Nutr Exerc Metab. 2015;25(3):243–51. [DOI] [PubMed] [Google Scholar]
- 30.Nunes CL, Matias CN, Santos DA, et al. Characterization and comparison of nutritional intake between preparatory and competitive phase of highly trained athletes. Medicina (Kaunas). 2018;54(3):E41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Guo X, Warden BA, Paeratakul S, Bray GA. Healthy Eating Index and obesity. Eur J Clin Nutr. 2004;58(12):1580–6. [DOI] [PubMed] [Google Scholar]
- 32.Rahi B, Morais JA, Dionne IJ, Gaudreau P, Payette H, Shatenstein B. The combined effects of diet quality and physical activity on maintenance of muscle strength among diabetic older adults from the NuAge cohort. Exp Gerontol. 2014;49:40–6. [DOI] [PubMed] [Google Scholar]
- 33.Pate RR, Taverno Ross SE, Liese AD, Dowda M. Associations among physical activity, diet quality, and weight status in U.S. adults. Med Sci Sports Exerc. 2015;47(4):743–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Farina EK, Taylor JC, Means GE, et al. Effects of combat deployment on anthropometrics and physiological status of U.S. Army Special Operations Forces Soldiers. Mil Med. 2017;182(3):e1659–68. [DOI] [PubMed] [Google Scholar]
- 35.Pasiakos SM, Karl JP, Lutz LJ, et al. Cardiometabolic risk in US Army recruits and the effects of basic combat training. PLoS One. 2012;7(2):e31222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Farina EK, Taylor JC, Means GE, et al. Effects of deployment on diet quality and nutritional status markers of elite U.S. Army special operations forces soldiers. Nutr J. 2017;16(1):41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lutz LJ, Gaffney-Stomberg E, Scisco JL, et al. Assessment of dietary intake using the Healthy Eating Index during military training. US Army Med Dep J. 2013;91–7. [PubMed] [Google Scholar]
- 38.Pasiakos SM, Austin KG, Lieberman HR, Askew EW. Efficacy and safety of protein supplements for U.S. Armed Forces personnel: consensus statement. J Nutr. 2013;143(11):1811S–4. [DOI] [PubMed] [Google Scholar]
- 39.Shirreffs SM, Sawka MN. Fluid and electrolyte needs for training, competition, and recovery. J Sports Sci. 2011;29(1 Suppl):S39–46. [DOI] [PubMed] [Google Scholar]
- 40.Nutrition and Menu Standards for Human Performance Optimization, Army Regulation 40–25. Washington, DC: Headquarters, Department of the Army; 2017. [Google Scholar]