

ABSTRACT
Background: Negative life events are a predictor for mental illness. However, most research has focused on selected domains, e.g. childhood or recent adversity. The Cumulative Lifetime Adversity Measure (CLAM), a newly introduced questionnaire not yet validated, examines cumulative effect of a range of events including number of exposure to the same event. This measure gives opportunity to collect detailed data on lifetime adversity in large cohort studies.
Objective: The aim of this study was translation of the CLAM into Danish and validation of the CLAM in a large general population cohort. Secondly, we aimed to describe the occurrence of adverse life events in a large representative sample of the general population in Denmark.
Methods: Translation and validation followed the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) for formative models. Content and construct validity were evaluated including hypothesis testing of accumulated lifetime adversity having a U-shaped pattern with low levels of cumulated lifetime adversity as opposed to no or high levels being associated with lower emotional distress, functional impairment, and pain impairment. The field testing sample was the DanFunD cohort (n = 7493) randomly drawn in a Danish population and examined between 2012 and 2015.
Results: Pilot interviews showed that the questions were confronting but not offensive, straight forward, and easy to answer. Acceptability was good. U-shaped patterns between accumulated lifetime adversity and the outcome measures were found. Quadratic term: Emotional distress (β(95%CI) 0.007(0.002;0.012), p < 0.007), functional impairment (β(95%CI) −0.002(−0.003;−0.001), p < 0.001), and pain impairment (β(95%CI) 0.004(0.002;0.006), p = 0.001). Field testing provided basic numbers for adverse life events for the Danish general population, with a cumulated lifetime adversity mean (SD), 5.9 (3.7). Compared to the US there were lower rates of violence, social/environmental stress, and disaster.
Conclusions: The results from the original version were replicated, indicating high construct validity. Furthermore, content validity was good.
KEYWORDS: Adverse life events, emotional distress, pain impairment, functional impairment, validation, formative model
HIGHLIGHTS: • Translation of the Cumulative Lifetime Adversity Measure (CLAM) into Danish and validation of the CLAM in a large general population cohort.• Translation and validation followed the COSMIN Standards for formative models.• Compared to the USA there were lower rates of violence, social/environmental stress, and disaster.• This measure gives opportunity to collect detailed data on lifetime adversity in large cohort studies.• Compared to the USA there were lower rates of violence, social/environmental stress, and disaster in Denmark.
Antecedentes: Los eventos vitales negativos son un predictor de trastorno mental. Sin embargo, la mayoría de las investigaciones se han centrado en dominios seleccionados, por ej. infancia o adversidad reciente. La Medida de Adversidad Acumulada a lo Largo de la Vida (CLAM en su sigla en inglés), un cuestionario recientemente introducido que no ha sido validado todavía, examina el efecto acumulado de un rango de eventos, incluyendo el número de exposiciones al mismo evento. Esta medida permite recolectar información detallada sobre la adversidad a lo largo de la vida en estudios de cohorte grandes.
Objetivo: El objetivo de este estudio fue la traducción de la CLAM al idioma danés y la validación de la CLAM en una cohorte grande de población general. En segundo lugar, buscamos describir la ocurrencia de los eventos vitales adversos en una muestra representativa grande de la población general en Dinamarca.
Métodos: La traducción y la validación siguió los Estándares basados en Consensos para la selección de los Instrumentos de Medición en Salud (COSMIN en su sigla en inglés) para modelos formativos. La validez de contenido y constructo fueron evaluadas incluyendo la puesta a prueba de la hipótesis de que la adversidad acumulada a lo largo de la vida tiene un patrón de forma en U con bajos niveles de adversidad acumulada a lo largo de la vida, en lugar de niveles nulos o altos, está asociado con más baja angustia emocional, discapacidad funcional, y deterioro del dolour. La muestra de prueba de campo fue una cohorte de DanFunD (n=7493) obtenida aleatoriamente de una población danesa y examinada entre el 2012-2015.
Resultados: Las entrevistas piloto mostraron que las preguntas fueron confrontativas pero no ofensivas, directas, y fáciles de contestar. La aceptabilidad fue buena. Se encontraron patrones en forma de U entre la adversidad acumulada a lo largo de la vida y las medidas de los resultados. En términos cuadráticos: Angustia emocional (β(IC 95%) 0,007(0,002;0,012), p<0.007), discapacidad funcional (β(IC 95%) −0,002(−0,003;-0,001), p<0.001), y deterioro del dolour (β(IC 95%) 0,004(0,002;0,006), p=0.001). La prueba de campo proporcionó los números básicos para los eventos vitales adversos para la población general danesa, con una adversidad acumulada a lo largo de la vida promedio (DE), 5.9 (3.7). En comparación con los Estados Unidos, se reportan tasas más bajas de violencia, estrés social/ambiental, y desastre.
Conclusiones: Los resultados de la versión original fueron replicados, indicando una validez de constructo alta. Además, la validez de contenido fue buena.
PALABRAS CLAVE: Eventos vitales adversos, angustia emocional, deterioro del dolour, discapacidad funcional, validación, modelo formativo
背景: 负性生活事件是精神疾病的一个预测因子。然而, 大多数研究都集中在选定的领域, 例如童年期或近期逆境。累积终身逆境测量 (CLAM) 是一个新引入, 尚未验证的量表, 考查一系列事件的累积影响, 包括暴露于同一事件的次数。这项测量为大型队列研究收集终身逆境的详细数据提供了机会。
目标: 本研究旨在将CLAM译为丹麦语, 并在大量普通人群中对CLAM进行验证。其次, 我们旨在描述一个大型丹麦普通人群代表性样本中不良生活事件的发生率。
方法: 翻译和验证遵循基于共识选择健康测量工具的标准 (COSMIN) 以选择形成性模型。对内容和结构效度进行评估, 包括针对累积终身逆境的U型模式假设检验, 即累积终身逆境低水平与虚无假设对比或高水平与较低情绪困扰, 功能损伤和疼痛障碍相关。现场试验样本是从丹麦人群中随机抽取的DanFunD群体 (n = 7493), 并在2012年至2015年之间进行考查。
结果: 试点访谈表明, 访谈问题是需要直面的但非冒犯, 直接的, 而且易于回答。可接受性很好。发现了累积终身逆境和结果之间的U型模式。二次项:情绪困扰 (β (95%CI):0.007 (0.002; 0.012), p<0.007), 功能损伤 (β (95%CI):-0.002 (−0.003; −0.001), p<0.001) 及疼痛障碍 (β (95%CI):0.004 (0.002; 0.006), p= 0.001) 。现场试验提供了丹麦普通人群不良生活事件的基本数字, 累积终身逆境平均值 (标准差) 为5.9 (3.7) 。与美国相比, 暴力, 社会/环境压力和灾难的发生率更低。
结论: 原始版本的结果得到重复, 表明结构效度很高。此外, 内容效度良好。
Abbreviations: CI: Confidence Interval; CLAM: The Cumulative Lifetime Adversity Measure; COSMIN: The COnsensus-based Standards for the selection of health Measurement Instruments; DanFunD study: Danish Study of Functional Disorders; FSS: Functional Somatic Syndromes; M: Mean; PI: Principle Investigator; RCPH: The Research Centre for Prevention and Health; SCL-8: Symptom Check List 8; SD: Standard Deviation; SF-12: Short Form 12; US: USA; WHO: World Health Organization
关键词: 不良生活事件, 情绪困扰, 疼痛障碍, 功能损伤, 验证, 形成性模型
1. Introduction
The experience of negative life events is associated with poor mental health and well-being (Turner & Lloyd, 1995), and stress vulnerability models generally assume that exposure to negative life events is a broad risk factor for the development of anxiety, depression, functional disorders, and psychosis (Dienstbier, 1989; Mayo et al., 2017; Turner & Lloyd, 1995). These findings represent the dose-response theory (Gerber et al., 2018; Turner & Lloyd, 1995). A wide array of questionnaires exists on negative life events with various foci and dimensions, e.g. childhood adversity (Lloyd & Turner, 2008) and adversity within the last year (Brown & Harris, 1978) versus lifelong adversity (Turner & Lloyd, 1995). Some focus on specific events such as divorce (Aseltine & Kessler, 1993) or traumatic events mainly found in low socio-economic populations (Liu et al., 2015). Other measures encompass most adverse life events, either weighting the impact of events (Holmes & Rahe, 1967; Keinan, Shrira, & Shmotkin, 2012) or using simple cumulated counts (Abravanel & Sinha, 2015; Shrira & Litwin, 2014) or checklists (Holmes & Rahe, 1967; Weathers et al., 2013) versus contextual measures (Brown & Harris, 1978), cumulated counts of events (Lloyd & Turner, 2008), or cumulated counts including multiple occurrence of the same event (Breslau et al., 1998; Seery, Leo, Holman, & Silver, 2010b).
