

Abstract
Introduction
Hearing loss (HL) is common in the adult working population. It is widely assumed that diving is a risk factor for HL. However, studies with sufficient follow-up comparing HL in divers to non-divers are limited. This study aimed to assess the hearing threshold (HT) of Royal Netherlands Navy divers who had been diving for more than 15 years and to compare it to the ISO standard 7029:2017 reference table.
Methods
In this 25-year retrospective cohort study the Royal Netherlands Navy Diving Medical Centre audited the medical records of 1,117 Navy divers. Yearly dive medical assessments were performed according to professional standards, including audiometry. HTs were compared to the ISO 7029:2017 reference table, including Z-distribution, using paired t-tests.
Results
Thirty-five divers were included who had been diving for 15 years or longer. The HT increased significantly in nine of the 16 measured frequencies, while the Z-score decreased significantly in nine of the 16 tested frequencies (eight in both ears). In the 25-year follow-up the pattern was more obvious, with one significantly increased HT, and 10 significantly decreased Z-scores.
Discussion
The absolute HT increases after 15 years of military diving, but less than would be expected from normal age-related deterioration. Moreover, when comparing Z-scores, this sample of divers actually hear better than non-divers. We conclude that military diving is not an increased risk for HL compared to regular occupational hazards and suggest withdrawing the requirement for routine yearly audiometric evaluation as part of a dive medical examination.
Keywords: Fitness to dive, Health surveillance, Hearing loss, Audiology, Military diving
Introduction
“Divers have always been deaf, so the story goes”.[ 1] It is a common belief that divers suffer from hearing loss (HL). However, HL is common in the general population. Aside from a physiological age-related reduction in hearing threshold (HT), occupational exposure to noise is the largest cause for HL in the developed world.[ 2 , 3]
It has been hypothesized that diving, particularly changes in atmospheric pressure (and as a consequence the risks of ear barotrauma) and decompression sickness, affects hearing and thus increases divers’ risk for HL.[ 4] Many studies have reported that hearing thresholds are reduced in occupational and military divers.[ 5 - 12] In contrast, studies in sports divers have found no HL.[ 13 , 14] Exposure to loud noises, such as airflow or communication systems inside a diving helmet could also contribute to HL.[ 4 , 15] Most studies are cross-sectional and lack comparison to baseline data. Incidence varies from as high as 50% in self-reported questionnaires to 5% in patient-controlled trials. In some studies, the HL was more predominant in the left ear, while other studies have found the opposite.[ 7 , 16] A few longitudinal studies have been conducted, with follow up periods varying from two to twelve years. Results vary from no significant HL to a severe rise in HT.[ 9 , 17 , 18]
Additional factors affecting HL are smoking and ear, nose and throat (ENT) problems. Compared to the general population, divers experience more ENT problems, such as middle-ear barotrauma.[ 19 - 21] The literature is inconclusive on the matter of whether these ENT problems affect HT. With regard to smoking there is a little more evidence, however, it is unclear if smoking induces HL by itself or accentuates HL after noise exposure. Sung et al. found a possible dose-response relationship between smoking and HL in the low-frequencies.[ 22 , 23] Even though the HL was statistically significant in this study, the clinical relevance of an increase of HT of 1 or 2 dB is debatable.
As the HT increases with age, it is often difficult to assess whether HL has been the result of noise exposure or physiological ageing. To better compare HL to a reference group, the ISO 7029:2017 standard provides equations to describe HL as a variance of a normal distribution (Z-score).[ 3] This is increasingly common in other fields of medicine, such as pulmonary medicine.[ 24] Recently, a study by Sames et al. used these equations and found no significant difference in HL between longitudinally assessed occupational divers and expected age-related changes.[ 25]
In this 25-year retrospective cohort study we assessed the HL in military divers and compared this to the HL in the common working population using the ISO standard 7029:2017, both as absolute dB-values and as Z-scores. We hypothesized that HL in divers is equal to the general working population.
