

Abstract
Background.
Technetium-99m pyrophosphate (Tc-99m PYP) protocols for transthyretin cardiac amyloidosis (ATTR CA) diagnosis have variably used one-hour and three-hour imaging time points. We investigated if imaging at one hour with superior efficiency had comparable diagnostic accuracy as three-hour imaging.
Methods.
This is a registry analysis of patients with suspected ATTR CA referred for Tc-99m PYP at a single tertiary center from June 2015 through January 2019. Patients underwent planar and single-photon emission computerized tomography (SPECT) imaging at one and three hours. Diffuse myocardial Tc-99m PYP on SPECT was considered diagnostic of ATTR CA. Visual semi-quantitative (grades 0–3, ≥2 defines a positive test) and quantitative heart to contralateral lung ratio (H/CL ≥ 1.5 defines a positive test) scales were utilized.
Results.
233 patients (69% men, median age 77 (69, 83) years) underwent the study protocol. There were 60 (25.8%) patients with diffuse myocardial uptake, 1 (0.4%) with regional uptake, and 172 (73.8%) with no myocardial uptake. Results of SPECT were identical at one and three hours. Planar imaging at one hour had 98% sensitivity and 96% specificity. Planar grade 0 uptake or H/CL ratio ≤1.2, and planar grade 3 uptake or H/CL ratio ≥ 2.0 were always associated with negative and positive SPECT, respectively. For planar grades 1–2 uptake and H/CL ratio 1.3–1.9, SPECT was needed to make a diagnosis. No patient with light chain CA had positive SPECT.
Conclusion.
An efficient one-hour Tc-99m PYP protocol had comparable diagnostic performance to a three-hour protocol.
Keywords: Cardiac amyloid, technetium pyrophosphate, transthyretin, nuclear cardiology
Introduction.
Technetium 99m pyrophosphate (Tc-99m PYP) scintigraphy is highly accurate for the diagnosis of transthyretin cardiac amyloidosis (ATTR CA), with a positive predictive value of 100% when concomitant serum and urine studies for light chain AL amyloidosis (AL CA) are negative1. This ability to make a confirmed diagnosis of ATTR CA noninvasively has resulted in the recognition of a significantly higher prevalence of this disease than previously reported. For example, a recent study reported a 13.3% prevalence of ATTR CA in elderly patients with heart failure with preserved ejection fraction and left ventricular hypertrophy2. Other studies have uncovered 15–20% ATTR CA prevalence in patients with aortic stenosis3–6. Thus, the referral base of patients for advanced imaging tests for ATTR CA is expanding considerably.
The cardiac Tc-99m PYP protocol continues to evolve, with centers variably performing planar and SPECT imaging at one and/or three hours. A recent survey of 101 centers showed low penetrance and high variability in Tc-99m PYP protocols7. For example, only 35% of centers acquired images one hour after tracer injection, relying on more delayed imaging resulting in a longer protocol8. The American Society of Nuclear Cardiology released its Practice Points9 in 2016 with a recent update10 in 2019 in an attempt to standardize Tc-99m PYP imaging. The writing committee recommended planar and single-photon emission computerized tomography (SPECT) imaging at one hour with optional imaging at three hours10. A similar recommendation was recently published in a multi-societal expert consensus on imaging CA11. However, the additive value of three-hour imaging when SPECT imaging is performed at one hour is unknown. We sought to determine whether an efficient one-hour protocol can be implemented with equal diagnostic accuracy as a three-hour protocol, to improve test efficiency and patient comfort.
Methods
The data, analytic methods, and study materials will not be made available to other researchers for purposes of reproducing the results or replicating the procedure.
This was an observational registry of patients referred for cardiac Tc-99m PYP for suspicion of ATTR CA at a single quaternary academic center from June 2015 to January 2019. Patients were excluded if they did not undergo imaging at both the one-hour and three-hour time points. Patients were referred for Tc-99m PYP for clinical suspicion of ATTR CA. Serum free light chains and their ratio, and serum immunofixation electrophoresis were performed in the majority of patients, according to the prevailing practice in our institution. Genetic testing for known TTR mutations was performed when a diagnosis of ATTR CA was established. The study was approved by the local institutional review board and informed consent was waived.
Technetium Pyrophosphate Scintigraphy
We followed the standard procedure recommendations of the American Society of Nuclear Cardiology9. After injecting 15 millicuries of technetium 99m pyrophosphate, planar (anterior, left anterior oblique and lateral views) and single photon emission computed tomography (SPECT) images were obtained at one and three hours. Imaging was performed using a dual-headed Phillips Forte gamma camera (Milpitas, CA) with a 90-degree detector configuration and low-energy high-resolution parallel-hole collimators. For planar imaging, non-gated acquisitions were performed for 8 min to acquire anterior and left lateral images simultaneously, and a left anterior oblique (LAO) image. We routinely acquire an LAO image to enable visualization of the right ventricle which is best seen in this view. Non-gated SPECT images were acquired over a 180-degrees orbit using a step and shoot approach, with a 20-second acquisition per stop for patients less than 200 pounds and 25-seconds per stop for heavier patients. When there was no myocardial uptake of the tracer, patient positioning was aided by using the upper and lower ends of the sternum as reference points. Images were processed using Pegasys Workstation. The planar mages were interpreted using the semi-quantitative visual scoring system proposed by Perugini12 (0=absent cardiac uptake, I = mild cardiac uptake less than bone, 2= moderate cardiac uptake equal to bone, 3= high cardiac uptake greater than bone)9. For planar only studies, a positive planar Tc-99m PYP test is diagnosed when there is semi-quantitative grade 2 or 3 uptake. A quantitative analysis of Tc-99m PYP uptake was performed using the heart to contralateral lung (H/CL) ratio13 on both the one and three-hour scans. A circular region of interest (ROI) was drawn to encompass the left ventricle without including surrounding lung or the sternum. This ROI was mirrored over the contralateral lung, again taking care to avoid the right border of the heart and the sternum. The mean counts per pixel in the heart (H) and contralateral lung (CL) ROIs were measured to derive a ratio the H/CL ratio. Prior studies have shown a H/CL ratio of ≥ 1.5 on planar imaging to be specific for ATTR CA (versus AL amyloidosis)13. Ratios were rounded to the nearest decimal point. The SPECT images were used to confirm diffuse myocardial uptake of Tc-99m PYP (rather than focal or LV cavity uptake giving the appearance of a positive planar scan). For the purpose of this study, we defined a positive Tc-99m PYP study as having diffuse myocardial uptake of Tc-99m PYP on SPECT imaging. In many institutions including ours practice patterns have evolved such that a myocardial biopsy in no longer routinely performed when the cardiac Tc-99 PYP scan is positive and the serum studies for AL amyloidosis are negative. All images (planar and SPECT) were interpreted by 2 independent readers (AM and SB), with any discordant reads adjudicated by a third reader (PS). At the time of image interpretation for the purpose of this study, the readers were not aware of the results of the clinical read.
