

Abstract
OBJECTIVE:
To assess the prevalence of malocclusion and orthodontic treatment needs in a Saudi sample of Jeddah city.
MATERIALS AND METHODS:
A cross-sectional (descriptive) study was performed in 2017 among 3016 subjects (1507 females and 1509 males) selected according to stratified random sampling design. The inclusion criteria were Saudi students aged between 14-18 years with no craniofacial deformities or syndromes and no orthodontic treatment carried out. Malocclusion was assessed using the modified Bjork et al. system, and Angle's classification and orthodontic treatment need to be evaluated by using the IOTN (DHC). Descriptive, associations and gender differences were assessed by one-way ANOVA, Chi-square, and Fisher exact tests. Data was analyzed using STATA version 13.0 (StataCorp, College Station, Texas, USA). Statistical significance was set at P < 0.05.
RESULTS:
Approximately 12% of the participants had normal occlusion, 57% had Class I malocclusion, 17% had Class II malocclusion, and 14% had Class III malocclusion. The highest prevalence of malocclusion traits was for displacement, followed by a crossbite. The IOTN results revealed slight need for orthodontic treatment in (n = 795-26%) moderate/borderline in (n = 1166-39%), and great need in (n = 1055-35%). Class II and III malocclusion, OJ, reverse overjet, scissor bite, open bite, midline discrepancies, and crowding were significantly higher in males than females (P < 0.05).
CONCLUSION:
Overall, there was a high prevalence of malocclusion and high orthodontic treatment need. The most common malocclusion was Class I. The most common orthodontic treatment need was moderate to borderline.
Keywords: IOTN (DHC), KSA, malocclusion, prevalence
Introduction
In dentistry, malocclusion is described as a mal-relationship between dental arches in any of the dimensions or the presence of anomalies in tooth position. Malocclusion can be regarded as a condition affecting oral health, leading towards increment in dental caries, periodontal diseases, possible Temporomandibular disorder (TMD), and psychosocial problems or other serious risks to oral health and hygiene.[1,2] According to the World Health Organization (WHO), malocclusion is the third-highest oral health concern around the globe. It is essential to note that malocclusion, dental, and periodontal disease has been designated as the most prevalent categories of oral pathologies. The etiology of a malocclusion involves both genetic and environmental factors, and due to the possible geographic aspects in the distribution of malocclusion, epidemiological studies of malocclusion conducted elsewhere out the premises of KSA are not of much use, since they were conducted among different populations in different environmental conditions and climatic variations.[3] Angle classified the normal occlusion and malocclusion according to molar relationship into; normal occlusion, Class I malocclusion, Class II malocclusion with two divisions according to incisors angulation (division I and II), and Class III malocclusion.[4] As recommended by the American Academy of Orthodontics (AAO), the conduction of orthodontic examination must be ensured for 7 year old children, because by analyzing the physical aspects of teeth, an expert can determine whether or not the child is at risk of malocclusion.[5] The early examination might also assist in the investigation and initiation of treatment during childhood, thus reducing the negative consequences on the health and well-being of patients as well as minimizing the severities related to dental and skeletal malformations.[6] In Saudi Arabia, the prevalence of malocclusion varies from one region to another due to a variety of factors, including racial, ethical, social, and environmental considerations.[7] Within the context of Saudi Arabia, a variety of studies assessed the prevalence of malocclusion, patterns of dental malocclusion and orthodontic treatments needs,[5,6,7,8,9,10,11,12] for the purpose of acquiring baseline features related to the occlusion characteristics of the population for the establishment of techniques and strategies related to their orthodontic services.[10] Previous studies indicated that the prevalence of malocclusion, along with other dental anomalies, is significantly higher among diversified age groups of the Saudi population. Findings also demonstrated that the needs of orthodontic treatment for the Saudi population are significantly high. Therefore it is imperative to establish strategies for the provision of appropriate treatment for the Saudi population. During recent years, the number of patients acquiring orthodontic treatment had been significantly increased. In this regard, it remains crucial to collect relevant epidemiological data for assessing treatment needs among the Saudi population. Furthermore, there is also a need to establish and implement diversified strategies for controlling the prevalence of this disorder. The indices of malocclusion pose several problems, including the multi-factorial nature of malocclusion, the difficulty in standardizing criteria, and the indication that malocclusion cannot be judged solely on physical terms. The psychological and social impacts of malocclusion are difficult to detect, predict, and quantify.[13] Despite those problems, several indices of malocclusion have been developed and have been used for the following: Diagnostic classification; Epidemiological indices; Treatment Need (treatment priority) and Treatment success (outcome).[14]
To measure the need for orthodontic treatment, the Index of Orthodontic Treatment Need (IOTN) was used in this study. The index determines the ranking of malocclusion in terms of its occlusal characteristics depending on the extent to which perceive dental and aesthetic impairment is identified. This index further helps in identifying those subjects in a population that can markedly benefit from an orthodontic treatment regime. The Index incorporates a Dental Health Component (DHC) and an Aesthetic Component (AC). However, in this study, only the DHC is used to assess the orthodontic needs of the participants. Brook and Shaw[15] have developed the Dental Health Component (DHC) and roughly modeled on the Index of the Swedish Dental Board (Linder-Aronson, 1974). It is imperative to note that DHC is a modified version of an index formerly known as the Swedish index and was initially meant to guide the implementation of practical implications necessary to make clinically sound judgments in orthodontic care delivery. The DHC was also developed with the intention to minimize this subjectivity in subsequent dental measurements to determine alignment and occlusal deformities. It also records the various occlusal traits of malocclusion, which are intended to increase the morbidity of the dentition and surrounding structures.[15]
The Aim of the Study
To assess a Saudi sample aged from 14-18 years, living in Jeddah city, Kingdom of Saudi Arabia, the following variables:
Prevalence of malocclusion based on modified Bjork et al.[16] system and Angle's classification
Orthodontic treatment needs to be based on the IOTN (DHC) index.