Methods
The Medical Ethics Committee affiliated with the Amsterdam University Medical Centre approved our methods for handling personal details and privacy and concluded that they were concordant with the guidelines of the Association of Universities in the Netherlands and the Declaration of Helsinki (document reference: W19-033).
DATA COLLECTION
The Royal Netherlands Navy Diving Medical Centre performs yearly medical assessments of military divers in compliance with international professional standards.[ 26] When entering the service as a navy diver, the candidate should have no significant hearing loss and no history of severe ENT problems, such as Meniere’s disease or surgical procedures.
Since the introduction of an electronic file system in 1993 up to 31 December 2018, 1,117 Navy divers had been assessed on more than one occasion. From this database audiometric data from divers who had dived for more than 15 years were selected. Audiometric data of divers that started diving before the introduction of the electronic file system were extracted from the paper archives.
The audiometric data of all Navy divers up to the age of 50 with a diving career of 15 years or longer were entered in an electronic database. Using the calculations provided in the ISO 7029:2017 standard, we computed the age-adjusted Z-scores. Cases with missing audiometric data or divers with non-diving related ENT problems, such as sudden deafness or perceptive hearing loss, were excluded. Also, divers who had already left military service at the time of the study could not be included, since their medical file was off-site for long term storage and not available for research. In contrast to many other studies, we chose not to exclude middle-ear barotrauma or successfully treated vestibular decompression sickness, since it is related to diving and possibly can induce hearing loss.
ANALYSIS
Audiometric data acquired when starting a career as a diver were considered as baseline. Data from fifteen (or 20 or 25 if applicable) years later were recorded. Data was registered both as hearing threshold (i.e., the level at which a subject hears a certain frequency) as well as standardized as deviation from the mean (Z-score). Statistical analyses were performed with SPSS Statistics for Windows (IBM Corp; Armonk, NY: 2015, version 23.0), using paired-samples t-tests for hypothesis testing. The alpha value was set at 0.05 and therefore statistical significance was assumed when P < 0.05.