Statistical Analysis
Continuous variables are reported as median (range). Categorical variables are reported as a frequency (percentage). Correlations are reported using Spearman’s or Kendall’s Tau correlation coefficient, as appropriate. Sensitivity, specificity, positive and negative predictive values were computed against diffuse Tc-99m PYP uptake on SPECT (which we considered the gold standard for the purposes of this study). Inter-observer variability of semiquantitative visual scores and H/CL ratio were evaluated using Cohen’s Kappa coefficient and Bland Altman plots, respectively. All statistical analysis was performed using STATA version 14 (Stata Corp LP, College Station, Texas, USA).
Results
From June 2015 through January 2019, 283 patients were referred for cardiac Tc-99m PYP. Of those, 233 [69% men, median age 77 years (25th and 75th percentile were 69 and 83, respectively] completed the full protocol of one and three-hour imaging, and were included in the analysis.
SPECT:
The final diagnosis of ATTR cardiac amyloidosis was based on the presence of diffuse uptake of Tc-99m PYP on the SPECT images. Figure 1 shows one and three hour Tc-99m PYP imaging examples. All one-hour and three-hour SPECT interpretations were concordant. There were 60 (25.8%) patients with diffuse myocardial uptake, 1 (0.4%) with regional uptake and 172 (73.8%) with no myocardial uptake. There was no change in the final diagnosis between the one-hour and three-hour images. Thus, the three-hour SPECT image had no additive value to the one-hour SPECT image. There were 2 SPECT reads that were discordant between the primary readers; one interpreted as showing localized sepal uptake, and the other as showing faint diffuse uptake. Both studies were adjudicated by the third reader and considered negative. Gadolinium-enhanced cardiac magnetic resonance imaging did not show features of cardiac amyloid in either case.
Figure 1.
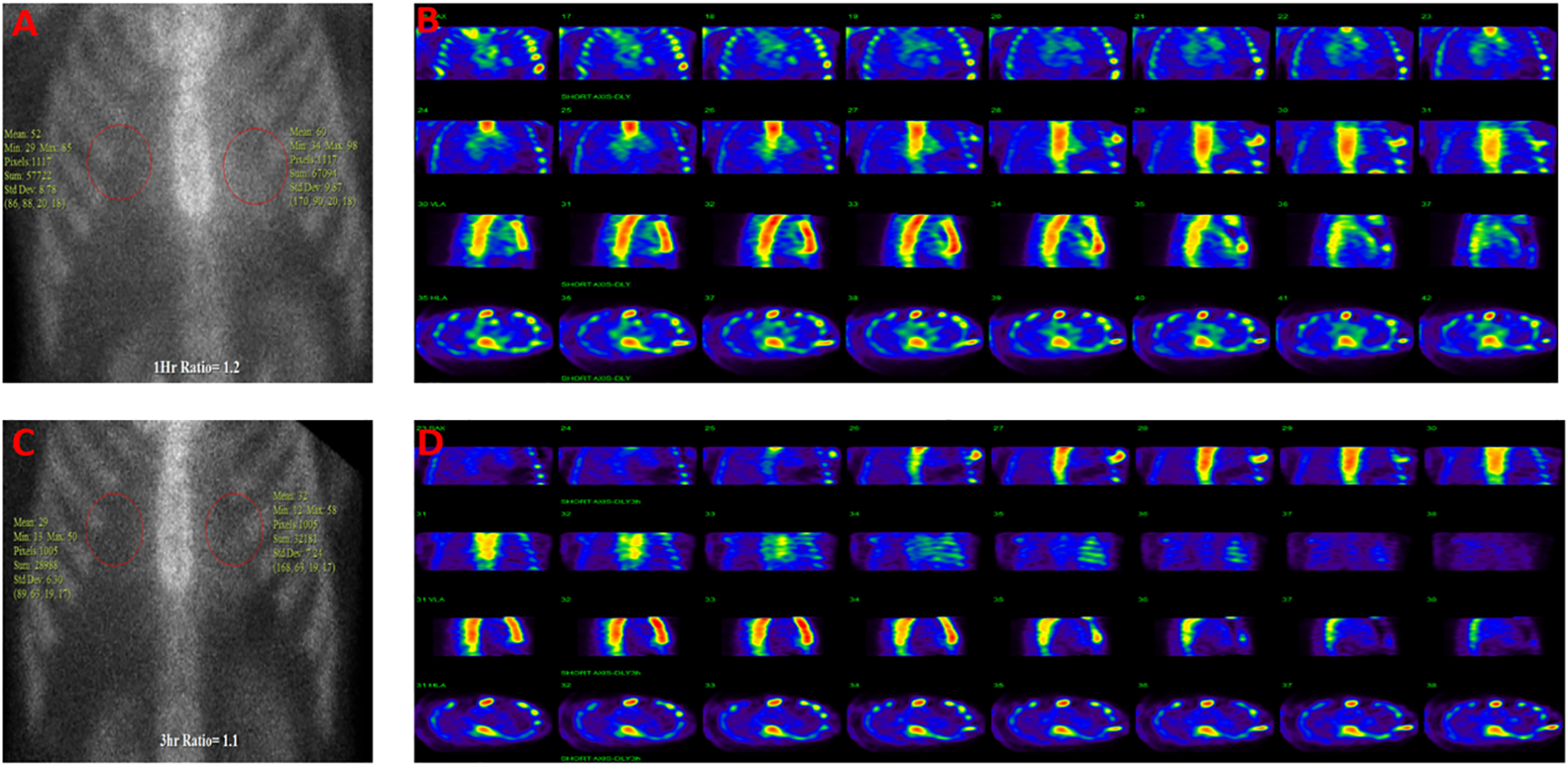
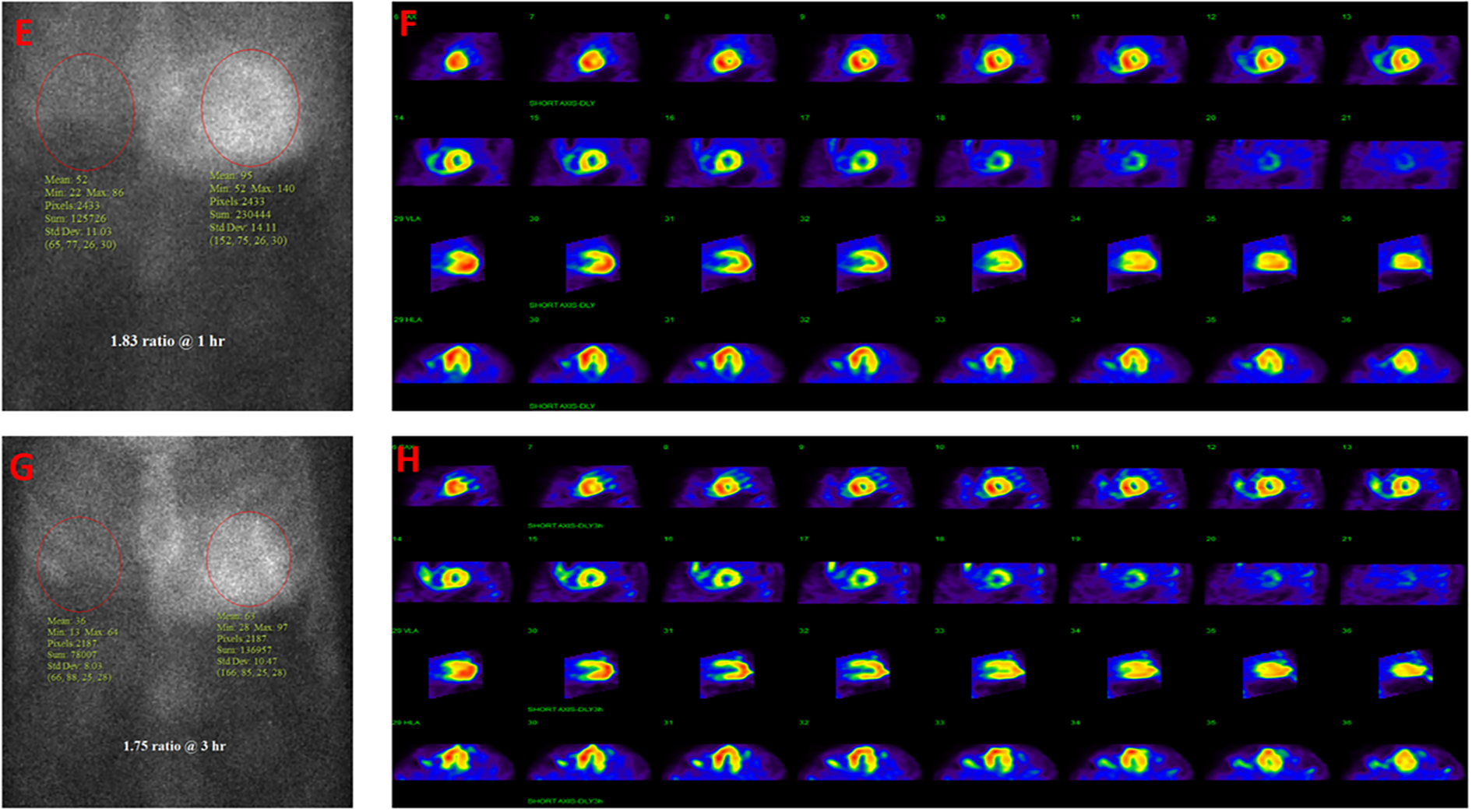
Examples of positive and negative Tc-99m PYP planar and SPECT scans obtained at one hour and three hours. (A-D) represents a negative Tc-99m PYP scan in a patient with heart failure showing grade 1 uptake at 1-hour (A) and grade 0 at 3-hour planar imaging (C) with concordant no tracer uptake on SPECT at 1 (B) or 3-hour (D) imaging. (E-H) represents a positive Tc-99m PYP scan in a patient with heart failure showing concordant grade 3 uptake on planar at 1 hour (E) and 3 hours (G), and diffuse trace uptake on SPECT at 1 (F) and 3 hours (H).
