

Abstract
School‐based breastfeeding education (SBBE) may help improve breastfeeding rates in the long‐term by targeting children and adolescents' knowledge, attitudes, skills, and intentions. Breastfeeding rates in Lebanon are suboptimal. Psychosocial drivers of breastfeeding intention among the youth are unknown. We administered a survey to 658 high school students (448 females; 210 males) at two large Lebanese schools to understand intentions, intention drivers, and views on SBBE as means to guide SBBE programme design on the basis of the theory of planned behaviour. We collected information on demographics, intention to breastfeed/support wife to breastfeed future. Intention was predicted by attitude related to breastfeeding health outcomes and family normative beliefs—χ 2(25) = 115, P < .001 for males, and χ 2(39.3) = 186, P < .001 for females. Among females, intention was also positively associated with being breastfed, higher socio‐economic status, and being more accepting of public breastfeeding. Seventy‐eight per cent of students felt they were not learning enough about breastfeeding in school but were interested in SBBE through didactic teaching methods and interactive experiences. Findings indicate that breastfeeding intention among adolescent students is not merely influenced by the extent of knowledge but by more complicated psychosocial drivers that may differ by gender. Our findings also suggest a misalignment exists between what schools are providing with what students feel they need, thereby opening up a potential space for intervention.
Keywords: adolescents, attitude, breastfeeding, education, schools, theory of planned behaviour
Key Messages.
School‐based breastfeeding education (SBBE) may help improve breastfeeding rates by targeting children and adolescents' knowledge, attitudes, skills, and intentions.
Breastfeeding rates in Lebanon are suboptimal, school‐based breastfeeding education is limited, and data on drivers of intention among adolescents had been lacking.
We found breastfeeding intention to be driven by attitudinal belief related to health and by family normative beliefs in general, and also with being breastfed, higher socio‐economic status, and being more accepting of public breastfeeding in females.
Most students felt they were not learning enough about breastfeeding in school but were interested in SBBE through both didactic teaching methods and interactive experiences and experts.
1. INTRODUCTION
In light of a large body of scientific literature demonstrating the importance of breastfeeding for maternal and infant health (Rollins et al., 2016; Victora et al., 2016), the World Health Organization (WHO) recommends infants be exclusively breastfed for the first 6 months of life, followed with continued breastfeeding until at least 2 years of age (WHO, 2003). The promotion, support, and protection of breastfeeding are crucial for the achievement of the WHO Global Strategy for Women's, Children's and Adolescents' Health (2016–2030) by helping prevent the death of mothers, infants, and children (Kuruvilla et al., 2016). Yet, low breastfeeding rates persist across many developed and developing countries. Efforts to improve the breastfeeding landscape worldwide vary in scope and approach, but they broadly encompass the “top‐down” nation‐level approach to change as well as the “bottom‐up” individual‐ and community‐level approaches. The former focuses on developing data‐driven policy recommendations for high‐level decision makers within a country to facilitate scaling up and sustaining national breastfeeding programmes (Pérez‐Escamilla et al., 2018; Pérez‐Escamilla, Curry, Minhas, Taylor, & Bradley, 2012; Rollins et al., 2016). The latter involves identifying and addressing individual‐level and household‐level barriers against breastfeeding within smaller groups of well‐characterized individuals within a community such as insufficient evidence‐informed knowledge, low self‐efficacy, negative attitudes, and lack of social support (Akik, 2014; Batal, Boulghourjian, Abdallah, & Afifi, 2006; BouDiab & Werle, 2018; Nabulsi, 2011). One of the strategies that holds promise for overcoming these barriers, helping normalize breastfeeding, and thereby increasing breastfeeding initiation, exclusivity, and duration in the long‐term, is school‐based breastfeeding education (SBBE). Intervening early on with children and adolescents may prime them to make informed decisions related to infant feeding as parents in the future and to become positive change agents in their communities even if they do not become parents themselves (Glaser, Roberts, Grosskopf, & Basch, 2016; Singletary, 2018; Singletary, Chetwynd, Goodell, & Fogleman, 2017; Stockley, 2002). Despite being advocated for by the WHO/United Nations Children's Fund (UNICEF) and several other health agencies for more than 15 years now (Li, Benton‐davis, & Grummer‐Strawn, 2015; Royal College of Paediatrics and Child Health, 2017; WHO, 2003), sustained implementation of theory‐driven and evidence‐based SBBE, beyond mere knowledge dissemination, is yet to be achieved in school systems globally.
Given the vast implications of breastfeeding for maternal and infant health and the potential for positive change through SBBE, we have been conducting a series of studies to understand how to sustainably and effectively implement SBBE in Lebanon (Moukarzel, Mamas, Farhat, & Daly, 2019). Lebanon reflects an important context as it is one of many middle‐high income, under‐researched, and underserved nations, with approximately 40% of infants exclusively breastfed at 1 month postpartum and 2% at 6 months (Central Administration of Statistics & UNICEF, 2009).
Individual‐level barriers to breastfeeding include negative beliefs, insufficient knowledge, and misconceptions among adult mothers, their family members, and physicians (Akik, Ghattas, Filteau, & Knai, 2017; Moukarzel et al., 2018; Nabulsi, 2011; Osman, El Zein, & Wick, 2009). Among the youth, several studies, mainly in developed countries, have reported that students at various ages may have insufficient knowledge about infant feeding recommendations and may hold negative attitudes about breastfeeding (Glaser et al., 2016; Singletary et al., 2017). There are no data currently available on Lebanese children and adolescents during their Pre‐K‐12 education: from first grade at around 5 years of age to 12th grade at around 17 years of age. Limited SBBE is taking place in Lebanon as it is only mandatory to briefly teach the students about the infant and maternal benefits of breastfeeding in fifth grade and about breastfeeding duration recommendations and breastfeeding barriers in 10th grade (Moukarzel et al., 2019). There is also no focus on leveraging SBBE to change psychosocial constraints such as negative attitudes, which have been shown to be consequential on intent to breastfeed (Giles et al., 2015).
