

Abstract
The purpose of the study was to examine the concurrent and construct validity of a new perceptual scale to control the exercise intensity using elastic bands (Resistance Intensity Scale for Exercise; RISE) in the elderly. Twenty-six participants underwent two sessions consisting of 4 exercises. The participants performed three sets of 15 repetitions per exercise of either low, medium, or high intensity. The criterion variables were heart rate and applied force (mean and peak). Following the final repetition of each set, active muscle (AM) and overall body (OB) ratings of perceived exertion (RPE) were collected from RISE and the OMNI-Resistance Exercise Scale of perceived exertion with elastic bands (OMNI-RES EB). Construct validity was established by correlating the perceptual score obtained from both scales, RISE and OMNI-RES EB. Significant (p ≤ 0.05) and positive linear relationships between both scales were found (RPE-AM R2 = 0.90; RPE-OB R2 = 0.77). Significant differences in heart rate, applied force, and RISE scores were observed between the sets of the three intensities. For all 4 analyzed exercises, high-intensity sets elicited higher heart rate, applied force, and perceptual scores compared with the medium- and low-intensity sets. Furthermore, the medium-intensity sets produced higher perceptual, physiologic, and performance responses than the low-intensity sets. Intersession reliability was 0.88 for heart rate, 0.94 and 0.95 for applied force, 0.88 for the RPE-AM, and 0.80 for the RPE-OB. Conclusion: The RISE scale can be considered a valid method for assessing the perceived exertion during resistance exercises performed with elastic bands in the elderly.
Key points.
Older adults can use the RISE scale to verbally rate (easy to maximal) their perceptions of effort during both upper- and lower-body exercises using elastic bands.
RISE scale can be used in older adults without reducing the accuracy of the training load dosage prescribed during training/rehabilitation sessions and while carrying out medium- or long-term periodized strength-training programs or therapeutic interventions.
Compared with previous scales, RISE is a more sensitive because can discriminate between medium and low intensities of overall body ratings of perceived exertion in the elderly.
Key words: Heart rate, applied force, variable resistance, prescribing exercise intensity
Introduction
Among the different resistance-training devices, elastic bands are a scientific, affordable, easy-to-use option (Aboodarda et al., 2016; de Oliveira et al., 2017; Soria-Gila et al., 2015), which has shown to be as effective as traditional resistance training for improving strength (Behm, 1991). Exercise with elastic bands facilitates the use of different levels of resistance (variable resistance) by modifying the length over which the band is stretched for a given range of motion (Soria-Gila et al., 2015). Well-designed elastic band based exercise programs resulted in increased strength, improved performance in conducting daily activities, independence, and quality of life in older adults (OA) (Delmonico et al., 2007; Mally et al., 2011; Martins et al., 2013; Romero-Arenas et al., 2011; Rieping et al., 2019; Rossi et al., 2017).
Monitoring exercise intensity is an important factor to ensure the safety and efficacy of resistance training in any context of its application, whether used by athletes or in recreational or therapeutic settings (Robertson, 2004). Scales estimating the rating of perceived exertion (RPE) have been successfully used to (a) prescribe training intensities, (b) guide daily training dosages, and (c) track training progress (Gearhart et al., 2009). The use of RPE scales is based on an assumed functional link between the observed physiological, perceptual, and performance responses that according to the basic tenet of Borg’s Effort Continua Model, occurs simultaneously when performing physical activities with increases in the intensity of physical activity performance (Borg, 1982). The aforementioned responses have been analyzed separately or in combination to monitor exercise intensity in recreationally trained athletes (Chapman et al., 2019; Lagally et al., 2002) and active OA (Morishita et al., 2019). RPE scales that combine verbal and visual descriptors could result in a better monitoring of the intensity during physical training activities, because combination of different sensory modalities can be necessary in cases where a single sensory or perception modality could provoke an ambiguous or incomplete result (Lalanneab and Lorenceaua, 2004; Small and Prescott, 2005). In consequence, studies that validate cross-modal perception RPE scales are needed for a proper application, even more when different pictorial, numerical, and/or verbal descriptors for specific exercise modes or type of population are used (Mays et al., 2010).
In order to establish concurrent validity of a new category scale to measure perception of physical exertion, one must correlate a criterion or stimulus variables (i.e., physiological and/or performance parameters, as for example heart rate or total weight lifted), with a concurrent or response variable (i.e., RPE from a previously validated scale) (Lagally and Robertson, 2006). Applied force and heart rate has been used in previous studies with different type of participants as a criterion variable to validate a perceived exertion metric (Colado et al., 2012b; 2014; 2018; Robertson et al., 2003; 2005). It should also be considered that when exercising, it is possible to differentiate between a global and peripheral exertional signal. Thus, RPE can be differentiated between anatomically regionalized perceptual signals that are associated with total body effort perception and active limbs as well as the chest and breathing (Colado et al., 2012b; 2014; 2018; Robertson et al., 2003; 2005). The RPE for active muscles (RPE-AM) is usually higher than the RPE for overall body (RPE-OB). It has been demonstrated that measurement of the RPE-AM increases the precision of perceptually based intensity self-regulation during the resistance exercises (Robertson et al., 2003). Both types of exertional perceptions provide useful information for prescription and intensity monitoring purposes (Robertson, 2004).
The application of different intensities during elastic resistance training can be monitored by associating the target number of repetitions, that is specific to a determinate training stimulus, with the width of the grip using and the resulted RPE score expressed at the end of the set (Colado and Triplett, 2008). Explained in greater detail, this means that the exerciser will firmly hold the elastic band estimating the grip width associated with the previously determined number of repetitions, which will be adjusted to the objective of the training and the corresponding local muscular fatigue rating expressed at the end of the set. If participants completed the prescribed repetitions expressing higher perceptual rating than prescribed, they were asked to use a wider grip or change the band according with the requested level of effort. Conversely, a narrowed grip or a “harder” band was used if the participants expressed a lower perceptual rating that prescribed (Colado et al., 2009; 2010; 2012a).
Colado et al. (2012b) validated the modified version of the OMNI-Resistance Exercise (OMNI-RES) scale by Robertson et al (2003) which was specifically designed to assess the perception of effort in young resistance-trained males during elastic band resistance exercises. A few years later, the same research group validated a new perceptual scale, including specific verbal descriptors for monitoring the intensity of the perceptual signal of exertion when exercising with this type of elastic devices (Colado et al., 2014). This approach was expected to be more broadly applicable to a wider range of the population, for example, those who have difficulty using the classical numerical category scales (Rogers, 2006; Tabbers et al., 2004). According to Revilla et al. (2014) and Weijters et al. (2010), it must be highlighted that: (i) Scales with more of five levels or categories are less recommended because decrease the quality of the perception; (ii) Scales without a midpoint must be avoided; (iii) 5-point scales are better for being applied in general population; and (iv) 5-point scales can improve the accuracy in the linear models of interpretation of the information than 3-points scales, thus the 5-point scales providing higher criterion validity.
Over the years, the scale validated by Colado et al. (2012b) was applied in different populations for whom it was not initially validated (i.e., young, healthy, physically active men), as, for example, is the case for OA (Chupel et al., 2017; Gargallo et al., 2018; Gómez-Tomás et al., 2018; Fritz et al., 2018; Fukuchi et al., 2016; Li et al., 2017; Rieping et al., 2019; Smith et al., 2017). Indeed, more recently, Colado et al. (2018) validated the application of the aforementioned scale for use with OA because strength tracking using RPE may be particularly beneficial for this population (Gearhart et al., 2009). However, the scale with verbal descriptors has not yet been validated for application in populations different from that originally used by Colado et al. (2014) (i.e., young, healthy, physically active men), despite have being used with positive results in recent long-term resistance training studies with different populations, including older people (Muntaner-Mas et al., 2017; Picha et al., 2017; Tada, 2018; Texeira et al., 2016; Wasser et al., 2017). Griep et al. (1998) suggested that older and young individuals differ in their willingness and ability to express their experience, and even this could be influenced when there are a wider number of available responses in combination with a complex variety both in the distribution and in the presentation of stimulus intensities. Guidetti et al. (2011) pointed out that: (i) Perceived exertion can be considered a cognitive function that reflects the progressive aging process; (ii) Cognitive decline associated with aging could be a factor that affects the ability to consistently assign numbers to words or even pictures when attempting to describe exercise-related feelings. Griep et al. (1998) pointed out that for OA is difficult using scales for matching their perceptions due to certain limitations in terms of comprehension, vision, memory and concentration. Although OA could respond much easier on a well bounded and labeled graphic rating scale (Griep et al., 1998), as for example this could be the case of the scale validated by Colado et al. (2014). Consequently, to ensure OA’s correct use of the pictorial scale proposed by Colado et al. (2014), it should be validated in this specific type of population.
