

Abstract
Objectives
This study aimed to estimate the prevalence of genital, anal and oral HPV infection in Brazil through systematic review and meta-analysis.
Methods
We searched EMBASE, LILACS, MEDLINE, Web of Science and SciELO from inception to December 2018. Original research articles that assessed the prevalence of genital (i.e., cervical, penile), anal and oral HPV infection in Brazil were selected in pairs by independent authors. No sex, age, HPV vaccination, language or date restrictions were applied. HPV prevalence was estimated and stratified according to risk factors population and by geographic area throughout the country. The study prevalence was pooled using a random effects model. Analysis was performed using R (version 3.5.2), packages meta version 4.9–4 and metaphor 2.0–0. This review is registered on PROSPERO under protocol number CRD42016032751.
Results
We identified 3,351 references. After the screening process, 139 of them were eligible for this systematic review (57,513 total participants). Prevalence of cervical HPV was 25.41% (95% CI 22.71–28.32). Additionally, prevalence was 36.21% (95% CI 23.40, 51.33) in the penile region, 25.68% (95%CI 14.64, 41.04) in the anal region, and 11.89% (95%CI 6.26, 21.43) in the oral region. Subgroup analysis showed prevalence in each anatomic site was higher in high-risk populations.
Conclusion
The prevalence of HPV is high in the Brazilian population and varies by population risk and anatomic body site, with lower rates in the oral cavity compared to that in the cervical, penile and anal region. Studies on HPV have primarily been developed to evaluate infection and cancer in the cervical region. There is a profound lack of HPV data in many geographic regions of Brazil and for different anatomic sites.
Introduction
Human papillomavirus (HPV) is a DNA virus from the Papillomaviridae family, comprising over 170 identified types [1]. HPV may infect skin and mucosal membranes among different anatomic sites such as the anogenital region and oral cavity [2]. The global prevalence of HPV infection is approximately 12% with substantial regional variation [3]. In Brazil, previous studies reported a prevalence of genital HPV varying between 10.4 and 72%, depending of sex [4,5], and a prevalence of 6.2% of oropharyngeal HPV [6].
HPV is the most common sexually transmitted infection, with sufficient evidence of its carcinogenic effects at different sites [1,4]. Worldwide, HPV is responsible for 5.1% of the burden of cancer [6] and is present in nearly 100% of cervical tumors, 88% of anal tumors and 50% of penile tumors [4]. In head and neck squamous cell carcinomas, HPV-16 is the most commonly found genotype, while overall HPV prevalence in these lesions is 26% [7].
HPV prevalence varies widely between genders as well as among anatomic sites [8]. The worldwide HPV prevalence varies according to the population analyzed and the status of economic development of the region [4]. Since Brazil is a country with continental proportions and significant socioeconomic diversity, the epidemiology of HPV infection within Brazil might also be impacted by these variables.
The HPV National Vaccination Program in Brazil started in 2014, and it will take time to determine the effect of vaccination on the HPV rates [9]. Understanding the HPV prevalence prior to vaccination will be useful to monitor changes related to the vaccine as well as changes in the distribution of HPV among different areas in Brazil. In addition, obtaining data that could help us make inferences about the HPV-infected population at a national level would facilitate the decision-making process and guide campaigns and public investments in the sexually active population in Brazil.
Therefore, the aim of this systematic review and meta-analysis was to assess the prevalence of genital, anal and oral HPV infection in Brazil to provide support for the Ministry of Health to establish health policies and programs.
Materials and methods
This review has been registered on PROSPERO under protocol number CRD42016032751. This protocol has also been published in a peer reviewed open access journal [10].
Search
We performed the search of the following databases through December 28, 2018 [10]: EMBASE, LILACS, MEDLINE, Web of Science and SciELO using terms as “human papillomavirus”, “HPV”, “prevalence” and “Brazil” (S1 Appendix); we also scanned the reference lists of identified publications for additional studies. Brazilian specialists in the field were contacted to identify unpublished and ongoing studies and we used the website “bancodeteses.capes.gov.br” to identify any thesis in the area, and websites such as the Grey Literature Report (www.greylit.org). Data from conference proceedings were included (even without an author response) if the abstract provided enough information to assess its eligibility and to extract at least the overall prevalence and number of participants.
Study selection and data extraction
The inclusion criteria for articles were as follows: (1) randomized controlled trials, cohort studies, cross-sectional studies, or prevalence studies; (2) studies evaluating the prevalence of genital (cervical and penile), anal, and oral HPV infection in Brazil; and (3) HPV assessment via polymerase chain reaction (PCR), hybrid capture or any well-described genotyping methodology. We excluded studies evaluating only pregnant women or HIV-positive participants as well as studies that analyzed material such as blood, sperm and urine. No sex, age, HPV vaccination, language or date restrictions were applied.
The evaluation of titles and abstracts was conducted by either VC and ABB or NK and FSF, always in pairs, and using standardized forms. Discrepancies were solved through consensus. We collected the following data: publication title, authors, publication year, study design, population characteristics (e.g., high-risk population, number of participants, gender, age, and geographic area in Brazil), the number of HPV-positive and HPV-negative, HPV type, HPV detection and genotyping methodology. For cohort and randomized studies, we extracted only the baseline characteristics of the population. For studies with no data regarding the geographic area where the samples were collected, we contacted the authors to obtain this information. If duplicate studies were discovered, either the study published earlier or the study that provided more information was included. An email was sent to the authors of the eligible duplicate studies to obtain more details about these articles.
We stratified the study population according to risk factors. The population samples/community were defined as low-risk when including asymptomatic healthy individuals who were enrolled in a cancer screening program, attended primary care clinics or did not have any clinical lesions, whereas the high-risk population was defined as partners of women positive for a lesion (HPV or cervical intraepithelial neoplasia; CIN), women with cervical lesion or recruited from a sexual health clinic or key populations (intravenous drug users, men who have sex with men, transgender persons, sex workers and prisoners).
The included studies were assessed for quality using an adapted version of the NIH’s ‘Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies [11]. Reviewers classified the methodological quality of each study and its risk of bias as good, unclear or poor, according to potentials flaws in the study methods. The overall quality of evidence was assessed using Grades of Recommendation, Assessment, Development, and Evaluation (GRADE), a methodology that rates the confidence in estimates of a body of evidence considering the following domains: risk of bias, imprecision, inconsistency, indirectness, and publication bias. We followed the approach proposed for the assessment of baseline risk in prognostic studies and we applied the GRADE framework developed for incidence, as there is no formal procedure for the assessment of certainty of evidence in estimates in the context of prevalence studies [12].
Statistical analysis
Random effects models were used to calculate the pooled prevalence measures and the corresponding 95% confidence intervals (CI). The heterogeneity of the findings was assessed using both the Cochran’s Q test and the I2 statistic. Sensitivity analysis was conducted by meta-regression analyses to investigate the effect of the genotyping method. We performed subgroup analyses for the population risk factor (low- or high-risk), geographic area (i.e., Brazilian region), anatomic site (i.e., cervical, penile, anal and oral regions), high-risk HPV (HR-HPV) type, and presence of HPV-16 and 18. Studies in which the HPV type (high- or low-risk) was either not assessed or not reported were excluded from the HPV type-specific analyses. We also estimated prediction intervals to provide a range of expected HPV prevalence among Brazilian population [13]. Publication bias across the studies was evaluated using funnel plots and Begg’s tests. Analysis was performed using R (version 3.6.1), packages meta version 4.9–7 and metafor 2.0–0.
Results
Descriptive overview of included studies
We identified 3,351 abstracts from the selected databases, and 16 additional studies were included from the listed references of the identified manuscripts as well as other sources. From the 1,562 unique citations, 1,024 were excluded, and the full text of the remaining 538 publications were read. We excluded 394 articles in the subsequent full-text assessments for reasons such as absence of full text, same population of articles already included, incomplete data, different designs form the inclusion criteria, different methods from the inclusion criteria, different anatomic site from the inclusion criteria, without specific data from Brazilian population, or without Brazilian population (Fig 1). After this evaluation, 144 articles reporting the prevalence of HPV [14–157] remained for qualitative synthesis and 139 articles remained for the quantitative analysis (meta-analysis).
Fig 1. PRISMA flow diagram for the selection of included studies.

A summary of the studies characteristics is presented in Table 1. The included studies evaluated 57,513 participants from 139 studies that provided data for quantitative analysis. There were 105 studies that evaluated the presence of HPV in the cervical region, 12 in the penile region, 7 in the anal region and 20 in the oral region. Regarding the diagnostic method, approximately 86.8% of articles used polymerase chain reaction. Most of the studies (42%) originated from the Southeast region (S1 Table).
Table 1. Meta-analysis of the prevalence of HPV by geographic region in Brazil.
| Region | N studies | N patients | Method | Prevalence (CI 95%) | I2 (%) |
|---|---|---|---|---|---|
| Cervical region | |||||
| South | 27 | 10,661 | 22 PCR / 3 HC / 2 undescribed | 21.59% (18.34, 25.23) | 94.0 |
| Southeast | 37 | 26,077 | 30 PCR / 7 HC* | 25.65% (20.70, 31.33) | 99.0 |
| North | 14 | 4,787 | PCR | 20.40% (17.20, 28.63) | 95.0 |
| Northeast | 15 | 5,574 | 13 PCR / 2 HC | 32.82% (22.47, 45.15) | 99.0 |
| Central-West | 8 | 1,558 | 7 PCR / 1 HC | 31.89% (24.91, 39.78) | 89.0 |
| Undefined | 4 | 2,165 | 3 PCR / 1 HC | 29.14% (25.99, 32.51) | 41 |
| Penile region | |||||
| South | 1 | 99 | PCR | 54.55% (44.23, 64.59) | |
| Southeast | 8 | 2,638 | PCR | 39.61% (22.54, 59.64) | 98.0 |
| North | |||||
| Northeast | 2 | 129 | PCR | 25.59% (18.80, 33.81) | 0 |
| Central-West | |||||
| Undefined | 1 | 90 | PCR | 18.89% (11.41, 28.51) | |
| Anal region | |||||
| South | |||||
| Southeast | 4 | 1,148 | 3 PCR / 1HC | 21.22% (8.38, 44.24) | 96.0 |
| North | 1 | 42 | PCR | 26.19% (15.14, 41.38) | - |
| Northeast | 2 | 82 | PCR / undescribed | 39.20% (29.21, 50.18) | |
| Central-West | |||||
| Undefined | |||||
| Oral region | |||||
| South | 2 | 596 | PCR | 1.26% (0.62, 2.55) | 0 |
| Southeast | 11 | 1,276 | 10 PCR / 1HC | 8.99% (3.47, 21.35) | 94.0 |
| North | 1 | 166 | PCR | 24.10% (18.20, 31.18) | |
| Northeast | 4 | 266 | PCR | 37.56% (10.63, 75.25) | 96.0 |
| Central-West | 1 | 65 | PCR | 6.15% (2.33, 15.28) | |
| Undefined | 1 | 125 | PCR | 23.20% (16.63, 31.39) | |
CI, Confidence Interval; HC, Hybrid Capture; PCR, Polymerase Chain Reaction.
