

Abstract
Background and study aims Endoscopic full-thickness resection (EFTR) allows for treatment of epithelial and sub-epithelial lesions (SELs) unsuitable to conventional resection techniques. This meta-analysis aimed to assess the efficacy and safety of clip-assisted method for non-exposed EFTR using FTRD or over-the-scope clip of gastrointestinal tumors.
Methods A comprehensive literature search was performed. The primary outcome of interest was the rate of histologic complete resection (R0). Secondary outcomes of interest were the rate of enbloc resection, FTR, adverse events, and post-EFTR surgery. Random-effects model was used to calculate pooled estimates and generate forest plots.
Results Eighteen studies with 730 patients and 733 lesions were included in the analyses. Indications for EFTR were difficult/residual colorectal adenoma, adenoma at a diverticulum or appendiceal orifice and early cancer (n = 634), colorectal SELs (n = 42), and upper gastrointestinal lesions (n = 51), other colonic lesions (n = 6). Median size of lesions was 13.5 mm. There were 22 failed EFTR attempts. Pooled overall R0 resection rate was 82 % (95 % CI: 75, 89). The pooled overall FTR rate was 83 % (95 % CI: 77, 89). The pooled overall enbloc resection rate was 95 (95 % CI: 92, 96). The pooled estimates for perforation and bleeding were < 0.1 % and 2 %, respectively. Following EFTR, a total of 110 patients underwent surgery for any reason [pooled rate 7 % (95 % 2, 14). The pooled rates for post-EFTR surgery due to invasive cancer, for non-curative endoscopic resection and for adverse events were 4 %, < 0.1 % and < 0.1 %, respectively. No mortality related to EFTR was noted.
Conclusions EFTR appears to be safe and effective for gastrointestinal lesions that are not amenable to conventional endoscopic resection. This technique should be considered as an alternative to surgery in selected cases.
Introduction
Advanced endoscopic resection procedures like endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD) are established techniques for the treatment of gastrointestinal (gastrointestinal) neoplasia. For large colorectal polyps, endoscopic resection is successful in avoiding the need for surgery in up to 90 % of cases with low rates of adverse events (1.5 % for endoscopic perforation and 6.5 % for bleeding) 1 . However, the efficacy of endoscopic resection is mired in the setting of non-lifting lesions associated with fibrosis and scaring or in lesions located in a difficult area such as in a diverticulum or the appendiceal orifice 2 . Moreover, subepithelial lesions (SELs) such as neuroendocrine tumors in the gastrointestinal tract can be difficult to manage endoscopically. Although EMR is feasible in duodenal SELs < 1.5 cm, it is associated with low rates of complete resection. ESD is a feasible option with higher chances of complete resection rate with increased risk of perforation 3 .
Recently, endoscopic full-thickness resection (EFTR) has emerged as an option to remove difficult superficial mucosal lesions and SELs 4 that are not amenable to standard resection techniques. EFTR enables full-thickness resection including the muscularis propria layer and provides a complete basis for pathological diagnosis 3 . There are two EFTR approaches: (1) the tumor is resected first and defect closure is then performed (exposed EFTR); or (2) creating a serosa-to-serosa apposition underneath the tumor before resection (non-exposed EFTR) 5 . In the non-exposed technique, the bowel segment is retracted into the lumen with fixation of the serosal surfaces which can be done with the use of different techniques, such as the endoscopic plication with suturing devices, which is a technique designed for antireflux therapy limited to gastric interventions. Currently, the device most frequently used in Europe is called GERDx (G-SURG GmbH, Seeon-Seebruck, Germany)used as an antireflux device and also to treat SELs 6 . Another technique is the Submucosal Tunnel Endoscopic Resection (STER), where a submucosal tunnel is performed to access and resect a submucosal lesion, after which the tunnel entry site is closed. Clip assisted techniques can be performed without a dedicated device such as those performed with the Over-the-scope clips (OTSC) such as OVESCO and Padlock clip.
OTSC-assisted EFTR is a “close-then-cut” non-exposed EFTR technique that, in theory, could be a safer method than “cut-then-close” EFTR, because it avoids contamination of gastrointestinal luminal content into the peritoneum and prevents bleeding before full thickness resection. OTSC-assisted EFTR has been reported using over the scope clips such as the OVESCO or Padlock followed by resection of the pseudopolyp using a snare resection or a needle knife, or by using a dedicated full-thickness resection device (FTRD; Ovesco Endoscopy, Tuebingen, Germany) which consists of an OTSC preloaded into a cap with an integrated snare. The FTRD has recently been approved by the FDA in the United States for colorectal EFTR 2 5 . Although the use of a cap-mounted clip may aid hemostasis, its use has some limitations in regards to the visualization through the scope and the size of the lesions that can be removed, which must be less than 30 mm. Also, the external location of the snare might be associated with difficulties in the resection of the pseudopolyp after the clip is deployed.
To date, a number of studies on the efficacy and safety of the clip-assisted EFTR technique have been published, but results are variable. Therefore, the aim of our study was to perform a meta-analysis to summarize the current scientific evidence on efficacy, safety and clinical outcomes of patients with gastrointestinal neoplasia treated with clip-assisted non-exposure EFTR.
Methods
Information sources
We conducted a comprehensive literature search for studies of clip-assisted EFTR using “close-then-cut” technique for treatment of gastrointestinal lesions. The following electronic databases were searched: PubMed, Embase, Cochrane Library, Scopus, and Web of Science, for the period July1966 to April 2019. Terms used for the search are reported in online supplementary material. We contacted the authors when further information from selected papers was needed.
Eligibility criteria
Studies were included if they met the following criteria: (1) Original articles that assessed the use of clip-assisted non-exposed EFTR for upper or lower gastrointestinal neoplasia and provided outcomes of interest. gastrointestinal neoplasia included mucosal or SELs of the esophagus, stomach, duodenum and colorectal; (2) studies performed in humans; (3) studies that included more than 5 patients and (4) studies that were published in English. Exclusion criteria were: (1) studies using the non-clip assisted FTR technique; (2) studies of EFTR performed in animals; (3) review papers; (4) studies written in languages other than English; (5) case reports with less than 5 patients and (6) abstracts.
Study selection
We reported our results according to the MOOSE statement for meta-analyses of observational studies 7 . The initial search strategy was performed by a librarian (MT). All titles and abstracts of retrieved articles were revised by three investigators (OIBG, YH, GGB). Full-length publications of selected articles were screened for final inclusion. Any disagreement was resolved by a third investigator (SN). Data from the included studies was extracted into a data extraction sheet.
Data collection process and listed items
From each series, the investigators retrieved the following information: (1) country; (2) publication year; (3) enrollment period; (4) setting (single center/multicenter); (5) study design (prospective/retrospective); (6) number of patients included; (7) number of patients excluded; (8) reasons for exclusion; (9) total of patients included; (10) total number of EFTR attempted; (11) gender distribution; (12) site distribution (gastric/duodenal/colonic) of the lesions; (13) size of lesions; (14) device used for EFTR; (15) total procedure time (16) outcome of endoscopic resection at endoscopy (rate of success/failure); (17) rate of complete endoscopic resection (enbloc resection); (18) rate of microscopically negative deep and lateral margins (R0 resection); (19) rate of FTR (defined as presence of all layers of the wall including serosa within the resected specimen or presence of muscle layer in the resected specimen, depending on the studies); (20) rate of total adverse events (AEs); (21) rate of intra-procedural or (22) post-procedural bleeding; (23) rate of perforation; (24) rate of surgery for AEs; (25) rate of surgery for non-curative endoscopic resection of precancerous lesions; (26) rate of surgery due to invasive cancer; (27) duration of post-procedural follow-up; (28) number of patients with follow-up data; (28) rate of loss of follow-up; (29) performance of biopsies from scar.