Before designing any SBBE curriculum, which could differ by school and region, it is important to first understand students' attitudes on breastfeeding and to identify the knowledge and psychosocial areas, if any, on which SBBE may focus. To address this aforementioned gap in the literature, the theory of planned behaviour (TPB) may be used as a guiding theoretical framework (Ajzen, 1985; Ajzen & Fishbein, 1980). TPB is one of the most commonly used psychosocial frameworks in designing health education interventions and more recently in designing one SBBE intervention in Ireland (Giles et al., 2015). According to the theory, intention is an important predictor of future behaviour and is influenced by three main direct constructs: attitude, subjective norm, and perceived control (Ajzen, 1985; Ajzen & Fishbein, 1980). Therefore, the goal of our study is to better understand the intention to breastfeed in the future (for females) and to support partner to breastfeed (for males) among adolescent Lebanese students as well as to explore the underlying demographic, psychosocial, and other factors that might influence their intention.
2. METHODS
2.1. Setting and study population
This study was conducted among high school students, in Grades 10 to 12, during the 2018–2019 academic year at two private schools in the governorate (province) of Mount Lebanon for which SBBE views of ~200 teachers have been recently reported (Moukarzel et al., 2019). Rates of adult literacy and school enrollment by gender and by school type (private/public) have been reported (Moukarzel et al., 2019). Teachers held generally positive views on SBBE and proposed we suggest the importance of and provide support to local teachers to deliver SBBE to male and female high school students in their schools. We chose these two large typical schools as our recruitment sites because they offer Pre‐K to Grade 12 classes for more than 7,000 economically diverse and predominantly Lebanese students who typically stay at the same school from Pre‐K classes until completion of Grade 12. This provides us with the unique opportunity to follow, intervene, and/or study the short‐ and long‐term impact of SBBE in almost the same cohort of students across the years. Additionally, most Lebanese private schools serve students from low, middle, and high‐income families, unlike in many countries where private schools are only affordable to high‐income families. Therefore, it is likely that students in Lebanese private schools more closely represent the population compared with public schools that predominantly serve students with lower socio‐economic status (SES). The most recently available data from 2014 show 103,660 students were enrolled in Pre‐K‐12 schools in Mount Lebanon, of which 74% were enrolled in private schools (Moukarzel et al., 2019).
The principal of one school (School A) agreed to participate in the study with both male and female students. However, the second (School B), although agreeing, restricted our protocol to female students only despite several attempts from our research team indicating the research significance of including students from both genders. The principal of School B held firm on his decision offering the rational that, “High school‐level male students are not mature enough to address the sensitive topic of breastfeeding in a serious way.”
Participant recruitment took place at the schools in collaboration with division principals by first explaining the study to the students and then distributing consent forms to be shared with parents or legal guardians. Those who returned signed consent forms within a week were enrolled. Six hundred fifty‐eight students (65.4%) completed the study out of the 1,006 high school eligible students: 210 out of the 658 students were males from School A (31.9%), 253 were females from School A (38.5%), and 195 were females from School B (29.6%; Table S1).
2.2. The survey
Largely grounded in previous work, which used TPB as framework to better understand adolescent breastfeeding intentions in Ireland (Giles et al., 2007; Giles et al., 2014; Giles et al., 2015; Giles, Connor, McClenahan, & Mallet, 2010), the survey included five sections that assessed demographic characteristics, intention to breastfeed/support wife to breastfeed, TPB direct and indirect constructs, basic knowledge related to breastfeeding, views on breastfeeding in public, and views on breastfeeding education. Two versions of the survey were available such that the male's version rotated around “supporting wife to breastfeed in the future” rather than “breastfeeding in the future.” The term “wife” was chosen as it is the most culturally responsive term to describe a male's significant other within the Lebanese context. The instrument was self‐administered and research staff were available to clarify questions when needed. The survey was completed by hand either in English or in French, and its legibility and comprehension were informally pilot tested with a purposeful sample of n = 40 students (a group of 10 males and 10 females to pilot test the English version and another group of 10 males and 10 females to pilot test the French version) reflecting the intended study population.
Background information included age, number of siblings, rank among siblings, school grade, number of academic years in current school, age, and perceived SES. The latter was assessed using the MacArthur scale of subjective social status, known to strongly correlate with traditional indicators of SES such as measures of education, family income, and wealth (Adler & Stewart, 2007); Students were presented with a picture of a 10‐rung ladder and were asked to place an “x” on one of the rungs as a ranking to one's socio‐economic position relative to others in Lebanon. Given the scarcity of data in this space, we chose the MacArthur scale as it might be a more culturally responsive way of collecting data on SES among Lebanese adolescents compared with more traditional methods. General students' views on breastfeeding education were also collected (Table S2).
The following sections are duplicated from the peer‐reviewed instrument by Giles et al. (2007) with minor changes in sentence wording, noted in their appropriate sections, to improve comprehension based on student feedback in the Lebanese context. Although previous exposure to breastfeeding and knowledge are not constructs of TPB per se, they may be important predictors of intention (Giles et al., 2007). Therefore, previous exposure to breastfeeding was assessed by asking “Have you been breastfed as a child? (yes/no/I don't know)” and “have you ever seen a mother breastfeeding her baby? (yes/no).” Breastfeeding‐related knowledge was assessed by asking students to label 14 statements as True or False (Table S6). The number of correctly labeled statements were reported as knowledge scores.
