

Abstract
Background:
Vitamin C as a supplement to treat hypertension has been proposed. However, it remains controversial whether vitamin C can improve blood pressure in patients with primary hypertension.
Objectives:
To analyze the effect of vitamin C (VitC) supplementation on systolic (SBP) and diastolic (DBP) blood pressure in patients with essential hypertension.
Methods:
We searched the Chinese Knowledge Infrastructure, VIP Database for Chinese Technical Periodicals, WANFANG Data, Cochrane Library, National Library of Medicine's PubMed, EMBASE, and other databases until June 2019. Eight RCTs involving 614 participants were analyzed. SBP and DBP before and after VitC supplementation were compared between the intervention and control groups. The risk of bias of individual studies was assessed using the Cochrane Collaboration risk of bias tool. Two reviewers selected studies independently of each other. The Cochrane Collaboration Review Manager 5.3 was used to perform the meta-analysis.
Results:
There was a significant difference in the change of SBP (weighted mean difference [WMD] = −4.09; 95% confidence interval [CI] −5.56, −2.62; P < .001) and DBP (WMD = −2.30; 95% CI −4.27, −.331; P = .02) between the groups. Further, there was a significant difference in the SBP (WMD = -3.75, 95% CI -6.24, -1.26, P = .003) and DBP (WMD = −3.29, 95% CI −5.98, −.60, P = .02) for the subgroup with an age ≥60 years and that with ≥35 participants. In the subgroup analysis, result for SBP with a study duration ≥6 weeks was statistically significant different (WMD = −4.77; 95% CI −6.46, −3.08; P < .001). For an intervention dose of VitC ≥500 mg daily, SBP was statistically significant (WMD = −5.01; 95% CI −8.55, −1.48; P = .005).
Conclusion:
VitC supplementation resulted in a significant reduction of blood pressure in patients with essential hypertension.
Keywords: arterial blood pressure, essential hypertension, meta-analysis, vitamin C
1. Introduction
One in 4 adults worldwide suffers from high blood pressure, and this ratio is expected to increase to 29% by 2025.[1] The prevalence of hypertension is 37.3% in developed countries and 22.9% in developing countries. Among the population with hypertension, more than 90% have essential hypertension, which makes this type of hypertension without a secondary cause a major global chronic non-communicable disease.[2] Although the pathogenesis of essential hypertension is not entirely clear, recent studies have indicated that oxidative stress and vascular endothelial cell injury might be important factors.[3,4]
Endothelial cell dysfunction, a characteristic of essential hypertension, is caused by damage to these cells and the release of large amounts of superoxide anions.[5] It is closely related to the development of vascular disease and has been found to promote hypertension and cardiovascular and cerebrovascular diseases.[6–9] Taddei et al[10] noticed abnormal endothelium-dependent vasodilation in descendants of patients with essential hypertension and concluded that endothelial dysfunction might facilitate the development of hypertension. An investigation of the blood pressure of individuals with abnormal L-arginine uptake and a family history of hypertension further confirmed that changes in endothelial function may lead to the development of essential hypertension.[11]
Vitamin C (VitC), or ascorbic acid, is frequently found in fruits, vegetables, vitamin supplements, energy drinks, formulated breakfasts, and dietary cereals.[12] As an essential vitamin involved in human metabolism, it possesses the ability to remove superoxide anions and prevent the formation of peroxynitrite as well as improve vascular endothelial function.[13–16] Numerous clinical studies have assessed the effect of VitC supplementation on blood pressure levels.[17–19] The results were inconsistent, probably because of their heterogeneous methods and the fact that they were small randomized controlled trials (RCTs). Some findings were even contradictory, and no conclusion on the effect of VitC on hypertension has been reached yet. Consequently, we performed a meta-analysis to systematically analyze the effects of VitC supplementation on essential hypertension with the aim to establish current evidence for the role of this intervention.
2. Methods
2.1. Research strategy
We searched the National Library of Medicine's PubMed, Cochrane Library, EMBASE, China National Knowledge Infrastructure, VIP Database for Chinese Technical Periodicals, and WANFANG databases for studies published before June 2019. The search terms were as follows: blood pressure, hypertension, hypertensive, primary hypertension, essential hypertension, vitamin C, ascorbic acid, and RCTs. Two independent reviewers selected and screened all results, and if they disagreed, we asked a third reviewer for his/her advice. This meta-analysis complies with the Reviews and Meta-Analyses (PRISMA) statement for reporting items for systematic reviews and meta-analyses.[20]
2.2. Eligibility criteria
The inclusion criteria for this systematic review were as follows:
-
1)
studies with a RCT design related to the therapeutic effect of VitC;
-
2)
the included subjects were explicitly diagnosed with essential hypertension based on laboratory findings, clinical signs, or reported symptoms;
-
3)
the effects of VitC on systolic (SBP) and diastolic (DBP) blood pressure were reported;
-
4)
VitC was included in the trial as a supplement and the study had a control group; and
-
5)
the dose of VitC was >200 mg.