*1 analysis by ELISA
The majority of the included studies were not population-based and did not have information regarding either the sample size power or the participation rate. The overall quality of evidence for HPV prevalence was rated as very low according to GRADE, mainly because the studies had selection bias, inconsistency and provided indirect evidence. The quality of evidence assessment is shown in S2 Table.
Funnel plots were symmetrical for the cervical HPV prevalence analysis, and Begg’s test was not significant for any region of the body, except for the anal region which could not be assessed by the asymmetry test due to the small number of articles (S1 Fig).
Prevalence of HPV in cervical samples
The overall prevalence of cervical HPV was 25.41% (95% CI 22.71–28.32; 105 studies; I2 = 98%; S2 Fig), and the prevalence of HR-HPV genotypes was 17.65% (95% CI 14.80–20.92; 44 studies; I2 = 96%; Fig 2). The prediction interval for HPV prevalence ranged from 7.17 to 60.04%, with 95% confidence. This prediction interval represents the range of expected Brazilian cervical HPV prevalence in 95% of settings. The prevalence of cervical HPV-16 was 5.30% (95% CI, 4.06–6.90; 52 studies; I2 = 94%, Fig 3), and HPV-18 was 1.87% (95% CI, 1.25–2.78; 38 studies; I2 = 91%, Fig 4).
Fig 2. Overall prevalence of cervical infection by high-risk HPV genotypes.

Forest plot of a metanalysis of studies reporting prevalence of infection of the cervix by HR-HPV genotypes in Brazil.
Fig 3. Overall prevalence of cervical infection by HPV-16.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV-16 in Brazil.
Fig 4. Overall prevalence of cervical infection by HPV-18.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV-18 in Brazil.
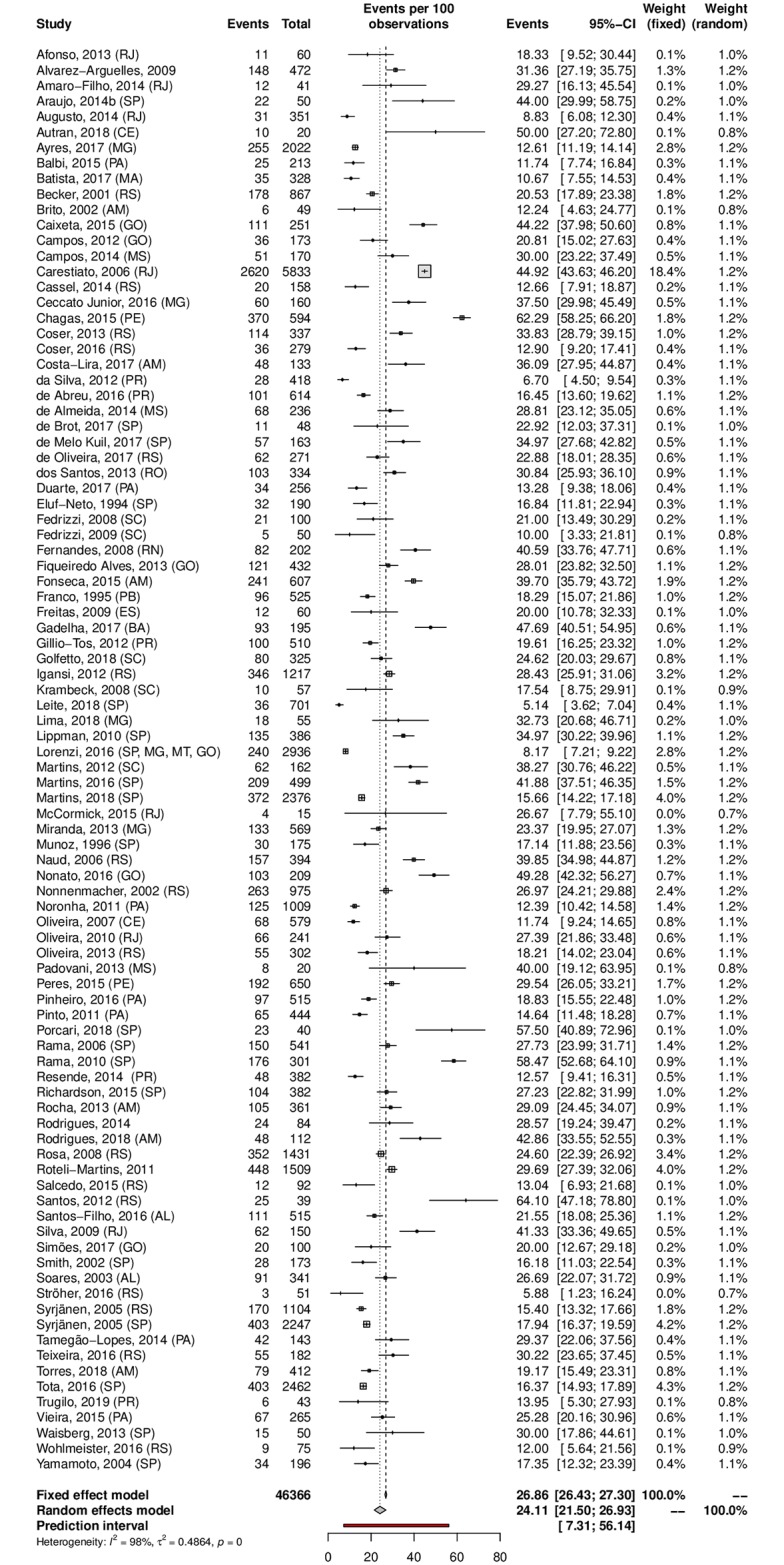
A subgroup analysis was performed in an attempt to explain the heterogeneity among the studies. The HPV prevalence was 24.11% (95% CI 21.50–26.93; I2 = 98%) in low-risk populations (Fig 5) and 38.01% (95% CI 25.90–51.82; I2 = 97%) in high-risk populations (Fig 6). Most studies were carried out in the Southeast region (n = 37), followed by the South (n = 27) and Northeast (n = 15) regions; the North region was represented by 4 studies, while the Central-west region was represented by eight of them. Interestingly, HPV prevalence was slightly higher in the Northeast and Central-West areas (Table 1). The forest plots with the estimates for each region are shown in Figs 7–11. The prevalence of HR-HPV genotypes could also be analysed by region. Results show generally wider confidence intervals and a markedly lower prevalence in the South region, when compared to the other regions of Brazil (S3 Fig).
Fig 5. Prevalence of cervical HPV infection in low-risk populations.
Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in low-risk populations in Brazil.
Fig 6. Prevalence of cervical HPV infection in high-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in high-risk populations in Brazil.
Fig 7. Prevalence of cervical HPV in the South region of Brazil.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in the South region of Brazil.
Fig 11. Prevalence of cervical HPV in the Central-West region of Brazil.

Forest plot of a metanlysis of studies reporting prevalence of cervical infection by HPV in the Central-west region of Brazil.
Fig 8. Prevalence of cervical HPV in the Southeast region of Brazil.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in the Southeast region of Brazil.
Fig 9. Prevalence of cervical HPV in the North region of Brazil.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in the North region of Brazil.
Fig 10. Prevalence of cervical HPV in the Northeast region of Brazil.

Forest plot of a metanalysis of studies reporting prevalence of cervical infection by HPV in the Northeast region of Brazil.
Prevalence of HPV in penile samples
The prevalence of penile HPV was 36.21% (95% CI 23.40–51.33; 12 studies; I2 = 98%; Fig 12). The prediction interval for HPV prevalence ranged from 4.59 to 87.01%, with 95% confidence. Eight were conducted in the Southeast, with a prevalence of 39.61% (95% CI 22.54–59.64). Upon analyzing HR-HPV types, the studies reported a prevalence of 18.13% (95% CI 9.90–30.85; 7 studies; I2 = 96%; Fig 13). HPV prevalence in the low-risk population was 25.49% (95% CI 12.63–44.74; 7 studies; I2 = 98%; Fig 14). In the high-risk population was 54.24% (26.78–79.34; 5 studies; I2 = 97%; Fig 15).
Fig 12. Overall prevalence of penile HPV.

Forest plot of metanalysis of studies reporting prevalence of penile HPV infection in Brazil.
Fig 13. Overall prevalence of penile infection by high-risk HPV genotypes.

Forest plot of a metanalysis of studies reporting prevalence of penile infection by HR-HPV genotypes in Brazil.
Fig 14. Prevalence of penile HPV infection in low-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of penile infection by HPV in low-risk populations in Brazil.
Fig 15. Prevalence of penile HPV infection in high-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of penile infection by HPV in high-risk populations in Brazil.
Prevalence of HPV in anal samples
Among the analyzed studies, the prevalence of anal HPV was 25.68% (95% CI 14.64–41.04; 7 studies; I2 = 93%) as shown in Fig 16. The prediction interval for HPV prevalence ranged from 2.87 to 80.19%, with 95% confidence. The prevalence of HR-HPV types was 14.07% (95% CI 7.02–26.2). Eleuterio et al.[124] and Nicolau et al.[156] reported a prevalence of 32% compared to the 14% and 5% reported in three other studies [125,127,128] (Fig 17). This discrepancy might be explained by the HPV genotyping method (56.18% prevalence based on hybrid capture and 14.80% prevalence based on PCR). Evaluating sexual partners of women who had cervical HPV infection, Nicolau et al. a higher prevalence than in other studies was found (70%; 95% CI 55.39–82.14) [156]. The prevalence in the low-risk population was 22.10% (95%CI, 11.36–38.59; 4 studies; I2 = 89% Fig 18) and in the high-risk population was 31.63% (95% CI, 7.04–73.86; 3 studies; I2 = 97%; Fig 19). The prevalence of HPV among the Southeast, North and Northeast regions was 21.22%, 26.19% and 39.20%, respectively (Fig 20). There was no data on the HPV prevalence in the anal region in South and Central-West regions (Table 1).
Fig 16. Overall prevalence of anal HPV infection.

Forest plot of a metanalysis of studies reporting prevalence of anal infection by HPV in Brazil.
Fig 17. Overall prevalence of anal infection by high-risk HPV genotypes.

Forest plot of a metanalysis of studies reporting prevalence of anal infection by HR-HPV in Brazil.
Fig 18. Prevalence of anal HPV infection in low-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of anal infection by HPV in low-risk populations in Brazil.
Fig 19. Prevalence of anal HPV infection in high-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of anal infection by HPV in high-risk populations in Brazil.
Fig 20. Prevalence of anal HPV infection in Brazil, by region.

Forest plot of a metanalysis of studies reporting prevalence of anal infection by HPV, stratified by region in which each of them took place.