Table 1 shows the baseline characteristics of the study cohort. Patients with diffuse uptake on Tc-99m PYP SPECT were older, less often women (13.3%), with a greater prevalence of atrial fibrillation, history of unilateral or bilateral carpal tunnel syndrome, history of spinal stenosis, low voltage on electrocardiogram and thicker left ventricle on echocardiography.
Table 1.
Baseline characteristics of the study cohort.
| Variable | Tc-99m PYP negative (n=173)* | Tc-99m PYP positive (n=60)* | p-value |
|---|---|---|---|
| Age (years) | 73.8 (64.8, 81.5) | 80.6 (75.7, 84.6) | <0.001 |
| Women | 65 (37.6%) | 8 (13.3%) | <0.001 |
| Weight (kg) | 83.0 (68.3, 96.0) | 82.0 (68.5, 94.5) | 0.570 |
| History of Syncope | 48 (27.7%) | 12 (20.0%) | 0.240 |
| History of Angina | 23 (13.4%) | 4 (6.7%) | 0.160 |
| Coronary artery disease | 83 (48.3%) | 24 (40.0%) | 0.270 |
| Heart failure | 130 (75.2%) | 48 (60%) | 0.180 |
| Hypertension | 146 (84.4%) | 43 (71.7%) | 0.030 |
| Diabetes | 72 (41.9%) | 11 (18.3%) | 0.001 |
| Hyperlipidemia | 119 (68.8%) | 36 (60.0%) | 0.210 |
| Atrial fibrillation | 62 (36.5%) | 30 (52.6%) | 0.031 |
| Embolic CVA | 28 (16.2%) | 6 (10.0%) | 0.240 |
| Hemorrhagic CVA | 7 (4.1%) | 2 (3.3%) | 0.800 |
| COPD | 23 (13.4%) | 4 (6.7%) | 0.160 |
| Bilateral | 16 (9.2%) | 13 (21.7%) | |
| Spinal stenosis | 23 (13.3%) | 23 (38.3%) | <0.001 |
| Peripheral neuropathy | 81 (46.8%) | 36 (60.0%) | 0.079 |
| LVH on ECG | 22 (14.1%) | 3 (6.7%) | 0.180 |
| Low voltage on ECG | 10 (6.6%) | 9 (20.0%) | 0.008 |
| Ejection fraction (%) | 52.0±15 | 48±13 | 0.056 |
| Interventricular septum thickness on echo (cm) | 1.4±0.3 | 1.7±0.3 | <0.001 |
| Posterior wall thickness on echo (cm) | 1.3±0.3 | 1.6±0.4 | <0.001 |
| Troponin I (ng/ml) | 0.0 (0.0, 0.1) | 0.0 (0.0, 0.1) | 0.640 |
| BNP (pg/ml) | 604 (265, 1522) | 461 (245, 778) | 0.200 |
| Creatinine (mg/dl) | 1.5 (1.0, 2.3) | 1.2 (1.1, 1.5) | 0.031 |
Tc-99m PYP: technetium-99m pyrophosphate scintigraphy; CVA: cerebrovascular accident; ECG: electrocardiogram; BNP: brain natriuretic peptide
Final determination of a positive or negative Tc-99m PYP was based on the presence of diffuse uptake of Tc-99m PYP on SPECT.