Therefore, the purposes of this investigation were (i) to assess the construct validity of the Resistance Intensity Scale for Exercise (RISE) with TheraBand elastic bands during resistance exercises performed by older people (>60 years); (ii) to examine the concurrent validity of the RISE scale during elastic resistance exercises performed by OA by means of to examine the effect of three different resistance exercise intensities on reported perceptual response, heart rate, and applied force; and (iii) to corroborate the scores reliability that RISE Scale provided when is employed for quantifying the intensity of the elastic resistance training in different sessions performed by OA. It was hypothesized that (i) RISE scale could be used for monitoring intensity during elastic resistance exercises performed by OA in the same way that the OMNI-RES EB has been used so far; and (ii) The RPE-AM obtained with the RISE scale will be higher than RPE-OB during elastic resistance exercises performed by OA.
Methods
Study design
The investigation used a cross-sectional, perceptual estimation design consisting of one familiarization and two experimental trials. During the session of familiarization, the participants were instructed on how to use both the OMNI-RES EB scale (Figure 1) and the RISE scale (Figure 2). According to Colado and Triplett (2008), Colado et al., (2012b) and Newsam et al. (2005), they also were asked to establish the grip width on the elastic band with which they would perform 15 maximum repetitions (RM) for the 4 prescribed exercises (i.e., shoulder abduction [SA] and elbow flexion [EF], abduction of the hip [AH], and extension of the hip [EH]). These selected exercises were the same as used in previous validation studies (Colado et al., 2012b; 2014; 2018) and commonly prescribed in OA population (Chupel et al., 2017; Fritz et al. 2018; Gargallo et al., 2018; Rieping et al., 2019). The following two assessment sessions were used to analyze the concurrent and construct validity along with the reliability of the RISE scale in the elderly. All dependent variables (RPE-AM and OB scores, applied force, and heart rate) were measured during all exercise sets performed at the three analyzed intensities (low, medium, and high).
Figure 1.
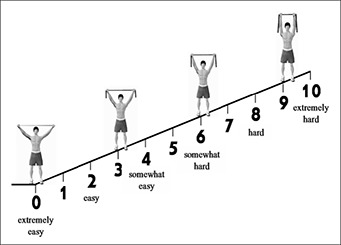
OMNI-Resistance Exercise Scale of perceived exertion with TheraBand resistance bands.
Figure 2.
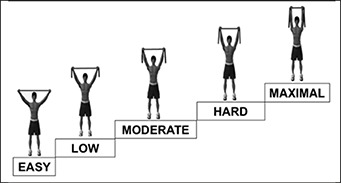
Resistance Intensity Scale for Exercise (RISE) with TheraBand elastic bands.
Participants
Sample size was determined using G* Power 3.1 software (Faul et al., 2009). The calculation indicated a sample size of 26 volunteers to meet a power of 0.80, α = 0.05, correlation coefficient of 0.5, nonsphericity correction of 1, and moderate effect size. This prior analysis was performed to reduce the probability of type II error by determining the minimum number of participants required to reject the null-hypothesis at the p < 0.05 level of confidence (Beck, 2013). Thus, twenty-six participants (5 men and 21 women; 67.21 ± 4.99 years old; body mass index 27.74 ± 2.96 kg/m2) volunteered to participate. Only participants with a minimum of 6 months of regular physical activity using elastic bands with a minimum frequency of twice per week were accepted as eligible to participate.
Participants taking performance-enhancing drugs at the time of the experiment or who were suffering musculoskeletal pain, or any neuromuscular and cardiovascular disorder were excluded. During the assessment sessions, participants were instructed to refrain from any nonexperimental hard exercises, maintain normal dietary habits, and abstain from alcohol, caffeine, and nicotine for at least 24 hours before the testing session. Before being considered, all participants were informed about the purpose, procedures, benefits, risks, and discomfort that might result from participation in the present study. All participants were retirees and voluntarily agreed to participate; each provided informed consent and were free to withdraw from the study at any time. All applied procedures were in accordance with the requirements listed in the 1975 Declaration of Helsinki and its amendment in 2008, and all experimental protocols were approved by the Ethics Committee of the University of Valencia (Spain) (H1464018006594). Data reported in the present study form a portion of a wide research project investigating the validation of scales for monitoring intensity during elastic resistance training in different types of participants. Some previous data from this project have already been published (Colado et al., 2018).
Familiarization session
Even though all the participants were well familiarized with the use of the OMNI-RES EB scale, because they have used it during previous training workouts, all of them attended the laboratory to: (i) become familiarized with the correct exercise execution; and (ii) review the proper application of both scales (OMNI-RES EB and RISE) associated with low and high numerical along with the word categories as scale anchor points were provided. Participants carried out two different orientation protocols, namely, high and low intensity. The high- and low-intensity protocols were used to anchor each particular exercise with the corresponding ratings of perceptual responses expressed with both the OMNI-RES EB scale and the RISE scale. The high-intensity protocol was carried out first. The participants provided a value of the experienced perceptual response after the completion a set of 15RM. Participants were instructed that the RPE-AM at that time corresponded to a rating of “10” on the OMNI-RES scale or “Maximal” on the RISE scale. During the low-intensity protocol, the participants performed a single repetition with a grip width that allowed the elastic band to tighten only very slightly at the end of the range of movement. It was explained to participants that RPE-AM at that time corresponded to a rating of “0” on the OMNI-RES scale or “Easy” on the RISE scale. The 15RM values were used to set the low and medium intensities thereafter used in the experimental session. The participants were not informed of the results of the 15RM assessment and were not aware of the intensities used during the experimental session until they had completed the experiment. They were instructed to use the correct exercise technique for each exercise, avoiding nonstandard movement, using the elastic band (TheraBand®; Hygenic Corporation, Akron, OH, USA). The exercises were performed using the dominant limbs (kick leg and throwing arm). In addition, the grip width associated with the 15RM was also determined (Colado et al., 2012b). Thus, for determining the 15RM overload, the participants performed several sets of each exercise until they were able to accurately identify the 15RM load adjusting the grip width, with 3 minutes of recovery between each failed attempt (Colado et al., 2018).
Experimental sessions
Two identical measurement sessions separated by 48 hours and at the same time of day to avoid diurnal variations were conducted. After a standardized warm up, the participants performed 1 set of 15 low-intensity repetitions, 1 set of 15 medium-intensity repetitions, and 1 set of high-intensity repetitions with 15RM. During the low-intensity set, the participants carried out the elastic band exercises using a grip width of +50% over the width corresponding to the previously determined 15RM. For the medium-intensity set, the exercise was performed with a grip width of +25% of that used for the high-intensity set. Each of the three assessed intensities was used for each singular exercise: SA, EF, EH, and AH. The order of the exercises, intensities and RPE rating for both scales was counterbalanced and randomized. Based on the participants’ experience in training with elastic bands, the workout configuration (only one set of each exercise was performed arriving to maximum fatigue) and the fact that longer recovery times (> 2 min) have been associated to extremely long-workouts durations, a 2-minute rest between sets was considered (Gearhart et al., 2009; 2011). The sequence assigned to each participant was the same for the two experimental sessions. All participants performed a total of 12 sets. At the end of each set, the level of applied force and heart rate were measured. In addition, participants were asked to report both the RPE-AM and RPE-OB perceived during the concentric phase immediately after the completion of the final repetition of each set (Robertson et al., 2003). Accordingly, simultaneous perceptual scores from both the OMNI-RES EB scale and letters from the RISE scale were assessed. Both scales were in clear view to the participants during the entire sessions. Participants were permitted to drink water ad libitum at all times. The laboratory temperature was maintained at 20°C. The measurement protocols were always strictly controlled by the same researchers following each one of the specific points highlighted in the procedures explained in the methods section.
Description of exercises and execution protocol
The range of movement for the two upper-limb exercises (SA and EF) was set from a position at which the hand was touching the hip to 90 degrees for the SA and to 135 degrees for the EF. For the two lower-limb exercises (AH and EH), the range of movement was set from a standing position (aligned feet shoulder-width apart) to 45 degrees for EH and to 30 degrees for AH. Joint angles were set using a manual goniometer (Baseline®. New York, USA). The range of colors used in the upper-limb exercises was from red to blue on the SA and from blue to gold on the EF; the range of colors used in both lower extremities exercises was from black to gold + black combined. A digital metronome set at 70 beats/min during the experimental session paced the repetition speed to ensure that the different exercises and sets were always performed at a standardized pace. Participants were asked to perform each repetition in a 2-count-up, 2-count-down pattern. Therefore, 1 repetition was performed for every 4 beats of the metronome. Each repetition lasted for approximately 3½ seconds (Colado et al., 2018).
Heart rate measurement
Heart rate monitors (Polar FT1, Polar Electro, Tampere, Finland) were attached around the chests of the participants. The heart rate value was collected immediately after the completion of the last repetition of every set.
Applied force measurement
A S-shaped load cell (Isocontrol; ATE micro, Madrid, Spain) was used to measure the applied force/weight (in kg). It is known that a load cell is a suitable instrument to quantify the variable resistive forces associated with elastic bands since there were no significant differences in force outputs between it and the force plate measurements (McMaster et al., 2010). The elastic band was attached to one side of the cell, which converted the force applied by the participants during the concentric phase into a measurable electrical output sent to a computer. Due to progressive resistance created by the elastic band trough the full range of motion of each exercise, peak and mean applied force value of the last concentric phase of the final repetition of each of the three intensities of each of the exercises performed were identified and recorded for further analysis.