Results
The 1,117 identified Navy divers had been diving for 7.8 years on average (median: 6, IQR: 3–11); 104 of them had been diving for 15 years or longer. Six cases were excluded due to acute sudden deafness, perceptive hearing loss or non-dive ENT related problems. More than half of the eligible divers had already left military service and their file was not available for research purposes. After exclusion (see Figure 1) 35 divers were included.
Figure 1.
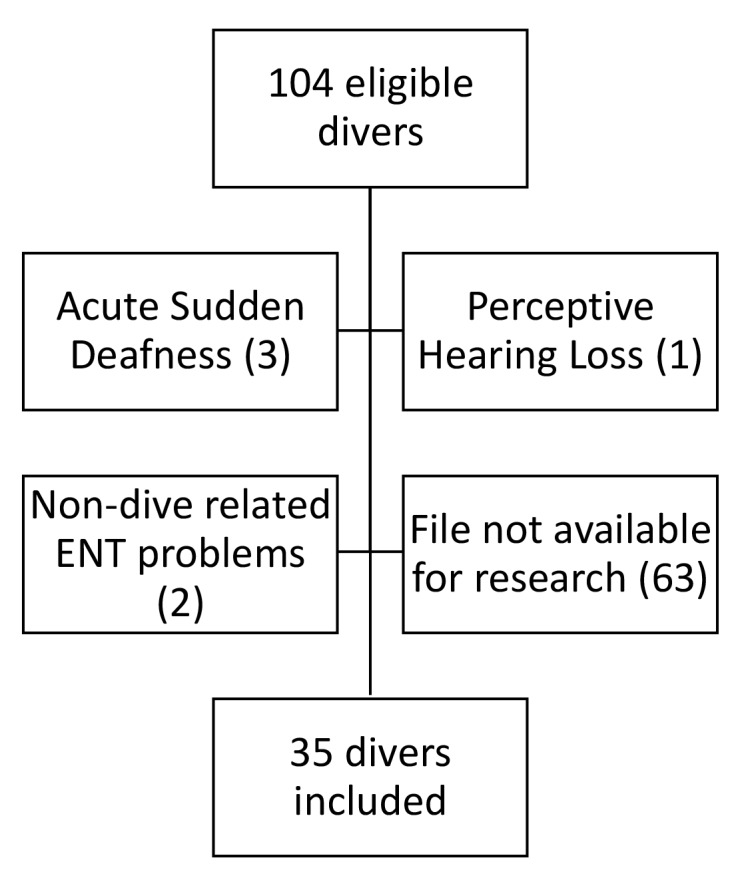
Flowchart to illustrate subject selection
Of these 35 subjects, 21 had been diving for more than 20 years and nine had been diving for more than 25 years. Baseline data on hearing threshold and associated Z-scores are displayed in Table 1. Tables 2, 3, 4 display the same data with delta values (compared to baseline) at 15, 20 and 25 year follow up respectively. Any statistically significant increase or decrease of hearing threshold or Z-score compared to baseline have been marked with an asterisk (*). Please note that due to decreasing numbers of subjects in the 20 and 25-year follow-up groups, delta values are slightly different than when manually calculated from the displayed data in the tables.
Table 1. Hearing thresholds as absolute values and Z-scores (with 95% CI): baseline values .
| Frequency | Left | Right | ||
| dB (95% CI) | Z-score (95% CI) | dB (95% CI) | Z-score (95% CI) | |
| 250 Hz | 4.9 (-0.7–10.5) | 0.62 (-0.38–1.62) | 3.6 (-1.4–8.6) | 0.48 (-0.4–1.36) |
| 500 Hz | 5.9 (-0.2–12) | 0.86 (-0.21–1.93) | 6.8 (1.2–12.4) | 1.09 (0.09–2.09) |
| 1 Hz | 5.5 (-0.4–11.4) | 0.88 (-0.19–1.95) | 7 (1.9–12.1) | 1.16 (0.19–2.13) |
| 2 Hz | 7.3 (-0.7–15.3) | 1.34 (-0.14–2.82) | 6.7 (0.6–12.8) | 1.21 (0.05–2.37) |
| 3 Hz | 7.1 (-1.3–15.5) | 1.24 (-0.29–2.77) | 4.7 (-2.7–12.1) | 0.77 (-0.6–2.14) |
| 4 Hz | 10.6 (1.4–19.8) | 1.82 (0.21–3.43) | 7.2 (-4.4–18.8) | 1.2 (-0.83–3.23) |
| 6 Hz | 5.1 (-4.6–14.8) | 0.67 (-0.98–2.32) | 6.3 (-1.6–14.2) | 0.9 (-0.58–2.38) |
| 8 Hz | 4.7 (-4.2–13.6) | 0.51 (-0.89–1.91) | 5.5 (-2.9–13.9) | 0.73 (-0.63–2.09) |
Table 2. Hearing thresholds as absolute values and Z-scores (with 95% CI): 15 year follow up (n = 35, mean age 37.5, SD 3.2 years). Statistically significant values have been marked with an asterisk. * P < 0.05, ** P < 0.01, *** P < 0.001 .