Methods
Study design
A cross-sectional descriptive study was performed in four geographic areas of Jeddah city (Northern, Southern, Eastern, and Western). All schools were first contacted, and based on their response, they were then randomly filtered to 8 schools from each geographic area as follows: 4 Intermediate and 4 high governmental.
Study subject selection
Subjects were chosen based on the following inclusion criteria; Saudi students aged between 14-18 years with no craniofacial deformities or syndromes and no orthodontic treatment carried out.
Sample size calculation
Based on the literature, the alpha level was set at 0.05 (two-sided test), and the confidence level was set at 95 percent. Based on the formula n =t 2 P (1 − p)/m2, the calculated needed sample size for Class I malocclusion was 288, for Class II malocclusion was 185, and for Class III malocclusion was 150; hence, the total needed sample size was calculated to be 623 participants. However, to accommodate the effect of multiple variables, including gender and different occlusal traits, the current study aimed to reach a sample size of more than 4 times the calculated sample size.
Assessment of malocclusion
Modified Bjork et al.[16] system It was developed based on a qualitative registration of the following anomalies:
Sagittal discrepancy (Anterior crossbite, Bimaxillary protrusion {Angle Class I with lip strain over protruded teeth}, Distocclusion {Angle Class II}, Mesiocclusion {Angle Class III}, Overjet (0 mm = edge to edge, 4-6 mm = moderate, >6 mm = severe). However, the current study used Angle's classification for recording the malocclusion classification.
Transverse discrepancy (scissors bite, posterior crossbite, midline shift {recorded when >2 mm}).
Vertical discrepancy (overbite {0 mm = edge to edge, 4-6 mm = moderate, greater than 6 mm = severe}).
Space discrepancy (recorded when 2 mm spacing in both arches or more crowding).
Angle's classification4
Angle4 classified the normal occlusion and malocclusion into:
-
Normal occlusion which defined as a normal molar relationship
(Mesiobuccal cusp of the upper 1st molar occludes in the buccal groove of the lower 1st molar) without crowding, spacing and rotations, or other dental abnormalities
Class I malocclusion which defined as a normal occlusion but with crowding, spacing, and rotations, or other dental abnormalities
-
Class II malocclusion which defined as a distobuccal cusp of the upper 1st molar occludes in the buccal groove of the lower 1st molar and divided into:
- Class II division 1 malocclusion with protrude maxillary incisors
- Class II division 2 malocclusion with retruded maxillary incisors
- Class II malocclusion subdivision right or left, which is Class I malocclusion in one side and Class II on another side.
Class III malocclusion, which defined as a mesiobuccal cusp of the upper 1st molar occludes in between the lower 1st molar and 2nd molar, and it has another category which is Class III malocclusion subdivision right or left, and that is Class I malocclusion in one side and Class III in another side.
Assessment of treatment needs
DHC of the IOTN
The index of orthodontic treatment need (IOTN) is a recording framework for malocclusion, created by Brook and Shaw.[16] It comprises of dental health component (DHC) and aesthetic component (AC). The DHC is considered a reliable five-grade index (Appendix B). Grade 1 represents a minimum need for orthodontic treatment, while Grade 5 indicates a great need for orthodontic treatment. Various features or traits of malocclusion are recorded in the DHC. The current study only assessed the following occlusal traits; overjet, reverse overjet, overbite, displacement, missing teeth, open bite, crossbite and scissor bite. The traits of cleft lip and palate, as well as hypodontia, were part of the exclusion criteria. The “pre and post-normal occlusion” were assessed following Angle's classification and not through the IOTN (DHC) index.
There are two ways of recording the DHC. The first is to record the grade only. The second method provides more information regarding the prevalence of individual occlusal traits. For example, an overjet greater than 9 mm would be graded as 5a; wherein the Grade being 5 and the overjet designated by the letter ‘a.’ In the current study, the grades were grouped to indicate the priority for treatment as Grade 1: No treatment need; Grade 2-3: Borderline treatment need; and Grade 4-5: Great treatment need.