Statistical analyses
Statistical analyses were performed using commercial software (SPSS, version 24.0; SPSS Inc., Chicago, IL). All variables were initially checked for normality using Kolmogorov-Smirnov test. Results are reported as mean and standard deviation (SD). A three-way (exercise [SA, EF, EH, and AH] intensity [high, medium, and low] RPE type [RPE-AM and RPE-OB]) analysis of variance (ANOVA) was performed to determine the possible influence of each one of the intensities (as a function of the different grip width of the elastic band) on the applied force (mean and peak), heart rate and RISE scale scores. An overall together perception from the scores of all the exercises performed was also analyzed for showing complementary information. In the event of significant main effects or interactions, planned pairwise comparisons were made using the Bonferroni post hoc analysis to test for differences. Chi-square test (χ2) was applied to examine the differences of the RPE-AM and RPE-OB for the RISE scale from the different corporal regions analyzed (i.e. between upper-limb exercises; between lower-limb exercises; and between upper-limb and lower-limb exercises). Construct validity was determined for RPE-OB and AM, using categorical linear regression analysis, with the RPE of the OMNI-RES EB scale as a predictor for the RISE scale. Regression equations were obtained from the categorical linear regression analysis between the criterion and conditional scales from rating of perceived exertion. That is regression equations were determined to predict an RPE on the OMNI-RES EB scale from an RPE derived from the RISE Scale. The analysis assigned a numerical value to each of the words of the RISE scale: Easy = 1; Low = 2; Moderate = 3; Hard = 4; Maximal = 5. These regression equations were undertaken separately for each of the exercises analyzed. Finally, the reliability of the applied force, heart rate, and RISE scale score measures were assessed by means of an intraclass correlation coefficient (ICC). The level of significance was set at P ≤ 0.05 before Bonferroni correction.
Results
Table 1 shows the mean (SD) values of the applied force measured at the three assessed intensities. There were significant differences in the response of the applied force generated as a function of the grip width of the elastic band (i.e., different intensities) for the mean and peak values: (i) SA, F (5, 120) = 159.57, p = 0.00, n2 = 0.87; (ii) EF, F (5, 120) = 138.85, p = 0.00, n2 = 0.85; AH, F (5, 120) = 199.17, p = 0.00, n2 = 0.89; EH, F (5, 120) = 344.12, p = 0.00, n2 = 0.93. The posteriori multiple comparison analysis found no significant differences between medium and low intensities for the upper-limb exercises (SA: p = 0.45, 95% confidence interval [CI] [–0.21, 1.23]; EF: p = 0.38, 95% CI [–0.46, 2.97]).
Table 1.
Differences in applied force and heart rate between intensities.
| High intensity | Medium intensity | Low intensity | ||
|---|---|---|---|---|
| Applied force | ||||
| Shoulder abduction | Mean | 1.26 (0.55)* | 0.83 (0.39)** | 0.56 (0.31) |
| Peak | 4.66 (1.11)* | 3.86 (0.98) | 3.35 (1.51) | |
| Elbow flexion | Mean | 3.78 (1.11)* | 2.66 (0.95)** | 1.73 (0.80) |
| Peak | 9.91 (1.92)* | 7.89 (1.77) | 6.63 (2.83) | |
| Hip abduction | Mean | 2.86 (1.69)* | 1.23 (0.77)** | 0.33 (0.35) |
| Peak | 11.44 (3.38)* | 7.16 (2.19)** | 3.32 (2.08) | |
| Hip extension | Mean | 5.34 (2.17)* | 2.77 (1.15)** | 1.16 (0.52) |
| Peak | 17.54 (3.43)* | 12.36 (2.39)** | 8.00 (2.07) | |
| Heart rate | ||||
| Shoulder abduction | 105.04 (15.96)* | 100.04 (15.11)† | 97.87 (14.19) | |
| Elbow flexion | 105.71 (14.94)* | 100.83 (15.19)** | 96.08 (14.05) | |
| Hip abduction | 107.17 (15.13)* | 100.37 (13.96)** | 97.42 (13.60) | |
| Hip extension | 107.87 (16.93)* | 101.08 (14.92)** | 96.79 (14.35) | |
Data are expressed as mean (standard deviation) of the different intensities (i.e., different grip widths). Applied force: kilograms for the peak and mean values obtained during the 15 repetitions at the different intensities; heart rate: beats per minute at just end of the 15 repetitions at the different intensities.
* Very significant differences (p ≤ 0.001) with medium and low intensities.
** Very significant differences (p ≤ 0.001) with low intensities.
† Significant differences (p < 0.05) with low intensities.
Heart rate
Table 1 shows the mean (SD) values of the heart rate measured at the three assessed intensities. Statistically significant differences were observed in the heart rate response generated as a function of the grip width used (i.e., different intensities) in all exercises: (i) SA, F (2, 46) = 33.73, p = 0.00, n2 = 0.59; (ii) EF, F (2, 46) = 47.27, p = 0.00, n2 = 0.67; AH, F (2, 46) = 41.69, p = 0.00, n2 = 0.64; EH, F (2, 46) = 35.27, p = 0.00, n2 = 0.60. A posteriori multiple comparison showed statistically significant differences in the measured heart rate as a function the intensity determined by the grip width used.
Active muscles RPE
Table 2 shows the mean (SD) values of the RPE-AM scores measured at the three assessed intensities. Statistically significant differences were determined for the RPE-AM expressed regarding the different grip width (i.e., different intensities), whether all the exercises were analyzed together for each performed intensity (F (2, 206) = 352.51, p = 0.00, n2 = 0.77) or when they were considered separately: (i) SA (F (2, 50) = 95.42, p = 0.00, n2 = 0.79); (ii) EF (F (2, 50) = 132.12, p = 0.00, n2 = 0.84); (iii) AH (F (2, 50) = 116.02, p = 0.000, n2 = 0.82); (iv) EH (F (2, 50) = 85.38, p = 0.00, n2 = 0.77). A posteriori multiple comparisons showed statistically significant differences in RPE-AM as a function of the grip width used.
Table 2.
Differences in RISE Scale scores between different intensities and types of perceptions.
| Active muscles | Overall body | |||||
|---|---|---|---|---|---|---|
| High | Medium | Low | High | Medium | Low | |
| Shoulder abduction | 4.73 (0.53)* | 3.65 (0.48)** | 2.85 (0.73) | 3.38 (0.70)* | 2.77 (0.91)† | 2.50 (0.76) |
| Elbow flexion | 4.77 (0.43)* | 3.50 (0.51)** | 2.77 (0.59) | 3.46 (0.71)* | 2.85 (0.83)† | 2.42 (0.70) |
| Hip abduction | 4.61 (0.57)* | 3.35 (0.80)** | 1.61 (0.80) | 3.35 (0.63)* | 2.61 (0.80)** | 1.61 (0.70) |
| Hip extension | 4.31 (0.62)* | 3.19 (0.75)** | 2.15 (0.88) | 3.42 (0.64)* | 2.69 (0.84)† | 2.15 (0.73) |
| Overall for all exercises | 4.60 (0.57)* | 3.42 (0.66)** | 2.35 (0.90) | 3.40 (0.66)* | 2.73 (0.84)** | 2.17 (0.79) |
Data are expressed as mean (standard deviation) of the different intensities (i.e., different grip widths) for the different types of perception analyzed. RISE Scale: Resistance Intensity Scale for Exercise with TheraBand elastic bands. Numerical equivalence of the data with the qualitative descriptors: 1 (easy); 2 (low); 3 (moderate); 4 (hard); 5 (maximal). Rating of perceived exertion (RPE) for active muscles and overall body: RPE at the end of the 15 repetitions at the different intensities.
* Very significant differences (p ≤ 0.001) with medium and low intensities.
** Very significant differences (p ≤ 0.001) with low intensities.
† Significant differences (p < 0.05) with low intensities.
Regarding the construct validity, categorical line regression analysis showed that the RPE-AM of the OMNI-RES EB scale was an excellent predictor of the RISE scale for AM (see Table 3), with values from the different exercises ranging from 0.84 to 0.93.
Table 3.