| Frequency | Left | Right | ||
| dB (95% CI) delta | Z-score (95% CI) delta | dB (95% CI) delta | Z-score (95% CI) delta | |
| 250 Hz | 1.2 (-5.1–7.5) -3.7 ** | 0.15 (-1.39–0.15) -0.47 | 1 (-4.1–6.1) -2.6* | 0.05 (-1.19–1.29) -0.43 |
| 500 Hz | 1.4 (-6.3–9.1) - 4.5 ** | 0.11 (-1.66–0.11) -0.75* | 1 (-5.2–7.2) -5.8*** | 0.02 (-1.36–1.4) -1.07*** |
| 1 Hz | 5 (-2.1–12.1) -0.5 | 0.68 (-0.77–0.68) -0.2 | 2.4 (-3.1–7.9) -4.6*** | 0.2 (-0.94–1.34) -0.96*** |
| 2 Hz | 5.6 (-3.6–14.8) -1.7 | 0.48 (-1.24–0.48) -0.86** | 4 (-2.8–10.8) -2.7** | 0.25 (-1.03–1.53) - 0.96*** |
| 3 Hz | 8.7 (-3.4–20.8) +1.6 | 0.78 (-1.19–0.78) -0.46 | 4 (-6.3–14.3) 0.7 | -0.04 (-1.79–1.71) -0.82*** |
| 4 Hz | 9.7 (-1.7–21.1) -0.9 | 0.71 (-0.92–0.71) -1.11*** | 7.6 (-4.6–19.8) +0.4 | 0.34 (-1.45–2.13) -0.86** |
| 6 Hz | 17.1 (3.7–30.5) +12 *** | 1.33 (-0.31–1.33) +0.66 | 15.6 (2.2–29) +9.3*** | 1.11 (-0.52–2.74) +0.21 |
| 8 Hz | 4.7 (-5–14.4) 0 | -0.26 (-1.42–0.9) -0.77** | 5.3 (-5.5–16.1) -0.2* | -0.22 (-1.45–1.01) -0.95** |
Table 3. Hearing thresholds as absolute values and Z-scores (with 95% CI): 20 year follow up (n = 21, mean age 41.9, SD 2.6 years). Statistically significant values have been marked with an asterisk. * P < 0.05, ** P < 0.01, *** P < 0.001 .
| Frequency | Left | Right | ||
| dB (95% CI) delta | Z-score (95% CI) delta | dB (95% CI) delta | Z-score (95% CI) delta | |
| 250 Hz | 4.3 (-3.5–12.1) -1.9 | 0.88 (-0.99–0.88) -0.04 | 4.1 (-3.1–11.3) +0.2 | 0.87 (-0.99–2.73) +0.32 |
| 500 Hz | 2.4 (-5.8–10.6) -4* | 0.28 (-1.59–0.28) -0.65 | 1.4 (-4.1–6.9) -5.3*** | 0.03 (-1.22–1.28) -1.07*** |
| 1 Hz | 5.5 (-4.2–15.2) -0.9 | 0.64 (-1.35–0.64) -0.43 | 3.1 (-2.5–8.7) -4.0* | 0.15 (-1–1.3) -1.02 |
| 2 Hz | 6.2 (-3.4–15.8) -1.2 | 0.22 (-1.47–0.22) -1.11** | 2.4 (-5.3–10.1) -3.8** | -0.34 (-1.79–1.11) -1.44*** |
| 3 Hz | 11.9 (-3.5–27.3) +4.8* | 0.95 (-1.37–0.95) -0.3 | 4.5 (-7.3–16.3) +1.7 | -0.19 (-2.07–1.69) -0.63 |
| 4 Hz | 11.9 (-2.1–25.9) +1.3 | 0.43 (-1.51–0.43) -1.4** | 10 (-5.1–25.1) +3.1 | 0.16 (-1.94–2.26) -1.01 * |
| 6 Hz | 18.1 (4.8–31.4) +12.2** | 0.80 (- 0.73–0.8) -0.05 | 16.2 (4.9–27.5) +8.8** | 0.64 (-0.68–1.96) -0.49 |
| 8 Hz | 9.8 (-3.5–23.1) +4.1 | -0.10 (-1.54–1.34) -0.73* | 6.4 (-4.7–17.5) +1.6 | -0.54 (-1.85–0.77) -1.13** |
Table 4. Hearing thresholds as absolute values and Z-scores (with 95% CI): 25 year follow up (n = 9, mean age 46.1, SD 2.3 years). Statistically significant values have been marked with an asterisk. * P < 0.05, ** P < 0.01, *** P < 0.001 .