Prevalence of HPV in oral samples
HPV prevalence in the oral region was 11.89% (95% CI 6.26–21.43; 20 studies; I2 = 95%; prediction interval 0.55 to 76.58%) (Fig 21), and the prevalence of HR-HPV types was 4.69% (95% CI 0.23–50.72; 5 studies; I2 = 96%; Fig 22). The prediction interval for HPV prevalence ranged from 0.55 to 76.58%, with 95% confidence. The subgroup analysis showed an HPV prevalence of 6.69% (95% CI 2.85–14.89; 11 studies; I2 = 94%; Fig 23) in the low-risk group and 22.42% (95% CI 8.64–49.89; 9 studies; I2 = 95%; Fig 24) in the high-risk group. The majority of studies were published in women and conducted in the Southeast followed by the Northeast and South regions. There was an important difference in oral HPV prevalence between studies (from 0% to 85.19%), with overall results being higher in the Northeast (37.56%) compared to that of Central-West and South regions (6.15% and 1.26%, respectively); the North and Central-West regions each had only one study included (Table 1) (Fig 25).
Fig 21. Overall prevalence of oral HPV infection.

Forest plot of a metanalysis of studies reporting prevalence of oral infection by HPV in Brazil.
Fig 22. Overall prevalence of oral infection by high-risk HPV genotypes.

Forest plot of a metanalysis of studies reporting prevalence of oral infection by HR-HPV in Brazil.
Fig 23. Prevalence of oral HPV infection in low-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of oral HPV infection in low-risk populations in Brazil.
Fig 24. Prevalence of oral HPV infection in high-risk populations.

Forest plot of a metanalysis of studies reporting prevalence of oral HPV infection in high-risk populations in Brazil.
Fig 25. Prevalence of oral HPV infection in Brazil, by region.

Forest plot of a metanalysis of studies reporting prevalence of oral infection by HPV, stratified by region in which each of them took place.
Discussion
This systematic review included more than 50,000 people and showed that Brazilian population have a high prevalence of HPV infection as compared to women with normal cytology in different world regions such as Central America (13%), Northern Africa (9.2%), Western Europe (9%) and Southern Asia (7.1%) [3,158]. The highest prevalence was found in the penile region with 36% followed by cervical and anal region with approximately 25% and then oral region with 12%. There is a variation in the HPV prevalence among different geographic areas in Brazil, with increased prevalence in the Northeast (except at the penile site) and scarce data from the North and Central-West geographic regions. To the best of our knowledge, this is the first study that has evaluated the prevalence of HPV at multiple sites on the body and different Brazilian regions in general population.
Overall prevalence of HPV and the prevalence of high-risk HPV differs slightly across regions in Brazil. Most studies included in this review were carried out in the South and Southeast regions. This was an expected result, as these are highly populated and the most economically developed regions of Brazil [159]. Cervical HPV prevalence was higher in the Central-west and Northeast regions. Few of the studies retrieved in our review were from these regions, and this could have an influence on the estimate. Alternatively, it could be that these differences are real, and they could be related to socioeconomical aspects, in particular when this analysis is focused in the Northeast region, which is highly populated, poorer and has worse general health indicators [159,160].
Our study showed a prevalence of cervical HPV of 24.11% and 38.01% in low- and high-risk populations, respectively. According to a meta-analysis of one million women, the estimated global HPV prevalence in women with normal cytological was 11.7%, but it was 16.1% in Latin America [3]. However, similar to our results, a previous review published in Brazil reported a cervical prevalence ranging from 13 to 54%, with most of the data representing the Southeast population [5]. With this systematic review, we focused on existing data regarding HPV prevalence and expanded the overall summaries to a national scope. The regional-specific HPV prevalence varies from 20–35%. It is important to highlight that the North region, which has the highest incidence of cervical cancer in Brazil (25.62/100.000) [9], did not present a higher prevalence of HPV according to our results. It could be the case that studies from the North region underestimated HPV prevalence, or, conversely, that prevalences in other regions are overestimated. Another reason for this apparent contradiction is less accessibility to cervical cancer screening programs and less access to health care in the North region of Brasil [161].
It was not possible to pool data for specific genotypes beyond HPV-16 and HPV-18. Our results show a relatively high prevalence HPV-18 in females when compared to data from the USA [162] and other countries [163]. While we attempted to address selection bias by categorizing high-risk and low-risk populations, it was not possible to completely eliminate it. Patients who sought screening programs or medical care could have different risk profiles than those who did not.
The HPV prevalence in the penile region was 25.49% in the people without clinical lesions and even higher among high-risk populations (54.24%). According to a previous systematic review, genital HPV infection in men ranges from 1.3% to 72.9% [164], and the HIM study reported an HPV prevalence of 72% among Brazilian men [165]. The reason for this high prevalence might be due to sampling differences among the studies, which includes the scrotum and/or penis, a larger sample size and the inclusion of a variety of recruitment strategies such as reference centers for urogenital care and general media advertising [165]. Furthermore, differences in the laboratory technique could partially explain the difference. The evaluation of penile HPV is underrepresented in most Brazilian regions, and the available studies have a large number of differences regarding their design. The Southeast and South regions tend to show higher HPV prevalence when compared to the Northeast, but the Southeast was the only region that published more than two studies. For example, one of the two Northeast studies represented a low-risk population [117], whereas the study originating from the South region included the partners of women with CIN [121].
The prevalence of HPV in the anal region was similar to that of the cervical region and comprised 25.68% of population. Anal HPV prevalence is typically higher among high-risk groups, which is in accordance with previous studies [4]. There were a limited number of studies in Brazil that evaluated HPV in this anatomic site, and four were conducted in Southeast. The available data on the general population are comparable with the prevalence of cervical HPV and could be explained by concomitant HPV infection in both anal and cervical regions.
Prevalence of cervical HPV in Brazil is higher than in other developing countries. A past review has estimated generally lower prevalence of HPV in the cervix of healthy females in most developing and developed countries, but some of this discrepancy could be explained by the broader inclusion criteria of our study [163]. While the prevalence of male genital HPV varies substantially among developing countries, most of them reported prevalences around 20%, which is higher than in developed countries but lower than our findings [166]. Finally, extending this comparison to oral HPV, our estimates seem to be in accordance to those found for South American countries in another review. That study also found that South America was the continent with the highest prevalence of HPV, at 12.4%, significantly above both Asia, at 2.6% and Africa, at 7.0%, and also higher than Oceania (4.6%), North America (7.7%) and Europe (9.9%) [167].
This meta-analysis shows an oral HPV prevalence of 6.69% among the population without clinical lesions and 22.42% within the high-risk population. As is commonly known, oropharyngeal cancers are associated with tobacco and alcohol intake, but the incidence of HPV-induced cancers increased and HPV infection is now recognized as an important etiological factor in this disease [168,169]. A previous systematic review developed in Brazil showed a 6% HPV prevalence among the healthy population but a higher prevalence (38.5%) within high-risk groups [170]. Although that review was developed using a different data analysis model compared to our model, the results of both studies were highly comparable. Similar to the other analysis of oral HPV prevalence, most of the studies were conducted in the Southeast region. The higher prevalence in the Northeast might be attributed to the inclusion of the high-risk population within the analyses. Although most of the studies included men and women, the reported data were insufficiently stratified to allow for analysis by gender. In addition, the studies that only included women generally evaluated participants with concomitant genital HPV. There was a high heterogeneity in HPV oral prevalence among the studies in Brazil, ranging from zero to 96%. The two studies with the highest oral HPV prevalence, around 80%, investigated the presence of oral HPV DNA in women with diagnosis of genital HPV [141,146].
In terms of public health policy, our results suggest that while some efforts could be targeted towards regions and populations with higher HPV prevalence, broad approaches [171] seem appropriate, as illustrated by the fact that the prevalence of HPV is high even in low-risk populations and that it differs only slightly across regions. Additionally, the high prevalence of HPV in anatomic sites other than the cervix suggests it should not be approached as a problem restricted to cervical cancer.
This study is a comprehensive systematic review that used a broad search strategy, including large studies that analyzed different anatomic sites and represented different geographic regions throughout the country. Additionally, the findings of this systematic review increase our understanding of overall and HR-HPV prevalence within the general population in Brazil and by geographic region. We understand that the included studies did not accurately represent a sampling of Brazilian cities; however, this review provides the best estimated data on HPV prevalence to date.
Our study has some limitations. Brazil is a vast country, and the prevalence of HPV in some regions was either reported in a small number of studies or not reported at all. Thus, the population included in our review may not be representative of the general population throughout Brazil. The high heterogeneity among studies may impact in the exact prevalence measured. In contrast with randomized trials, non-controlled studies, such as the included in this systematic review, have smaller sample size and consequently higher imprecision and statistical inconsistency. Given that the estimates of individual studies are included in the prediction interval, we hypothesize that most of the heterogeneity are result of the different settings (for example, patients characteristics and age). Furthermore, participants of all ages were included in the present study, and it is known that HPV genital infection decrease with increasing age [172]. On this way, some discrepancies in prevalence could be due to differences in age range of included studies. As the majority of studies reported age in ranges, we could not aggregate the studies in age categories or perform meta-regression analysis. Most of the included studies looked at small groups and did not report the sample size statistical power; given the rarity of HPV infection at some anatomic sites (i.e., oral), a larger population-based sample size is needed to better evaluate HPV prevalence.
Prevalence studies are often used to devise public health actions and improve health services as well as serve as the first step to evaluate national control programs. The overall quality of the evidence for HPV prevalence was low or very low for all anatomic sites. In 2014, Brazil launched a national HPV vaccination program that includes girls between 9 and 13 years old and since 2017 the program started including boys of 12 and 13 years of age. Robust evidence is important for adequate monitoring of the populational impact of the program across Brazil. In view of the lack of proper national evidence regarding the HPV prevalence and databases tracking HPV infection rates, as well as to meet the needs of the Brazilian Ministry of Health, we conclude that is necessary to develop a nationwide study to investigate HPV presence among the Brazilian population. A nationwide HPV prevalence study (POP-Brazil study) with young adults between 16–25 years is in development, and it is predicted that the results of this study will fulfill the lack of epidemiological information detected in this review [173].
In summary, the prevalence of HPV in Brazilian population is high and varies by anatomical body site, with lower rates in the oral cavity compared to that in the cervical, penile and anal region. Studies on HPV have been primarily developed to evaluate infection and cancer in the cervical region. There is a profound lack of HPV data in many geographic regions of Brazil and for different anatomic sites.
Supporting information
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This work was supported by the Brazilian Ministry of Health (Institutional Development Support Program of the Brazilian National Health System – PROADI-SUS) and the National Program of Immunizations through the Pan American Health Organization, project number BR/CNT/1500013.