The exclusion criteria were as follows:
-
1)
duplicate publications;
-
2)
non-interventional study designs, such as a case
-
3)
-control study, cohort study, cross-sectional study, case reports and experiences, theory research, and reviews; and
-
4)
non-clinical tests and animal experiments.
2.3. Data extraction
The following information was extracted:
-
1)
participants’ basic characteristics, including mean age, sex, and treatment with antihypertensive medications;
-
2)
detailed descriptions of how patients’ blood pressure was measured, such as their position (e.g., seated, lying, or standing), the location, device used (e.g., oscillometric monitor, sphygmomanometer cuff; sphygmomanometer, etc.);
-
3)
mean pretreatment SBP and DBP; and
-
4)
mean SBP, DBP, and plasma VitC concentration after the trial.
2.4. Risk of bias assessment
The risk of study bias was assessed using the Cochrane Collaboration risk of bias tool. The risk of bias was evaluated with regard to the following aspects: the method of generating random sequences, allocation of hidden methods, application of the blinding method, incomplete results, selective reporting of results, and other bias. Funnel diagrams were used to detect publication bias.
2.5. Statistical analysis
2.5.1. Extracting and merging data
The Cochrane Collaboration Review Manager 5.3 software was used to extract relevant dichotomous or continuous data from the literature for analysis. The risk ratio was calculated for dichotomous data, whereas the weighted mean difference (WMD) and standard deviations (SD) were calculated for continuous variables. The corresponding 95% confidence interval (CI) and forest plots were used in both cases. In our meta-analysis, we used SD values when data were in the same unit of measure. When they were in different units of measure, we performed a conversion. The chi-square and I2 (inconsistency) tests were used to detect heterogeneity. A P value < .10 or I2 > 50% indicated a significant difference in heterogeneity. The fixed-effect model was used when P > .10 and I2 < 50%, and the random-effect model was used when P < .10 or I2 ≥ 50%.
2.5.2. Data conversion
Mean changes in SBP and DBP were used as indicators to evaluate the effect of VitC in the intervention group and of the placebo in the control group. When there was no explicit reference to SBP or DBP in the studies, we calculated the mean and SD of ΔSBP and ΔDBP using the following formulae.
-
1)If the number of samples (n) and standard error (SE) were known, the SD was calculated as follows:

- 2)
3. Results
3.1. Study selection
We screened 552 study reports, of which 156 were excluded because of duplicate publications. After reading the title and abstract, 212 articles were further excluded, and 184 articles were retained. Among them, 112 articles did not meet the inclusion criteria, 32 studies were improperly compared, and for 32 studies, we could not extract data. Finally, 8 RCTs comprising 614 participants were included. The PRISMA flow diagram is shown in Figure 1.
Figure 1.