Direct measures of TPB constructs were assessed as summarized in Table S3. Indirect measures of attitude, subjective norm, and perceived control were also assessed and sample questions are listed in Table S4. Attitude largely refers to the degree to which a student has a positive or negative evaluation of breastfeeding/breastfeeding support and its consequences. Subjective norm refers to the belief about whether individuals who are important to the student would approve of them engaging in breastfeeding/breastfeeding support. Finally, perceived control refers to the student's belief in the ease or difficulty in breastfeeding/supporting breastfeeding. Each of the three direct constructs are influenced by a set of underlying beliefs, referred to as indirect TPB constructs that include attitudinal beliefs, normative beliefs, and control beliefs. Briefly, to calculate indirect measures of attitude, students were first asked to rate how bad/good they considered twelve factors, including bonding with one's baby, providing health benefits to one's baby, and using a convenient method of infant feeding (Table S5). Then, students were asked to rate how likely these factors would occur with breastfeeding. For each factor, the good/bad score was multiplied by its likeliness of occurrence score to give an attitudinal belief score, ranging between −21 and 21 (example is provided in Table S4). For the indirect measure of subjective norm, students were asked to rate how likely they thought their mothers, family, husband/wife, close friends, and health professionals would each want them to breastfeed. Then, they were asked to rate how much they wanted to follow what these groups of individuals expected. A normative belief score, ranging between −21 and 21, for each of the five individual groups was calculated. Due to the complexity of comprehending a similar rating approach for indirect measures of perceived control, we based the indirect measures of control on single items consistent with others (Giles et al., 2007; Giles et al., 2010; Giles et al., 2014; Giles et al., 2015). Accordingly, students were asked to rate how much nine factors, including support of others, having more knowledge about infant feeding, and tolerance of others to public breastfeeding (Table S5), would make it easier or more difficult for them to breastfeed/support wife to breastfeed on a 7‐point scale where 1 corresponds to more difficult and 7 to much easier. Finally, to assess acceptance of public breastfeeding, participants were provided with four statements, for which they were asked to rate their level of agreement (strongly disagree/disagree/agree/strongly agree).
Exploratory factor analysis with principal component extraction was conducted to assess the reliability of the scales for attitudinal belief, control belief, and public breastfeeding acceptance. Kaiser–Meyer–Olkin test indicated items for all three scales could be factorable (Kaiser–Meyer–Olkin = 0.713, 0.734, 0.701, respectively, P < .001), and the Bartlett's test of sphericity was significant for all (P < .001). The attitudinal belief scale factored into two components: (a) health‐related attitudinal beliefs consisting of the five factors numbered 1, 2, 3, 4, and 7 in Table S5 and (b) social impact‐related attitudinal beliefs consisting of the three factors numbered 9, 10, and 12 (Cronbach's alpha = .674). The control belief scale and public breastfeeding acceptance scale each factored into one component. The control belief scale had a Cronbach's alpha value equivalent to .690 and consisted of individual variables (factors) numbered 4, 5, 6, and 8. The public breastfeeding acceptance scale had a Cronbach's alpha equivalent to .620 and consisted of factors numbered 2 and 3. Accordingly, mean scores of each subscale were calculated and reported instead of mean scores for individual factors.
2.3. Statistical methods
Kolmogorov–Smirnov test was used to test distributions of continuous variables that were found to be skewed except for age. Descriptive statistics for continuous variables are expressed as mean ± SD or median (interquartile range; range) as appropriate and for categorical variables as frequency (%). Multinomial and multivariate logistic regression modelling was performed for male and female students to predict the relationship between level of intent to breastfeed/support wife to breastfeed (dependent variable with 1 = extremely likely and 6 = extremely likely as reference) and student characteristics, including background characteristics, knowledge scores, previous exposure to breastfeeding, and mean scores of the various TPB constructs. spss software (Version 25 for Mac OS X) was used, and the level of statistical significance was set at P < .05. Responses to the open‐ended survey question were coded on MAXQDA 2018 (VERBI Software, 2017) and analyzed through thematic analysis starting with open coding (Bryman, 2016). Responses were reviewed independently by two researchers who first identified themes separately then revised the themes together to reach consensus.
2.4. Ethics statement
Ethics approval was obtained from the Institutional Review Board at Notre Dame University.
3. RESULTS
3.1. Description of study participants
Participants were 14–19 years old, and the majority had at least one sibling (Table 1). More males than females were the youngest sibling in the family, with no difference in median number of siblings between gender groups. Median score on the MacArthur scale of subjective social status was 6 (interquartile range = 2; range = 1–10) for both genders. Around 60% of students have been enrolled in their current school since preschool. Although more males reported not knowing if they were ever breastfed, more females reported that they had been breastfed and that they have seen a mother breastfeed before. No significant differences in descriptive variables were found among females between the two schools.
Table 1.
Student characteristics
| Background information | Male student, n = 210 | Female student, n = 448 | P value |
|---|---|---|---|
| Age, yearsa | 16 ± 1.0 | 16 ± 0.9 | .367 |
| Have at least one sibling, n (%) | 195 (92.8) | 418 (93.2) | .84 |
| Number of siblingsb | 2 (1; 0–9) | 2 (1; 0–9) | .407 |
| Eldest sibling, n (%) | 65 (33.3) | 163 (39.0) | .195 |
| Youngest sibling, n (%) | 112 (57.4) | 197 (47.1) | .039 |
| Enrolled since preschool, n (%) | 124 (59.0) | 267 (59.6) | .127 |
| Number of years in current school | 13 (5; 1–15) | 13 (6; 1–15) | .309 |
| Score on socio‐economic status scaleb , c | 6 (2; 1–10) | 6 (2; 1–10) | .256 |
| Breastfed, n (%) | |||
| Yes | 156 (74.3) | 368 (82.1) | .021 |
| No | 18 (8.7) | 37 (8.26) | |
| I don't know | 36 (17.1) | 43 (9.60) | |
| Ever seen a mother breastfeed, n (%) | 178 (84.7) | 426 (95.1) | <.001 |
Note. P values determined using chi‐square test for categorical variables and Mann–Whitney U test for continuous variables except for age, which was normally distributed and analysed by independent student t test.
Values are mean ± SD.
Values are median (interquartile range; range).
Score on the 10‐point MacArthur scale of subjective social status with higher score indicating higher perceived status.