One-hour Planar Images (Figure 2A, Tables 2 and 3):
Figure 2.
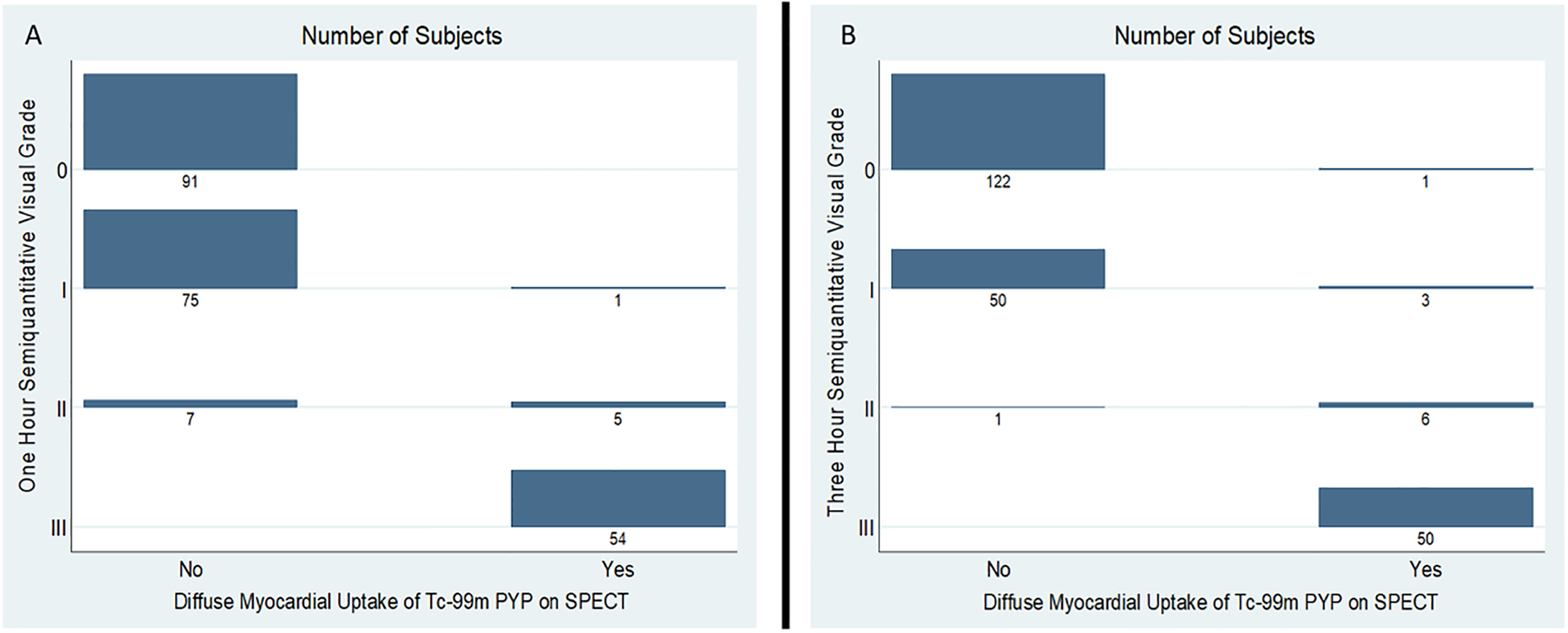
Distribution of semiquantitative visual grade (from 0 to 3) stratified by the presence of absence of diffuse myocardial uptake of Tc-99m PYP on SPECT at one hour (A) and three hours (B). The numbers reflect the frequency of subjects within each grade.
Tc-99m PYP: technetium-99m pyrophosphate scintigraphy; SPECT: single-photon emission computerized tomography
Table 2.
Semiquantitative visual grade (0 to 3) at one hour and three hours post Tc-99m PYP tracer injection.
| One-hour grade | Three-hour grade | |||
|---|---|---|---|---|
| 0 | 1 | 2 | 3 | |
| 0 | 89 | 2 | 0 | 0 |
| 1 | 32 | 44 | 0 | 0 |
| 2 | 2 | 7 | 3 | 0 |
| 3 | 0 | 0 | 4 | 50 |
Table 3.
Summary of diagnostic performance of one and three-hour planar imaging as compared to diffuse myocardial uptake of Tc-99m PYP.
| Against SPECT | TP | TN | FP | FN | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|
| One-hour grade (2/3) | 59 | 166 | 7 | 1 | 98.3% | 96.0% | 89.4% | 99.4% |
| Three-hour grade (2/3) | 56 | 172 | 1 | 4 | 93.3% | 99.4% | 98.3% | 97.7% |
| One-hour H/CL ratio (≥1.5) | 58 | 157 | 16 | 2 | 96.7% | 90.8% | 78.4% | 98.7% |
| Three-hour H/CL ratio (≥1.5) | 57 | 163 | 10 | 3 | 95.0% | 94.2% | 85.1% | 98.2% |
Tc-99m PYP: technetium-99m pyrophosphate scintigraphy; H/CL: heart/contralateral; SPECT: single-photon emission computerized tomography
On the semiquantitative visual grade, 91 (39%) patients had grade 0, 76 (32.5%) had grade 1, 12 (5.2%) had grade 2, and 54 (23.3%) had grade 3. Compared to diffuse uptake on SPECT, the presence of grade 2 or 3 uptake on planar images had 98% sensitivity, 96% specificity, 89% positive predictive value (PPV), 99% negative predictive value (NPV) and 96.6% accuracy. Only 1 patient in our study had SPECT evidence of PYP in the LV cavity at one hour, not myocardium, with a corresponding planar grade of 2 and a H/CL ratio of 1.6. The three-hour SPECT showed no tracer in the cavity or myocardium.
For the one-hour image the mean H/CL ratio was 1.9±0.3 for SPECT positive as compared to 1.2±0.1 in SPECT negative patients; p<0.001. The mean H/CL ratio for grade 0 and grade 1 were 1.23±0.13 and 1.18±0.16, respectively. Planar grade 0 in combination with H/CL ratio < 1.2 and planar grades 2/3 with H/CL ratio > 2 were always associated with negative and positive SPECT, respectively.
Three-hour planar images (Figure 2B, Tables 2 and 3):
On the semiquantitative visual grade, 123 (52.7%) patients had grade 0, 53 (22.8%) had grade 1, 7 (3%) had grade 2, and 50 (21.5%) had grade 3. Compared to diffuse uptake on SPECT, planar grade 2 or 3 uptake had a sensitivity of 93%, specificity of 99%, PPV of 98% and NPV of 98%. Notably, the sensitivity of the three-hour planar scan was lower than the one-hour planar grade. For patients with grade 2/3, the mean H/CL ratio at three hours was 1.9±0.3 as compared with 1.2±0.2 in patients with grade 0/1; p<0.001. The one-hour and three-hour H/CL ratios were highly correlated; Spearman’s correlation coefficient 0.92, p<0.0001, Figure 3.