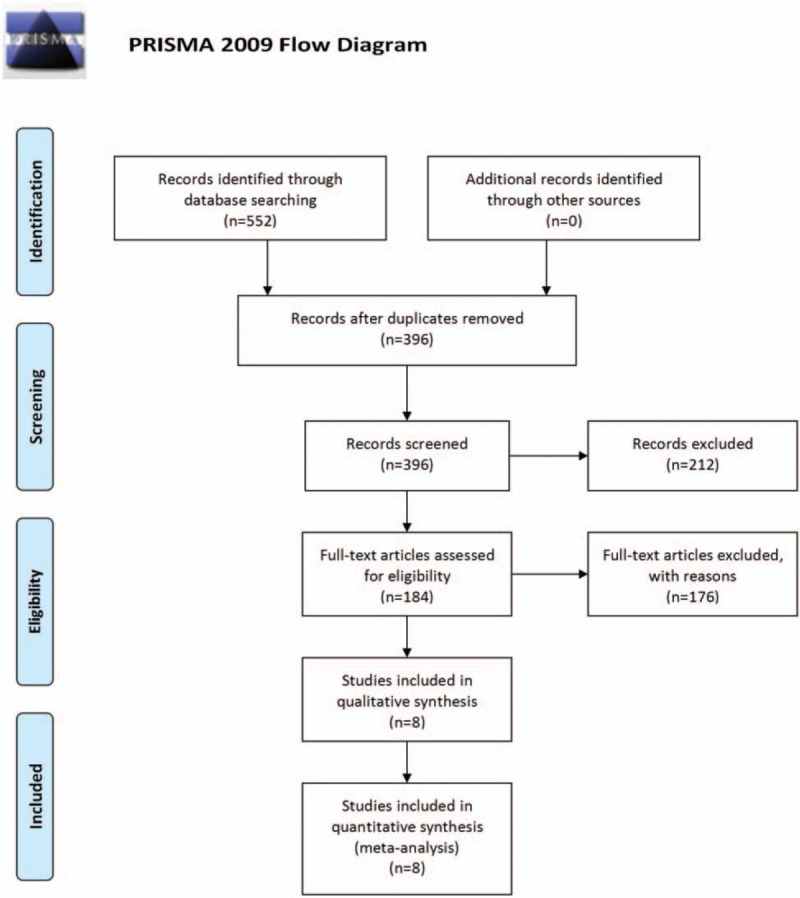
Study selection procedure according to the PRISMA statement.[20] PRISMA = Preferred Reporting Items Systematic Reviews and Meta-Analyses.
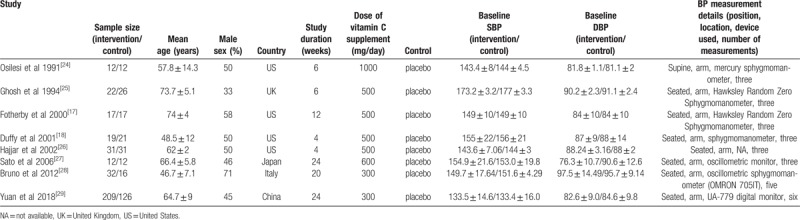
3.2. Study characteristics
The principal study characteristics are summarized in Table 1. The 8 studies were published between 1991 and 2018. Overall, 614 participants were included. The number of participants in the individual studies ranged from 12 to 480. Participants’ mean age ranged from 46 to 78 years. The duration of the intervention varied from 4 to 24 weeks. All participants had essential hypertension. The average SBP and DBP of the participants ranged from 143 to 173 mmHg and from 76 to 97 mmHg, respectively. The supplementary dose of VitC in the treatment group varied between 300 and 1000 mg/dL.
Table 1.
Randomized controlled trials included in the systematic review of the effects of vitamin C on essential hypertension.
3.3. Quality assessment
Table 2 provides an overview of the risk of bias for the included studies. All included studies used a double-blind approach and reported the number of dropouts. Most trials reported allocation concealment and random allocation but did not mention the specific method used. Selective reporting was unbiased, but without any description to ensure the existence of other biases. Few trials reported adverse events.
Table 2.
Results of the Cochrane Collaboration risk of bias tool for assessing the risk of bias in the 8 randomized controlled trials included in the systematic review of the effect of vitamin C supplementation on essential hypertension.

3.4. Study results
3.4.1. Main results
Figures 2 and 3 show the forest plots of the SBP and DBP, respectively. There was a significant difference in SBP between the intervention and control groups (WMD = −4.09; 95% CI −5.56, −2.62; P < .001). There was no indication of heterogeneity (P = .15, I2 = 35%, fixed-effect model).
Figure 2.
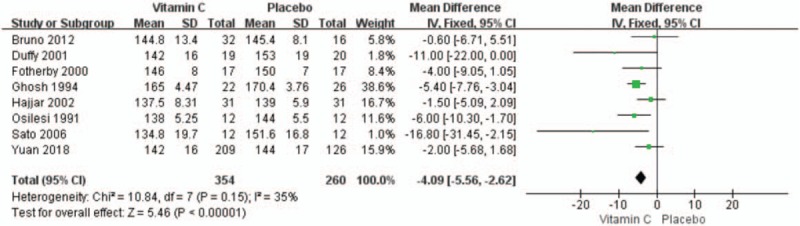
Forest plot of the comparison of mean systolic blood pressure in the 8 randomized control trials on the effect of vitamin C on essential hypertension. CI = confidence interval, SD = standard deviation.
Figure 3.