| Frequency | Left | Right | ||
| dB (95% CI) delta | Z-score (95% CI) delta | dB (95% CI) delta | Z-score (95% CI) delta | |
| 250 Hz | 6.1 (-2.5–14.7) +2.4 | 0.88 (-0.99–0.88) +0.65 | 5.6 (-1.7–12.9) +1.2 | 0.87 (-0.99–2.73) +0.43 |
| 500 Hz | 1.7 (-5.8–9.2) -5.3 | 0.28 (-1.59–0.28) -1.16 | 2.2 (-3.5–7.9) -3.40 | 0.03 (-1.22–1.28) -0.96* |
| 1 Hz | 5 (-3.2–13.2) -0.1 | 0.64 (-1.35–0.64) -0.6 | 2.8 (- 2.9–8.5) -3.70 | 0.15 (-1–1.3) -1.13* |
| 2 Hz | 5 (-6.2–16.2) -1.8 | 0.22 (-1.47–0.22) -1.52** | 2.2 (- 4.9–9.3) -4.40 | -0.34 (-1.79–1.11) -1.82*** |
| 3 Hz | 3.9 (-5.3–13.1) -0.7 | 0.95 (-1.37–0.95) -1.45** | 0 (-7.1–7.1) -1.3 | -0.19 (-2.07–1.69) -1.32* |
| 4 Hz | 12.2 (1.3–23.1) +1.9 | 0.43 (-1.51–0.43) -1.75** | 6.7 (-8.1–21.5) -0.6 | 0.16 (-1.94–2.26) -1.83** |
| 6 Hz | 19.4 (7.3–31.5) +11.0 * | 0.8 (-0.73–0.8) -0.68 | 15.1 (6.3–23.9) +4.60 | 0.64 (-0.68–1.96) -1.6** |
| 8 Hz | 11.7 (-1.6–25) +4.4 | -0.1 (-1.54–1.34) -1.11 | 6.1 (-4.1–16.3) -0.9 | -0.54 (-1.85–0.77) -1.79** |
Visual representations of the data are given in Figures 2, 3, 4, 5. These figures combine the 7029:1017 reference values with the collected data.
Figure 2.

Hearing thresholds (with 95% CI) vs. ISO 7029:1017 reference values (with SD): baseline values
Figure 3.

Hearing thresholds (with 95% CI) vs. ISO 7029:1017 reference values (with SD): 15 year follow up
Figure 4.

Hearing thresholds (with 95% CI) vs. ISO 7029:1017 reference values (with SD): 20 year follow up
Figure 5.

Hearing thresholds (with 95% CI) vs. ISO 7029:1017 reference values (with SD): 25 year follow up
Discussion
Hearing thresholds increased after 15 years of military diving, but not by more than the general working population. Increased hearing thresholds were more common at 6kHz, the typical frequency for noise-induced hearing loss, however, in comparison with age-adjusted norms, divers’ hearing was better than that of the general population. At the lower frequencies (500, 1000 and 2000 Hz) hearing thresholds decreased or remained almost unchanged. This effect is more profound after 20 or 25 years’ diving.
