

ABSTRACT
Background: The ICD-11 classifies posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) as two distinct diagnoses. Few studies have tested the validity of ICD-11 CPTSD in non-Western settings, particularly in Asia.
Objective: This study assessed the factorial, concurrent, and discriminant validity of CPTSD symptoms with four samples of young adults from mainland China, Hong Kong, Japan, and Taiwan.
Method: Young adults aged 18–24 years were recruited by convenience sampling and provided their data anonymously online. Study measures included the International Trauma Questionnaire (ITQ) to measure PTSD and CPTSD, and measures of childhood adversity, depression, anxiety, age, and sex. Confirmatory factor analysis (CFA) was performed for each sample to evaluate the validity of two CPTSD measurement models. Structural equation modelling (SEM) was used to determine the multivariate associations between study variables for the full sample.
Results: A total of 1,346 young adults completed the survey. CFA showed both models of CPTSD examined fit the data well across all four samples. SEM findings showed that number of childhood adversities significantly associated with both PTSD and CPTSD factors; depression significantly associated with CPTSD factors but not PTSD, whereas anxiety significantly associated with both.
Conclusions: Study findings provide evidence for PTSD and CPTSD as separate and valid diagnoses in Asia. More cross-cultural comparisons are needed to understand whether risks for either condition differ by geographical or sociocultural norms.
KEYWORDS: Posttraumatic Stress Disorder, Complex Posttraumatic Stress Disorder, ICD-11, International Trauma Questionnaire, Asia, young adults
HIGHLIGHTS: • The ICD-11 proposes PTSD and Complex PTSD (CPTSD) as separate trauma-related diagnoses.• The validity of CPTSD in East Asia was confirmed with a convenient sample of 1346 young adults. • A higher proportion of Asian young adults met diagnostic criteria for CPTSD than PTSD.
Antecedentes: La CIE-11 clasifica el trastorno de estrés postraumático (TEPT) y el trastorno de estrés postraumático complejo (TEPT-C) como dos diagnósticos distintos. Pocos estudios han probado la validez del TEPT-C de la CIE-11 en escenarios no occidentales, particularmente en Asia.
Objetivo: Este estudio evaluó la validez factorial, concurrente y discriminante de los síntomas de TEPT-C de 4 muestras de adultos jóvenes de China continental, Hong Kong, Japón y Taiwán.
Método: Fueron reclutados adultos jóvenes entre 18 y 24 años de edad a través de una muestra por conveniencia y proveyeron sus datos en forma anónima en línea. Las mediciones del estudio incluyeron el Cuestionario Internacional de Trauma (ITQ por sus siglas en inglés) para medir TEPT y TEPT-C y mediciones de adversidad en la infancia, depresión, ansiedad, edad y sexo. Se realizó el análisis factorial confirmatorio (CFA por sus siglas en inglés) para cada muestra para evaluar la validez de los dos modelos de medición de TEPT-C. Se usó el modelado de ecuaciones estructurales (SEM por sus siglas en inglés) para determinar las asociaciones multivariadas entre las variables del estudio para la muestra completa.
Resultados: un total de 1.346 adultos jóvenes completaron la encuesta. La CFA mostró que ambos modelos de TEPT-C examinados se ajustan bien los datos en las cuatro muestras. Los hallazgos del SEM mostraron que el número de adversidades en la infancia se asociaba significativamente tanto con los factores de TEPT y TEPT-C; la depresión se asociaba significativamente para TEPT-C pero no para TEPT; mientras que la ansiedad se asociaba significativamente con ambos.
Conclusiones: los hallazgos del estudio proveen evidencia para TEPT y TEPT-C como dos diagnósticos separados y válidos en Asia. Se necesitan más comparaciones transculturales para comprender si los riesgos de cualquiera de estas condiciones difieren geográficamente o por normas socioculturales.
PALABRAS CLAVE: Trastorno de estrés postraumático, Trastorno de estrés postraumático complejo, CIE-11, Cuestionario Internacional de trauma, Asia, adultos jóvenes
背景: ICD-11将创伤后应激障碍 (PTSD) 和复杂性PTSD (CPTSD) 分为两个不同的诊断。很少有研究考查ICD-11 CPTSD在非西方国家中 (尤其是在亚洲) 的效度。
目标: 本研究使用来自中国大陆, 香港, 日本和台湾的四个年轻人样本评估了CPTSD症状的因素效度, 同期效度和区分效度。
方法: 通过便利抽样招募了18–24岁的年轻人, 并在线收集了他们的匿名数据。研究测量包括测量PTSD和CPTSD的《国际创伤问卷》 (ITQ), 以及对于童年期逆境, 抑郁, 焦虑, 年龄和性别的测量。对每个样本进行验证性因子分析 (CFA), 以评估两个CPTSD测量模型的效度。使用结构方程模型 (SEM) 来确定完整样本研究变量之间的多元相关。