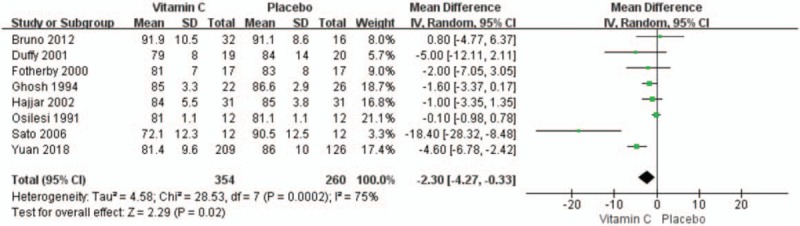
Forest plot of the comparison of mean diastolic blood pressure in the 8 randomized control trials on the effect of vitamin C on essential hypertension. CI = confidence interval, SD = standard deviation.
There was a significant difference in DBP between the intervention and control groups (WMD = −2.30; 95% CI −4.27, −.33; P = .02). There was an indication of heterogeneity (P = .0002; I2 = 75%; random-effect model).
3.4.2. Subgroup results
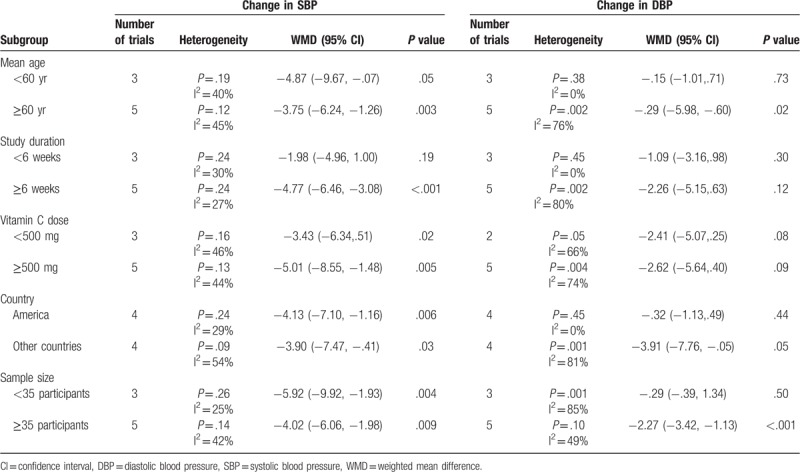
There was a significant difference in the SBP (WMD = −3.75, 95% CI −6.24, −1.26, P = .003) and DBP (WMD = −3.29, 95% CI −5.98, −.60, P = .02) for the subgroup with an age ≥60 years. Combined results of five studies showed that ≥35 participants did significantly reduce DBP (WMD = −2.27, 95% CI −3.42, −1.13; P < .001) with relatively low heterogeneity (I2 = 49%, P = .10). In the subgroup analysis, result for SBP with a study duration ≥6 weeks was statistically significant different (WMD = −4.77; 95% CI −6.46, −3.08; P < .001), with low heterogeneity (I2 = 27%, P = .24). For an intervention dose of VitC ≥500 mg daily, SBP was statistically significant (WMD = −5.01; 95% CI −8.55, −1.48; P = .005), with relatively low heterogeneity (I2 = 44%, P = .13). Results of the analyses of SBP and DBP for different subgroups of the study populations are listed in Table 3.
Table 3.
Results of ΔSBP and ΔDBP in different study population subgroups from the 8 randomized controlled trials on the effect of vitamin C supplementation in essential hypertension.
3.4.2.1. SBP
There was a significant difference in SBP (WMD = −3.75; 95% CI −6.24, −1.26; P = .003) and DBP (WMD = −3.29; 95% CI −5.98, −.60; P = .02) for the subgroups of age ≥60 years or sample of ≥35 participants compared with the control group. Compared with the control group, differences in the SBP for the subgroup with a study duration ≥6 weeks (WMD = −4.77, 95% CI −6.46, −3.08, P < .001) and that with a VitC dose ≥500 mg (WMD = −5.01, 95% CI −8.55, −1.48; P = .005) were statistically significant.
3.4.2.2. DBP
Compared with the control groups, the subgroup analysis for DBP showed that only the subgroup with a sample of ≥35 participants had a significantly different DBP (WMD = −2.27; 95% CI −3.42, −1.13; P < .001).
3.5. Publication bias
The publication bias of the 8 RCTs was evaluated with a funnel plot. Figure 4 shows that the publication bias across the studies was small.
Figure 4.