Seery et al. have focused on accumulated life stress and have developed the Cumulative Lifetime Adversity Measure (CLAM) (Seery, Holman, & Silver, 2010a; Seery et al., 2010b). According to theories of resilience, they assume that the ability to successfully cope with life stressors and adapt to changing life circumstances derives from some exposure to risk (Dienstbier, 1989; Masten, 2001). Therefore, they hypothesize a U-shaped relationship between adversity exposure and resilience, i.e. individuals with an experience of low/some adversity should demonstrate greater resilience compared to those with an experience of either no or high adversity. Their studies have confirmed that participants with a history of some adversity, as opposed to no or high levels of adversity, report better psychological well-being (Seery et al., 2010a), lower functional impairment and health care utilization (Seery et al., 2010b). These findings represent the stress-inoculation theory (Seery, 2011).
The strength of the CLAM is that it examines not only a wide range of life events but also the cumulative effect of different kinds of events including number of exposures to the same event. Furthermore, it has the advantage of both evaluating age-specific (e.g. childhood adversity) and lifetime adversity. Usually, interview data have to be collected to get this kind of information (Breslau et al., 1998), and the option of collecting data in large population samples is therefore limited. The CLAM gives the opportunity to collect detailed data on lifetime adversity in large cohort studies like the present study. Prior to this study, the CLAM was not available in any other language than English and has only been used in American (US) cohorts (Seery et al., 2010a, 2010b). In this study, we hypothesized that the Danish version of the CLAM would replicate the results from the US version, i.e. participants with low levels of cumulated lifetime adversity as opposed to no or high levels have statistically significantly lower emotional distress, functional impairment, and pain impairment (quadratic pattern/U-shaped or inverted U-shaped). Secondly, we hypothesized, as found in the US version, that adversity history was not a proxy for age, i.e. age and cumulated adversity score were not correlated.
The first aim of this study was translation of the CLAM into Danish. The second aim was validation of the CLAM in a large general population cohort. Thirdly, we aimed to describe the occurrence of adverse life events in a large representative sample of the general population in Denmark.
2. Methods
2.1. Study design and ethics
The study sample is part of the DanFunD study (The Danish Study of Functional Disorders) investigating the epidemiology of functional somatic syndromes (FSS) from 2012 to 2015, where a random sample of 25,368 men and women aged 18–72 years living in the western part of greater Copenhagen obtained via Danish registers were invited of whom 29.5% (n = 7,493) agreed to participate (Dantoft et al., 2017). Exclusion criteria were: Not born in Denmark, not being a Danish citizen, and pregnancy. All participants completed two sets of questionnaires, underwent clinical health examination, and gave written informed consent at the Research Centre for Prevention and Health, Glostrup, Denmark, (RCPH). The study was approved by the Ethical Committee of Copenhagen County (Ethics Committee: KA-2006-0011, H-3-2011-081, and H-3-2012-0015) and the Danish Data Protection Agency (2012-58-006, 1-16-02-227-16) and was conducted in accordance with the Helsinki II declaration.
2.2. Measures
2.2.1. Cumulative lifetime adversity measure
The CLAM (Seery et al., 2010a, 2010b) is a measure modified from the Diagnostic Interview Schedule trauma section (Robins, Helzer, Croughan, Williams, & Spitzer, 1981) expanded with items on stressful life events retrieved from primary care patients’ reports (Holman, Silver, & Waitzkin, 2000). The questionnaire addresses seven life categories, i.e. 37 different life stressors (Figure 1). It captures stress to the individual (social/environmental stress, relationship stress, and stress to body and mind) on items regarding oneself but also related to loved ones thus including indirect consequences. It includes the whole life span from childhood up to the time of measurement. The original American version of the measurement is analysed as a total sum score (accumulation of life events).
Figure 1.
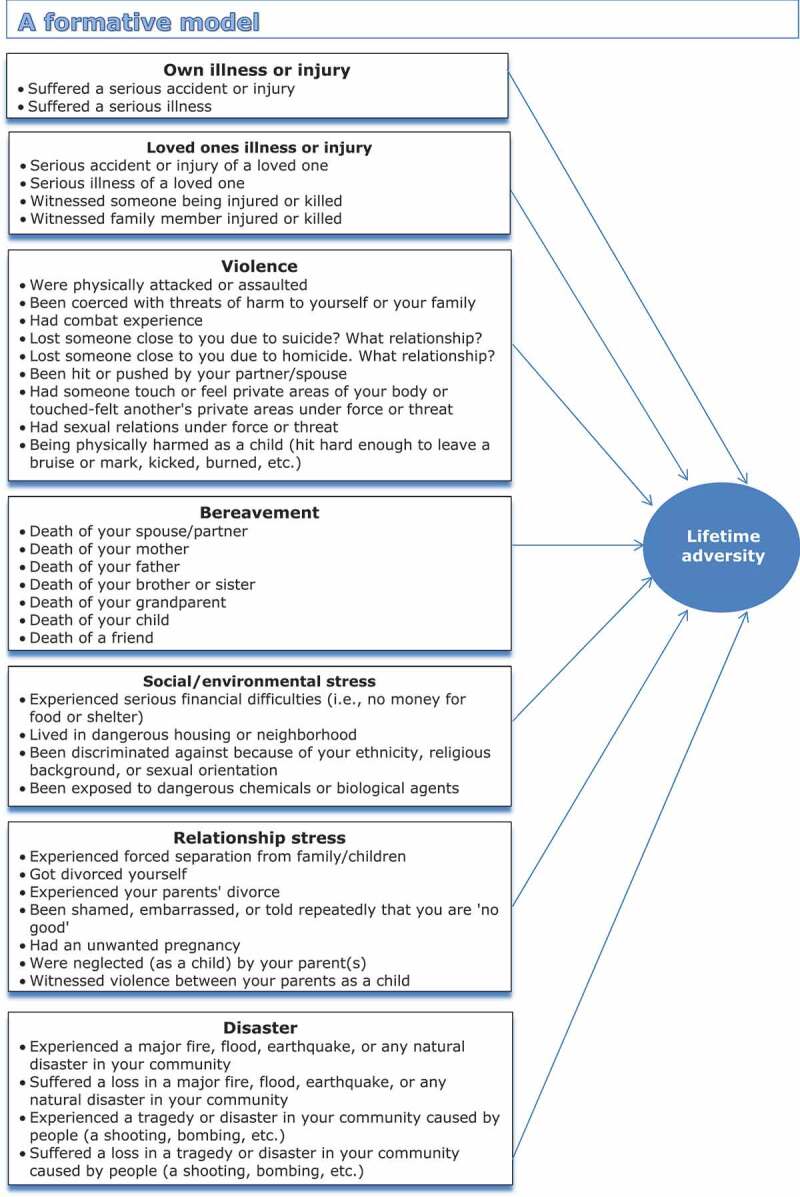
The formative model of the Cumulative lifetime adversity measure organized in the seven life categories.
Exposure to lifetime adversity was obtained by asking the participants whether they had ever experienced 37 different adverse life events plus a possibility to add one other unnamed life event. Participants wrote the age at which each event occurred or an age interval if the event had occurred for a time period. It was possible to record up to four instances for each event regardless of duration. In accordance with the original CLAM measure, the sum score for the CLAM is the addition of age time-points and age ranges by simply counting age time-points and age ranges, i.e. an age range counted for one event and an age time-point counted for one event. This may not be the most beneficial way as an event that took place for a longer period of time may put a heavier burden on the individual than an event that has taken place once or within one year. However, we have contacted the original author of the questionnaire and asked if they have weighted the questions in the counting of events and they did not. The primary aim of this paper was to validate the translation of the questionnaire in another population; therefore we stuck to the same decisions as the original authors in the intension to keep the questionnaire and the analyses of the data as identical as possible.
2.2.2. Background characteristics
The socio-demographic variables include sex, age, marriage/cohabiting status, and attachment to labour market.
2.2.3. Outcome variables
2.2.3.1. Emotional distress
Emotional distress within the last week (Symptom Check List 8; SCL-8) is an 8-item scale with response scale ranging from 0 = ‘not at all’ to 4 = ‘extremely’. Sum score is calculated 0–32 with high values indicating high level of emotional distress. The SCL-8 is derived from the SCL-90 depression and anxiety subscales (Derogatis, Lipman, & Covi, 1973). The SCL-8 (dichotomized version) has been internally and externally validated (Fink, Ornbol, Hansen, Sondergaard, & De Jonge, 2004a; Fink et al., 2004b). A Cronbach’s alpha in this study was computed to 0.82.