In some previous studies a longitudinal decrease in hearing thresholds has been described at the lower frequencies.[ 18 This has been attributed to the learning effect of frequently performing pure tone audiometry.[ 27] Also similar to other studies is the greater HL at 4 to 8 kHz,[ 7 , 8 , 11] but our absolute increase of HT is less than most previous studies. In line with the findings of Sames et al., we conclude that HL after 15–25 years of diving is less than might be expected from age-related decrease.[ 25]
In comparison to previous studies of divers, our different results could perhaps be attributed to increased awareness and usage of protective measures to prevent hearing loss. Many of the previous studies were conducted as long as 30 years ago. Technology to reduce noise generated from airflow and communication systems has been improved significantly over the years. Given the fact that underwater noise has more effect when ears are directly exposed in-water, the increased usage of helmet diving could also reduce HL.[ 15 , 28] An alternative explanation could be that military divers are relatively less exposed to underwater noise than commercial divers. Indeed, the tasks of military divers included relatively noise-free activities such as clearance diving and ship inspections. However, this explanation is unlikely because our population included Navy divers with a history of exposure to explosions, construction work or handling firearms.[ 10 , 16]
This study incorporated evaluation of HL as an age-corrected normal distribution. While an absolute increase of hearing threshold is easier to interpret, the Z-score ranks the individual patient against peers of the same age. Although natural deterioration due to ageing leads to increased hearing thresholds even in healthy individuals, we would like to emphasize that clinicians should still encourage their patients to wear hearing protection when they are exposed to noisy working environments. It is important to keep in mind that high incidences of self-reported HL could possibly be the result of awareness in patients due to successful preventive medicine, and not audiometric abnormalities.[ 10 , 12]
Many professional standards recommend yearly audiometric evaluation in divers. Our data suggest military diving is not an additional risk factor for HL. Some other studies suggest only very small increases of HT.[ 22 , 23] The clinical relevance of these very small changes in HT is doubtful. Also, the value of routine annual medical examinations has been questioned.[ 25 , 29] We feel our data support the policy in some countries to reduce the frequency of dive medical examinations, or at least perform audiometry ‘on indication’, for instance after noise exposure or barotrauma, and not as a routine investigation. Our data cannot give an evidence-based suggestion for the optimal frequency of audiometric investigation. The Royal Netherlands Navy considers that once every five years, or earlier when indicated, is frequent enough to monitor long term health effects of military divers. This is in line with current policy in New Zealand and the UK for occupational divers.[ 25 , 26]
STRENGTHS AND LIMITATIONS
To our knowledge the present study is the first to evaluate hearing loss after 25 years of military diving. With increasing age of occupational divers these data are relevant for both clinicians and divers. Additionally, approaching HL as a normal distribution allows a more contextually accurate evaluation of hearing change compared with absolute changes in hearing thresholds.
Some limitations also need to be addressed. Firstly, this study did not include data describing depth and number of dives. Our population typically dives up to a depth of 80 metres’ sea water with helium-oxygen gas mixtures, but additional research is required to evaluate whether our results can be translated to saturation divers or alternative breathing gases. Secondly, the small sample in the 20 and 25 year follow up group (21 and 9 respectively) could possibly leave our study unable to detect small changes compared to the reference group. However, the clinical relevance of very small statistically significant differences is doubtful. Lastly, small samples could make this study susceptible to selection bias as a result of the ‘healthy worker effect’, where individuals with health issues, hearing loss being one of them, are more likely to discontinue diving than their healthy colleagues. And while our electronic file system is not able to screen for the individuals excluded for ENT-problems, our general experience is that ENT-problems are seldom a reason to be discharged from diving.
Conclusions
The present study is the longest longitudinal analysis of HL in navy divers. While the absolute HT increases at 6 kHz after 15 to 25 years of military diving, this is well within the range of physiological hearing deterioration. While our sample is small, the results agree with the study by Sames et al. We conclude that military diving does not seem to be an additional hazard for developing HL compared to general occupational hazards. At longer follow-up periods, this effect becomes more pronounced, with divers age-adjusted hearing being better than 20 or 25 years earlier. This could be the result of effective awareness and usage of hearing protection. We encourage clinicians to adopt the normal distribution as given in the ISO-7029 standards to evaluate changes in HL in divers more accurately, and to reduce the frequency of mandatory audiometric testing in healthy divers.
Footnotes
Conflict of interest and funding: nil
Contributor Information
Thijs T Wingelaar, Diving Medical Center, Royal Netherlands Navy, Den Helder, the Netherlands; Department of Anesthesiology, Amsterdam University Medical Center, Amsterdam, the Netherlands.