Categorical linear regression analysis between the criterion and conditional scales from rating of perceived exertion.
| r | R2 (SEE) | p | RE | ||
|---|---|---|---|---|---|
| Shoulder abduction | AM | 0.92 | 0.84 (0.86) | 0.000 | 2.03 x (WN) – 0.303 |
| OB | 0.85 | 0.73 (1.07) | 0.000 | 2.019 x (WN) – 0.823 | |
| Elbow flexion | AM | 0.94 | 0.88 (0.79) | 0.000 | 2.185 x (WN) – 0.861 |
| OB | 0.85 | 0.73 (1.03) | 0.000 | 1.98 x (WN) – 0.673 | |
| Hip abduction | AM | 0.96 | 0.93 (0.84) | 0.000 | 2.078 x (WN) – 0.799 |
| OB | 0.90 | 0.82 (0.96) | 0.000 | 2.001 x WN) – 0.811 | |
| Hip extension | AM | 0.95 | 0.89 (0.87) | 0.000 | 2.171 x (WN) – 0.703 |
| OB | 0.88 | 0.77 (1.13) | 0.000 | 2.306 x (WN) – 1.576 | |
| Overall for all exercises | AM | 0.95 | 0.90 (0.85) | 0.000 | 2.123 x (WN) – 0.694 |
| OB | 0.88 | 0.77 (1.05) | 0.000 | 2.078 x (WN) – 0.975 |
SEE: Standard error of the estimation. RE: regression equation (i.e., value in RPE EB can be predicted for RISE Scale value); WN: word number from RISE Scale (1 = easy, 2 = low, 3 = moderate, 4 = hard, 5 = maximal). AM: active muscles. OB: overall body.
Table 4 shows score equivalences between the rating of perception scales of the RPE-AM from the categorical linear regression analysis determined by the “overall for all exercises equation” as described in Table 3.
Table 4.
Rating of perceived exertion score equivalences between scales from the categorical linear regression analysis.
| Rating of perceived exertion | ||||||
|---|---|---|---|---|---|---|
| OMNI-RES EB scale | RPE-AM | 1.43 | 3.55 | 5.67 | 7.80 | 9.92 |
| RPE-OB | 1.1 | 3.2 | 5.26 | 7.34 | 9.41 | |
| RISE scale | Easy | Low | Moderate | Hard | Maximal | |
OMNI-RES EB: OMNI-Resistance perception scale for use with elastic bands (0-10). RISE Scale: Resistance Intensity Scale for Exercise with TheraBand elastic bands. RPE-AM: rating of perceived exertion of the active muscles. RPE-OB: rating of perceived exertion of the overall body.
A significant association between the RPE-AM was reported for the upper-limb (χ212 = 82.55, p = 0.00) and lower-limb (χ216 = 76.30, p = 0.00) exercises. This significant association between the RPE-AM was also observed between the upper- and lower-limb exercises: SA/EH χ216 = 70.92, p = 0.00; SA/AH χ216 = 61.57, p = 0.00; EF/EH χ212 = 84.74, p = 0.00; EF/AH χ212 = 52.10, p = 0.00.
Overall body RPE
Table 2 shows the mean (SD) values of the RPE-OB scores. Statistically significant differences for the RPE-OB were determined as a function of the used grip (i.e., different intensities), whether all the exercises were analyzed together for each performed intensity (F (2, 206) = 122.67, p = 0.00, n2 = 0.54) or were considered separately: (i) SA (F (2, 50) = 28.72, p = 0.00, n2 = 0.53); (ii) EF (F (2, 50) = 24.47, p = 0.00, n2 = 0.49); (iii) AH (F (2, 50) = 45.84, p = 0.00, n2 = 0.65); (iv) EH (F (2, 50) = 35.41, p = 0.00, n2 = 0.59). A posteriori multiple comparison analysis showed statistically significant differences in RPE-OB as a function of the grip width used, that is RPE-OB differed significantly between the different intensities analyzed.
Regarding the construct validity, categorical line regression analysis showed that the RPE-OB of the OMNI-RES EB scale was an excellent predictor for the RISE scale for OB (see Table 3), with values from the different exercises ranging from 0.73 to 0.82.
Table 4 shows score equivalences between the rating of perception scales for the overall body from the categorical linear regression analysis determined by the “overall for all exercises equation” as described in Table 3.
There was a significant association between the RPE-OB scores measured for the upper-body (χ216 = 42.88, p = 0.00) and the lower body (χ216 = 129.76, p = 0.00) exercises. This significant association between the RPE-OB was also observed between the upper- and lower-body exercises: SA/EH χ216 = 75.89, p = 0.00; SA/AH χ216 = 60.77, p = 0.00; EF/EH χ216 = 56.65, p = 0.00; EF/AH χ216 = 44.88, p = 0.00.
Comparison between scores obtained from RPE-AM and RPE-OB
Statistically significant differences were determined between the scores obtained from the RPE-OB and RPE-AM. The RPE-OB always showed lower scores than those reported for the RPE-AM, with the exception of RPE from the lower-limb low-intensity exercises that produced similar scores: (i) SA: high intensity F (1, 25) = 59.24, p = 0.00, n2 = 0.70, 95% CI [0.99, 1.71]; medium intensity F (1, 25) = 47.74, p = 0.00, n2 = 0.66, 95% CI [0.62, 1.15]; low intensity F (1, 25) = 5.61, p = 0.026, n2 = 0.18, 95% CI [0.04, 0.65]; (ii) EF: high intensity F (1, 25) = 96.33, p = 0.00, n2 = 0.79, 95% CI [1.03, 1.58]; medium intensity F (1, 25) = 23.38, p = 0.00, n2 = 0.48, 95% CI [0.37, 0.93]; low intensity F (1, 25) = 7.88, p = 0.010, n2 = 0.24, 95% CI [0.09, 0.60]; (iii) AH: high intensity F (1, 25) = 147.16, p = 0.00, n2 = 0.85, 95% CI [1.03, 1.58]; medium intensity F (1, 25) = 26.46, p =0 .00, n2 = 0.51, 95% CI [0.37, 0.93]; low intensity F (1, 25) = 0.00, p = 1.00, n2 = 0.00, 95% CI [–0.228, 0.228]. (iv) EH: high intensity F (1, 25) = 47.74, p = 0.00, n2 = 0.66, 95% CI [0.62, 1.15]; medium intensity F (1, 25) = 19.12, p = 0.00, n2 = 0.43, 95% CI [0.26, 0.74]; low intensity F (1, 25) = 0.00, p = 1.00, n2 = 0.00, 95% CI [–0.280, 0.280].
Intersession reliability of the RPE method for quantifying intensity with elastic bands
The internal consistency analysis of the values obtained from the applied force, heart rate, and RISE scale across different sessions showed almost excellent reliability. Regarding the RPE, the OMNI-RES EB scale provided similar intersession reliability to that observed for the RISE scale. Results of ICC analysis are shown in Tables 5 and 6.
Table 5.
Intersession reliability of the RISE Scale, applied force, and heart rate.
| ICC | p | 95%CI | ||
|---|---|---|---|---|
| Rating of perceived exertion | ||||
| Shoulder abduction RPE-AM | 0.85 | 0.00 | 0.77, 0.90 | |
| Shoulder abduction RPE-OB | 0.78 | 0.00 | 0.65, 0.86 | |
| Elbow flexion RPE-AM | 0.89 | 0.00 | 0.83, 0.93 | |
| Elbow flexion RPE-OB | 0.77 | 0.00 | 0.65, 0.86 | |
| Hip abduction RPE-AM | 0.90 | 0.00 | 0.84, 0.93 | |
| Hip abduction-RPE-OB | 0.81 | 0.00 | 0.71, 0.88 | |
| Hip extension RPE-AM | 0.86 | 0.00 | 0.78, 0.91 | |
| Hip extension RPE-OB | 0.76 | 0.00 | 0.63, 0.85 | |
| OEI RPE-AM | 0.88 | 0.00 | 0.85, 0.91 | |
| OEI RPE-OB | 0.80 | 0.00 | 0.74, 0.83 | |
| Applied force | ||||
| Shoulder abduction | Mean | 0.71 | 0.00 | 0.54, 0.82 |
| Peak | 0.88 | 0.00 | 0.80, 0.92 | |
| Elbow flexion | Mean | 0.70 | 0.00 | 0.51, 0.80 |
| Peak | 0.93 | 0.00 | 0.88, 0.95 | |
| Hip abduction | Mean | 0.94 | 0.00 | 0.91, 0.96 |
| Peak | 0.91 | 0.00 | 0.86, 0.94 | |
| Hip extension | Mean | 0.93 | 0.00 | 0.89, 0.95 |
| Peak | 0.93 | 0.00 | 0.90, 0.96 | |
| OEI | Mean | 0.95 | 0.00 | 0.93, 0.96 |
| Peak | 0.94 | 0.00 | 0.93, 0.95 | |
| Heart rate | ||||
| Shoulder abduction | 0.9 | 0.00 | 0.85, 0.94 | |
| Elbow flexion | 0.88 | 0.00 | 0.81, 0.92 | |
| Hip abduction | 0.88 | 0.00 | 0.81, 0.92 | |
| Hip extension | 0.87 | 0.00 | 0.80, 0.92 | |
| OEI | 0.88 | 0.00 | 0.85, 0.91 | |
RISE Scale: Resistance Intensity Scale for Exercise with TheraBand elastic bands. RPE-AM: rating of perceived exertion for active muscles. RPE-OB: rating of perceived exertion for overall body. OEI: overall for all exercises and intensities. Applied force: kilograms for the maximum and average values obtained during the 15 repetitions at the different intensities (i.e., different grip widths); Heart rate: beats per minute at end of the 15 repetitions at the different intensities (i.e., different grip widths). ICC: Intraclass correlation coefficient. Reliability interpretation values: ICC ≥ 0.70 acceptable or adequate; ICC ≥ 0.80 excellent.