结果: 共有1346名年轻人完成了调查。 CFA表明所考查的CPTSD的两个模型都很好地拟合了四个样本的数据。SEM结果表明, 童年期逆境数量与PTSD和CPTSD因子均显著相关;抑郁与CPTSD因子显著相关, 与PTSD无关;而焦虑与两者均显著相关。
结论: 研究结果为PTSD和CPTSD在亚洲可作为独立, 有效的诊断提供了证据。需要更多的跨文化比较来了解两种状态的风险是否因地理或社会文化规范而不同。
关键词: 创伤后应激障碍, 复杂性创伤后应激障碍, ICD-11, 国际创伤问卷, 亚洲, 年轻人
1. Introduction
The recently published ICD-11 includes two disorders in response to traumatic life events: Posttraumatic Stress Disorder (PTSD) and Complex PTSD (CPTSD). PTSD includes three symptom clusters of re-experiencing of the trauma in the here and now, avoidance of traumatic reminders, and a persistent sense of current threat. CPTSD includes the three PTSD symptom clusters and three additional symptom clusters that are referred to as ‘Disturbances of self-organization’ (DSO). The three DSO clusters include affective dysregulation, negative self-concepts, and disturbances in relationships. The International Trauma Questionnaire (ITQ) (Cloitre et al., 2018) was recently validated, and is the only self-report measure of the ICD-11 symptoms of CPTSD. The ITQ includes 18 items, 12 measuring the six aforementioned symptom clusters, and six measuring functional impairment in relation to the PTSD and DSO symptoms (Cloitre et al., 2018). The existing literature, predominately derived from ‘Western’ samples, indicates that the latent structure of the ITQ can be well represented by two models. One model is a correlated six-factor model distinguishing between the PTSD and DSO symptoms at the first-order level, and the second model is two-factor second-order model where the first order correlations are explained by two second-order factors reflecting PTSD and DSO (see Figure 1) (Hyland et al., 2017b; Karatzias et al., 2017; Shevlin et al., 2018). Recent studies have also demonstrated that, in general, the first-order model seems to have better fit in general population samples (Ben‐Ezra et al., 2018; Shevlin et al., 2017), whereas the second-order model fits better in clinical or highly traumatized samples (Cloitre et al., 2018; Vallières et al., 2018).
Figure 1.
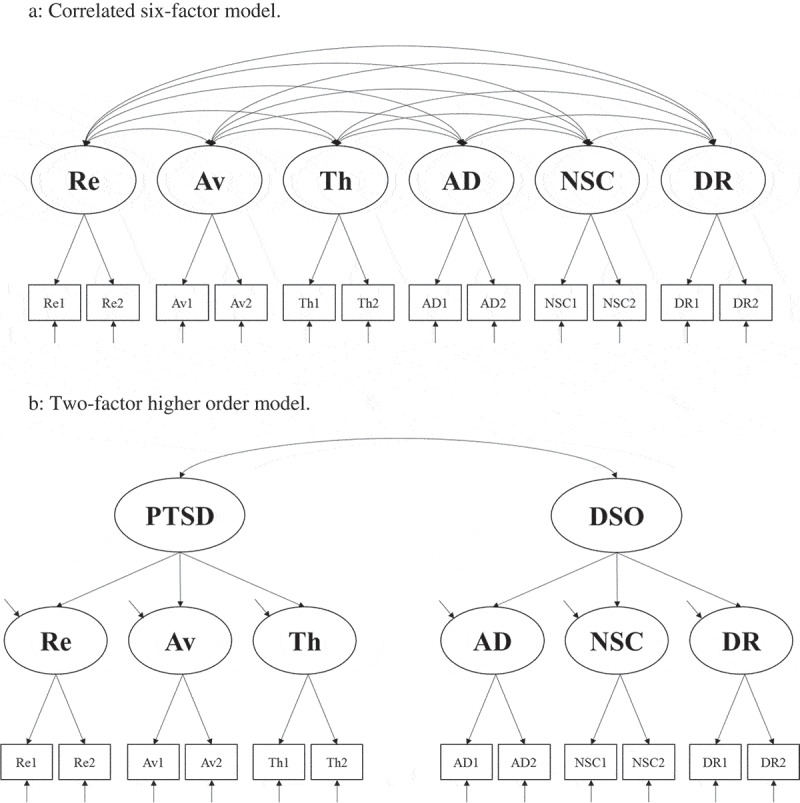
First- and second-order factor models of CPTSD. (a) Correlated six-factor model. (b) Two-factor higher order model.
Re = Re-experiencing; Av = Avoidance; Th = Sense of threat; AD = Affective Dysregulation; NSC = Negative self-concept; DR = Disturbed Relationships; PTSD = Posttraumatic stress disorder; DSO = Disturbances in self-organization.
There is a paucity of research on the latent structure, and overall construct validity, of the ICD-11 model of CPTSD in non-Western settings, particularly in Asia. In a prior study (Ho et al., 2019b), we investigated the latent structure of CPTSD symptoms in a sample of young adults from Hong Kong, and found that both the first- and second-order models fit the data well. In the current study, we set out to assess the factorial, concurrent, and discriminant validity of CPTSD symptoms using the ITQ in three additional samples of young Asian adults drawn from mainland China, Japan, and Taiwan. This study, therefore, represents an important test of whether the latent structure of CPTSD symptoms, as measured by the ITQ, in an Asian context is consistent with previous findings from Europe and North America.
We hypothesized that the factor structure of the ITQ in each of the four Asian samples would be consistent with findings from Western samples, whereby the first- and/or second-order models would provide an acceptable representation of the sample data. Additionally, we examined the concurrent validity of the ITQ by examining the associations between the PTSD and DSO factors with sex, age, cumulative exposure to childhood adversities, depression, and anxiety using structural equation modelling (SEM). Consistent with findings from Western samples (Cloitre, Hyland, & Bisson et al., 2019; Hyland et al., 2017b), we hypothesized that (a) exposure to a higher number of childhood adversities would be positively, and similarly strongly, associated with the PTSD and DSO factors (at the first- and/or second-order levels); (b) the DSO factor(s) would be positively associated with depression whereas the PTSD factor(s) would not be; and (c) the PTSD and DSO factors would be positively associated with anxiety, but the magnitude of these associations would be stronger for the PTSD factor(s) than the DSO factor(s).