References
- 1.Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer; 2018. https://gco.iarc.fr/today [Google Scholar]
- 2.Beltrão M, Wanderley MSO, de Santana NA, Bruneska D, de Lima Filho JL. Site of infections associated with human papillomavirus. Arch Gynecol Obstet. 2015;291: 481–491. 10.1007/s00404-014-3480-5 [DOI] [PubMed] [Google Scholar]
- 3.Bruni L, Diaz M, Castellsagué X, Ferrer E, Bosch FX, de Sanjosé S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202: 1789–1799. 10.1086/657321 [DOI] [PubMed] [Google Scholar]
- 4.Giuliano AR, Nyitray AG, Kreimer AR, Pierce Campbell CM, Goodman MT, Sudenga SL, et al. EUROGIN 2014 roadmap: differences in human papillomavirus infection natural history, transmission and human papillomavirus-related cancer incidence by gender and anatomic site of infection. Int J Cancer. 2015;136: 2752–2760. 10.1002/ijc.29082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ayres ARG, Silva GA. Cervical HPV infection in Brazil: systematic review. Rev Saúde Pública. 2010;44: 963–974. [DOI] [PubMed] [Google Scholar]
- 6.Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55: 74–108. 10.3322/canjclin.55.2.74 [DOI] [PubMed] [Google Scholar]
- 7.Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2005;14: 467–475. 10.1158/1055-9965.EPI-04-0551 [DOI] [PubMed] [Google Scholar]
- 8.Gillison ML, Broutian T, Pickard RKL, Tong Z, Xiao W, Kahle L, et al. Prevalence of Oral HPV Infection in the United States, 2009–2010. JAMA. 2012;307: 693–703. 10.1001/jama.2012.101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Estimativa 2018: Incidência de Câncer no Brasil / Instituto Nacional de Câncer José Alencar Gomes da Silva. Coordenação de Prevenção e Vigilância.–Rio de Janeiro: INCA, 2017. In: INCA—Instituto Nacional de Câncer [Internet]. [cited 27 Mar 2019]. https://www.inca.gov.br/publicacoes/livros/estimativa-2018-incidencia-de-cancer-no-brasil
- 10.Colpani V, Bidinotto AB, Falavigna M, Giozza SP, Benzaken AS, Pimenta C, et al. Prevalence of papillomavirus in Brazil: a systematic review protocol. BMJ Open. 2016;6: e011884 10.1136/bmjopen-2016-011884 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Assessing Cardiovascular Risk: Systematic Evidence Review from the Risk Assessment Work Group | National Heart, Lung, and Blood Institute (NHLBI). [cited 27 Mar 2019]. https://www.nhlbi.nih.gov/health-topics/assessing-cardiovascular-risk
- 12.Iorio A, Spencer FA, Falavigna M, Alba C, Lang E, Burnand B, et al. Use of GRADE for assessment of evidence about prognosis: rating confidence in estimates of event rates in broad categories of patients. BMJ. 2015;350: h870 10.1136/bmj.h870 [DOI] [PubMed] [Google Scholar]
- 13.IntHout J, Ioannidis JPA, Rovers MM, Goeman JJ. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open. 2016;6: e010247 10.1136/bmjopen-2015-010247 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alvarez-Argüelles M, Melon S, Villa L, Palacio A, Boga J, Junquera M, et al. Distribution of genotypes of human papilloma virus in women from different countries. Clin Microbiol Infect. 2009;15: S107–S612. 10.1111/j.1469-0691.2009.02858.x [DOI] [Google Scholar]
- 15.Amaro Filho SM, Nuovo GJ, Cunha CB, de O Ramos Pereira L, Oliveira-Silva M, Russomano F, et al. Correlation of MCM2 detection with stage and virology of cervical cancer. Int J Biol Markers. 2014;29: e363–371. 10.5301/jbm.5000081 [DOI] [PubMed] [Google Scholar]
- 16.Amorim AT, Marques LM, Campos GB, Lobão TN, Souza Lino V, Cintra RC, et al. Co-infection of sexually transmitted pathogens and Human Papillomavirus in cervical samples of women of Brazil. BMC Infect Dis. 2017;17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Araujo MP, Kleine HT, Parmigiano TR, Gomes NT, Caparroz GP, Silva IDCG, et al. Prevalence of sexually transmitted diseases in female athletes in São Paulo, Brazil. Einstein São Paulo. 2014;12: 31–35. 10.1590/S1679-45082014AO2949 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Augusto EF, Santos LS, Oliveira L do H dos S, Augusto EF, Santos LS, Oliveira L do H dos S. Human papillomavirus detection in cervical scrapes from women attended in the Family Health Program. Rev Lat Am Enfermagem. 2014;22: 100–107. 10.1590/0104-1169.3189.2398 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ayres ARG, Silva GA, Teixeira MTB, Duque K de CD, Machado MLSM, Gamarra CJ, et al. HPV in women assisted by the Family Health Strategy. Rev Saúde Pública. 2017;51: 92 10.11606/S1518-8787.2017051000065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Balbi F do SM. Estudo da prevalência da infecção pelo Papiloma Vírus Humano (HPV) em mulheres no climatério em um hospital de referência de Belém. Universidade Federal do Pará. 2015. http://repositorio.ufpa.br:8080/jspui/handle/2011/7026
- 21.Baldin-Dal Pogetto MR, Silva MG, Parada CMG de L. Prevalence of sexually transmitted diseases in female sex workers in a city in the interior of São Paulo, Brazil. Rev Lat Am Enfermagem. 2011;19: 493–499. 10.1590/S0104-11692011000300007 [DOI] [Google Scholar]
- 22.Batista JE, Saddi VA, Carvalho KPA, Ribeiro AA, Segati KD, Carneiro MA dos S, et al. Human papillomavirus genotypes 68 and 58 are the most prevalent genotypes in women from quilombo communities in the state of Maranhão, Brazil. Int J Infect Dis. 2017;55: 51–55. 10.1016/j.ijid.2017.01.001 [DOI] [PubMed] [Google Scholar]
- 23.Becker E, Edelweiss MI, Nonnenmacher B, Bozzetti MC. Prevalence and epidemiologic correlates of atypical squamous cells of undetermined significance in women at low risk for cervical cancer. Diagn Cytopathol. 2001;24: 276–282. 10.1002/dc.1059 [DOI] [PubMed] [Google Scholar]
- 24.Boon ME, Veen G, Barlow Y, Graudenz MS, Kok LP. Presence of proliferating (MiB-1-positive) cells in cervical smears of women infected with HIV is associated with clinical outcome: a study of Brazilian women. Diagn Cytopathol. 2001;24: 373–377. 10.1002/dc.1083 [DOI] [PubMed] [Google Scholar]
- 25.Brito EB, Martins SJ, Menezes RC. Human papillomaviruses in Amerindian women from Brazilian Amazonia. Epidemiol Infect. 2002;128: 485–489. 10.1017/s0950268802006908 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Caixeta RCA, Ribeiro AA, Segatti KD, Saddi VA, Figueiredo Alves RR, Santos Carneiro MA, et al. Association between the human papillomavirus, bacterial vaginosis and cervicitis and the detection of abnormalities in cervical smears from teenage girls and young women. Diagn Cytopathol. 2015;43: 780–785. 10.1002/dc.23301 [DOI] [PubMed] [Google Scholar]
- 27.Campos ACC, Murta EFC, Michelin MA, Reis C. Evaluation of Cytokines in Endocervical Secretion and Vaginal pH from Women with Bacterial Vaginosis or Human Papillomavirus. ISRN Obstet Gynecol. 2012;2012: 342075 10.5402/2012/342075 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Campos KLM, Machado AP, Almeida FG, Bonin CM, Prata TTM, Almeida LZ, et al. Good agreements between self and clinician-collected specimens for the detection of human papillomavirus in Brazilian patients. Mem Inst Oswaldo Cruz. 2014;109: 352–355. 10.1590/0074-0276130397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cassel APR, Barcellos RB, Silva CMD, Matos Almeida SE, Rossetti MLR. Association between human papillomavirus (HPV) DNA and micronuclei in normal cervical cytology. Genet Mol Biol. 2014;37: 360–363. 10.1590/s1415-47572014005000010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ceccato BPV Junior, Lopes APC, Nascimento LF, Novaes LM, Melo VH, Ceccato BPV Junior, et al. Prevalence of cervical infection by human papillomavirus and cervical intraepithelial neoplasia in HIV-positive and negative women. Rev Bras Ginecol E Obstetrícia. 2015;37: 178–185. 10.1590/SO100-720320150005184 [DOI] [PubMed] [Google Scholar]
- 31.Chagas BS, Comar M, Gurgel APAD, Paiva S, Seraceni S, Freitas AC, et al. Association Study between Cervical Lesions and Single or Multiple Vaccine-Target and Non-Vaccine Target Human Papillomavirus (HPV) Types in Women from Northeastern Brazil. PLoS One. 2015;10: e0132570 10.1371/journal.pone.0132570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Coser J, Rocha Boeira T, Simon D, Kazantzi Fonseca AS, Ikuta N, Lunge VR. Prevalence and genotypic diversity of cervical human papillomavirus infection among women from an urban center in Brazil. Genet Mol Res GMR. 2013;12: 4276–4285. 10.4238/2013.February.19.3 [DOI] [PubMed] [Google Scholar]
- 33.Coser J, Boeira T da R, Wolf JM, Cerbaro K, Simon D, Lunge VR. Cervical human papillomavirus infection and persistence: a clinic-based study in the countryside from South Brazil. Braz J Infect Dis. 2016;20: 61–68. 10.1016/j.bjid.2015.10.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Costa-Lira E, Jacinto AHVL, Silva LM, Napoleão PFR, Barbosa-Filho RAA, Cruz GJS, et al. Prevalence of human papillomavirus, Chlamydia trachomatis, and Trichomonas vaginalis infections in Amazonian women with normal and abnormal cytology. Genet Mol Res GMR. 2017;16: gmr16029626. 10.4238/gmr16029626 [DOI] [PubMed] [Google Scholar]
- 35.da Silva MC, Martins HPR, Souza JL, Tognim MCB, Svidzinski TIE, Teixeira JJV, et al. Prevalence of HPV infection and genotypes in women with normal cervical cytology in the state of Paraná, Brazil. Arch Gynecol Obstet. 2012;286: 1015–1022. 10.1007/s00404-012-2399-y [DOI] [PubMed] [Google Scholar]
- 36.de Abreu AL, Malaguti N, Souza RP, Uchimura NS, Ferreira ÉC, Pereira MW, et al. Association of human papillomavirus, Neisseria gonorrhoeae and Chlamydia trachomatis co-infections on the risk of high-grade squamous intraepithelial cervical lesion. Am J Cancer Res. 2016;6: 1371–1383. [PMC free article] [PubMed] [Google Scholar]