2.2.3.2. Functional impairment
Functional impairment in work and social activities resulting from physical or emotional health within the last 4 weeks on a categorical scale 1–5 ranging from 1 = ‘all the time’ to 5 = ‘not at all’. The measure has been derived from the SF-12 using 4 single items from this scale (Ware, Kosinski, & Keller, 1996). The total mean of the 4 items are used as applied in the US study (Seery et al., 2010a). A Cronbach’s alpha in this study was computed to 0.81.
2.2.3.3. Pain impairment
A non validated single item on impairment of daily activities due to pain in neck, chest, or back within the last 12 months on a 1–10 numeric scale ranging from 1 = ‘not at all’ to 10 = ‘impairment of daily activities’.
2.3. Procedures
2.3.1. Process of translation and pilot testing
We used instructions from two known guidelines as a template for the translation process (Beaton, Bombardier et al. 2000; World Health Organization, 2018). An expert committee was gathered including two translators uninformed of the concepts being qualified, two informed translators, two experts within the area experienced in research and clinical work, and one recording observer. All translators’ native language was the target language. The four translators did the forward translation independently. Translation followed a cross-cultural and conceptual focus rather than a linguistic focus. A synthesis meeting was set up between the translators resulting in a consensus version of the translations and a report documenting the synthesis process. This version was brought to the expert committee to be reviewed resulting in a pre-final version, which was pilot tested in a small sample of 10 participants purposefully chosen to broadly represent the general population regarding gender, age, socio-economic group, and region of residence; five men and five women, 22–61 of age, different socio-economic groups, habitants of South and Central Regional Denmark. The participants completed the questionnaire and were then interviewed about comprehensibility and acceptability. The semi-structured interview was carried out by an interviewer (a bachelor in psychology) with fixed questions but open-ended answers for each item and the possibility to add reflections freely. On the basis of the report from pilot testing and interviews, the expert committee reviewed the pre-final version and consented on necessary modifications. The original author reviewed and accepted the modifications. When applying the questionnaire to field testing, the DanFunD steering group modified the layout and instruction of the questionnaire to improve the visual impression and to streamline the comprehensive examinations and questionnaires. All items and the wording of these were kept as decided by the expert committee. After field testing was carried out, a back-translation was performed on the field testing version of the questionnaire by a translator blind to the original version, uninformed to the construct, and whose native language was the source language. The expert committee compared the two versions and discussed potential disagreements. Questions of doubt were conferred with the original author, who had only few comments. For detailed information about back-translation and all modifications, please refer to Appendix 1.
2.4. Validation
For the assessment of validity, we applied the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) (Mokkink et al., 2010). The CLAM is based on a formative model as opposed to a reflective model (Figure 1). When working with multi-item measurement instruments we need to know the underlying relationship between the items and the construct and in this case it is a formative model where the items form or cause the construct (Figure 1 – the arrows points from the items to the construct) as apposed to a reflective model where the construct manifests itself in its items (i.e. the arrows points from the construct to the items). The items in a formative model forms an index (an index is made from the items in the measure, in this case there is seven categories of life events). The term index is used for an instrument consisting of multiple dimensions as the CLAM, and a sum score is presented as an estimate of the index. On the other hand the items in a reflective model form a scale (De Vet, Terwee, Mokkink, & Knol, 2011). Due to the CLAM being a formative model internal consistency cannot meaningfully be applied (Diamantopoulos, Riefler, & Roth, 2008). According to recommendations, we also omitted all reliability assessment as correlations are very hard to interpret, and important indicators could be deleted due to misinterpretations (Diamantopoulos et al., 2008). Common sense and the knowledge of clinical reality is what measurement theory of a formative model is based on (De Vet et al., 2011). As the items are not an effect of the construct, it is not relevant to measure structural validity in the form of factor analysis. Criterion validity cannot be assessed as there is no gold standard for assessing cumulative lifetime adversity. Responsiveness and measurement error are not possible to assess in this study as we have only measured lifetime adversity at one point in time. Two measurement properties are relevant for the validation of the CLAM: Content validity (including face validity) and one aspect of construct validity (hypotheses testing).
2.4.1. Content validity
Content validity is the degree to which the content of a measure is an adequate reflection of the construct we want to measure (Mokkink et al., 2010). At first, the construct to measure should therefore be described. The construct to be measured is simple accumulated lifetime adversity or strain and not if or how much the individual actually appraised the experience as a challenge or a threat. The construct holds a broad spectrum of negative events and not only highly traumatic events but also events that are common. Accumulated strain is in focus by taking both episodes being for a period of time and episodes at a specific point in time in to account.
2.4.1.1. Face validity
Face validity was assessed in two ways; firstly, simply by looking at the questionnaire, e.g. the number of questions and the appropriateness of the questions, and secondly by evaluating the pilot interview participants’ evaluation.
2.4.1.2. Relevance
The relevance was evaluated on the field testing data based on missing observations. According to informal criteria, an acceptable rate of missings in field testing is less than 3% per item, more than 15% is not acceptable. In-between rates are open to discussion (De Vet et al., 2011).
2.4.1.3. Comprehensiveness
Evaluation of comprehensiveness was carried out by evaluating the last item, 38, named ‘other’ in the intension to examine if the CLAM holds all possible adverse life events that one can experience. This was done by looking into the free text provided by participants producing such information and subsequently categorizing the free text answers.
2.4.2. Construct validity
2.4.2.1. Hypotheses testing
Outcome measures that were equivalent to the outcome measures used on the original version was chosen. Seery et al. employed global distress measuring psychological distress (depression, anxiety, and somatizations) and functional impairment in work and social activities resulting from physical and/or emotional health using the mean of four items from the SF-36 (Seery et al., 2010a). They have used the CLAM in a healthy population sample (Seery et al., 2010a) similar to our study but also in a clinical population sample (chronic back pain) (Seery et al., 2010b). We applied a third outcome measure of pain impairment from pain in neck, chest or back to be able to compare the results.
We hypothesized that the Danish version of the CLAM would replicate the results from the US version, i.e. participants with low levels of cumulated lifetime adversity as opposed to no or high levels have statistically significantly lower emotional distress, functional impairment, and pain impairment (quadratic pattern/U-shaped or inverted U-shaped). This was tested via regression analyses employing a transformed sum score of the CLAM explained in detail in the statistical section. Secondly, we hypothesized, as found in the US version, that adversity history was not a proxy for age, i.e. age and cumulated adversity score were not correlated.
2.5. Statistical analysis
2.5.1. Regressions
Linear regression analyses were performed for emotional distress, functional impairment, and pain impairment as dependent continuous outcome variables and lifetime adversity as independent variable. Firstly, the linear lifetime adversity term alone was tested (according to the ‘dose-response theory’), secondly, the inclusion of a quadratic relationship to lifetime adversity, i.e. curved shape (according to the ‘stress-inoculation theory’). For evaluation of the assumptions, we checked the residuals on scatterplot, histogram, and Q-Q plot. Due to the skewed distribution of the residuals, we performed bootstrap estimates of the standard errors with repetitions of 1000. We performed likelihood ratio test to examine the potential significant difference between the linear and the quadratic models. To examine if the Danish translation of the original version of the CLAM would perform in the same way as the original, the cumulative lifetime adversity score was transformed according to , and outcome variables were converted to z-scores (M = 0, SD = 1). The regression coefficients (βs) represent the standard deviations of change in outcome predicted for each standard deviation change in adversity. In the graphic presentation, the x-axis is restricted in range to enable a comparison to the original research. To evaluate the clinical importance of the potential protective effect of a low score on lifetime adversity, we calculated the difference between ‘no adversity’ and ‘low adversity’, the value 0 and the value 3, respectively, in the model with the quadratic relationship. In the intention to check if adversity history could be a proxy for age, we performed a Spearman’s rank correlation between age and life events. We checked if the covariates age and sex could possibly explain the associations between outcome and life events in the linear and the quadratic models. The covariate variables that were used in these analyses were (1) a simple continuous age variable (age at the time of filling in the questionnaire – independent of the age registrations in the CLAM questionnaire) and (2) a dichotomous variable for sex. The statistical programme used for the analysis was STATA 15.0 (STATA, 2003).
3. Results
3.1. Study population and measurements
The cohort consisted of 7,493 participants aged 18–72 years (mean age 52.0) of whom 53.9% were women (Table 1). The completion rate of the CLAM was 98.8% as only 88 participants did not fill in the questionnaire. The completion rate on outcome measures was 97.4% on pain impairment, 99.6% on functional impairment, and 98.2% on emotional distress. The total number of lifetime adverse events experienced in the Danish sample ranged from 0 to 35 (M = 5.87, SD = 3.69, Median = 5), while the sample range was 0–71 (M = 7.69, SD = 6.04, Median = 7) in the US population (Seery et al., 2010a). In the Danish sample, 4.2% reported no adverse events as opposed to 8.1% in the US population sample.