3.2. Intention to breastfeed/support wife to breastfeed and contributing factors
Intent to breastfeed/support wife to breastfeed was skewed towards the three likely levels, as shown in Figure 1, with no significant difference in the distribution of intent levels by gender (P = .077), by school for females (P = .181), or by school grade (P = .08). We first sought to broadly examine the relationship between breastfeeding intention and direct measures of TPB: attitude, subjective norm, and perceived control. Intention was significantly associated with the direct measure of attitude in males and females (Table 2). Indeed, 73.1% of males and 81.3% of females who are likely to breastfeed/support wife to breastfeed reported breastfeeding would be a pleasant experience compared with 60.1% of males and 40% of females who are unlikely to do so. Attitude itself was also associated with subjective norm (i.e., with how much others approve of participant breastfeeding/supporting breastfeeding) and with perceived control (how strongly the participant feels the decision to breastfeed/support breastfeeding is up to them). Therefore, there seems to be a wide array of underlying beliefs influencing intention beyond direct attitudinal beliefs alone, possibly extending to normative and control beliefs.
Figure 1.
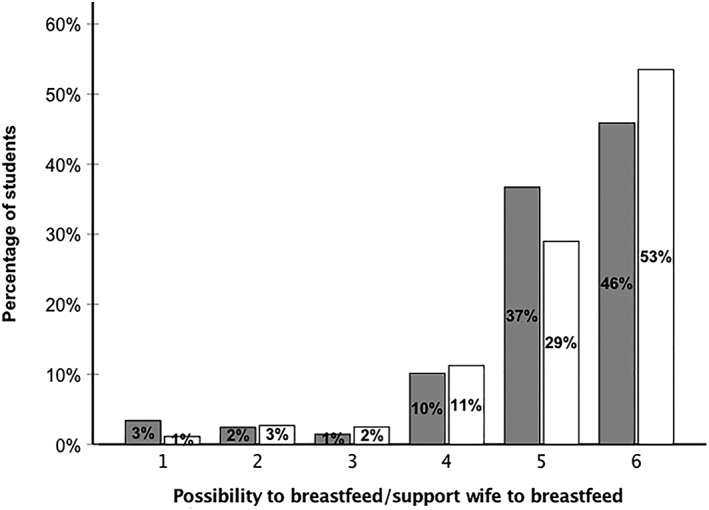
Intention to breastfeed/support wife to breastfeed among high school students. Six levels of intention indicate: 1 = extremely unlikely, 2 = quite unlikely, 3 = slightly unlikely, 4 = slightly likely, 5 = quite likely, 6 = extremely likely. Gray indicates males, and white indicates females
Table 2.
Magnitude of correlations between intention to breastfeed/support wife to breastfeed and the direct measures of theory of planned behaviour constructs
| Constructs | Attitude | Subjective norm | Perceived control |
|---|---|---|---|
| Males, n = 210 | |||
| Intention | .27 (.048) | .17 (<.588) | .12 (.616) |
| Moderate | None | None | |
| Attitude | — | .33 (<.001) | .23 (<.017) |
| Moderate | Moderate | ||
| Subjective norm | — | — | .22 (.089) |
| None | |||
| Females, n = 440 | |||
| Intention | .25 (<.001) | .15 (.127) | .12 (.436) |
| Moderate | None | None | |
| Attitude | — | .28 (<.001) | .16 (<.014) |
| Moderate | Weak | ||
| Subjective norm | — | — | .16 (<.014) |
| Weak | |||
Note. Values are Cramer's V (P value for chi‐square test). Magnitude of correlations were determined based on Rea and Parker (1992).
We therefore explored the underlying indirect TPB belief constructs that might shape intention, along with the potential roles of knowledge and acceptance of public breastfeeding. As reflected by their scores (Table S6), females had significantly stronger beliefs related to the importance of breastfeeding for maternal and infant health, and they seemed to have more evidence‐informed knowledge about breastfeeding compared with males. Males, however, were more likely than females to believe that feeling tired, embarrassed, or feeling physically ill themselves would hinder their willingness to support breastfeeding. The students' social ecosystem that includes, in decreasing order of influence, their health professionals, mothers, family, and close friends, seem to be more influential on female's intention than males'.
To ascertain the collective effects of TPB constructs and other characteristics on breastfeeding intention, we performed multinomial logistic regression with intention to breastfeed/support wife to breastfeed as dependent variable (1 = extremely unlikely to 6 = extremely likely as reference). After removing statistically insignificant characteristics and recoding scores on the SES scale into two variables (score ≤5 or >5), the logistic regression models whose predictors are presented in Table 3 were statistically significant—χ 2(25) = 115, P < .001 for males, and χ 2(39.3) = 186, P < .001 for females. The models explained 51.4% (Nagelkerke R 2) of the variance, correctly predicting 65% of male cases and explained 39.3% of the variance for females, correctly predicting 59% of cases. Goodness of fit was explored using Pearson and deviance tests, which did not result in statistically significant results.
Table 3.
Predictors' unique contributions in multinomial logistic regression models
| Predictor | χ 2 | df | P value |
|---|---|---|---|
| Males, n = 194 | |||
| Attitudinal belief score related to health effectsa | 36.8 | 5 | <.002 |
| Attitudinal belief score related to social effectsb | 21.4 | 5 | .002 |
| Normative belief score related to familyc | 30.1 | 5 | <.001 |
| Normative belief score related to wifec | 18.0 | 5 | .003 |
| Ever seen a mother breastfeed (yes, no) | 29.9 | 5 | <.001 |
| Females, n = 431 | |||
| Attitudinal belief score related to health effects | 34.2 | 5 | <.001 |
| Attitudinal belief score related to social effects | 13.9 | 5 | .016 |
| Normative belief score related to family | 61.3 | 5 | <.001 |
| Breastfeeding acceptance scored | 13.8 | 5 | .017 |
| Breastfed as an infant (yes; no; I don't know) | 20.8 | 10 | .023 |
| Score on socio‐economic status scale (≤5; >5) | 11.3 | 5 | .045 |
Note. χ 2 is the amount by which −2 log likelihood increases when predictor is removed from the full model.
Abbreviation: df, degrees of freedom.