2. Methods
2.1. Participants and procedures
Participants were recruited from two government-funded universities in Hong Kong, and four national universities in other sites (i.e. one in China, two in Taiwan, and one in Japan). Ethical approval of this study were obtained from The Hong Kong Polytechnic University, National Chengchi University, and Okayama Prefectural University. Participants were eligible if they were aged 18–24 years, and enrolled into a full-time undergraduate degree programme. All participants were recruited between April 2017 and July 2018 by convenience sampling through distributing flyers across campuses and through mass emails, or publicizing in student social media networks and invitations in class. Those who were interested in participating were directed to the webpage of this survey, and data were collected using MySurvey v1.1 (The Hong Kong Polytechnic University, 2016). The study purpose, procedures, and rights as research participants were stated in full in the survey landing page. Participants provided implied consent to complete the survey anonymously, which is a common practice to reduce risks for confidentiality breach in online surveys (Jacobson, 1999). The study website was set to allow one-time entry per electronic device to prevent repeated/multiple entries by the same respondent. All participants completed the survey anonymously. No direct incentives were given, however participants in Hong Kong could provide their contact information if they wished to be included in a lucky draw to win an electronic tablet; this information was stored separate from their survey responses. The average time to complete the survey was 27 minutes.
In total, there were 2,465 clicks into the survey webpage and 1,346 provided responses (i.e. a completion rate of 54.6%). From this total sample, 428 (31.80%) were from Hong Kong, 340 (25.56%) were from China, 254 (18.87%) were from Taiwan, and 324 (24.07%) were from Japan. There was minimal missing data (< 1%) present across the entire sample, which was not missing completely at random (Little’s MCAR test: Chi-square = 1048.44, df = 667, p < 0.001). Therefore, listwise deletion was not appropriate and missing values were imputed using mean/mode substitution given the negligible amount of missing data (Saunders et al., 2006). Demographic information for the four samples is presented in Table 1. The mean age of participants in the combined sample was 20 years (Mdn = 20.0, SD = 1.55), and 67.9% were female.
Table 1.
Frequency of exposure to childhood adversity and PTSD/CPTSD diagnostic rates in each sample and the total sample.
| Variables | Hong
Kong (n = 428) |
China (n = 340) |
Taiwan (n = 254) |
Japan (n = 324) |
Total
Sample (n = 1346) |
|---|---|---|---|---|---|
| Age (mean, SD) | 20.16 (1.66) | 20.54 (1.55) | 19.87 (1.44) | 19.34 (1.19) | 20.00 (1.55) |
| Female (n,%) | 252 (58.88) | 235 (69.12) | 200 (78.74) | 227 (70.06) | 914 (67.90) |
| Number of childhood adversities (n,%) | |||||
| 0 | 109 (25.47) | 125 (36.76) | 62 (24.41) | 158 (48.77) | 454 (33.73) |
| 1 | 122 (28.50) | 103 (30.29) | 85 (33.46) | 71 (21.91) | 381 (28.31) |
| 2 | 63 (14.72) | 54 (15.88) | 42 (16.54) | 45 (13.89) | 204 (15.16) |
| 3 | 54 (12.62) | 32 (9.41) | 24 (9.45) | 21 (6.48) | 131 (9.73) |
| 4 | 51 (11.92) | 10 (2.94) | 17 (6.69) | 16 (4.94) | 94 (6.98) |
| 5 | 15 (3.50) | 9 (2.65) | 13 (5.12) | 8 (2.47) | 45 (3.34) |
| 6 | 9 (2.10) | 3 (0.88) | 9 (3.54) | 2 (0.62) | 23 (1.71) |
| 7 or more | 5 (0.96) | 4 (1.18) | 2 (0.79) | 1 (0.31) | 14 (1.04) |
| PTSD diagnosis (n,%) | 15 (3.50) | 3 (0.88) | 4 (1.57) | 4 (1.23) | 26 (1.93) |
| CPTSD diagnosis (n,%) | 26 (6.07) | 3 (0.88) | 11 (4.33) | 9 (2.78) | 49 (3.64) |
2.2. Study measures
PTSD and DSO symptoms were measured using the ITQ (Cloitre et al., 2018). Each PTSD and DSO symptom cluster was measured using two items scored on a five-point Likert scale from 0 (‘Not at all’) to 4 (‘Extremely’). The PTSD symptoms are answered in terms of how much a respondent has been bothered by that symptom over the past month, and the DSO symptoms are answered in terms of how one typically responds. Diagnostic criteria for PTSD requires (a) a score of ≥ 2 (‘Moderately’) for at least one of the two items from each symptom cluster (Re-experiencing, Avoidance, and Sense of Threat), and (b) endorsement of at least one item on functional impairment. Diagnostic criteria for CPTSD requires (a) that the criteria for PTSD are met, (b) a score of ≥ 2 for at least one of the two items from each DSO symptom cluster (Affective Dysregulation, Negative Self-Concept, and Disturbed Relationships), and (c) endorsement of at least one item on functional impairment associated with these symptoms. Based on the diagnostic principles of the ICD-11, a person may be diagnosed with PTSD or CPTSD, but not both (World Health Organization, 2018).