Table 1.
Cohort characteristics on socio-demographics, adversity, and outcome measures.
| Total cohort N = 7493 |
Participants completing The CLAM N = 7405 |
||
|---|---|---|---|
| Socio-demographics: | |||
| Mean age years (SD) | Age | 52.0 (13.3) | 52.0 (13.3) |
| Gender (%) | Men | 3456 (46.1) | 3405 (46.0) |
| Women | 4037 (53.9) | 4000 (54.0) | |
| Marital/cohabiting status (%) | Married or cohabiting with partner | 5778 (77.1) | 5719 (77.2) |
| Other | 1664 (22.2) | 1640 (22.2) | |
| Unaccounted | 51 (0.7) | 46 (0.6) | |
| Attachment to labour market (%) | Currently employed | 5104 (68.1) | 5055 (68.3) |
| Previously employed | 2183 (29.1) | 2149 (29.0) | |
| Never been employed | 121 (1.6) | 121 (1.6) | |
| Unaccounted | 85 (1.1) | 80 (1.1) | |
| The CLAM: Mean (SD) | |||
| Cumulated lifetime total score | Lifetime experienced events | – | 5.9 (3.7) |
| Cumulated childhood total score | 0–18 years experienced events | – | 1.5 (1.8) |
| 7 dimensions– lifetime | |||
| Own illness or injury | – | 0.6 (0.9) | |
| Loved ones illness or injury | – | 1.0 (1.1) | |
| Violence | – | 0.4 (0.9) | |
| Bereavement | – | 2.8 (1.9) | |
| Social/environmental stress | – | 0.3 (0.6) | |
| Relationship stress | – | 0.7 (1.0) | |
| Disaster | – | 0.1 (0.4) | |
| Outcome measures: Mean (SD) | |||
| Emotional distress | Range 0-32 | 2.7 (3.8) | 2.7 (3.8) |
| Missing = 136 | |||
| Functional impairment | Range 1-5 | 4.5 (0.6) | 4.5 (0.6) |
| Missing = 33 | |||
| Pain impairment | Range 1–10 | 2.2 (2.0) | 2.2 (2.0) |
| Missing = 197 | |||
SD = Standard deviation, Unaccounted = missing observations.
3.2. Error corrections
After participants filling in questionnaires errors set to missing were 1,510 events in total, corresponding to 3.4% of the total 44.995 registered life adversity events. After error correction in data, 43,485 lifetime adversity events were registered in this cohort. Corrections of errors in data see Appendix 1.
3.3. Validation
3.3.1. Content validity
3.3.1.1. Face validity
When evaluating interview data from the pilot testing, all 10 participants found the questions easy to understand, straight forward to answer, and felt that the questions were clear, somewhat confronting but not offensive, and all pilot participants evaluated the questionnaire acceptable. The field test showed that the participants accepted the questionnaire, but some errors indicated that the filling in of the age part may be somewhat challenging for a minority.
3.3.1.2. Relevance
The percentage of missing observations on any item varied between 1.8% and 4.2%, but on one item (item 37 – unwanted pregnancy), the percentage of missing observations was 5.7% (Table 2). Two thirds of the missing observations on this item were men, indicating that some males did not know how to apply this question to their life. Overall, all items seem relevant for the general population as the percentage of missing observations was low. Due to the low amount of missing observations we did not impute or otherwise attribute to data.
Table 2.
Distributions on item level on the CLAM.
| Distributions |
||||||||
|---|---|---|---|---|---|---|---|---|
| Cumulative 0–18 years (%) |
Cumulative All (%) |
|||||||
| Events |
||||||||
| Items | Unaccounted | 0 | 1 | 2+ | 0 | 1 | 2+ | |
| 1 | Suffered a serious accident or injury | 3.3 | 89.9 | 6.1 | 0.7 | 77.9 | 14.5 | 4.3 |
| 2 | Were physically attacked or assaulted | 2.2 | 94.0 | 3.4 | 0.4 | 88.4 | 7.8 | 1.6 |
| 3 | Serious accident or injury of a loved one | 2.9 | 92.8 | 3.9 | 0.4 | 78.6 | 15.2 | 3.3 |
| 4 | Suffered a serious illness | 3.2 | 93.9 | 2.7 | 0.2 | 80.6 | 12.8 | 3.4 |
| 5 | Serious illness of a loved one | 3.5 | 86.8 | 8.8 | 0.9 | 41.9 | 37.4 | 17.2 |
| 6a | Witnessed family member injured or killed | 2.2 | 96.3 | 1.4 | 0.1 | 92.5 | 4.7 | 0.6 |
| 7a | Witnessed someone being injured or killed | 2.0 | 95.4 | 2.4 | 0.2 | 87.2 | 8.8 | 2.0 |
| 8 | Been coerced with threats of harm to yourself or your family | 1.9 | 97.5 | 0.5 | 0.1 | 96.1 | 1.8 | 0.2 |
| 9 | Experienced forced separation from family/children | 2.1 | 96.0 | 1.6 | 0.3 | 93.6 | 3.6 | 0.7 |
| 10 | Had combat experience | 1.9 | 98.1 | 0.0 | 0.0 | 97.5 | 0.4 | 0.2 |
| 11 | Death of your spouse/partner | 2.0 | 97.9 | 0.1 | 0.0 | 93.9 | 3.9 | 0.2 |
| 12 | Death of your mother | 1.9 | 95.5 | 2.6 | – | 58.7 | 39.4 | – |
| 13 | Death of your father | 1.8 | 93.6 | 4.6 | – | 47.9 | 50.3 | – |
| 14 | Death of your brother or sister | 2.4 | 96.0 | 1.5 | 0.1 | 85.0 | 10.6 | 2.0 |
| 15 | Death of your grandparent | 3.3 | 61.4 | 23.1 | 12.2 | 35.4 | 20.1 | 41.2 |
| 16 | Death of your child | 2.5 | 97.3 | 0.2 | 0.0 | 95.0 | 2.3 | 0.2 |
| 17 | Death of a friend | 2.5 | 93.8 | 3.4 | 0.3 | 70.8 | 21.0 | 5.7 |
| 18 | Lost someone close to you due to suicide | 2.0 | 96.4 | 1.6 | 0.0 | 89.8 | 7.6 | 0.6 |
| 19 | Lost someone close to you due to homicide | 2.3 | 97.4 | 0.3 | 0.0 | 96.7 | 0.9 | 0.1 |
| 20 | Got divorced yourself | 4.0 | 95.9 | 0.1 | 0.0 | 68.9 | 23.1 | 4.0 |
| 21 | Experienced your parents divorce | 3.9 | 80.8 | 14.6 | 0.7 | 76.8 | 18.2 | 1.1 |
| 22 | Experienced serious financial difficulties | 4.0 | 94.6 | 1.3 | 0.1 | 90.5 | 4.8 | 0.7 |
| 23 | Experienced a major, fire, flood, earthquake, or any natural disaster in your community | 3.9 | 94.5 | 1.4 | 0.2 | 91.1 | 4.4 | 0.6 |
| 24 | Suffered a loss in a major, fire, flood, earthquake, or any natural disaster in your community | 3.9 | 95.9 | 0.2 | 0.0 | 94.9 | 1.1 | 0.1 |
| 25 | Experienced a tragedy or disaster in your community caused by people | 3.9 | 95.5 | 0.5 | 0.1 | 94.1 | 1.8 | 0.2 |
| 26 | Suffered a loss in a tragedy or disaster in your community caused by people | 3.9 | 96.0 | 0.1 | 0.0 | 95.9 | 0.2 | 0.0 |
| 27 | Lived in dangerous housing or neighbourhood | 4.0 | 95.2 | 0.8 | 0.0 | 93.8 | 1.9 | 0.3 |
| 28 | Been discriminated against your ethnicity, religious background, or sexual orientation | 3.9 | 95.6 | 0.4 | 0.1 | 95.2 | 0.7 | 0.2 |
| 29 | Been exposed to dangerous chemicals or biological agents | 4.2 | 94.4 | 1.3 | 0.1 | 92.9 | 2.5 | 0.4 |
| 30 | Were neglected as a child by your parents | 4.2 | 91.8 | 3.5 | 0.5 | 91.8 | 3.5 | 0.5 |
| 31 | Being physically harmed as a child | 4.0 | 93.1 | 2.5 | 0.4 | 93.1 | 2.5 | 0.4 |
| 32 | Witnessed violence between your parents as a child | 4.0 | 91.7 | 3.6 | 0.7 | 91.7 | 3.6 | 0.7 |
| 33 | Been hit or pushed by your partner/spouse | 4.0 | 95.4 | 0.5 | 0.1 | 92.2 | 3.1 | 0.7 |
| 34 | Been shamed, embarrassed or told repeatedly that you are no good | 4.1 | 92.3 | 3.3 | 0.3 | 90.0 | 5.2 | 0.7 |
| 35 | Had someone touch or feel private areas of your body or touched/felt another’s private areas under force or threat | 4.1 | 94.7 | 1.1 | 0.1 | 94.0 | 1.7 | 0.2 |
| 36 | Had sexual relations under force or threat | 4.1 | 93.9 | 1.8 | 0.2 | 93.5 | 2.1 | 0.3 |
| 37 | Had an unwanted pregnancy | 5.7 | 92.4 | 1.8 | 0.1 | 84.9 | 7.9 | 1.5 |
| 38 | Other event, Specify | 38.5 | 60.4 | 1.0 | 0.1 | 56.8 | 4.1 | 0.6 |
aItem number according to Danish version, Unaccounted = missing observations.