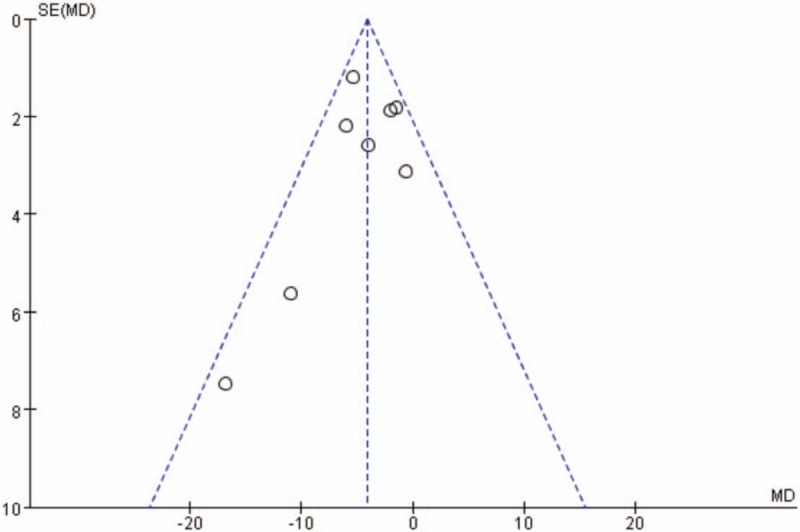
Funnel plot of the 8 randomized control trials on the effect of vitamin C on essential hypertension.
4. Discussion
4.1. Effect of VitC supplementation on essential hypertension
VitC is a vitamin found in fresh fruits and vegetables and is an essential water-soluble antioxidant in the human body.[30] According to a review by Taddei et al[31] in 1998, VitC might improve endothelial-dependent vasodilation in patients with essential hypertension and reverse the nitric oxide synthase inhibitor NG-monomethyl-L-arginine 1. Other studies also attempted to explain the possible mechanism of VitC efficacy in the treatment of essential hypertension.[32,33] At present, the main theory is that VitC increases intracellular concentrations of tetrahydrobiopterin, an endothelial nitric oxide synthase co-factor that promotes the production of nitric oxide, which is a potent vasodilator.[34] There is also evidence that VitC enhances the biological activity of nitric oxide.[35] Furthermore, VitC supplementation improved endothelial function in the brachial and coronary arteries in short-term human trials.[36] All aforementioned reports suggest that VitC is an effective preventive and therapeutic supplement in essential hypertension.
However, all studies so far have shown large individual differences and arrived at different conclusions. In several previous meta-analyses,[37,38] the main focus was on the relationship between antioxidants and blood pressure. The present meta-analysis is the first quantitative review of RCTs evaluating the effect of VitC supplementation on essential hypertension. Our meta-analysis included 8 studies with 614 participants and our results showed that VitC supplementation can significantly reduce SBP and DBP in patients with essential hypertension. The meta-analysis by Juraschek et al[39] in 2012 included patients treated with VitC, vitamin E, or magnesium, whereas we focused on participants receiving only VitC. This difference may be the reason why the two studies came to different conclusions.
In the analysis of the subgroup of patients aged ≥60 years, we found a significant difference in SBP and DBP after VitC supplementation as compared to those before supplementation. The reason for this difference is likely the increasing prevalence of hypertension with age. With age, excessive production of reactive oxygen species is observed, resulting in the inability to scavenge all free oxygen radicals and consequently, a decrease in endothelial function.
In the ≥60-year-old subgroup, differences in SBP and DBP between the observation and control groups were statistically significant. The results from Jaja et al's[40] report in 2008 showed that both 6-week and long-term oral VitC in appropriate doses reduced blood pressure levels. These results are consistent with those of our subgroup analyses, where we found a significant difference in SBP between the duration of treatment, VitC dose, country, and sample size.
In the review by Cheng et al[41] in 2017, blood pressure variability also increased with age. This result is because an increase in stiffness of the large arteries is accompanied by early wave reflection, which results in a significant augmentation of the central SBP in the late systole and further adds to the increased cardiac afterload. Blood pressure variability is closely related to the occurrence of heart disease, which can lead to injury of other target organs and increase the risk of vascular and degenerative diseases. Studies have confirmed that blood pressure variability increases the risk of cerebral hemorrhage and Alzheimer disease.[42,43]
Recent studies have shown that the mechanisms of blood pressure variability include endothelial dysfunction and arteriosclerosis; oxidative stress is also often involved.[44] Markers of inflammation and endothelial activation are significantly associated with blood pressure variability, although strong evidence has been found that anti-inflammatory and antioxidant therapies protect target organs from the effect of blood pressure variability.[45] These findings corroborate the results of our study in that antioxidant adjuvant therapy with VitC can reduce blood pressure variability in patients with essential hypertension, thereby protecting the target organs.