Results of the Chinese translation and initial validation of the ITQ are available elsewhere (Ho et al., 2019b). The Japanese version followed forward and backward translation protocols as per WHO guidelines (World Health Organization, 2017). The internal consistencies of the PTSD and DSO items for the full sample were good (α = 0.87 and α = 0.89, respectively), and ranged from 0.84–0.89 and 0.86–0.90 across the four samples. The traditional Chinese, simplified Chinese, and Japanese versions of the ITQ are attached in the appendix of this paper. More information about the ITQ and its translations into other languages are available at www.traumameasuresglobal.com.
Exposure to childhood adversities was measured using the 29-item WHO Adverse Childhood Experiences – International Questionnaire (ACE-IQ) (World Health Organization, 2016), which assesses exposure to 13 categories of childhood adversities. These include physical abuse; sexual abuse; emotional abuse; physical neglect; emotional neglect; domestic violence; household member with mental illness; household member imprisonment; household member who was a substance abuser; parental separation or death, bullying, community violence; and collective violence. Endorsement of these 13 categories were summed to generate a total number of childhood adversities. Results of the Chinese translation and initial validation of the ACE-IQ are reported elsewhere (Ho, Chan, Chien, Bressington, & Karatzias, 2019a). The Japanese version followed forward and backward translation protocols as per WHO guidelines (World Health Organization, 2017).
Depression and anxiety symptoms were measured using the 14-item Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983). Depression and anxiety were each measured using seven items. Each item was scored on a four-point Likert scale with higher scores indicating greater distress. Prior evaluations of the Chinese and Japanese versions have demonstrated sound psychometric properties and support of the two-factor model (i.e. anxiety and depression) (Chan, Leung, Fong, Leung, & Lee, 2010; Matsudaira et al., 2009). The internal consistencies of the depression and anxiety subscales were acceptable for the four samples in this study (α = 0.67–0.75 and α = 0.77–0.84, respectively).
2.3. Statistical analysis
The analytical strategy included three elements. First, the age, gender, total number of childhood adversities, and proportions of individuals meeting caseness for ICD-11 PTSD and CPTSD were assessed in each sample, and in the total sample. Second, the two measurement models of CPTSD (i.e. the correlated six-factor first-order model and the two-factor second-order model; see Figure 1) were tested using confirmatory factor analysis (CFA). The mean and variance-adjusted weighted least squares estimator was used as it provides accurate parameter estimates, standard errors, and test statistics for ordinal indicators (Flora & Curran, 2004). The factorability of the 12 ITQ items was good (Kaiser-Meyer-Olkin measure of sampling adequacy was 0.88; Bartlett’s test of sphericity was significant, i.e. (χ2 (66) = 9830.51, p < .01). Third, the four samples were combined and SEM was used to determine the multivariate associations between the CPTSD factors (as per both factorial models), and sex (0 = males, 1 = females), age, total number of childhood adversities, levels of depression, and levels of anxiety. Anxiety and depression were added to the model as latent variables; age, gender, and number of childhood adversities were added to the model as observed variables. The CFA and SEM analyses were performed in Mplus 7.4 (Muthén & Muthén, 2013) and standard guidelines for determining model fit were followed (see Bollen, 1989; Hu & Bentler, 1999). Acceptable model fit was indicated by a non-significant chi-square (χ2) result; Comparative Fit Index (CFI) and Tucker-Lewis Index (TLI) values ≥ .90 and ≥ .95 reflecting acceptable and excellent model fit, respectively; and Root Mean Square Error of Approximation (RMSEA) values, with 90% confidence intervals, ≤ .08 and ≤ .06 reflecting acceptable and excellent model fit, respectively. The two CFA models were compared based on the change in the RMSEA value (ΔRMSEA), wherein values of ≥ .015 suggest a meaningful difference in fit (Chen, 2007).
3. Results
3.1. Descriptive statistics
Participant age and gender, as well as rates of childhood adversities and PTSD and CPTSD caseness are presented in Table 1 for all four samples and the combined sample. The Taiwanese sample had the highest proportion of female participants (78.7%). The Hong Kong sample had the highest number of people meeting caseness for ICD-11 PTSD and CPTSD (9.6%, n = 41), and the mainland China sample had the fewest cases (1.8%, n = 6). In the Hong Kong, Taiwanese, and Japanese samples, more people met the diagnostic criteria for CPTSD than PTSD, whereas an equal number of people met the criteria for PTSD and CPTSD in the China sample.
3.2. CFA results
The CFA results are reported in Table 2. The first- and second-order models provided acceptable fit in all samples with the exception of the first-order model in the Taiwanese sample which included a correlation of 1.002 between Affective Dysregulation and Disturbed Relationships, indicating a misspecification of the model. All χ2 results were statistically significant, but Tanaka (1987) warned against rejecting models on this basis because Type-1 errors increase with larger sample sizes. The CFI and TLI results indicated that both models provided a close fit to the data in every sample, and the RMSEA results indicated acceptable fit for both models across all samples. The first-order model was statistically superior to the second-order model in the Hong Kong sample (ΔRMSEA = .022) but no meaningful differences were observed in the China and Japan samples. On the basis of these results, the second-order model was favoured in the Taiwan sample, the first-order model was favoured in the Hong Kong sample, while both models were viable in the China and Japan samples.
Table 2.