All 37 items had registered events. However, some events were rare in this sample. The following items had 1% or less events registered: ‘Had combat experience’ 0.6% (n = 44), ‘Lost someone close to you due to homicide’ 1% (n = 72), ‘Suffered a loss in a tragedy or disaster in your community caused by people’ 0.2% (n = 17), ‘Been discriminated against your ethnicity, religious background, or sexual orientation’ 0.9% (n = 66) (Table 2). We found lower rates of violence, social/environmental stress, and disaster in the Danish compared to the US sample (Table 3).
Table 3.
Seven categories US and Danish samples.
| Seven categories | US – national sample (% of all events) N = 2398 |
DK – national sample (% of all events – 43.485) N = 7405 |
|---|---|---|
| Own illness or injury | 6.9 | 9.3 |
| Loved ones illness or injury | 15.0 | 16.8 |
| Violence | 11.4 | 6.6 |
| Bereavement | 39.5 | 45.3 |
| Social/environmental stress | 8.9 | 4.3 |
| Relationship stress | 12.7 | 11.6 |
| Disaster | 5.5 | 1.6 |
3.3.1.3. Comprehensiveness
402 participants used the possibility to add an unnamed event. The majority of these events would actually fit into existing categories such as ‘discrimination’ or ‘illness of your child or yourself’, while some events did not fit into existing categories (Table 4).
Table 4.
Number of ‘other events’ (item 38).
| Event | Number |
|---|---|
| Miscarriage | 47 |
| Handicapped child | 17 |
| Witnessed robbery e.g. bank or post office | 13 |
| ‘Close to’ experiences e.g. death, suicide attempts (self or loved ones) | 12 |
| Illness due to stress | 11 |
| Psychological strain at work | 10 |
| Bullying | 10 |
| Dismissal | 9 |
| Psychological distress e.g. depression, anxiety, psychosis. | 7 |
| Alcoholic parents or other substance abuse | 7 |
| Involuntary childlessness | 5 |
| Burglary | 4 |
| Loved one at war | 4 |
| Witnessed violence against others | 3 |
| Adoption of a child | 3 |
| Harm to others e.g. partner, children. | 3 |
| Dangerous travels e.g. slum area, war-affected countries | 3 |
| False accusations | 3 |
| Loved one has killed someone | 2 |
| Falling foul of others e.g. gang members | 2 |
| Imprisoned | 1 |
| Events that fit into existing categories | 49 |
| Blank text box but filled in age on item 38 | 177 |
3.3.2. Construct validity
3.3.2.1. Hypotheses testing
Consistent with previous research, we found, on the three outcomes of emotional distress, functional impairment, and pain impairment, that the greater the adversity the greater the distress and impairment (Table 5). This supports the ‘dose-response theory’. Furthermore, analyses confirmed a significant U-shaped/inverted U-shaped quadratic relationship on all three outcomes and likelihood ratio tests showed a significant difference between the linear and the quadratic models for all three outcome measures (Table 5). This supports the ‘stress-inoculation theory’. The results on the linear and the quadratic curve on one outcome measure (functional impairment) are graphically presented in Figure 2 on original scales.
Table 5.
Regression models on lifetime adversity and the three outcome variables with beta coefficients and confidence intervals on original scales examining linear and quadratic relationships and expected values based on original outcome scores and lifetime adversity examining the difference between no and low score on lifetime adversity.
| Emotional distressa (last 7 days)d n = 7296 |
Functional impairmentb (last 4 weeks)e n = 7376 |
Pain impairmentc (last 12 months)f n = 7237 |
||||
|---|---|---|---|---|---|---|
| Cumulative lifetime adversity | β (95%CI) | p-Value | β (95%CI) | p-Value | β (95%CI) | p-Value |
| Linear relationship | 0.143 (0.114;0.171) | <0.001 | −0.029 (−0.034;-0.024) | <0.001 | 0.068 (0.054;0.082) | <0.001 |
| Quadratic relationship | ||||||
| 1.term, x | 0.029 (−0.050;0.108) | 0.472 | −0.001 (−0.012;0.012) | 0.985 | 0.003 (−0.034;0.039) | 0.877 |
| 2.term, x2 | 0.007 (0.002;0.012) | 0.007 | −0.002 (−0.003;-0.001) | <0.001 | 0.004 (0.002;0.006) | 0.001 |
| Quadratic relationship | ||||||
| Lifetime adversity (expected values) | ||||||
| No (0) | 2.168 (1.915;2.420) | 4.636 (4.596;4.676) | 1.973 (1.847;2.099) | |||
| Low (3) | 2.318 (2.213;2.422) | 4.619 (4.602;4.637) | 2.017 (1.960;2.074) | |||
| High (9.5) | 3.084 (2.931;3.238) | 4.472 (4.448;4.497) | 2.364 (2.291;2.438) | |||
| Difference between ‘no’ and ‘low’ | −0.150 (−0.344;0.044) | 0.130 | 0.016 (−0.013;0.045) | 0.269 | −0.044 (−0.135;0.046) | 0.334 |
| Difference between ‘low’ and ‘high’ | −0.767 (−0.955;-0.580) | <0.001 | 0.147 (0.116;0.178) | <0.001 | −0.347 (−0.442;-0.252) | <0.001 |
aScl-8: Sumscore 0–32, bSF-12: Total mean of 4 single items, cNumeric rating scale 1–10, dLikelihood-ratio test: x2(1) = 19.53, p < 0.0001, eLikelihood-ratio test: x2(1) = 45.99, p < 0.0001, fLikelihood-ratio test: x2(1) = 23.00, p < 0.0001. Bold values indicate significance lower than 0.01.
Figure 2.
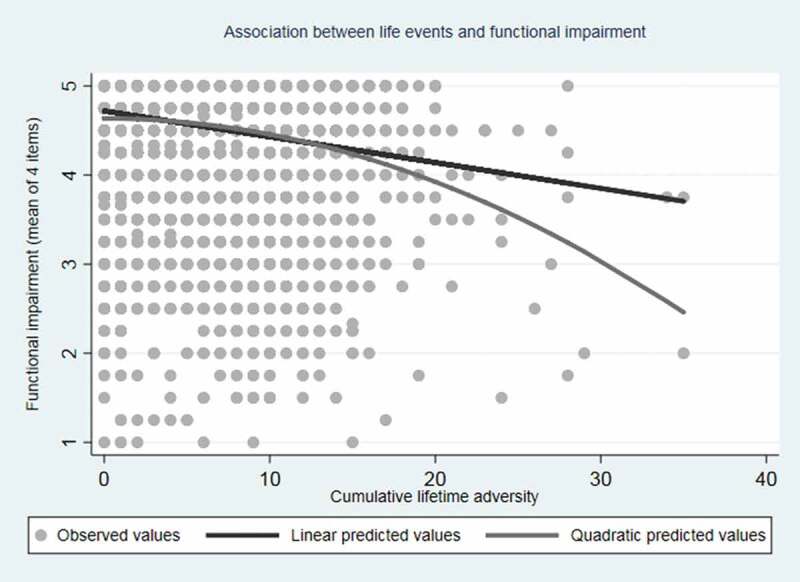
Association between life events and functional impairment.
Lifetime adversity and outcome variables were then transformed. The results regarding the quadratic relationship were statistically significant on all three outcome measures (p < 0.001). Figure 3 presents the results on z scores and log-transformed score restricted in range to show the U-curves/inverted U-curves comparable to the original version of the CLAM. The Danish translation of the CLAM performed as hypothesized with a quadratic relationship showing a statistically significant resilience effect of a low score (value = 3) on lifetime adversity on all three outcome measures.