Edwin L Endert, Diving Medical Center, Royal Netherlands Navy, Den Helder, the Netherlands.
Rigo Hoencamp, Department of Surgery, Alrijne Hospital, Leiderdorp, the Netherlands; Defense Healthcare Organisation, Ministry of Defence, Utrecht, the Netherlands; Leiden University Medical Center, Leiden, the Netherlands.
Peter-Jan AM van Ooij, Diving Medical Center, Royal Netherlands Navy, Den Helder, the Netherlands.
Rob A van Hulst, Department of Anesthesiology, Amsterdam University Medical Center, Amsterdam, the Netherlands.
References
- Bornmann RC. Symposium on decompression sickness and its therapy . Allentown (PA): USA; 1979. [Google Scholar]
- Prevention of deafness and hearing loss (A70/34). Seventieth World Health Assembly Geneva, Switzerland: World Health Organisation; 2017. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_R13-en.pdf [cited 2019 March 18]. [Google Scholar]
- International Organization for Standardization. (ISO 7029:2017) Acoustics – Statistical distribution of hearing thresholds related to age and gender Geneva, Switzerland; 2017. Available from: https://www.iso.org/standard/42916 [cited 2019 March 18]. [Google Scholar]
- Goplen FK. Thesis: Effects of diving on hearing and balance. Bergen, Norway: University of Bergen; 2010. Available from: http://bora.uib.no/handle/1956/4841 [cited 2019 March 18]. [Google Scholar]
- Molvaer OI, Lehmann EH. Hearing acuity in professional divers . Undersea Biomed Res. 1985;12:333–49. [PubMed] [Google Scholar]
- Ross JA, Macdiarmid JI, Osman LM, Watt SJ, Godden DJ, Lawson A. Health status of professional divers and offshore oil industry workers . Occup Med (Lond) 2007;57:254–61. doi: 10.1093/occmed/kqm005. [DOI] [PubMed] [Google Scholar]
- Skogstad M, Eriksen T, Skare Ø. A twelve-year longitudinal study of hearing thresholds among professional divers . Undersea Hyperb Med. 2009;36:25–31. [PubMed] [Google Scholar]
- Macdiarmid JI, Ross JA, Taylor CL, Watt SJ, Adie W, Osman LM, et al. Examination of the long term health impact of diving: The ELTHI diving study . Hampshire (UK): Health and Safety Executive; 2007. [Google Scholar]
- Goplen FK, Aasen T, Gronning M, Molvaer OI, Nordahl SH. Hearing loss in divers: a 6-year prospective study . Eur Arch Otorhinolaryngol. 2011;268:979–85. doi: 10.1007/s00405-011-1486-1. [DOI] [PubMed] [Google Scholar]
- Abid AH, Al-Asadi JN, Habib OS. Hearing loss in Iraqi divers . Med J Basrah University. 2006;24:1–5. doi: 10.33762/mjbu.2006.46419. [DOI] [Google Scholar]
- Chung J, Brugger J, Curley MD, Wallick M, Perkings R, Regis D, et al. Health survey of US Navy divers from 1960 to 1990: A first look. Technical report 11/11. Panama City (FL): Navy Experimental Diving Unit; 2011. [Google Scholar]
- Ross JA, Macdiarmid JI, Dick FD, Watt SJ. Hearing symptoms and audiometry in professional divers and offshore workers . Occup Med. 2010;60:36–42. doi: 10.1093/occmed/kqp152. [DOI] [PubMed] [Google Scholar]
- Hausmann D, Laabling S, Hoth S, Plinkert PK, Klingmann C. Assessment of the central hearing system of sport divers . Undersea Hyperb Med. 2011;38:527–35. [PubMed] [Google Scholar]
- Klingmann C, Knauth M, Ries S, Tasman AJ. Hearing threshold in sport divers: is diving really a hazard for inner ear function? . Arch Otolaryngol Head Neck Surg. 2004;130:221–5. doi: 10.1001/archotol.130.2.221. [DOI] [PubMed] [Google Scholar]