Fit statistics based on the ITQ in the four Asian samples and the total sample.
| Sample | χ2 | CFI | TLI | RMSEA (90% CI) | ΔRMSEA |
|---|---|---|---|---|---|
| Hong Kong (n = 428) | |||||
| First-order model | 87.832* | .996 | .994 | .054 (.039-.069) | |
| Second-order model | 161.746* | .991 | .987 | .076 (.063-.088) | .022 |
| China (n = 340) | |||||
| First-order model | 111.599* | .988 | .980 | .074 (.058-.090) | |
| Second-order model | 148.560* | .984 | .977 | .080 (.065-.094) | .006 |
| Taiwan (n = 254) | |||||
| First-order model^ | 65.457* | .997 | .995 | .052 (.028-.073) | |
| Second-order model | 99.666* | .994 | .992 | .066 (.048-.085) | .014 |
| Japan (n = 324) | |||||
| First-order model | 85.832* | .994 | .990 | .061 (.043-.078) | |
| Second-order model | 106.036* | .993 | .990 | .062 (.047-.078) | .001 |
| Full sample (n = 1346) | |||||
| First-order model | 157.495* | .996 | .994 | .048 (.040-.055) | |
| Second-order model | 456.445* | .987 | .982 | .080 (.074-.087) | .032 |
*p < .001; χ2 = chi-square test (all first-order model have 39 degrees of freedom and all second-order model have 47 degrees of freedom); CFI = comparative fit indices; TLI = Tucker Lewis indices; RMSEA (90% CI) = Root mean square of approximation (90% confidence intervals); ΔRMSEA = change in the RMSEA between the two models; ^correlation of 1.002 between Affective Dysregulation and Disturbed Relationships.
The parameters of the different models are available in Supplementary Table 1. All factor loadings in each sample were positive, high, and statistically significant (ps < .001). In relation to the first-order models, the correlations between the factors were all statistically significant (p < .001) and moderate-to-strong (Hong Kong, r values ranged from .49 to .89; China, r values ranged from .53 to .91; and Japan, r values ranged from .56 to .83). In relation to the second-order model, the correlations between PTSD and DSO were statistically significant (p < .001) and strong (Hong Kong, r = .79; China, r = .79; Taiwan, r = .71; and Japan, r = .82).
The four datasets were combined and the two models were tested using the full sample (see Table 2). Both models provided satisfactory model fit, however, the first-order model was statistically superior to second-order model (ΔRMSEA = .032). The factor loadings and factor correlations for both models were satisfactory. All factors loadings were positive, statistically significant (p < .001), and high (see Supplementary Table 1); and the factor correlations at the first-order level ranged from .48 to .84, and the correlation between the second-order factors was .78.
3.3. SEM results
The results of the SEM analyses are presented in Table 3. The SEM model based on the correlated six-factor model of CPTSD fit the data well (χ2 (331) = 1619.44, p < .001; CFI = .965; TLI = .957; RMSEA = .055 [90% CI = .053-.058]). The six CPTSD factors were positively and significantly associated with childhood adversities (β’s ranged from .25 to .43). Depression was significantly and positively associated with the negative self-concepts (β = .30) and disturbed relationships (β = .33), and significantly and negatively associated with sense of threat symptoms (β = −.23). The six CPTSD factors were also significantly and positively associated with anxiety, and the strongest association was with sense of threat symptoms (β = .71). Gender was not significantly associated with any of the CPTSD factors, while age was significantly, positively, and weakly associated with re-experiencing, avoidance, and affective dysregulation (all β’s = .09).
Table 3.
Standardized regression effects (standard errors) derived from the structural equation modelling results for the full sample (n = 1,346).
| Gender | Age | Childhood Adversities | Depression | Anxiety | |
|---|---|---|---|---|---|
| First-order model | |||||
| Re-experiencing | −.03 (.03) | .09 (.03)** | .34 (.03)*** | −.09 (0.07) | .51 (.06)*** |
| Avoidance | .01 (.03) | .09 (.03)** | .34 (.03)*** | .01 (.07) | .41 (.06)*** |
| Sense of threat | −.05 (.03) | .01 (.03) | .33 (.03)*** | −.23 (.07)** | .71 (.06)*** |
| Affective dysregulation | −.01 (.03) | .09 (.03)** | .43 (.03)*** | .06 (.07) | .53 (.06)*** |
| Negative self-concept | −.02 (.03) | −.02 (.03) | .25 (.03)*** | .30 (.06)*** | .31 (.05)*** |
| Disturbed relationships | −.01 (.03) | .00 (.03) | .28 (.03)*** | .33 (.06)*** | .21 (.06)** |
| Second-order model | |||||
| PTSD | −.03 (.03) | .07 (.03)* | .39 (.03)*** | −.12 (.06) | .63 (.06)*** |
| DSO | −.02 (.03) | .02 (.03) | .34 (.03)*** | .27 (.06)*** | .37 (.05)*** |
Statistical significance: *p < .05, **p < .01, ***p < .001.
The SEM model based on the two-factor second-order model of CPTSD also fit the data well (χ2 (359) = 1947.65, p < .001; CFI = .959; TLI = .954; RMSEA = .057 [90% CI = .055-.060]). The ΔRMSEA (.002) indicated no meaningful difference between the two structural models. The PTSD (β = .39) and DSO (β = .34) factors were positively associated with childhood adversities. DSO (β = .27), but not PTSD, was significantly associated with depression, while PTSD (β = .63) and DSO (β = .37) were significantly associated with anxiety. Gender was not associated with PTSD or DSO, and age was significantly associated with PTSD (β = .07) but not DSO.