Materials
The examinations were conducted in the school nurse's room with student seated on a chair by using the kit of the IOTN [Figure 1], head flashlights (portable 60 Watt white-blue spectrum lamp) as the source of illumination, disposable gloves, masks, and Sterilized wooden tongue depressors. No radiographs were taken.
Figure 1.
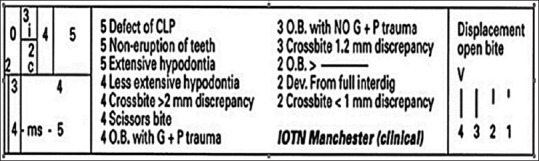
IOTN ruler
Ethical approval
Ethical approval was obtained from the Faculty of Dentistry, King Abdul-Aziz University (KAUFD), Jeddah, Saudi Arabia. Permission by the General Directorate of Education in Jeddah city was also obtained.
Calibration
The examination was conducted by six orthodontic residents (3 males and 3 females). Calibration between examiners was conducted on 20 patients who attended KAUFD clinics. Examiners were trained under the supervision of an expert faculty member who published 2 or more researches using IOTN. Examiners were also calibrated to standardize the diagnosis and assessment procedures. The collected variables were malocclusion type, overjet, reverse overjet, crossbite, scissor bite, open bite, deep bite, space condition, midline condition, and dental health component. Cohen Kappa coefficient was then calculated for inter-examiner reliability, and the results ranged from 0.85-1, indicating a good to almost perfect results.
Statistical analysis
Malocclusion type based on the modified Bjork et al. system
The malocclusion type was assessed on the following variables:
-
Angle's classification (Normal occlusion, Class I, Class II and
Class III malocclusion)
Overjet (edge to edge, moderate and severe overjet)
Scissor bite (scissor bite >2 mm)
Crossbite (anterior and posterior crossbite)
Midline shift >2 mm (upper and lower midline shift >2 mm)
Overbite (moderate and severe deep bite and open bite)
Crowding (upper and lower crowding >2 mm)
Spacing (upper and lower spacing >2 mm)
Descriptive statistics were done on all variables. Association between malocclusion type variables and gender were also assessed using Chi-square, Fischer's exact and One-way ANOVA tests.
Orthodontic treatment needs based on the DHC:
The occlusal traits were recorded and the treatment need was assessed using the IOTN (DHC) index 15 [Figure 1]. Moreover, the treatment need was grouped into the following groups as recommended in the literature review,[8] Hassan H,[9] Al Barakati et al.,[7] Aldrees,[11] AlQarni et al.,[17] Asiry[5] and Al Jobair (2016):
No or slight need (Grade 1)
Moderate or borderline need (Grade 2 and 3)
Great need (Grade 4 and 5).
Descriptive statistics were done on all groups. Association between treatment need groups and gender were also assessed using Chi-square, Fischer's exact and One-way ANOVA tests. Data entry was carried out manually using Microsoft Excel Version 2013, and statistical analysis was conducted using STATA Version 13.0 (StataCorp, College Station, Texas, USA). The significance level was set at P < 0.05.
Results
Sample distribution
The number of subjects examined was 3520 subjects. However, 504 subjects were excluded from the study because they didn’t match the inclusion criteria. The net sample size was 3016 (1507 females and 1509 males). The sample distribution is presented in Table 1. The mean age of the participants was 15.8 ± 1.4 years (ranged from 14-18 years), with equal gender distribution (M: 1509, 50.03%; F: 1507, 49.97%). The sample distribution according to the geographic area was almost equal; 760 (25.1%) subjects from the North area, 766 (25.4%) from the East area, 755 (25.1%) from the South area, and 735 (24.4%) from the West area.
Table 1.