Figure 3.
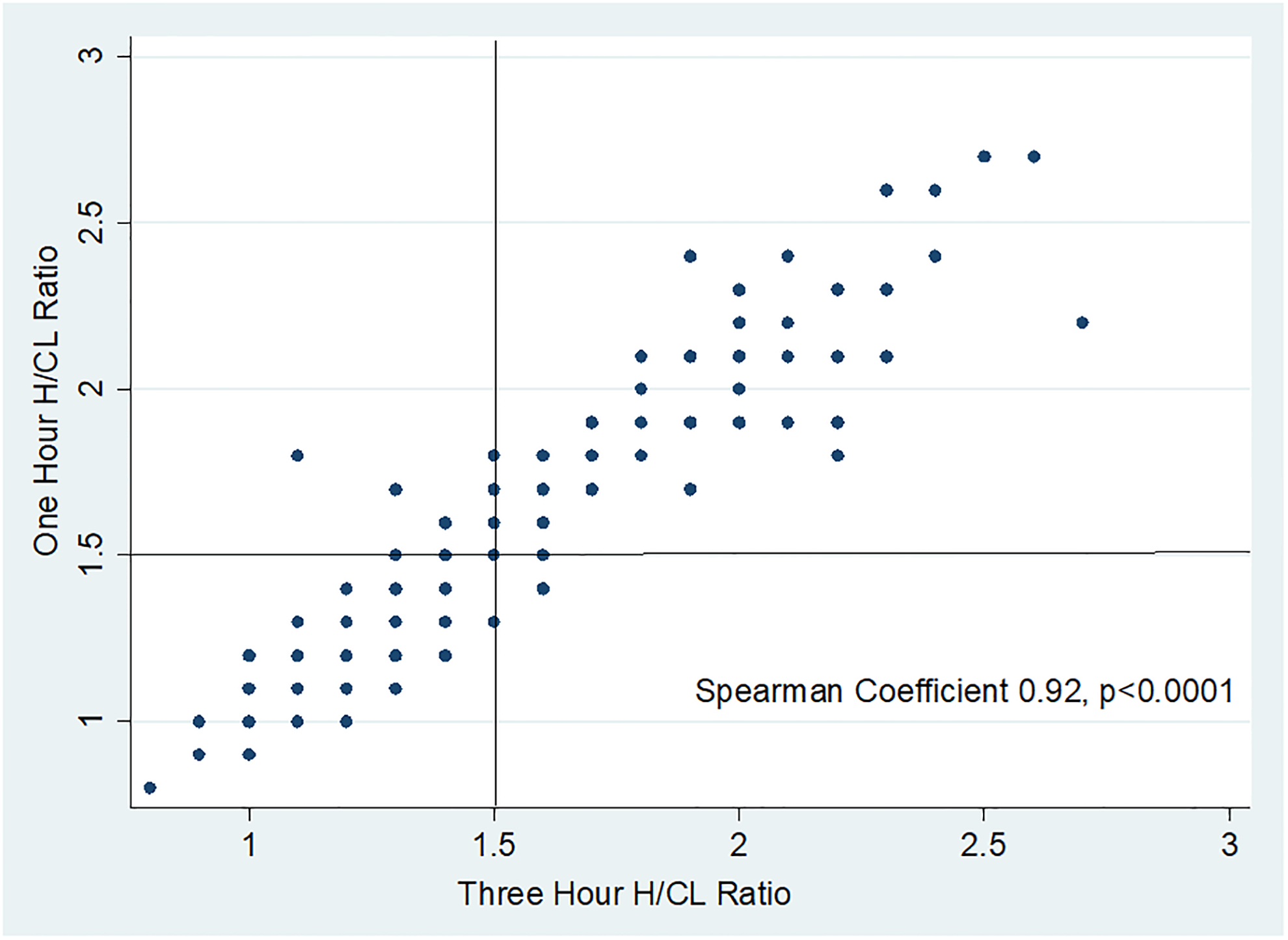
Scatterplot of heart to contralateral (H/CL) ratio at one-hour and three-hour. Scatterplot shows excellent correlation, Spearman’s correlation coefficient 0.92, p<0.0001
H/CL: heart/contralateral
Table 4 shows that a number of patients had a discrepant planar grade and H/CL ratio at both 1 and 3-hours. In these patients, SPECT was useful for diagnosis. At one hour, 5 patients with grade 1 or 0 uptake had H/CL ratio > 1.5, and 6 patient had grade 2 or 3 uptake with H/CL ratio < 1.5. In 10 of these 11 patients, the SPECT findings were concordant with the planar grade interpretation. At 3 hours, 13 patients had grade 0 or 1 planar uptake and H/CL ratio > 1.5, and 3 patients who had grade 2 planar uptake, but H/CL ratio < 1.5. Of these 16 patients, the SPECT findings were concordant with the planar grade in 13 patients. Thus, the one-hour planar grades were the most concordant with SPECT reads.
Table 4.
Discordant one-hour and three-hour Tc-99m PYP imaging results.
| Subjects | One Hour | Three Hour | Comments | CMR | ||||
|---|---|---|---|---|---|---|---|---|
| Planar grade | SPECT | Ratio | Planar grade | SPECT | Ratio | |||
| 1 | 1 | No uptake | 1.3 | 0 | No uptake | 1.5 | ND | |
| 2 | 0 | No uptake | 1.4 | 0 | No uptake | 1.6 | ND | |
| 3 | 2 | Regional uptake | 1.5 | 1 | Regional uptake | 1.4 | Thr60Ala mutation | ND |
| 4 | 0 | No uptake | 1.5 | 1 | No uptake | 1.4 | ND | |
| 5 | 0 | No uptake | 1.5 | 0 | No uptake | 1.3 | Negative | |
| 6 | 1 | No uptake | 1.5 | 0 | No uptake | 1.4 | Negative | |
| 7 | 1 | No uptake | 1.5 | 1 | No uptake | 1.4 | Negative | |
| 8 | 0 | No uptake | 1.5 | 0 | No uptake | 1.4 | ND | |
| 9 | 0 | No uptake | 1.6 | 0 | No uptake | 1.4 | Blood pool | ND |
| 10 | 2 | Diffuse uptake | 1.7 | 2 | Diffuse uptake | 1.3 | ND | |
| 11 | 0 | No uptake | 1.8 | 0 | No uptake | 1.1 | ND | |
| Discordant grade concordant ratio | ||||||||
| 12 | 2 | Diffuse uptake | 1.5 | 1 | Diffuse uptake | 1.6 | ND | |
| 13 | 2 | Diffuse uptake | 1.7 | 1 | Diffuse uptake | 1.6 | ND | |
| 14 | 2 | No uptake | 1.2 | 0 | No uptake | 1.0 | ND | |
| 15 | 2 | No uptake | 1.2 | 0 | No uptake | 1.3 | Phe64Leu mutation | Negative |
| 16 | 2 | No uptake | 1.8 | 1 | No uptake | 1.5 | ND | |
| 17 | 2 | No uptake | 1.3 | 1 | No uptake | 1.2 | Negative | |
| 18 | 2 | No uptake | 1.3 | 1 | No uptake | 1.3 | ND | |
| 19 | 2 | Diffuse uptake | 1.6 | 1 | Diffuse uptake | 1.5 | ND | |
Tc-99m PYP: technetium-99m pyrophosphate scintigraphy; H/CL: heart/contralateral; SPECT: single-photon emission computerized tomography; CMR: cardiac magnetic resonance imaging; ND: not done. Negative: negative for features suggestive of cardiac amyloidosis.