Table 6.
Intersession reliability of OMNI-RES EB Scale scores.
| ICC | p | 95%CI | ||
|---|---|---|---|---|
| Rating of perceived exertion | ||||
| Shoulder abduction RPE-AM | 0.85 | 0.00 | 0.77, 0.91 | |
| Shoulder abduction RPE-OB | 0.76 | 0.00 | 0.63, 0.85 | |
| Elbow flexion RPE-AM | 0.91 | 0.00 | 0.85, 0.94 | |
| Elbow flexion RPE-OB | 0.86 | 0.00 | 0.77, 0.91 | |
| Hip abduction RPE-AM | 0.91 | 0.00 | 0.85, 0.94 | |
| Hip abduction-RPE-OB | 0.85 | 0.00 | 0.77, 0.90 | |
| Hip extension RPE-AM | 0.88 | 0.00 | 0.82, 0.92 | |
| Hip extension RPE-OB | 0.78 | 0.00 | 0.65, 0.86 | |
| OEI RPE-AM | 0.90 | 0.00 | 0.87, 0.92 | |
| OEI RPE-OB | 0.82 | 0.00 | 0.77, 0.85 | |
OMNI-RES EB: OMNI-Resistance perception scale for use with elastic bands (0-10). RPE-AM: rating of perceived exertion for active muscles. RPE-OB: rating of perceived exertion for overall body. OEI: overall for all exercises and intensities. ICC: Intraclass correlation coefficient. Reliability interpretation values: ICC ≥ 0.70 acceptable or adequate; ICC ≥ 0.80 excellent.
Discussion
Findings of the present study suggest the suitability of the RISE scale for monitoring exercise intensity in OA exercising with elastic bands. The RISE scale was shown to be a sensitive tool for discriminating between different levels of intensities (Table 2). It is worth highlighting that the applicability of the RISE scale was not affected by the type of exercise performed or the muscle mass involved (i.e., upper or lower limb). Consequently, the RISE scale can be used for monitoring exercises of any region of the body regardless of whether they can involve a global or regional muscle activation. Moreover, both RPE-AM as RPE-OB showed excellent reliability between sessions. Therefore, RISE scale could be and attractive alternative for monitoring the exercise intensity across sessions using different training configurations. Furthermore, compared with previous scales, RISE could be considered more sensitive because can discriminate between medium and low intensities of RPE-OB in the four exercises analyzed, unlike OMNI-RES EB validated in OA that only discriminated it in one of the four exercises. As previously highlighted, the specific design of the present scale can have helped to improve the ability of the OA in achieving a more accurate estimation of the exercise intensity when training with bands. It is therefore possible that using RISE scores, entails an suitable methodology for monitoring the perceptual response associated with different resistance exercise intensity in OA (Colado and Triplett, 2008; Day et al., 2004). It is known that the positive responsiveness of RPE between different levels of resistance intensities is a method of concurrent validation of perceived exertion category scales for both female and male adults (Mays et al., 2010). The present investigation is one of the first to examine the concurrent validity of a pictorial-verbal category perceptual scale in older females and males exercising with elastic bands using both upper- and lower-body resistance exercises.
This new simplified version of the OMNI scale favors a more accurate control of intensity in OA. A concurrent paradigm has been used to corroborate the application of the RISE scale in the elderly. Both the RPE-AM and RPE-OB represent a positive linkage with the applied force and the heart rate response in OA during workout routines using elastic bands. According to previous studies (Colado et al., 2012b; 2014; 2108), the RPE-AM produced a higher perceptual response than RPE-OB for both upper- and lower-body exercise. One of the applications of the perceptual response is to differentiate anatomically regionalized perceptual signals from the total body signal when both assessments are made within a comparatively narrow time frame (Robertson et al., 2001). Consequently, we can confirm that the RISE scale is accurate and valid in monitoring the differentiated responsiveness of RPE-AM with OA performing different intensities of elastic band exercise.
In addition, it can be confirmed that a reduction in the elastic band grip width (i. e., an intensity modification) resulted in an increase in the physiological and performance variables (i. e., applied force) and in the corresponding RPE-AM and OB (Colado et al., 2012b; 2014: 2018). Narrowed grip width is normally used with elastic bands as the equivalent to increasing resistance when training with weight-based devices (Colado and Triplett, 2008). Therefore, our findings are also consistent with previous studies using Borg (i.e., 6–20, CR-10) or the OMNI-RES scales, which showed RPE increased as a function of increasing the total weight lifted (Naclerio and Larumbe-Zabala, 2017a; 2017b; Pincivero et al., 2001; Suminski et al., 1997). The current study corroborated that for the same number of repetitions performed without reaching muscular failure, a shorter grip width (a greater resistance) elicits a higher RPE than that produced when exercising with a longer grip width (lighter resistance). Thus, we have objectively confirmed the validity of the method for prescribing intensity while performing resistance exercises using variable resistance devices (i.e., elastic bands). This methodology follows the suggestions of previous studies (Kraemer et al., 2001; Suminski et al., 1997), in which the number of repetitions was adapted to the training aims using the perceptual response as a criterion to adapt the exercise intensity. Strength gains become possible in OA, but training adjustments must be made for continued progress, as for example could be the modification of the exercise intensity (Gargallo et al., 2018). It seems that assessing the perceptual response from the OMNI-RES EB or RISE scale could be used to track strength changes or for designing training programs over time in OA (Gearhart et al., 2009).
Regarding the level of applied force, the present results are in line with those of other studies that used Borg scales demonstrating a positive association between the RPE score and the total weight lifted (Gearhart et al., 2002; Lagally and Robertson, 2006; Pierce et al., 1993). Our study used elastic bands in which the level of applied resistance was controlled by altering the grip width. As has been observed previously (Colado et al., 2018), this practical strategy for controlling the exercise intensity is endorsed by the differences in the applied force observed between all the used intensities, with the exception of the peak force measured for the medium and low intensities when performing upper-limb exercises.
In addition to other factors, the adjustments of the cardiovascular system during the exercise are influenced by the progressive recruitment of motor units (Nobrega et al., 2014; Strange et al., 1993). The autonomic nervous system and its sympathetic and parasympathetic afferents modulate the heart rate, increasing the number of heart beats as the intensity and the level of effort increase (Quitério et al., 2011). In this study, the heart rate was considered an expression of the cardiovascular stress, reflecting the amount of applied force during the performed exercises (Miller et al., 2009; Quitério et al., 2011; Rozenek et al., 1993). Therefore, heart rate served as a co-criterion variable with the applied force in assessing concurrent RPE responsiveness during the different intensities (Miller et al., 2009). The observed differences in the physiological and perceptual variables in response to changes in exercise intensity as a result of elastic band grip width are in the line with previous studies (Colado et al., 2014; 2018). From the practical standpoint, a reduction in elastic band grip width is related to an increase in heart rate and the RPE values obtained from both the AM and OB scores. These scores can be considered for safety, representing useful criteria for inferring the cardiovascular stress in exercising older populations, particularly in patients where an upper heart rate limit should be respected or when a range of RPE scare is advised for controlling the exercise overload and the corresponding impact on the cardiovascular system (Arakelian et al., 2019; Gearhart et al., 2009; Morishita et al., 2019). The excellent reliability of the heart rate was also observed across sessions.
As with the present study, several previous investigations have been conducted to obtain the construct validity of different scales for different types of exercises, with all of them obtaining similar validity coefficients as those observed in our study (Lagally and Robertson, 2006; Nakamura et al., 2009; Utter et al., 2006). The Borg 6-20 Scale was used as the criterion metric, as was the case with the construct validity of the OMNI-RES scale (Lagally and Robertson, 2006), OMNI-Kayak RPE Scale (Nakamura et al., 2009), and Omni Perceived Exertion Scale for Elliptical Ergometry (Mays et al., 2010). Specifically, the present study considered only resistance exercises performed with elastic bands by OA and examined the construct validity of the RISE scale using the OMNI-RES EB scale as the criterion metric. In accordance with our hypothesis, the RISE scale and the OMNI-RES EB scale obtained validity coefficients for the RPE-AM of R2 = 0.90 (r = 0.95) and R2 = 0.77 (r = 0.88) for the RPE-OB. Thus, whether the resulting perceptual response from the OMNI-RES scale is high, medium, or low, similar values will be expected from the RISE scale.
This investigation followed the same methodological guidelines of previous studies (Colado et al., 2012b; Colado et al., 2014; Lagally et al., 2002; Robertson et al., 2003) but with the advantage that the concurrent and construct validation has been performed using four exercises (two for upper body and two for lower body) versus only two exercises (one of each) used in the previous investigations. In addition, the present study used three different intensities for each of the performed exercises. Indeed, using the RISE scale to quantifying resistance-training intensity was demonstrated to be a reliable method for measuring the perceptual response and the applied force across two different measurements (i.e. this could be workouts in an applied setting) sessions. The observed reliability of the RISE scale is consistent with the results of previous studies using a similar population in which the targeted number of repetitions was maintained while using the RISE scale for controlling the intensity over medium-term band-based resistance protocols (Muntaner-Mas et al., 2017; Tada, 2018).