Risk of bias in individual studies
Newcastle-Ottawa Scale (NOS) was used to record the information on the methodological quality of each included study and for quality assessment 8 . Representativeness of the study cohorts, ascertainment of exposure, demonstration that the outcome of interest was not present at the start of a study, assessment of outcome and adequate length of endoscopic follow-up was assessed for each study.
Over-the-scope clips and FTRD
The OVESCO OTSC (Ovesco Endoscopy, Tuebingen, Germany) has been used for clip-assisted EFTR. It resembles a bear claw once deployed. The cap diameter is available in three sizes (11, 12 and 14 mm) and two depths (3 and 6 mm). There are three different teeth configurations: type a (blunt teeth), type t (small spikes on teeth) and type gc (spikes on elongated teeth). For EFTR in upper gastrointestinal lesions, it is recommended to use the 12/6 type t clip. For colorectal lesion, the 12/6 or 14/6 type t clip are considered best options 2 .
Another type of OTSC that has been used for EFTR is a flat star-shaped nitinol clip with six inner needles preloaded into a cap (Padlock Pro-select, Aponos Medical Corp., Kingston, New Hampshire, United States). This clip is available in two sizes; the standard Padlock fits a 9.5–11-mm diameter scope and the Padlock Pro-select fits an 11.5–14 mm diameter scope. An advantage of this clip design is that the wire that deploys the clip goes along the shaft of the scope, freeing the working channel of the endoscope 2 3 .
The FTRD (Ovesco Endoscopy, Tuebingen, Germany) consists of an OTSC preloaded into a cap with an integrated snare. The inner diameter of the cap of the device limits the maximum size of the lesion to be removed 5 . Its use is recommended for epithelial lesions < 30 mm and SELs < 20 mm in the colo-rectum. The current system has an outer diameter of 21 mm making per-oral insertion and passage through the esophagus significantly more difficult than in the colo-rectum. Insertion of the FTRD through the esophagus has to be performed carefully because of the large outer diameter of the FTRD (21 mm). Balloon dilation or bougienage of the upper esophageal sphincter may be necessary in some cases. Further technical modifications (i.e., smaller cap size, more flexibility) could facilitate usage of the FTRD in the upper gastrointestinal tract.
Outcomes
The primary outcomes of this meta-analysis were rates of complete histological resection (R0), microscopically negative deep and lateral margins , of upper and lower gastrointestinal epithelial and SELs. Secondary outcomes were en bloc resection, FTR (defined as the presence of all layers of the wall including the serosa in the resected specimen or presence of muscle layer in the resected specimen) and AEs related to the EFTR (bleeding, perforation, and appendicitis). In addition, rates of surgery for any reasons, surgery due to incomplete resection, surgery due to AEs and surgery due to invasive cancer were also investigated. Subgroup analyses were also performed according to the type of OTSC device used, lesion location and indications, such as patients with difficult colorectal adenoma due to recurrent or incomplete resected lesions or adenomas at a difficult location such as the appendiceal orifice or diverticulum, and early carcinomas.
Statistical analysis
Data on the primary and secondary outcomes relevant to this study were extracted when available. Missing information was obtained by contacting the primary authors through personal communication, if available.
For each of the study questions, cumulative data from each individual study was summarized to obtain pooled rates and the 95 % confidence intervals. All analyses were done in StataMP (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, Texas, United States: StataCorp LP). Given the clinical heterogeneity noted among the individual studies, random effects models were used for all analyses. Metaprop statistical program was used in Stata to perform the meta-analyses of proportions 9 . Metaprop is most suitable for binomial data and provides methods for proportions which are close to margins by allowing the Freeman-Tukey double arcsine transformation to stabilize the variances. Subgroup analyses were performed when appropriate. The heterogeneity between the sub-groups and among the individual studies was calculated using the I 2 statistic, reported with the associated p-value. The I 2 statistic can be categorized as for low level (< 25 %), moderate level (25 %–50 %) and high level of heterogeneity (> 75 %), respectively. P < 0.05 was considered statistically significant. The risk of publication bias was assessed for the primary outcome, R0 pooled resection rates of all lesions, using funnel plots and funnel plot asymmetry was tested using Egger’s regression test. To further evaluate the effect of small studies with less precise estimate, we performed cumulative meta-analysis by adding studies sequentially in step-wise fashion according to the sample size, i. e. the largest study was used in step 1, and the second largest study was added in step 2 and so on until all studies were added to the analysis. This also serves as sensitivity analysis by comparing summary estimate in each step to the full sample estimate, examining the drifts from center.
Results
Study selection
The study flow chart is shown in Fig. 1 . A total of 620 studies were retrieved, of which 229, 187, 148, 53 and 3 studies were identified by the searches in Scopus, PubMed, EMBASE, Web of Science and Cochrane respectively. After excluding the duplicates, 380 were included. Then upon reviewing titles and abstracts, 97 studies were found to be eligible and reviewed in full text. Of these, 18 were included in the analyses, while 79 were excluded.
Fig. 1.
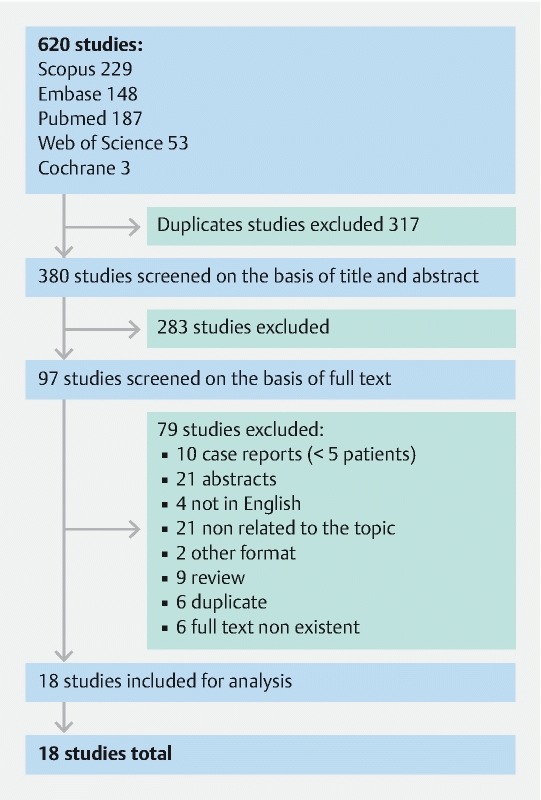
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097
Characteristics of the included studies
Main characteristics of the included studies are provided in Table 1 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 . Overall, 15 (83.3 %) studies were performed in Europe, two (11.1 %) being from the United States and one (5.5 %) from China. Three (16.7 %) series were published in the 2019, five (27.8 %) in 2018, eight (44.4 %) in 2017, one (5.5 %) in 2015 and one (5.5 %) in 2014 . Median duration of the enrollment per study was 1.5 years (range: 7.2 months–4.4 years). Most of the studies were single-center (10, 55.5 %), four two-center (22.2 %), three multicenter (16.7 %) and one not specified (5.5 %). The majority (13, 72.2 %) were retrospective.