Sample distribution (n=3016)
| Variables | Number |
|---|---|
| Age | |
| Mean±SD | 15.8±1.4 Years |
| Minimum | 14 years |
| Maximum | 18 years |
| Gender | |
| Male (n (%)) | 1509 (50.03%) |
| Female (n (%)) | 1507 (49.97%) |
| Regional distribution | |
| North (n (%) | 760 (25.1) |
| East (n (%)) | 766 (25.4%) |
| South (n (%)) | 755 (25.1%) |
| West (n (%)) | 735 (24.4%) |
Malocclusion distribution based on modified Bjork et al. system
The distribution of malocclusion in Saudi adolescence based on modified Bjork et al. system is presented in Table 2. The most prevalent malocclusion type was Class I malocclusion (n = 1718, 57%; M: 699, 23%; F: 1019, 34%), followed by Class II malocclusion (n = 518, 17%; M: 347, 11.5%; F: 171, 5.7%) distributed as 13% division 1 and 4% Division 2, followed by Class III malocclusion (n = 422, 14%; M: 286, 9.5%; F: 136, 4.5%). The least prevalent malocclusion type was normal Class I occlusion (n = 358, 12%; M: 177, 5.8%; F: 181, 6%). A significant difference was reported between genders in malocclusion classification (P < 0.001). The prevalence of overjet was found to be; 14% (n = 430) in the moderate category, 4% (n = 72) in the severe category, and 3.8% (n = 1140) were in the edge to edge category. Furthermore, a significantly higher percentage of males than females were found in the three categories (P < 0.001). The prevalence of scissor bite was found to be low (n = 47, 2%), with males significantly higher than females (P < 0.05). The prevalence of anterior crossbite was also found to be low (n = 178, 6%), with males significantly higher than females (P < 0.001). On the other hand, a quarter of the participants were diagnosed to have posterior crossbite (n = 764, 25%) with significantly more females (n = 429, 14%) than males (n = 335, 11%) (P < 0.001). A high prevalence of lower midline shift of more than 2 mm was reported (n = 1191, 39.5%; M: 672, 22%; F: 519, 17%), while a low prevalence of upper midline shift (n = 380, 13%; M: 245, 8.1%; F: 135, 4.5%) was reported. Males were significantly higher than females in both problems (P < 0.001). Almost one-quarter of the population showed moderate to severe deep bite (n = 851, 28.5%; M: 443, 15%; F: 408, 13.6%) with no significant difference between gender (P > 0.05). However, the prevalence of moderate to severe open bite (n = 308, 10%; M: 285, 9.5%; F: 23, 0.7%) was found to be low, also with no significant difference between gender. Almost half of the population had more than 2 mm crowding problems; the prevalence of upper crowding problem was found to be (n = 1382, 46%; M: 894, 30%; F: 488, 16%), while the prevalence of lower crowding problem was (n = 1518, 52%; M: 933, 31%; F: 648, 21.5%). Males showed significantly higher prevalence than females in crowding problems (P < 0.001). The prevalence of upper (n = 459, 15%; M: 224, 7%; F: 235, 7.8%) and lower (n = 336, 11%; M: 153, 5.1%; F: 183, 6.1%) spacing problems was found to be low with females being significantly higher than males (P < 0.05).
Table 2.
Distribution of malocclusion among 3016 Saudi Adolescence according to gender using modified Bjork et al. system
| Malocclusion type | Male | Female | Total | P | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Angle’s classification | |||||||
| Normal Class I | 177 | 5.8 | 181 | 6 | 358 | 12 | <0.001 |
| Class I malocclusion | 699 | 23 | 1019 | 34 | 1718 | 57 | |
| Class II malocclusion | 347 | 11.5 | 171 | 5.7 | 518 | 17 | |
| Class II Division1 | 238 | 7.9 | 150 | 5 | 388 | 13 | |
| Class II Division2 | 109 | 4 | 21 | 0.7 | 130 | 4 | |
| Class III malocclusion | 286 | 9.5 | 136 | 4.5 | 422 | 14 | |
| Overjet | |||||||
| Edge to edge 0mm | 49 | 21.6 | 65 | 2 | 114 | 3.8 | <0.001 |
| Moderate 4-6 mm | 250 | 8 | 180 | 5.9 | 430 | 14 | |
| Severe >6mm | 54 | 1.8 | 18 | 0.6 | 72 | 4 | |
| Scissor bite | |||||||
| Scissor bite >2mm | 31 | 1 | 16 | 0.5 | 47 | 2 | 0.02 |
| Crossbite | |||||||
| Anterior crossbite | 159 | 5.3 | 19 | 0.62 | 178 | 6 | <0.001 |
| Posterior crossbite | 335 | 11 | 429 | 14.2 | 764 | 25 | <0.001 |
| Midline shift >2mm | |||||||
| Upper midline shift | 245 | 8.1 | 135 | 4.5 | 380 | 13 | <0.001 |
| Lower midline shift | 672 | 22 | 519 | 17 | 1191 | 39.5 | <0.001 |
| Overbite | |||||||
| Moderate deep bite 4-6 mm | 416 | 14 | 389 | 13 | 805 | 27 | 0.35 |
| Severe deep bite >6 mm | 27 | 1 | 19 | 0.62 | 46 | 1.5 | |
| Moderate open bite 4-6 mm | 165 | 5.5 | 16 | 0.5 | 181 | 6 | 0.27 |
| Severe open bite >6 mm | 120 | 4 | 7 | 0.2 | 127 | 4 | |
| Crowding >2 mm | |||||||
| Upper crowding | 894 | 30 | 488 | 16 | 1382 | 46 | <0.001 |
| Lower crowding | 933 | 31 | 648 | 21.5 | 1581 | 52 | <0.001 |
| Spacing >2 mm | |||||||
| Upper spacing | 224 | 7 | 235 | 7.8 | 459 | 15 | <0.001 |
| Lower spacing | 153 | 5.1 | 183 | 6.1 | 336 | 11 | 0.02 |
Orthodontic treatment needs to be based on the IOTN (DHC)
Figure 2 further shows the overall orthodontic treatment needs to be based on the prevalence of occlusal traits as recorded by the IOTN (DHC) index. The slight need for orthodontic treatment was found in (795, 26%) of the subjects, moderate/borderline in (1166, 39%), and the great need for orthodontic treatment was found in (1055, 35%) of the study sample. Table 3 further shows the distribution of different occlusal traits based on the IOTN (DHC) index. The prevalence of occlusal trait in descending order was; displacement (n = 2290, 76%), increased overjet (n = 1412, 46.8%), crossbite (n = 903, 30%), increased overbite (n = 851, 28%), missing teeth (n = 631, 21%), open bite (n = 308, 10.2%), reversed overjet (n = 178, 5.9%), and the least was scissor bite (n = 47, 1.6%). Further analysis showed that the “no, slight” treatment need was significant for the increased overjet (n = 910, 30.2%) only (P < 0.001), while the “great” treatment need was significant in the missing teeth (n = 631, 21%) only (P < 0.001). On the other hand, the “moderate/borderline” treatment need was significant in the following occlusal traits; displacement (n = 1027, 34%), increased overbite (n = 805, 27%), crossbite (n = 583, 19%), open bite (n = 285, 9.5%), reversed overjet (n = 161, 5.3%) (P < 0.001). Table 4 illustrates the association between treatment needs using the IOTN (DHC) and gender difference. A significant difference was reported between males and females in their orthodontic treatment needs according to the IOTN (DHC) index (P < 0.05). Males were significantly higher than females in the great needs category (M: 600, 20%; F: 455, 15.1%).