Figure 3.
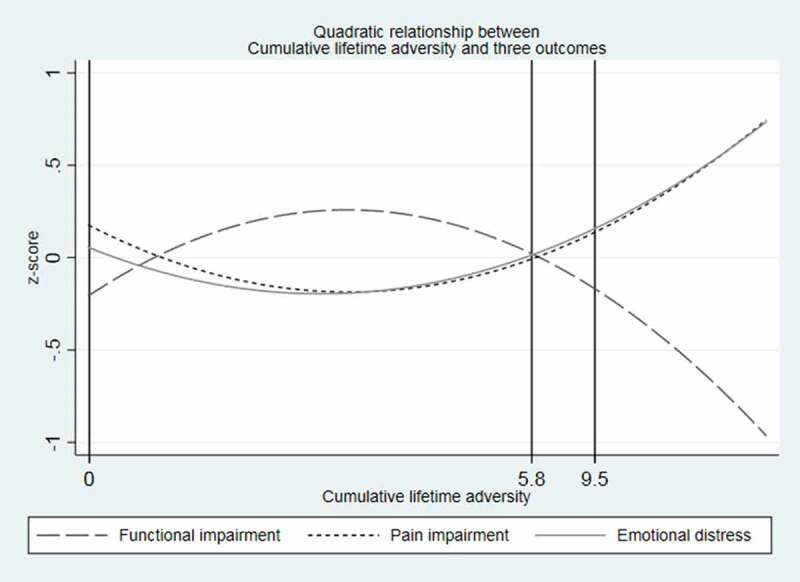
Quadratic relationship between cumulative lifetime adversity and three outcomes.
Regression models including the covariates age and sex showed that these covariates did not explain the relationship, i.e. the associations were still significant in all six models (all p-values < 0.001) (results not shown). The Spearman’s rank correlation of age and the cumulative score of life events showed a statistical significant correlation of r = 0.10, p < 0.001. However, this is considered a very weak correlation as correlations of up to approximately 0.30 are considered weak, moderate correlations are approximately from 0.30 to 0.60, and strong correlations are approximately from 0.60 and up (Coolican, 1999). Therefore, age does not account for the observed relationship between the outcome variables and lifetime adversity in this sample, i.e. the sum score of the CLAM is not a proxy for age.
Evaluation of assumptions for regression models: Via inspection of graphs on adversity lifetime events, we found that the assumptions were not met as residuals were highly skewed and thus not normally distributed. We still did regression analyses to validate the Danish version performing the same analyses as for the US version. Due to the skewed distribution of the residuals, we performed bootstrap estimates of the standard errors with repetitions of 1000.
3.3.3. Clinical importance of resilience effect
Lifetime adversity was categorized into three points; no [0], low [3], or high level [9.5] of adversity, and the difference between ‘no adversity’ (value = 0) and ‘low adversity’ (value = 3) was calculated (Table 5). Low level of adversity was based on the 25th percentile. High level of adversity was based on the work of Seery and colleagues who based their high level on a standard choice for continuous predictor variables, which reflects a point in the distribution that is relatively high but not unreliably extreme (Aiken & West, 1991; Seery et al., 2010b). We did not find any clinical importance of the resilience effect of a low score on lifetime adversity on the three outcome measures on the original scales. The difference for e.g. pain impairment (β (95%CI)) was −0.044 (−0.135;0.046) (Table 5). This means that the difference in pain impairment on a numeric scale is maximum 0.12 between a person with a low score of lifetime adversity and a person having experienced no adversity. The resilience effect of a low score is less than a half point on the numeric pain impairment scale ranging from 1 to 10. As the quite flat curve in Figure 2 indicates, this is not a clinical relevant effect.
4. Discussion
In this large validation of the CLAM in a Danish population sample, the measure was evaluated as comprehensively translated, and construct validity was assessed as high. Furthermore, pilot interviews showed good acceptability in that questions were confronting but not offensive, straight forward, and easy to answer. The back-translation showed similar item content. Relevance and comprehensiveness of the items based on field testing data were fulfilled as data showed low rates of missing observations, no irrelevant items in terms of zero observations, and the possibility to rate ‘other events’ all reflected good content validity. We replicated results from the US version as quadratic patterns between accumulated lifetime adversity and emotional distress, functional impairment, and pain impairment were found.
This study is the first to validate the CLAM. Our study was comprehensive as 7493 randomly selected persons in a 54-year age span participated. The completion rate of the CLAM was high (98.8%) as only 88 participants failed to fill in the questionnaire, and the completion rate on all outcome measures was high (97.4–99.6%). Participants were randomly obtained from the Danish registers. However, only 29.5% of the invited individuals agreed to participate introducing possible selection bias. Non-responder analysis has not yet been performed, but analysis of non-responders in a similar sample obtained in a similar manner covering the same population area and age span conducted in 2006 showed that non-responders had lower socioeconomic status, lower educational level, and lower personal income (Thuesen et al., 2014). We expect to find similar characteristics in the non-responders of this current cohort indicating that the study group is not fully representative of the general population. Therefore, the reported prevalence of each adverse life event and the prevalence of the seven categories of life events may be underestimated (Tables 2 and 3).
The self-reported measures represent a limitation as this may introduce recall bias. In particular, there may be recall bias regarding age of exposure to an event. Furthermore, even though the field testing showed (from evaluating the missing observations) that the CLAM was acceptable, some of the items presented are confronting, e.g. ‘had sexual relations under force or threat’ and may introduce potential bias due to unwillingness to report on these issues. In the field testing we did not evaluate the distress and/or thoughts and feelings on filling out the CLAM as the field testing of the CLAM was part of a larger study with a comprehensive battery of questionnaires. Therefore we kept it to the items of the original version of the questionnaire. However, for some individuals there may be perceived distress after filling out such a questionnaire. Still, in the phase of pilot testing we interviewed the participants regarding their thoughts and feelings on the CLAM. Overall the pilot participants felt that the questionnaire was touching very important issues. Furthermore, they overall thought that some of the questions were somewhat intrusive but did not feel that it was too much or did not feel that they were incapable of filling out the questionnaire due to contemporary perceived distress. When calculating the sum score for the CLAM.
We conservatively counted errors and missings to having no events. This is a limitation as we have an underestimation in our cumulated score. Back-translation was carried out after the field test, which is not in line with procedures of translation (Beaton, Bombardier et al. 2000; World Health Organization, 2018), and the option of making modifications based on the back-translation before field testing was therefore not present. However, there were only few comments and disagreements in the expert committee, and the author approved the back-translation with only few comments.
We made modifications to the original design of the US version and this might have jeopardized cross-cultural validation. This may be the case with the shortening of the introduction or simplifying the layout. However, the modifications may have improved the measure, and hypothesis testing showed that we could replicate results from the US measure implying that the construct measured is retained.
Some events were rare in this sample compared to the US sample in terms of lower rates of violence, social/environmental stress, and disaster. During an 11-year period from 2006 to 2016, there was an average manslaughter rate per year of 0.84 per 100.000 inhabitants according to Statistics Denmark (Statistics Denmark, 2018), while the average rate per year in the same period was 5.0 (UCR FBI US Government, 2016) in the US. The fact that we added ‘seriously’ in item 6 and 7 and ‘violently pushed’ in item 33 could have reduced the number of violent events registered as the wording may have limited the registrations. The lower rate of social/environmental stress in Denmark could be due to socio-demographic differences between the Danish and US cohorts. The fact that non-responders in our sample may have lower socioeconomic status than responders could also influence the results. Natural disasters in Denmark are unusual. Occasionally, Denmark experiences storms that cause flooding but not phenomena such as typhoons, tornados, or earthquakes, so natural disasters are exceptional. Even if these events are rare in Denmark, it is a significant event in your life should you experience one of these, so they are relevant to include in the measure. We would not expect great differences between the countries in consideration to most items e.g. grief, relational issues, death of relatives, or illness. However, we would expect differences on a few items e.g. higher levels of experience of disaster or violence in the US as stated above. Therefore we would expect the sum score to be slightly larger in the US sample than our sample.