- 37.de Aguiar SRV, Villanova FE, Martins LC, Santos MS, de P Maciel J, Falcão LFM, et al. Human papillomavirus: prevalence and factors associated in women prisoners population from the Eastern Brazilian Amazon. J Med Virol. 2014;86: 1528–1533. 10.1002/jmv.23972 [DOI] [PubMed] [Google Scholar]
- 38.de Almeida FG, Machado AP, Fernandes CEDS, Ferreira AT, Padovani CTJ, Tozetti IA. Molecular epidemiology of the human papillomavirus infection in self-collected samples from young women. J Med Virol. 2014;86: 266–271. 10.1002/jmv.23725 [DOI] [PubMed] [Google Scholar]
- 39.De Brot L, Pellegrini B, Moretti ST, Carraro DM, Soares FA, Rocha RM, et al. Infections with multiple high-risk HPV types are associated with high-grade and persistent low-grade intraepithelial lesions of the cervix. Cancer Cytopathol. 2017;125: 138–143. 10.1002/cncy.21789 [DOI] [PubMed] [Google Scholar]
- 40.de Mattos AT, Freitas LB, Lima BMC, Miranda AE, Spano LC. Diversity and uncommon HPV types in HIV seropositive and seronegative women attending an STI clinic. Braz J Microbiol. 2011;42: 786–793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.de Melo Kuil L, Lorenzi AT, Stein MD, Resende JCP, Antoniazzi M, Longatto-Filho A, et al. The Role of Self-Collection by Vaginal Lavage for the Detection of HPV and High-Grade Intraepithelial Neoplasia. Acta Cytol. 2017;61: 425–433. 10.1159/000477331 [DOI] [PubMed] [Google Scholar]
- 42.de Oliveira GR, Vieira VC, Ávila EC, Finger-Jardim F, Caldeira TD, Gatti FA, et al. Human papillomavirus type distribution and HPV16 intratype diversity in southern Brazil in women with and without cervical lesions. Mem Inst Oswaldo Cruz. 2017;112: 492–498. 10.1590/0074-02760160530 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.dos Santos JC, dos S Cezar MR, Lisboa MR, Moura MM da F. Occurrence of human papillomavirus in uterine cervix of women in the western Brazilian Amazon. Acta Amaz. 2013;43: 185–190. 10.1590/S0044-59672013000200008 [DOI] [Google Scholar]
- 44.Duarte D, Vieira R, Brito E, Pinheiro M, Monteiro J, Valente M, et al. Prevalence of Human Papillomavirus Infection and Cervical Cancer Screening among Riverside Women of the Brazilian Amazon. Rev Bras Ginecol E Obstetrícia. 2017;39: 350–357. 10.1055/s-0037-1604027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eluf-Neto J, Booth M, Muñoz N, Bosch FX, Meijer CJ, Walboomers JM. Human papillomavirus and invasive cervical cancer in Brazil. Br J Cancer. 1994;69: 114–119. 10.1038/bjc.1994.18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Fedrizzi EN, Schlup CG, Menezes ME, Ocampos M. Infecção pelo Papilomavírus Humano (HPV) em Mulheres HIV-Positivo de Florianópolis, Santa Catarina. J Bras Doenças Sex Transm DST. 2008;20: 73–79. [Google Scholar]
- 47.Fedrizzi EN, Villa LL, Souza IV, Sebastião APM, Urbanetz AA, De Carvalho NS. Does human papillomavirus play a role in endometrial carcinogenesis? Int J Gynecol Pathol. 2009;28: 322–327. 10.1097/PGP.0b013e318199943b [DOI] [PubMed] [Google Scholar]
- 48.de M Fernandes TAA, de V Meissner R, Bezerra LF, Azevedo PRM, Fernandes JV. Human papillomavirus infection in women attended at a cervical cancer screening service in Natal, Brazil. Braz J Microbiol. 2008;39: 573–578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Figueiredo Alves RR, Turchi MD, Santos LE, Guimarães EM de B, Garcia MMD, Seixas MSC, et al. Prevalence, genotype profile and risk factors for multiple human papillomavirus cervical infection in unimmunized female adolescents in Goiânia, Brazil: a community-based study. BMC Public Health. 2013;13 10.1186/1471-2458-13-1041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Fonseca AJ, Taeko D, Chaves TA, Amorim LD da C, Murari RSW, Miranda AE, et al. HPV Infection and Cervical Screening in Socially Isolated Indigenous Women Inhabitants of the Amazonian Rainforest. PLOS ONE. 2015;10: e0133635 10.1371/journal.pone.0133635 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Franco EL, Villa LL, Ruiz A, Costa MC. Transmission of cervical human papillomavirus infection by sexual activity: differences between low and high oncogenic risk types. J Infect Dis. 1995;172: 756–763. 10.1093/infdis/172.3.756 [DOI] [PubMed] [Google Scholar]
- 52.Freitas LB, Pereira CC, Checon R, Leite JPG, Nascimento JP, Spano LC. Adeno-associated virus and human papillomavirus types in cervical samples of pregnant and non-pregnant women. Eur J Obstet Gynecol Reprod Biol. 2009;145: 41–44. 10.1016/j.ejogrb.2009.03.024 [DOI] [PubMed] [Google Scholar]
- 53.Gadelha SR, Soares-Barreto DMV, Costa GB, Leal VCN, Gomes LGS, Santos UR, et al. Clinical, laboratory and epidemiological aspects of HPV infection in a low-income population from South Bahia, Brazil. Epidemiol Infect. 2017;145: 3398–3404. 10.1017/S0950268817002448 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gillio-Tos A, Bicalho M da G, Fiano V, Grasso C, Tarallo V, De Marco L, et al. Case-control study of HLA-G promoter methylation status, HPV infection and cervical neoplasia in Curitiba, Brazil: a pilot analysis. BMC Cancer. 2012;12: 618 10.1186/1471-2407-12-618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Girianelli VR, Thuler LCS, Silva GA. [Prevalence of HPV infection among women covered by the family health program in the Baixada Fluminense, Rio de Janeiro, Brazil]. Rev Bras Ginecol E Obstet Rev Fed Bras Soc Ginecol E Obstet. 2010;32: 39–46. [DOI] [PubMed] [Google Scholar]
- 56.Golfetto L, Alves EV, Martins TR, Sincero TCM, Castro JBS, Dannebrock C, et al. PCR-RFLP assay as an option for primary HPV test. Braz J Med Biol Res. 2018;51 10.1590/1414-431x20177098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Holanda F, Castelo A, Veras TMCW, Almeida FML, Lins MZ, Dores GB. Primary screening for cervical cancer through self sampling. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. 2006;95: 179–184. 10.1016/j.ijgo.2006.07.012 [DOI] [PubMed] [Google Scholar]
- 58.Igansi CN, Santos VK, Rosa MI, Rosa MTM, Calil LN, Cortez-Herrera E, et al. Infecção genital pelo HPV e Chlamydia trachomatis em mulheres assintomáticas: prevalência, fatores associados e relação com lesões cervicais. Cad Saúde Coletiva. 2012;20: 287–96. [Google Scholar]
- 59.Krambeck WM, Cadidé RM, Dalmarco EM, Cordova CMM. HPV detection and genotyping as an earlier approach in cervical cancer screening of the female genital tract. Clin Exp Obstet Gynecol. 2008;35: 175–178. [PubMed] [Google Scholar]
- 60.Leite KRM, Silva T, Naum B, Canavez F, Canavez J, Pimenta R, et al. Validation of a New Low-Cost, Methanol-Based Fixative for Cervical Cytology and Human Papillomavirus Detection. Acta Cytol. 2018;62: 393–396. 10.1159/000489873 [DOI] [PubMed] [Google Scholar]
- 61.Lima L, Hoelzle C, Simões R, Lima M, Fradico J, Mateo E, et al. Sexually Transmitted Infections Detected by Multiplex Real Time PCR in Asymptomatic Women and Association with Cervical Intraepithelial Neoplasia. Rev Bras Ginecol E Obstetrícia RBGO Gynecol Obstet. 2018;40: 540–546. 10.1055/s-0038-1669994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lippman SA, Sucupira MCA, Jones HE, Luppi CG, Palefsky J, Wijgert JHHM, et al. Prevalence, distribution and correlates of endocervical human papillomavirus types in Brazilian women. Int J STD AIDS. 2010;21: 105–109. 10.1258/ijsa.2009.008436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Lopes F, Latorre M do RD de O, Pignatari ACC, Buchalla CM. HIV, HPV, and syphilis prevalence in a women’s penitentiary in the city of São Paulo, 1997–1998. Cad Saúde Pública. 2001;17: 1473–1480. [DOI] [PubMed] [Google Scholar]
- 64.Lorenzato F, Ho L, Terry G, Singer A, Santos LC, De Lucena Batista R, et al. The use of human papillomavirus typing in detection of cervical neoplasia in Recife (Brazil). Int J Gynecol Cancer Off J Int Gynecol Cancer Soc. 2000;10: 143–150. [DOI] [PubMed] [Google Scholar]
- 65.Lorenzi AT, Fregnani JHT, Possati-Resende JC, Antoniazzi M, Scapulatempo-Neto C, Syrjänen S, et al. Can the careHPV test performed in mobile units replace cytology for screening in rural and remote areas? Cancer Cytopathol. 2016;124: 581–588. 10.1002/cncy.21718 [DOI] [PubMed] [Google Scholar]
- 66.Lugo LZA, Jacob CMB, Machado AP, Almeida FG, Ávila LS, Prata TTM, et al. Human papillomavirus and coinfections with Chlamydia trachomatis, Gardnerella vaginalis, and Trichomonas vaginalis in self-collected samples from female sex workers in the Central-Western region of Brazil. J Bras Patol E Med Lab. 2018;54: 46–51. 10.5935/1676-2444.20180010 [DOI] [Google Scholar]
- 67.Martins TR, Fedrizzi EN, Alves EV, Vituri CL, Silva RM, Bazzo ML. Cervical Cytology, HPV DNA and MRNA—A Comparative Study in 162 Patients. J Bras Doenças Sex Transm DST. 2012;24: 79–84. 10.5533/DST-2177-8264-201224203 [DOI] [Google Scholar]
- 68.Martins TR, Mendes de Oliveira C, Rosa LR, Campos Centrone C, Rodrigues CLR, Villa LL, et al. HPV genotype distribution in Brazilian women with and without cervical lesions: correlation to cytological data. Virol J. 2016;13: 138 10.1186/s12985-016-0594-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Martins TR, Longatto-Filho A, Cohen D, Viscondi JYK, Fuza LM, Cury L, et al. Influence of Prior Knowledge of Human Papillomavirus Status on the Performance of Cytology Screening. Am J Clin Pathol. 2018;149: 316–323. 10.1093/ajcp/aqx163 [DOI] [PubMed] [Google Scholar]
- 70.McCormick TM, Canedo NHS, Furtado YL, Silveira FA, Lima RJ, Rosman ADF, et al. Association between human papillomavirus and Epstein—Barr virus DNA and gene promoter methylation of RB1 and CDH1 in the cervical lesions: a transversal study. Diagn Pathol. 2015;10: 59 10.1186/s13000-015-0283-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Miranda PM, Silva NNT, Pitol BCV, Silva IDCG, Lima-Filho JL, Carvalho RF, et al. Persistence or clearance of human papillomavirus infections in women in Ouro Preto, Brazil. BioMed Res Int. 2013;2013: 578276 10.1155/2013/578276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Muñoz N, Kato I, Bosch FX, Eluf-Neto J, De Sanjosé S, Ascunce N, et al. Risk factors for HPV DNA detection in middle-aged women. Sex Transm Dis. 1996;23: 504–510. 10.1097/00007435-199611000-00012 [DOI] [PubMed] [Google Scholar]
