

Abstract
STUDY QUESTION
What are the European trends and developments in ART and IUI in 2015 as compared to previous years?
SUMMARY ANSWER
The 19th ESHRE report on ART shows a continuing expansion of treatment numbers in Europe, and this increase, the variability in treatment modalities and the rising contribution to the birth rates in most participating countries all point towards the increasing impact of ART on European society.
WHAT IS KNOWN ALREADY
Since 1997, the ART data generated by national registries have been collected, analysed and reported in 18 manuscripts published in Human Reproduction.
STUDY DESIGN, SIZE, DURATION
Collection of European data by the European IVF-Monitoring Consortium (EIM) for ESHRE. The data for treatments performed between 1 January and 31 December 2015 in 38 European countries were provided by national registries or on a voluntary basis by clinics or professional societies.
PARTICIPANTS/MATERIALS, SETTINGS, METHODS
From 1343 institutions in 38 countries offering ART services a total of 849 811 treatment cycles, involving 155 960 with IVF, 385676 with ICSI, 218098 with frozen embryo replacement (FER), 21 041 with preimplantation genetic testing (PGT), 64 477 with egg donation (ED), 265 with IVM and 4294 with FOR were recorded. European data on IUI using husband/partner’s semen (IUI-H) and donor semen (IUI-D) were reported from 1352 institutions offering IUI in 25 countries and 21 countries, respectively. A total of 139 050 treatments with IUI-H and 49 001 treatments with IUI-D were included.
MAIN RESULTS AND THE ROLE OF CHANCE
In 18 countries (14 in 2014) with a population of approximately 286 million inhabitants, in which all institutions contributed to their respective national registers, a total of 409 771 treatment cycles were performed, corresponding to 1432 cycles per million inhabitants (range: 727–3068 per million). After IVF the clinical pregnancy rates (PRs) per aspiration and per transfer were slightly lower in 2015 as compared to 2014, at 28.5 and 34.6% versus 29.9 and 35.8%, respectively. After ICSI, the corresponding PR achieved per aspiration and per transfer in 2015 were also slightly lower than those achieved in 2014 (26.2 and 33.2% versus 28.4 and 35.0%, respectively). On the other hand, after FER with own embryos the PR per thawing continued to rise from 27.6% in 2014 to 29.2% in 2015. After ED a slightly lower PR per embryo transfer was achieved: 49.6% per fresh transfer (50.3% in 2014) and 43.4% for FOR (48.7% in 2014). The delivery rates (DRs) after IUI remained stable at 7.8% after IUI-H (8.5% in 2014) and at 12.0% after IUI-D (11.6% in 2014). In IVF and ICSI together, 1, 2, 3 and ≥4 embryos were transferred in 37.7, 53.9, 7.9 and in 0.5% of all treatments, respectively (corresponding to 34.9, 54.5, 9.9 and in 0.7% in 2014). This evolution towards the transfer of fewer embryos in both IVF and ICSI resulted in a proportion of singleton, twin and triplet DR of 83.1, 16.5 and 0.4%, respectively (compared to 82.5, 17.0 and 0.5%, respectively, in 2014). Treatments with FER in 2015 resulted in twin and triplet DR of 12.3 and 0.3%, respectively (versus 12.4 and 0.3% in 2014). Twin and triplet delivery rates after IUI-H were 8.9 and 0.5%, respectively (in 2014: 9.5 and 0.3%), and 7.3 and 0.6% after IUI-D (in 2014: 7.7 and 0.3%).
LIMITATIONS, REASONS FOR CAUTION
The methods of data collection and reporting vary among European countries. The EIM receives aggregated data from various countries with variable levels of completeness. Registries from a number of countries have failed to provide adequate data about the number of initiated cycles and deliveries. As long as incomplete data are provided, the results should be interpreted with caution.
WIDER IMPLICATIONS OF THE FINDINGS
The 19th EIM report on ART shows a continuing expansion of treatment numbers in Europe. The number of treatments reported, the variability in treatment modalities and the rising contribution to the birth rates in most participating countries point towards the increasing impact of ART on reproduction in Europe. Being the largest data collection on ART worldwide, detailed information about ongoing developments in the field is provided.
STUDY FUNDING/COMPETING INTEREST(S)
The study has no external funding and all costs are covered by ESHRE. There are no competing interests.
Keywords: IVF/ICSI/IUI using partner’s semen or donor semen, egg donation, frozen embryo replacement/insemination, surveillance, vigilance, registry/data collection
Introduction
This is the 19th annual report of the European IVF-monitoring Consortium (EIM) under the umbrella of ESHRE containing the data on ART reported by 38 participating European countries in 2015 (Supplementary Data).
Eighteen previous reports, all published in Human Reproduction (https://www.eshre.eu/Data-collection-and-research/Consortia/EIM/Publications.aspx), covered treatment cycles from 1997 to 2014. As in previous reports, the printed version contains the five most relevant tables. Nineteen additional supplementary tables are available online. The settings of the data are consistent with those published in the previous reports, allowing optimal comparisons with earlier trends.
Materials and Methods
Aggregated data on various forms of ART were provided by 38 European countries, covering the following treatment modalities: IVF, ICSI, frozen embryo replacement (FER), egg donation (ED), IVM, pooled data on preimplantation genetic testing (PGT) and frozen oocyte replacement (FOR). In addition, data on IUI using either husband’s/partner’s semen (IUI-H) and donor semen (IUI-D) were included. The report includes treatments started between 1 January and 31 December in 2015. Data on pregnancies and deliveries are derived from follow-up of the treatments performed in 2015. Each register was informed about the need to obtain signed informed consent prior to the initiation of infertility treatment from each infertile individual for whom data have to be reported to the registry.
For the collection of the data, the national representatives of 43 countries were asked to fill out questionnaires and data were transmitted through an online software package, specially designed for the requirements of this data collection (Dynamic Solutions, Barcelona, Spain). The dataset of 2014 has been extended with an optional module on fertility preservation and now consists of 10 different modules. The software performs all calculations automatically and evaluates the plausibility of all results. If inconsistencies are detected, the administrator of the ESHRE central office (V.G.) contacts the national representative for clarification. The data were assembled similarly as in the previous reports making the results comparable. As usual, footnotes to the tables provide additional information on diverging results reported by individual countries, when applicable.
The terminology used was based on the glossary of The International Committee for Monitoring Assisted Reproductive Technology (ICMART) (Zegers-Hochschild et al., 2017).
Results
Participation and data completeness
In Table I, the number of institutions or clinics offering ART services and those performing IUI is listed together with all available treatment modalities. In comparison to the 2014 data (De Geyter et al., 2018) not only has the number of reporting clinics increased (1279) in 2014 to 1343 in 2015, +4.9%), but also the overall number of reported treatments (776 556 in 2014 to 849 811 in 2015, +9.4%). Among the 51 European countries, eight are not members of the EIM Consortium (Supplementary Table SI), most being smaller countries not offering ART services. Georgia became a member of the EIM Consortium but has not yet provided any data to the Consortium. Croatia, Ireland, Slovakia and Turkey failed to deliver data. Of the 43 members, 38 submitted their data (88.4%) and in 18 countries (47.4%) all ART centres reported complete data sets. Currently, 1343 clinics reported their data (90.6% of all known clinics in Europe, 85.4% in 2013). As in 2014, the four European countries with the largest treatment numbers in 2015 were Spain (119 875 treatments), Russia (110723), Germany (96512) and France (93918).
Table I.
Treatment frequencies after ART in European countries in 2015.