The obtained results may have important implications for exercise prescription, offering valuable information to researchers, clinicians, and coaches by assisting in the development and management of resistance-training programs in the elderly population. Coaches and clinicians will be able to accurately distinguish between different levels of intensity using the same material (i.e., elastic bands) and, consequently, vary the proper training load for individuals with different levels of physical activity targeting different outcomes (Day et al., 2004; Robertson et al., 2005). Moreover, resistance training with submaximal efforts by means of the RPE could reduce the risk of injury in OA and attenuate the cardiovascular stress with respect to training with heavy resistance. This is an important consideration for increasing exercise adherence and guaranteeing the achievement of the expected outcomes (Gearhart et al., 2008, 2009; 2011; Morishita et al., 2019).
Finally, it must be highlighted that compared with other scales, RISE has an easier to understand design (visual and verbal with only five levels). These characteristics make RISE easier to apply in OA, avoiding some inconveniences raised by the use of other perceptual scales in controlling resistance training (Glass and Stanton, 2004).
Limitations
Previous scales for monitoring intensity in resistance exercise have used two key words (easy and hard) combined with adjectives to represent a cognitive unidirectional change in the intensity of perceptual response expressed through gradations of physical exertion (Robertson et al., 2003; 2005). Some RPE scales have been validated to different languages to improve accuracy due to possible misunderstandings between similar verbal descriptors coming from different languages (Guidetti et al., 2011; Suminski et al., 2008). These modifications are even more necessary when the level of each stage of perceived effort is described with one to four words using short sentences with a subtle semantic differences between them. Although our study has been developed with not English-speakers, the validate RISE scale does not combine adjectives and shows only one adjective in each level of the gradation of physical exertion. Moreover, they were accustomed with the easy meaning of the English adjectives in the familiarization sessions, taking in consideration that some of them were written similarly between both languages (Spanish and English). Additionally, OMNI-RES EB was also employed for the construct validation of the RISE scale. Although this scale was used considering only the numerical descriptors. Thus, despite the verbal descriptors employed in the RISE scale are only a clear word that is easy of understand by non-English-speakers, futures studies aimed to validate the Spanish version of the RISE are still warranted. Additionally, similar studies using larger sample size are needed. It is worth noting that our study considered both sex together without analyzing possible perceptual differences between sexes. Indeed, previous specific already stated that this type of pictograms are equally valid for their use by both sexes during upper- and lower-body resistance exercises when are performed isotonic and isometric muscle actions at the same relative exercise intensity (Pincivero et al., 2000; Robertson et al., 2003). However, future studies may consider validating the RISE scale with other elder population profiles, e.g. less familiarized participants in using the perceptual response for controlling physical efforts. Additionally, it is still needed to analyze potential differences between men and women participants (Robertson et al., 2003). Furthermore, our findings need to be confirmed using other types of exercises (i.e., multi-joint exercises), and, brands of elastic bands offering different levels of resistance.
Conclusion
The present findings suggest that the RISE and OMNI-RES EB appear to be equally valid metrics to measure perceived exertion in older adults exercising with bands. OA can use the RISE scale to verbally rate (easy to maximal) their perceptions of effort during both upper- and lower-body exercises using elastic bands. The strong positive and linear relationship observed between the perceptual responses expressed by RISE scale scores and heart rate and applied force provides evidence of the concurrent validity of this scale to monitor exercise intensity in OA exercising with elastic bands. In summary, the good concurrent and construct validity coefficients obtained in the present study showed that the RISE scale can be used in OA without reducing the accuracy of the training load dosage prescribed during usual resistance exercises performed with elastic bands.
Acknowledgements
The authors thank Juan J. Carrasco for his statistical advice at the beginning stage of this global project and Filipa M. Pedrosa for help during the initial phase of the data collection process. This work was supported by the grant Ignacio Larramendi 2014 from the Mapfre Foundation (Code: OTR2015-140931NVES). The results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The experiments comply with the current laws of the country in which they were performed. The authors have no conflicts of interests.
Biographies

Juan C. COLADO
Employment
Full Professor, University of Valencia, Spain. Director of the Research Group in Prevention and Health in Exercise and Sport and Director of the Research Unit in Sport and Health at the University of Valencia, Spain.
Degree
PhD
Research interests
Strength and conditioning, health and quality of life, special populations, pediatric and aging.
E-mail: juan.colado@uv.es

Guilherme Eustáquio FURTADO
Employment
Invited research of Research Unit for Sport and Physical Activity (CIDAF) Faculty of Sport Science and Physical Education, University of Coimbra, Portugal
Degree
PhD
Research interests
Relationships between regular exercise, biochemical (immune and hormonal) parameters and the contemporary problems that challenge older populations to adopt an active and healthy lifestyle: falls; cognitive decline, physical frailty and sarcopenia
E-mail: furts2001@yahoo.com.br

Ana Maria TEIXEIRA
Employment
Associated Professor, University of Coimbra, Portugal. Coordinator of the PhD course in Sport Sciences, Faculty of Sport Sciences and Physical Education, University of Coimbra, Coimbra, Portugal
Degree
PhD
Research interests
Exercise and the immune system, health and quality of life, frailty, chronic diseases and aging.
E-mail: ateixeira@fcdef.uc.pt
Jorge FLANDEZ
Employment
Tenured Professor, Faculty of Pedagogy in Physical Education, Sports and Recreation, Austral University of Valdivia, Chile.
Degree
PhD
Research interests
Strength and conditioning, measurement and evaluation.
E-mail: jflandezv@gmail.com

Fernando NACLERIO
Employment
Associate Professor in Strength Training and Sports Nutrition. University of Greenwich, UK. Programme Leader MSc Strength and Conditioning.
Degree
PhD
Research interests
Strength, conditioning, and Sport Nutrition.
E-mail: f.j.naclerio@gre.ac.uk
References
- Aboodarda S. J., Page P.A., Behm D. G. (2016) Muscle activation comparisons between elastic and isoinertial resistance: A meta-analysis. Clinical Biomechanics (Bristol, Avon) 39, 52-61. [DOI] [PubMed] [Google Scholar]
- Arakelian V. M., Goulart C. D. L., Mendes R. G., Sousa N. M., Trimer R., Guizilini S., Sampaio L. M. M., Baldissera V., Arena R., Reis M. S., Borghi-Silva A. (2019) Physiological responses in different intensities of resistance exercise - Critical load and the effects of aging process. Journal of Sports Sciences 37, 1420-1428. [DOI] [PubMed] [Google Scholar]
- Beck T. W. (2013) The importance of a priori sample size estimation in strength and conditioning research. Journal of Strength and Conditioning Research 27, 2323-2337. [DOI] [PubMed] [Google Scholar]
- Behm D. G. (1991) An analysis of intermediate speed exercises for velocity specific strength gains. The Journal of Applied Sport Science Research 5, 1-5. [Google Scholar]
- Borg G. A. (1982) Psychophysical bases of perceived exertion. Medicine and Science in Sports and Exercise 14, 377-381. [PubMed] [Google Scholar]
- Chapman M., Larumbe-Zabala E., Gosss-Sampson M., Colpus M, Triplett N. T., Naclerio F. (2019) Perceptual, mechanical, and electromyographic responses to different relative loads in the parallel squat. Journal of Strength and Conditioning Research 33, 8-16. [DOI] [PubMed] [Google Scholar]
- Chupel M. U., Direito F., Furtado G. E., Minuzzi L.G., Pedrosa F. M., Colado J. C., Ferreira J. P., Filaire E., Teixeira A. M. (2017) Strength training decreases inflammation and increases cognition and physical fitness in older women with cognitive impairment. Frontiers in Physiology 8, 377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colado J. C., Triplett N.T. (2008) Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. Journal of Strength and Conditioning Research 22, 1441-1448. [DOI] [PubMed] [Google Scholar]