Table 1. Main characteristics of included studies.
| Author | Year of publication | Country | Study design | Multicenter/single center | Study period | Total patients | Males (%) | Age (mean) | Attempted/failed attempt EFTR |
| Al-Bawardy, et al 10 | 2017 | US | Retrospective | 1 center | Jun 2014–Oct 2015 | 9 | 7 (78) | 63 | 9/0 |
| Backes, et al 11 | 2017 | The Netherlands | Prospective | 2 centers | Oct 2015–Dec 2016 | 26 | 13 (50) | 70 | 26/0 |
| Dinelli, et al 12 | 2017 | Italy | Retrospective | 2 centers | Unknown, 18-month period | 6 | 4 (67) | 68.5 | 7/0 |
| Schmidt, et al 13 | 2017 | Germany | Prospective | Multicenter (9) | Feb 2015–Apr 2016 | 181 | 99 (55) | 65 | 181/0 |
| Valli, et al 14 | 2017 | Switzerland | Retrospective | 1 center | Jun 2012–Oct 2016 | 60 | Not reported | 68 | 60/2 |
| Kappelle, et al 3 | 2017 | The Netherlands | Prospective | 1 center | Jan 2015–Jul 2016 | 12 | 8 (67) | 52.8 | 13/2 |
| Bas van der Spek 15 | 2018 | The Netherlands | Retrospective | 1 center | July 2015–October 2017 | 48 | 30 (63) | 67 | 51/1 |
| Markus Bauder 16 | 2018 | Germany | Retrospective | 1 center | March 2014–June 2017 | 20 | 13 (65) | 68 | 20/1 |
| Schmidt, et al 17 | 2015 | Germany | Retrospective | 2 centers | Jul 2012–Jul 2014 | 25 | Not reported | 70 | 25/1 |
| Sarker, et al 18 | 2014 | US | Retrospective | 1 center | Unknown, 12-month period | 8 | 8 (67) | 61.6 | 8/0 |
| Aepli P. 19 | 2017 | Switzerland | Retrospective | Multicenter (2) | May 2015–November 2016 | 33 | 23 (74.19) | 65.9 years | 33/2 |
| G. Andrisani 20 | 2019 | Italy | Retrospective | Multicenter (12) | January 2015–March 2018 | 114 | 61 (55.4) | 68 years | 107/0 |
| Armin Kuellmer 21 | 2019 | Germany | Retrospective | Multicenter (96) | September 2015–July 2018 | 1234 | 101 (64.7) | 72 years | 156/12 |
| Maxime E. S. Bronzwaer 22 | 2018 | The Netherlands | Prospective | 1 center | November 2016–December 2017 | 8 | 1 (14.2) | 64 years | |
| Francesco Vitali 23 | 2018 | Germany | Retrospective | 1 center | June 2015–June 2017 | 13 | 7 (53.8) | 64.3 years | |
| Wenhai Wang 24 | 2019 | China | Retrospective | 1 center | December 2014–August 2016 | 11 | 2 (40) | 60.2 years | |
| Paola Soriani 25 | 2017 | Italy | Retrospective | 1 center | June 2015–February 2016 | 6 | 5 (83.3) | 63 years | |
| Susana Mão de-Ferro 26 | 2018 | Portugal | Prospective | 1 center | March 2017–February 2018 | 9 | 6 (66) | 69 years |
EFTS, endoscopic full-thickness resection
Risk of bias assessment
Selection bias
The representativeness of each study’s cohort was appropriate, with no major selection bias identified ( Table 2 ) 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 . All study cohorts included patients who were felt to have lesions amenable to clip-assisted EFTR. These patients had undergone endoscopy that either identified lesions that were inadequately (i. e. R1 resection) or unsuccessfully (i. e. recurrent non-lifting adenoma) resected by conventional polypectomy or found lesions that would be unfeasible with conventional polypectomy. However, not all studies were explicit in their exclusion criteria.
Table 2. Quality assessment performed using the Newcastle-Ottawa Scale (NOS).
| Selection | Exposure | Outcome | ||||
| Study | Representativeness of cohort | Demonstration that outcome of interest was not present at start of study | Ascertainment of exposure | Assessment of outcome | Was follow-up long enough for outcomes to occur? | Adequacy of follow-up of cohorts |
| Al-Bawardy, et al 10 | Yes | Yes | Yes | Yes | Yes | No |
| Backes, et al 11 | Yes | Yes | Yes | Yes | Yes | No |
| Dinelli, et al 12 | Yes | Yes | Yes | Yes | Yes | Yes |
| Schmidt, et al 13 | Yes | Yes | Yes | Yes | Yes | Yes |
| Valli, et al 14 | Yes | Yes | Yes | Yes | Yes | Yes |
| Kappelle, et al 3 | Yes | Yes | Yes | Yes | Yes | Yes |
| Bas van der Spek 15 | Yes | Yes | Yes | Yes | Yes | No |
| Markus Bauder 16 | Yes | Yes | Yes | Yes | Yes | Yes |
| Schmidt, et al 17 | Yes | Yes | Yes | Yes | Yes | Yes |
| Sarker, et al 18 | Yes | Yes | Yes | Yes | Yes | No |
| Aepli P. 19 | Yes | Yes | Yes | Yes | Yes | No |
| G. Andrisani 20 | Yes | Yes | Yes | Yes | Yes | Yes |
| Armin Kuellmer 21 | Yes | Yes | Yes | Yes | Yes | Yes |
| Maxime E. S. Bronzwaer 22 | Yes | Yes | Yes | Yes | Yes | No |
| Francesco Vitali 23 | Yes | Yes | Yes | Yes | Yes | Yes |
| Wenhai Wang 24 | Yes | Yes | Yes | Yes | Yes | Yes |
| Paola Soriani 25 | Yes | Yes | Yes | Yes | Yes | Yes |
| Susana Mão de-Ferro 26 | Yes | Yes | Yes | Yes | Yes | Yes |
Ascertain of exposure
All studies utilized a medical record to access patient data, endoscopic reports, and histopathologic reports.
Outcome bias
Regarding assessment of outcomes, all studies reported R0 resection, post-EFTR histologic findings, adverse events, and technical success, which was defined by all studies as uncomplicated clip deployment and complete macroscopic removal of the lesion.
The studies included in this study demonstrated variability in adequacy and duration of cohort follow-up. Five studies experienced loss of greater than 20 % of its cohort at follow-up (21 %–42 %), while an additional three studies experienced loss of greater than 10 % of its cohort at follow-up (11 %–15 %). Follow-up was not systematically scheduled in all studies, however, all studies had a mean or median follow-up duration exceeding eight weeks, which was felt to be clinically adequate to monitor for post-procedural complications.
Patient characteristics
Study population comprised 730 patients with at least one gastrointestinal neoplasia. Distribution of the population age and sex was available for 18 and 16 series, respectively. Medians of age and male sex were 66.4 (range: 20–92 years) and 63.8 % (range: 14.2–83.3 %), respectively.
The total number of gastrointestinal lesions included was 733. Mean size was reported in 17 out of the 18 series, with the median being 13.5 mm (range: 11–24 mm). Distribution sites within the gastrointestinal tract was available for 18 series. Overall, 682/733 (93 %) were located in the colon or rectum and 51 of 733 (6.9 %) were in the upper gastrointestinal tract.