| IVF clinics in the country | Cycles/million* | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | IVF clinics | Included IVF clinics | IUI labs | Included IUI labs | IVF | ICSI | FER | PGT | ED | IVM | FOR | All | Women 15–44 | Population |
| Albania | 8 | 1 | 8 | 1 | 112 | 50 | 16 | 178 | ||||||
| Armenia | 5 | 4 | 5 | 4 | 361 | 435 | 490 | 178 | 1 | 1465 | ||||
| Austria | 28 | 28 | 1347 | 5220 | 2204 | 7 | 8778 | 5331 | 1011 | |||||
| Belarus | 8 | 6 | 10 | 6 | 1489 | 1242 | 196 | 26 | 13 | 3 | 2969 | |||
| Belgium | 18 | 18 | 32 | 29 | 2909 | 14 239 | 11 699 | 580 | 802 | 71 | 30 300 | 14 272 | 2684 | |
| Bosnia–Herzegovina | 2 | 1 | 1 | 93 | 105 | 82 | 280 | |||||||
| Bulgaria | 35 | 35 | 1 | 1 | 933 | 6624 | 1643 | 37 | 612 | 9849 | 7417 | 1372 | ||
| Cyprus | 6 | 6 | 0 | 264 | 835 | 286 | 34 | 318 | 1737 | 9650 | 2044 | |||
| Czech Republic | 42 | 41 | 0 | 13 228 | 10 357 | 1561 | 4961 | 30 107 | ||||||
| Denmark | 21 | 21 | 56 | 54 | 6718 | 5737 | 4494 | 129 | 360 | 16 | 17 454 | 16 535 | 3068 | |
| Estonia | 5 | 5 | 5 | 5 | 623 | 1241 | 911 | 180 | 2955 | 11 913 | 2247 | |||
| Finland | 19 | 19 | 24 | 24 | 2567 | 2062 | 3839 | 44 | 831 | 9343 | 9576 | 1704 | ||
| France | 102 | 102 | 186 | 186 | 20 477 | 40 864 | 30 101 | 1328 | 1072 | 76 | 93 918 | 8047 | 1457 | |
| Germany | 134 | 130 | 0 | 0 | 17 382 | 55 904 | 23 226 | 96 512 | 6809 | |||||
| Greece | 46 | 46 | 46 | 46 | 2872 | 13 922 | 4127 | 793 | 5182 | 5 | 248 | 27 149 | 13 000 | 2420 |
| Hungary | 13 | 11 | 0 | 0 | 1098 | 4541 | 510 | 12 | 101 | 6262 | ||||
| Iceland | 1 | 1 | 1 | 1 | 198 | 181 | 252 | 108 | 739 | 11 029 | 2238 | |||
| Italy | 201 | 201 | 366 | 366 | 7985 | 47 344 | 12 903 | 2029 | 1615 | 1529 | 73 405 | 7199 | 1234 | |
| Kazakhstan | 23 | 6 | 23 | 6 | 1734 | 1883 | 667 | 132 | 600 | 4 | 5020 | |||
| Latvia | 5 | 4 | 5 | 4 | 372 | 769 | 452 | 103 | 441 | 6 | 2143 | |||
| Lithuania | 6 | 2 | 7 | 2 | 266 | 389 | 655 | |||||||
| Macedonia | 7 | 4 | 0 | 0 | 400 | 1519 | 157 | 58 | 2 | 2136 | ||||
| Malta | 2 | 2 | 2 | 0 | 231 | 80 | 311 | 3696 | 727 | |||||
| Moldova | 4 | 3 | 3 | 3 | 110 | 747 | 128 | 8 | 993 | |||||
| Montenegro | 5 | 4 | 6 | 4 | 9 | 439 | 58 | 506 | ||||||
| Norway | 11 | 11 | 11 | 11 | 3316 | 3140 | 3868 | 10 324 | 10 138 | 1985 | ||||
| Poland | 41 | 33 | 27 | 1050 | 14 382 | 9458 | 416 | 1031 | 30 | 124 | 26 491 | |||
| Portugal | 25 | 25 | 27 | 27 | 2376 | 3800 | 1573 | 104 | 797 | 10 | 8660 | 4327 | 831 | |
| Romania | 18 | 12 | 18 | 12 | 1196 | 1641 | 1021 | 3 | 68 | 1 | 5 | 3935 | ||
| Russia | 188 | 144 | 0 | 0 | 34 497 | 41 137 | 25 397 | 2913 | 6270 | 127 | 382 | 110 723 | ||
| Serbia | 18 | 3 | 18 | 3 | 260 | 205 | 23 | 488 | ||||||
| Slovenia | 3 | 3 | 3 | 3 | 986 | 2355 | 1271 | 28 | 3 | 6 | 4649 | 12 255 | 2241 | |
| Spain | 250 | 231 | 365 | 280 | 5786 | 47 893 | 23 692 | 7045 | 34 176 | 20 | 1263 | 119 875 | ||
| Sweden | 17 | 17 | 0 | 0 | 5976 | 6155 | 5838 | 323 | 311 | 18 603 | 10 203 | 1905 | ||
| Switzerland | 28 | 27 | 0 | 0 | 947 | 4604 | 4487 | 10 038 | ||||||
| The Netherlands | 13 | 13 | 0 | 0 | 6509 | 7605 | 11 327 | 695 | 26 136 | 8388 | 1543 | |||
| Ukraine | 43 | 38 | 18 | 18 | 1666 | 9221 | 5868 | 1417 | 1037 | 55 | 19 264 | |||
| UK | 84 | 84 | 105 | 105 | 21 188 | 23 725 | 15 443 | 1289 | 3321 | 4 | 491 | 65 461 | 5209 | 1001 |
| All | 1483 | 1343 | 1352 | 1229 | 155 960 | 385 676 | 218 098 | 21 041 | 64 477 | 265 | 4294 | 849 811 | 7795 | 1432 |
FER: frozen embryo replacement, PGT: preimplantation genetic testing, ED: egg donation, FOR: frozen oocyte replacement.
Bosnia–Herzegovina consists of two parts: the Federation part and the Republic of Srpska.
Treatment cycles in IVF and ICSI refer to initiated cycles.
For Belgium, France, Iceland and Lithuania, treatment cycles refer to aspirations. For Austria, Belgium and France the total number of initiated cycles was only available for IVF and ICSI together, being 9101, 20 050 and 682 582, respectively.
For the Czech Republic and Bosnia and Herzegovina, no distinction between IVF and ICSI is made. All cycles are counted as ICSI. For Belgium, there are 881 aspiration cycles for which it is not known whether IVF or ICSI was performed, in 1367 aspirations IVF and ICSI was used.
Treatment cycles in FER refer to thawings.
For Czech Republic, Kazakhstan, Sweden and The Netherlands, treatment cycles refer to transfers.
Treatment cycles in PGD contain both fresh and frozen cycles and refer to initiated cycles in the fresh cycles (except for Finland where it refers to aspirations) and thawings in the frozen cycles (except for The Netherlands where it refers to transfers).
Treatment cycles in ED refer to transfer cycles and contain fresh and frozen cycles.
Treatment cycles in IVM refer to aspirations.
Treatment cycles in FOR refer to thawings.
Women of reproductive age and population were found at the following link: https://population.un.org/wpp/DataQuery/
Reporting methods and size of the clinics
There is a large variability in the size of reporting institutions offering ART services, as defined by the number of treatment cycles (Supplementary Table SII). In 2015, clinics with cycle numbers between 200 and 499 were the most common (29.9%). When compared to previous EIM reports, the trend towards more large institutions may have stopped (≥1000 cycles, 17.9% in 2015 versus 18.3% in 2014 versus 17.8% in 2013 and 16.9% in 2012).
The motivation for collecting the data may be either voluntary or compulsory (Supplementary Table SIII). Among all participating countries, 19 fulfilled compulsory requirements (50.0%). In another 19 countries, the data collection was based on voluntary initiatives (50.0%). In countries with partial reporting, single personal initiatives continue to play a major role (five countries), as do medical organisations (in 11 countries). In 16 of 20 countries (80.0%) with incomplete data due to partial reporting, a voluntary data collection was present, whereas the data collection was more complete in countries with compulsory data collections (15 of 18 countries, 83.3%).
Aggregate data submission by single ART institutions to the respective national registries was still the most commonly used method (26 countries) in 2015. Individual cycles were reported from 12 countries (Supplementary Table SIII). Aggregate data collection was similarly prevalent in countries with complete and with partial reporting (61.1 versus 75.0%, respectively). Public access to individual clinic data was available only in 12 countries: Bosnia-Herzegovina, Republic of Srpska, Bulgaria, Estonia, Germany, Greece, Hungary, Romania, Slovenia, Spain, Sweden, The Netherlands and the UK. Additional financial support for the national registration was offered by the public, pharmaceutical industries or professional societies in 27 countries. In five countries, the centres covered part of the expenses while in three countries (Germany, Poland and Switzerland) all the expenses were covered by the centres alone. This information is missing in eight countries.
Number of treatment cycles per technique and availability
In 2015, up to a total of 849 811 treatment cycles were reported to EIM (73 255 more than in 2014, +9.4%) (Table I). Since the beginning of its activities, EIM has now recorded more than 8.8 million treatments with ART leading to the birth of more than 1.6 million infants (Table II). In 2015, the most commonly used technique was ICSI (385 676 cycles, 45.4%) followed by FER (218 098, 25.7%) and IVF (155 960, 18.4%). Compared to 2014, all treatment modalities numbers increased, except IVM. The steepest increase in treatment number was observed in FER (+13.6%), in ED (+14.1%) and in PGT (+32.4%). A small number of countries reported fewer treatment cycles (Austria, Belarus and Bosnia-Herzegovina). As in 2014, two countries reported a large increment in treatment numbers (Russia and Spain), both with more participating ART institutions.
Table II.
Number of institutions offering ART services, treatment cycles and infants born after ART in Europe, 1997–2015.
| Year | countries | clinics | Cycles | Cycle increase (%) | Infants born |
|---|---|---|---|---|---|
| 1997 | 18 | 482 | 203 225 | 35 314 | |
| 1998 | 18 | 521 | 232 225 | +14.3 | 21 433 |
| 1999 | 21 | 537 | 249 624 | +7.5 | 26 212 |
| 2000 | 22 | 569 | 275 187 | +10.2 | 17 887 |
| 2001 | 23 | 579 | 289 690 | +5.3 | 24 963 |
| 2002 | 25 | 631 | 324 238 | +11.9 | 24 283 |
| 2003 | 28 | 725 | 365 103 | +12.6 | 68 931 |
| 2004 | 29 | 785 | 367 056 | +0.5 | 67 973 |
| 2005 | 30 | 923 | 419 037 | +14.2 | 72 184 |
| 2006 | 32 | 998 | 458 759 | +9.5 | 87 705 |
| 2007 | 33 | 1029 | 493 420 | +7.7 | 96 690 |
| 2008 | 36 | 1051 | 532 260 | +7.9 | 107 383 |
| 2009 | 34 | 1005 | 537 463 | +1.0 | 109 239 |
| 2010 | 31 | 991 | 550 296 | +2.4 | 120 676 |
| 2011 | 33 | 1314 | 609 973 | +11.3 | 134 106 |
| 2012 | 34 | 1354 | 640 144 | +4.9 | 143 844 |
| 2013 | 38 | 1169 | 686 271 | +7,2 | 149 466 |
| 2014 | 39 | 1279 | 776 556 | +13,1 | 170 163 |
| 2015 | 38 | 1343 | 849 811 | +10.2 | 187 542 |
| total | 8 854 745 | 1 665 994 |
Among the total of 541 636 fresh treatments (ICSI+IVF), 71.2% were performed with ICSI, showing a rise of +6.5% compared to 2014. The preponderance of ICSI over conventional IVF still continues to be more pronounced (Fig. 1).
Figure 1.
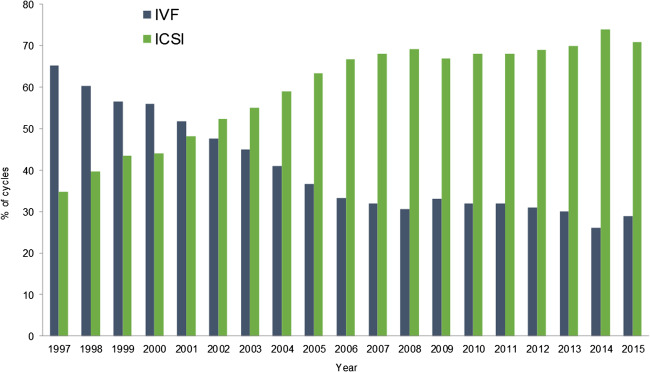
Proportion of IVF versus ICSI in Europe, 1997–2015.
As in previous years, with 218 098 treatments, FER is rapidly gaining ground (+13.6%) but the relative proportion of FER to fresh treatments was stable (40.3% in 2015 and 37.8% in 2014). Switzerland is the country with the highest proportion of FER (44.7% of all treatment modalities) and Serbia with the lowest (4.7%).