4. Discussion
The present findings are largely consistently with prior work conducted in Western contexts (Cloitre et al., 2018; Hyland et al., 2017b; Karatzias et al., 2017; Shevlin et al., 2018), supporting the validity of the ICD-11 model CPTSD in an Asian context. Specifically, the CFA results demonstrated that across the four samples, the first- and second-order models of CPTSD symptoms fit the respective sample data well (with the exception of the first-order model in the Taiwanese sample where one factor correlation was outside the acceptable boundary). Additionally, the results largely point to a better model fit for the first-order model, which is consistent with work conducted elsewhere using general population and non-clinical samples (Ben‐Ezra et al., 2018; Shevlin et al., 2017), and a recent study of combat-exposed soldiers in the Philippines (Mordeno, Nalipay, & Mordeno, 2019). These results indicate that the ITQ is valid measure of CPTSD symptoms in East Asia, and by extension, that the ICD-11 model of CPTSD appears to manifest in the same way in Asia as it does in Western settings. Given that a primary goal of the ICD-11 was to produce diagnostic categories that have international applicability (World Health Organization, 2018), these findings represent important empirical support of the WHO’s efforts. Despite the convenience nature of the student samples, our rate of participants meeting criteria for either trauma diagnosis (5.6%) was comparable to those found in the World Mental Health Surveys (WMHS) of 5% (Koenen et al., 2017). The low rates of PTSD and CPTSD from mainland China (1.7%) were a little bit higher than, but still reasonably consistent with, the WMHS results from China (0.3%).
Contrary to previous studies using nationally representative samples in the United States, where rates of CPTSD were comparable to PTSD (Cloitre et al., 2019), and in Israel, where rates of PTSD were higher than CPTSD (Ben‐Ezra et al., 2018), our findings indicated that a higher proportion of Asian young adults met criteria for CPTSD (3.6%) than PTSD (1.9%). Two potential explanations are offered. First, nearly half of the total sample (46.0%) reported two or more childhood adversities, and given that exposure to multiple, distinct types of childhood trauma is a well-established risk factor for CPTSD (Hyland et al., 2017a; World Health Organization, 2018), the higher rates of CPTSD may be attributable to this fact. Indeed, in a highly traumatized community sample of adults from the United Kingdom, CPTSD was more common than PTSD (Cloitre et al., 2018). Therefore, it may be the case that CPTSD is the more common diagnosis in community samples characterized by higher rates of childhood trauma/adversity. Further, our young adult university student sample may have imparted additional age-related effects, as some evidence suggests CPTSD is independently associated with younger age in trauma-exposed samples (Karatzias et al., 2019a). Alternatively, it is possible that DSO symptoms are more commonly endorsed in East Asian cultures regardless of PTSD presentation, which may lead to a higher potential for meeting CPTSD diagnosis. For example, East Asian cultural norms of modesty, humility, and emotional restraint (Park, Streamer, Huang, & Galinsky, 2013) may influence responses to DSO items related to negative self-concept (e.g. ‘I feel worthless’) or disturbances in relationships (e.g. ‘I feel distant or cut off from people.’) In fact, prior studies have shown that East Asians have higher tendencies to agree with negative self-statements compared with their Western counterparts (Kim, Peng, & Chiu, 2008). Taken together, while our results provide novel evidence supporting the ICD-11 model of CPTSD in the Asian context, more research with nationally representative and clinical samples is needed to confidently determine the validity of this model in Asia.
The associations between the PTSD and DSO factors with childhood adversities were, as hypothesized, consistent with similar findings from Western contexts. For example, exposure to more childhood adversities was positively associated with all PTSD and DSO factors (Karatzias et al., 2017), and the magnitude of these associations were similar (Cloitre et al., 2018). Additionally, the associations between the PTSD and DSO factors with the depression and anxiety factors were also consistent with prior findings, whereby depression was positively associated with DSO symptoms but not PTSD symptoms, and anxiety was positively associated with both PTSD and DSO symptoms but more strongly with the former (Hyland et al., 2017b). These findings are important as they show that PTSD and DSO symptoms, while strongly associated with one another, are differentially related to two clinically relevant exogenous variables, and support recent discussions on how PTSD and DSO symptoms likely require different clinical interventions and treatment approaches (Karatzias & Cloitre, 2019; Karatzias et al., 2019b). Lastly, gender was not associated with any of the CPTSD factors, and this contradicts with prior reviews supporting biological and behavioural sex differences that heighten risk for PTSD in females (Olff, 2017), and ICD-11 related finding from Western samples (e.g. Cloitre et al., 2019). However, some studies have shown that sex differences in PTSD are not yet established in childhood and adolescence and only become evident in adulthood (Contractor et al., 2013; Kilpatrick et al., 2003; Tolin & Foa, 2006). More research is needed on possible sex differences in relation to CPTSD symptoms across cultures and along the age spectrum.
Several study limitations should be acknowledged. First, the convenience and age-restricted nature of our student sample precludes generalizing our findings to the larger East Asian population. For example, tertiary education enrolment only reach approximately half of the population in Hong Kong, Taiwan, and Japan, and the rate is likely much lower in mainland China (Marginson, 2011). Further, only 54.6% of participants who entered the webpage completed the survey, and proportionately more participants were females than males; it is not clear whether non-completers were characteristically different from those who completed the survey. Second, the instruments used in the Japanese sample did not undergo formal psychometric evaluation prior to this study. Lastly, our measure of childhood adversity encompassed a wide spectrum of different negative experiences, some of which may not necessarily be traumatic for the respondents.