Some events could not be categorized by participants, and they chose to fill in the ‘other’ category (Table 4). In particular, ‘miscarriage’ (n = 47) could not be placed under any other item. Use of fertility treatment has grown and therefore also the possibility of miscarriage. When considering applying additional items to the measure, ‘miscarriage’ would be one of them. We recommend that ‘miscarriage’ is added as an additional item in the questionnaire. Also adding ‘raising a handicapped child’ could be considered since the item ‘serious illness of a loved one’ is not viewed as fulfilling by the participants. Furthermore, events that nearly happened, regardless they did not, still affect the individual, and hence items such as near death experience or suicide attempts of loved ones could be important events to add. Lastly, bullying could be placed under the item ‘been shamed, embarrassed or told repeatedly that you are no good’. We recommend this particular modification of the questionnaire placing bullying under item 34, i.e. ‘been shamed, bullied, embarrassed or told repeatedly that you are no good’. Participants in the pilot testing also pointed out that the concept of bullying was missing in the measure. However, in the evaluation of comprehensiveness, the measure still shows good content validity as it is possible to report ‘other’ experiences, and therefore all events are included.
With respect to the item ‘got divorced yourself’, participants from the pilot test stated that it could be a problem if a break-up from a cohabiting partner was not included as many people in Denmark are lifelong cohabitants but not married. The expert committee agreed to alter the item to ‘divorced (marriage or cohabitant)’. The back-translation inevitably came out differently than the original, and the author stated that in English, the term ‘divorce’ was incorrect for that situation. However, we believe that the rewording on this item makes the comprehensiveness better for the measure.
Regarding the item 37 ‘unwanted pregnancy’, the percentage of missing observations was 5.7%. Two thirds of the missing observations on this item were men, indicating that some males did not know how to apply this question to their life. One solution could be to target the question per gender as it may be difficult for men to provide an answer to this item. However, the questionnaire may be perceived as taxing due to the fact that you have to recall your age for every experience, and additional complication of the questionnaire may not be beneficial. Furthermore, we believe that males can experience an ‘unwanted pregnancy’ i.e. their girlfriend being pregnant and they themselves not wanting the child. Still the rate of missings on this item is not unacceptably high (5.7%) implicating that 94.3% of the cohort has been able to provide an answer to the item. Therefore we recommend keeping the item as it is and then have to accept a certain amount of unavoidable missings on this item.
A statistically significant quadratic relationship between lifetime adversity and poor outcome was found in this study supporting the ‘stress-inoculation theory’, interpreted as a resilience effect when experiencing a low number of adverse life events, as was also found by Seery et al. in their studies (Seery et al., 2010a, 2010b). We have to point out that research within resilience and the findings within this area are not an attempt to disparage the negative effects of a lifetime of great adversity, but it also backs up the findings of several studies showing that high levels of negative life stress are associated with poor mental health later in life, i.e. the one theory does no preclude the other. In our study we also found the link between poor outcome and a high number of experienced negative life events supporting the dose-response theory. Nevertheless, regarding the finding of a resilience effect, we examined the clinical relevance of these results. Finding only very little protective effect of low adversity score versus no adversity experience leaves us with no clinical protective effect as the differences are so small. Research within resilience takes two approaches in the explanation of outcome variance, one is variable-focused using multivariate statistics to test associations between the degree of adversity and outcome, the other is person-focused comparing groups of people with different profiles (Masten, 2001). In this study, a variable-focused approach was taken. Taking our findings into consideration, future examinations of the clinical effect of potential resilience of a low score on the CLAM might benefit from a person-focused rather than a variable-focused approach. This study brings to the research field a meticulous evaluation and validation of a lifetime adversity measure which examines cumulative effect allowing for both measurement of lifetime adversity and childhood adversity. Furthermore, a checklist approach that is free from individual appraisal and solely based on objective count of events experienced. This measure allows for detailed data collection on adversity in large cohorts.
Appendix 1
A full copy of the Danish version of the questionnaire can be retrieved on request from the authors.
Modifications from the original version to the Danish version
[a] Layout was changed; in the Danish version it was only possible to fill in the possible number of exposure to an event. E.g. you could only fill in your mother’s death once. [b] Layout was changed; participants could fill in either specific age (up to three options) or age interval (one option). In the original version there was four options altogether, with options to fill in either four specific age points or four age intervals or a mix [c] The introduction was shortened [d] Item order of question six and seven was interchanged due to comments from the interviewed participants in the pilot testing. Participants were confused that ‘witnessed someone being injured or killed’ came before ‘witnessed family member being injured or killed’ as there might be overlap. The expert committee decided to put the family member version before the broader version. [e] In item six and seven the word ‘seriously’ was added, i.e. ‘witnessed family member being seriously injured or killed’. The expert committee agreed on this as in Danish an injury could also be minor hand injury, an ankle sprain etc. The original author was contacted and approved the addition as injury has the same ambiguity in English and saw the addition as an improvement as it better fitted the intention behind the item. [f] In item 18 and 19 we did not give the option to fill in the relationship of the one lost to suicide or homicide. [g] In the original version item 20 said ‘got divorced yourself’. The pilot test interviews revealed that we should take into consideration that nowadays people are often cohabiting without being married. The expert committee agreed to alter the item to ‘Divorced (marriage or cohabitant)’. The back-translation inevitable came out differently than the original, and the author stated that it had a different meaning and the term ‘divorce’ is not used for that situation (break-up of a relationship with a cohabitating partner) in English. [h] In item 33 the word ‘violently’ was added, i.e. ‘been hit or violently pushed by your partner’ as in Danish ‘pushed’ could be understood as a somewhat weak term. The author approved of the addition and in the back-translation the wording inevitable came out differently but the author evaluated that the meaning of the sentences were very similar. [i] It was only possible to fill in one other/unnamed event as opposed to the original where there were two options of unnamed events.
Back translation
The back-translation showed some minor inconsistencies with no conceptual errors (evaluated by the expert committee and the author) and two items showed inconsistency that altered the concept. [a] Item 10 ‘had combat experience’ in the back-translation it was worded ‘participated in acts of war’. The author agreed with the expert committee that ‘acts of war’ seemed more ambiguous than ‘combat experience’ and this item seemed potentially different regarding the meaning of the item. [b] Item 20 ‘Got divorced yourself’ in the back-translation it was worded ‘Divorced (marriage or cohabitant)’. This inconsistence was deliberate as the pilot test interviews revealed that we should take into consideration that nowadays people are cohabitant and often not married. The expert committee agreed to alter the item. The author stated that it has a different meaning and the term ‘divorce’ is not used for that situation (break-up of a relationship with a cohabitating partner) in English. However, this may not be a conceptual error as it was the intension to capture the concept of divorce in a board perspective not solely in a legal way.
Process of correction of errors in data
[a] Indicated age higher than age when completing questionnaire was set to missing [b] Only start or end age are indicated in age interval then (1) if any age was indicated in the non-interval column then the age point indicated in age interval was set to missing or (2) if no age was indicated in the non-interval column then start or end age indicated in age interval was kept unaltered and counted in the sum score [c] Indicated start age in age interval was higher than end age then (1) if any age was indicated in the non-interval column then age points indicated in age interval were set to missing or (2) if no age was indicated in the non-interval column then end age indicated in age interval was kept unaltered and counted in the sum score and start age was set to missing [d] Indicated age <10 years old was set to missing regarding item 11 (death of your spouse/partner), item 16 (death of your child), item 20 (got divorced yourself), item 33 (been hit or pushed by your spouse/partner), item 37 (had an unwanted pregnancy) [e] Indicated age >18 years old was set to missing regarding item 30 (were neglected as a child by your parents), 31 (being physically harmed as a child), 32 (witnessed violence between your parents as a child). [f] Indicated age in the non-interval column was set to missing if included in the age interval.
Funding Statement
This study was supported by The Lundbeck Foundation under Grant number R155-2013-14070, The Tryg Foundation under Grant number 7-11-0213, The Jascha Foundation under Grant number 6187, and The Danish Rheumatism Association under Grant number R144-A4180. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
We would like to thank the original author of the CLAM, Mark Seery, who has been very helpful during the translation process. We would also like to thank translators and members of the expert committee Charlotte Rask, Lena Bering, Lisbeth Frostholm, Majbritt Mostrup Pedersen, Malene Skjøth, Per Fink, and Peter Lambourne for their skillful participation in this study. This study was a part of the Danish study of Functional Disorders (DanFunD). The DanFunD scientific management group consists of Professor Torben Jørgensen (PI), Professor Per Fink, PhD Lene Falgaard Eplov, PhD Michael Benros, PhD Susanne Brix Pedersen, PhD Betina Heinsbæk Thuesen, and DanFunD scientific officer PhD Thomas M. Dantoft.
Disclosure statement
No potential conflict of interest was reported by the authors.
Data availability statement
Raw data were generated at Center for Clinical Research and Prevention, Bispebjerg and Frederiksberg Hospital, Capital Region of Denmark. Derived data supporting the findings of this study are available from the corresponding author Tina Birgitte Wisbech Carstensen on request.