- Nedwell JR, Mason TI, Collett AG, Gardiner RW. Noise exposure of commercial divers in the Norwegian sector of the North Sea . Undersea Hyperb Med. 2015;42:151–8. [PubMed] [Google Scholar]
- Bohnker B, Rovig G, Page J, Philippi A, Butler F, Sack D. Navy hearing conservation program: hearing threshold comparisons to Navy SEALS and divers . Undersea Hyperb Med. 2003;30:155–62. [PubMed] [Google Scholar]
- Chng J, Chan G, Tang KC. Does diving affect the hearing of Asian military divers? A study in the Republic of Singapore Navy . Undersea Hyperb Med. 2014;41:41–7. [PubMed] [Google Scholar]
- Molvaer OI, Albrektsen G, Kriem B. Hearing deterioration in professional divers: an epidemiologic study . Undersea Biomed Res. 1990;17:231–46. [PubMed] [Google Scholar]
- Wingelaar TT, van Ooij PA, van Hulst RA. Otitis externa in military divers: more frequent and less harmful than reported . Diving Hyperb Med. 2017;47:4–8. doi: 10.28920/dhm47.1.4-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evens RA, Bardsley B, Becker K, C Manchaiah VK. Auditory complaints in scuba divers: an overview . Indian J Otolaryngol Head Neck Surg. 2012;64:71–8. doi: 10.1007/s12070-011-0315-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lechner M, Sutton C, Fishman JM, Kaylie DM, Moon RE, Masterson L, et al. Otorhinolaryngology and diving-Part 1: Otorhinolaryngological hazards related to compressed gas scuba diving: A Review . JAMA Otolaryngol Head Neck Surg. 2018;144:252–8. doi: 10.1001/jamaoto.2017.2617. [DOI] [PubMed] [Google Scholar]
- Sung JH, Sim CS, Lee CR, Yoo CI, Lee H, Kim Y, et al. Relationship of cigarette smoking and hearing loss in workers exposed to occupational noise . Ann Occup Environ Med. 2013;25:8. doi: 10.1186/2052-4374-25-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nomura K, Nakao M, Morimoto T. Effect of smoking on hearing loss: quality assessment and meta-analysis . Prev Med. 2005;40:138–44. doi: 10.1016/j.ypmed.2004.05.011. [DOI] [PubMed] [Google Scholar]
- Wingelaar TT, Clarijs P, van Ooij PA, Koch DA, van Hulst RA. Modern assessment of pulmonary function in divers cannot rely on old reference values . Diving Hyperb Med. 2018;48:17–22. doi: 10.28920/dhm48.1.17-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sames C, Gorman DF, Mitchell SJ, Zhou L. The impact of diving on hearing: a 10-25 year audit of New Zealand professional diver . Diving Hyperb Med. 2019;49:2–8. doi: 10.28920/dhm49.1.2-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health and Safety Executive . The medical examination and assessment of commercial divers (MA1, rev 4). Hampshire (UK): Health and Safety Executive; 2015. Available from: http://www.hse.gov.uk/pubns/ma1.htm. [cited 2019 March 18]. [Google Scholar]
- Royster JD, Royster LH. Using audiometric data base analysis . J Occup Med. 1986;28:1055–68. doi: 10.1097/00043764-198610000-00029. [DOI] [PubMed] [Google Scholar]
- Anthony TG Wright NA Evans MA Review of diver noise exposure (RR735) Hampshire (UK): Health and Safety Executive; 2009. Available from: http://www.hse.gov.uk/research/rrpdf/rr735.pdf. [cited 2019 March 18]. [Google Scholar]
- Sames C, Gorman D, Mitchell S, Sandiford P. An evidence-based system for health surveillance of occupational divers . Intern Med J. 2016;46:1146–52. doi: 10.1111/imj.13204. [DOI] [PubMed] [Google Scholar]