Availability of ART in any particular country is calculated by dividing the number of treatment cycles by the number of women of reproductive age (15 to 45 years) (Supplementary Table SIV). Availability can only be calculated in the 18 countries with full coverage, and in those 18 countries, a huge variability in availability was observed, ART being most available in Denmark and least available in Malta. As a result, the proportion of newborns resulting from ART born in Denmark was 6.6% of all newborns in that country and 0.6% in Malta.
Pregnancies and deliveries after treatment
Table III lists pregnancy (PR) and delivery rates (DR) after IVF or ICSI and after FER (after both IVF and ICSI). As in previous reports, data on the number of initiated cycles were incomplete. For that reason, we calculated outcome data per aspiration. Among the 38 participating countries, only 34 were able to provide pregnancy and delivery data after aspiration after IVF and ICSI (completeness rate: 89.5%). Six countries failed to provide those after FER (completeness rate: 84.2%). Complete coverage data on both pregnancies and deliveries were provided by 18 countries (Supplementary Table SIV). As in earlier reports, the PR and DR (all treatment modalities included) varied significantly from one country to another, with PR ranging from 19.6 to 44.0%, and DR ranging from 10.2 to 40.0% in fresh cycles after IVF or ICSI. After FER, the DR varied between 12.8 and 37.5% among different countries.
Table III.
Results after ART in 2015.
| IVF | ICSI | FER | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Initiated Cycles IVF + ICSI | Aspirations | Pregnancies per aspiration (%) | Deliveries per aspiration (%) | Aspirations | Pregnancies per aspiration (%) | Deliveries per aspiration (%) | Thawings FER | Pregnancies per thawing (%) | Deliveries per thawing (%) | ART infants | ART infants per national births (%) |
| Albania | 112 | 110 | 40.9 | 32.7 | 50 | 34.0 | 26.0 | 65 | ||||
| Armenia | 796 | 361 | 40.4 | 33.8 | 435 | 37.7 | 29.2 | 490 | 38.0 | 31.8 | 597 | 1.4 |
| Austria | 9101 | 1347 | 35.5 | 30.6 | 5220 | 30.4 | 25.9 | 2204 | 34.0 | 29.2 | 2414 | 2.9 |
| Belarus | 2731 | 1435 | 39.2 | 30.8 | 1239 | 39.2 | 32.0 | 196 | 32.1 | 17.3 | 1116 | 0.9 |
| Belgium | 20 050 | 2909 | 22.3 | 18.0 | 14 239 | 21.0 | 17.2 | 11 699 | 21.1 | 17.1 | 5702 | 4.7 |
| Bosnia–Herzegovina | 105 | 93 | 82 | 44.8 | 24.1 | 200 | 0.2 | |||||
| Bulgaria | 7557 | 823 | 29.4 | 20.5 | 5770 | 26.5 | 19.1 | 1643 | 34.4 | 20.7 | 1830 | 2.8 |
| Cyprus | 1099 | 243 | 30.0 | 28.0 | 799 | 41.8 | 39.0 | 286 | 24.1 | 18.9 | ||
| Czech Republic | 13 228 | 12 872 | 25.6 | 16.3 | 5590 | 5 | ||||||
| Denmark | 12 455 | 6396 | 22.3 | 19.4 | 5718 | 24.8 | 21.9 | 4494 | 24.5 | 21.2 | 3865 | 6.6 |
| Estonia | 1864 | 623 | 27.6 | 21.3 | 1241 | 27.3 | 19.0 | 911 | 19.4 | 12.8 | 633 | 4.5 |
| Finland | 4629 | 2424 | 26.6 | 20.2 | 1982 | 26.4 | 20.8 | 3839 | 25.7 | 20.0 | 1667 | 3.0 |
| France | 68 258 | 20 477 | 22.9 | 18.7 | 40 864 | 23.4 | 19.2 | 30 101 | 21.6 | 16.5 | 19 181 | 2.4 |
| Germany | 73 286 | 15 990 | 26.4 | 19.4 | 51 448 | 26.9 | 19.7 | 23 226 | 25.3 | 17.1 | 20 878 | 2.8 |
| Greece | 16 794 | 2684 | 27.5 | 20.5 | 13 407 | 26.5 | 16.3 | 4127 | 32.3 | 20.0 | 5059 | |
| Hungary | 5638 | 1094 | 24.7 | 4539 | 22.9 | 510 | 37.8 | |||||
| Iceland | 198 | 26.3 | 17.7 | 181 | 24.3 | 19.9 | 252 | 26.2 | 17.5 | 149 | 3.6 | |
| Italy | 55 329 | 7107 | 23.0 | 15.8 | 43 107 | 19.6 | 12.5 | 12 903 | 26.2 | 18.6 | 11 275 | 2.3 |
| Kazakhstan | 3617 | 1734 | 36.5 | 24.8 | 1883 | 42.8 | 32.2 | 1618 | 0.4 | |||
| Latvia | 1141 | 372 | 28.2 | 22.3 | 764 | 30.8 | 21.7 | 452 | 46.0 | 35.4 | 634 | |
| Lithuania | 266 | 33.8 | 389 | 33.4 | ||||||||
| Macedonia | 1919 | 372 | 41.9 | 10.2 | 1378 | 40.2 | 34.3 | 157 | 29.3 | 14.6 | 655 | 2.8 |
| Malta | 231 | 216 | 25 | 0.6 | ||||||||
| Moldova | 857 | 100 | 44.0 | 37.0 | 707 | 43.1 | 40.0 | 128 | 31.3 | 27.3 | ||
| Montenegro | 448 | 9 | 33.3 | 22.2 | 432 | 25.2 | 17.6 | 58 | 36.2 | 31.0 | 118 | 1.6 |
| Norway | 6456 | 3316 | 26.5 | 22.4 | 3140 | 28.3 | 23.5 | 3868 | 19.3 | 15.4 | ||
| Poland | 15 432 | 1010 | 29.4 | 21.4 | 14 191 | 27.7 | 18.4 | 9458 | 31.2 | 19.8 | 5482 | 1.5 |
| Portugal | 6176 | 2242 | 29.9 | 22.9 | 3613 | 26.1 | 19.3 | 1573 | 31.3 | 21.6 | 2260 | 2.6 |
| Romania | 2837 | 1159 | 36.8 | 28.8 | 1598 | 33.6 | 27.8 | 1021 | 25.2 | 18.1 | 1236 | 0.7 |
| Russia | 75 634 | 33 757 | 30.9 | 22.5 | 40 204 | 28.3 | 20.5 | 25 397 | 38.7 | 27.8 | 30 039 | 1.6 |
| Serbia | 465 | 238 | 33.6 | 25.6 | 202 | 31.7 | 24.8 | 23 | 34.8 | 34.8 | 141 | 0.2 |
| Slovenia | 3341 | 944 | 34.3 | 27.9 | 2274 | 26.6 | 20.4 | 1271 | 33.8 | 25.3 | 1172 | 5.7 |
| Spain | 53 679 | 5235 | 28.0 | 20.0 | 42 261 | 25.0 | 17.6 | 23 692 | 33.6 | 22.1 | 29 941 | 7.1 |
| Sweden | 12 131 | 5594 | 30.7 | 25.7 | 5799 | 26.8 | 22.7 | 4790 | 4.1 | |||
| Switzerland | 5551 | 852 | 27.2 | 20.3 | 4232 | 23.3 | 17.9 | 4487 | 20.8 | 14.3 | 1836 | 2.1 |
| The Netherlands | 14 114 | 5687 | 30.9 | 22.7 | 6820 | 32.0 | 23.9 | |||||
| Ukraine | 10 887 | 1626 | 36.3 | 26.0 | 9028 | 31.1 | 24.4 | 5868 | 44.4 | 37.5 | 6795 | 1.7 |
| UK | 44 913 | 18 535 | 32.4 | 28.2 | 23 592 | 33.7 | 29.6 | 15 443 | 33.3 | 28.7 | 20 599 | 2.7 |
| All | 552 861 | 147 252 | 28.5 | 21.8 | 365 894 | 26.2 | 19.3 | 189 909 | 29.2 | 21.3 | 187 542 | 2.3 |
Total rates refer to these countries were all data were reported for the given technique.
†ART infants also include ED.
For IVF and ICSI, there were for France, Greece, Ireland, Kazakhstan, Russia and Spain, respectively, 177, 46, 1, 8, 543 and 27 deliveries with unknown outcome. These were accepted as singletons to calculate the ART infants.
For FER, there were for France, Greece, Kazakhstan, Russia and Spain, respectively, 41, 4, 2, 8 and 4 deliveries with unknown outcome. These were accepted as singletons to calculate the ART infants.
For the Netherlands, no data on the number of thawings were available.
For ED, there were for France, Greece, Kazakhstan, Poland, Russia, Spain and Ukraine respectively 1, 2, 1, 1, 23, 8 and 9 deliveries with unknown outcome. These were accepted as singletons to calculate the ART infants.
For PGD, there was for Russia one delivery with unknown outcome. This one was accepted as singleton to calculate the ART infants.
In the Czech Republic, IVF and ICSI were reported together, no details on pregnancies and deliveries.
Detailed accounts of cycle numbers, aspirations, transfers, pregnancies, deliveries in IVF, ICSI and FER (after both IVF and ICSI) are given in the Supplementary Tables SV, SVI and SVII. For the second time, information about ‘freeze all’ cycles was collected (Supplementary Table SV). As in 2014, ‘freeze all’ was carried out at the oocyte level in six reporting countries (15.8%) and at the embryonic level in 21 reporting countries (55.2%) (46.1%, in 2014: 18 countries).
Whereas in 2014 only 22 countries were able to provide egg/oocyte donation (ED) data, in 2015 the data from 29 of 38 participating countries are available (76.3%) (Supplementary Table SVIII). In most of the other countries, this technology is not being performed for legal reasons. Most donation cycles were carried out in Spain, Russia, the Czech Republic and Greece. Approximately 31 511 ED cycles were carried out with freshly collected oocytes, fewer with frozen oocytes (FOR, 13107 cycles). Pregnancy rates were only available per embryo transfer (ET), but were considerably higher with freshly donated oocytes (49.6%) than after thawing of oocytes (40.3%). The differences among countries were considerable, ranging between 16.7 and 58.1% after thawing. A total of 19 849 deliveries were counted, which considerably exceeds the 17 259 deliveries counted in 2014 (+15.0%). This increment is due to overall higher numbers of reported treatments with ED, regardless of whether eggs were frozen or not.