References
- Abravanel, B. T., & Sinha, R. (2015). Emotion dysregulation mediates the relationship between lifetime cumulative adversity and depressive symptomatology. Journal of Psychiatric Research, 61, 89–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions (1st ed.). Thousand Oaks: Sage. [Google Scholar]
- Aseltine, R. H., Jr, & Kessler, R. C. (1993). Marital disruption and depression in a community sample. Journal of Health and Social Behavior, 34(3), 237–251. [PubMed] [Google Scholar]
- Beaton, D. E., Bombardier, C., Guillemin, F., & Ferraz, M. B. (2000). Guidelines for the process of cross-cultural adaptation of self-report measures. Spine, 25(24), 3186–3191. [DOI] [PubMed] [Google Scholar]
- Breslau, N., Kessler, R. C., Chilcoat, H. D., Schultz, L. R., Davis, G. C., & Andreski, P. (1998). Trauma and posttraumatic stress disorder in the community: The 1996 Detroit area survey of trauma. Archives of General Psychiatry, 55(7), 626–632. [DOI] [PubMed] [Google Scholar]
- Brown, G., & Harris, T. (1978). Social origins of depression: A study of psychiatric disorders in women. New York, NY: Free Press. [Google Scholar]
- Coolican, H. (ed). (1999). Research methods and statistics in psychology (3rd ed.). London, Great Britain: Hodder and Stoughton. [Google Scholar]
- Dantoft, T. M., Ebstrup, J. F., Linneberg, A., Skovbjerg, S., Madsen, A. L., Mehlsen, J., … Jorgensen, T. (2017). Cohort description: The Danish study of functional disorders. Clinical Epidemiology, 9, 127–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Vet, H. C. W., Terwee, C. B., Mokkink, L. B., & Knol, D. L. (eds). (2011). Measurement in medicine. A practical guide. Cambridge, UK: Cambridge University Press. [Google Scholar]
- Derogatis, L. R., Lipman, R. S., & Covi, L. (1973). SCL-90: An outpatient psychiatric rating scale–Preliminary report. Psychopharmacology Bulletin, 9(1), 13–28. [PubMed] [Google Scholar]
- Diamantopoulos, A., Riefler, P., & Roth, K. (2008). Advancing formative measurement models. Journal of Business Research, 61, 1203–1218. [Google Scholar]
- Dienstbier, R. A. (1989). Arousal and physiological toughness: Implications for mental and physical health. Psychological Review, 96(1), 84–100. [DOI] [PubMed] [Google Scholar]
- Fink, P., Ornbol, E., Hansen, M. S., Sondergaard, L., & De Jonge, P. (2004a). Detecting mental disorders in general hospitals by the SCL-8 scale. Journal of Psychosomatic Research, 56(3), 371–375. [DOI] [PubMed] [Google Scholar]
- Fink, P., Ornbol, E., Huyse, F. J., De Jonge, P., Lobo, A., Herzog, T., … Hansen, M. S. (2004b). A brief diagnostic screening instrument for mental disturbances in general medical wards. Journal of Psychosomatic Research, 57(1), 17–24. [DOI] [PubMed] [Google Scholar]
- Gerber, M. M., Frankfurt, S. B., Contractor, A. A., Oudshoorn, K., Dranger, P., & Brown, L. A. (2018). Influence of multiple traumatic event types on mental health outcomes: Does count matter? Journal of Psychopathology and Behavioral Assessment, 40(4), 645–654. [Google Scholar]
- Holman, E. A., Silver, R. C., & Waitzkin, H. (2000). Traumatic life events in primary care patients: A study in an ethnically diverse sample. Archives of Family Medicine, 9(9), 802–810. [DOI] [PubMed] [Google Scholar]
- Holmes, T. H., & Rahe, R. H. (1967). The social readjustment rating scale. Journal of Psychosomatic Research, 11(2), 213–218. [DOI] [PubMed] [Google Scholar]
- Keinan, G., Shrira, A., & Shmotkin, D. (2012). The association between cumulative adversity and mental health: Considering dose and primary focus of adversity. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 21(7), 1149–1158. [DOI] [PubMed] [Google Scholar]
- Liu, H., Prause, N., Wyatt, G. E., Williams, J. K., Chin, D., Davis, T., … Myers, H. F. (2015). Development of a composite trauma exposure risk index. Psychological Assessment, 27(3), 965–974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lloyd, D. A., & Turner, R. J. (2008). Cumulative lifetime adversities and alcohol dependence in adolescence and young adulthood. Drug and Alcohol Dependence, 93(3), 217–226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masten, A. S. (2001). Ordinary magic. Resilience processes in development. The American Psychologist, 56(3), 227–238. [DOI] [PubMed] [Google Scholar]
- Mayo, D., Corey, S., Kelly, L. H., Yohannes, S., Youngquist, A. L., Stuart, B. K., … Loewy, R. L. (2017). The role of trauma and stressful life events among individuals at clinical high risk for psychosis: A review. Front Psychiatry, 20(8), 55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mokkink, L. B., Terwee, C. B., Patrick, D. L., Alonso, J., Stratford, P. W., Knol, D. L., … De Vet, H. C. (2010). The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Quality of Life Research: an International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 19(4), 539–549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robins, L., Helzer, J., Croughan, J., Williams, J., & Spitzer, R. (eds). (1981). Diagnostic interview scedule: Version III. Roskville, MD: National Institute of Mental Health. [Google Scholar]
- Seery, M. D. (2011). Resilience a silver lining to experiencing adverse life events? Current Directions in Psychological Science, 20(6), 390–394. [Google Scholar]
- Seery, M. D., Holman, E. A., & Silver, R. C. (2010a). Whatever does not kill us: Cumulative lifetime adversity, vulnerability, and resilience. Journal of Personality and Social Psychology, 99(6), 1025–1041. [DOI] [PubMed] [Google Scholar]
- Seery, M. D., Leo, R. J., Holman, E. A., & Silver, R. C. (2010b). Lifetime exposure to adversity predicts functional impairment and healthcare utilization among individuals with chronic back pain. Pain, 150(3), 507–515. [DOI] [PubMed] [Google Scholar]
- Shrira, A., & Litwin, H. (2014). The effect of lifetime cumulative adversity and depressive symptoms on functional status. The Journals of gerontology.Series B, Psychological Sciences and Social Sciences, 69(6), 953–965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- STATA . (2003). STATA 15.0. 4905 Lakeway drive college station, Texas: Author. Anonymous. [Google Scholar]
- Statistics Denmark . (2018, February 2). Statistikbanken. Retrieved from http://www.statistikbanken.dk/statbank5a/
- Thuesen, B. H., Cerqueira, C., Aadahl, M., Ebstrup, J. F., Toft, U., Thyssen, J. P., … Linneberg, A. (2014). Cohort profile: The Health2006 cohort, research centre for prevention and health. International Journal of Epidemiology, 43(2), 568–575. [DOI] [PubMed] [Google Scholar]
- Turner, R. J., & Lloyd, D. A. (1995). Lifetime traumas and mental health: The significance of cumulative adversity. Journal of Health and Social Behavior, 36(4), 360–376. [PubMed] [Google Scholar]
- UCR FBI US Government . (2016). Crime in the USA. Retreived from https://ucr.fbi.gov/crime-in-the-u.s/2016/crime-in-the-u.s.-2016/tables/table-1
- Ware, J., Jr, Kosinski, M., & Keller, S. D. (1996). A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Medical Care, 34(3), 220–233. [DOI] [PubMed] [Google Scholar]
- Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., & Keane, T. M. (2013). The life events checklist for DSM-5 (LEC-5). Instrument available from the National Center for PTSD at www.ptsd.va.gov. Retrieved from https://www.ptsd.va.gov/professional/assessment/te-measures/life_events_checklist.asp
- World Health Organization . (2018, May 29). Research Tools. Retrieved from http://www.who.int/substance_abuse/research_tools/translation/en/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Citations
- Statistics Denmark . (2018, February 2). Statistikbanken. Retrieved from http://www.statistikbanken.dk/statbank5a/
- UCR FBI US Government . (2016). Crime in the USA. Retreived from https://ucr.fbi.gov/crime-in-the-u.s/2016/crime-in-the-u.s.-2016/tables/table-1
- Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., & Keane, T. M. (2013). The life events checklist for DSM-5 (LEC-5). Instrument available from the National Center for PTSD at www.ptsd.va.gov. Retrieved from https://www.ptsd.va.gov/professional/assessment/te-measures/life_events_checklist.asp
Data Availability Statement
Raw data were generated at Center for Clinical Research and Prevention, Bispebjerg and Frederiksberg Hospital, Capital Region of Denmark. Derived data supporting the findings of this study are available from the corresponding author Tina Birgitte Wisbech Carstensen on request.