Figure 2.
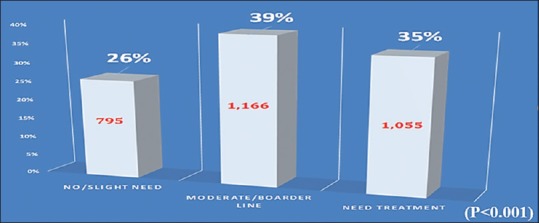
The distribution of orthodontic treatment needs among the study sample (N = 3016 subjects) using the IOTN (DHC)
Table 3.
Occlusal traits distribution based on the IOTN (DHC). Sample size (n=3016 subjects)
| Scoring occlusal trait | Dental Health Component | P | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No, slight need | Moderate/borderline | Great need | Total | ||||||||||||||||
| Grade 1 | Total | Grade 2 | Grade 3 | Total | Grade 4 | Grade 5 | Total | ||||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| Increased OJ | 910 | 30.2 | 910 | 30.2 | 327 | 11 | 103 | 3 | 430 | 14 | 63 | 2 | 9 | 0.3 | 72 | 2.3 | 1412 | 46.8 | <0.001 |
| Reversed OJ | 0 | 0 | 0 | 0 | 52 | 1.7 | 109 | 3.6 | 161 | 5.3 | 16 | 0.5 | 1 | 0.66 | 17 | 0.66 | 178 | 5.9 | <0.001 |
| Displacement | 623 | 21 | 623 | 21 | 597 | 20 | 430 | 14 | 1027 | 34 | 640 | 21 | 0 | 0 | 640 | 21 | 2290 | 76 | <0.001 |
| Missing teeth | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 360 | 12 | 271 | 9 | 631 | 21 | 631 | 20.9 | <0.001 |
| Increased OB | 0 | 0 | 0 | 0 | 654 | 22 | 151 | 5 | 805 | 27 | 46 | 1.5 | 0 | 0 | 46 | 1.5 | 851 | 28 | <0.001 |
| Open bite | 0 | 0 | 0 | 0 | 179 | 6 | 106 | 3.5 | 285 | 9.5 | 23 | 0.7 | 0 | 0 | 23 | 0.7 | 308 | 10.2 | <0.001 |
| Crossbite | 0 | 0 | 0 | 0 | 276 | 9 | 307 | 10 | 583 | 19 | 320 | 11 | 0 | 0 | 320 | 11 | 903 | 30 | <0.001 |
| Scissor bite | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 47 | 1.6 | 0 | 0 | 47 | 1.6 | 47 | 1.6 | 0.06 |
Table 4.