Composite score, ranging between −21 and 21, based on attitudinal beliefs that breastfeeding (BF) is convenient, is a natural method of feeding and results in bonding with one's baby, providing health benefits to infant, and regaining women's pre‐pregnancy weight.
Composite score, ranging between −21 and 21, on the basis of attitudinal beliefs that BF results in feeling embarrassed, in limited social activity and that BF is an uncomfortable and painful method of infant feeding.
Score ranging between −21 and 21 on extent of influence of family or wife on participant's decision to breastfeed.
Composite score ranging between 1 and 4, assessing belief that BF is not socially acceptable and that student would be offended by the sight of a woman BF.
Significant predictors of intention were found predominantly across the likely intention groups (Table 4). In males, the odds of being in the extremely likely group rather than the slightly likely and quite likely groups increased significantly with increasing health‐related attitudinal belief score as well as in the family normative belief score. In females, not only did the health‐related attitude score and family normative belief score predict intention but so did several other factors highly related to the personal and social context in which participants live. Being breastfed as an infant, perceiving higher SES, and being more accepting of public breastfeeding significantly increased odds of being in the extremely likely group compared with most other groups. Collectively, these findings show that intention to breastfeed/support wife to breastfeed among high school students is not only influenced by health‐related knowledge but also driven by much more complicated psychosocial drivers for which the extent of influence on intention might be influenced by gender.
Table 4.
Summary of significant parameter estimates contrasting the extremely likely group versus other intention groups
| Predictor | Extremely likely vs. | B | OR | 95% CI | P value |
|---|---|---|---|---|---|
| Males, n = 194 | |||||
| Attitudinal belief score related to health effects | Slightly likely | −0.22 | 0.80 | 0.69, 0.93 | .004 |
| Quite likely | −0.14 | 0.87 | 0.79, 0.95 | .003 | |
| Normative belief score related to family | Slightly likely | −0.22 | 0.80 | 0.71, 0.90 | <.001 |
| Normative belief score related to wife | Quite likely | −0.06 | 0.94 | 0.90, 0.98 | .014 |
| Females, n = 431 | |||||
| Attitudinal belief score related to health effects | Slightly unlikely | −0.44 | 0.65 | 0.52, 0.80 | <.001 |
| Slightly likely | −0.21 | 0.81 | 0.73, 0.90 | <.001 | |
| Attitudinal belief score related to social effects | Slightly unlikely | −0.29 | 0.75 | 0.62, 0.90 | .003 |
| Normative belief score related to family | Quite unlikely | −0.13 | 0.88 | 0.80, 0.96 | .007 |
| Slightly likely | −0.17 | 0.84 | 0.79, 0.89 | <.001 | |
| Quite likely | −0.06 | 0.95 | 0.92, 0.97 | <.001 | |
| Breastfeeding acceptance score | Quite likely | −0.54 | 0.58 | 0.39, 0.87 | .009 |
| Has been breastfed as an infant | Slightly unlikely | −3.27 | 0.04 | 0.01, 0.28 | .002 |
| Score on socio‐economic status scale as ≤5 | Extremely unlikely | 1.59 | 13.3 | 1.18, 1.49 | .037 |
Note. Six intent categories are 1 = extremely unlikely, 2 = quite unlikely, 3 = slightly unlikely, 4 = slightly likely, 5 = quite likely, and 6 = extremely likely as reference.
Abbreviations: CI, confidence interval; OR, odds ratio.
3.3. Potential for change through SBBE: Students' views on breastfeeding education
Beyond the analysis on intention drivers, we also present descriptive analysis of responses to opportunities to learn about breastfeeding as well as qualitative data we gathered on what schools can do to assist in learning more about breastfeeding. Most students felt they were not learning enough about breastfeeding in school (71.1% of males and 81.7% of females) and that they needed to learn more before having a child (74.3% of males and 88.3% of females). Indeed, 96% of both genders reported not being formally introduced to the topic in class. In decreasing order of frequency, students reported that they can ask questions about breastfeeding from their parents (74.3 % of males and 88.3% of females), classmates (48.1% of males and 42.3% of females), and teachers (41% of males and 38% of females). To complement these quantitative findings, we thematically analyzed student responses (n = 476, 72% answered) to the open‐ended question “What can your school do to help you learn more about breastfeeding.”
Two common themes were identified with no differences indicated by gender. First, students predominantly suggested the school organize breastfeeding‐focused workshops, conferences, and talks with health professionals, citing physicians, nurses, and researchers as examples. Second, students suggested incorporating breastfeeding education in biology classes and provided suggestions for broad teaching methods as “powerpoint presentations,” “lectures,” “showing a documentary in class,” and “school projects.” Therefore, both male and female students seem to be interested to learn about breastfeeding in school, not only through didactic teaching methods but also through interactive experiences and experts. Taken together, these data suggest a misalignment between what schools are providing and what students feel they need in this area and as such opens up a potential space for intervention.
4. DISCUSSION
In this study, we found generally positive intentions towards breastfeeding/supporting partner to breastfeed and that intention was not largely influenced by the extent of evidence‐informed knowledge per se. Instead, intention was mainly driven by an array of psychosocial beliefs and attitudes that shaped what adolescents perceive as important and socially acceptable in this period of their development. We also found that students were interested in participating in SBBE that extends beyond knowledge dissemination to include building interactive experiences within the school and out with the health professional community.
Positive intention was common in our cohort, with almost all students reporting to likely breastfeed/support partner to breastfeed in the future. This aligns with results from a smaller study in Lebanon where ~89% (n = 194 total) of 18‐ to 25‐year‐old undergraduate females without children reported they “were planning to at least give breastfeeding a try” (Hamade et al., 2014). Consistent with these findings, breastfeeding initiation rate in Lebanon is high (~92%); however, breastfeeding is mostly nonexclusive with no more than 40% of women exclusively breastfeeding at 1 month postpartum and 2% at 6 months (Central Administration of Statistics /UNICEF, 2009). To put this into perspective, this is dramatically lower than 30%, the estimated average rate of exclusive breastfeeding at 6 months for infants in other upper‐middle‐income countries around the world (Victora et al., 2016). Although positive effects on large‐scale policy aimed at improving breastfeeding rates in Lebanon have been limited thus far (Akik et al., 2017), we have an opportunity to influence individual‐level beliefs, which in turn can change public opinion and ultimately policy.