Although the exact mechanism of the effect of antioxidant therapy on blood pressure remains to be fully elucidated, there is increasing evidence that antioxidant adjuvant therapy can reduce blood pressure in patients with hypertension to protect the target organs. It is hoped that more detailed information about this mechanism will be obtained in future studies.
4.2. Limitations
This study has several limitations. First, in some cases, we had to calculate and transform data, rather than these being provided directly. Second, the dosage of VitC differed between the 8 RCTs, which may have affected the results of this meta-analysis. In addition, language and publication bias limited our study. Finally, this review included only RCT. In future, there is a need for a greater diversity of research included in the analysis, such as multi-centered studies, more rigorous clinical reports, and prospective studies.
4.3. Clinical implications
Aiming at influencing the pathophysiological mechanisms associated with hypertension, prevention and adjuvant therapy efforts focus on the benefits associated with VitC. Several clinical studies are currently investigating the significance of such potential benefits.[42]
Drug therapy alone does not suffice to effectively treat essential hypertension. Multi-factorial interventions, including increased vitamin intake with defined dosages and duration of treatment, may help to ameliorate and manage the various hypertension-associated vascular endothelial phenomena.
5. Conclusions
Our meta-analysis found that VitC supplementation may play an important role in reducing blood pressure in patients with essential hypertension. However, in view of the current level of evidence, large-scale trials should be conducted, and attention should be paid to the evaluation of blood pressure variability.
Acknowledgments
The authors thank Professor Huaien Bu for providing us with important information.
Author contributions
Conceptualization: Yuanyuan Guan, Pengju Dai, Hongwu Wang
Data curation: Yuanyuan Guan, Pengju Dai
Formal analysis: Yuanyuan Guan, Pengju Dai
Investigation: Pengju Dai
Methodology: Yuanyuan Guan, Pengju Dai, Hongwu Wang
Project administration: Hongwu Wang
Software: Yuanyuan Guan
Supervision: Hongwu Wang
Writing – original draft: Yuanyuan Guan
Writing – review & editing: Yuanyuan Guan
Footnotes
Abbreviations: CI = confidence interval, DBP = diastolic blood pressure, PRISMA = Preferred Reporting Items Systematic Reviews and Meta-Analyses, RCT = randomized controlled trial, SBP = systolic blood pressure, SD = standard deviation, SE = standard error, VitC = Vitamin C, WMD = weighted mean difference.
How to cite this article: Guan Y, Dai P, Wang H. Effects of vitamin C supplementation on essential hypertension: A systematic review and meta-analysis. Medicine. 2020;99:8(e19274).
This paper includes all the data that support the results of this study.
This project was supported by the Basic Research on Health Identification of traditional Chinese Medicine in Tianjin Colleges and Universities “Innovation Team Training Plan” (approval number: TD13-5049) during the 13th 5-year plan period.
The authors have no conflicts of interest to disclose.