Age distribution
As in previous reports, the age distribution of women treated with IVF and ICSI varied among different countries (Supplementary Tables SIX and SX). Not all countries were able to provide data on the age distribution in ICSI and in IVF, some because no IVF treatments were carried out. As in 2013 and in 2014, the highest percentage of women aged 40 years and older undergoing aspiration for IVF was found in Greece, whereas the highest percentage of women aged <34 years was found in Montenegro. Also in ICSI, the highest percentage of women aged 40 years and older undergoing aspiration was found in Greece, whereas the highest percentage of women undergoing aspiration aged <34 years was recorded in Albania (as in 2013 and in 2014). Overall, the well-known age-dependent decline of the reported PR and DR was very similar in IVF and ICSI, but the differences among countries were considerable.
Although the age-related decline was present in FER cycles as well (Supplementary Table SXI), the outcome data of FER were generally higher than in the fresh cycles. In contrast, in ED donation cycles (Supplementary Table SXII) age of the recipient women did not impact on PR or on DR.
Number of embryos transferred and multiple births
The number of embryos transferred after IVF and ICSI together is presented in Table IV. Although the specific number of elective single embryo transfers (SET) cannot be identified, the number of transfers of only one embryo per cycle continued to rise (37.7% in 2015, as compared to 34.9% in 2014), whereas the number of transfers of three or more embryos per cycle decreased (Fig. 2). As in 2014, the same eight countries performed more than 50% SET (Austria, Belgium, Czech Republic, Denmark, Finland, Iceland, Poland and Sweden). Only one country with more than 40% of transfers with three embryos remained in 2015, i.e. Serbia. In Greece, 4.9% of all embryo transfers were carried out with four or more embryos.
Table IV.
Number of embryos transferred after ART and deliveries in 2015.
| IVF + ICSI | FER | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Transfers | 1 embryo (%) | 2 embryos (%) | 3 embryos (%) | 4+ embryos (%) | Deliveries | Twin (%) | Triplet (%) | Deliveries | Twin (%) | Triplet (%) |
| Albania | 103 | 5.8 | 79.6 | 13.6 | 1.0 | 36 | 19.4 | 2.8 | 13 | 7.7 | 0.0 |
| Armenia | 651 | 14.9 | 62.7 | 22.4 | 0.0 | 249 | 32.0 | 4.5 | 156 | 21.2 | 0.0 |
| Austria | 5692 | 62.0 | 37.5 | 0.5 | 0.0 | 1766 | 643 | ||||
| Belarus | 2498 | 13.4 | 64.3 | 22.3 | 0.0 | 838 | 25.5 | 0.6 | 34 | 17.6 | 2.9 |
| Belgium | 14 101 | 59.9 | 34.3 | 5.2 | 0.6 | 2976 | 8.8 | 0.2 | 2006 | 6.2 | 0.2 |
| Bosnia–Herzegovina | 476 | 13.7 | 45.8 | 39.5 | 1.0 | 128 | 30.5 | 1.6 | 20 | 25.0 | 0.0 |
| Bulgaria | 4737 | 21.7 | 56.3 | 21.9 | 0.2 | 1269 | 340 | ||||
| Cyprus | |||||||||||
| Czech Republic | 10 344 | 66.3 | 32.6 | 1.2 | 0.0 | 2092 | 9.8 | 0.2 | 1727 | 9.8 | 0.3 |
| Denmark | 9760 | 64.0 | 34.2 | 1.9 | 0.0 | 2498 | 8.3 | 0.1 | 953 | 8.2 | 0.0 |
| Estonia | 1618 | 39.3 | 53.6 | 7.0 | 0.0 | 369 | 14.4 | 0.0 | 117 | 18.8 | 0.9 |
| Finland | 3568 | 82.0 | 18.0 | 0.0 | 0.0 | 900 | 767 | ||||
| France | 46 946 | 42.4 | 52.1 | 5.2 | 0.4 | 11 678 | 13.8 | 0.1 | 4958 | 8.4 | 0.1 |
| Germany | 56 112 | 21.6 | 69.2 | 9.2 | 0.0 | 13 239 | 21.5 | 0.6 | 3976 | 15.3 | 0.6 |
| Greece | 11 428 | 20.6 | 55.1 | 19.3 | 4.9 | 2743 | 24.5 | 0.6 | 825 | 18.0 | 0.8 |
| Hungary | 5129 | 20.8 | 57.3 | 18.2 | 3.8 | ||||||
| Iceland | 314 | 69.7 | 30.3 | 71 | 7.0 | 0.0 | 44 | 9.1 | 0.0 | ||
| Italy | 37 975 | 28.8 | 48.3 | 21.0 | 1.9 | 6498 | 17.3 | 0.8 | 2403 | 8.7 | 0.2 |
| Kazakhstan | 1036 | 17.3 | 1.4 | 168 | 9.5 | 0.0 | |||||
| Latvia | 880 | 33.1 | 65.7 | 1.2 | 0.0 | 249 | 16.8 | 0.8 | 160 | 5.8 | 1.0 |
| Lithuania | |||||||||||
| Macedonia | 1637 | 25.8 | 67.1 | 7.1 | 0.0 | 510 | 16.5 | 0.8 | 23 | 30.4 | 0.0 |
| Malta | 287 | 22 | 13.6 | 0.0 | |||||||
| Moldova | |||||||||||
| Montenegro | 394 | 25.4 | 36.8 | 36.8 | 1.0 | 78 | 21.8 | 0.0 | 18 | 27.8 | 0.0 |
| Norway | |||||||||||
| Poland | 11 214 | 63.0 | 36.6 | 0.4 | 0.0 | 2821 | 10.6 | 0.3 | 1874 | 8.2 | 0.2 |
| Portugal | 4479 | 29.9 | 68.5 | 1.7 | 0.0 | 1212 | 19.9 | 0.3 | 339 | 17.7 | 0.3 |
| Romania | 2279 | 16.9 | 60.0 | 21.1 | 2.1 | 778 | 25.3 | 0.7 | 185 | 23.9 | 0.0 |
| Russia | 59 934 | 32.9 | 61.5 | 5.5 | 0.2 | 15 833 | 19.1 | 0.6 | 7069 | 14.9 | 0.3 |
| Serbia | 386 | 20.7 | 31.6 | 47.7 | 0.0 | 111 | 23.4 | 0.0 | |||
| Slovenia | 2688 | 44.0 | 55.5 | 0.5 | 0.0 | 727 | 10.7 | 0.0 | 321 | 13.1 | 0.0 |
| Spain | 33 039 | 27.9 | 67.4 | 4.7 | 0.0 | 8497 | 19.2 | 0.2 | 5237 | 15.0 | 0.2 |
| Sweden | 9326 | 81.2 | 18.8 | 0.0 | 0.0 | 2750 | 4.4 | 0.0 | 1709 | 2.8 | 0.1 |
| Switzerland | 4043 | 32.1 | 58.1 | 9.7 | 0.0 | 929 | 17.8 | 0.2 | 642 | 15.0 | 0.0 |
| The Netherlands | |||||||||||
| Ukraine | 7845 | 22.8 | 64.2 | 12.9 | 0.2 | 2630 | 19.0 | 0.5 | 2198 | 18.4 | 0.0 |
| UK | 37 846 | 49.9 | 46.4 | 3.7 | 0.0 | 12 213 | 12.7 | 0.2 | 4434 | 13.4 | 0.4 |
| All* | 387 729 | 37.7 | 53.9 | 7.9 | 0.5 | 97 746 | 16.5 | 0.4 | 43 359 | 12.3 | 0.3 |
*Totals refer only to these countries where data on number of transferred embryos and on multiplicity were reported.
Figure 2.
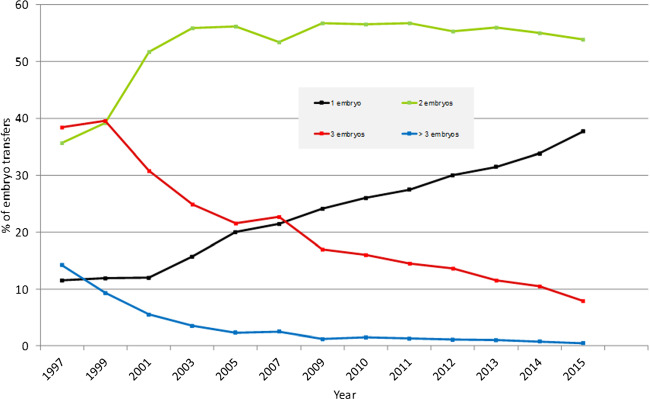
Number of embryos transferred in IVF and ICSI during fresh cycles in Europe, 1997–2015.
Additional details about the pregnancy and delivery data are given in Supplementary Tables SXIII and SXIV. The recorded incidence of pregnancy loss was 16.4% after IVF + ICSI (in 2014: 15.5%) and 20.6% after FER (in 2014: 18.6%). The recorded loss to follow-up was 6.3% after IVF + ICSI (in 2014: 9.9%) and 7.4% after FER (in 2014: 7.3%).
Since the first recorded European data sets, as recorded by EIM, the proportion of both twin and triplet deliveries was found to be declining. Twin and triplet deliveries were similar after IVF + ICSI treatments as after FER. Those countries with the highest proportion of SET also had the lowest twin and triplet delivery rates (the lowest in Sweden, 4.4 and 0%, respectively) after fresh cycles. The countries still proceeding with the transfer of three or more embryos in fresh cycles present with DR of twins ranging between 21.8% (Montenegro) and 32.0% (Bosnia-Herzegovina), and with DR of triplets ranging between 0.6% (Greece) and 4.5% (Armenia). Unfortunately, Finland with the highest SET rate of 82% did not report on multiplicity.
Regarding ED, of 15 178 deliveries with information regarding multiplicity, 3001 were twins (19.8%) and 37 were triplets (0.2%) (data not presented in tables).