Similar to findings in several countries around the world (Singletary et al., 2017), we are the first to show in Lebanon that intention among adolescents is significantly associated with attitude towards breastfeeding. In both males and females, intention was stronger when positive beliefs about the beneficial health outcomes of breastfeeding were stronger. In females, intention was also negatively associated with beliefs that breastfeeding is socially restrictive, embarrassing, uncomfortable, and painful. In general terms, attitude is the product of both “knowing” and “believing in the significance of a topic” (Ajzen & Fishbein, 1980). For example, attitude towards breastfeeding is not only related to knowing about health outcomes (e.g., reduced risk of infant infections) but also to believing that the reduction in infections is important. Accordingly, and given the wide variability in knowledge assessment scores found particularly among males, our findings suggest that improving knowledge, such as through SBBE, might be a necessary but not sufficient condition to reinforce intention among adolescents. SBBE is likely to be more effective on influencing breastfeeding practices in the long‐term if it is tailored towards improving knowledge as well as psychosocial drivers. This suggests that developers and implementers of SBBE programmes must intentionally package both aptitude and attitude in a comprehensive approach.
In addition to attitudinal beliefs, and similar to other studies (Singletary et al., 2017), we found students' families to be influential on their intentions. Adolescents are more likely to support breastfeeding if they believed their families would approve. This suggests that SBBE in schools in contexts such as Lebanon, which is more family oriented, must also consider the larger familiar and social system in which students are embedded. School programmes alone without strong linkages to the family may be less impactful on change in attitudes. Research with pregnant and lactating Lebanese women has demonstrated the importance of social norms in shaping breastfeeding behaviour (BouDiab & Werle, 2018; Nabulsi, 2011; Osman et al., 2009). Family members, especially women's mothers and husbands, have been reported to discourage women to breastfeed, to spread misconceptions around breastfeeding, and to pressure women to introduce infant formula (BouDiab & Werle, 2018; Nabulsi, 2011; Osman et al., 2009). We add to this body of literature that family influence is a powerful driver of breastfeeding/breastfeeding support intention in Lebanon beginning much earlier on in life, starting at least during adolescence. To break the cycle of negative social influence on breastfeeding handed down from generation to generation as we concurrently prime the future generation of adults to normalize breastfeeding, it seems that effective SBBE programme within the Lebanese context should include community‐based learning (Bouillion & Gomez, 2001).
Community‐based learning holds the potential to bridge the practices and culture of a school with the culture of a students' home and community. School‐based health education programmes, including nutrition interventions, with links to the larger community, have been shown to enhance learning (Lewallen, Hunt, Potts‐Datema, Zaza, & Giles, 2015; Roseman, Riddell, & Haynes, 2011). We offer a few examples of community‐based learning approaches that might expand positive impact to student's communities including (a) making instructional connections, such as discussing local breastfeeding‐related research findings in class, (b) integrating the community such as inviting local health experts to give presentations and inviting parents to participate in panel discussions, and (c) participating in the community such as having students contribute to breastfeeding awareness campaigns in collaboration with local nonprofit organizations and other schools. To improve knowledge but also attitudes, we suggest the topic of breastfeeding be also discussed as part of larger discussions around social justice and equity, social norms, and empowerment of youth for social change.
Independent of choice for learning approach(es), designing an effective SBBE programme in male‐dominant settings like Lebanon comes with an added layer of complexity. First, on the basis of our research field experience, approval of Pre‐K‐12 schools to access their male student populations is not a given. Despite many educators being supportive of teaching both male and female high school students about breastfeeding in School B (Moukarzel et al., 2019), the school principal did not allow our research team to even explore male students' views on breastfeeding for this study. In accordance with the persisting cultural view that breastfeeding is a women‐only issue (Moukarzel et al., 2019), the principal considered the topic too sensitive to be discussed with male students. This is intriguing because School B, similar to School A, serves students of both genders and is located in an urban city. We could not find a similar incident published in either the Lebanese or the international literature. Second, our findings suggest that being breastfed as an infant, perceiving one self as having low SES, and being accepting of public breastfeeding without feeling offended are all important predictors of positive breastfeeding intention, at least among females. In males, these do not seem to matter based on our models. If this is indeed true, without being a consequence of the smaller sample size of males compared with females in this study, then learning objectives for an effective SBBE programme may be even more tailored to student gender. For example, an SBBE programme for females, but not necessarily for males, might include an attitude‐changing objective to decrease the feeling of being offended by the sight of a woman breastfeeding in public. Indeed, in Giles et al. (2014), a short‐term TPB‐based intervention (60‐ to 80‐min classroom session) designed to promote positive attitudes towards breastfeeding was effective with female but not male students. The authors speculated that it is possible that the intervention did not sufficiently target the underlying intention drivers most important and relevant to males. Although the intervention included discussions on the naturalness of breastfeeding, the importance of the family network in supporting breastfeeding, and health effects of breastfeeding on mother and infant (Giles et al., 2010), it is possible male students' intentions were influenced by other factors (e.g., impact on their social life), which were not identified and therefore not addressed in the intervention. Future studies need to address gender differences in intention drivers among Lebanese adolescents to enable the development of interventions that more specifically target the needs of both genders.
Finally, we measured intention and its drivers cross‐sectionally and broadly (likelihood to breastfeed/support partner to breastfeed in the future) without including breastfeeding‐specific nuances such as intention related to breastfeeding exclusivity and duration. We had speculated based on other work (Singletary et al., 2017) that students in our cohort will not have the adequate background knowledge to even reflect on their own intentions related to exclusivity and duration. Our research would benefit from a deeper and also longitudinal exploration of intention and its drivers as attitudes and beliefs may shift over time. As adolescents transition into adulthood and eventually into parenthood, experiences within and around them might (e.g., related to career development and new social relationships) change intentions they previously held. In addition, future work could explore the “ideal” time to introduce and reintroduce SBBE in the trajectory of a student's life in schools.