Regarding type of lesions in colorectal EFTR group: 414 of 682 non-lifting/residual/recurrent adenomas, 57 adenomas at the appendiceal orifice, 42 of 682 were colonic SELs, 15 of 682 colonic adenomas involving diverticulum, and 148 of 682 early carcinomas; six of 682 were classified as other lesions. Site distribution within the colo-rectum was as follows: In the proximal colon 295 of 682, distal colon 385 of 682 of which 295 of 682 were located in the rectum and two of 682 were ileo-colon anastomosis.
For clip-assisted EFTR for upper gastrointestinal lesions: 35 of 51 esophageal, gastric and duodenal lesions were SELs, six of 51 were duodenal non-lifting adenomas, seven of 51 treatment-naïve duodenal adenomas, one duodenal adenocarcinoma, one lesion classified as other duodenal lesion. In detail, distribution within the upper gastrointestinal tract was as follows: one of 51 in the fundus, two of 51 were located in the gastric cardia, seven of 51 in the gastric body, three of 51 in the gastric antrum, none of 51 in the duodenal bulb and 20 of 51 in the descending duodenum; two of 51 in the horizontal duodenum. Six of 51 were not specified, of which two were in the stomach, four in the duodenum. One lesion was found in the esophagus.
Procedure characteristics
Information about the devices used for EFTR was available in all series. Twelve studies used the FTRD, three used the Padlock clip, two used the OVESCO clips and in one study, both the Padlock and OVESCO clips were used. Overall, there were 22 unsuccessful attempts of EFTR. The reasons for failure were inability to advance the device through a narrowed/fixed space (n = 6), malfunction of the snare (n = 11), incorrect application (n = 2) and inability to suction the lesion into the cap (n = 3). Data on procedure time were recorded in 17 studies (89.5 %), and defined as time from scope in to scope out. Mean procedure time was 52.2±14.8 minutes. After the procedure, in 14 of 18 series (77.8 %), authors reported that patients were routinely hospitalized for observation for a median of 2 days [IQR 1.1–2.4].
Definition of histologic FTR was reported in 12 of 18 (66.7 %) series. FTR was defined as presence of all layers of the wall including the serosa in the resected specimen in seven studies, and as presence of muscle layer in the resected specimen in five studies.
Outcomes
Primary outcomes
Information regarding R0 resection was available in all series. Of the entire cohort, 568 patients achieved R0 resection. The pooled overall R0 resection rate was 82 % (95 % CI: 75, 89; I 2 = 72.2 %, P < 0.01) ( Fig. 2 ). The pooled overall R0 resection rate in the studies using the Padlock or OVESCO clips was 83 % (CI 95 %: 52, 100; I 2 = 83 %, P < 0.01) and 83 % (CI: 76, 88; I 2 = 61.1%, P < 0.01) in the studies using the FTRD. In addition, the pooled R0 resection rate for difficult adenoma was 80 % (95 % CI: 67, 91; I 2 = 81.8 %, P < 0.01) ( Fig. 3 ) and 78 % (95 %, CI: 54, 95, I 2 = 68.2, P = 0.01) for early carcinomas ( Fig. 4 ). The subgroup analysis of the R0 resection rates is available in Table 3 .
Fig. 2.
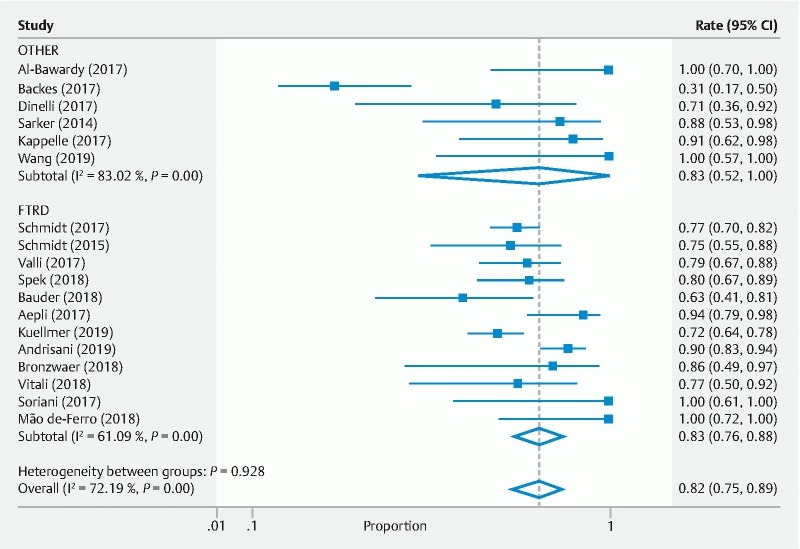
Pooled Rates of Overall R0 Resection. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
Fig. 3.
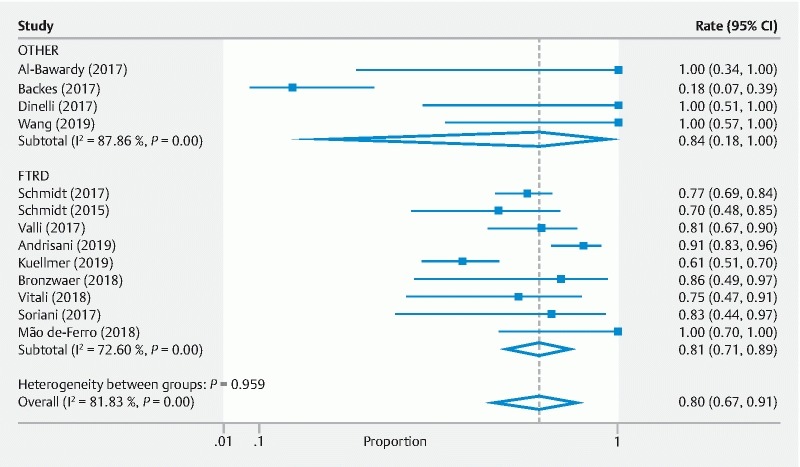
Pooled rates of R0 resection for colon difficult adenoma. Other: OTSC (OVESCO, Padlock); FTRD, full thickness resection device
Fig. 4.
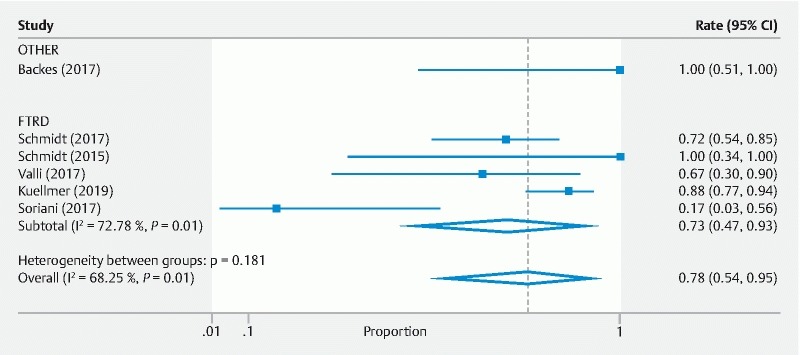
Pooled rates of R0 resection for colon early carcinoma. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
Table 3. Subgroup analyses for R0 resection rates.