Perinatal risks and complications
In 2015, data on premature deliveries were available from 18 European countries (in 2014 from 20 countries). The incidence of premature delivery is listed according to the number of newborns in Supplementary Table SXV. The prematurity data resulting from fresh IVF and ICSI, from FER and from ED, are listed together. The incidence of extreme preterm birth (gestational weeks 20–27) reached 1.3% in singleton pregnancies (0.9% in 2014), 3.7% in twin pregnancies (3.4% in 2014) and 13.4% in triplet pregnancies (10.0% in 2014). A high incidence of very premature birth rates (gestational weeks 28–32) was found in twin pregnancies: 9.9% (in 2014: 10.7%) and in triplet pregnancies: 39.2% (in 2014: 34.9%). Term delivery (≥37 weeks) was 86.4% in singleton pregnancies, 44.7% in twin pregnancies and 7.5% in triplet pregnancies, all similar to the results achieved in 2014. Interestingly, the premature DR (<37 weeks) of singleton pregnancies calculated per ET is similar to the premature DR of twin pregnancies (Fig. 3).
Figure 3.
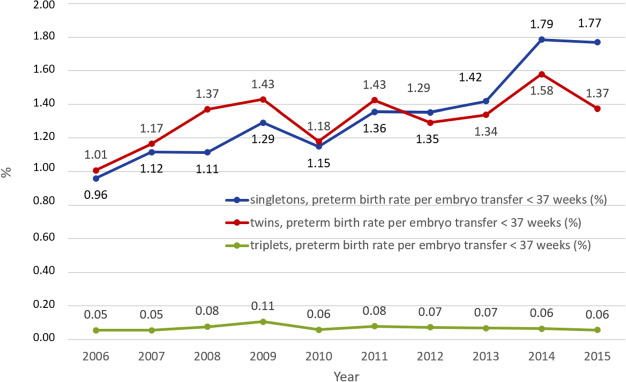
Proportion of premature deliveries (<37 weeks of gestation in relation to pregnancies ≥37 weeks of gestation) in singleton, twin and triplet pregnancies in Europe, 2006–2015.
As in 2014, complications of various steps of ART, such as ovarian hyperstimulation syndrome (OHSS), haemorrhage, infections and maternal deaths, were reported by 31 countries (Supplementary Table SXVI). With 2167 cases, OHSS was the most common reported complication of ART (incidence rate: 0.44% of all reported cycles, compared to 0.3% in 2014 with 2040 cases). Other complications were much rarer, such as haemorrhage (0.11% of all treatment cycles), infections (0.01%) and maternal death (two per 850 000 treatment cycles). The circumstances of the observed maternal deaths were not provided.
Foetal reductions were reported from 26 countries and were performed in 0.06% of all treatment cycles. Most foetal reductions were reported by the UK, Spain and Russia, as in 2014.
PGT-M/SR/PGT-A
PGT-M/SR (for monogenic disorders or structural rearrangements) and PGT-A (for aneuploidy) activities were reported from 23 countries (22 in 2014, 20 in 2013). The number of treatment cycles was 21 041 (2.48% of all ART treatments, Table I), which compared to 2014 represents a drastic rise in treatment numbers. These involved 16 685 fresh cycles and 4356 thawings, resulting in 6696 fresh ET and 4059 FER. In total, 2662 pregnancies (39.7% per transfer) and 2161 deliveries (32.3% per transfer) resulted from fresh cycles. Corresponding figures for FER were 1666 (41.0% per transfer) and 1398 (34.4% per transfer). The main contributor was Spain with 7045 cycles followed by Russia with 2913 cycles. A more detailed survey of PGT activities can be found in the annual reports of the ESHRE PGT Consortium (De Rycke et al., 2017).
IVM
A total of 265 treatments with IVM were reported from eight countries (292 in 2014) (Table I). Most IVM cycles were performed in Russia. A total of 154 transfers resulted in 45 pregnancies and 33 deliveries.
FOR
FOR was reported by 17 countries (16 in 2014), and this accounted for 4294 thawing cycles (3404 in 2014) (Table I), 3478 transfers, 1067 pregnancies and 716 deliveries, Italy and Spain being the largest contributors (1529 and 1263 cycles, respectively).
IUI
Data on IUI-H (Supplementary Table SXVII) and IUI-D (Supplementary Table SXVIII) were collected by 1229 institutions in 26 and 22 countries, respectively (Table V). Spain, Belgium and Denmark were the most active countries in both treatment modalities. Altogether, 189 764 treatments with IUI-H resulted in 14 886 deliveries (7.8%), whereas 49 514 treatments with IUI-D resulted in 5926 deliveries (12.0%). Many more treatment IUI cycles were reported in 2015 than in 2014, but the outcome results are similar to those reported earlier. In all three age groups (≤34, 35–39 and ≥40 years), most pregnancies led to singleton deliveries (90.6% in IUI-H, 92.1% in IUI-D). The twin and triplet DRs for IUI-H and IUI-D were generally low, depending on the age of the treated patient and were similar to those reported in previous years (twin deliveries: 8.9 and 7.3%, respectively; triplet deliveries: 0.5 and 0.6%, respectively).
Table V.
IUI with husband or donor semen in 2015.
| IUI-H | IUI-D | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Cycles | Deliveries | Deliveries (%) | Singleton (%) | Twin (%) | Triplet (%) | Cycles | Deliveries | Deliveries (%) | Singleton (%) | Twin (%) | Triplet (%) |
| Albania | ||||||||||||
| Armenia | 571 | 98 | 17.2 | 90.8 | 9.2 | 0.0 | 313 | 60 | 19.2 | 91.7 | 8.3 | 0.0 |
| Austria | ||||||||||||
| Belarus | 952 | 107 | 11.2 | 99.1 | 0.9 | 0.0 | ||||||
| Belgium | 13 162 | 769 | 5.8 | 95.3 | 4.4 | 0.3 | 8112 | 597 | 7.4 | 94.5 | 5.4 | 0.2 |
| Bosnia–Herzegovina | 191 | 17 | 8.9 | 94.2 | 5.8 | 0.0 | ||||||
| Bulgaria | 2976 | 171 | 5.7 | 590 | 35 | 5.9 | ||||||
| Cyprus | ||||||||||||
| Czech Republic | ||||||||||||
| Denmark | 10 339 | 1291 | 12.5 | 88.9 | 9.6 | 1.5 | 9924 | 879 | 8.9 | 95.2 | 4.4 | 0.3 |
| Estonia | 139 | 6 | 4.3 | 100.0 | 0.0 | 0.0 | 91 | 4 | 4.4 | 100.0 | 0.0 | 0.0 |
| Finland | 3126 | 284 | 9.1 | 1171 | 138 | 11.8 | ||||||
| France | 50 714 | 5065 | 10.0 | 89.7 | 9.9 | 0.3 | 3294 | 570 | 17.3 | 89.6 | 10.2 | 0.2 |
| Germany | ||||||||||||
| Greece | 4561 | 313 | 6.9 | 94.2 | 5.8 | 0.0 | 287 | 41 | 14.3 | 95.1 | 4.9 | 0.0 |
| Hungary | ||||||||||||
| Iceland | ||||||||||||
| Italy | 22 549 | 1588 | 7.0 | 90.9 | 8.2 | 0.9 | 513 | 61 | 11.9 | 88.5 | 9.8 | 1.6 |
| Kazakhstan | 810 | 25 | 3.1 | 100.0 | 0.0 | 0.0 | 125 | 8 | 6.4 | 100.0 | 0.0 | 0.0 |
| Latvia | 96 | 10 | 10.4 | 85.7 | 14.3 | 0.0 | 53 | 6 | 11.3 | 100.0 | 0.0 | 0.0 |
| Lithuania | ||||||||||||
| Macedonia | 1186 | 62 | 5.2 | 100.0 | 0.0 | 0.0 | 29 | 3 | 10.3 | 100.0 | 0.0 | 0.0 |
| Malta | ||||||||||||
| Moldova | 102 | 7 | 6.9 | 100.0 | 0.0 | 0.0 | ||||||
| Montenegro | 222 | 24 | 10.8 | 87.5 | 12.5 | 0.0 | ||||||
| Norway | 20 708 | 47 | 0.2 | 83.0 | 17.0 | 0.0 | 614 | 119 | 19.4 | 95.8 | 4.2 | 0.0 |
| Poland | 9036 | 570 | 6.3 | 94.3 | 5.5 | 0.2 | 1729 | 173 | 10.0 | 96.3 | 3.7 | 0.0 |
| Portugal | 2188 | 195 | 8.9 | 90.3 | 8.7 | 1.0 | 236 | 50 | 21.2 | 88.0 | 12.0 | 0.0 |
| Romania | 2091 | 169 | 8.1 | 91.7 | 8.3 | 0.0 | 191 | 21 | 11.0 | 90.5 | 9.5 | 0.0 |
| Russia | 10 013 | 1181 | 11.8 | 93.2 | 6.7 | 0.2 | 4128 | 574 | 13.9 | 90.9 | 6.3 | 2.8 |
| Serbia | 408 | 28 | 6.9 | 89.3 | 10.7 | 0.0 | ||||||
| Slovenia | 246 | 18 | 7.3 | 88.9 | 11.1 | 0.0 | 1 | 0 | 0.0 | |||
| Spain | 26 959 | 2713 | 10.1 | 88.9 | 10.7 | 0.4 | 11 944 | 1747 | 14.6 | 88.8 | 10.8 | 0.4 |
| Sweden | 760 | 115 | 15.1 | 100.0 | 0.0 | 0.0 | ||||||
| Switzerland | ||||||||||||
| The Netherlands | ||||||||||||
| Ukraine | 1570 | 128 | 8.2 | 89.6 | 10.4 | 0.0 | 468 | 53 | 11.3 | 92.5 | 7.5 | 0.0 |
| UK | 4849 | 4941 | 672 | 13.6 | 94.9 | 4.6 | 0.4 | |||||
| All* | 189 764 | 14 886 | 7.8 | 90.6 | 8.9 | 0.5 | 49 514 | 5926 | 12.0 | 92.1 | 7.3 | 0.6 |
*Total refers to these countries where data were reported, and mean percentage was computed on countries with complete information.
Iceland 125 IUI with husband semen (IUI-H) and 177 IUI with donor semen (IUI-D) cycles performed without further information.
Italy: underestimation of deliveries because of high number of pregnancies is lost to follow-up.
Slovenia: Data from two clinics only.