- 73.Naud P, Matos J, Hammes L, Stuckzynski J, Brouwers K, Magno V, et al. Factors predicting intermediate endpoints of cervical cancer and exposure to human papillomavirus (HPV) infections in young women screened as potential targets for prophylactic HPV vaccination in south of Brazil. Eur J Obstet Gynecol Reprod Biol. 2006;124: 110–118. 10.1016/j.ejogrb.2005.02.001 [DOI] [PubMed] [Google Scholar]
- 74.Nonato DR, Alves RRF, Ribeiro AA, Saddi VA, Segati KD, Almeida KP, et al. Prevalence and factors associated with coinfection of human papillomavirus and Chlamydia trachomatis in adolescents and young women. Am J Obstet Gynecol. 2016;215: 753.e1–753.e9. 10.1016/j.ajog.2016.07.003 [DOI] [PubMed] [Google Scholar]
- 75.Nonnenmacher B, Breitenbach V, Villa LL, Prolla JC, Bozzetti MC. Identificação do papilomavírus humano por biologia molecular em mulheres assintomáticas. Rev Saúde Pública. 2002;36: 95–100. [DOI] [PubMed] [Google Scholar]
- 76.Noronha VL, Cruz EM, Pinho CN, Mello WA, Villa LL, Russomano FB. Papilomavírus humano (HPV) em mulheres submetidas a rastreamento para câncer de cérvice uterina, Belém—Pará—Brasil. J Bras Doenças Sex Transm DST. 2011;23: 5–11. 10.5533/2177-8264-201123103 [DOI] [Google Scholar]
- 77.Oliveira FA, Pfleger V, Lang K, Heukelbach J, Miralles I, Fraga F, et al. Sexually transmitted infections, bacterial vaginosis, and candidiasis in women of reproductive age in rural Northeast Brazil: a population-based study. Mem Inst Oswaldo Cruz. 2007;102: 751–756. 10.1590/s0074-02762007000600015 [DOI] [PubMed] [Google Scholar]
- 78.Oliveira LHS, Ferreira MDPL, Augusto EF, Melgaço FG, Santos LS, Cavalcanti SMB, et al. Human papillomavirus genotypes in asymptomatic young women from public schools in Rio de Janeiro, Brazil. Rev Soc Bras Med Trop. 2010;43: 4–8. 10.1590/s0037-86822010000100002 [DOI] [PubMed] [Google Scholar]
- 79.Oliveira GR, Vieira VC, Barral MFM, Döwich V, Soares MA, Conçalves CV, et al. Fatores de risco e prevalência da infecção pelo HPV em pacientes de Unidades Básicas de Saúde e de um Hospital Universitário do Sul do Brasil. Rev Bras Ginecol E Obstetrícia. 2013;35: 226–232. [DOI] [PubMed] [Google Scholar]
- 80.Padovani CTJ, Bonin CM, Tozetti IA, Ferreira AMT, dos S Fernandes CE, Costa IP. Glucocorticoid-induced tumor necrosis factor receptor expression in patients with cervical human papillomavirus infection. Rev Soc Bras Med Trop. 2013;46: 288–292. 10.1590/0037-8682-0029-2013 [DOI] [PubMed] [Google Scholar]
- 81.Paesi S, Correa L, Tregnago MC, Mandelli J, Roesch-Ely M. Human papillomavirus among women with atypical squamous cells of undetermined significance in southern Brazil. Int J Gynecol Obstet. 2015;128: 23–26. 10.1016/j.ijgo.2014.07.027 [DOI] [PubMed] [Google Scholar]
- 82.Peres AL, Camarotti JRSL, Cartaxo M, Alencar N, Stocco RC, Beçak W, et al. Molecular analysis and conventional cytology: association between HPV and bacterial vaginosis in the cervical abnormalities of a Brazilian population. Genet Mol Res. 2015;14: 9497–9505. 10.4238/2015.August.14.13 [DOI] [PubMed] [Google Scholar]
- 83.Pinheiro MCN, Baia de Brito E, Nascimento Pinheiro D, Emanuelle Sanches Borges B, Silva Soares E, Antônia Nunes Gomes J, et al. Principais genótipos de papilomavírus humano em mulheres ribeirinhas na Amazônia brasileira. Rev Bras Em Promoção Saúde. 2016;29: 68–74. 10.5020/18061230.2016.p68 [DOI] [Google Scholar]
- 84.Pinto D da S, Fuzii HT, Quaresma JAS. Prevalence of genital HPV infection in urban and rural women in the Eastern Brazilian Amazon. Cad Saúde Pública. 2011;27: 769–778. 10.1590/s0102-311x2011000400016 [DOI] [PubMed] [Google Scholar]
- 85.Porcari AM, Negrão F, Tripodi GL, Pitta DR, Campos EA, Montis DM, et al. Molecular Signatures of High-Grade Cervical Lesions. Front Oncol. 2018;8: 99 10.3389/fonc.2018.00099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Rama CH, Roteli-Martins CM, Derchain SFM, Oliveira EZ, Aldrighi JM, Mariani Neto C. Serological detection of anti HPV 16/18 and its association with pap smear in adolescents and young women. Rev Assoc Médica Bras. 2006;52: 43–47. 10.1590/S0104-42302006000100021 [DOI] [PubMed] [Google Scholar]
- 87.Rama CH, Villa LL, Pagliusi S, Andreoli MA, Costa MC, Thomann P, et al. Opportunity for catch-up HPV vaccination in young women after first delivery. J Epidemiol Community Health. 2010;64: 610–615. 10.1136/jech.2008.086439 [DOI] [PubMed] [Google Scholar]
- 88.Resende LS de A, Rabelo-Santos SH, Sarian LO, Figueiredo Alves RR, Ribeiro AA, Zeferino LC, et al. A portrait of single and multiple HPV type infections in Brazilian women of different age strata with squamous or glandular cervical lesions. BMC Infect Dis. 2014;14: 214 10.1186/1471-2334-14-214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Richardson LA, El-Zein M, Ramanakumar AV, Ratnam S, Sangwa-Lugoma G, Longatto-Filho A, et al. HPV DNA testing with cytology triage in cervical cancer screening: Influence of revealing HPV infection status: HPV/Pap: Concealed Versus Revealed HPV. Cancer Cytopathol. 2015;123: 745–754. [DOI] [PubMed] [Google Scholar]
- 90.Rocha DAP, Barbosa Filho RAA, de Queiroz FA, dos Santos CMB. High Prevalence and Genotypic Diversity of the Human Papillomavirus in Amazonian Women, Brazil. Infect Dis Obstet Gynecol. 2013;2013: 514859 10.1155/2013/514859 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Rodrigues DA, Pereira ÉR, Oliveira LS de S, Speck NM de G, Gimeno SGA, Rodrigues DA, et al. Prevalence of cytological atypia and high-risk human papillomavirus infection in Panará indigenous women in Central Brazil. Cad Saúde Pública. 2014;30: 2587–2593. [PubMed] [Google Scholar]
- 92.Rodrigues LLS, Morgado MG, Sahasrabuddhe VV, De Paula VS, Oliveira NS, Chavez-Juan E, et al. Cervico-vaginal self-collection in HIV-infected and uninfected women from Tapajós region, Amazon, Brazil: High acceptability, hrHPV diversity and risk factors. Gynecol Oncol. 2018;151: 102–110. 10.1016/j.ygyno.2018.08.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Rosa MI, Fachel JMG, Rosa DD, Medeiros LR, Igansi CN, Bozzetti MC. Persistence and clearance of human papillomavirus infection: a prospective cohort study. Am J Obstet Gynecol. 2008;199: 617.e1–7 10.1016/j.ajog.2008.06.033 [DOI] [PubMed] [Google Scholar]
- 94.Roteli-Martins CM, Carvalho NS, Naud P, Teixeira J, Borba P, Derchain S, et al. Prevalence of human papillomavirus infection and associated risk factors in young women in Brazil, Canada, and the United States: a multicenter cross-sectional study. Int J Gynecol Pathol. 2011;30: 173–184. 10.1097/PGP.0b013e3181f38dfe [DOI] [PubMed] [Google Scholar]
- 95.Salcedo MMBP, Damin APS, Agnes G, Pessini SA, Beitune PE, Alexandre COP, et al. Prevalence of human papillomavirus infection in pregnant versus non-pregnant women in Brazil. Arch Gynecol Obstet. 2015;292: 1273–1278. 10.1007/s00404-015-3752-8 [DOI] [PubMed] [Google Scholar]
- 96.Santos CR, Franciscatto LG, Barcellos RB, Almeida SEM, Rossetti MLR. Use of FTA elute card impregnated with cervicovaginal sample directly into the amplification reaction increases the detection of human papillomavirus DNA. Braz J Microbiol. 2012;43: 389–392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Santos Filho MVC, Gurgel APAD, Lobo CDP, Freitas ACF, Silva-Neto JC, Silva LAF. Prevalence of human papillomavirus (HPV), distribution of HPV types, and risk factors for infection in HPV-positive women. Genet Mol Res. 2016;15: gmr8315. 10.4238/gmr.15028315 [DOI] [PubMed] [Google Scholar]
- 98.Silva KC, Rosa MLG, Moyse N, Afonso LA, Oliveira LH, Cavalcanti SM. Risk factors associated with human papillomavirus infection in two populations from Rio de Janeiro, Brazil. Mem Inst Oswaldo Cruz. 2009;104: 885–891. 10.1590/s0074-02762009000600011 [DOI] [PubMed] [Google Scholar]
- 99.Simões R, Silva E, Barth O. Lb3.246 Prevalence and risk factors of human papillomavirus infection in unimmunized women in brazil. Sex Transm Infect. 2017;93: A185–A186. 10.1136/sextrans-2017-053264.481 [DOI] [Google Scholar]
- 100.Smith JS, Muñoz N, Herrero R, Eluf-Neto J, Ngelangel C, Franceschi S, et al. Evidence for Chlamydia trachomatis as a human papillomavirus cofactor in the etiology of invasive cervical cancer in Brazil and the Philippines. J Infect Dis. 2002;185: 324–331. 10.1086/338569 [DOI] [PubMed] [Google Scholar]
- 101.Soares CP, Benatti Neto C, Fregonezi PAG, Teresa DB, de M Santos RT, Longatto Filho A, et al. Computer-assisted analysis of p53 and PCNA expression in oral lesions infected with human papillomavirus. Anal Quant Cytol Histol. 2003;25: 19–24. [PubMed] [Google Scholar]
- 102.Ströher DJ, Aramburu TDB, Nunes VT. Analysis of cytopathologic examination and hybrid capture in women receiving care in basic health units. J Bras Doenças Sex Transm DST. 2016;28: 110–114. [Google Scholar]
- 103.Syrjänen K, Naud P, Derchain S, Roteli-Martins C, Longatto-Filho A, Tatti S, et al. Comparing PAP smear cytology, aided visual inspection, screening colposcopy, cervicography and HPV testing as optional screening tools in Latin America. Study design and baseline data of the LAMS study. Anticancer Res. 2005;25: 3469–3480. [PubMed] [Google Scholar]