This study contributes to the emerging body of literature identifying determinants of effective SBBE as means to improve breastfeeding rates globally. This study is the first to explore breastfeeding intention and its drivers among Lebanese adolescents and is grounded in a well‐studied theory (Ajzen, 1985). However, results should be interpreted bearing in mind the following study limitations. The TPB constructs were measured by asking about potential factors influencing intention, such as the significance of bonding with one's baby and extent of influence from one's mother, which were previously identified among adolescents in Ireland (Giles et al., 2010). Due to cultural differences, it is possible Lebanese adolescents have additional influencing factors that have not yet been explored. A future study eliciting new factors might prove helpful in developing more rigorous statistical models and importantly, comprehensive SBBE programmes. Additionally, although recruiting students at urban private schools provided us with access to an economically diverse sample, results might not reflect the perspectives of students from public schools, especially those in rural areas that serve families with lower SES. Our goal is to build partnerships with public school principals and to raise research funds that are necessary for a more comprehensive understanding of this student population.
To conclude, our findings indicate breastfeeding intention among adolescent students is not merely influenced by extent of knowledge but by more complicated psychosocial drivers that may differ by gender. Our findings also suggest a misalignment exists between what schools are providing in terms of breastfeeding education with what students feel they need to effectively learn about breastfeeding, thereby opening up a potential space for intervention. SBBE could be viewed as one opportunity to provide the youth with a strong and resilient foundation to counteract barriers of breastfeeding in the future. By equipping youth with adequate evidence‐informed knowledge and instilling in them and their families positive attitudes towards breastfeeding, perhaps we can better leverage the tremendous benefits afforded by breastfeeding.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
SM, AF, and AJD designed the study. SM, MAJ, and MS performed the research. SM and CM analyzed the data. SM and AJD wrote the first draft of the manuscript. All authors have read and approved the final manuscript.
Supporting information
Table S1. Number of participants completing the study by school and grade
Table S2. List of questions to assess general students' views on breastfeeding education
Table S3. Direct measures of TPB constructs
Table S4. Sample questions used to determine indirect measures of attitude, subjective norm and perceived control.
Table S5. List of factors used to assess attitudinal beliefs, control beliefs, and acceptance of public breastfeeding
Table S6. Summary of indirect measure scores for student beliefs (attitudinal, normative and control), acceptance of public breastfeeding and knowledge
ACKNOWLEDGMENTS
We thank graduate research assistants Priscilla Bedran, Marytha Ibrahim, and Lea Majdalani for their help with recruitment and data collection. We gratefully acknowledge the support of the Family Larsson‐Rosenquist Foundation.
Moukarzel S, Abou Jaoudeh M, Farhat A, Saade M, Mamas C, Daly AJ. Exploring the latitude of attitude: Intentions to breastfeed among adolescents in Lebanese schools. Matern Child Nutr. 2020;16:e12888 10.1111/mcn.12888
REFERENCES
- Adler, N. , & Stewart, J. (2007). The MacArthur scale of subjective social status. Retrieved from https://macses.ucsf.edu/research/psychosocial/subjective.php.
- Ajzen, I. (1985). From intentions to action: A theory of planned behavior In Kuhl J., & Beckman J. (Eds.), Action control: From cognition to behavior (pp. 11–39). New York, NY: Springer. [Google Scholar]
- Ajzen, I. , & Fishbein, M. (1980). Understanding attitudes and predicting behavior. Englewood Cliffs, NJ: Prentice‐Hall. [Google Scholar]
- Akik, C. (2014). Breastfeeding in Lebanon: Barriers and policy dynamics. (DrPH thesis), London School of Hygiene & Tropical Medicine DOI: uk.bl.ethos.631575,
- Akik, C. , Ghattas, H. , Filteau, S. , & Knai, C. (2017). Barriers to breastfeeding in Lebanon: A policy analysis. Journal of Public Health Policy, 38(3), 314–326. [DOI] [PubMed] [Google Scholar]
- Batal, M. , Boulghourjian, C. , Abdallah, A. , & Afifi, R. (2006). Breast‐feeding and feeding practices of infants in a developing country: A national survey in Lebanon. Public Health Nutrition, 9(3), 313–319. [DOI] [PubMed] [Google Scholar]
- BouDiab, S. , & Werle, C. (2018). What motivates women to breastfeed in Lebanon: An exploratory qualitative analysis. Appetite, 123, 23–31. [DOI] [PubMed] [Google Scholar]
- Bouillion, L. M. , & Gomez, L. M. (2001). Connecting school and community with science learning: Real world problems and school‐community partnerships as contextual scaffolds. Journal of Reseach in Science Teaching, 38(8), 878–898. [Google Scholar]
- Bryman, A. (2016). Social research methods (5th ed.). London: Oxford University Press. [Google Scholar]
- Central Administration of Statistics, & United Nations Children's Fund . Mulitple indicator cluster survey‐ Lebanon 2009. ‐2010.