References
- [1].Task Force for the management of arterial hypertension of the European Society of Hypertension. 2013 ESH/ESC guidelines for the management of arterial hypertension. Blood Press 2013;22:193–278. [DOI] [PubMed] [Google Scholar]
- [2].Bruno RM, Masi S, Taddei M, et al. Essential hypertension and functional microvascular ageing. High Blood Press Cardiovasc Prev 2018;25:35–40. [DOI] [PubMed] [Google Scholar]
- [3].Mittal BV, Singh AK. Hypertension in the developing world: challenges and opportunities. Am J Kidney Dis 2010;55:590–8. [DOI] [PubMed] [Google Scholar]
- [4].Perticone F, Ceravolo R, Pujia A, et al. Prognostic significance of endothelial dysfunction in hypertensive patients. Circulation 2001;104:191–6. [DOI] [PubMed] [Google Scholar]
- [5].Rodrigo R, Libuy M, Feliú F, et al. Oxidative stress-related biomarkers in essential hypertension and ischemia-reperfusion myocardial damage. Dis Markers 2013;35:773–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Deanfield JE, Halcox JP, Rabelink TJ. Endothelial function and dysfunction: testing and clinical relevance. Circulation 2007;115:1285–95. [DOI] [PubMed] [Google Scholar]
- [7].Landmesser U, Drexler H. Endothelial function and hypertension. Curr Opin Cardiol 2007;22:316–20. [DOI] [PubMed] [Google Scholar]
- [8].Landmesser U, Hornig B, Drexler H. Endothelial function: a critical determinant in atherosclerosis? Circulation 2004;109:II27–33. [DOI] [PubMed] [Google Scholar]
- [9].Giannotti G, Doerries C, Mocharla PS, et al. Impaired endothelial repair capacity of early endothelial progenitor cells in prehypertension: relation to endothelial dysfunction. Hypertension 2010;55:1389–97. [DOI] [PubMed] [Google Scholar]
- [10].Taddei S, Virdis A, Mattei P, et al. Defective L-arginine-nitric oxide pathway in offspring of essential hypertensive patients. Circulation 1996;94:1298–303. [DOI] [PubMed] [Google Scholar]
- [11].Schlaich MP, Parnell MM, Ahlers BA, et al. Impaired L-arginine transport and endothelial function in hypertensive and genetically predisposed normotensive subjects. Circulation 2004;110:3680–6. [DOI] [PubMed] [Google Scholar]
- [12].Lykkesfeldt J, Michels AJ, Frei B. Vitamin C. Adv Nutr 2014;5:16–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Granger M, Eck P. Eskin MNA. Dietary Vitamin C in Human Health. New research and developments of water-soluble vitamins. Cambridge: Academic Press; 2018. 281–310. [DOI] [PubMed] [Google Scholar]
- [14].Huang A, Vita JA, Venema RC, et al. Ascorbic acid enhances endothelial nitric-oxide synthase activity by increasing intracellular tetrahydrobiopterin. J Biol Chem 2000;275:17399–406. [DOI] [PubMed] [Google Scholar]
- [15].d’Uscio LV, Milstien S, Richardson D, et al. Long-term vitamin C treatment increases vascular tetrahydrobiopterin levels and nitric oxide synthase activity. Circ Res 2003;92:88–95. [DOI] [PubMed] [Google Scholar]
- [16].Donato AJ, Gano LB, Eskurza I, et al. Vascular endothelial dysfunction with aging: endothelin-1 and endothelial nitric oxide synthase. Am J Physiol Heart Circ Physiol 2009;297:H425–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Fotherby MD, Williams JC, Forster LA, et al. Effect of vitamin C on ambulatory blood pressure and plasma lipids in older persons. J Hypertens 2000;18:411–5. [DOI] [PubMed] [Google Scholar]
- [18].Duffy SJ, Gokce N, Holbrook M, et al. Effect of ascorbic acid treatment on conduit vessel endothelial dysfunction in patients with hypertension. Am J Physiol Heart Circ Physiol 2001;280:H528–34. [DOI] [PubMed] [Google Scholar]
- [19].Block G, Mangels AR, Norkus EP, et al. Ascorbic acid status and subsequent diastolic and systolic blood pressure. Hypertension 2001;37:261–7. [DOI] [PubMed] [Google Scholar]
- [20].Moher D, Liberati A, Tetzlaff J, et al. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol 2005;5:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 2014;14:135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Xu YP, Yu YY, Fu WJ. Introduction of methods for estimating standardized mean difference when missing standard deviation conversion in meta-analysis. Chin J Evidence-Based Cardiovasc Med 2016;8:1412–5. [Google Scholar]
- [24].Osilesi O, Ogunwole JO, Clover EE. Blood pressure and plasma lipids during ascorbic acid supplementation in borderline hypertensive and normotensive adults. Nutr Res 1991;11:405–12. [Google Scholar]