| Subgroup | Number of studies included | Number of patients | Pooled rate (95 % CI) | I2 | P value |
| Difficult colorectal polyps | 14 10 11 12 13 14 17 20 21 22 23 24 25 26 | 324 | 80 (67–91) | 81.83 % | < 0.01 |
| Colorectal early carcinoma | 7 11 13 14 17 21 25 | 88 | 78 (54–95) | 68.25 % | < 0.01 |
| Colorectal SELs | 8 10 12 13 17 18 20 23 26 | 38 | 100 (95–100) | 0 | 0.99 |
| Upper GI SELs | 5 3 10 14 16 18 24 | 30 | 81 (58–97) | 47.97 % | 0.09 |
| Devices | |||||
| Lower EFTR | |||||
|
12 13 14 15 17 19 20 21 22 23 25 26 | 508 | 84 (77–89) | 60.71 % | < 0.01 |
|
5 10 11 12 18 24 | 21 | 68 (31–197) | 65.37 % | 0.02 |
| Upper EFTR | |||||
|
2 14 16 | 5 | 80 (47–100) | N/A 1 | N/A 1 |
|
4 3 10 18 24 | 22 | 80 (45–100) | 68.62 % 1 | 0.02 1 |
SELs, subepithelial lesions; EFTR, endoscopic full-thickness resection; FTRD, full-thickness resection device; OTSC, over the scope clips
Insufficient numbers/degrees of freedom (2)
Secondary outcomes
Regarding enbloc resection rates, information was available in 18/18 series. Of the total cohort, 672 cases reported successful en bloc resection, with a pooled overall en bloc resection rate of 95 % (95 % CI: 92, 96; I 2 = 0 %, P = 0.62) ( Fig. 5 ). The pooled en bloc resection rate was 100 % (95 % CI: 93,100; I 2 = 0 %, P = 0.79) for upper gastrointestinal SELs, 100 % (95 % CI 95, 100; I 2 = 0 %, P = 1.00) for colorectal SELs, 96 % (95 % CI: 92, 99; I 2 = 14.5 %, P = 0.30) for difficult colorectal adenomas and 95 % (95 % CI: 83,100; I 2 = 0 %, P = 0.89) for early carcinomas. The pooled en bloc resection rate per type of device was 100 % (95 % CI: 97, 100; I 2 = 0 %, P = 1.00) in the Padlock or OVESCO clip group and 95 % (95 % CI: 91, 95; I 2 = 0 %, P = 0.76) in the FTRD group.
Fig. 5.
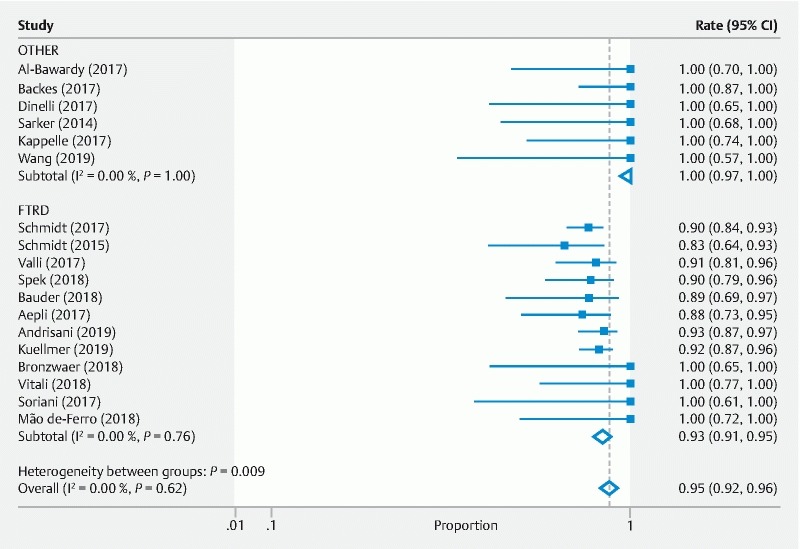
Pooled rates of overall en bloc resection. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
Overall, FTR was achieved in 593 patients. The pooled overall FTR rate was 83 % (95 % CI: 77, 89; I 2 = 62.7 %, P < 0.01) ( Fig. 6 ). The pooled FTR rate was 69 % (95 % CI: 41, 92; I 2 = 53.8 %, P = 0.07), 94 % (95 % CI 78, 100; I 2 = 0 %, P = 0.98), 91 % (95 %CI: 85, 96; I 2 = 29.3 %, P = 0.17) and 93 % (95 % CI: 82, 99, I 2 = 25.9 %, P = 0.23) for upper gastrointestinal SELs, colorectal SELs, difficult colorectal adenomas and early carcinomas, respectively. The pooled FTR rate by device was 72 % (95 % CI: 40, 96; I 2 = 81.5 %, P ≤ 0.01) in the Padlock or OVESCO clip group and 86 % (95 % CI: 81, 90; I 2 = 38.3 %, P = 0.09) in the FTRD group.
Fig. 6.
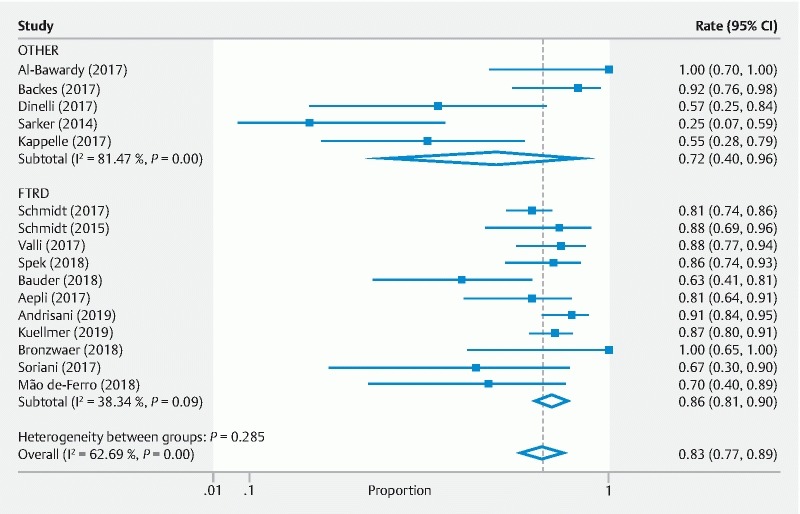
Pooled rates of overall FTR. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
Adverse events
Information pertained to AEs was reported in all studies. A total of 90 adverse events were reported. The overall pooled rate of adverse events was 11 % (95 % CI: 7, 15; I 2 = 35.5 %, P = 0.07) including: bleeding (28 patients), perforation (17 patients), micro perforation (3 patients), appendicitis (6 patients), post polypectomy syndrome (9 patients), abdominal pain (6 patients), post procedure cardiac event (1 patient), urinary retention and tenesmus (2 patients), traumatic wall lesions (4 patients), perineal pain (1 patient), peritonitis (2 patients), abscess adjacent to the OTSC (1 patient), leak (1 patient), stenosis (1 patient), entero-colonic fistula (1 patient) and seven patients described with mild AEs ( Fig. 7 ). The pooled estimate rates for perforation and bleeding were 0 % (95 % CI: 0, 1; I 2 = 0 %, P = 0.88) and 2 % (95 % CI: 1, 3; I 2 = 4.3 %, P = 0.40), respectively. Of 57 patients with adenoma involving the appendiceal orifice, the pooled estimates of appendicitis after EFTR was 3 % (95 % CI: 0, 14; I 2 = 0 %, P = 0.82). One patient developed an entero-colonic fistula after EFTR of a cecal adenoma. It was believed to occur due to entrapment of small bowel into the clip during resection. This patient was referred to surgery. No mortality related to EFTR was reported.