Hereditary ATTR CA.
There were 8 patients with a gene mutation consistent with Hereditary ATTR CA (four Val30Met, two Thr60Ala, one Val122Ile, one Phe61Leu). Three patients had diffuse myocardial uptake of Tc-99m PYP on SPECT, 1 had regional uptake (Thr60Ala), and 5 had no myocardial uptake on SPECT.
AL CA.
A final diagnosis of AL CA was made in 8 patients. None of these patients had Tc-99m PYP uptake on SPECT. In these patients one-hour planar imaging showed grade 1 uptake in 3 patients and grade 0 in the remaining. H/CL ratio was ≤ 1.5 in all (Table 5). Eight patients with diffuse Tc-99m PYP uptake on SPECT required additional workup to rule out AL CA because of abnormal serum studies. All underwent formal evaluation by a hematologist. Two patients had a final diagnosis of monoclonal gammopathy of uncertain significance (MGUS) and 5 had no evidence of a plasma cell dyscrasia. One patient who had a mildly abnormal free light chain assay and a clinical suspicion of MGUS refused further workup.
Table 5.
Tc-99m PYP characteristics of patients who were eventually diagnosed with AL cardiac amyloid.
| Subjects | One Hour | Three Hour | Blood pool on SPECT | ||||
|---|---|---|---|---|---|---|---|
| Planar grade | SPECT | Ratio | Planar grade | SPECT | Ratio | ||
| 1 | 0 | No uptake | 1.2 | 0 | No uptake | 1.3 | 0 |
| 2 | 0 | No uptake | 1.2 | 0 | No uptake | 1.0 | 0 |
| 3 | 0 | No uptake | 1.4 | 0 | No uptake | 1.3 | 0 |
| 4 | 0 | No uptake | 1.1 | 0 | No uptake | 1.1 | 0 |
| 5 | 1 | No uptake | 1.1 | 1 | No uptake | 1.1 | 0 |
| 6 | 0 | No uptake | 1.0 | 0 | No uptake | 0.9 | 0 |
| 7 | 1 | No uptake | 1.3 | 0 | No uptake | 1.2 | 0 |
| 8 | 1 | No uptake | 1.2 | 0 | No uptake | 1.4 | 0 |
SPECT: single-photon emission computerized tomography
Inter-observer variability.
There was excellent inter-observer agreement differentiating a positive (grade 2 and 3) from a negative (grade 0 and 1) Tc-99m PYP scan based on visual semiquantitative grade at one-hour (actual agreement 94%, k=0.86, p<0.0001) and three-hours (actual agreement 97%, k=0.93, p<0.0001). There was frequent inter-observer disagreement between grade 0 and 1, resulting in an overall poor agreement in the semi-quantitative visual grade from 0 to 3 at one-hour (actual agreement 58%, k=0.41, p<0.0001), and three-hour (actual agreement 49%, k=0.34, p<0.0001). There was excellent interobserver agreement in one-hour and three-hour measured H/CL ratios as depicted by the Bland-Altman plots in Figure 4A–B.
Figure 4.
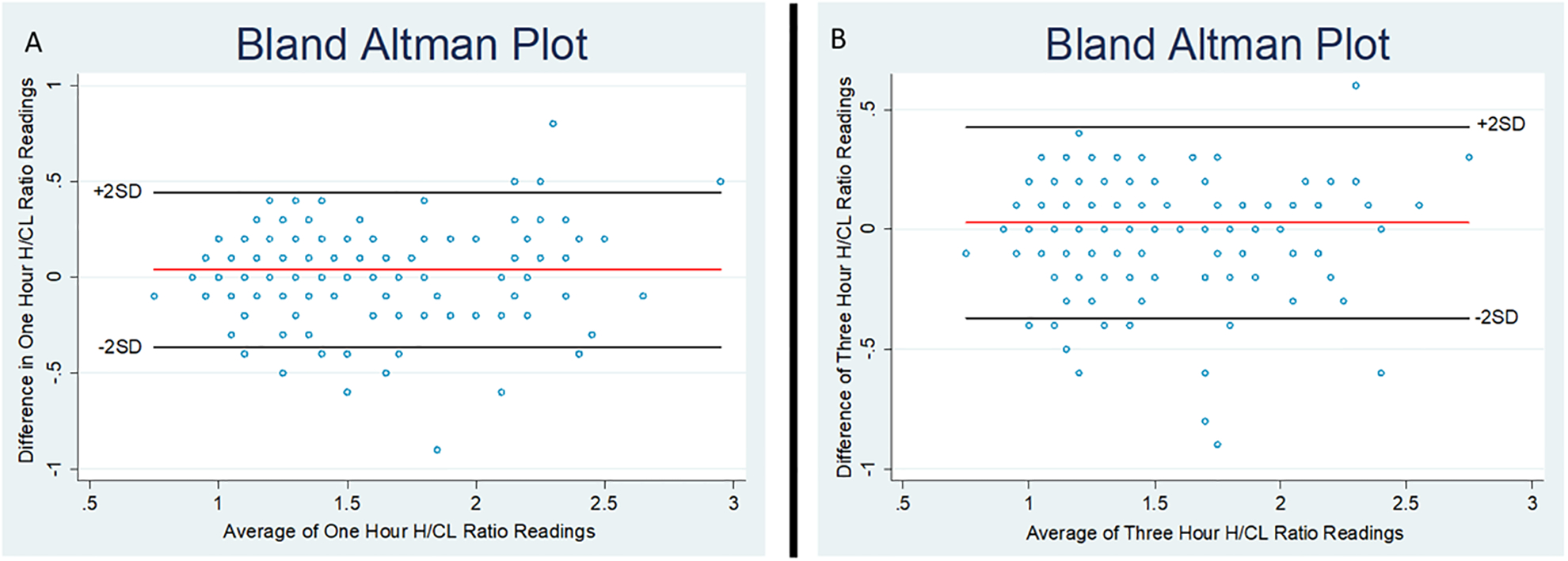
Bland-Altman Plots of the inter-observer agreement of measured heart to contralateral (H/CL) ratio. (A) At one hour, mean difference (red line) was 0.04 (95% CI 0.01, 0.07) and the two-standard deviation (SD) limit of agreement (black lines) were −0.4 and 0.4. B) At three hours, mean difference (red line) was 0.03 (95% CI 0.001, 0.05) and the two-standard deviation (SD) limit of agreement (black lines) were −0.4 and 0.4.