In conclusion, this study provides initial and tentative support for the validity of the ICD-11 model of CPTSD in an Asian context, and indicates that the ITQ is a reliable and valid measure of these symptoms among young Asian adults. Clinicians and researchers may be confident that the ITQ effectively captures both the PTSD and DSO symptoms that comprise the CPTSD diagnosis. The CFA findings indicate that researchers and clinicians may score the ITQ in two ways, depending on their research and clinical needs. These are to either construct scores for the six CPTSD symptom clusters (re-experiencing, avoidance, sense of threat, affect dysregulation, negative self-concepts, and disturbed relationships) in line with the first-order model, or, to construct scores for the PTSD (re-experiencing, avoidance, and threat) and DSO (affect dysregulation, negative self-concepts, and disturbed relationships) symptoms, in line with the second-order model. The findings of this study in Asia have replicated those from multiple Western studies with clinical and community samples, and thus provide novel evidence in support of the validity of the ITQ, and by extension, the ICD-11 model of CPTSD.
Funding Statement
This study was supported by The Hong Kong Polytechnic University Internal Start-Up Fund [1-ZE7A].
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Disclosure statement
No potential conflict of interest was reported by the authors.
Ethics approval and consent to participate
This study received ethics approval and consent from the Human Subjects Ethics Application Review System from The Hong Kong Polytechnic University
Supplementary material
Supplemental data for this article can be accessed here.
References
- Ben‐Ezra, M., Karatzias, T., Hyland, P., Brewin, C. R., Cloitre, M., Bisson, J. I., … Shevlin, M. (2018). Posttraumatic stress disorder (PTSD) and complex PTSD (CPTSD) as per ICD‐11 proposals: A population study in Israel. Depression and Anxiety, 35, 264–9. [DOI] [PubMed] [Google Scholar]
- Bollen, K. A. (1989). Structural equations with latent variables. New York, NY: John Wiley. [Google Scholar]
- Chan, Y. F., Leung, D. Y., Fong, D. Y., Leung, C.-M., & Lee, A. M. (2010). Psychometric evaluation of the hospital anxiety and depression scale in a large community sample of adolescents in Hong Kong. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 19, 865–873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen, F. F. (2007). Sensitivity of Goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal, 14, 464–504. [Google Scholar]
- Cloitre, M., Hyland, P., Bisson, J. I., Brewin, C. R., Roberts, N., Karatzias, T., & Shevlin, M. (2019). ICD-11 PTSD and complex PTSD in the United States: A population-based study. Journal of Traumatic Stress. [DOI] [PubMed] [Google Scholar]
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., … Hyland, P. (2018). The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138, 536–546. [DOI] [PubMed] [Google Scholar]
- Contractor, A. A., Layne, C. M., Steinberg, A. M., Ostrowski, S. A., Ford, J. D., & Elhai, J. D. (2013). Do gender and age moderate the symptom structure of PTSD? Findings from a national clinical sample of children and adolescents. Psychiatry Research, 210, 1056–1064. [DOI] [PubMed] [Google Scholar]
- Flora, D. B., & Curran, P. J. (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9(4), 466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ho, G. W. K., Chan, A. C. Y., Chien, W.-T., Bressington, D. T., & Karatzias, T. (2019a). Examining patterns of adversity in Chinese young adults using the Adverse Childhood Experiences—International Questionnaire (ACE-IQ). Child Abuse & Neglect, 88, 179–188. [DOI] [PubMed] [Google Scholar]
- Ho, G. W. K., Karatzias, T., Cloitre, M., Chan, A. C. Y., Bressington, D., Chien, W. T., … Shevlin, M. (2019b). Translation and validation of the Chinese ICD-11 International Trauma Questionnaire (ITQ) for the Assessment of Posttraumatic Stress Disorder (PTSD) and Complex PTSD (CPTSD). European Journal of Psychotraumatology, 10, 1608718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1––55.. [Google Scholar]
- Hyland, P., Murphy, J., Shevlin, M., Vallières, F., McElroy, E., Elklit, A., … Cloitre, M. (2017a). Variation in post-traumatic response: The role of trauma type in predicting ICD-11 PTSD and CPTSD symptoms. Social Psychiatry and Psychiatric Epidemiology, 52, 727–736. [DOI] [PubMed] [Google Scholar]
- Hyland, P., Shevlin, M., Brewin, C. R., Cloitre, M., Downes, A. J., Jumbe, S., & Roberts, N. P. (2017b). Validation of post-traumatic stress disorder (PTSD) and complex PTSD using the International Trauma Questionnaire. Acta Psychiatrica Scandinavica, 136, 313–322. [DOI] [PubMed] [Google Scholar]
- Jacobson, D. (1999). Doing research in cyberspace. Field Methods, 11, 127–145. [Google Scholar]
- Karatzias, T., & Cloitre, M. (2019). Treating adults with complex posttraumatic stress disorder using a modular approach to treatment: Rationale, evidence, and directions for future research. Journal of Traumatic Stress, 32(6), 870–876. [DOI] [PubMed] [Google Scholar]
- Karatzias, T., Hyland, P., Bradley, A., Cloitre, M., Roberts, N. P., Bisson, J. I., & Shevlin, M. (2019a). Risk factors and comorbidity of ICD-11 PTSD and complex PTSD: Findings from a trauma-exposed population based sample of adults in the United Kingdom. Depression and Anxiety, 36, 887–894. [DOI] [PubMed] [Google Scholar]