Fig. 7.
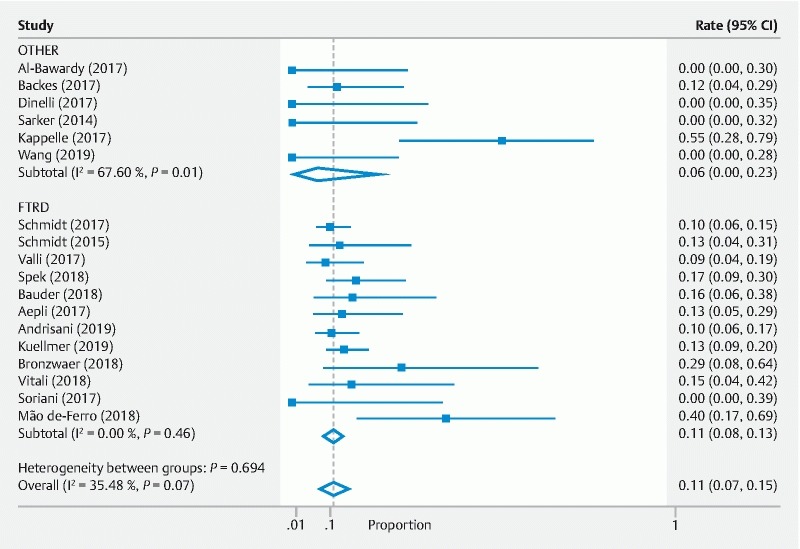
Pooled rates of adverse events. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
When analyzing adverse events by type of study (prospective vs. retrospective), in the retrospective studies the pooled rate of adverse events was 11 % (95 % CI: 9,15; I 2 = 0 %, P = 0.89) whereas in the prospective studies was 23 % (95 % CI: 8, 43; I 2 = 76.4 %, P < 0.01).
Need for surgery after EFTR
Following EFTR, 110 patients in total underwent surgery [pooled rate 7 % (95 % CI: 2, 14; I 2 = 82.3 %, P < 0.01) ( Fig. 8 ). Seventy-nine (79) for non-curative/deep invasive cancer, 13 for incomplete or unsuccessful resection of precancerous lesions, 15 underwent surgery due to adverse events, two due to recurrence and one due to EFTR failure. This information was available from 12 of 18 (66.6 %) studies. The pooled rates for post-EFTR surgery due to invasive cancer, for non-curative endoscopic resection of precancerous lesions and for adverse events was 4 % (95 % CI: 0, 10; I 2 = 81.8 %, P < 0.01), < 0.1 % (95 % CI: 0, 1; I 2 = 0 %, P = 0.73) and < 0.1 % (95 % CI: 0, 1; I 2 = 0 %, P = 0.94), respectively.
Fig. 8.
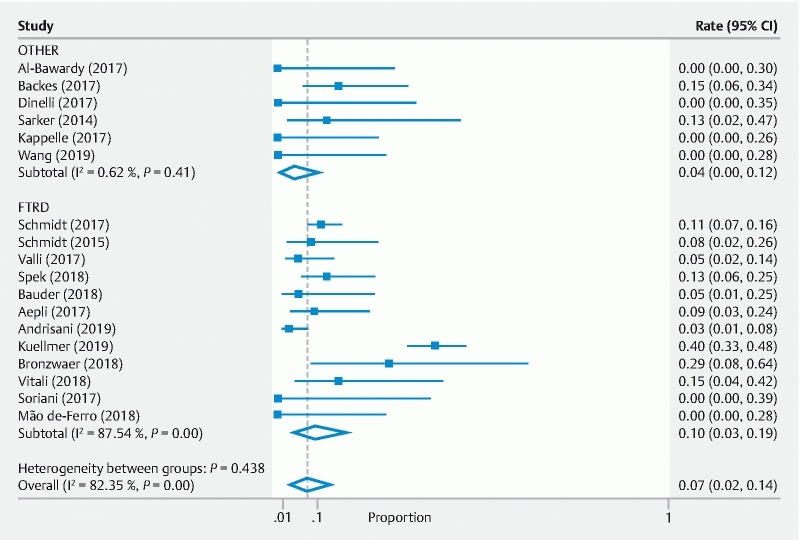
Pooled rates for need for surgery. Other: OTSC (OVESCO, Padlock); FTRD, full-thickness resection device
Follow-up
Follow-up time after EFTR was reported in all series with a median of 196.5 days [IQR 131.2–271.7]. Information on follow up endoscopy after EFTR was reported in 18/18 (100 %) series. Overall, 540 of 730 (74 %) patients underwent a follow up endoscopy while 85 of 730 (11.6 %) patients were lost to follow up and there is no information in 105 of 730 (14.3 %) patients. In the 540 patients who underwent a follow-up endoscopy, 374 (69.2 %) had spontaneous clip detachment while 25 (4.6 %) underwent clip removal; in the remaining 141 patients (25.1 %) the clip was left in place. Biopsy was taken in 273 of 540 (50.5%) patients who underwent endoscopy. There was recurrence/residual disease in 47 of 540 patients (8.7 %).
Publication bias
We evaluated the possibility of publication bias for the main outcome, R0 pooled resection rate of all lesions. The Egger’s regression ( P = 0.578) demonstrated no significant publication bias ( Fig. 9 ). The small study effect was also evaluated by cumulative analysis. This cumulative meta-analysis method demonstrated that as less precise studies were added there was no drift in the cumulative effect estimate ( online supplementary Fig. 1 ).
Fig. 9.
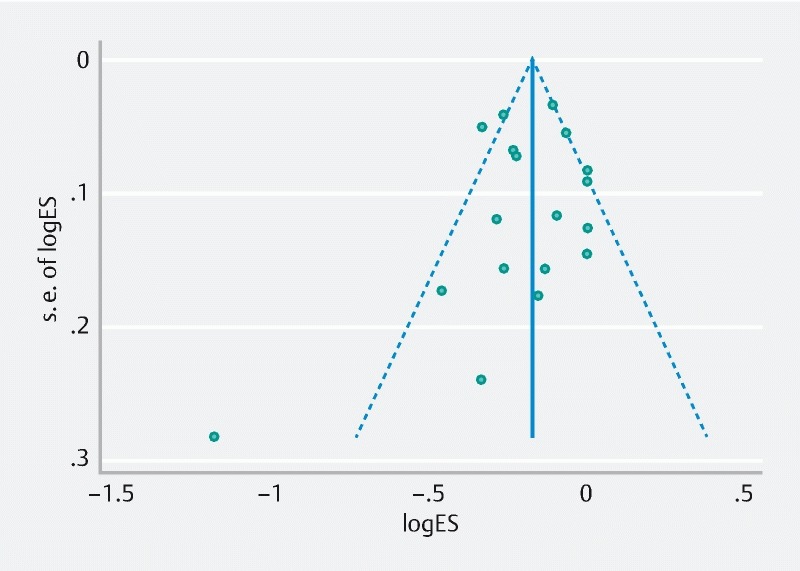
Publication bias Forest plot.
Discussion
In this meta-analysis, we found that clip assisted non-exposure EFTR is a feasible technique for difficult gastrointestinal lesions, such as difficult colorectal adenomas, early carcinomas and gastrointestinal SLEs, with overall R0 resection rates of 82 %, en bloc resection rates of 95 % and FTR rates of 83 %. Moreover, there is an acceptable rate of AEs (11 %) and a risk of surgery due to EFTR-related adverse events (< 0.1 %). The above-mentioned results support this technique as a potential alternative to surgery for colorectal lesions that failed to respond to standard endoscopic resection, challenging locations such as polyps involving the appendiceal orifice or a diverticulum, and SELs.