The association between the IOTN (DHC) groups and gender (P<0.05) (n=3016)
| No/Slight Need (n (%)) | Moderate/Borderline (n (%)) | Great need treatment (n (%)) | Total | P | |
|---|---|---|---|---|---|
| Male | 350 (11.6%) | 559 (18.5%) | 600 (20%) | 1509 (50.03%) | <0.001 |
| Female | 445 (14.8%) | 607 (20.1%) | 455 (15.1%) | 1507 (49.97%) |
On the other hand, females were significantly higher than males in the “no, slight needs” (M: 350, 11.6%; F: 445, 14.8%), and the “moderate, borderline needs” (M: 559, 18.5%; F: 607, 20.1%) categories (P < 0.001). Distribution of occlusal traits according to gender-based on the Dental Health Component Grades is illustrated in Table 5. A significant difference between males and females in the following occlusal traits; increased overjet, reversed overjet, displacement, missing teeth, and crossbite (P < 0.001). On the other hand, no significant difference between genders in: increased overbite, open bite, and scissor bite (P > 0.05). In the “no, slight” treatment needs category; males were significantly higher than females in increased overjet (M: 621, 20.6%; F: 289, 9.6%), and the opposite was reported in the displacement (F: 453, 15%; M: 170, 6%) (P < 0.001). In the “moderate/borderline” treatment needs category; males were significantly higher than females in increased overjet (M: 250, 8%; F: 150, 6%), reversed overjet (M: 143, 5%; F: 18, 0.3%), and displacement (M: 626, 21%; F: 401, 13%). On the other hand, females were significantly higher than males in crossbite only (F: 365, 12%; M: 218, 7%) (P < 0.001). In the “great” treatment needs category, males were significantly higher than females in increased overjet (M: 54, 2%; F: 18, 0.6%), reversed overjet (M: 16, 0.5%; F: 1, 0.16%), displacement (M: 515, 17%; F: 125, 4%), and crossbite (M: 240, 8%; F: 80, 3%). On the other hand, females were significantly higher than males in missing teeth only (F: 326, 11%; M: 305, 10%) (P < 0.001).
Table 5.
Occlusal trait distribution according to gender using the IOTN (DHC) (n=3016)
| Scoring occlusal trait | Dental Health Component | P | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No, slight need | Moderate/borderline | Great need | |||||||||||
| Male | Female | Male | Female | Male | Female | ||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | ||
| Increased OJ | 621 | 20.6 | 289 | 9.6 | 250 | 8 | 180 | 6 | 54 | 2 | 18 | 0.6 | <0.001 |
| Reversed OJ | 0 | 0 | 0 | 0 | 143 | 5 | 18 | 0.3 | 16 | 0.5 | 1 | 0.16 | <0.001 |
| Displacement | 170 | 6 | 453 | 15 | 626 | 21 | 401 | 13 | 515 | 17 | 125 | 4 | <0.001 |
| Missing teeth | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 305 | 10 | 326 | 11 | <0.001 |
| Increased OB | 0 | 0 | 0 | 0 | 416 | 14 | 389 | 13 | 27 | 0.9 | 19 | 0.6 | 0.35 |
| Open bite | 0 | 0 | 0 | 0 | 165 | 5.5 | 120 | 4 | 16 | 0.5 | 7 | 0.2 | 0.27 |
| Crossbite | 0 | 0 | 0 | 0 | 218 | 7 | 365 | 12 | 240 | 8 | 80 | 3 | <0.001 |
| Scissor bite | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 31 | 1 | 16 | 0.5 | 0.06 |
Discussion
In the present epidemiological cross-sectional (descriptive) study, a sample of 3016 Saudi subjects (1507 females and 1509 males) from Jeddah, Saudi Arabia, aged 14-18 years were examined and the prevalence of malocclusion, as well as the orthodontic treatment needs, was reported. The sample was collected from 32 schools and was randomly selected from each geographic area of Jeddah city (8 schools from each area) to obtain a representative sample of Jeddah population, which is considered the first population-based study that included schools from different regions of the city. Subjects with a history of orthodontic treatment and craniofacial deformities or syndromes were excluded. To assess the prevalence of the different malocclusion types, the current study used the modified Bjork et al. system.[16] While the malocclusion classification was assessed based on Angle's classification.[4] To measure the need for orthodontic treatment, the Index of Orthodontic Treatment Need (IOTN) was used in this study. The Index incorporates a Dental Health Component (DHC) and an Aesthetic Component (AC). However, in this study, only the DHC was used to assess the orthodontic treatment needs of the population. Brook and Shaw[16] have developed the Dental Health Component (DHC) and roughly modeled on the Index of the Swedish Dental Board.[16] Thus the DHC was a modified version of the Swedish index and was initially meant to guide the implementation of practical implications necessary to make clinically sound judgments in orthodontic care delivery.[15] Various epidemiological studies have been conducted in the KSA in order to estimate the prevalence of different types of malocclusion,[5,6,7,8,9,10,11,12,13,14,15,16,17] and the orthodontic treatment needs Hassan[9] and reported varied outcomes. The current study assessed 3016 (male and female) aged 14-18 years old school adolescence.