- Giles, M. , Connor, S. , McClenahan, C. , & Mallet, J. (2010). Attitudes to breastfeeding among adolescents. Journal of Human Nutrition and Dietetics, 23(3), 285–293. [DOI] [PubMed] [Google Scholar]
- Giles, M. , Connor, S. , McClenahan, C. , Mallett, J. , Stewart‐Knox, B. , & Wright, M. (2007). Measuring young people's attitudes to breastfeeding using the theory of planned behaviour. Journal of Public Health Policy, 29(1), 17–26. [DOI] [PubMed] [Google Scholar]
- Giles, M. , McClenahan, C. , Armour, C. , Millar, S. , Rae, G. , Mallett, J. , & Stewart‐Knox, B. (2014). Evaluation of a theory of planned behaviour‐based breastfeeding intervention in Northern Irish schools using a randomized cluster design. British Journal of Health Psychology, 19(1), 16–35. [DOI] [PubMed] [Google Scholar]
- Giles, M. , Millar, S. , Armour, C. , McClenahan, C. , Mallett, J. , & Stewart‐Knox, B. (2015). Promoting positive attitudes to breastfeeding: The development and evaluation of a theory‐based intervention with school children involving a cluster randomised controlled trial. Maternal & Child Nutrition, 11(4), 656–672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glaser, D. B. , Roberts, K. J. , Grosskopf, N. A. , & Basch, C. H. (2016). An evaluation of the effectiveness of school‐based breastfeeding education. Journal of Human Lactation, 32(31), 46–52. [DOI] [PubMed] [Google Scholar]
- Hamade, H. , Naja, F. , Keyrouz, S. , Hwalla, N. , Karam, J. , Al‐Rustom, L. , & Nasreddine, L. (2014). Breastfeeding knowledge, attitude, perceived behavior, and intention among female undergraduate university students in the Middle East: The case of Lebanon and Syria. Food and Nutrition Bulletin, 35(2), 179–190. [DOI] [PubMed] [Google Scholar]
- Kuruvilla, S. , Bustreo, F. , Kuo, T. , Mishra, C. , Taylor, K. , Fogstad, H. , & Gupta, G. (2016). The global strategy for women's, children's and adolescents' health (2016–2030): A roadmap based on evidence and country experience. Bulletin of the World Health Organization, 94, 398–400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewallen, T. C. , Hunt, H. , Potts‐Datema, W. , Zaza, S. , & Giles, W. (2015). The whole school, whole community, whole child model: A new approach for improving educational attainment and healthy development for students. The Journal of School Health, 85(11), 729–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, R. , Benton‐davis S, & Grummer‐Strawn, L. (2015) The CDC guide to breastfeeding interventions. https://www.cdc.gov/breastfeeding/pdf/breastfeeding_interventions.pdf. Accessed Jan 31, 2019.
- Moukarzel, S. , Mamas, C. , Farhat, A. , & Daly, A. J. (2019). Getting schooled: Teachers' views on school‐based breastfeeding education in Lebanon. International Breastfeeding Journal, 14, 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moukarzel, S. , Mamas, C. , Warstadt, M. , Bode, L. , Farhat, A. , Abi Abboud, A. , & Daly, A. (2018). A case study on breastfeeding education in Lebanon's public medical school: Exploring the potential role of social networks in medical education. Medical Education Online, 23(1), 1527629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nabulsi, M. (2011). Why are breastfeeding rates low in Lebanon? A qualitative study. BMC Pediatrics, 30(11), 75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osman, H. , El Zein, L. , & Wick, L. (2009). Cultural beliefs that may discourage breastfeeding among Lebanese women: A qualitative analysis. International Breastfeeding Journal, 4(12), 12 10.1186/1746-4358-4-12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez‐Escamilla, R. , Curry, L. , Minhas, D. , Taylor, L. , & Bradley, E. (2012). Scaling up of breastfeeding promotion programs in low‐ and middle‐income countries: The “breastfeeding gear” model. Advances in Nutrition, 13(6), 790–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pérez‐Escamilla, R. , Hromi‐Fiedler, A. J. , Gubert, M. B. , Doucet, K. , Meyers, S. , & Dos Santos Buccini, G. (2018). Becoming Breastfeeding Friendly Index: Development and application for scaling‐up breastfeeding programmes globally. Maternal & Child Nutrition, 14, e12596 10.1111/mcn.12596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rea, L. , & Parker, R. (1992). Conventions for describing the magnitude of association in contingency tables In Parker R. (Ed.), Designing and conducting survey research. San Francisco: Jossey‐Boss. [Google Scholar]
- Rollins, N. , Bhandari, N. , Hajeebhoy, N. , Horton, S. , Lutter, C. , Martines, J. , … Victora, C. (2016). Why invest, and what it will take to improve breastfeeding practices? Lancet, 387(10017), 491–504. 10.1016/S0140-6736(15)01044-2 [DOI] [PubMed] [Google Scholar]
- Roseman, M. G. , Riddell, M. C. , & Haynes, J. N. (2011). A content analysis of kindergarten‐12th grade school‐based nutrition interventions: Taking advantage of past learning. Journal of Nutrition Education and Behavior, 43(1), 2–18. [DOI] [PubMed] [Google Scholar]
- Royal College of Paediatrics and Child Health . (2017). Position statement: Bbreastfeeding in the UK. Retrieved from https://www.rcpch.ac.uk/resources/position-statement-breastfeeding-uk
- Singletary, N. (2018) Exploring teachers' attitudes towards breastfeeding education and infant feeding education practices in North Carolina family and consumer sciences classrooms. PhD [dissertation]. Raleigh: North Carolina State University.
- Singletary, N. , Chetwynd, E. , Goodell, L. S. , & Fogleman, A. (2017). Stakeholder views of breastfeeding education in schools: A systematic mixed studies review of the literature. International Breastfeeding Journal, 27(12), 14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stockley, L. (2002). Consolidating and updating the evidence base for the promotion of breastfeeding. http://www.wales.nhs.uk/publications/bfeedingevidencebase.pdf.
- Victora, C. , Bahl, R. , Barros, A. , França, G. , Horton, S. , Krasevec, J. , … Rollins, N. C. (2016). Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet, 30, 387(10017), 475–490. 10.1016/S0140-6736(15)01024-7 [DOI] [PubMed] [Google Scholar]
- World Health Organization (2003). Global strategy for infant and young child feeding. Geneva: Report of a Joint WHO/UNICEF Consultation. Technical Report Series. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Number of participants completing the study by school and grade
Table S2. List of questions to assess general students' views on breastfeeding education
Table S3. Direct measures of TPB constructs
Table S4. Sample questions used to determine indirect measures of attitude, subjective norm and perceived control.
Table S5. List of factors used to assess attitudinal beliefs, control beliefs, and acceptance of public breastfeeding
Table S6. Summary of indirect measure scores for student beliefs (attitudinal, normative and control), acceptance of public breastfeeding and knowledge