In this study, non-lifting from fibrosis due to recurrent adenomas or prior incompletely resected lesions was the most common indication of EFTR (in 414 of 682 cases) with pooled R0 rates of 80 % for this indication. This group of patients represent a challenging situation and are commonly referred to surgical resection 27 . Other endoscopic techniques to manage these lesions have been described such as ablation using soft coagulation or argon plasma coagulation, ESD, dissection-enabled scaffold-assisted resection, cold snare, and underwater resection 28 29 30 . Success rates of these techniques vary between 59 % and 100 % 28 29 30 and require close endoscopic monitoring for recurrence if the lesion is not removed en bloc. ESD for non-lifting or recurrent lesion is technically demanding and requires extensive experience in colorectal ESD which limits its use in the Western countries. Clip-assisted EFTR represents a viable option for this indication with potential advantages being the ability to perform complete resection and lower risk of recurrence. Further comparative studies are required to evaluate safety and efficacy of EFTR compared to other techniques.
Regarding the subgroup of patients with adenomas involving the appendiceal orifice this is considered to be a difficult anatomic location for endoscopic resection. There have been few reports of endoscopic resection of colon polyps involving the appendiceal orifice 31 32 33 . In patients with no prior history of appendectomy, when the deep margin into the appendiceal lumen is not well visualized, complete resection is not possible endoscopically. Thus, these lesions generally require surgical resection. One major concern of EFTR for these lesions is post-procedural appendicitis. In this study, risk of appendicitis following EFTR of lesions involving appendiceal orifice was 3 %. However, most included studies did not report proportions of patients who had undergone prior appendectomy, thus future prospective studies are needed to assess true risk of appendicitis for those with intact appendix. Currently, clip-assisted EFTR seems to be a potential option for these lesions and should be limited to patients with prior history of appendectomy.
Clip-assisted EFTR has emerged as a technique for the resection of SELs in both the upper and lower gastrointestinal tract, such as neuroendocrine tumors or gastrointestinal stromal tumors. In the subgroup of SELs in this study, a high overall R0 resection rate was also observed (81 % in upper SELs and 100 % in lower SELs), making EFTR an attractive endoscopic alternative to surgery in cases where conventional endoscopic resection seems to be at high risk for severe AEs or unlikely to achieve complete resection. Notably, in the study by Kappelle et al 3 , EFTR using the flat-based OTSC (Padlock clip) in the duodenum was complicated by perforation (n = 1) and micro perforation (n = 3), whereas no AEs were reported in other studies using this clip 10 11 12 13 14 18 . The use of the flat-based OTSC clip-assisted EFTR in the duodenum requires further technical refinements. In addition, only one study 14 reported use of the FTRD device for SELs in the upper gastrointestinal tract, while the remaining studies used the OVESCO/Padlock clip 5 10 18 . Due to the large diameter cap, the current FTRD system is difficult to advance through the upper esophageal sphincter or pyloric ring, increasing the risk of tearing and/or perforation, therefore limiting its use in the upper gastrointestinal tract. Moreover, the available FTRD system has not been approved for EFTR in the upper gastrointestinal tract.
EFTR is a technically demanding procedure despite the favorable risk/benefit ratio, and requires expertise. Advancing the device to the target lesion can be challenging due to friction and decreased visibility due to the long cap. In a small number of patients (n = 9) clip-assisted EFTR was unsuccessful because the device could not be advanced through a narrowed sigmoid colon. The impaired visibility once the lesion is entrapped in the cap can potentially limit complete resection 2 . Tumor size is a major limitation of resection with this technique. To obtain a full-thickness resection specimen and to achieve complete resection, it is critical to include the entire lesion into the cap. The maximum lesion size of a colorectal polyp should not exceed 25 to 30 mm. However, in case of scaring or location in the rectum, incorporation of the entire lesion into the cap is even more difficult. For these reasons, some experts recommend limiting the size of the lesion to 20 to 25 mm 10 .
There are limitations in the current analysis. Most studies were either single-center or retrospective and based on small sample sizes with inherent possibility of selection bias. Second, some information was missing or incomplete from few case series. In addition, there is heterogeneity in the included data. Therefore, this meta-analysis is intended to provide initial data that will aid in performing better design for further analysis. Even though data on clip-assisted EFTR is promising, further prospective, randomized control trials are required to assess long-term efficacy and safety of this technique compared to conventional endoscopic resection techniques and/or surgery.
Conclusion
In conclusion, in this meta-analyses, we found that clip-assisted EFTR is an effective and safe technique for difficult mucosal and submucosal gastrointestinal lesions with high rates of complete resection and acceptable rates of AEs. These findings emphasize the importance of optimizing and standardizing the EFTR technique, to attain widespread implementation of this procedure to remove difficult colorectal adenomas and SELs and sparing the need of surgery.
Footnotes
Competing interests Dr. Kumbhari is a consultant for Boston Scientific, Apollo Endosurgery, Medtronic, and ReShape Medical. Dr. Kalloo is a founding member, equity holder, and consultant for Apollo Endosurgery. Dr. Khashab is a consultant and advisory board for Boston Scientific and consultant for Olympus.
All other authors have no conflicts of interest relevant to the subject of the article.
Note.
Ovesco Endoscopy AG has notified us that the term “OTSC” used in the article is a registered trademark and that “OTSC” is not the generic term for all “over-the-scope clips”. Additionally, the following terms are – according to information from various register databases – registered trademarks: “Apollo Endosurgery”, “Boston Scientific”, “Cochrane”, “Embase”, “FTRD”, “GERDx”, “Olympus Medical Systems”, “Ovesco”, “Padlock Clip”, “Pubmed”, “Reshape Medical”, “Scopus”, “STATA” and “Web of Science”.