H/CL: heart/contralateral
Discussion
From this single center registry of 233 patients referred for Tc-99m PYP for suspicion of ATTR CA, the main finding is that a one hour protocol using planar and SPECT imaging had the same diagnostic accuracy as a three-hour protocol for the detection of diffuse myocardial uptake of Tc-99m PYP. Our findings suggest there is no additive value in three-hour imaging when SPECT imaging is performed at one hour. Thus, a time-efficient one-hour protocol has the same diagnostic efficacy as a three-hour protocol when the diagnosis of ATTR CA is based on the presence of diffuse myocardial uptake of Tc-99m PYP.
Laboratories that utilize a traditional Anger scintillation camera have the ability to perform both planar and SPECT imaging. Planar imaging has a higher sensitivity for counts, while SPECT offer better spatial resolution. However, cardiac SPECT reconstruction and interpretation can be challenging when there is no myocardial uptake of tracer. In our laboratory, patient positioning in such cases is accomplished using the PYP-avid sternum as a reference point, and a chest SPECT (rather than a cardiac SPECT) reconstruction is performed. Planar images are also quicker to perform and less challenging for some heart failure patients who might find it difficult to lie flat and still for the duration of a SPECT acquisition. For these reasons, we start with planar imaging in all patients.
When planar imaging is performed at one hour, grade 0 uptake in combination with H/CL ratio < 1.2 and grades 2/3 with H/CL ratio > 2 were always associated with negative and positive SPECT, respectively. Thus, SPECT imaging could conceivably be omitted in these patients. However, inter-observer variability is the highest when differentiating planar grades 1 and 2, and discordant planar grades and H/CL ratios are not infrequently encountered (Table 4). There were 16 false positive and 2 false negative H/CL ratios at one hour in this study. Thus, we recommend that both planar and SPECT images be routinely performed at one hour. This approach obviates the need for on-the fly interpretation of planar images, and offers an efficient and consistent protocol for laboratories. Furthermore, in patients with a positive planar scan, SPECT imaging is useful to confirm that the tracer uptake is in fact, in the myocardium and not the ventricular cavities, as was noted in one patient in this study (grade 2, H/CL ratio 1.6).
The H/CL ratio was introduced as a quantitative measure of the avidity of myocardial Tc-99m PYP uptake, to differentiate ATTR CA patients from the occasional AL CA patient with mild Tc-99m PYP uptake13. Prior studies have reported that a H/CL ratio ≥ 1.5 at one hour to be highly specific for ATTR CA. However, making a distinction between ATTR CA and AL CA is one of the most important clinical steps in the diagnostic evaluation of suspected cardiac CA, and is generally effectively done with serum and urine studies to exclude a paraprotein. While a H/CL ≥ 1.5 ratio may improve diagnostic confidence in patients with a positive planar Tc-99m PYP scan and mildly abnormal serum or urine studies due to MGUS or inflammation, physicians are unlikely to rely on a H/CL alone for this critical distinction.
In our study, no patients with a confirmed diagnosis of AL CA had diffuse Tc-99m PYP myocardial uptake on SPECT imaging or ≥ grade 2 uptake or a H/CL ratio ≥ 1.5 on the planar scan. However, less severe degrees of abnormality were seen on the planar scan as shown in Table 5. Conversely, among the eight patients with diffuse uptake of Tc-99m PYP on SPECT and abnormal serum testing, none had a final diagnosis of AL CA after hematology workup. However, with the high prevalence of MGUS in the elderly populations usually referred for Tc-99m PYP testing with suspected wild-type ATTR, endomyocardial biopsies may be required in some patients for definitive typing of amyloid.14–18.
Two patients with less common mutations had discordant test results, one with Thr60Ala mutation had only regional uptake of Tc-99m PYP on SPECT (one-hour grade 2, H/CL ratio 1.5), while another with Phe64Leu mutation had grade 2 uptake at one-hour but no Tc-99m PYP uptake on SPECT imaging (and no classic features of CA on cardiac magnetic resonance imaging). Two types of ATTR fibrils have been demonstrated in variant ATTR amyloidosis and the type of fibril may affect the sensitivity of scintigraphic testing with bone tracers. Type A fibrils are composed of full-length and N-terminal TTR fragments, while Type B is made of full-length TTR only. In the V30M mutation which has been studied extensively, patients with Type B fibrils and morphological evidence of cardiac involvement did not show myocardial uptake of Tc-99m-3,3-diphosphono-1,2-propanodicarboxylicacid (DPD)19. Such differences in tracer uptake based on fibril type have not been reported in the Tc-99m PYP literature, but also have not been systematically studied. Type A fibrils appear to be the standard in wild type ATTR20. There are anecdotal reports of other TTR mutations showing unexpected scintigraphic results13.
Study Limitations:
Tissue biopsy was not required in most patients, reflecting contemporary clinical practice and thus, was not generally available as a comparator standard. Only 63% of the patients had serum and urine workup for AL amyloidosis, performed at the discretion of the referring physician. However, the objective of the study was not to determine diagnostic performance of Tc-99m PYP against a comparator standard, but rather to determine whether three-hour imaging is necessary when planar and SPECT are performed at one hour.
Conclusion.
An efficient one-hour Tc-99m PYP planar and SPECT protocol had comparable diagnostic performance to a three-hour protocol.
Clinical Perspective.
Technetium 99m pyrophosphate (Tc-99m PYP) scintigraphy is highly accurate for the diagnosis of transthyretin cardiac amyloidosis. We investigated if imaging at one hour with superior efficiency had comparable diagnostic accuracy as three-hour imaging. We found that one-hour Tc-99m PYP single-photon emission computerized tomography (SPECT) imaging had identical diagnostic accuracy to three-hour SPECT imaging. SPECT imaging should be always utilized for patients with semiquantitative visual grade I or II and H/CL ratio between 1.3–1.9. Our findings support the standardization of Tc-99m PYP scintigraphy to one-hour imaging protocol. Adopting a uniform one-hour protocol is more efficient, cost-saving, and does not compromise the diagnostic accuracy of the test.