- 104.Tamegão-Lopes BP, Sousa-Júnior EC, Passetti F, Ferreira CG, Mello WA, Duarte Silvestre RV. Prevalence of human papillomavirus infection and phylogenetic analysis of HPV-16 E6 variants among infected women from Northern Brazil. Infect Agent Cancer. 2014;9: 25 10.1186/1750-9378-9-25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Teixeira LO, Vieira VC, Germano FN, Gonçalves CV, Soares MA, Martinez AMB. Prevalence of Human Papillomavirus types in women attending at University hospital in southern Brazil. Medicina (Mex). 2016;49: 116. [Google Scholar]
- 106.Torres KL, Mariño JM, Pires Rocha DA, Mello MB, Melo Farah HH, Reis R dos S, et al. Self-sampling coupled to the detection of HPV 16 and 18 E6 protein: A promising option for detection of cervical malignancies in remote areas. Tornesello ML, editor. PLoS One. 2018;13: e0201262 10.1371/journal.pone.0201262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Tota JE, Ramanakumar AV, Villa LL, Richardson H, Burchell AN, Coutlée F, et al. Cervical Infection With Vaccine-Associated Human Papillomavirus (HPV) Genotypes as a Predictor of Acquisition and Clearance of Other HPV Infections. J Infect Dis. 2016;214: 676–684. 10.1093/infdis/jiw215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Trugilo KP, Cebinelli GCM, Berti FCB, Okuyama NCM, Cezar-dos-Santos F, Sena MM, et al. Polymorphisms in the TGFB1 signal peptide influence human papillomavirus infection and development of cervical lesions. Med Microbiol Immunol (Berl). 2019;208: 49–58. 10.1007/s00430-018-0557-y [DOI] [PubMed] [Google Scholar]
- 109.Vieira RC, Monteiro J do SV, Manso EP, Dos Santos MRM, Tsutsumi MY, Ishikawa EAY, et al. Prevalence of type-specific HPV among female university students from northern Brazil. Infect Agent Cancer. 2015;10: 21 10.1186/s13027-015-0017-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Waisberg MG, Ribeiro ACM, Candido WM, Medeiros PB, Matsuzaki CN, Beldi MC, et al. Human papillomavirus and chlamydia trachomatis infections in rheumatoid arthritis under anti-TNF therapy: an observational study. Rheumatol Int. 2015;35: 459–463. 10.1007/s00296-014-3157-1 [DOI] [PubMed] [Google Scholar]
- 111.Wohlmeister D, Vianna DRB, Helfer VE, Gimenes F, Consolaro MEL, Barcellos RB, et al. Association of human papillomavirus and Chlamydia trachomatis with intraepithelial alterations in cervix samples. Mem Inst Oswaldo Cruz. 2016;111: 106–113. 10.1590/0074-02760150330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Xavier-Souza E, Rapp A, Teles P, Timbó M, Lessa K, Trindade R, et al. Risk factors associated to STI in female adolescents attending a reference centre in Bahia, Brazil. Int J Gynecol Obstet. 2018;143: EP0555. [Google Scholar]
- 113.Yamamoto LSU, Alves VAF, Maeda MYS, Longatto-Filho A, Utagawa ML, Eluf Neto J. A morphological protocol and guide-list on uterine cervix cytology associated to Papillomavirus infection. Rev Inst Med Trop São Paulo. 2004;46: 189–193. 10.1590/s0036-46652004000400003 [DOI] [PubMed] [Google Scholar]
- 114.Afonso LA, Cordeiro TI, Carestiato FN, Ornellas AA, Alves G, Cavalcanti SMB. High Risk Human Papillomavirus Infection of the Foreskin in Asymptomatic Men and Patients with Phimosis. J Urol. 2016;195: 1784–1789. 10.1016/j.juro.2015.12.096 [DOI] [PubMed] [Google Scholar]
- 115.Eleutério J, Barros IC, Cavalcante DIM, Eleutério RMN, Giraldo PC. HPV-DNA hybrid capture test: influence of cellularity in penile samples. Acta Cytol. 2010;54: 546–550. 10.1159/000325175 [DOI] [PubMed] [Google Scholar]
- 116.Franceschi S, Castellsagué X, Dal Maso L, Smith JS, Plummer M, Ngelangel C, et al. Prevalence and determinants of human papillomavirus genital infection in men. Br J Cancer. 2002;86: 705–711. 10.1038/sj.bjc.6600194 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Giraldo PC, Eleutério J, Cavalcante DIM, Gonçalves AKS, Romão JAA, Eleutério RMN. The role of high-risk HPV-DNA testing in the male sexual partners of women with HPV-induced lesions. Eur J Obstet Gynecol Reprod Biol. 2008;137: 88–91. 10.1016/j.ejogrb.2006.12.026 [DOI] [PubMed] [Google Scholar]
- 118.Menezes W, Ceperuelo DL, Cordeiro TI, Dobao E, Gouvêa TVD, Carestiato FN, et al. Human papillomavirus infection in healthy men from Rio de Janeiro, Brazil. J Bras Doenças Sex Transm DST. 2014;26: 21–24. 10.5533/DST-2177-8264-2014261-405 [DOI] [Google Scholar]
- 119.Rocha MG de L, Faria FL, Gonçalves L, Souza M do CM, Fernandes PÁ, Fernandes AP. Prevalence of DNA-HPV in male sexual partners of HPV-infected women and concordance of viral types in infected couples. PLoS One. 2012;7: e40988 10.1371/journal.pone.0040988 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Rocha WM, Afonso LA, Dobao E, Gouvea TD, Carestiato FN, Cavalcanti SMB. Evaluation of anogenital Human Papillomavirus Infection in asymptomatic men from Rio de Janeiro, Brazil. Rev Patol Trop. 2015;44: 375–385. [Google Scholar]
- 121.Rombaldi RL, Serafini EP, Villa LL, Vanni AC, Baréa F, Frassini R, et al. Infection with human papillomaviruses of sexual partners of women having cervical intraepithelial neoplasia. Braz J Med Biol Res. 2006;39: 177–187. 10.1590/s0100-879x2006000200003 [DOI] [PubMed] [Google Scholar]
- 122.Silva RJC, Casseb J, Andreoli MA, Villa LL. Persistence and clearance of HPV from the penis of men infected and non-infected with HIV. J Med Virol. 2011;83: 127–131. 10.1002/jmv.21950 [DOI] [PubMed] [Google Scholar]
- 123.Sudenga SL, Torres BN, Silva R, Villa LL, Lazcano-Ponce E, Abrahamsen M, et al. Comparison of the Natural History of Genital HPV Infection among Men by Country: Brazil, Mexico, and the United States. Cancer Epidemiol Biomarkers Prev. 2017;26: 1043–1052. 10.1158/1055-9965.EPI-17-0040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Eleutério J, Benício GC, Giraldo PC, Gonçalves AKS, Eleutério RMN, Oliveira DN, et al. Liquid-based cytology and HPV DNA testing using intra-anal specimens from HIV-negative women with and without genital HPV-induced lesions. Diagn Cytopathol. 2015;43: 360–365. 10.1002/dc.23238 [DOI] [PubMed] [Google Scholar]
- 125.Nyitray AG, Smith D, Villa L, Lazcano-Ponce E, Abrahamsen M, Papenfuss M, et al. Prevalence of and risk factors for anal human papillomavirus infection in men who have sex with women: a cross-national study. J Infect Dis. 2010;201: 1498–1508. 10.1086/652187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Soares PC, Ferreira S, Villa LL, Matos D. Identification of human papillomavirus in patients with anal squamous cell carcinoma and its relation with the grade of cellular differentiation and staging. Rev Bras Coloproctologia. 2011;31: 8–16. 10.1590/S0101-98802011000100002 [DOI] [Google Scholar]
- 127.Sudenga SL, Nyitray AG, Torres BN, Silva R, Villa L, Lazcano-Ponce E, et al. Comparison of anal HPV natural history among men by country of residence: Brazil, Mexico, and the United States. J Infect. 2017;75: 35–47. 10.1016/j.jinf.2017.03.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Veo CAR, Saad SS, Fregnani JHTG, Scapulatempo-Neto C, Tsunoda AT, Resende JCP, et al. Clinical characteristics of women diagnosed with carcinoma who tested positive for cervical and anal high-risk human papillomavirus DNA and E6 RNA. Tumour Biol J Int Soc Oncodevelopmental Biol Med. 2015;36: 5399–5405. 10.1007/s13277-015-3205-9 [DOI] [PubMed] [Google Scholar]
- 129.Antunes LCM, Lopes A de B, Pacheco LS, Brites PC, Muller LB, Fagundes RB. No role for infection with human papillomavirus in upper aerodisgestive tract cancers in smokers and alcoholics. J Clin Oncol. 2012;30: e14597–e14597. [Google Scholar]
- 130.Araújo MV de A, Pinheiro HHC, Pinheiro J de JV, Quaresma JAS, Fuzii HT, Medeiros RC. Prevalência do papilomavírus humano (HPV) em Belém, Pará, Brasil, na cavidade oral de indivíduos sem lesões clinicamente diagnosticáveis. Cad Saúde Pública. 2014;30: 1115–1119. [DOI] [PubMed] [Google Scholar]
- 131.Cavenaghi VB, Ghosn EJE, Cruz N, Rossi LM, da Silva L, Costa HO, et al. Determination of HPV prevalence in oral/oropharyngeal mucosa samples in a rural district of São Paulo. Braz J Otorhinolaryngol. 2013;79: 599–602. 10.5935/1808-8694.20130107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.da Silva CEX dos SR, Silva IDCG, Cerri A, Weckx LLM. Prevalence of human papillomavirus in squamous cell carcinoma of the tongue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104: 497–500. 10.1016/j.tripleo.2007.04.028 [DOI] [PubMed] [Google Scholar]
- 133.do Sacramento PR, Babeto E, Colombo J, Cabral Ruback MJ, Bonilha JL, Fernandes AM, et al. The prevalence of human papillomavirus in the oropharynx in healthy individuals in a Brazilian population. J Med Virol. 2006;78: 614–618. 10.1002/jmv.20583 [DOI] [PubMed] [Google Scholar]
- 134.Esquenazi D, Bussoloti Filho I, Carvalho M da G da C, Barros FS. The frequency of human papillomavirus findings in normal oral mucosa of healthy people by PCR. Braz J Otorhinolaryngol. 2010;76: 78–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Gonçalves AKS, Giraldo P, Barros-Mazon S, Gondo ML, Amaral RL, Jacyntho C. Secretory immunoglobulin A in saliva of women with oral and genital HPV infection. Eur J Obstet Gynecol Reprod Biol. 2006;124: 227–231. 10.1016/j.ejogrb.2005.06.028 [DOI] [PubMed] [Google Scholar]
- 136.Horewicz VV, Feres M, Rapp GE, Yasuda V, Cury PR. Human papillomavirus-16 prevalence in gingival tissue and its association with periodontal destruction: a case-control study. J Periodontol. 2010;81: 562–568. 10.1902/jop.2009.090571 [DOI] [PubMed] [Google Scholar]