- Colado J. C., Triplett N. T., Tella V., Saucedo P., Abellán J. (2009) Effects of aquatic resistance training on health and fitness in postmenopausal women. European Journal of Applied Physiology 106, 113-122. [DOI] [PubMed] [Google Scholar]
- Colado J. C., Garcia-Masso X., Pellicer M., Alakhdar Y., Benavent J., Cabeza-Ruiz R. (2010) A comparison of elastic tubing and isotonic resistance exercises. International Journal of Sports Medicine 31, 810-781. [DOI] [PubMed] [Google Scholar]
- Colado J. C., Garcia-Masso X., Rogers M. E., Tella V., Benavent J., Dantas E. H. (2012a) Effects of aquatic and dry land resistance training devices on body composition and physical capacity in postmenopausal women. Journal of Human Kinetics 32, 185-195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Colado J. C., Garcia-Masso X., Triplett N. T., Flandez J., Borreani S., Tella V. (2012b) Concurrent validation of the OMNI-resistance exercise scale of perceived exertion with Thera-band resistance bands. Journal of Strength and Conditioning Research 26, 3018-3024. [DOI] [PubMed] [Google Scholar]
- Colado J. C., Garcia-Masso X., Triplett N. T., Calatayud J., Flandez J., Behm D., Rogers M. E. (2014) Construct and Concurrent Validation of a New Resistance Intensity Scale for Exercise with Thera-Band® Elastic Bands. Journal of Sports Science and Medicine 13, 758-766. [PMC free article] [PubMed] [Google Scholar]
- Colado J. C., Pedrosa F. M., Juesas A., Gargallo P., Carrasco J. J., Flandez J., Chupel M. U., Teixeira A. M., Naclerio F. (2018) Concurrent validation of the OMNI-Resistance Exercise Scale of perceived exertion with elastic bands in the elderly. Experimental Gerontology 103, 11-16. [DOI] [PubMed] [Google Scholar]
- Day M. L., McGuigan M. R., Brice G., Foster C. (2004) Monitoring exercise intensity during resistance training using the session RPE scale. Journal of Strength and Conditioning Research 18, 353-358. [DOI] [PubMed] [Google Scholar]
- de Oliveira P. A., Blasczyk J. C., Souza Junior G., Lagoa K. F., Soares M., de Oliveira R. J., Filho P.J.B.G., Carregaro R. L., Martins W. R. (2017) Effects of Elastic Resistance Exercise on Muscle Strength and Functional Performance in Healthy Adults: A Systematic Review and Meta-Analysis. Journal of Physical Activity and Health 14, 317-327. [DOI] [PubMed] [Google Scholar]
- Delmonico M. J., Harris T. B., Lee J. S., Visser M., Nevitt M., Kritchevsky S. B., Tylavsky F. A., Newman A. B. (2007) Alternative definitions of sarcopenia, lower extremity performance, and functional impairment with aging in older men and women. Journal of the American Geriatrics Society 55, 769-774. [DOI] [PubMed] [Google Scholar]
- Faul F., Erdfelder E., Buchner A., Lang A. G. (2009) Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods 41, 1149-1160. [DOI] [PubMed] [Google Scholar]
- Fritz N. B., Juesas Á., Gargallo P., Calatayud J., Fernández-Garrido J., Rogers M. E., Colado J. C. (2018) Positive Effects of a Short-Term Intense Elastic Resistance Training Program on Body Composition and Physical Functioning in Overweight Older Women. Biological Research for Nursing 20, 321-334. [DOI] [PubMed] [Google Scholar]
- Fukuchi R. K., Stefanyshyn D. J., Stirling L., Ferber R. (2016) Effects of strengthening and stretching exercise programmes on kinematics and kinetics of running in older adults: a randomised controlled trial. Journal of Sports Sciences 34, 1774-1781. [DOI] [PubMed] [Google Scholar]
- Gargallo P., Colado J. C., Juesas A., Hernando-Espinilla A., Estañ-Capell N., Monzó-Beltran L., García-Pérez P., Cauli O., Sáez G. T. (2018) The Effect of Moderate- Versus High-Intensity Resistance Training on Systemic Redox State and DNA Damage in Healthy Older Women. Biological Research for Nursing 20, 205-217. [DOI] [PubMed] [Google Scholar]
- Gearhart R. F., Goss F. L., Lagally K. M., Jakicic J. M., Gallagher J., Gallagher K. I., Robertson R. J. (2002) Ratings of perceived exertion in active muscle during high-intensity and low-intensity resistance exercise. Journal of Strength and Conditioning Research 16, 87-91. [PubMed] [Google Scholar]
- Gearhart R. F., Jr., Lagally K. M., Riechman S. E., Andrews R. D., Robertson R. J. (2008) RPE at relative intensities after 12 weeks of resistance-exercise training by older adults. Perceptual and Motor Skills 106, 893-903. [DOI] [PubMed] [Google Scholar]
- Gearhart R. F., Jr, Lagally K. M., Riechman S. E., Andrews R. D., Robertson R. J. (2009) Strength tracking using the OMNI resistance exercise scale in older men and women. Journal of Strength and Conditioning Research 23,1011-1015. [DOI] [PubMed] [Google Scholar]
- Gearhart R. F., Jr, Lagally K. M., Riechman S. E., Andrews R. D., Robertson R. J. (2011) Safety of using the adult OMNI Resistance Exercise Scale to determine 1-RM in older men and women. Perceptual and Motor Skills 113, 671-676. [DOI] [PubMed] [Google Scholar]
- Glass S. C., Stanton D. R. (2004) Self-selected resistance training intensity in novice weightlifters. Journal of Strength and Conditioning Research 18, 324-327. [DOI] [PubMed] [Google Scholar]
- Gómez-Tomás C., Chulvi-Medrano I., Carrasco J. J., Alakhdar Y. (2018) Effect of a 1-year elastic band resistance exercise program on cardiovascular risk profile in postmenopausal women. Menopause 25, 1004-1010. [DOI] [PubMed] [Google Scholar]
- Griep M. I., Borg E., Collys K., Massart D. L. (1998) Category ratio scales as an alternative to magnitude matching for age-related taste and odour perception. Food Quality and Preference 9, 67-72. [Google Scholar]
- Guidetti L., Broccatelli M., Baldari C., Buzzachera C. F., Goss F. L., Utter A. C., Sgadari A. (2011) Validation of the Italian version of the OMNI Scale of Perceived Exertion in a sample of Italian-speaking adults. Perceptual and Motor Skills 112, 201-210. [DOI] [PubMed] [Google Scholar]
- Guidetti A., Sgadari A., Buzzachera F. C., Broccatelli M., Utter A. C., Goss F. L., Baldari C. (2011) Validation of the OMNI-Cycle Scale of Perceived Exertion in the Elderly. Journal of Aging aAnd Physical Activity 19, 214-224. [DOI] [PubMed] [Google Scholar]
- Kraemer W. J., Keuning M., Ratamess N. A., Volek J. S., McCormick M., Bush J. A., Nindl B. C., Gordon S. E., Mazzetti S. A., Newton R. U., Gomez A. L., Wickham R. B., Rubin M. R., Hakkinen K. (2001) Resistance training combined with bench-step aerobics enhances women’s health profile. Medicine and Science in Sports and Exercise 33, 259-269. [DOI] [PubMed] [Google Scholar]
- Lagally K. M., Robertson R. J., Gallagher K. I., Goss F. L., Jakicic J. M., Lephart S., Goodpaster B. (2002) Perceived exertion, electromyography, and blood lactate during acute bouts of resistance exercise. Medicine and Science in Sports and Exercise 34, 552-559. [DOI] [PubMed] [Google Scholar]
- Lagally K. M., Robertson R. J. (2006) Construct validity of the OMNI Resistance Exercise Scale. Journal of Strength and Conditioning Research 20, 252-256. [DOI] [PubMed] [Google Scholar]
- Lalanneab C., Lorenceaua J. (2004) Crossmodal integration for perception and action. Journal of Physiology 98, 265-279. [DOI] [PubMed] [Google Scholar]
- Li X., Lin C., Liu C., Ke S., Wan Q., Luo H., Huang Z., Xin W., Ma C., Wu S. (2017) Comparison of the effectiveness of resistance training in women with chronic computer-related neck pain: a randomized controlled study. International Archives of Occupational and Environmental Health 90, 673-683. [DOI] [PubMed] [Google Scholar]
- Mally K., Trentmann J., Heller M., Dittmar M. (2011) Reliability and accuracy of segmental bioelectrical impedance analysis for assessing muscle and fat mass in older Europeans: a comparison with dual-energy X-ray absorptiometry. European Journal of Applied Physiology 111, 1879-1887. [DOI] [PubMed] [Google Scholar]
- Martins W., de Oliveira R., Carvalho R., de Oliveira V., da Silva V., Silva M. (2013) Elastic resistance training to increase muscle strength in elderly: a systematic review with meta-analysis. Archives of Gerontology and Geriatrics 57, 8-15. [DOI] [PubMed] [Google Scholar]
- Mays R. J., Goss F. L., Schafer M., Kim K. H., Nagle-Stilley E. F., Robertson R. J. (2010) Validation of adult Omni perceived exertion scales for elliptical ergometry. Perceptual and Motor Skills 111, 848-862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMaster D. T., Cronin J., McGuigan M. R. (2010) Quantification of Rubber and Chain-Based Resistance Modes. Journal of Strength and Conditioning Research 24, 2056-2064. [DOI] [PubMed] [Google Scholar]