The subjects were randomly collected from all areas of Jeddah city, KSA. Out of the other studies conducted in KSA, three were in Jeddah city,[9,10] 3 were in Riyadh city,[5,8,11] 1 in Dammam city, 7, and 1 in Abha city.[17] The age of the subjects included in those studies varied, however, most of them were done on adolescent subjects.[5,6,7,8,9,10] Accordingly, our findings will be compared to the latter studies only. Also, the studies of Hassan,[9] Murshid et al.,[10] and Asiry included males and females in their studies.[5,7,10] While Feteih et al., and Al Barakati et al.[7] assessed female subjects only;[7] and Al-Emran et al.[8] assessed male subjects only.[8] The studies of Al-Emran et al.,[8] Feteih et al., and Asiry[5] were population-based conducted on schoolchildren.[5,8] While the studies of Hassan and Albarakati et al. were hospital-based on patients seeking orthodontic treatment.[7,9] However, the study of Murshid et al.[10] was conducted on patients seeking general dental treatment.[10] Of the studies conducted on adolescence, almost all of them had a sample size of 500 and more,[5,6,7,8,9,10] except for Albarakati et al.,[7] which had a sample size of 255 adolescent subjects.[7] Concerning the different malocclusion among adolescents in the present study; it was evident that Class I malocclusion showed the highest occurrence, followed by mandibular and maxillary crowding. Furthermore, spacing was more prevalent in the maxillary arch as compared to the mandibular arch. Such findings indicate the importance of space discrepancies, particularly crowding in demand for orthodontic treatment. It was interesting to note that such space anomalies were more frequent in the maxilla than in the mandible. This was in disagreement with most of the previous studies that assessed space anomalies on the Saudi population. Based on Angle's classification, Class I malocclusion was found in 57% of our sample, followed by Class II malocclusion (17%) of the subjects. The third most prevalent malocclusion was Class III malocclusion (14%). Normal occlusion was the least prevalent (12%) in our sample. Similar prevalence results were reported by Al-Emran et al.,[8] Murshid et al.,[10] Aldrees,[11] and AlQarni et al.[7,8,11,17] This was in disagreement with Albarakati et al. as well as Asiry who reported that the most common type of malocclusion was Class I, followed by Class III and then Class II malocclusion.[5,7] This might be due to the differences in the methodological assessment, sample size, gender and age, or most probably due to distinct features of the Saudi population in different regions.
The frequency of crowding discrepancy greater than 2 mm were more common in the mandible (52%) than in the maxilla (46%) in our sample, while the frequency of spacing discrepancy greater than 2 mm was recorded as 15% in the upper arch and 11% in the lower arch. This was in agreement with Al-Emran et al.,[8] Murshid et al.,[10] and Al Barakati et al.[7,8,9,10] On the contrary, Asiry reported a higher frequency of crowding and spacing in the maxillary arch.[5] Such disagreement could be related to the different age, gender distribution and hereditary factors in tooth-arch size discrepancies in the latter study. The following highest rate of malocclusion in our study was the midline shift greater than 2 mm and crossbite discrepancies. The frequency of midline shift in the mandible was more common than in the maxilla, 39.5%, and 13%, respectively. However, the posterior crossbite (25%) was more frequent than the anterior crossbite (6%). This was similar to Al Barakati et al.[7] and Asiry.[5] Around 27% of the sample in the current study had a moderate deep bite (4-6 mm), while 1.5% had a severe deep bite (>6 mm). This was in agreement with Al-Emran et al.,[8] and Murshid et al.[10] In addition, about 6% of the sample had moderate open bite 4-6 mm while severe open bite more than 6 mm was recorded in 4% of the sample. This is in agreement with Murshid et al.[10] and Asiry.[5] Almost 14% of the adolescent subjects in the current study had moderate overjet 4-6 mm, while severe overjet more than 6 mm was found in 4% of the sample. This is in agreement with Murshid et al.,[10] Al Barakati et al.,[7] and Asiry.[5] The frequency of scissor bite among the studied subjects was only 2%, which is in agreement with Al-Emran et al.[8] and Al Barakati et al.[7] According to our results, there was a significant difference between genders in most recorded malocclusion types.
This is in agreement with all studies that have been done in KSA, except for the findings of Murshid et al., who reported no statistically significant differences between males and females.[10] According to the IOTN/DHC results reported in the current study, 35% of subjects were in great need, 39% were in moderate need, 26% were in little or no need for orthodontic treatment. The results obtained from this study were in disagreement with the results of Feteih et al., who studied orthodontic treatment need in 491 female Saudi school children in Jeddah city and found a great need in 15.5%, moderate need in 18.7% and little or no need in 65.8%. It is also in disagreement with the findings of Hassan, who studied the orthodontic treatment need in 743 patients attended KAUFD and 2 private clinics in Jeddah city on both genders (male and female) and found a great need in 71.6%, moderate need in 13.2% and little or no need in 15.2%. 9 This disagreement could be related to the different age and gender distribution in the latter studies. With regard to the occlusal trait distribution, the highest prevalence was for displacement, which affected more than 76% of the subjects. This finding was similar to Feteih et al. and Hassan.[9] This was followed by increased overjet (46.8%), crossbite (30%), increased overbite (28%), missing teeth (21%), open bite (10.2%), reversed overjet (5.9%), and the least was scissor bite (1.6%). In contrary, the studies of Feteih et al. and Hassan[9] found a higher percentage of crossbite problems than overjet.[9] Hassan also reported a higher percentage of open bite problems (20%) than the current study (Hassan, 2006). In conclusion, the current study provided a baseline for the prevalence of malocclusion and orthodontic treatment needs in Jeddah city. Despite, it also had some limitations. The socio-economic and aesthetic issues were not considered. In addition, the sample was collected from governmental schools only. The distinction between missing teeth and impacted teeth was not made due to the lack of radiographic images of the samples.