- Karatzias, T., Murphy, P., Cloitre, M., Bisson, J., Roberts, N., Shevlin, M., … Hutton, P. (2019b). Psychological interventions for ICD-11 complex PTSD symptoms: Systematic review and meta-analysis. Psychological Medicine, 49, 1761–1775. [DOI] [PubMed] [Google Scholar]
- Karatzias, T., Shevlin, M., Fyvie, C., Hyland, P., Efthymiadou, E., Wilson, D., … Cloitre, M. (2017). Evidence of distinct profiles of posttraumatic stress disorder (PTSD) and complex posttraumatic stress disorder (CPTSD) based on the new ICD-11 trauma questionnaire (ICD-TQ). Journal of Affective Disorders, 207, 181–187. [DOI] [PubMed] [Google Scholar]
- Kilpatrick, D. G., Ruggiero, K. J., Acierno, R., Saunders, B. E., Resnick, H. S., & Best, C. L. (2003). Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: Results from the National Survey of Adolescents. Journal of Consulting and Clinical Psychology, 71, 692. [DOI] [PubMed] [Google Scholar]
- Kim, Y.-H., Peng, S., & Chiu, C.-Y. (2008). Explaining self-esteem differences between Chinese and North Americans: Dialectical self (vs. self-consistency) or lack of positive self-regard. Self and Identity, 7, 113–128. [Google Scholar]
- Koenen, K. C., Ratanatharathorn, A., Ng, L., McLaughlin, K. A., Bromet, E. J., Stein, D. J., & Kessler, R. C. (2017). Posttraumatic stress disorder in the World Mental Health Surveys. Psychological Medicine, 47, 2260–2274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marginson, S. (2011). Higher education in East Asia and Singapore: Rise of the Confucian model. Higher Education, 61, 587–611. [Google Scholar]
- Matsudaira, T., Igarashi, H., Kikuchi, H., Kano, R., Mitoma, H., Ohuchi, K., & Kitamura, T. (2009). Factor structure of the hospital anxiety and depression scale in Japanese psychiatric outpatient and student populations. Health and Quality of Life Outcomes, 7, 42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mordeno, I. G., Nalipay, M. J. N., & Mordeno, E. R. (2019). The factor structure of complex PTSD in combat-exposed Filipino soldiers. Psychiatry Research, 278, 65–69. [DOI] [PubMed] [Google Scholar]
- Muthén, L. K., & Muthén, B. O. (2013). Mplus user's guide. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Olff, M. (2017). Sex and gender differences in post-traumatic stress disorder: An update. European Journal of Psychotraumatology, 8(sup4), 1351204. [Google Scholar]
- Park, L. E., Streamer, L., Huang, L., & Galinsky, A. D. (2013). Stand tall, but don’t put your feet up: Universal and culturally-specific effects of expansive postures on power. Journal of Experimental Social Psychology, 49, 965–971. [Google Scholar]
- Saunders, J. A., Morrow-Howell, N., Spitznagel, E., Dore, P., Proctor, E. K., & Pescarino, R. (2006). Imputing missing data: A comparison of methods for social work researchers. Social Work Research, 30, 19–31. [Google Scholar]
- Shevlin, M., Hyland, P., Karatzias, T., Fyvie, C., Roberts, N., Bisson, J. I., … Cloitre, M. (2017). Alternative models of disorders of traumatic stress based on the new ICD‐11 proposals. Acta Psychiatrica Scandinavica, 135, 419–428. [DOI] [PubMed] [Google Scholar]
- Shevlin, M., Hyland, P., Roberts, N. P., Bisson, J. I., Brewin, C. R., & Cloitre, M. (2018). A psychometric assessment of Disturbances in Self-Organization symptom indicators for ICD-11 complex PTSD using the International Trauma Questionnaire. European Journal of Psychotraumatology, 9(1), 1419749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanaka, J. S. (1987). “How big is big enough?”: Sample size and goodness of fit in structural equation models with latent variables. Child Development, 134–146. [Google Scholar]
- The Hong Kong Polytechnic University . (2016). mySurvey (version 1.1) [software]. Retrieved from https://www.polyu.edu.hk/mysurvey/
- Tolin, D. F., & Foa, E. B. (2006). Sex differences in trauma and posttraumatic stress disorder: A quantitative review of 25 years of research. Psychological Bulletin, 132, 959. [DOI] [PubMed] [Google Scholar]
- Vallières, F., Ceannt, R., Daccache, F., Abou Daher, R., Sleiman, J., Gilmore, B., … Hyland, P. (2018). ICD‐11 PTSD and complex PTSD amongst Syrian refugees in Lebanon: The factor structure and the clinical utility of the International Trauma Questionnaire. Acta Psychiatrica Scandinavica, 138, 547–557. [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2016). Adverse Childhood Experiences International Questionnaire (ACE-IQ). Retrieved from www.who.int/violence_injury_prevention/violence/activities/adverse_childhood_experiences
- World Health Organization . (2017). Process of translation and adaptation of instruments. Retrieved from http://www.who.int/substance_abuse/research_tools/translation/en/
- World Health Organization . (2018). International statistical classification of diseases and related health problems: Eleventh revision. Geneva: Author. [Google Scholar]
- Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361–370. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- The Hong Kong Polytechnic University . (2016). mySurvey (version 1.1) [software]. Retrieved from https://www.polyu.edu.hk/mysurvey/
- World Health Organization . (2016). Adverse Childhood Experiences International Questionnaire (ACE-IQ). Retrieved from www.who.int/violence_injury_prevention/violence/activities/adverse_childhood_experiences
Supplementary Materials
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.