Supplementary material :
References
- 1.Hassan C, Repici A, Sharma P. Efficacy and safety of endoscopic resection of large colorectal polyps: a systematic review and meta-analysis. Gut. 2016;65:806–820. doi: 10.1136/gutjnl-2014-308481. [DOI] [PubMed] [Google Scholar]
- 2.Rajan E, Wong Kee Song L M. Endoscopic full thickness resection. Gastroenterology. 2018;154:1925–1937. doi: 10.1053/j.gastro.2018.02.020. [DOI] [PubMed] [Google Scholar]
- 3.Kappelle W FW, Backes Y, Valk G D et al. Endoscopic full-thickness resection of gastric and duodenal subepithelial lesions using a new, flat-based over-the-scope clip. Surg Endosc. 2018;32:2839–2846. doi: 10.1007/s00464-017-5989-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yang F, Wang S, Sun S et al. Factors associated with endoscopic full-thickness resection of gastric submucosal tumors. Surg Endosc. 2015;29:3588–3593. doi: 10.1007/s00464-015-4113-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bauder M, Schmidt A, Caca K. Non-Exposure, Device-Assisted Endoscopic Full-thickness Resection. Gastrointest Endosc Clin N Am. 2016;26:297–312. doi: 10.1016/j.giec.2015.12.008. [DOI] [PubMed] [Google Scholar]
- 6.Weitzendorfer M, Spaun G O, Antoniou S A et al. Interim report of a prospective trial on the clinical efficiency of a new full-thickness endoscopic plication device for patients with GERD: impact of changed suture material. Surg Laparosc Endosc Percutan Tech. 2017;27:163–169. doi: 10.1097/SLE.0000000000000396. [DOI] [PubMed] [Google Scholar]
- 7.Stroup D F, Berlin J A, Morton S C et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA. 2000;283:2008–2012. doi: 10.1001/jama.283.15.2008. [DOI] [PubMed] [Google Scholar]
- 8.Wells G A, Shea B, O’Connell D The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 9.Nyaga V N, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. 2014;72:39. doi: 10.1186/2049-3258-72-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al-Bawardy B, Rajan E, Wong Kee Song L M. Over-the-scope clip-assisted endoscopic full-thickness resection of epithelial and subepithelial gastrointestinal lesions. Gastrointest Endosc. 2017;85:1087–1092. doi: 10.1016/j.gie.2016.08.019. [DOI] [PubMed] [Google Scholar]
- 11.Backes Y, Kappelle W FW, Berk L et al. Colorectal endoscopic full-thickness resection using a novel, flat-base over-the-scope clip: a prospective study. Endoscopy. 2017;49:1092–1097. doi: 10.1055/s-0043-114730. [DOI] [PubMed] [Google Scholar]
- 12.Dinelli M, Omazzi B, Andreozzi P et al. First clinical experiences with a novel endoscopic over-the-scope clip system. Endosc Int Open. 2017;5:E151–E156. doi: 10.1055/s-0043-101692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schmidt A, Beyna T, Schumacher B et al. Colonoscopic full-thickness resection using an over-the-scope device: a prospective multicentre study in various indications. Gut. 2018;67:1280–1289. doi: 10.1136/gutjnl-2016-313677. [DOI] [PubMed] [Google Scholar]
- 14.Valli P V, Mertens J, Bauerfeind P. Safe and successful resection of difficult gastrointestinal lesions using a novel single-step full-thickness resection device (FTRD ® ) . Surg Endosc. 2018;32:289–299. doi: 10.1007/s00464-017-5676-9. [DOI] [PubMed] [Google Scholar]
- 15.van der Spek B, Haasnoot K, Meischl C et al. Endoscopic full-thickness resection in the colorectum: a single-center case series evaluating indication, efficacy and safety. Endosc Int Open. 2018;6:E1227–E1234. doi: 10.1055/a-0672-1138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bauder M, Schmidt A, Caca K. Endoscopic full-thickness resection of duodenal lesions-a retrospective analysis of 20 FTRD cases. United Europ Gastroenterol J. 2018;6:1015–1021. doi: 10.1177/2050640618773517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schmidt A, Bauerfeind P, Gubler C et al. Endoscopic full-thickness resection in the colorectum with a novel over-the-scope device: first experience. Endoscopy. 2015;47:719–725. doi: 10.1055/s-0034-1391781. [DOI] [PubMed] [Google Scholar]
- 18.Sarker S, Gutierrez J P, Council L et al. Over-the-scope clip-assisted method for resection of full-thickness submucosal lesions of the gastrointestinal tract. Endoscopy. 2014;46:758–761. doi: 10.1055/s-0034-1365513. [DOI] [PubMed] [Google Scholar]
- 19.Aepli P, Criblez D, Baumeler S et al. Endoscopic full thickness resection (EFTR) of colorectal neoplasms with the Full Thickness Resection Device (FTRD): Clinical experience from two tertiary referral centers in Switzerland. United Europ Gastroenterol J. 2018;6:463–470. doi: 10.1177/2050640617728001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Andrisani G, Soriani P, Manno M et al. Colo-rectal endoscopic full-thickness resection (EFTR) with the over-the-scope device (FTRD ® ): A multicenter Italian experience . Dig Liver Dis. 2019;51:375–381. doi: 10.1016/j.dld.2018.09.030. [DOI] [PubMed] [Google Scholar]
- 21.Kuellmer A, Mueller J, Caca K et al. Endoscopic full-thickness resection for early colorectal cancer. Gastrointest Endosc. 2019;89:1180–1189. doi: 10.1016/j.gie.2018.12.025. [DOI] [PubMed] [Google Scholar]
- 22.Bronzwaer M ES, Bastiaansen B AJ, Koens L et al. Endoscopic full-thickness resection of polyps involving the appendiceal orifice: a prospective observational case study. Endosc Int Open. 2018;6:E1112–E1119. doi: 10.1055/a-0635-0911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vitali F, Naegel A, Siebler J et al. Endoscopic full-thickness resection with an over-the-scope clip device (FTRD) in the colorectum: results from a university tertiary referral center. Endosc Int Open. 2018;6:E98–E103. doi: 10.1055/s-0043-124079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wang W, Li P, Ji M et al. Comparison of two methods for endoscopic full-thickness resection of gastrointestinal lesions using OTSC. Minim Invasive Ther Allied Technol. 2019;16:1–9. doi: 10.1080/13645706.2019.1602544. [DOI] [PubMed] [Google Scholar]
- 25.Soriani P, Tontini G E, Neumann H et al. Endoscopic full-thickness resection for T1 early rectal cancer: a case series and video report. Endosc Int Open. 2017;5:E1081–E1086. doi: 10.1055/s-0043-118657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mão de-Ferro S S, Castela J, Pereira D et al. Endoscopic full-thickness resection of colorectal lesions with the new FTRD system: single-center experience. GE Port J Gastroenterol. 2019;26:235–224. doi: 10.1159/000493808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Pimentel-Nunes P, Dinis-Ribeiro M, Ponchon T et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:829–854. doi: 10.1055/s-0034-1392882. [DOI] [PubMed] [Google Scholar]
- 28.Stier M W, Chapman C G, Kreitman A et al. Dissection-enabled scaffold-assisted resection (DeSCAR): a novel technique for resection of residual or non-lifting gastrointestinal neoplasia of the colon (with video) Gastrointest Endosc. 2018;87:843–851. doi: 10.1016/j.gie.2017.11.011. [DOI] [PubMed] [Google Scholar]
- 29.Binmoeller K F, Weilert F, Shah J et al. Underwater EMR without submucosal injection for large sessile colorectal polyps (with video) Gastrointest Endosc. 2012;75:1086–1091. doi: 10.1016/j.gie.2011.12.022. [DOI] [PubMed] [Google Scholar]
- 30.Tutticci N J, Hewett D G. Cold EMR of large sessile serrated polyps at colonoscopy (with video) Gastrointest Endosc. 2018;87:837–842. doi: 10.1016/j.gie.2017.11.002. [DOI] [PubMed] [Google Scholar]
- 31.Tate D J, Desomer L, Awadie H et al. EMR of laterally spreading lesions around or involving the appendiceal orifice: technique, risk factors for failure, and outcomes of a tertiary referral cohort (with video) Gastrointest Endosc. 2018;87:1279–1288. doi: 10.1016/j.gie.2017.12.018. [DOI] [PubMed] [Google Scholar]
- 32.Nemoto Y, Tokuhisa J, Shimada N et al. Acute appendicitis following endoscopic mucosal resection of cecal adenoma. World J Gastroenterol. 2015;21:8462–8466. doi: 10.3748/wjg.v21.i27.8462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Imai K, Hotta K, Kakushima N et al. Precutting EMR for cecal tumors extending to the appendiceal orifice. Gastrointest Endosc. 2015;82:750. doi: 10.1016/j.gie.2015.05.007. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.