Sum of fresh and FER (‘cumulative’) DR
Supplementary Table SXIX provides us with an estimate (not a true rate, as the data set presented here is cross-sectional) of a cumulative DR, calculated from the fresh ET and those carried out after thawing. The data are presented based on the sum of the fresh and FER deliveries and the number of aspirations of the same year as the denominator. As no data on deliveries were available from Hungary, Bosnia and Herzegovina and Lithuania, we were able to calculate cumulative delivery rates for 35 countries (38 countries in 2014). Whereas in all data taken together, the DR after the fresh cycle amounted to 20.0%, the cumulative DR was 28.9%. The countries with the highest benefit resulting from FER were Ukraine (+20.6%), Armenia (+19.6%) and Finland (+17.4). The countries with the lowest benefit resulting from FER were Belarus (+1.3%) and Macedonia (+1.4%).
Cross-border reproductive care
Eleven countries reported data on cross-border patients: Albania, Belarus, Denmark, Iceland, Macedonia, Malta, Poland, Portugal, Slovenia, Spain and Switzerland. A total of 14 273 cycles were reported, 29.4% of which involved IVF/ICSI with the couple’s own gametes, 47.1% were oocyte donations and 22.3% were IVF or ICSI with semen donation. Additionally, 7714 IUI with sperm donation were registered. Information regarding the countries of origin was very incomplete and not reliable enough to draw any meaningful conclusions. The main reasons reported by patients were to have access to a technique not legally available in their home countries (41.7%) or to seek a higher quality treatment (16.6%).
Fertility preservation
Twelve countries were able to provide data on fertility preservation: Albania, Belarus, Belgium, the Czech Republic, France, Greece, Italy, Macedonia, Poland, Portugal, Slovenia and Spain. There were 3659 cases with oocyte cryopreservation and 10 590 cases with ejaculated sperm collection and cryopreservation reported. All other forms of preservation were carried out in 614 cases (prepubertal ovarian tissue, postpubertal ovarian tissue, prepubertal testicular tissue, postpubertal testicular tissue and epididymal sperm).
Only four countries report non-medical oocyte cryopreservation, and three countries report non-medical ejaculated semen collection and cryopreservation. In all other cases, preservation is only carried out for medical reasons.
At this moment, too few data were obtained to report on the outcome.
Discussion
This is the 19th annual report of the combined activities of the European (national) registries collecting data on ART. From 1997 to 2015, the EIM Consortium of ESHRE has reported on close to 9 million treatments (8860338) leading to the birth of more than 1.6 million infants (1665994).
The present data report summarizes the totality of the data collections provided by 38 European countries (39 in 2014). For the first time, Armenia provided data. Georgia joined the EIM Consortium, but has not yet been able to submit data, nor did Croatia and Ireland for organisational reasons. Azerbaijan, Kosovo and Luxemburg have not yet joined the EIM Consortium. Another group of small European countries have not considered joining the Consortium, such as Andorra, Liechtenstein, Monaco, San Marino and the Vatican, most likely all without ART services. Excluding these eight countries, the level of completeness at the national level amounts to 88.4% and the number of reporting clinics to 90.6%, which is similar to the participation levels achieved in 2014 (92.9%, respectively 87.5%, De Geyter et al., 2018). Whereas the tendency towards large ART services with more than 1000 cycles per year seems to have stabilized in recent years, there are now more middle-sized ART institutions with treatment numbers between 200 and 1000 cycles per year (Supplementary Table SII). The level of completeness is highly variable among countries with 18 countries now able to present data with complete coverage (in 2014: 14 countries).
Despite the fluctuating participation of a few countries with high frequency activities in ART, the reported treatment numbers in ART continue to rise (+9.4%, as compared to 2014) together with more children born (+7.3%, as compared to 2014). Although access to ART services is highly variable among European countries, the proportion of children born after ART continues to rise, particularly in those countries with optimal access to ART. In 2015 up to 6.6% of all newborn babies in Denmark (Supplementary Table SIV) were born after ART (in 2014: 6.4%).
When comparing the 2015 with the 2014 data sets, all treatment modalities in ART were used more frequently except IVM and FOR (Table I). Whereas the preponderance of ICSI over IVF seems to be stabilizing (Fig. 1), FER is becoming more and more important over fresh treatments and the treatment numbers of FER now exceed those of IVF. Since 2014, the elective freezing of all oocytes and embryos is being recorded systematically (Supplementary Tables SV and SVI): when comparing the 2014 and the 2015 data sets, the prevalence of freezing all embryos is on the rise, less so is freezing of all oocytes. Other treatment modalities with a rapidly gaining momentum are PGT and ED.
As in previous years, fewer embryos are now being replaced per treatment cycle. More and more treatments are being performed in which only one embryo is transferred, elective or not (37.7%, Fig. 2). Whereas the transfer of three or more embryos is rapidly disappearing in most countries, even the transfer of two embryos has become less prevalent in recent years (Fig. 2). SET is predominantly carried out in a few countries, the same as in previous years, and those countries are the ones with fewer multiple deliveries. Unfortunately, the same goes for the few countries in which three or more embryos are being transferred. Legal and financial constraints may be the main drivers for this practice (Gianaroli et al., 2016), but also attitudes among physicians and patients (Stormlund et al., 2019).
This impressive shift in the ET strategy has not yet translated into a major change in the number of multiple deliveries (Table IV). Whereas birth rates of triplets have been on the decline ever since the early recordings by the EIM Consortium, the incidence of twin deliveries has dropped to a much lesser extent. The proportion of premature deliveries of twins and triplets remained similar to previous years. The proportion of premature deliveries (<37 weeks) of singletons per ET has risen from 0.96% in 2006 to 1.77% in 2015 (Fig. 3). Singleton pregnancies after ART are prone to a higher risk of obstetric complications, including prematurity (Wennerholm et al., 2013; Sunkara et al., 2015; Qin et al., 2016), but pregnancy outcome does not depend on the number of retrieved oocytes (Magnusson et al., 2018).
Two cases of maternal death were reported in 2015, but the exact conditions under which these events occurred were not given (Supplementary Table SXVI). Other complications of ART, such as OHSS, infections and haemorrhage, remain prevalent at low frequencies. Foetal reduction for the prevention of multiple births is reported by 15 countries. All these numbers, however, most likely are under-reported.
Under-reporting of treatment numbers leads to overestimation of the efficacy of outcome of the offered treatments and at the same time to an underestimation of safety. The steady rise in ART activities in all European countries clearly demonstrates that ART has become an integral part of medical care and has a significant and measurable impact on society, and for that reason data on both efficacy and safety should therefore be of interest to all stakeholders, not least to the patients themselves. Data collection can only be optimized in the presence of good governance (De Geyter, 2019). Compulsory data collection systems have been shown previously to be more effective than voluntary systems: countries with voluntary registries provided more incomplete data sets due to partial reporting (Supplementary Table SIII). In addition, modern software systems enable prospective registration of cycle by cycle data sets instead of aggregate data, which are collected retrospectively. Currently, aggregate data submission by single ART institutions to the national registries is still the most commonly used method for reporting (Supplementary Table SIII). Coherent and systematic data registration and monitoring of all treatment outcomes should become mandatory in ART and must be considered as an indicator of excellent quality of care and good governance.
The instalment of prospective data registration is more and more urgent in light of the current rapid expansion of freezing technology, allowing the long-term storage of gametes, embryos and gonadal tissues (De Geyter et al., 2016). Infertility treatments are being segmented into small treatment units, for which the outcome cannot be reported within a 1-year period as was done in the past. Traditionally, the data collection organized and managed by the EIM Consortium is cross-sectional and based on annual data reporting. A concept for prospective follow-up of infertility treatment outcomes has been elaborated earlier (De Geyter et al., 2016). This would require the development of a European data collection software tool including an international coding system, with which the different therapeutic steps of infertile individuals and couples can be traced prospectively, even if they change the treating institution or their country of origin.
The organisation of data collection, as managed by EIM, must be further developed towards real surveillance and vigilance in ART (Kissin et al., 2019). Surveillance is defined by the continuous and systematic collection of health data (here related to ART and its outcome) needed for the analysis and interpretation of trends in medical care with a special focus on safety. That goal can best be achieved if data submission to the national registries becomes compulsory.
Practitioners, professional bodies, and national and European political bodies have a duty to realise that such therapies require appropriate logistical and financial support to set up national reporting electronic databases, ideally a pan-European centralised data collection (De Geyter et al., 2016), to monitor not only the efficiency and safety of therapy but also the long-term health of children born after treatment. The creation of a unique individual patient European coding system will ensure all aspects of an ever-increasing spectrum of ART care can be measured and analysed thus ensuring full surveillance and vigilance. The concept of evolving the current cross-sectional register towards prospective surveillance and vigilance of care in ART will take years to become a reality and will require top down support from national and supranational health care authorities. Such a concept can only be supported by all stakeholders of ART, including the patients, and should be motivated by the desire to provide care with excellence.
Supplementary Material
Appendix
Contact persons who are collaborators and represent the data collection programmes in participating European countries, 2015.