- [25].Ghosh SK, Ekpo EB, Shah IU, et al. A double-blind, placebo-controlled parallel trial of vitamin C treatment in elderly patients with hypertension. Gerontology 1994;40:268–72. [DOI] [PubMed] [Google Scholar]
- [26].Hajjar IM, George V, Sasse EA, et al. A randomized, double-blind, controlled trial of vitamin C in the management of hypertension and lipids. Am J Ther 2002;9:289–93. [DOI] [PubMed] [Google Scholar]
- [27].Sato K, Dohi Y, Kojima M, et al. Effects of ascorbic acid on ambulatory blood pressure in elderly patients with refractory hypertension. Arzneimittelforschung 2006;56:535–40. [DOI] [PubMed] [Google Scholar]
- [28].Bruno RM, Daghini E, Ghiadoni L, et al. Effect of acute administration of vitamin C on muscle sympathetic activity, cardiac sympathovagal balance, and baroreflex sensitivity in hypertensive patients. Am J Clin Nutr 2012;96:302–8. [DOI] [PubMed] [Google Scholar]
- [29].Yuan X, Li X, Ji Z, et al. Effects of vitamin C supplementation on blood pressure and hypertension control in response to ambient temperature changes in patients with essential hypertension. Clin Exp Hypertens 2019;41:414–21. [DOI] [PubMed] [Google Scholar]
- [30].Enstrom JE, Kanim LE, Klein MA. Vitamin C intake and mortality among a sample of the United States population. Epidemiology 1992;3:194–202. [DOI] [PubMed] [Google Scholar]
- [31].Taddei S, Virdis A, Ghiadoni L, et al. Vitamin C improves endothelium-dependent vasodilation by restoring nitric oxide activity in essential hypertension. Circulation 1998;97:2222–9. [DOI] [PubMed] [Google Scholar]
- [32].Rodrigo R, Prat H, Passalacqua W, et al. Decrease in oxidative stress through supplementation of vitamins C and E is associated with a reduction in blood pressure in patients with essential hypertension. Clin Sci (Lond) 2008;114:625–34. [DOI] [PubMed] [Google Scholar]
- [33].Natali A, Sironi AM, Toschi E, et al. Effect of vitamin C on forearm blood flow and glucose metabolism in essential hypertension. Arterioscler Thromb Vasc Biol 2000;20:2401–6. [DOI] [PubMed] [Google Scholar]
- [34].Al-Khudairy L, Flowers N, Wheelhouse R, et al. Vitamin C supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 2017;3:CD011114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Ashor AW, Siervo M, Lara J, et al. Effect of vitamin C and vitamin E supplementation on endothelial function: a systematic review and meta-analysis of randomised controlled trials. Br J Nutr 2015;113:1182–94. [DOI] [PubMed] [Google Scholar]
- [36].Cottone S, Mulè G, Nardi E, et al. Relation of C-reactive protein to oxidative stress and to endothelial activation in essential hypertension. Am J Hypertens 2006;19:313–8. [DOI] [PubMed] [Google Scholar]
- [37].Emami MR, Safabakhsh M, Alizadeh S, et al. Effect of vitamin E supplementation on blood pressure: a systematic review and meta-analysis. J Hum Hypertens 2019;33:499–507. [DOI] [PubMed] [Google Scholar]
- [38].Golzarand M, Shab-Bidar S, Koochakpoor G, et al. Effect of vitamin D3 supplementation on blood pressure in adults: an updated meta-analysis. Nutr Metab Cardiovasc Dis 2016;26:663–73. [DOI] [PubMed] [Google Scholar]
- [39].Juraschek SP, Guallar E, Appel LJ, et al. Effects of vitamin C supplementation on blood pressure: a meta-analysis of randomized controlled trials. Am J Clin Nutr 2012;95:1079–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Jaja SI, Ogungbemi SI, Kehinde MO. Electrocardiographic and blood pressure changes in apparently healthy male subjects following oral, chronic, low-dose vitamin C supplementation and/or change in posture. Nig Q J Hosp Med 2008;18:96–100. [DOI] [PubMed] [Google Scholar]
- [41].Cheng HM, Park S, Huang Q, et al. Vascular aging and hypertension: Implications for the clinical application of central blood pressure. Int J Cardiol 2017;230:209–13. [DOI] [PubMed] [Google Scholar]
- [42].Divani AA, Liu X, Di Napoli M, et al. Blood pressure variability predicts poor in-hospital outcome in spontaneous intracerebral hemorrhage. Stroke 2019;50:2023–9. [DOI] [PubMed] [Google Scholar]
- [43].Lattanzi S, Brigo F, Vernieri F, et al. Visit-to-visit variability in blood pressure and Alzheimer's disease. J Clin Hypertens 2018;20:918–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Lattanzi S, Brigo F, Silvestrini M. Hypertension and arterial stiffness. J Clin Hypertens 2019;21:1481–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Lattanzi S, Vernieri F, Silvestrini M. Blood pressure variability and neurocognitive functioning. J Clin Hypertens (Greenwich) 2018;20:645–7. [DOI] [PMC free article] [PubMed] [Google Scholar]