Conclusions and Recommendations
A significantly high prevalence of malocclusion (88%) and high orthodontic treatment need (74%) were reported.
The most common malocclusion was Class I (57%) and the most common orthodontic treatment need was moderate to borderline (39%).
There were significant gender differences in most of the malocclusion traits.
The public dental providers to prioritize their treatment and make orthodontic treatment as one of the most important services to be considered can use the outcomes.
Future studies are needed to assess malocclusion in the whole Kingdom in order to increase the number of orthodontics providing necessary services.
Financial support and sponsorship
Nil.
Conflict of interest
The authors declare that there is no conflict of interest.
Acknowledgements
First of all, I offer my greetings and gratitude to my supervisors Prof. Zuhair Murshid and Prof. Fahd Alsulimani, for all the effort and motivation to help me complete this work
I also wish to acknowledge with special thanks, the General Directorate of Education in Jeddah city
Lastly, many thanks and appreciation to all the faculty members in the Orthodontics department, my parents, wife, brothers, sisters, colleagues, and friends who supported me in preparing this work.
References
- 1.Housten WJ. Walther's Orthodontic Notes. 4th ed. Oregon, USA: The Stonebridge Publishers; 2000. [Google Scholar]
- 2.Shivakumar KM, Chandu GN, Reddy VS, Shafiulla MD. Prevalence of malocclusion and orthodontic treatment needs among middle and high school children of Davangere city, India by using the Dental Aesthetic Index. J Indian Soc Pedod Prev Dent. 2009;27:211–8. doi: 10.4103/0970-4388.57655. [DOI] [PubMed] [Google Scholar]
- 3.Joshi N, Hamdan AM, Fakhouri WD. Skeletal malocclusion: A developmental disorder with life-long morbidity. J Clin Med Res. 2014;6:399–408. doi: 10.14740/jocmr1905w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Angle EH. Malocclusion of the teeth. In: Moyers RE, editor. Handbook of Orthodontics. 4th ed. Chicago: Yearbook Med Publ; 1988. pp. 186–8. [Google Scholar]
- 5.Asiry MA. Occlusal status among 12-16-year-old school children in Riyadh, Saudi Arabia. J Int Oral Health. 2015;7:20–3. [PMC free article] [PubMed] [Google Scholar]
- 6.Prabhakar RR, Saravanan R, Karthikeyan MK, Vishnuchandran C, Sudeepthi Prevalence of malocclusion and need for early orthodontic treatment in children. J Clin Diagn Res. 2014;8:ZC60–1. doi: 10.7860/JCDR/2014/8604.4394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Albarakati SF, Taher S. Malocclusion traits in Saudi females seeking orthodontic treatment. Pak Oral Dent J. 2010;30:127–32. [Google Scholar]
- 8.Al-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dent Oral Epidemiol. 1990;18:253–5. doi: 10.1111/j.1600-0528.1990.tb00070.x. [DOI] [PubMed] [Google Scholar]
- 9.Hassan AH. Orthodontic treatment needs in the western region of Saudi Arabia: A research report. Head Face Med. 2006;2:2. doi: 10.1186/1746-160X-2-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Murshid ZA, Amin HE, Al-Nowaiser AM. Distribution of certain types of occlusal anomalies among Saudi Arabian adolescents in Jeddah city. Community Dent Health. 2010;27:238–41. [PubMed] [Google Scholar]
- 11.Aldrees AM. A pattern of skeletal and dental malocclusions in Saudi orthodontic patients. Saudi Med J. 2012;33:315–20. [PubMed] [Google Scholar]
- 12.Almasri M. The prevalence of skeletal malocclusion in the southern Aseer Region of Saudi Arabia. Am J Med Sci Med. 2014;2:13–5. [Google Scholar]
- 13.Kumar P, Londhe SM, Kotwal A, Mitra R. Prevalence of malocclusion and orthodontic treatment need in schoolchildren–An epidemiological study. Med J Armed Forces India. 2013;69:369–74. doi: 10.1016/j.mjafi.2012.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bellot-Arcís C, Almerich-Silla JM. Psychosocial impact of malocclusion in Spanish adolescents. Korean J Orthod. 2013;43:193–200. doi: 10.4041/kjod.2013.43.4.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod. 1989;11:309–20. doi: 10.1093/oxfordjournals.ejo.a035999. [DOI] [PubMed] [Google Scholar]
- 16.Björk A, Krebs AA, Solow B. A method for epidemiological registration of malocclusion. Acta Odontol Scand. 1964;22:27–41. doi: 10.3109/00016356408993963. [DOI] [PubMed] [Google Scholar]
- 17.AlQarni MA, Banihuwaiz AH, Alshehri FD, Alqarni AS, Alasmari DS. Evaluate the malocclusion in subjects reporting for orthodontic treatment among Saudi population in Asser region. J Int Oral Health. 2014;6:42–6. [PMC free article] [PubMed] [Google Scholar]