Albania
Prof. Orion Gliozheni, University Hospital for Obstetrics & Gynecology, Department of Obstetrics & Gynecology, Bul. B. Curri, Tirana, Albania. Tel: +355 4222 36 32; Fax: +355 42 257 688; Mobile: +355 68 20 29 313; E-mail: glorion@abcom.al
Armenia
Mr Eduard Hambartsoumian, Fertility Center, IVF Unit, 4 Tigvan Nets, 375 010 Yerevan, Armenia; Tel: +374 10 544 368; E-mail Hambartsoumian@hotmail.com
Austria
Prof. Dr Heinz Strohmer, Dr Obruca & Dr Strohmer Partnerschaft Goldenes Kreuz-Kinderwunschzentrum, Lazarettgasse 16–18, 1090 Wien, Austria. Tel: +43 401 111 400; Fax: +43 401 111 401; E-mail: heinz.strohmer@kinderwunschzentrum.at
Belarus
Dr Elena Petrovskaya (Alena Piatrouskaya), ART centre ‘Embryo’, Filimonova 53, 220053 Minsk, Belarus. Tel. +375 293 830 570; E-mail: elenaembryoby@gmail.com
Dr Oleg Tishkevich, Centre For Assisted Reproduction ‘Embryo’ Belivpul, Filimonova Str. 53, 220 114 Minsk, Belarus. Tel: +375 296 222 722; Fax: +375 172 376 404; Mobile: +375 296 222 722; E-mail: tishol@tut.by
Belgium
Dr Kris Bogaerts, I-Biostat, Kapucijnenvoer 35 bus 7001, 3000 Leuven, Belgium. Tel: +32 (0) 16 33 68 90; Fax: +32 (0) 16 33 70 15; E-mail: Kris.Bogaerts@med.kuleuven.be
Prof. Christine Wyns, Gynaecology-Andrology, Cliniques Universitaires Saint Luc, Service FIV-Andrology, Université Catholique de Louvain; Av. Hippocrate, 10, 1200 Brussels, Belgium. Tel: +32 27646576; Fax: +32 27649050; Mobile: +32 477943374; E-mail: christine.wyns@uclouvain.be
Bosnia
Professor Dr Devleta Balic, Zavod za humanu reprodukciju ‘Dr Balic’, Kojsino 25, 75 000 Tuzla, Bosnia–Herzegovina. Tel: +387 35 260 650, Mobile: +387 611 402 22; E-mail drbalic@bih.net.ba
Professor Dr Sanja Sibincic, Health Center Medico-S, Jevrejska 58/A, 78000 Banja Luka, Bosnia–Herzegovina. Tel: +387 512 321 00; Mobile: +387 655 159 42; E-mail sanjasibincic@gmail.com
Bulgaria
Irena Antonova, ESHRE certified clinical embryologist (2011), Ob/Gyn Hospital Dr Shechterev, 25–31, Hristo Blagoev Strasse, 1330 Sofia, Bulgaria. Tel: +359 887 127 651; E-mail: irendreaming@gmail.com
Cyprus
Dr Michael Pelekanos, AKESO Fertility Centre, 1, Pavlou Nirvana strasse, 3021 Limassol, Cyprus. Tel: +357 99645333; Fax: +357 25824477; Mobile +30 6944248433; E-mail: pelekanos@akeso.com
Czech Republic
Dr Karel Rezabek, Medical Faculty, University Hopsital, CAR-Assisited Reproduction Center, Gyn/Ob Departement, Apolinarska 18, 12000 Prague, Czech Republic. Tel: +420 224 967 479; Fax: +420 224 922 545; Mobile: +420 724 685 276; E-mail: krezabek@vfn.cz
Mgr. Jitka Markova, Institute of Health Information and Statistics of the Czech Republic, Palackeho namesti 4, 12801 Prague, Czech Republic. Tel: +420 224 972 832; Mobile: +420 721 827 532; E-mail: jitka.markova@uzis.cz
Denmark
Dr Josephine Lemmen, Vitanova, Fertility clinic, Vester Voldgade 106, 1552 Copenhagen, Denmark. Tel: +45 333 371 01; E-mail: jglemmen@gmail.com
Estonia
Dr Deniss Sõritsa, Tartu University Hospital and Elitre Clinic, Tartu, Estonia. Tel.: +372 740 9930; Fax: +372 740 9931; E-mail: soritsa@hotmail.com
Finland
Prof. Mika Gissler, THL National Institute for Health and Welfare, P.O.Box 30, 00271 Helsinki, Finland. Tel: +385 29524 7279; E-mail: mika.gissler@thl.fi
Dr Sari Pelkonen, Oulu University Hospital, Department of Obstetrics and Gynaecology, P.O. Box 23, 90 029 Oys, Finland. Tel:+358 83153040; E-mail sari.pelkonen@fimnet.fi
France
Dr Fabienne Pessione, Agence de la biomedecine, 1 av stade de France, 93 Saint Denis, France; Tel: +33 1 5593 69 46; E-mail: fabienne.pessione@biomedecine.fr
Prof. Jacques de Mouzon, 15–29 rue Guilleminot, 75014 Paris, France; Mobile: +33 662 062 274; Tel: +33 143 224 679; E-mail: jacques.de.mouzon@gmail.com
Germany
Dr Andreas Tandler—Schneider; Fertility Center Berlin; Spandauer damm 130; 14050 Berlin; Germany; Tel: +49 30 233 20 81 10; Fax: +49 30 233 20 81 19; E-mail: tandler-schneider@fertilitycenter-berlin.de
Greece
Prof. Sophia Kalantaridou; National Authority of Medically Assisted Reproduction, Ploutarxou 3, P.O. 10675 Athens; Tel: +30 213 2072000; E-mail: secretary@eaiya.gov.gr
Hungary
Prof. Janos Urbancsek, Semmelweis University, 1st Dept. of Ob/Gyn, Baross utca 27, 1088 Budapest, Hungary. Tel: +36 1266 01 15; Fax: +36 1266 01 15; E-mail: urbjan@noi1.sote.hu
Prof. G. Kosztolanyi, University of Pecs, Dept. of Medical Genetics and Child Development, Jozsef A.u;7., 7623 Pecs, Hungary. Tel: +36 72535977; Fax: +36 7 2535972; E-mail: gyorgy.kosztolanyi@aok.pte.hu
Iceland
Mr Hilmar Bjorgvinsson, IVF Klinikin Reykjavik, Alfheimum 74, 104 Reykjavik, Iceland. Tel: +354 430 4000; Fax: +354 430 4040; E-mail: Hilmar.bjorgvinsson@ivfklinikin.is
Ireland
Dr Edgar Mocanu, Human Assisted Reproduction Ireland Rotunda Hospital, HARI Unit, Master’s House, Parnell Square, 1 Dublin, Ireland. Tel: +353 180 72 732; Mobile: + 353 86 818 839; Fax: +353 18 727 831; E-mail: emocanu@rcsi.ie
Jennifer Cloherty, Galway Fertility, Western distribution Road, Rahoon, Ireland. Tel: 35361476800; E-mail: JCloherty@GFU.ie
Italy
Dr Giulia Scaravelli, Istituto Superiore di Sanità, Registro Nazionale della Procreazione Medicalmente Assistita, CNESPS, Viale Regina Elena, 299, 00161 Roma. Tel: +3906 499 04050; Fax: +39064 99 04 324; E-mail: giulia.scaravelli@iss.it
Dr Roberto de Luca, Istituto Superiore di Sanità, Registro Nazionale della Procreazione Medicalmente Assistita, CNESPS, Viale Regina Elena, 299, 00161 Roma. Tel: +3906 499 04320; E-mail: roberto.deluca@iss.it
Kazachtstan
Prof. Dr Vyacheslav Lokshin, The Urban Center of Human reproduction, Tole Be Street 99, 50012 Almaty, Kazakhstan. Tel: +7 727 234 3434; Fax: +7 727 264 66 15; Mobile: +7 701 755 8209; E-mail: vyacheslav.lokshin@ipsen.kz
Dr Sholpan Karibayeva, The Urban Center of Human reproduction, Tole Be Street 99, 50012 Almaty, Kazakhstan. Tel: +7 727 237 2118; E-mail: sh.karibaeva@gmail.com
Latvia
Dr Valeria Magomedova, Jusu Arsti Private Clinic, Apuzes 14, 1046 Riga, Latvia. Tel: +371 678 700 29; Fax: +371 678 704 29; E-mail: godunova@inbox.lv
Lithuania
Raminta Bausyte, Vilnius University Hospital Santaros Clinics, Santaros Fertility Center, Simono Staneviciaus 64–69, 07113 Vilnius, Lithuania. Tel: +370 620 86826, Email: raminta.bausyte@gmail.com
Ieva Masliukaite, Academic Medical Center, Cener for Reproductive Medicine, Ijburglaan, 1086ZJ Amsterdam, The Netherlands; Tel: +31 653 688 815; E-mail: i.masliukaite@amc.uva.nl
Macedonia
Mr Zoranco Petanovski, Hospital ReMedika, Nas. Zelezara, 1000 Skopje, Macedonia. Tel: +389 224 475 45; Fax: +389 226 031 00; E-mail: zpetanovski@yahoo.com
Malta
Dr Jean Calleja-Agius, University of Malta, 12, Mon Nid, Gianni Faure Street, TXN2421 Tarxien, Malta. Tel: +356 216 930 41; Mobile: +356 995 536 53; E-mail: jean.calleja-agius@um.edu.mt
Moldova
Prof. Dr Veaceslav Moshin, Medical Director at Repromed Moldova, Center of Mother @ Child Protection, State Medical and Pharmaceutical University ‘N.Testemitanu’, Bd. Cuza Voda 29/1, Chisinau, Republic of Moldova. Tel: +37322 263855; Mobile: +37369724433; E-mail: mosin@repromed.md; veaceslavmoshin@yahoo.com
Montenegro
Dr Tatjana Motrenko Simic, Human Reproduction Center Budva, Prvomajska 4, 85310 Budva, Montenegro, Tel.: +382 33402432; Mobile: +382 69 052 331; E-mail: motrenko@t-com.me
Dragana Vukicevic, Hospital ‘Danilo I’, Humana reprodukcija, Vuka Micunovica bb, 86000 Cetinje, Montenegro. Tel: +382 675 513 71; E-mail: vukicevic.dragana@yahoo.com
The Netherlands
Dr Jesper M.J. Smeenk, St Elisabeth Hospital Tilburg, Dept. of obstetrics and Gynaecology, Hilv, The Netherlands. Tel: +31 13 539 31 08; Mobile: +31 622 753 853; E-mail: j.smeenk@elisabeth.nl,
Norway
Dr Liv Bente Romundstad, Spiren Fertility Clinic, Nardoskrenten 11, 7032 Trondheim, Norway. Tel: +47 73523000; Mobile: +47 90550207; E-mail libero@klinikkspiren.no
Poland
Dr Anna Janicka, VitroLive, Kasprzaka 2A, 71-074 Szczecin, Poland. Tel: +48 226 543 525; E-mail: anna.janicka@vitrolive.pl
Portugal
Prof. Dr Carlos Calhaz—Jorge, CNPMA, assembleia da Republica, Palacio de Sao Bento, 1249-068 Lisboa, Portugal. Tel: +351 21 391 93 03; Fax: +351 21 391 75 02; E-mail: calhazjorgec@gmail.com
Ms Ana Rita Laranjeira, CNPMA, Assembleia da Republica, Palaio de Sao Bento 1249-068 Lisboa, Portugal, Tel: +351 21 391 93 03; Fax: +351 21 391 75 02; E-mail: cnpma.correio@ar.parlamento.pt