Funding.
This work is supported by the National Institute of Health grant T32HL129964-02 (AM).
Footnotes
Disclosures: Prem Soman serves on the advisory board of Alnylam Pharmaceuticals, and is the principal investigator of a grant from Astellas Pharmaceuticals to the University of Pittsburgh.
References
- 1.Gillmore JD, Maurer MS, Falk RH, Merlini G, Damy T, Dispenzieri A, Wechalekar AD, Berk JL, Quarta CC, Grogan M, et al. Nonbiopsy Diagnosis of Cardiac Transthyretin Amyloidosis. Circulation. 2016;133:2404–12. [DOI] [PubMed] [Google Scholar]
- 2.Gonzalez-Lopez E, Gallego-Delgado M, Guzzo-Merello G, de Haro-Del Moral FJ, Cobo-Marcos M, Robles C, Bornstein B, Salas C, Lara-Pezzi E, Alonso-Pulpon L, et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J. 2015;36:2585–94. [DOI] [PubMed] [Google Scholar]
- 3.Castano A, Narotsky DL, Hamid N, Khalique OK, Morgenstern R, DeLuca A, Rubin J, Chiuzan C, Nazif T, Vahl T, et al. Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. Eur Heart J. 2017;38:2879–2887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cavalcante JL, Rijal S, Abdelkarim I, Althouse AD, Sharbaugh MS, Fridman Y, Soman P, Forman DE, Schindler JT, Gleason TG, et al. Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. J Cardiovasc Magn Reson. 2017;19:98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sperry BW, Jones BM, Vranian MN, Hanna M and Jaber WA. Recognizing Transthyretin Cardiac Amyloidosis in Patients With Aortic Stenosis: Impact on Prognosis. JACC Cardiovasc Imaging. 2016;9:904–6. [DOI] [PubMed] [Google Scholar]
- 6.Treibel TA, Fontana M, Gilbertson JA, Castelletti S, White SK, Scully PR, Roberts N, Hutt DF, Rowczenio DM, Whelan CJ, et al. Occult Transthyretin Cardiac Amyloid in Severe Calcific Aortic Stenosis. Circ Cardiovasc Imaging. 2016;9:e005066. [DOI] [PubMed] [Google Scholar]
- 7.Harb SC, Haq M, Flood K, Guerrieri A, Passerell W, Jaber WA and Miller EJ. National patterns in imaging utilization for diagnosis of cardiac amyloidosis: A focus on Tc99m-pyrophosphate scintigraphy. J Nucl Cardiol. 2017;24:1094–1097. [DOI] [PubMed] [Google Scholar]
- 8.Harb SC, Haq M, Flood K, Guerrieri A, Passerell W, Jaber WA and Miller EJ. National patterns in imaging utilization for diagnosis of cardiac amyloidosis: A focus on Tc99m-pyrophosphate scintigraphy. J Nucl Cardiol. 2017;24:1094–1097 [DOI] [PubMed] [Google Scholar]
- 9.ASNC Practice Points: 99mTechnetium-Pyrophosphate Imaging for Transthyretin Cardiac Amyloidosis. The American Society of Nuclear Cardiology website. http://www.asnc.org/Files/Practice%20Resources/Practice%20Points/ASNC%20Practice%20Point-99mTechnetiumPyrophosphateImaging2016.pdf. February 2016. Accessed January 7, 2020.
- 10.ASNC Practice Points: 99mTechnetium-Pyrophosphate Imaging for Transthyretin Cardiac Amyloidosis. The American Society of Nuclear Cardiology website. https://www.asnc.org/content.asp?contentid=182. February 27, 2019. Accessed January 7, 2020.
- 11.Dorbala S, Ando Y, Bokhari S, Dispenzieri A, Falk RH, Ferrari VA, Fontana M, Gheysens O, Gillmore JD, Glaudemans A, et al. ASNC/AHA/ASE/EANM/HFSA/ISA/SCMR/SNMMI expert consensus recommendations for multimodality imaging in cardiac amyloidosis: Part 1 of 2-evidence base and standardized methods of imaging. J Nucl Cardiol. 2019;26:2065–2123. [DOI] [PubMed] [Google Scholar]
- 12.Perugini E, Guidalotti PL, Salvi F, Cooke RM, Pettinato C, Riva L, Leone O, Farsad M, Ciliberti P, Bacchi-Reggiani L, et al. Noninvasive etiologic diagnosis of cardiac amyloidosis using 99mTc-3,3-diphosphono-1,2-propanodicarboxylic acid scintigraphy. J Am Coll Cardiol. 2005;46:1076–84. [DOI] [PubMed] [Google Scholar]
- 13.Bokhari S, Castano A, Pozniakoff T, Deslisle S, Latif F and Maurer MS. (99m)Tc-pyrophosphate scintigraphy for differentiating light-chain cardiac amyloidosis from the transthyretin-related familial and senile cardiac amyloidoses. Circ Cardiovasc Imaging. 2013;6:195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Phull P, Sanchorawala V, Connors LH, Doros G, Ruberg FL, Berk JL and Sarosiek S. Monoclonal gammopathy of undetermined significance in systemic transthyretin amyloidosis (ATTR). Amyloid. 2018;25:62–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Wadhera RK and Rajkumar SV. Prevalence of monoclonal gammopathy of undetermined significance: a systematic review. Mayo Clin Proc. 2010;85:933–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Geller HI, Singh A, Mirto TM, Padera R, Mitchell R, Laubach JP and Falk RH. Prevalence of Monoclonal Gammopathy in Wild-Type Transthyretin Amyloidosis. Mayo Clin Proc. 2017;92:1800–1805. [DOI] [PubMed] [Google Scholar]
- 17.Katzmann JA, Abraham RS, Dispenzieri A, Lust JA and Kyle RA. Diagnostic performance of quantitative kappa and lambda free light chain assays in clinical practice. Clin Chem. 2005;51:878–81. [DOI] [PubMed] [Google Scholar]
- 18.Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, Mateos MV, Kumar S, Hillengass J, Kastritis E, Richardson P, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15:e538–48. [DOI] [PubMed] [Google Scholar]
- 19.Pilebro B, Suhr OB, Naslund U, Westermark P, Lindqvist P and Sundstrom T. (99m)Tc-DPD uptake reflects amyloid fibril composition in hereditary transthyretin amyloidosis. Ups J Med Sci. 2016;121:17–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ihse E, Rapezzi C, Merlini G, Benson MD, Ando Y, Suhr OB, Ikeda S, Lavatelli F, Obici L, Quarta CC, et al. Amyloid fibrils containing fragmented ATTR may be the standard fibril composition in ATTR amyloidosis. Amyloid. 2013;20:142–50. [DOI] [PubMed] [Google Scholar]