- 137.Kreimer AR, Pierce Campbell CM, Lin H-Y, Fulp W, Papenfuss MR, Abrahamsen M, et al. Incidence and clearance of oral human papillomavirus infection in men: the HIM cohort study. The Lancet. 2013;382: 877–887. 10.1016/S0140-6736(13)60809-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Machado AP, Gatto de Almeida F, Bonin CM, Martins Prata TT, Sobrinho Ávilla L, Junqueira Padovani CT, et al. Presence of highly oncogenic human papillomavirus in the oral mucosa of asymptomatic men. Braz J Infect Dis. 2014;18: 266–270. 10.1016/j.bjid.2013.07.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Marques AEM, Barra GB, Resende Oyama CN, Guerra ENS. Low rate of oropharyngeal human papillomavirus infection of women with cervical lesions and their partners: new data from Brazilian population. J Oral Pathol Med. 2015;44: 453–458. 10.1111/jop.12252 [DOI] [PubMed] [Google Scholar]
- 140.Oliveira LHS, Santos LS, Silva CO, Augusto EF, Neves FPG. Papillomavirus infections in the oral and genital mucosa of asymptomatic women. Braz J Infect Dis. 2017;21: 88–91. 10.1016/j.bjid.2016.08.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Peixoto AP, Campos GS, Queiroz LB, Sardi SI. Asymptomatic oral human papillomavirus (HPV) infection in women with a histopathologic diagnosis of genital HPV. J Oral Sci. 2011;53: 451–459. 10.2334/josnusd.53.451 [DOI] [PubMed] [Google Scholar]
- 142.Silva CO, Santos LS, Pereira OMD, Azevedo KML, Oliveira LHS. High frequency of human papillomavirus type 53 in oral cavity of asymptomatic HIV-infected people. Braz J Infect Dis. 2016;20: 111–112. 10.1016/j.bjid.2015.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Tristão W, Ribeiro RMP, Oliveira CA, Betiol JC, Bettini J de SR. Epidemiological study of HPV in oral mucosa through PCR. Braz J Otorhinolaryngol. 2012;78: 66–70. 10.1590/S1808-86942012000400013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Vidotti LR, Vidal FCB, Monteiro SCM, Nunes JD, Salgado JV, Brito LMO, et al. Association between oral DNA-HPV and genital DNA-HPV. J Oral Pathol Med Off Publ Int Assoc Oral Pathol Am Acad Oral Pathol. 2014;43: 289–292. 10.1111/jop.12141 [DOI] [PubMed] [Google Scholar]
- 145.Xavier SD, Bussoloti Filho I, Carvalho JM, Castro TMPPG, Framil VM de S, Syrjänen KJ. Prevalence of human papillomavirus (HPV) DNA in oral mucosa of men with anogenital HPV infection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108: 732–737. 10.1016/j.tripleo.2009.06.020 [DOI] [PubMed] [Google Scholar]
- 146.Zonta MA, Monteiro J, Santos G Jr, Pignatari ACC. Infecção oral pelo HPV em mulheres com lesão escamosa de colo uterino no sistema prisional da cidade de São Paulo, Brasil. Braz J Otorhinolaryngol. 2012;78: 66–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Bomfim-Hyppólito S, Eleuterio J, Nunes GC, Bomfim-Hyppólito E, Franco ES, Neto R da JP. HIV or human papillomavirus co-infection among Brazilian individuals infected with hepatitis B and/or hepatitis C. Int J Gynecol Obstet. 2013;122: 258–260. 10.1016/j.ijgo.2013.04.012 [DOI] [PubMed] [Google Scholar]
- 148.Soares CC, Georg I, Lampe E, Lewis L, Morgado MG, Nicol AF, et al. HIV-1, HBV, HCV, HTLV, HPV-16/18, and Treponema pallidum infections in a sample of Brazilian men who have sex with men. PloS One. 2014;9: e102676 10.1371/journal.pone.0102676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Stiepcich MM, Silva ID, Scarpellini B. Abstract 5506: HPV genotyping of 15,307 Brazilian patients using a microarray based platform. Cancer Res. 2012;72: 5506–5506. 10.1158/1538-7445.AM2012-5506 [DOI] [Google Scholar]
- 150.Afonso LA, Rocha WM, Carestiato FN, Dobao EA, Pesca LF, Passos MRL, et al. Human papillomavirus infection among sexual partners attending a Sexually Transmitted Disease Clinic in Rio de Janeiro, Brazil. Braz J Med Biol Res. 2013;46: 533–538. 10.1590/1414-431X20132519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Autran R, Mont’Alverne R, Eleuterio J, Melo KMRL, Rebouças KCF, Moraes A, et al. Correlation between cytology and DNA-HPV screening of the cervix and anus of immunocompetent women. Int J Gynecol Obstet. 2018;143: 433. [Google Scholar]
- 152.Beder Ribeiro CM, Ferrer I, Santos de Farias AB, Fonseca DD, Morais Silva IH, Monteiro Gueiros LA, et al. Oral and genital HPV genotypic concordance between sexual partners. Clin Oral Investig. 2014;18: 261–268. 10.1007/s00784-013-0959-6 [DOI] [PubMed] [Google Scholar]
- 153.Carestiato FN, Silva KC, Dimetz T, Oliveira LHS, Cavalcanti SMB. Prevalence of human papillomavirus infection in the genital tract determined by hybrid capture assay. Braz J Infect Dis. 2006;10: 331–336. 10.1590/s1413-86702006000500006 [DOI] [PubMed] [Google Scholar]
- 154.Castro TMPPG, Bussoloti Filho I, Nascimento VX, Xavier SD. HPV detection in the oral and genital mucosa of women with positive histopathological exam for genital HPV, by means of the PCR. Rev Bras Otorrinolaringol. 2009;75: 167–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Lima MDM, Braz-Silva PH, Pereira SM, Riera C, Coelho AC, Gallottini M. Oral and cervical HPV infection in HIV-positive and HIV-negative women attending a sexual health clinic in São Paulo, Brazil. Int J Gynaecol Obstet. 2014;126: 33–36. 10.1016/j.ijgo.2014.01.017 [DOI] [PubMed] [Google Scholar]
- 156.Nicolau SM, Camargo CGC, Stávale JN, Castelo A, Dôres GB, Lörincz A, et al. Human papillomavirus DNA detection in male sexual partners of women with genital human papillomavirus infection. Urology. 2005;65: 251–255. 10.1016/j.urology.2004.09.031 [DOI] [PubMed] [Google Scholar]
- 157.Rosenblatt C, Lucon AM, Pereyra E a. G, Pinotti JA, Arap S, Ruiz CA. HPV prevalence among partners of women with cervical intraepithelial neoplasia. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet. 2004;84: 156–161. 10.1016/j.ijgo.2003.08.008 [DOI] [PubMed] [Google Scholar]
- 158.Forman D, de Martel C, Lacey CJ, Soerjomataram I, Lortet-Tieulent J, Bruni L, et al. Global Burden of Human Papillomavirus and Related Diseases. Vaccine. 2012;30: F12–F23. 10.1016/j.vaccine.2012.07.055 [DOI] [PubMed] [Google Scholar]
- 159.Brasil, Instituto Brasileiro de Geografia e Estatística. Sinopse do censo demográfico : 2010. Rio de Janeiro: IBGE; 2011.
- 160.Brasil, IBGE, Coordenação de População e Indicadores Sociais. Tábua completa de mortalidade para o Brasil [: análises e tabelas]. Rio de Janeiro: IBGE, Coordenação de População e Indicadores Sociais; 2018.
- 161.de Oliveira MM, de A Andrade SSC, de Oliveira PPV, Silva GA e, da Silva MMA, Malta DC. Cobertura de exame Papanicolaou em mulheres de 25 a 64 anos, segundo a Pesquisa Nacional de Saúde e o Sistema de Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico, 2013. Rev Bras Epidemiol. 2018;21: e180014. [DOI] [PubMed] [Google Scholar]
- 162.Dunne EF, Unger ER, Sternberg M, McQuillan G, Swan DC, Patel SS, et al. Prevalence of HPV infection among females in the United States. JAMA. 2007;297: 813–819. 10.1001/jama.297.8.813 [DOI] [PubMed] [Google Scholar]
- 163.Bruni L, Diaz M, Castellsagué X, Ferrer E, Bosch FX, Sanjosé S. Cervical human papillomavirus prevalence in 5 continents: meta-analysis of 1 million women with normal cytological findings. J Infect Dis. 2010;202: 1789–1799. 10.1086/657321 [DOI] [PubMed] [Google Scholar]
- 164.Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis. 2006;194: 1044–1057. 10.1086/507432 [DOI] [PubMed] [Google Scholar]
- 165.Giuliano AR, Lazcano-Ponce E, Villa LL, Flores R, Salmeron J, Lee J-H, et al. The Human Papillomavirus Infection in Men Study: Human Papillomavirus Prevalence and Type Distribution among Men Residing in Brazil, Mexico, and the United States. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2008;17: 2036–2043. 10.1158/1055-9965.EPI-08-0151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Dunne EF, Nielson CM, Stone KM, Markowitz LE, Giuliano AR. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis. 2006;194: 1044–1057. 10.1086/507432 [DOI] [PubMed] [Google Scholar]
- 167.Tam S, Fu S, Xu L, Krause KJ, Lairson DR, Miao H, et al. The epidemiology of oral human papillomavirus infection in healthy populations: A systematic review and meta-analysis. Oral Oncol. 2018;82: 91–99. 10.1016/j.oraloncology.2018.04.005 [DOI] [PubMed] [Google Scholar]
- 168.Syrjänen K, Pyrhönen S, Aukee S, Koskela E. Squamous cell papilloma of the esophagus: a tumour probably caused by human papilloma virus (HPV). Diagn Histopathol. 1982;5: 291–296. [PubMed] [Google Scholar]
- 169.Liyanage SS, Rahman B, Ridda I, Newall AT, Tabrizi SN, Garland SM, et al. The Aetiological Role of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma: A Meta-Analysis. PLOS ONE. 2013;8: e69238 10.1371/journal.pone.0069238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 170.de Matos LL, Miranda GA, Cernea CR, de Matos LL, Miranda GA, Cernea CR. Prevalence of oral and oropharyngeal human papillomavirus infection in Brazilian population studies: a systematic review. Braz J Otorhinolaryngol. 2015;81: 554–567. 10.1016/j.bjorl.2015.04.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.Brasil, Ministério da Saúde, Secretaria de Vigilância em Saúde, Depratamento de Vigilânida das Doenças Transmissíveis, Coordenação-geral do Programa Nacional de Imunizações. Informe técnico da ampliação da oferta das vacinas papilomavírus humano 6, 11, 16 e 18 (recombinante)–vacina HPV quadrivalente e meningocócica C (conjugada). Brasília; 2018 Mar.
- 172.Smith JS, Melendy A, Rana RK, Pimenta JM. Age-specific prevalence of infection with human papillomavirus in females: a global review. J Adolesc Health Off Publ Soc Adolesc Med. 2008;43: S5–25, S25.e1–41. 10.1016/j.jadohealth.2008.07.009 [DOI] [PubMed] [Google Scholar]
- 173.Wendland EM, Caierão J, Domingues C, Maranhão AGK, de Souza FMA, Hammes LS, et al. POP-Brazil study protocol: a nationwide cross-sectional evaluation of the prevalence and genotype distribution of human papillomavirus (HPV) in Brazil. BMJ Open. 2018;8: e021170 10.1136/bmjopen-2017-021170 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
(PDF)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.