Romania
Mrs Ioana Rugescu, Gen Secretary of AER Embryologist association and Representative for Human Reproduction Romanian Society. Tel: +40744500267; E-mail: irugescu@rdsmail.ro
Dr Bogdan Doroftei, Univ. of Medicine and Pharmacy Iasi; Teaching Hospital Obgyn ‘Cuza Voda’; Cuza Voda Str. 34; 700038 Iasi; Romania. Tel: +40 232 213 000/int. 176; Mobile: +40 744 515 297; E-mail bogdandoroftei@gmail.com; bogdan.doroftei@umfiasi.ro
Russia
Dr Vladislav Korsak, International Center for Reproductive Medicine, General Director, Liniya 11, Building 18B, Vasilievsky Island, 199034 St-Petersburg, Russia C.I.S. Tel: +7 812 328 2251; Fax: +7 812 327 19 50. Mobile: +7921 9651977; E-mail: korsak@mcrm.ru
Serbia
Prof. Nebojsa Radunovic, Institute for Obstetrics and Gynecology,Visegradska 26, 11000 Belgrade, Serbia. Tel: +38 111 361 55 92; Fax: +38 111 361 56 03; Mobile: +381 63 200 204; E-mail: radunn01@gmail.com
Dr Sci. Nada Tabs, Klinika za ginekologiju i akuserstvo, Klinicki centar Vojvodine, Branimira Cosica 37, 21000 Novi Sad, Serbia. Mobile: +381 63 50 81 85; E-mail: nada.tabs@yahoo.com
Slovenia
Dr Irma Virant-Klun, University Medical Centre Ljubljana, Departement of Obstetrics and Gynecology, Slajmerjeva 3, 1000 Ljubljana, Slovenia. Tel: +386 1522 60 13; Fax: +386 1431 43 55; Mobile:+38631625774 E-mail: irma.virant@kclj.si
Spain
Mrs Irene Cuevas Saiz, Hospital General de Alicante, Infertility Dept., Av Pintor Baeza, 12, 03010 Valencia, Spain; Tel: +34 961972000; Fax: +34 91 799 4407; Mobile: 0034677245650; E-mail: cuevas_ire@gva.es
Dr Fernando Prados Mondéjar, Hospital de Madrid-Montepríncipe, HM Fertility Center Monteprincipe, C/Montepríncipe 25, 28660 Boadilla del Monte, Spain; Tel: +34 917 089 931; Mobile: +34 646 737 237; E-mail: fernandojprados@gmail.com
Sweden
Prof. Christina Bergh, Sahlgrenska University Hospital, Department of Obstetrics and Gynaecology, Bla Straket 6, 413 45 Göteborg, Sweden. Tel: +4631 3421000, +46736 889325; Fax: +4631 418717; Mobile: +46 736 889325; E-mail Christina.bergh@vgregion.se
Switzerland
Dr Elisabeth Berger-Menz, Kinderwunschpraxis Berger, FMH Gyn/GH, Brembartenstrasse 119, 3012 Berne, Switzerland. Tel: +41 31 305 84 17; E-mail: praxis@berger-gyn.ch
Ms Maya Weder, Administration FIVNAT, Postfach 754, 3076 Worb, Switzerland. Tel: +41 (0)31819 76 02; Fax: +41 (0)31819 89 20; E-mail: fivnat@bluewin.ch
UK
Mr Howard Ryan, Data Analyst H.F.E.A, 10 Spring Gardens, London SW1A 2BU, UK. Tel: +44 (0)207291 8203; E-mail: Howard.Ryan@HFEA.GOV.UK
Mr Richard Baranowski, Deputy Information Manager, Human Fertilization and Embryology Authority (HFEA), Finsbury Tower, 103–105 Bunhill Row, London EC1 Y 8HF, UK. Tel: +44 (0) 20 7539 3329; Fax: +44 (0) 20 7377 1871; E-mail: Richard.baranowski@hfea.gov.uk
Ukraine
Professor Dr Mykola Gryshchenko, IVF Clinic Implant Ltd, Academician V.I.Gryshchenko Clinic for Reproductive Medicine, 25 Karl Marx Str., 61 000 Kharkiv, Ukraine. Tel: +380 57 124522; Fax: +380 57 705070703; Mobile +380 57 705070703; E-mail: nggryshchenko@gmail.com
EIM Committee 2017–2019: chairman: C.D.; chairman elect: C.W.; past chairman: C.C-J. members: M.K., E.M., T.M., G.S., J.S. and S.V.. V.G. is a science manager at ESHRE Central Office, Brussels. See also Appendix for contributing centres and contact persons representing the data collection programmes in the participating European countries.The main results of this report were presented at the annual ESHRE congress in Barcelona, July 2018
Contributor Information
The European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE):
Orion Gliozheni, Eduard Hambartsoumian, Heinz Strohmer, Elena Petrovskaya, Oleg Tishkevich, Kris Bogaerts, Christine Wyns, Devleta Balic, Sanja Sibincic, Irena Antonova, Michael Pelekanos, Karel Rezabek, Jitka Markova, Josephine Lemmen, Deniss Sõritsa, Mika Gissler, Sari Pelkonen, Fabienne Pessione, Jacques de Mouzon, Andreas Tandler—Schneider, Sophia Kalantaridou, Janos Urbancsek, G Kosztolanyi, Hilmar Bjorgvinsson, Edgar Mocanu, Jennifer Cloherty, Giulia Scaravelli, Roberto de Luca, Vyacheslav Lokshin, Sholpan Karibayeva, Valeria Magomedova, Raminta Bausyte, Ieva Masliukaite, Zoranco Petanovski, Jean Calleja-Agius, Veaceslav Moshin, Tatjana Motrenko Simic, Dragana Vukicevic, Jesper M J Smeenk, Liv Bente Romundstad, Anna Janicka, Carlos Calhaz—Jorge, Ana Rita Laranjeira, Ioana Rugescu, Bogdan Doroftei, Vladislav Korsak, Nebojsa Radunovic, Nada Tabs, Irma Virant-Klun, Irene Cuevas Saiz, Fernando Prados Mondéjar, Christina Bergh, Elisabeth Berger-Menz, Maya Weder, Howard Ryan, Richard Baranowski, and Mykola Gryshchenko
Authors’ roles
V.G. performed the calculations. C.D.G. wrote the manuscript. All other co-authors reviewed the final manuscript and made appropriate corrections and suggestions to improve it. In all, this document represents a fully collaborative work.
Funding
The study did not receive any external funding. All costs were covered by ESHRE.
Conflict of interest
There are no competing interests.
References
- De Geyter C, Wyns C, Mocanu E, de Mouzon J, Calhaz-Jorge C. Data collection systems in ART must follow the pace of change in clinical practice. Hum Reprod 2016;31:2160–2163. [DOI] [PubMed] [Google Scholar]
- De Geyter C, Calhaz-Jorge C, Kupka MS, Wyns C, Mocanu E, Motrenko T, Scaravelli G, Smeenk J, Vidakovic S, Goossens Vet al. . ART in Europe, 2014: results generated from European registries by ESHRE: the European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod 2018;33:1586–1601. [DOI] [PubMed] [Google Scholar]
- De Geyter C Assisted reproductive technology: impact on society and need for surveillance. Best Pract Res Clin Endocrinol Metab 2019;33:3–8. [DOI] [PubMed] [Google Scholar]
- De Rycke M, Goossens V, Kokkali G, Meijer-Hoogeveen M, Coonen E, Moutou C, ESHRE PGD . Consortium data collection XIV-XV: cycles from January 2011 to December 2012 with pregnancy follow-up to October 2013. Hum Reprod 2017;32:1974–1994. [DOI] [PubMed] [Google Scholar]
- European IVF-monitoring Consortium (EIM), European Society of Human Reproduction and Embryology (ESHRE), Calhaz-Jorge C, De Geyter C, Kupka MS, de Mouzon J, Erb K, Mocanu E, Motrenko T, Scaravelli Get al. . Assisted reproductive technology in Europe, 2013: results generated from European registers by ESHRE. Hum Reprod 2017;32:1957–1973. [DOI] [PubMed] [Google Scholar]
- Gianaroli L, Ferraretti AP, Magli MC, Sgargi S. Current regulatory arrangements for assisted conception treatment in European countries. Eur J Obstet Gynecol Reprod Biol 2016;207:211–213. [DOI] [PubMed] [Google Scholar]
- Kissin DM, Adamson GD, Chambers G, De C (eds). Assisted Reproductive Technology Surveillance. Cambridge: Cambridge University Press, 2019 [Google Scholar]
- Magnusson Å, Wennerholm UB, Källén K, Petzold M, Thurin-Kjellberg A, Bergh C. The association between the number of oocytes retrieved for IVF, perinatal outcome and obstetric complications. Hum Reprod 2018;33:1939–1947. [DOI] [PubMed] [Google Scholar]
- Qin J, Liu X, Sheng X, Wang H, Gao S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril 2016;105:73–85. [DOI] [PubMed] [Google Scholar]
- Stormlund S, Schmidt L, Bogstad J, Løssl K, Prætorius L, Zedeler A, Pinborg A. Patients’ attitudes and preferences towards a freeze-all strategy in ART treatment. Hum Reprod 2019;34:679–688. [DOI] [PubMed] [Google Scholar]
- Sunkara SK, La Marca A, Seed PT, Khalaf Y. Increased risk of preterm birth and low birthweight with very high number of oocytes following IVF: an analysis of 65 868 singleton live birth outcomes. Hum Reprod 2015;30:1473–1480. [DOI] [PubMed] [Google Scholar]
- Wennerholm UB, Henningsen AK, Romundstad LB, Bergh C, Pinborg A, Skjaerven R, Forman J, Gissler M, Nygren KG, Tiitinen A. Perinatal outcomes of children born after frozen-thawed embryo transfer: a Nordic cohort study from the CoNARTaS group. Hum Reprod 2013;28:2545–2553. [DOI] [PubMed] [Google Scholar]
- Zegers-Hochschild F, Adamson GD, Dyer S, Racowsky C, de Mouzon J, Sokol R, Rienzi L, Sunde A, Schmidt L, Cooke IDet al. . The international glossary on infertility and fertility care, 2017. Hum Reprod 2017;32:1786–1801. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.