- Miller P. C., Hall E. E., Chmelo E. A., Morrison J. M., DeWitt R. E., Kostura C.M. (2009) The influence of muscle action on heart rate, RPE, and affective responses after upper-body resistance exercise. Journal of Strength and Conditioning Research 23, 366-372. [DOI] [PubMed] [Google Scholar]
- Morishita S., Tsubaki A., Nakamura M., Nashimoto S., Fu J. B., Onishi H. (2019) Rating of perceived exertion on resistance training in elderly subjects. Expert Review of Cardiovascular therapy 17,135-142. [DOI] [PubMed] [Google Scholar]
- Muntaner-Mas A., Vidal-Conti J., Borràs P.A., Ortega F.B., Palou P. (2017) Effects of a Whatsapp-delivered physical activity intervention to enhance health-related physical fitness components and cardiovascular disease risk factors in older adults. Journal of Sport Medicine Aand Physical Fitness 57, 90-102. [DOI] [PubMed] [Google Scholar]
- Naclerio F., Larumbe-Zabala E. (2017) Loading Intensity Prediction by Velocity and the OMNI-RES 0-10 Scale in Bench Press. Journal of Strength and Conditioning Research 31, 323-329. [DOI] [PubMed] [Google Scholar]
- Naclerio F., Larumbe-Zabala E. (2017) Relative Load Prediction by Velocity and the OMNI-RES 0-10 Scale in Parallel Squat. Journal of Strength and Conditioning Research 31, 1585-1591. [DOI] [PubMed] [Google Scholar]
- Nakamura F. Y., Perandini L. A., Okuno N. M., Borges T. O., Bertuzzi R. C., Robertson R. J. (2009) Construct and concurrent validation of OMNI-Kayak rating of Perceived Exertion Scale. Perceptual & Motor Skills 108, 744-758. [DOI] [PubMed] [Google Scholar]
- Newsam C. J., Leese C., Fernandez-Silva J. (2005) Intratester reliability for determining an eight-repetition maximum for three shoulder exercises using elastic bands. Journal of Sport Rehabilitation 14, 35-47. [Google Scholar]
- Nobrega A. C., O'Leary D., Silva B. M., Marongiu E., Piepoli M. F., Crisafulli A. (2014) Neural regulation of cardiovascular response to exercise: role of central command and peripheral afferents. BioMed Research International 2014, 478965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Picha K. J., Almaddah M. R., Barker J., Ciochetty T., Black W. S., Uhl T. L. (2017) Elastic resistance effectiveness on increasing strength of shoulders and hips. Journal of Strength and Conditioning Research 33, 931-943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce K., Rozenek R., Stone M. H. (1993) Effects of high volume weight training on lactate, heart rate and perceived exertion. Journal of Strength and Conditioning Research 7, 211-215. [Google Scholar]
- Pincivero D. M., Coelho A. J., Campy R. M., Salfetnikov Y., Bright A. (2001) The effects of voluntary contraction intensity and gender on perceived exertion during isokinetic quadriceps exercise. European Journal of Applied Physiology 84, 221-226. [DOI] [PubMed] [Google Scholar]
- Pincivero D. M., Coelho A. J., Erikson W. H. (2000) Perceived exertion during isometric quadriceps contraction. A comparison between men and women. Journal of Sport Medicine and Physical Fitness 40, 319-326. [PubMed] [Google Scholar]
- Quitério R. J., Melo R. C., Takahashi A.C.M., Aniceto I.A.V., Silva E., Catai A. M. (2011) Torque, myoelectric signal and heart rate responses during concentric and eccentric exercises in older men. Revista Brasileira de Fisioterapia 15, 8-14. [DOI] [PubMed] [Google Scholar]
- Revilla M. A., Saris W. E., Krosnick J. A. (2014) Choosing the Number of Categories in Agree–Disagree Scales. Sociological Methods and Research 43, 73-97. [Google Scholar]
- Rieping T., Furtado G. E., Letieri R. V., Chupel M. U., Colado J. C., Hogervorst E., Filaire E., Teixeira A.M.M.B., Ferreira J. P. (2019) Effects of Different Chair-Based Exercises on Salivary Biomarkers and Functional Autonomy in Institutionalized Older Women. Research Quarterly for Exercise and Sport 90, 36-45. [DOI] [PubMed] [Google Scholar]
- Robertson R. J. (2004) Perceived Exertion for Practitioners. Champaign, IL: Human Kinetics. [Google Scholar]
- Robertson R. J., Goss F. L., Boer N. F., Gallagher J. D., Thompkins T., Bufalino K., Balasekaran G., Meckes C., Pintar J., Williams A. (2001) OMNI Scale of perceived exertion at ventilatory breakpoint in children: response normalized. Medicine and Science in Sports and Exercise 33, 1946-1952. [DOI] [PubMed] [Google Scholar]
- Robertson R. J., Goss F. L., Rutkowski J., Lenz B., Dixon C., Timmer J., Andreacci J. (2003) Concurrent validation of the OMNI perceived exertion scale for resistance exercise. Medicine and Science in Sports and Exercise 35, 333-341. [DOI] [PubMed] [Google Scholar]
- Robertson R. J., Goss F. L., Andreacci J., Dubé J., Rutkowski J., Frazee K. M., Aaron D. J., Metz K. F., Kowallis R. A., Snees B. M. (2005) Validation of the children’s OMNI-resistance exercise scale of perceived exertion. Medicine and Science in Sports and Exercise 37, 819-826. [DOI] [PubMed] [Google Scholar]
- Rogers W. T. (2006) The Contribution of Kinesic Illustrators Towards the Comprehension of Verbal Behaviour Within Utterances. Human Communication Research 5, 54-62. [Google Scholar]
- Romero-Arenas S., Pérez-Gómez J, Alcaraz P. E. (2011) Circuit training. A useful tool for preventing the effects of aging? Culture, Science and Sport 6, 185–192. [Google Scholar]
- Rossi A. P., Bianchi L., Volpato S., Bandinelli S., Guralnik J., Zamboni M., Ferrucci L. (2017) Dynapenic abdominal obesity as a predictor of worsening disability, hospitalization, and mortality in older adults: Results from the InCHIANTI Study. The journals of gerontology. Series A, Biological Sciences and Medical Sciences 1, 1098-1104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rozenek R. L., Rosenau L., Rosenau P., Stone M. H. (1993) The effect of intensity on heart rate and blood lactate response to resistance exercise. Journal of Strength and Conditioning Research 7, 51-54. [Google Scholar]
- Small D. N., Prescott J. (2005) Odor/taste integration and the perception of flavor. Experimental Brain Research 166, 345-357. [DOI] [PubMed] [Google Scholar]
- Smith M. F., Ellmore M., Middleton G., Murgatroyd P. M., Gee T. I. (2017) Effects of Resistance Band Exercise on Vascular Activity and Fitness in Older Adults. International Journal of Sports Medicine 38,184-192. [DOI] [PubMed] [Google Scholar]
- Soria-Gila M. A., Chirosa I. J., Bautista I. J., Baena S., Chirosa L. J. (2015) Effects of Variable Resistance Training on Maximal Strength: A Meta-Analysis. Journal of Strength and Conditioning Research 29, 3260-7320. [DOI] [PubMed] [Google Scholar]
- Strange S., Secher N. H., Pawelczyk J. A., Karpakka J., Christensen N. J., Mitchell J. H., Saltin B. (1993) Neural control of cardiovascular responses and of ventilation during dynamic exercise in man. The Journal of Physiology 470, 693-704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suminski R. R., Robertson R. J., Arslanian S., Kang J., Utter A. C., DaSilva S. G., Goss F. L., Metz K. F. (1997) Perception of effort during resistance exercise. Journal of Strength and Conditioning Research 11, 261-265. [Google Scholar]
- Suminski R. R., Robertson R. J., Goss F. L., Olvera N. (2008) Validation of the Omni Scale of Perceived Exertion in a sample of Spanish-speaking youth from the USA. Perceptual and Motor Skills 107, 181-188. [DOI] [PubMed] [Google Scholar]
- Tabbers H. K., Martens R. L., van Merrienboer J.J.G. (2004) Multimedia instructions and cognitive load theory: effects of modality and cueing. British Journal of Educational Psychology 74, 71-81. [DOI] [PubMed] [Google Scholar]
- Tada A. (2018) Psychological effects of exercise on community-dwelling older adults. Clinical interventions in aging 13, 271-276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teixeira A. M., Ferreira J. P., Hogervorst E., Braga M. F., Bandelow S., Rama L., Figueiredo A., Campos M. J., Furtado G. E., Chupel M. U., Pedrosa F. M. (2016) Study Protocol on Hormonal Mediation of Exercise on Cognition, Stress and Immunity (PRO-HMECSI): Effects of Different Exercise Programmes in Institutionalized Elders. Frontiers in Public Health 4, 133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Utter A. C., Kang J., Nieman D. C., Dumke C. L., McAnulty S. R. (2006) Validation of Omni scale of perceived exertion during prolonged cycling. Medicine and Science in Sports and Exercise 38, 780-786. [DOI] [PubMed] [Google Scholar]
- Wasser J. G., Herman D. C., Horodyski M. B., Zaremski J. L., Tripp B., Page P., Vincent K. R., Vincent H. K. (2017) Exercise intervention for unilateral amputees with low back pain: study protocol for a randomised, controlled trial. Trials 18, 630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weijters B., Cabooter E., Schillewaert N. (2010) The effect of rating scale format on response styles: The number of response categories and response category labels. International Journal of Research in Marketing 27, 236-247. [Google Scholar]